hypertensive emergencies amy staples, md, mph unm department of pediatrics
TRANSCRIPT

Hypertensive Emergencies
Amy Staples, MD, MPH
UNM Department of Pediatrics
Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat
Clinical Quiz
1. 11 yo girl with a sinusitis, HA and BP 124/83
2. 5 yo boy with rash, abd pain, joint pain, tea colored urine and BP 117/81
3. 16 yo athletic boy in clinic for sports PE BP 132/84
HTNTreat
___ ___
___ ___
___ ___

Clinical Quiz
4. 3 yo girl with NF, alert and playful; BP 125/77
5. 2 yo girl with nephrotic syndrome admitted for albumin/lasix due to anarsca, with severe HA and seizure, BP 119/76; on admit 93/52
HTN Treat
______
______

Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat

Measuring accurate BP’s
• Cuff too small → high reading
• Cuff too big → OK reading or no reading (usually not falsely low)
• Lower extremities - Normally, BP is 10 to 20 mmHg higher in the legs than the arms– Prefer arm if at all possible– Right arm for comparison with standards

Cuff Size
• Bladder width > 40% of mid-arm circumference.
• Bladder length 80-100% of arm circumference.
A. Ideal arm circumferenceB. Range of acceptable arm circumferencesC. Bladder lengthD. Midline of bladderE. Bladder widthF. Cuff width

Oscillometric Devices
Measure mean arterial pressure (MAP) and calculates SBP and DBP– The algorithms used are proprietary and
NOT standardized – Results can vary widely and they do not
always closely match BP values obtained by auscultation
– These machines must be calibrated regularly

Manual vs. Automatic
• Manual is the gold standard
• Oscillometric measurements preferred in infants and ICU settings ONLY
• All high readings should be confirmed with a manual

Confirming High BP’s
• Repeat BP in both arms and one leg (both not usually necessary)
• Repeat 3 times to assure accurate
• Dx of HTN requires elevated BP’s on 3 separate occasions

Disappearance of “HTN” with Repeated Measurement
83%
48%20%
17%
52%80%
0%
20%
40%
60%
80%
100%
1st Screen(N=2460)
2d Screen(N=323)
3d Screen(N=87)
HTN
Normal

Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat

New BP Normals
• 4th report on the diagnosis, evaluation and treatment of high blood pressure in children and adolescents– Correlates with the JNC 7– Uses new growth parameter data from
NHANES

Definitions
Normotensive • Average SBP and DBP <90th % for age, sex and
heightPre-hypertension • Average SBP or DBP >90th but <95th percentile
(OR >120/80)Hypertension • Average SBP and/or DBP >95th percentile for
age, sex and height on 3 separate occasions– Stage 1: 95th-99th percentile + 5 mmHg– Stage 2: >99th percentile + 5 mm Hg

How to use the tables
• Need:– Age, gender, height percentage– BP charts

7 yo boy
Ht 75%tile
http://www.cc.nih.gov/ccc/pedweb/pedsstaff/bptable1.PDF
50% 99/5890% 113/7395% 119/8099% 127/88

BP tables for Infants
*Task Force on Blood Pressure Control in Children. Report of the Second Task Force on Blood Pressure Control in Children—1987.Pediatrics.1987;79:1–25(PR)

Urgency vs. Emergency
• Urgency – severely elevated BP with no current evidence of secondary organ damage, although if left untreated, target organ injury may result imminently→ Decrease BP Soon
• Emergency – severely elevated BP with evidence of target organ injury→ Decrease BP Immediately
• Target organs – CNS, heart, kidney, eye
Constantine and Linakis, Pediatric Emergency Care, 2005

Severe Hypertension
“Hypertension that represents a threat to life or to the function of vital organs”
OR
Severe hypertension is when your blood pressure goes up too!
Adelman, et al. Pediatric Nephrology, 2000

Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat

Etiology of Hypertension
Newborn Early Childhood (Infant-6 yo)
School Age
(6-12 yo)
Adolescence
•Renal vein thrombosis
•Coarctation
•Renal artery stenosis
•Congenital renal anomalies
•Renal parenchymal disease
•Renovascular disease
•Coarctation
•Renal parenchymal disease
•Renovascular disease
•Essential hypertension
•Essential hypertension
•Renal parenchymal disease
•Renovascular disease
Constantine and Linakis, Pediatric Emergency Care, 2005

Miscellaneous Causes
• Endocrine– Hyperthyroid– Pheochromocytoma
• Elevated ICP/CNS disease• Drug use (cocaine, ecstasy)• Medication (abrupt withdrawal)• Exercise• Traction• Hypovolemia

Overall
• 15-20% Essential Hypertension
• 80-85% Secondary Hypertension– 60-80% Renal– 8-10% Renovascular– 2% Coarctation
Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat

Which hypertensive patients need immediate treatment?
1. Severe HTN • Malignant HTN - >30% above 95%• Moderate – Severe HTN - >99% with target
organ damage
2. Symptomatic HTN
3. Target Organ Damage

Complications of Severe HTN
Retinopathy 27%
Encephalopathy 25%
LVH 13%
Facial palsy 12%
Visual changes 9%
Hemiplegia 8%
Deal, et al. Arch Dis Child, 1992

Clinical Signs of Malignant HTN
• Eyes– Retinal hemorrhages, exudates and papilledema
• Malignant Nephrosclerosis– ARF, Hematuria, Proteinuria
• Hypertensive Encephalopathy– Headache, nausea, vomiting– Restlessness, confusion seizures, coma– MRI (T2-weighted images) ;
• Edema of the white matter of the parieto-occipital regions: posterior leukoencephalopathy

Eyes
Papilledema, blurred optic disk, hemorrhages
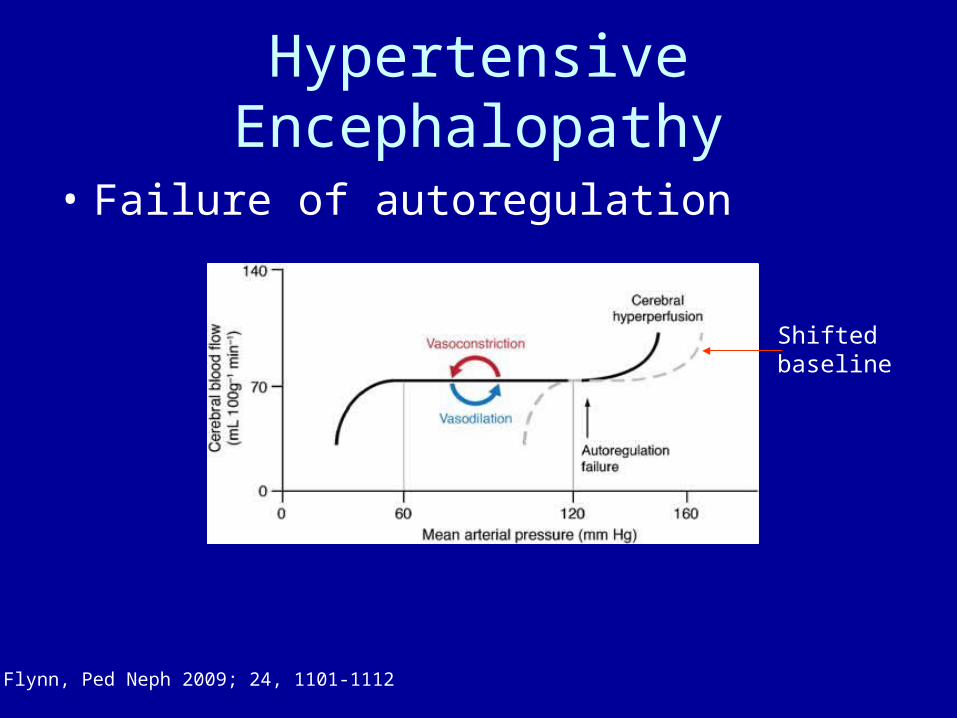
Hypertensive Encephalopathy
• Failure of autoregulation
Flynn, Ped Neph 2009; 24, 1101-1112
Shiftedbaseline

Hypertensive Encephalopathy
• Headache, nausea, vomiting
• Restlessness, confusion → seizures, coma
• Posterior Leukoencephalopathy
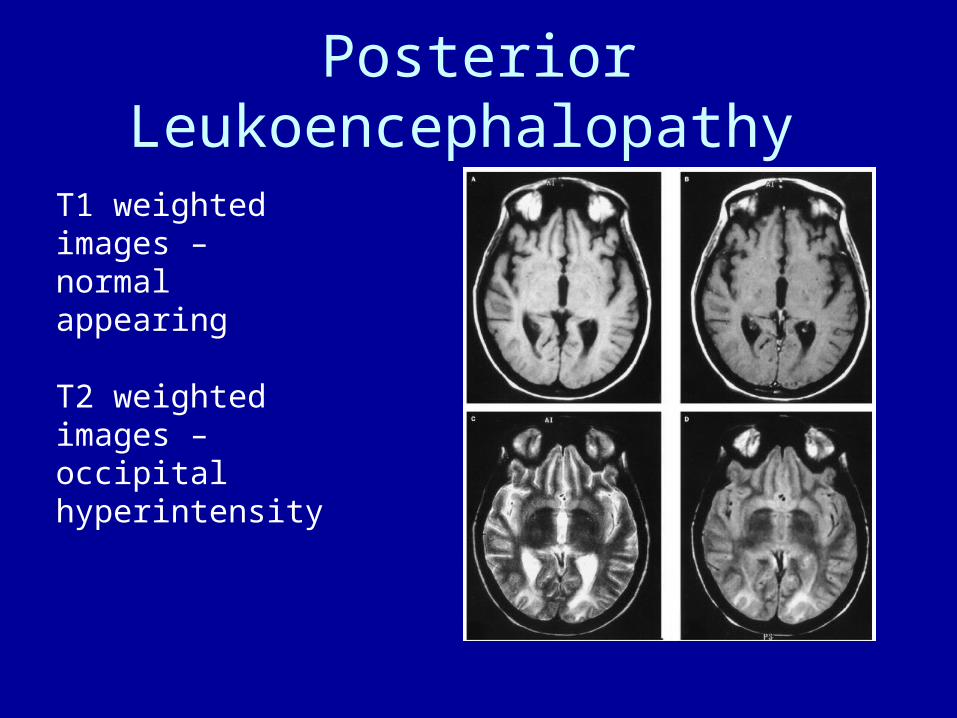
Posterior Leukoencephalopathy
T1 weighted images – normal appearing
T2 weighted images – occipital hyperintensity

Outline
• Measuring BP
• Definition of Hypertension
• Etiology of hypertension in kids
• When to treat
• How to treat

Severe Hypertension
• Treatment Goals– Prevent adverse events– Reduce BP in controlled manner– Preserve target organ function– Minimize complications of therapy

Severe Hypertension
• Treatment Risks– Rapid reduction of BP can lead to
complications• Risk of hypoperfusion (ischemia) secondary to
autoregulation• Medication side effects may have adverse effects
depending on cause of hypertension (e.g. ACEi)
How Much
Just Enough
Depends on Acute vs. Chronic
How Much
• Reduce by 25% of the planned reduction over 8-12 hrs
• Another 25% over the next 8-12 hrs • Final 50% over the next 24 hrs• Planned reduction – goal is to the 95-99%
for age and height
If Unsure, slower is safer

What to do 1st
• Monitor, Monitor, Monitor
• Need cardiopulmonary monitoring
• Need continual BP monitoring (frequently cycling cuff vs. arterial line)
• Decide oral vs. IV– Oral OK if asymptomatic– IV necessary if acute target organ damage is
present or imminent

Oral vs. IV
IV Medication• Rapid Action• Titratable• Easy to adjust the
dose• Requires IV access
PO Medication• Don’t need an IV• Harder to control
effects• Absorption variable• Slower kinetics can
make titrating more difficult


What to choose
First Line• PO
– Isradipine– Nifedipine
• IV– Nicardipine– Nitroprusside– Labetalol
Second Line• PO
– Clonidine
• IV– Hydralazine– Enalaprilat– Fenoldopam

Isradipine
• Ca channel blocker (Inhibit Ca++ entry into smooth muscle cells → vasodilitation)
• Onset of action 30-60 minutes• Side Effects: peripherial edema, flushing,
nausea, headache, tachycardia
• 0.05-0.1 mg/kg/dose q 4-6 hrs• 2.5 mg and 5 mg tab, 1mg/1ml suspension
Nifedipine – 0.1-0.25 mg/kg q 4-6 hours (10 mg tab available)Onset of action 15-30 min

A note on Short acting Ca Channel Blockers
• In adults with severe elevations in BP, Nifedipine has been associated with*:– Cerebral ischemia– Myocardial ischemia– Symptomatic hypotension Preexisting MI, CAD, and hypovolemia predispose to these
events.
• In children Nifedipine / Isradapine have not been associated with cerebral or myocardial events. †
*Grossman E, JAMA 1996;276:1328-31
†Sinaiko AR, NEJM 1997;336:1675

Nicardipine
• Ca channel blocker
• Onset of action within minutes
• Side Effects: same as isradipine
• 1-3 mcg/kg/min continuous infusion

Nitroprusside
• Direct arteriolar/venous dilator (via nitric oxide donation)
• Onset of action within seconds• Side Effects: cyanide/thiocyanate toxicity
• 0.5-1 mcg/kg/ min initially, titrate to max 10 mcg/kg/min
• Must monitor cyanide levels if used for >24 hrs

Labetalol
• Mixed alpha/beta blocker
• Onset of action 5-10 min
• Side Effects: bronchospasm, contraindicated in asthma, cardiogenic shock, pulmonary edema, or heart block
• 0.2-0.3 mg/kg/dose q 10-20 min (max dose 20mg) can be converted into a drip

Enalaprilat
• ACE inhibitor (prevents the vaso-constrictive and Na retaining effects of the RAS)
• Onset of action 15 min, long duration of action
• Side Effects: risk of decreased GFR
• 0.005-0.01 mg/kg/dose• Use in cases of severe renin mediated
HTN

Hydralazine
• Direct arteriolar vasodilator
• Side Effects: may cause Lupus-like syndrome
• Can be given PO, IV, IM
• 0.1 - 0.5 mg/kg q 4-6 hr (max 20 mg/dose)

Case # 1
11 yo girl with a sinusitis, HA and BP 124/83
Ht 75th%
Blood Pressures
50% -105/62 95% -122/80 99% -128/87
Diagnosis
Pain, repeat when well, no treatment
Case # 2
5 yo boy with rash, abd pain, joint pain, tea colored urine and BP 117/81
Ht 25th%
Blood Pressures
50% - 93/52 95% - 110/71 99% - 118/79
Diagnosis
GN, treat with medication, likely Ca channel blocker

Case # 3
16 yo athletic boy in clinic for sports PE
BP 132/84Ht 90th%
Blood Pressures
50% - 119/67 95% - 137/86 99% - 144/94
Diagnosis
Possibly Pre HTN, need repeat measurements and TLC

Case # 4
3 yo girl with NF, alert and playfulBP 125/77Ht 25%Blood Pressures50% - 88/48 95% - 105/66 99% - 113/74DiagnosisNF (possible associated renal artery stenosis),
Stage 2 HTN, treat with medication, renal vascular imaging

Case # 5
2 yo girl with nephrotic syndrome admitted for albumin/lasix due to anarsca, with severe HA and seizure BP 119/76; on admit 93/52
Ht – 75th%Blood Pressures50% - 89/46 95% - 107/64 99% - 114/71DiagnosisAcute HTN with end organ involvement, stop
albumin, give lasix, consider IV therapy if sz continues


Flynn, Ped Neph 2009; 24, 1101-1112