hyponatremia in the icu: morbidity, mortality and...
TRANSCRIPT

Hyponatremia in the ICU: Morbidity,Mortality and Therapy
Mitchell H. Rosner, MD
Division of Nephrology
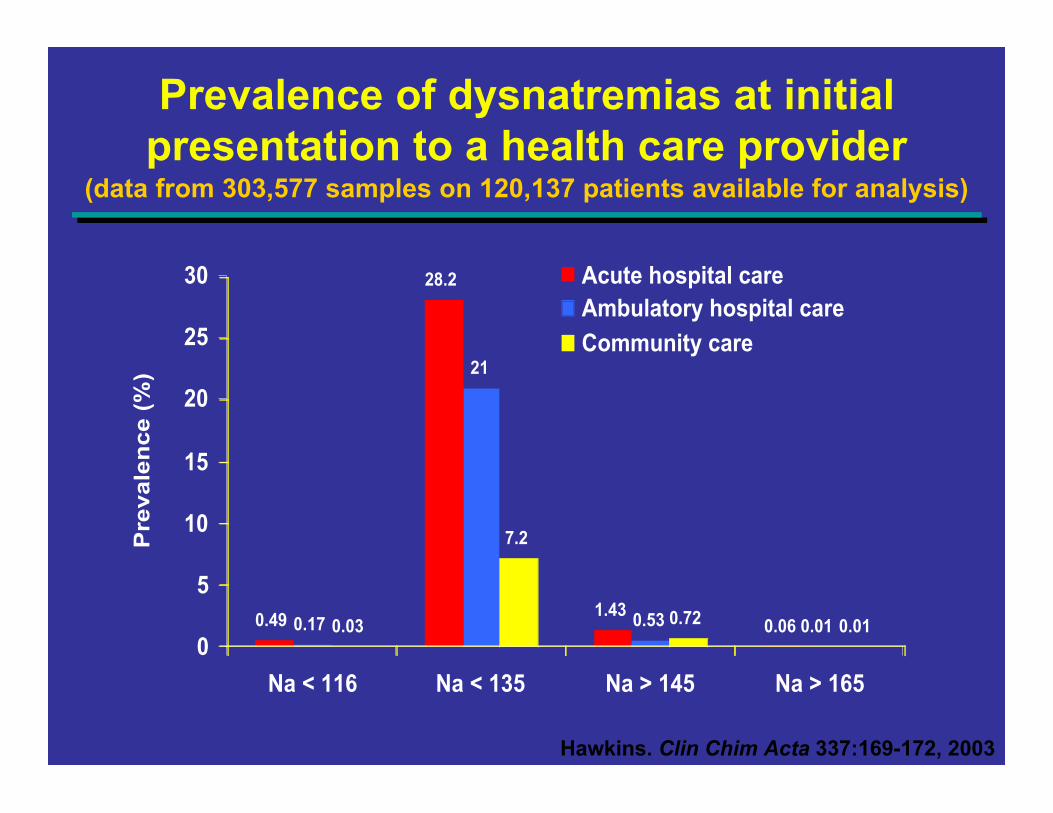
Prevalence of dysnatremias at initialpresentation to a health care provider
0.49
28.2
1.430.060.17
21
0.53 0.010.03
7.2
0.72 0.010
5
10
15
20
25
30
Na < 116 Na < 135 Na > 145 Na > 165
Pre
va
len
ce
(%
)
Acute hospital careAmbulatory hospital care
Community care
Hawkins. Clin Chim Acta 337:169-172, 2003
(data from 303,577 samples on 120,137 patients available for analysis)

Hyponatremia is an independent risk factorfor in-hospital mortality
Serum [Na +] >130 mEq/L
Serum [Na +] <130 mEq/L Serum [Na +]
120-129 mEq/L
Serum [Na +] <120 mEq/L
0
5
10
15
20
25
Mo
rta
lity
(%
)
Study of 4,123 patients ≥65 years old admitted to a community hospital3.5% had a serum [Na+] <130 mEq/L at admissionIn this study, hyponatremia was found to be a predictor of in-hospital
mortality (RR=2.0)
RR=relative risk.
Terzian C et al. J Gen Intern Med.9:89-91, 1994
Most recently…
Prospective cohort study of 98,411 adultshospitalized between 2000-2003
Assessed mortality in-hospital and at 1 and 5 years
Prevalence of serum Na+ < 135 meq/L was 14.5%
Those with hyponatremia: older (67 v. 63.1 yrs) andmore comorbid conditions
Waikar et al. Am J Med 2009; 122: 857
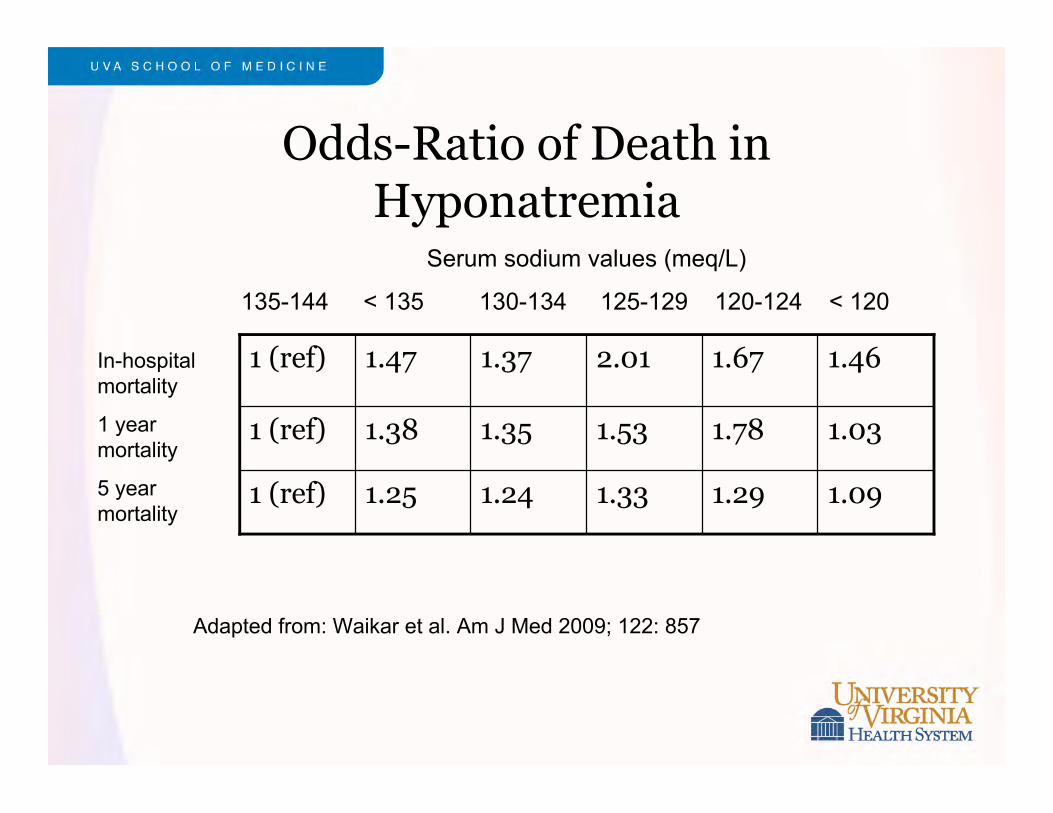
Odds-Ratio of Death inHyponatremia
1.091.291.331.241.251 (ref)
1.031.781.531.351.381 (ref)
1.461.672.011.371.471 (ref)
Serum sodium values (meq/L)
135-144 < 135 130-134 125-129 120-124 < 120
In-hospitalmortality
1 yearmortality
5 yearmortality
Adapted from: Waikar et al. Am J Med 2009; 122: 857

Resolution of hyponatremia
In this study, more than one serum sodium level was available on52,468 patients.
Allowed investigators to look into the effects of resolution v. non-resolution of hyponatremia on mortality:
38.5%40.8%
18.5%23.5%
3.9%6.2%
Persistent (n = 4254) Resolved (n = 3794)
In-hospitalmortality
1 yearmortality
5 yearmortality
Impact on length of stay and otheroutcomes
2 recent studies:
LOS is increased from 1 to 2 days in patients withhyponatremia
Patients with hyponatremia had between 12-58%increased risk of requiring an ICU stay (higher riskassociated with lower initial sodium level)
Total cost per admission increased from $1300 to $3500(higher costs associated with lower sodium levels)
Callahan et al. Hosp Pract 2009; 121
Zilberberg et al. BMC Pulm Med 2008; 8:16
Does treatment matter?Prospective review of lab and chart data over 6 months in a
large teaching hospital
104 patients with serum [Na+] <125 mEq/L identified
Only 28 (26%) had plasma osmolality measured, 29 (27%)urine osmolality, 11 (10%) urinary sodium, 8 (8%)
33% had “significant” management errors
-Fluid restriction and IV saline, fluid restriction inhypovolemia, hypotonic fluids in SIADH
27% mortality rate (28 of 104 patients)– 20% mortality in patients managed appropriately– 41% mortality in patients with management errors
Huda et al. Postgrad Med J. 82:216-219, 2006

Therapy of Hyponatremia
Two Key Questions
How much correction is enough to improveoutcomes?
How much correction is too much?

Clinical Hyponatremia– Acute (<48 hrs): Cerebral edema, seizures, death due to herniation especially in young
women and children
– Chronic (>48 hrs): Adaptations minimize brain cell swelling, but reversibly alterneurologic function:
• Nausea and vomiting
• Confusion & personality changes
• Gait disturbances
• Seizures with very low serum sodium values
Acute Hyponatremia:Water Intoxication
Clinical symptoms first described in 1920’s andreproduced in experimental animals
Rowntree LG. Pharmacol Exp Ther 1926:29:135
First case of fatal cerebral edema from tap water byproctoclysis reported in 1935
Helwig FC. JAMA 1935:104:1569

Normal study Fatal hyponatremia
Acute Hyponatremia
Clinical Hyponatremia:Rapid Correction
Rapid Correction
Acute hyponatremia: Generally well tolerated
Chronic hyponatremia (>48 hrs): Delayed onset ofneurological deterioration associated with pontine andextrapontine demyelination

Central Pontine Myelinolysis
New disease of unknownetiology was found in fourpatients in Boston CityHospital and first reportedin 1959. Dozens of casereports soon followedprompting a search for anetiology.Eventually an associationwith hyponatremia wasmade.
Laureno R, Karp BI. Ann Intern Med 1997; 126(1): 57-62
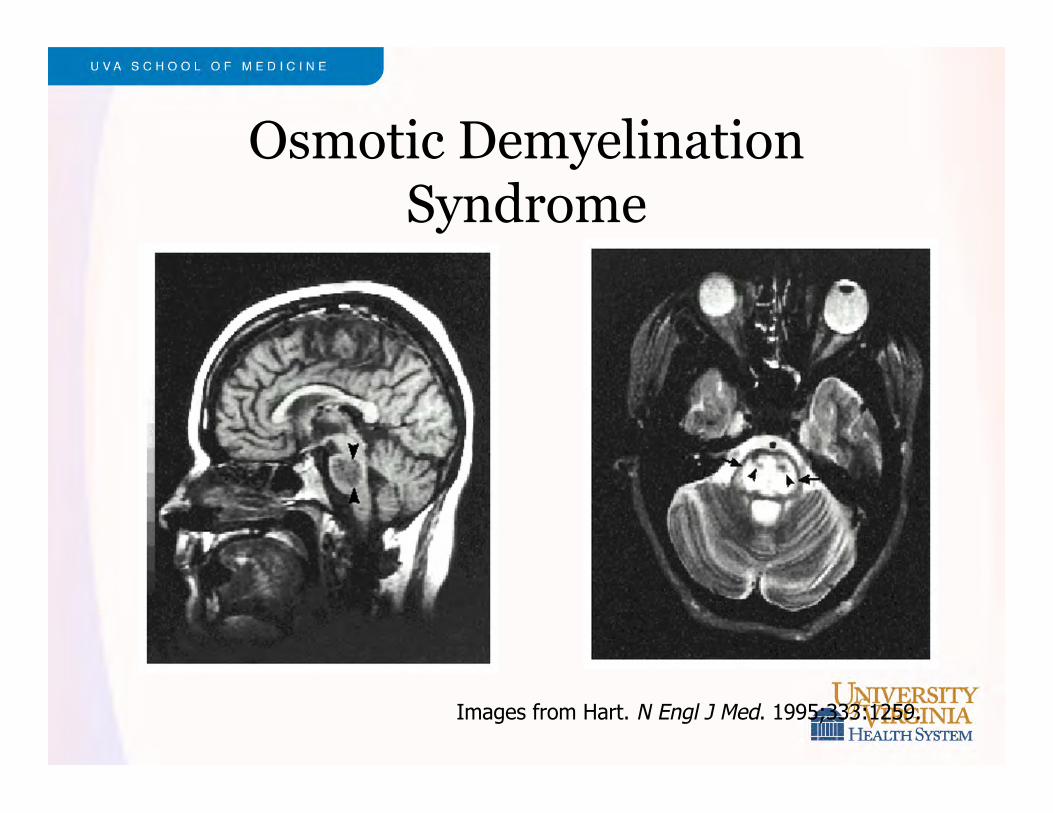
Osmotic DemyelinationSyndrome
Images from Hart. N Engl J Med. 1995;333:1259.
Question #1
How much correction of hyponatremia is “enough”to prevent complications in severe acutehyponatremia?
Consensus Conference on Treatment of AcuteHyponatremia in Marathon Runners
Recommended Therapy:
In the field: 3% saline 100 ml over 10 minutes,repeated x 2 if needed
In hospital: 3% saline 100 ml or 1 ml/kg bolusfollowed by 100 ml/hr or 1-2 ml/kg/hr
Hew-Butler, Clin J Sport Med 2008;18:111-121
Therapeutic hypernatremia forcerebral edema
30 ml bolus of 23.4% saline (equivalent to 238 ml3% saline)
Δ Serum Na = 5 mEq/L
Reversed clinical signs of brain herniation in mostcases
Decreased intracranial pressure by 40%
Koenig, MA. Neurology 70: 1023–1029, 2008

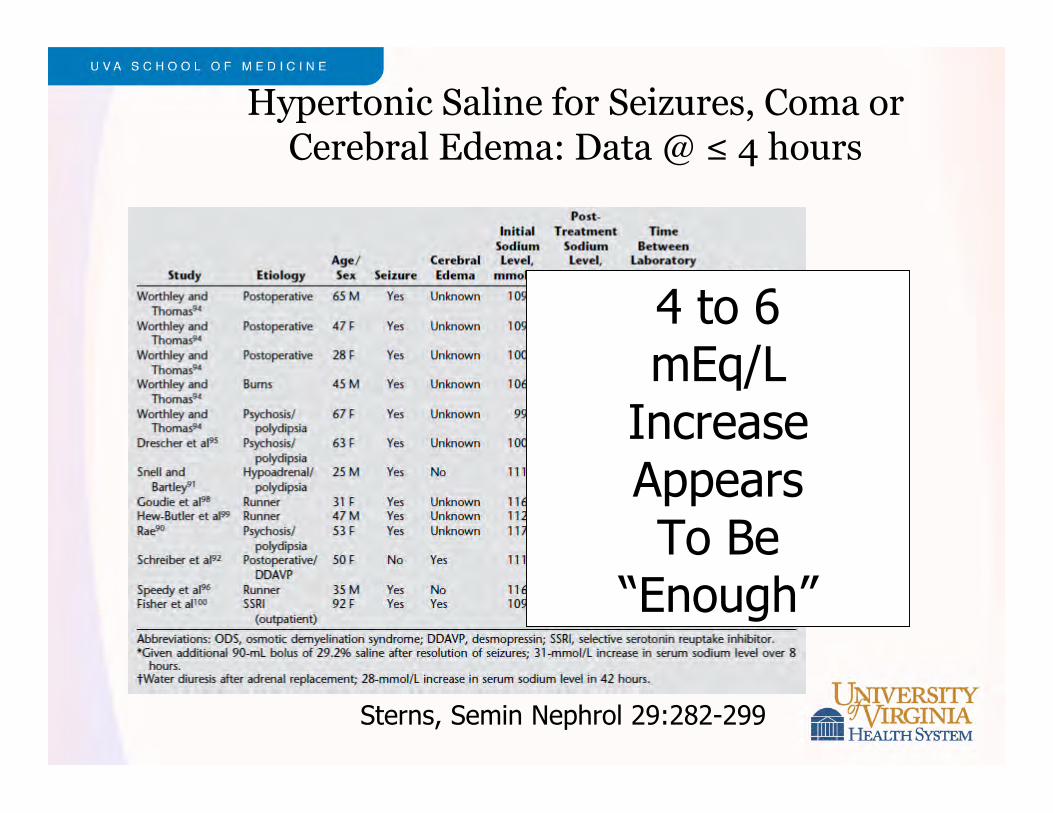
Hypertonic Saline for Seizures, Coma orCerebral Edema: Data @ ≤ 4 hours
Sterns, Semin Nephrol 29:282-299
Hypertonic Saline for Seizures, Coma orCerebral Edema: Data @ ≤ 4 hours
Sterns, Semin Nephrol 29:282-299
4 to 6mEq/L
IncreaseAppearsTo Be
“Enough”
Therapy of HyponatremicEmergencies- Summary
Goal: 4 to 6 mEq/L increase in serum sodiumconcentration
2 ml/kg bolus of 3% saline for severe symptoms(repeated if necessary) or
1 to 2 ml/kg infusion of 3% saline for 2 to 3 hours
Question #2
How much correction of hyponatremia is “enough”to cause complications in severe chronichyponatremia?
How much is too much?

How Much is Too Much?
CPM by Autopsy (Fatal cases)
Norenberg1 20 mEq/L in 3 daysAyus 2 25 mEq/L in 2 days
Non-fatal cases
Author Δ Na/day Δ Na/2 daysSterns1,2,3 12 mEq/L 18 mEq/LElllis4 10 mEq/L Karp5 10 mEq/L 21 mEq/L
1. N Engl J Med 1986; 314:15352. Ann Internal Med 1987; 107:6563. JASN 1994;4:15224. QJM 1995; 88:9055. Medicine 1993; 72:359

Serum Na ≤ 105 mEq/LRate of Correction and Outcome
0 10 20 30
Rapid
Slow
Rapid
Slow
Uncomplicated Transient SequelaePermanent Sequelae
{{
Chronic Cases
Acute Cases
Data from SternsJASN 1994;4:1522 Number of Patients

Serum Na ≤ 105 mEq/LRate of Correction and Outcome
0 10 20 30
Rapid
Slow
Rapid
Slow
Uncomplicated Transient SequelaePermanent Sequelae
{{
Chronic Cases
Acute Cases
Data from SternsJASN 1994;4:1522 Number of Patients
“Rapid”:>12/day>18/48h

Treatment of ChronicHyponatremia
• Limits are not goals
• Target therapy to stay well clear of limits– 6 to 8 mEq/L daily
• Use special care in patients at high risk for osmoticdemyelination:
– Chronic hyponatremia
– Alcoholism
– Malnutrition
– Liver disease
– Burns
– Hypokalemia– Serum Na ≤ 105 mEq/L
Avoiding Inadvertent RapidCorrection
Reversibly impaired water excretion– Volume depletion– DDAVP– Hypocortisolism– Thiazide diuretics– SSRI’s– Nausea & alcohol withdrawalIn these cases, the stimulus for impaired water excretion is
corrected quickly, and a rapid water diuresis then ensues.
Maximally dilute urine increases the serum sodium concentration by > 2mEq/L/hr
Continued vigilance with frequent measurements of the serum sodiumconcentration and attention to urine output is essential in all patientswith very low serum sodium concentrations
Equations- serious pitfalls
Δ SNa after 1 liter of infusate =
Infusate Na – Serum NaTotal Body Water + 1
Assumes all of the infusate is retained; does not consider urinelosses of electrolyte or water
Must be vigilant to watch for water diuresis which will lead to muchmore rapid correction than predicted
Adrogue. N Engl J Med 2000:342:1581-9
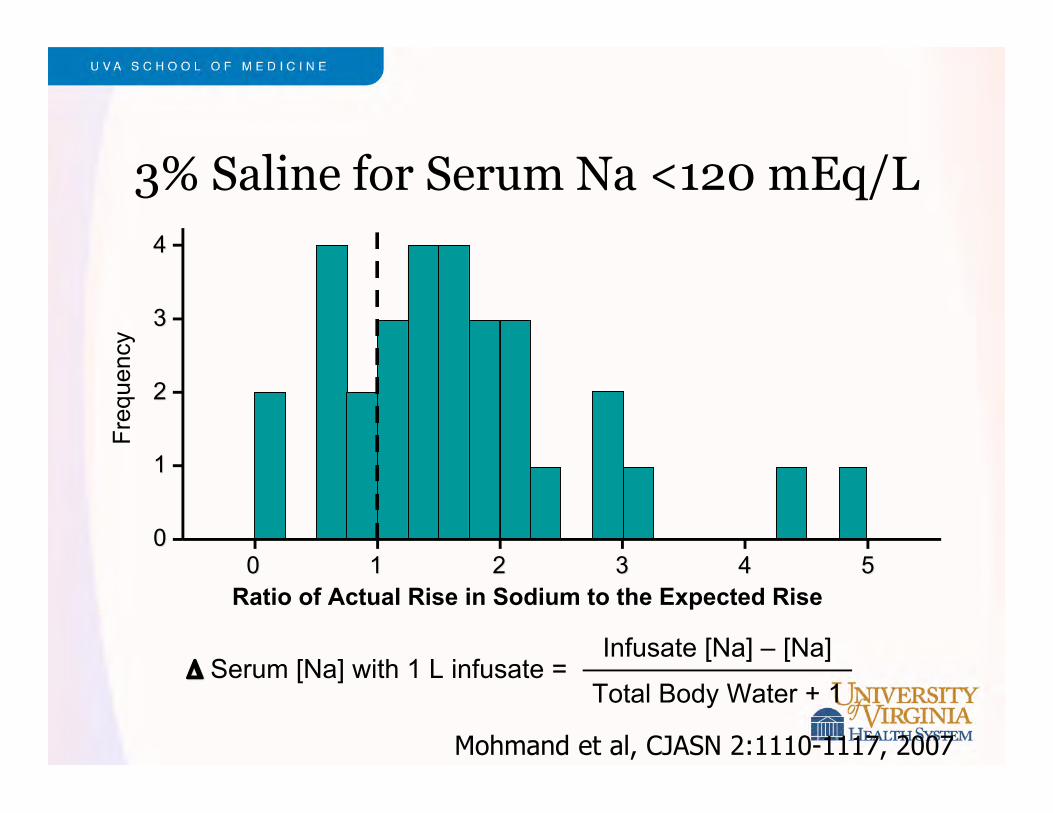
3% Saline for Serum Na <120 mEq/L
Total Body Water + 1 ΔΔ Serum [Na] with 1 L infusate =
Infusate [Na] – [Na]
00
11
22
33
44
00 11 22 33 44 55Ratio of Actual Rise in Sodium to the Expected Rise
Fre
quen
cy
Mohmand et al, CJASN 2:1110-1117, 2007

3% Saline for Serum Na <120 mEq/L
Total Body Water + 1 ΔΔ Serum [Na] with 1 L infusate =
Infusate [Na] – [Na]
00
11
22
33
44
00 11 22 33 44 55Ratio of Actual Rise in Sodium to the Expected Rise
Fre
quen
cy
Mohmand et al, CJASN 2:1110-1117, 2007
Less Than
Expected

3% Saline for Serum Na <120 mEq/L
Total Body Water + 1 ΔΔ Serum [Na] with 1 L infusate =
Infusate [Na] – [Na]
00
11
22
33
44
00 11 22 33 44 55Ratio of Actual Rise in Sodium to the Expected Rise
Fre
quen
cy
Mohmand et al, CJASN 2:1110-1117, 2007
More than expected

Lower Serum Na=Higher Riskof Overcorrection
––55
00
55
1010
1515
2020
105105 110110 115115 120120 125125 130130 135135
Serum Sodium Before Infusion (mEq/L)
Ris
e in
Ser
um
in
48 H
ou
rs (
mE
q/L
))
Mohmand et al, CJASN 2:1110-1117, 2007
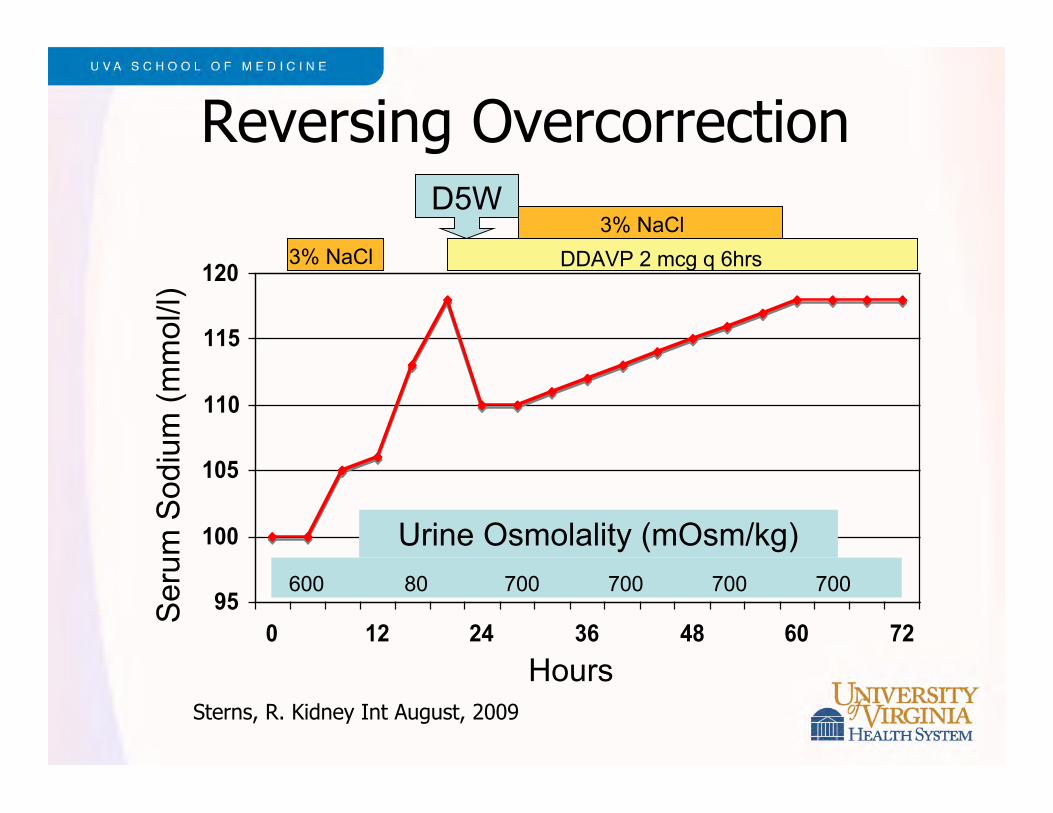
95
100
105
110
115
120
0 12 24 36 48 60 72
Ser
um S
odiu
m (
mm
ol/l )
Hours
DDAVP 2 mcg q 6hrs3% NaCl
3% NaClD5W
Urine Osmolality (mOsm/kg)
600 80 700 700 700 700
Reversing Overcorrection
Sterns, R. Kidney Int August, 2009

Re-Induction of HyponatremiaPrevents Myelinolysis
1/1612/12Deaths Day 10
1/1612/12Sx’s Day 5
14 ± 1 mmol/l29 ± mmol/lΔSNa at 24 hrs
29 ± 1 mmol/l--ΔSNa at 12 hrs
104 ± 2 mmol/l108 ± 2 mmol/lSNa Pre-Rx
Rapid CorrectionPlus Re-Lowering
Rapid Correction
Gankam Kengne, F. Kidney International 2009;76:614-621
Vasopressin ReceptorVasopressin ReceptorAntagonistsAntagonists
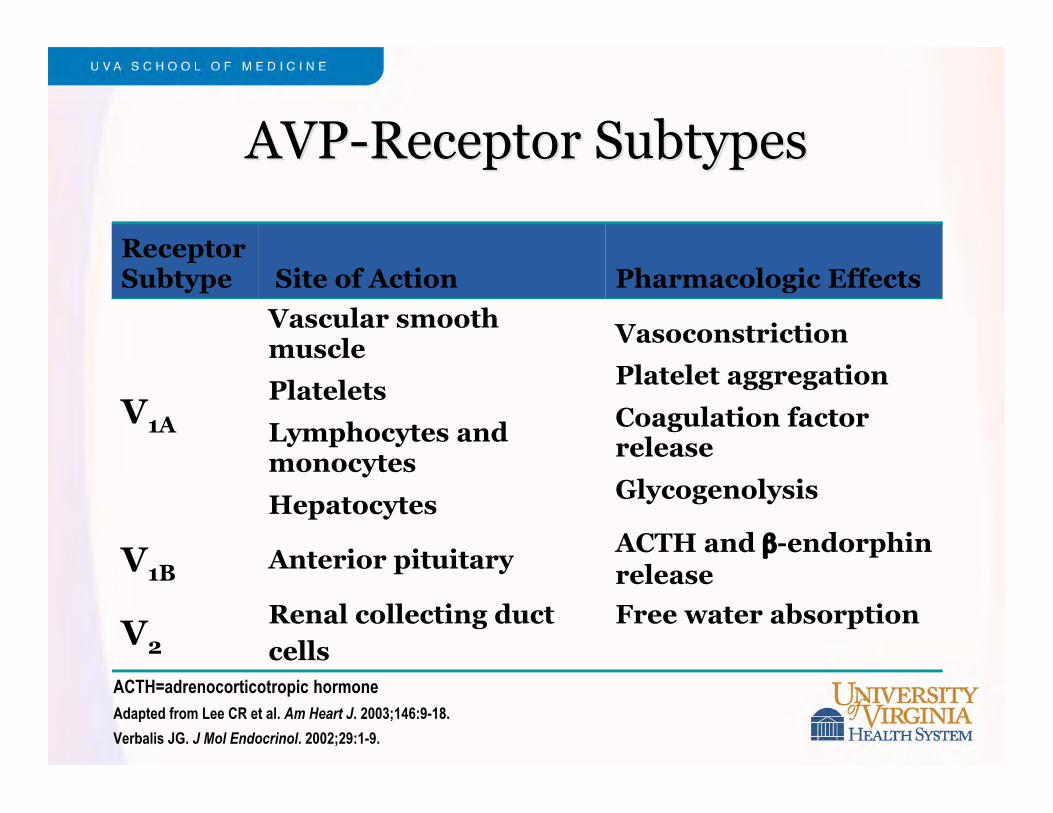
AVP-Receptor SubtypesAVP-Receptor Subtypes
ReceptorSubtype Site of Action Pharmacologic Effects
V1A
Vascular smoothmuscle
Platelets
Lymphocytes andmonocytes
Hepatocytes
Vasoconstriction
Platelet aggregation
Coagulation factorrelease
Glycogenolysis
V1B Anterior pituitaryACTH and β-endorphinrelease
V2Renal collecting ductcells
Free water absorption
ACTH=adrenocorticotropic hormoneAdapted from Lee CR et al. Am Heart J. 2003;146:9-18.
Verbalis JG. J Mol Endocrinol. 2002;29:1-9.
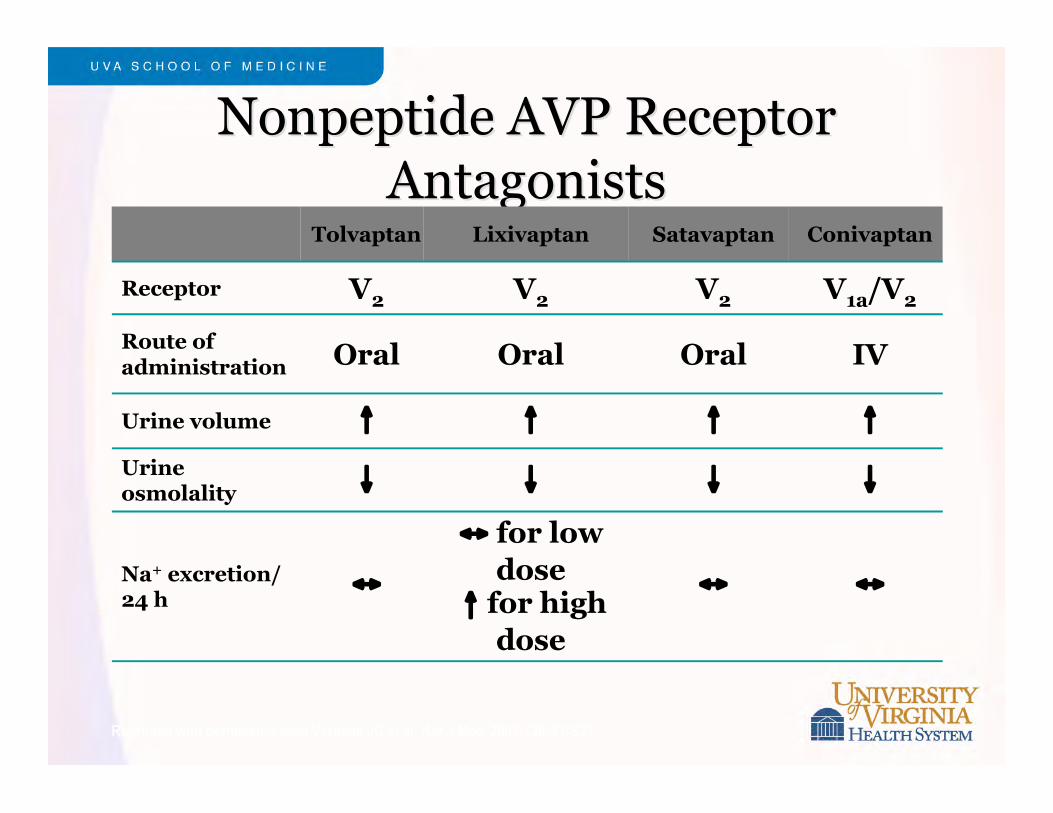
NonpeptideNonpeptide AVP Receptor AVP ReceptorAntagonistsAntagonists
Tolvaptan Lixivaptan Satavaptan Conivaptan
Receptor V2 V2 V2 V1a/V2
Route ofadministration Oral Oral Oral IV
Urine volume ↑ ↑ ↑ ↑
Urineosmolality
↓ ↓ ↓ ↓
Na+ excretion/24 h
↔
↔ for lowdose
↑ for highdose
↔ ↔
Reprinted with permission from Verbalis JG et al. Am J Med. 2007;120:S1-S21.

Serum Sodium by VisitSerum Sodium by VisitSevere Severe HyponatremiaHyponatremia Group Group
120
125
130
135
140
Seru
m N
a (m
Eq/L
)
120
125
130
135
140
Seru
m N
a (m
Eq/L
)
Baseli
neDay
1
8-hr Day
2Day
3Day
4
Week 1
Week 2
Week 3
Day 30
7 Day
Follow-U
p
p<0.0001
p<0.0001
PlaceboTolvaptan
SALT-1
SALT-2
Schrier RW et al. SALTInvestigators. N Eng J Med.2006;355:2099-2112.
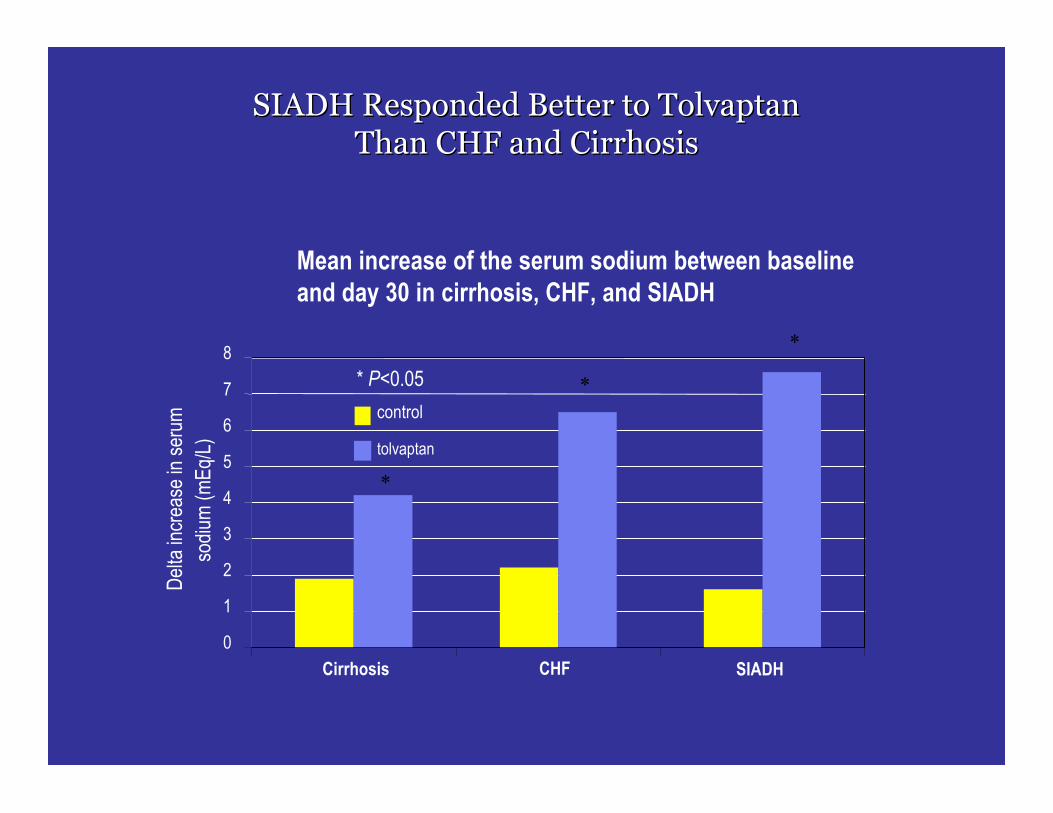
SIADH Responded Better to TolvaptanSIADH Responded Better to TolvaptanThan CHF and CirrhosisThan CHF and Cirrhosis
Mean increase of the serum sodium between baselineand day 30 in cirrhosis, CHF, and SIADH
0
1
2
3
4
5
6
7
8
Cirrhosis CHF SIADH
Del
ta in
crea
se in
ser
umso
dium
( mEq
/L)
control
tolvaptan
*
*
*
* P<0.05
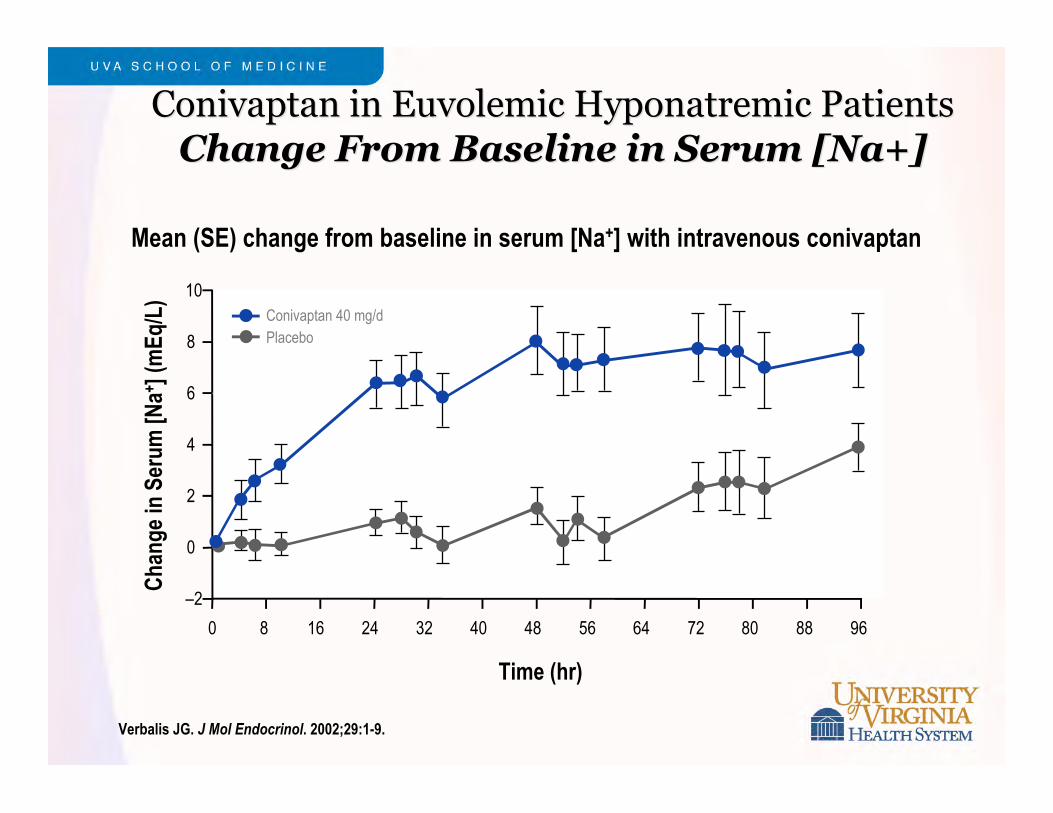
ConivaptanConivaptan in in EuvolemicEuvolemic HyponatremicHyponatremic Patients PatientsChange From Baseline in Serum [Na+]Change From Baseline in Serum [Na+]
Time (hr)
0 96
Cha
nge
in S
erum
[Na+ ]
(mEq
/L)
–2
4
6
8
10
2
0
8 16 24 32 40 48 56 64 72 80 88
Conivaptan 40 mg/dPlacebo
Mean (SE) change from baseline in serum [Na+] with intravenous conivaptan
Verbalis JG. J Mol Endocrinol. 2002;29:1-9.

Treatment of HyponatremiaSummary
Acute hyponatremia:– Prompt correction may avoid morbidity and mortality from
cerebral edema
– Adequate correction: 4 to 6 mmol/l
Chronic symptomatic hyponatremia:– Limited correction avoids iatrogenic neurologic injury: <10
mmol/l/24 hrs; <18 mmol/l/48 hr; <20 mmol/l/72 hrs