ic05-l: controversies and advances in aseptic necrosis of
TRANSCRIPT

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH.
No statement or presentation made is to be regarded as dedicated to the public domain.
IC05-L: Controversies and Advances in Aseptic
Necrosis of the Hand and Wrist
Moderator(s): David M. Lichtman, MD
Faculty: Claudia Lamas, MD, PhD, Gregory I. Bain, FRACS, PhD, Robert M. Szabo, MD, MPH and Ryosuke
Kakinoki, MD, PhD
Session Handouts
76th Annual Meeting of the ASSH
September 30 – October 2, 2021
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

4/9/21
1
The case for a biologic etiology of Kienböck´s disease
C. Lamas, MD, Ph DHand Unit and Upper Extremity. Department of Orthopaedic Surgery. Hospital de la Santa Creu i Sant Pau. Associate Professor Universitat Autònoma de [email protected]
Etiology: Historical background
Hypothesis by R. Kienböck (1910):
“The disease is a traumatic lesion of the lunate. It apparently arises as a result of a contusion or sprain of the wrist, with tears of the interosseous ligaments and blood vessels. The disturbance of blood supply leads to progressive weakening and final decay of the affected lunate”.
The strongest argument against this hypothesis is that even complete dislocation of the lunate is rarely ever followed by lunate necrosis.
KIENBÖCK R. (1871-1953). “Über traumatische Malazie des Mondbeins und ihre Folgezustande: Eutartungs formen und Kompressionsfrakturen”. Fortschr. a.d. Geb. d. Röntgensti, 16, 11, 78, 1910.

4/9/21
2
Etiology: Historical background
Hypothesis by Marek (1957):
“The pathogenesis of avascular necrosis of the lunate has been explained by traumatic interference with the arterial blood supply, followed secondarily by compression and fragmentation of the bone”.
SCAPHOID
LUNATERSL LIG.
SLIL TEAR
Etiology: Historical backgroundHypothesis by Stahl (1947):
“There is a primary compression fracture which does not heal because the wrist is not immobilized”.
The strongest argument against this hypothesis is that the author could demostrate only four freshfractures out of 184 cases presented and that 97% of cases occurred in manual workers.
The concept of “occupational lunatomalacia” caused by manual work, is supported by Therkelsen(1949) who found 98 manual workers in a group of 107 patients.However, these studies collected cases from hospitals dedicated to the care of manual workers andcontradict the results of series collected in general hospitals, and cannot explain the cases in children,adolescents, adults with sedentary work and elderly.

4/9/21
3
Etiology
Age at the onset of the disease
Children: 7-12 yearsAdolescent: 13-19 yearsAdults: 20-55 yearsElderly: Patients older than 56 years
12 years 14 years
23 years
Biological Pathomecanics
DIRECT VESSEL BREAK OR LIGAMENT DISRUPTIONS
LACK OF CONSISTENT ARTERIAL SUPPLY OF
THE LUNATE
EMBOLIC PROCESSOBLITERATING ENDARTERITIS
VASCULITIS IMMUNOLOGICAL
DISEASES
GENETIC AND FAMILIARCONGENITAL
HYPERCOAGULOPATHY
CORTICOSTEROID THERAPY
LUNATE MORPHOLOGY
NEUROHORMONALBLOOD SUPPLY INTERRUPTION
BONE NECROSIS
PATHOLOGIC FRACTURE
BONE COLLAPSE
CARPAL INSTABILITY
OSTEOARTHRITIS
VIRUS INFECTION

4/9/21
4
• Types I, II and III (Antuña-Zapico, 1966): The lunate was classified into three different shapes on the basis of the angle between the lateral scaphoid side of the lunate and the proximal radial side of the lunate.
Type I Type II Type III
Etiology Lunate bone morphology
Lunate Type I is associate with KD
Type II
2
Arthrosis capitate-hamate: There was a correlation between arthrosis at the hamate and the presence of a lunate facet for the hamate.
Lunate bone morphology
Types I and II (Viegas, 1990):
Type I has a single articular facet for the capitateType II has a medial facet that articulates with the hamate
Type I
112
1
21

4/9/21
5
Etiology: Intraosseus arterial pattern of the lunate bone and its relation to avascular necrosis
Lee (1963)
Arterial supply of 53 normal lunatesTechnique described by Trueta & Harrison (1953)Lunate is supplied via the dorsal and palmar interosseous surfaces alone and that the inteosseous vascular pattern falls into one of the three groups:
GROUP A. A single palmar or dorsal vessel crossing the bone obliquely (26%) GROUP B. Palmar and dorsal vessels which do not anastomose (7.5%)GROUP C. Palmar and dorsal vessels which anastomose (66.5%)
Etiology: Intraosseus arterial pattern of the lunate bone and its relationto avascular necrosis
Lee (1963)
“A transverse compression fracture across the proximal partsof the lunates will deprive the proximal part of the bone of its blood supply leading to Kienböck´disease. This fracture will cross and interrupt the arterial branches as they run between the anastomotic vessels and the proximal surface of the lunate”.

4/9/21
6
Etiology: Intraosseus arterial pattern of the lunate bone and its relation to avascular necrosis
Gelberman (1980)
35 fresh cadaver limbs. Spalteholz method.
The lunates receives is blood supply from either palmar and dorsal sources (80%) or from the palmar aspect alone (20% of specimens).
Hyphotesis: “The vascular patterns support a theory of compression fracture from repeated trauma as the most likely cause of Kienböck´s disease”.
Gelberman et al. The vascularity of the lunate bone and Kienböck´s disease. J hand Sur Am 1980; 5 (3): 272-278Gelberman RH et al. The arterial anatomy of the human carpus. Part I. The extraosseous vascularity. J Hand Surg Am 1983; 8 (4): 367-375.Panagis JS, Gelberman RH. Taleisnik J, Baumgaertner M. The arterial anatomy of the human carpus. Part II. The intraosseous vascularity. J Hand Surg Am 1983; 8 (4): 375-382.Freedman DM, Botte MJ, Gelberman RH. Vascularity of the carpus. Clin Orthop 2001; 383: 47-59.
“The vascularity formed one of three consistent patterns with anastomoses of dorsal and volar vessels in each specimen: The Y pattern occurs in 59%, the I pattern in 30% and the X pattern in 10% of specimens. The dorsal and palmar vessels anastomose intraosseously just distal to the midportion of the lunate. The proximal pole has relatively less vascularity”.
Cross section of the wrist and Spalteholz technique. Intraosseous vascular pattern formed by two dorsal and one palmar vessels: Y-pattern of Gelberman.

4/9/21
7
• 27 adult hands from fresh cadavers (18 male - 12 female). Mean age 73 years (62-90 yrs). • Specimens were injected through the brachial artery with coloured latex. • Dissected using magnifying loupes and processed using the Spalteholz technique. • We investigated the lunate morphology and the extra- and intraosseous blood supply to the lunate bone.
Etiology: Intraosseus arterial pattern of the lunate bone and its relation to avascular necrosis
Spalteholz technique
The lunates were immersed in ethanol and dehydrated: - Ethanol (4 weeks);- Methylbenzene (2 weeks); - Mixture liquid made with one part of methyl salicylate and two parts of benzyl benzoate (2 weeks).
Etiology: Intraosseus arterial pattern of the lunate bone and its relation to avascular necrosis
4/9/21
8
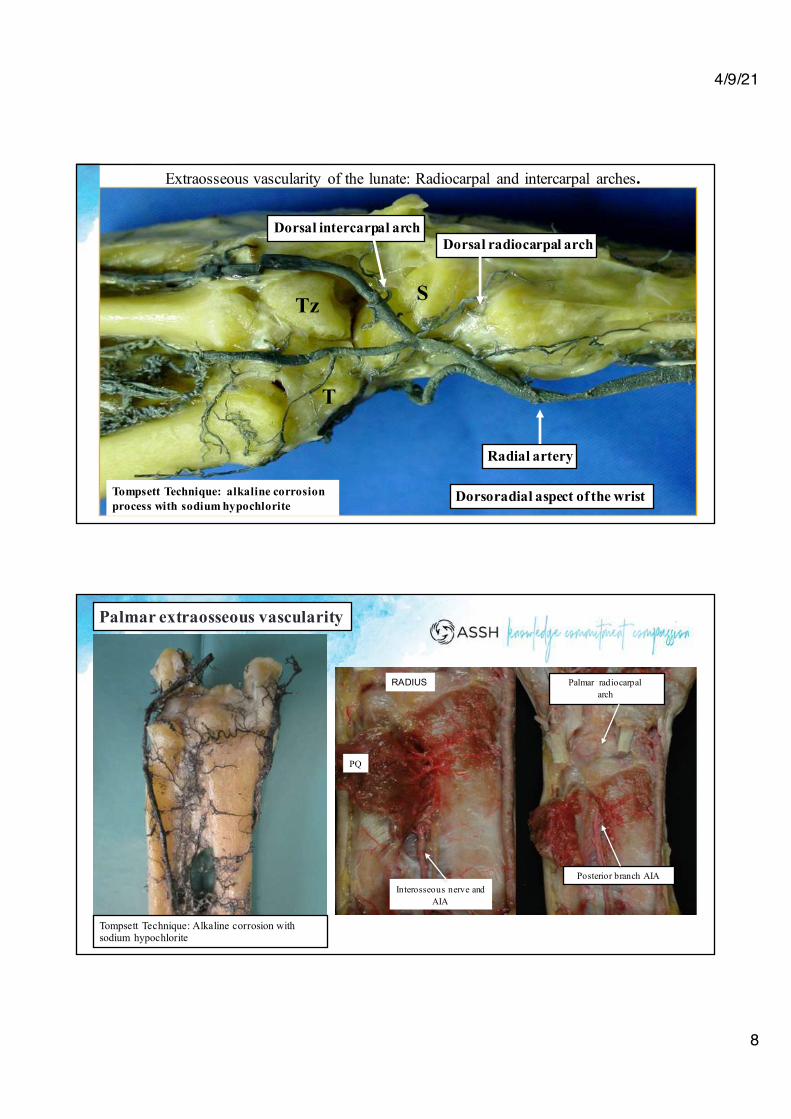
Extraosseous vascularity of the lunate: Radiocarpal and intercarpal arches.
Radial artery
Dorsal radiocarpal archDorsal intercarpal arch
Dorsoradial aspect of the wrist
T
Tz S
Tompsett Technique: alkaline corrosion process with sodium hypochlorite
Tompsett Technique: Alkaline corrosion with sodium hypochlorite
Palmar extraosseous vascularity
RADIUS
PQ
Interosseous nerve and AIA
Palmar radiocarpal arch
Posterior branch AIA

4/9/21
9
Palmar lunate vascularity is supplied by branches from a palmar plexus formed directly from ulnar, radial and AIA vessels.
Anterior branch of the AIAPalmar carpal arch
Radial artery
Coronal section and Spalteholz technique (Diaphanization)
Branches from the AIA provide blood to the lunate. The vessels perforate the bone.
Coronal section and Spalteholz technique (Diaphanization). Arterial injection, Spalteholz-cleared specimen

4/9/21
10
Dorsal foramina
Dorsal aspect of the lunate showing three dorsal foramina and blood vessels withanastomoses entering the bone.
C.Lamas.LaenfermedaddeKienböck.BoschPublisher2005.
Lunate
RLT and ULT lig.Radioscapholunate lig.Testut - Kuentz
Scaphoid

4/9/21
11
CrosssectionandSpalteholztechnique.Arterialsupplyofthedorsalandpalmaraspectofthewrist.
Lunate
Radioscapholunate lig. RLT and ULT lig.
Coronal sectionand intraosseousvascularityofthelunatebone.
Lunate Scaphoid
Radio-scapho-lunate lig.
LunateTriquetrum
RLT and ULT Ligs
Microscopic image: vessels enter the lunate from RSL and ULT ligaments

4/9/21
12
Embolic process, obliterating endarteritis
Axhaussen (1924) was the first author to suggest that Kienböck´s disease was an embolic process.
Santozki (1929) described an inflammatory vascular process resembling and “obliterating endarteritis”.
Obliterating endarteritis is a medical condition of the vessels where there is severe proliferating inflammation of the inner lining intima of an artery resulting in occlusion in the lumen of the artery.
Hematoxylin and eosin staining demonstrating bone marrow necrosis.
Kaur G et al. (2019). Bone Marrow Necrosis and Fat Embolism in a Patient with Sickle Cell Crisis, a Fatal Complication. Int J Pathol Clin Res 5:104.

4/9/21
13
Rheumatoid disorders
Patient with Systemic Lupus Erithematosus34-years-old housewife. No history of trauma or overuse of the hand Bilateral KienböckHigh dose of corticosteroid use
Rheumatoid disorders
4/9/21
14
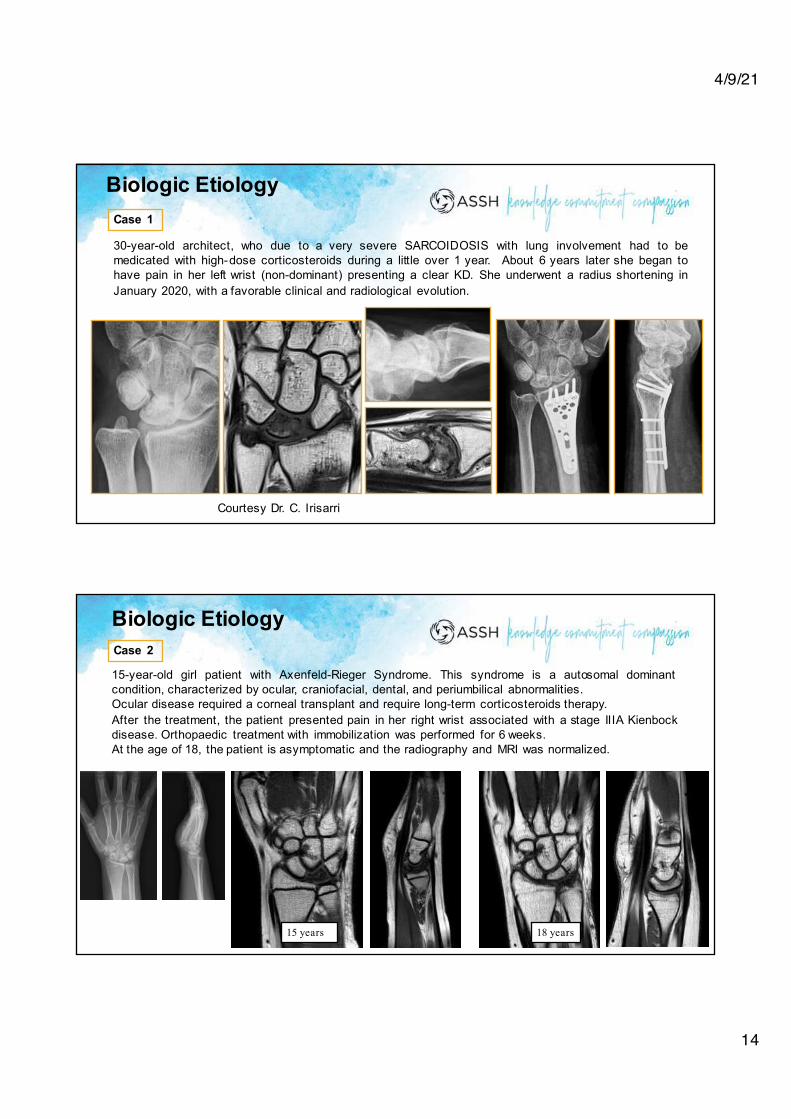
Biologic Etiology
30-year-old architect, who due to a very severe SARCOIDOSIS with lung involvement had to bemedicated with high-dose corticosteroids during a little over 1 year. About 6 years later she began tohave pain in her left wrist (non-dominant) presenting a clear KD. She underwent a radius shortening inJanuary 2020, with a favorable clinical and radiological evolution.
Case 1
Courtesy Dr. C. Irisarri
Biologic EtiologyCase 2
15-year-old girl patient with Axenfeld-Rieger Syndrome. This syndrome is a autosomal dominantcondition, characterized by ocular, craniofacial, dental, and periumbilical abnormalities.Ocular disease required a corneal transplant and require long-term corticosteroids therapy.After the treatment, the patient presented pain in her right wrist associated with a stage IIIA Kienbockdisease. Orthopaedic treatment with immobilization was performed for 6 weeks.At the age of 18, the patient is asymptomatic and the radiography and MRI was normalized.
15 years 18 years

4/9/21
15
Congenital hypercoagulopathy
JHandSurgEur,2019;44,8:859-861
Virus infection
Osteomyelitis of low grade virulence in the lunate has been suggested as a possible cause of the KD.
Madier A, Segal (1937). Maladie de Kienböck bilaterale du semilunaire carpien. Mem. Acad. Chir, 63, 191.Brown P, Crane L (2001). Avascular Necrosis of Bone in Patients with Human Immunodeficiency Virus Infection: Report of 6 Cases and Review of the Literature. Clinical Infectious Diseases 2001; 32:1221–6
Courtesy Dr. C. Irisarri

4/9/21
16
Genetic and familiar cases
Ringsted (1932). Familiar cases. Therkelsen and Andersen (1949). Individual predisposition. Genetic.
This study suggest that there is a potential genetic contribution to the etiology of KD and that the disease has a significant association with several risk factors. Kazmers et al. J Hand Surg Am 2019.
Kienbock's disease has different anatomical risk factors, mechanical causes, andbiological causes that try to explain its appearance in differents group of people :children, adolescents, manual workers, non-force workers and elderly.
A single cause, hypothesis or factor is not able to explain all patients withKienbock's disease.
Conclusion

�1
Greg Bain Adelaide, Australia
Thecaseforamechanicale1ologyofKienbock’sDisease
2
Low Risk
1
Lunate-Type1(Viegas)-Type1AZTrapezoid-Smaller-SingleVessel-Uncovered
At Risk
Ulnar-Negativevariance
Radial-Flatterinclination
• Spanning Trabeculi
• Single SBP 0.1mm
• Low S Bain J Ortho Res 14
• Double SBP
Radial Ulnar
Anatomy
!5
CT Scan
Osseous
G Bain, Ch 7 KD Book
Nut Cracker
ICantilever
G Bain, Ch 7 KD Book

Radial
0.1mm
Stress Fracture
Capitate Nut Cracker
CORONALFRACTURESCoronalfracture=“nutcracker”
G Bain, Ch 7 KD Book
AXIALFRACTURES
“shearing”
CORONALFRACTURES
SAGITTALFRACTURES
Nut-Cracker
COMPLEX
Kienbock’s Lunate
n=5
• Low S Bain J Ortho Res 14
FracturesResorption
Joint Irregularity
Kienbock’s Lunate• Low S Bain J Ortho Res 14
!12
Radial Template
Kissing Lesion
Impaction fracture
Comminution
Collapse of radial column
2021

!13
Lunate Collapse
Sclerosis
Ulnar styloid Copyright Dr Gregory Bain
Movement through lunate
2021
4D CTMFo IIIC
Interosseous LigamentAvulsions
SRL
SL
LT
SLLT
T SL
Internal lunate instability
Osteoligamentous Units
Ulnar Translocation
Scapholunate equivalent KD Intrinsic Instability
Kienbock’s diseaseKH - II
SL
LT
SRL
Volar lunate fragment
Volar Lunate fracture in progression?
SRL
TS L
Avulsion
Impingement
Volar lunate fragment
Locked In-progress
Kienbock’s Disease
Central column collapse
Lunate fragmentation
Radial column collapse
DRC / DIC maintained Carpal collapse “Pseudolaxity”
Carpus settles -Ulnar translocation
Kienbock’s Disease
Central column collapse
Lunate fragmentation
Radial column collapse
KD Extrinsic Instability

Venous HT
Volar
Generalised Venous HT
Stress fracture
Venous Drainage
Copyright HV Crock AO
Subarticular Plexus - Parallel
G Bain, Ch 7 KD Book
!20
Normal
Ischemia
Arterial Inflow
Venous Outflow
Compartment Syndrome of Bone
Sinusoids
Intra-osseous Pressure, Increases - Ext and KD Jensen JHS 93
5 -10 mmHg
G Bain, Ch 7 KD Book
Subchondral fractures (Crest)
Coronal fractures
Sagittal fractures
Ligament avulsions
Cantilever - forces
Localised compression“Nut cracker”
Tensile forces
Forces on the lunate
Shear force
Fluoro
!22MRI - perfusion Histo - NecrosisGross - Necrotic
4D CT Arthroscopy
LunateMechanical, BUT ……
Acknowledgements
David LichtmanSimon Mac Lean
JWS 2016
2021
!24
4D CT Arthroscopy
LunateMechanical, BUT ……
Venous HTAnatomy Compartment Syn
Fluoro

IC05: Controversies and Advances in Aseptic Necrosis of the Hand and Wrist
The Case for Non-Operative Management of Kienböck’s Disease
Robert M. Szabo, M.D., M.P.H.
1
Kienbӧck’s Disease
Previous description of lunate osteonecrosis from cadavers (1843 Peste)
1910 Kienbӧck’s publication was first clinical description of lunatomalacia
Kienbӧck felt disease was result of disturbance of nutrition to the lunate secondary to
ligamentous injury from wrist sprain/contusion
Robert Kienbock was a Viennese radiologist
Definition
Avascular necrosis of lunate
Leads to lunate collapse
Progressive disease with carpal collapse and finally carpal arthritis
Expectation Paradox
Patients’ expectations regarding an intervention tend to increase as the intervention moves
up the “Ladder of Invasiveness”.
Yet as we move this ladder, the interventions seem to be supported by less and less
evidence
Medical decisions are complicated
2 ways to learn about different outcomes
One’s experience (uncontrolled clinical series)
Method OK if outcomes are obvious & immediate, and treatments cause
dramatic changes in outcomes
Clinical research
systematic assignment of treatments and observation of outcomes
This is Evidenced Based Medicine
“Happiness” factor in our patients {Kevin Chung JHS 33A 2008}
Patient satisfaction is highly dependent on intangible factors, such as patients’ underlying
psychosocial state and their expectations, rather than a scientific standard of the quality of
care that they receive

IC05: Controversies and Advances in Aseptic Necrosis of the Hand and Wrist
The Case for Non-Operative Management of Kienböck’s Disease
Robert M. Szabo, M.D., M.P.H.
2
Kienbock’s disease is progressive and passes through the stages as described by Lichtman.

IC05: Controversies and Advances in Aseptic Necrosis of the Hand and Wrist
The Case for Non-Operative Management of Kienböck’s Disease
Robert M. Szabo, M.D., M.P.H.
3
Retrospective analysis of 66 patients: No significant difference was found between surgical and
conservative treatment

IC05: Controversies and Advances in Aseptic Necrosis of the Hand and Wrist
The Case for Non-Operative Management of Kienböck’s Disease
Robert M. Szabo, M.D., M.P.H.
4
Our results are consistent with the observations of Beckenbaugh (1980), who in a series of 46
patients with Kienbock’s disease found that the patients were relieved of pain and had
functionally good results, whether they were treated or not, and regardless of the surgical
treatment.

David M. Lichtman, MDASSH ICL # 06September 30, 2021San Francisco, CA
Stan Ollie
Kienböck’s Disease
A Precision Algorithm for the
Twenty First Century

Wikipedia:
“A medical [surgical] model that proposes thecustomization of healthcare [surgical care], withmedical [surgical] decisions, treatments,practices, or products being tailored to asubgroup of patients, instead of aone-drug-fits-all model.”
“Precision Medicine”

MY DILEMMA1977 (!!)
ØKienbock’s disease was a chronic disorder which presents different surgical challenges over time.
ØThere was no algorithm to guide treatment selection from a wide array of choices
DML
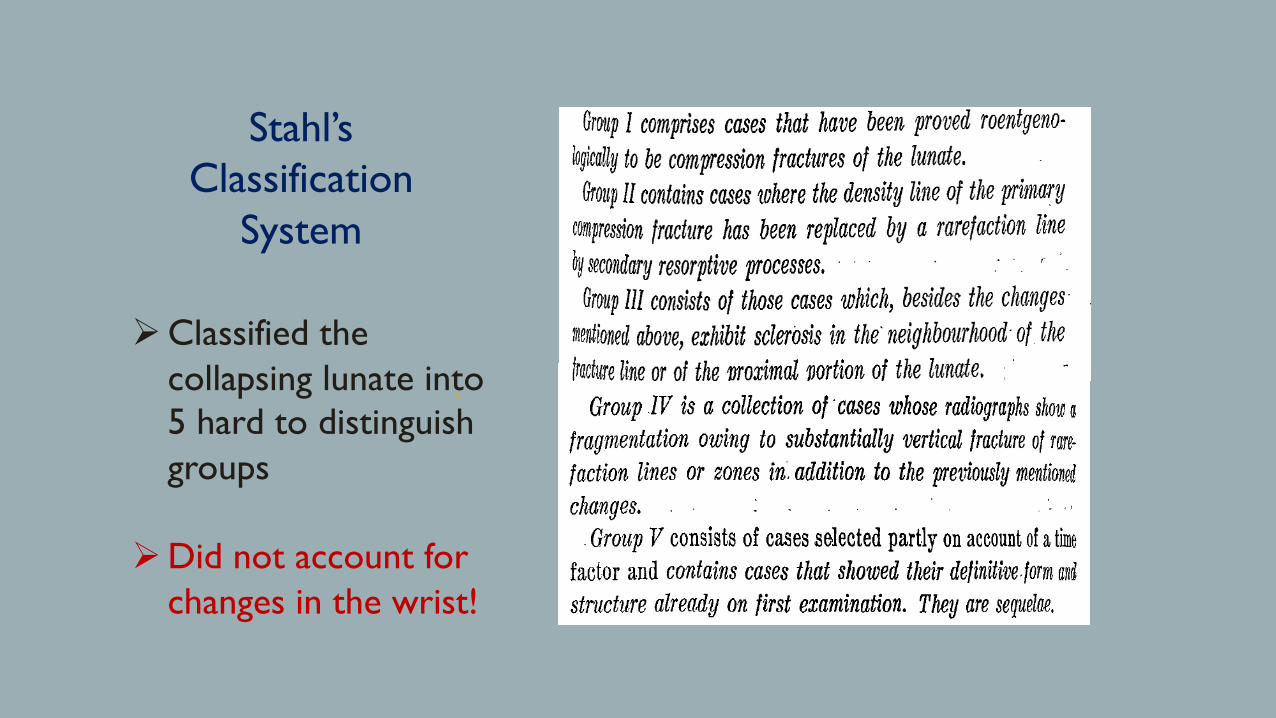
Stahl’s Classification
System
ØClassified the collapsing lunate into 5 hard to distinguish groups
ØDid not account for changes in the wrist!

Solution:Set the Stage
Develop an x-ray staging system that documents progressive lunate and wrist pathology.
JBJS April 1977
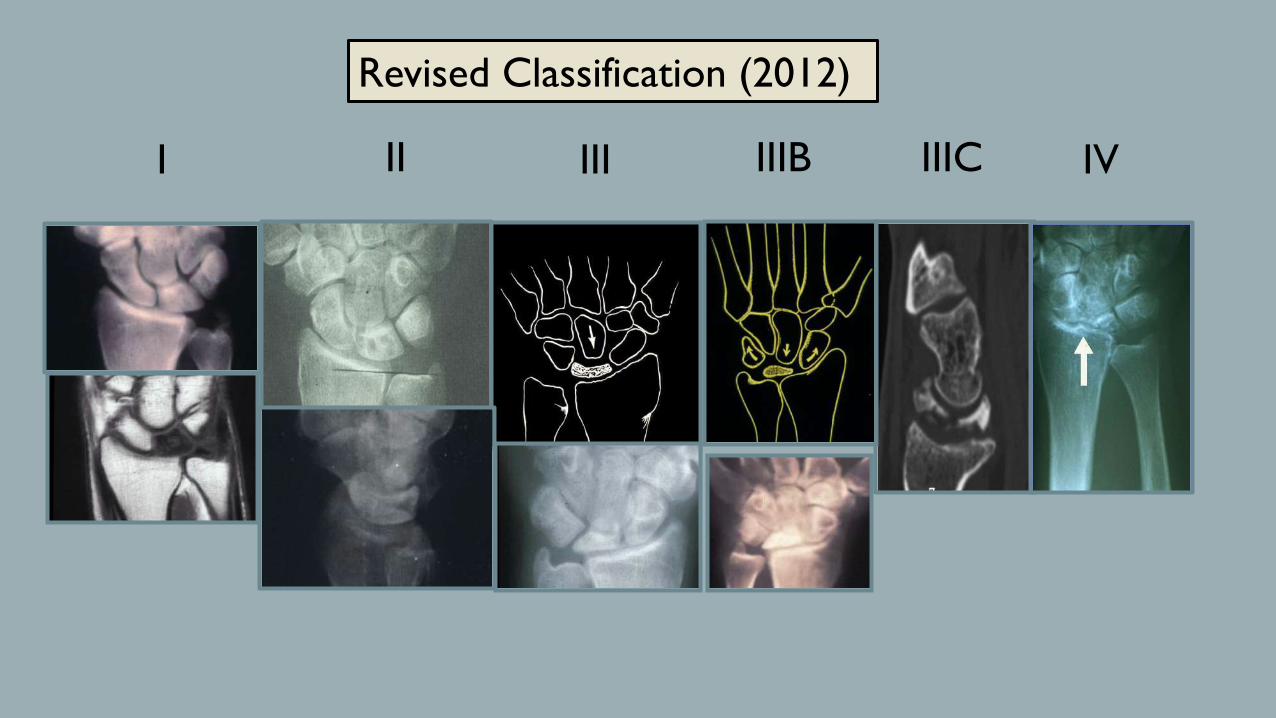
I IIIB IVIIIII IIIC
Revised Classification (2012)

TREATMENT BY STAGE/VARIANCE(LICHTMAN)
Stage Variance TreatmentI (+/-) Immobilization (3-6 mos.)II/III-A (-) Radial shorteningII/III-A (+) Capitate shorteningIII-B (+/-) SC (STT) fusionIII-C (+/-) Excise lunate + SC fusionIV (+/-) Wrist Arthrodesis

RECENT ADVANCESMOSTLY 21 ST CENTURY
Is an X-ray Based Algorithm Still Valid?
1. Age matters: Better understanding of natural history in children and the elderly
2. Ability to predict revascularization potential via gadolinium MRI sequences
3. Ability to determine cartilage viability via arthroscopy
4. Additional treatment options

“Teenböck’s Disease”
1. Better understanding of natural history in children and the elderly

M.H.-16 yr. old female gymnast with 5 mos. wrist painOctober 15, 2001

T-1 weighted MRI T-2 weighted MRI
M.H.-October15, 2001

M.H.-July 12, 2002
T-1 weighted T-2 weighted

DIFFERENT PATHWAY IN “THE ELDERLY”
Taniguchi et al…
• Studied 14 pts. with onset > 60
• Etiology different?
ØUlnar minus less frequent
ØWomen more frequent
ØRelated to osteoporosis?
• Natural history different
ØCollapse progressed in all
ØConservative treatment effective

Kienböck’s in “The Elderly”

ØEnhanced signal on standard T2 eitherGOOD or BAD
ØFibro-vascular tissue in lunate = GOODØEdema in/around necrotic lunate = BAD
But…ØEnhanced signal on gadolinium infused fat
suppressed T1 images always indicates fibro-vascular regenerative tissue = GOOD
Rainer Schmitt, M.D.Munich, Germany
T-2
FS Gad+ T-1
2. Ability to predict revascularization potential via special MRI sequences

Standard T1Fat Sup. T1 + Gad
Pattern AGood Prognosis
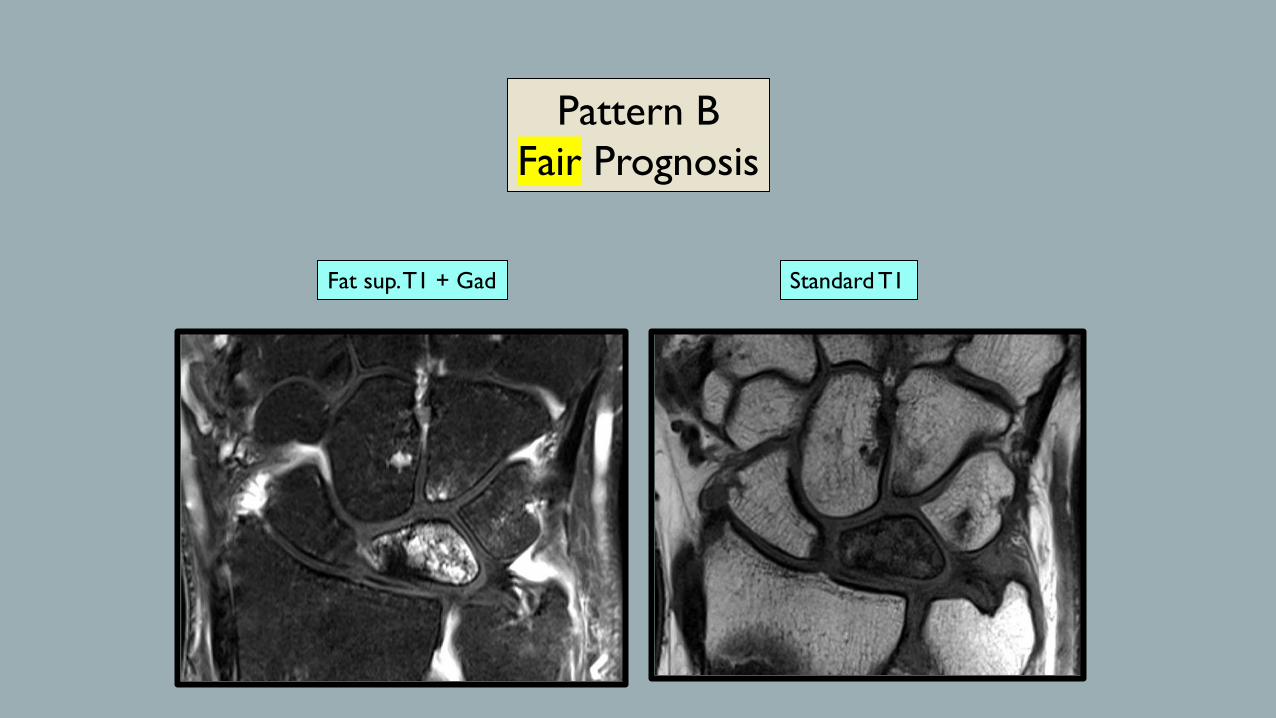
Standard T1Fat sup. T1 + Gad
Pattern BFair Prognosis
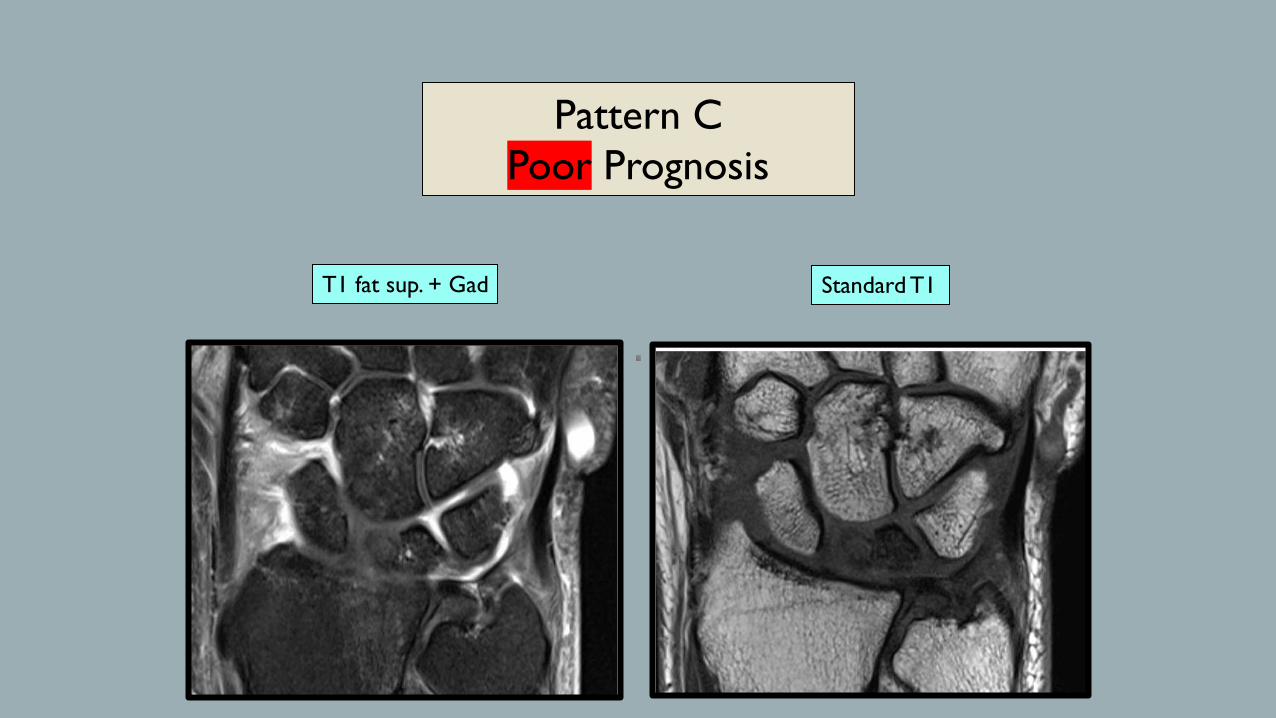
T1 fat sup. + Gad Standard T1
Pattern CPoor Prognosis

• Described by Bain and Begg, 2006
• Classification and Rx based on arthroscopic location of “non-functional” articular surfaces of the lunate
• Not necessarily in chronological sequence (2b may be an earlier stage)
• What really is non-functional (arthroscopic or eyeball)?
3. Ability to determine cartilage viability via arthroscopy

• Intact: • Bain Class 0 • (Schmitt C add revascularization)
• Compromised: • Bain 1: Salvageable w. vascularized osteochondral graft-MFT• Bain 2b + Schmitt A,B: Salvageable w. compression screw
• Non-salvageable: • Bain 2b + Schmitt C: Excise lunate, plus reconstriction
Ability to determine lunate salvageability (in adults) Depends on Bain and Schmitt stages!!
Intact Non-salvageableCompromised
SchmittA,B
SchmittCSchmitt
A,BSchmitt
C
Bain stages 2a, 3 and 4 -----
Not isolated to lunate bone
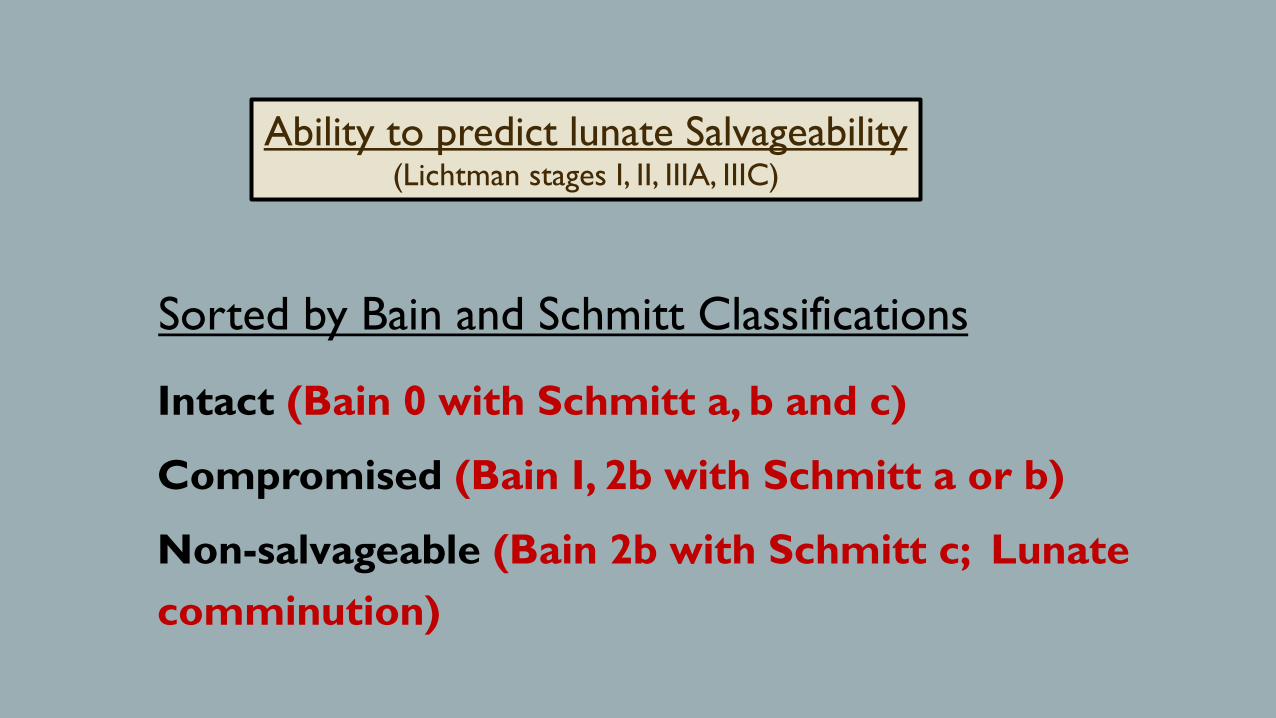
Intact (Bain 0 with Schmitt a, b and c)
Compromised (Bain I, 2b with Schmitt a or b)
Non-salvageable (Bain 2b with Schmitt c; Lunate comminution)
Ability to predict lunate Salvageability(Lichtman stages I, II, IIIA, IIIC)
Sorted by Bain and Schmitt Classifications

Minimally Invasive procedures:Temporary STT PinningLunate Forage (open or arthroscopic)Arthroscopic debridement/synovectomy
Combined revascularization/reconstruction:Free MFT pedicle bone/cartilage graft
Miscellaneous:Capitate lengtheningPyrocarbon implantsArthroscopic assisted fusionsStem Cell Grafts***
4. Additional treatment options

How can we apply this new information…
Advances in: Ø Knowledge of the natural history in
kids and the elderly Ø Ability to detect revascularization
potential w. gadolinium scansØ Ability to determine cartilage viabilityØ Surgical technology
...to create a more nuanced and patient specific “precise” treatment algorithm.

A. What is the patient’s Age?
B. Is the disease limited to the lunate Bone?
C. What is the state of the Carpus?
D. What is the patient Desire?
E. What is the surgeon’s Expertise?

A. Age of pt: Children/Elderly No need for staging…
A1. < 15 years
A2. 15-20 years
A3. > 70 years
B. Adult-Limited to Lunate Bone Applicable to Lichtman stages I-IIIA, IIIC.
B1. Intact (Bain 0)
B2. Compromised (Bain1; Bain 2b [Lichtman IIIC] with Schmitt a)
B3. Non-salvageable (Bain 2b-with Schmitt c, Lunate comminution)
C. Adult-Carpus Affected
C1. Carpal instability with intact radioscaphoid RS and RL articulations (IIIB)
C2. Scaphoid and/or lunate fossa compromised w/wo carpal collapse (Includes Bain 2a, 3-4)
C3. Extensive wrist degeneration (Stage IV-KDAC)
Unified Classification for Kienböck’s

A1. Under 15: -Non-invasive
A2. 15-20 years:-Noninvasive 0-3 mos.-Minimally invasive
A3. Elderly:-Medical workup:
Autoimmune disorder Osteoporosis
-NSAIDS, Splint, Physical therapySynovectomy (Arthrodesis/TWA)
Rx AlgorithmClass “A” (Children/Elderly)
All Stages (Lichtman/Bain/Schmitt)

B1. Salvageable lunate (Bain 0):-Radial Shortening*** (ulna minus) or forage-Capitate shortening*** (ulna plus) or forage***If Schmitt C add revascularization
B2. Compromised lunate Bain 1- MFT free vascular graft or SC fusion or PRCBain 2b with Schmitt A, B- Lunate screw fixation or PRC
B3. Non-salvageable lunateBain 2b with Schmitt CComminuted Lunate
-Excise lunate (esp. w. Synovitis) and:SC or Graner fusionCapitate lengtheningLunate prosthesis
*Bain 2a, 3 and 4 (see adult, wrist involved)
Class “B” (adult and limited to lunate)(Lichtman stages I, II, IIIA, IIIC)
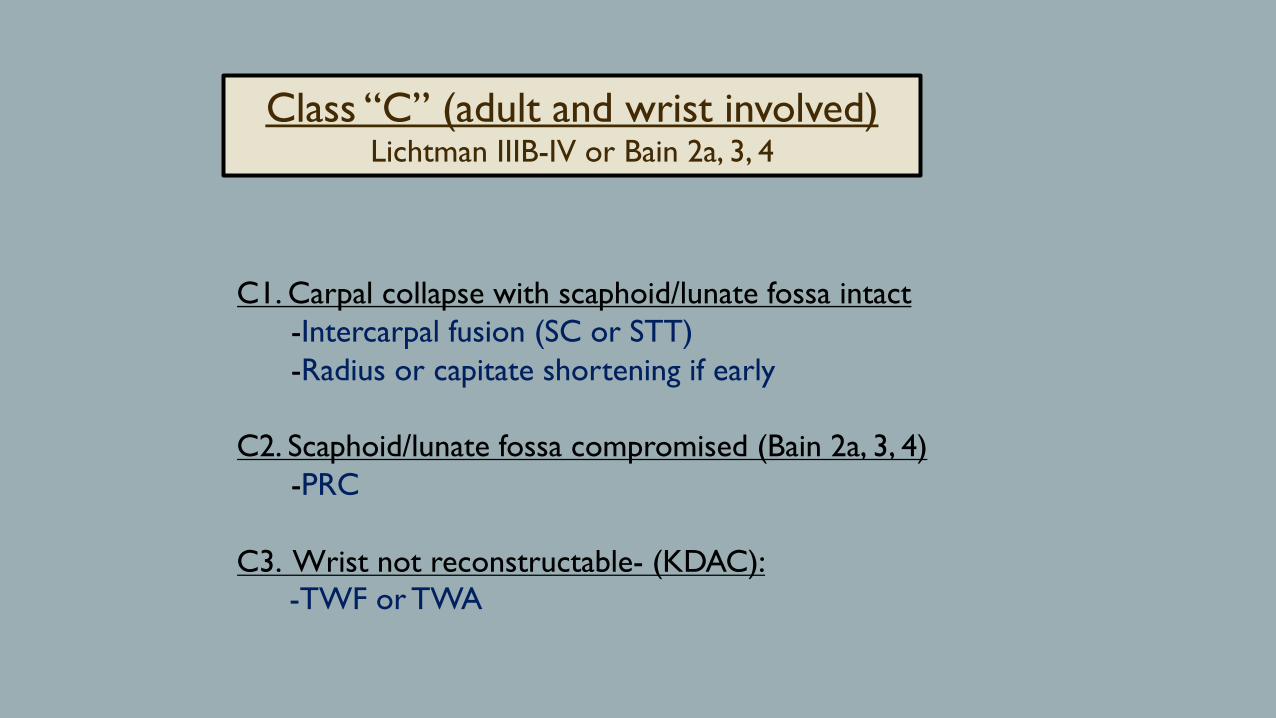
C1. Carpal collapse with scaphoid/lunate fossa intact-Intercarpal fusion (SC or STT)-Radius or capitate shortening if early
C2. Scaphoid/lunate fossa compromised (Bain 2a, 3, 4)-PRC
C3. Wrist not reconstructable- (KDAC):-TWF or TWA
Class “C” (adult and wrist involved)Lichtman IIIB-IV or Bain 2a, 3, 4
A. Children/ElderlyA1. Non operative
A2. Non-operative for 3-6 months; then minimally invasive (or Rx. as adult)
A3. Non operative; consider w/u for osteoporosis or inflammatory arthritis -(consider synovectomy)
B. Adult-Limited to LunateB1. Salvageable:
Schmitt a/b-Radius shortening (+) or capitate shortening (-) Schmitt c-Add vascularized bone graft
B2. Compromised:Bain1--Osteochondral vascularized graft (MFT) Bain 2b– Compression Screw
B3. Non-salvageable: PRC -Scaphocapitate /STT fusion) (Graner/Capitate length)
C. Adult-Wrist AffectedC1. Scaphocapitate/STT fusion. (PRC)
C2. PRC
C3. Radiocarpal fusion (TWA)
Precision Treatment Algorithm for Kienböck’s

SUMMARY
Advances in KD make a patient specific algorithm possible…
§ Consolidate osseous (Lichtman), cartilage (Bain) and vascular (Schmitt) staging systems
§ Add in new knowledge of natural history and up-to-date treatment options
§ Result: “A Precision Algorithm for the 21st Century”

I IIIA IVII

2021/9/24
1
AVN of the hand and wrist bones: Treatment with
autologous stem cell grafts
Ryosuke Kakinoki, MD, Ph.D.Professor of Hand Surgery and Microsurgery
Kindai UniversityOsaka Japan
1
I have no financial support nor have I any other conflict of interests regarding this presentation.
Ryosuke Kakinoki, MD, Ph.D.Department of Orthopedic Surgery,Kindai University
2
Number of articles reporting carpal AVN except the lunate and scaphoid
Carpal bones Number of cases reported
capitate 48
hamate 13
trapezium 3
trapezoid 2
triquetrum 3
pisiforms 3
Afshar A et al. JHS(Am) 20203
1
2
3

2021/9/24
2
Causes of carpal AVN
• Trauma• Repetitive forceful sport activities• Corticosteroid use• Goat• Alcoholic consumption• Chemotherapy• Gausher’s disease• Mucolipidosis Ⅲ• Collagen disease
SclerodermaSystemic loops erythematosus
4
Symptoms of carpal AVN
• Wrist pain• Tenderness• Swelling • Restricted ROM• Deformity• Tendon raptures
5
Hamate AVN
Afshar A et al. JHS(Am) 20206
4
5
6

2021/9/24
3
Capitate AVN
Hattori Y et al. 2009 JHS (Am)7
Pisiformis AVN
Match R & Cove G1974 JHS (Am)8
Trapezium AVN
G-Lopetz et al. 2002 JHS (Am)9
7
8
9

2021/9/24
4
Bilateral Trapezoid AVN
D’Agostino et al. 1983 JHS (Am)10
Triquetral and lunate AVN
Amsallem et al. hand Surg Rehabil 201611
Intraosseous vascularity of carpal bones
Type 1• Insufficient intraosseous anastomoses• A single vessel nourishes a great area of a
bone• Greater risk to develop AVNType 2• Having 2 vessel entry area with lack of
interosseous anastomosesType 3• Having 2 nutrient vessel entry zones (non-
articular areas) with consistent interosseous anastomoses
Panagis et al. 1983 JHS (Am)
• scaphoid, • capitate, • lunate (a small population)
• trapezoid, • hamate
• trapezium, • triquetrum, • pisiformis, • lunate (a large population)
12
10
11
12

2021/9/24
5
Scaphoid vascularity 1• Proximal 70-80%; nourished by proximal vessels entering the dorsal
ridge.
• Distal 20-30%; nourished by distal vessels entering the tubercle.
tubercle
dorsal ridge
Morsy M et al. JHS(Am) 2019
A-P view Lateral view
Gelberman RH et al. JHS(Am) 1980
13
Preiser’s disease
MRI Whole scaphoid AVN• Partial scaphoid AVN (proximal part)
1 of 13 specimens had a single vascular system extending from the proximal dorsal ridge without receiving any vascularity at the tubercle.
Kalainov et al. JHS(Am) 2003
14
Morsy M et al. JHS(Am) 2019
Do scaphoid bones having a single vascular network easily develop into the whole scaphoid AVN??
Scaphoid vascularity 2
# nutrient vessels from the dorsal ridge: 3.18 # nutrient vessels from the dorsal ridge: 1.5
Type 1 scaphoid(short capitate fossa with wide waist thickness)
Type 2 scaphoid(long capitate fossa with narrow waist thickness)
Morsy M et al. JHS 2019
May the scaphoid having the long capitate fossa and narrow waist be vulnerable to AVN??
A-P view
Lateral view
15
13
14
15
2021/9/24
6
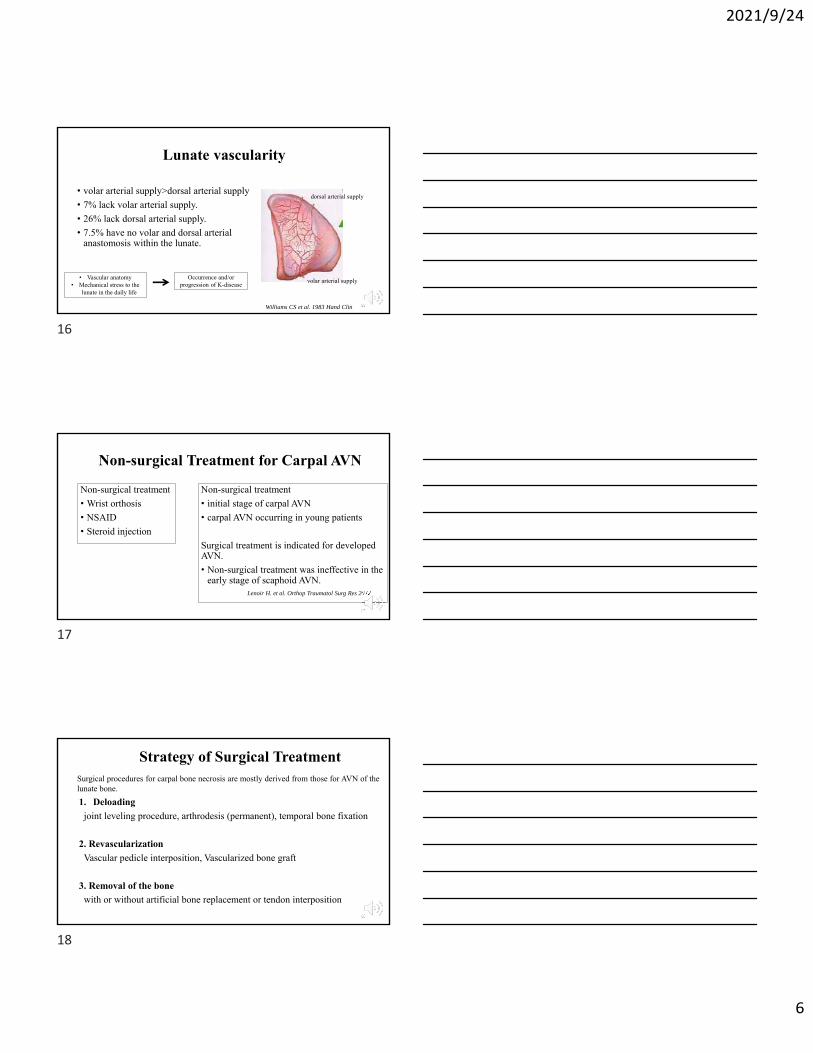
Lunate vascularity
• volar arterial supply>dorsal arterial supply
• 7% lack volar arterial supply.
• 26% lack dorsal arterial supply.
• 7.5% have no volar and dorsal arterial anastomosis within the lunate.
Williams CS et al. 1983 Hand Clin
dorsal arterial supply
volar arterial supply• Vascular anatomy• Mechanical stress to the
lunate in the daily life
Occurrence and/or progression of K-disease
16
Non-surgical Treatment for Carpal AVN
Non-surgical treatment
• initial stage of carpal AVN
• carpal AVN occurring in young patients
Surgical treatment is indicated for developed AVN.
• Non-surgical treatment was ineffective in the early stage of scaphoid AVN.
Non-surgical treatment
• Wrist orthosis
• NSAID
• Steroid injection
Lenoir H. et al. Orthop Traumatol Surg Res 2012
17
Strategy of Surgical Treatment
1. Deloading
joint leveling procedure, arthrodesis (permanent), temporal bone fixation
2. Revascularization
Vascular pedicle interposition, Vascularized bone graft
3. Removal of the bone
with or without artificial bone replacement or tendon interposition
Surgical procedures for carpal bone necrosis are mostly derived from those for AVN of the lunate bone.
18
16
17
18

2021/9/24
7
Surgical Treatment of Carpal Necrosis 11. Deloading (joint leveling procedure, arthrodesis)
• radial shortening, lunate lengthening, capitate shortening; lunate
• Radial wedge osteotomy (closing, open); lunate, scaphoid
• Temporal STT fusion, SC; lunate
• Arthrodesis of STT or SL; lunate
2. Vascularization
• Vascular pedicle interposition; lunate, trapezium
• Vascularized bone graft; lunate, capitate, scaphoid, hamate
• Core depression of metaphysial bones; lunate, hamate (Irraramendi AA et al. 2001, JHS-A)
19
Surgical Treatment of Carpal Necrosis 2
3. Removal of the bones
• Interposition of tendon; lunate
• Artificial bone replacement; lunate
• Ligament reconstruction; trapezium
• Arthrodesis; lunate (STT fusion), scaphoid (four corner fusion)
• Only removal of bone; pisiformis, hamate hook, scaphoid, lunate(proximal raw carpectomy)
20
Bone Marrow-Derived Mesenchymal Stem Cells (BMSCs)
Bone Marrow-Derived Mesenchymal Stem Cells
(BMSCs)
Osteogenic cells
Adipogenic cells
Cartilagenous cells
Glia cells
Bone
Fat
Cartilag
Nerve21
19
20
21

2021/9/24
8
Treatment of Kienböck’s disease model using vascularized bone graft & bone marrow stem cells in canine.
• Removal of as much cancellous bone as possible from the cortical window (5X10mm) created in the scapholuate bone.
• Freezing the cavity with liquid nitrogen treatment for 10min.
• The cavity was thawed in room temperature for 10min.
• Repeat 3 times these freeze and thaw procedure.
• The cavity was filled with β-TCP + 1X107 BMSCs.
• The cortical window was plugged with a pedicled VBG.
• As a control, the cavity filled with β-TCP + 1X107 fibroblasts in the opposite scapholunate bone.
VBG
β-TCP
BMSCs or Fibroblasts
Ikeguchi R, Kakinoki R, Aoyama T, Toguchida J et al. Cell transplant 2006
Scapholunate bone
22
Liquid –Nitrogen treatmentPre-treatment
Just after treatment
24 W
No treatment24W after L-N
treatment
The scapholunate bone became collapsed.23
BMSC vs fibroblast (4W)
CT
Plain X-P
MRI Collapse of the scapholunate bone can be seen in the fibroblast transplantation
group.
24
22
23
24

2021/9/24
9
Histological Study (4W)
The bone cavity was filled with bone tissue in the BMSC
transplantation group, while with soft tissue in the fibroblast
transplantation group.
BMSC Fibroblast
25
Treatment of Kienböck’s disease using vascularized bone graft & bone marrow stem cells.
• 5 pts with stage 3A or B• Removal of as much cancellous bone as possible from
the dorsal window.• The cavity was filled with β-TCP + 1X107 BMSCs.• The cortical window was plugged with a VBG based
on the 4th and 5th ICAs.• Temporal S-C fixation for 16 weeks.
VBG BMSCs β-TCP
Ikeguchi R, Kakinoki R, Aoyama T, Toguchida J et al. J. Orthop Sci 201926
Surgery
Elevation of a VBG Creating a bone cavity in the lunate β-TCP blended with
1X107 BMSCs27
25
26
27

2021/9/24
10
VBG + temporal S-C fixation
Kienböck’s disease with Stage 3 or Stage early 4
VBG combined with some deloading procedure
Matsumoto T, Kakinoki R et al. JHS(Am) 201728
Case 1; 24 y.o. man with stage 3B
Pre-op Post-op
Post-op 1Y Post-op 2YStage 3B, RS-angle 60°, MWS fair
Stage 3B, RS-angle 60°, MWS poor
29
Case 5; 27 y.o. man with stage 3A
Stage 3A, RS-angle 55°, MWS poor
Stage 3A, RS-angle 52°, MWS fair
Pre-op Post-op 1Y
Pre-op 2Y
30
28
29
30

2021/9/24
11
Results of VBG + BMSCs
• Bone can be formed by BMSC transplantation with VBG in Kienböck’s disease.
• Effective to prevent the progression of the collapse.31
Take Home Messages
• AVN happens in all carpal bones.
• Spontaneous recovery from AVN can be seen in trapezoid, triquetrum and young patients’ lunate necrosis.
• The main vascular vessels enter the scaphoid from the dorsal ridge.
• The main nutrient vessels enter the volar portion of the lunate.
• Occurrence of carpal AVN is related to the bone morphology, intraosseous vascularity, geographic variation of the ligament attachment, and mechanical stress on the wrist.
• The surgical treatment of carpal necrosis is categorized into deloading, vascularization or removal of the bones. To treat advanced carpal AVN, several procedures with different categories should be combined.
32
31
32