hypertensive disorders in pregnancy
DESCRIPTION
Hypertensive Disorders in Pregnancy. Professor Hassan Chairman Department of Obstetrics and Gynecology Faculty of Medicine King Abdulaziz University. Mrs F is a 30-year-old woman with a history of chronic hypertension and possible preeclampsia during her first pregnancy. - PowerPoint PPT PresentationTRANSCRIPT

Hypertensive Disorders in Pregnancy
Professor HassanChairman Department of Obstetrics and Gynecology
Faculty of Medicine King Abdulaziz University

Mrs F is a 30-year-old woman with a history of chronic hypertension and possible preeclampsia during her first pregnancy.
She is currently trying to conceive and wants to know how her hypertension will affect a future pregnancy and how it should best be managed, both now and during a pregnancy.

Hypertension Disorders in Pregnancy
Hypertension Disorders in Pregnancy
1. Preeclampsia- eclampsia:
2. Pre-existing hypertension:
3. Preeclampsia superimposed upon preexisting hypertension:
4. Gestational hypertension:

Preeclampsia :
• Systolic BP ≥ 140 Mm Hg Or Diastolic BP ≥ 90 Mm Hg Occurring ≥ 20 Weeks' Gestation• Proteinuria ≥ 300 Mg In A 24 Hour Urine Collection.
Eclampsia: The Development Of Grand Mal Seizures In A Woman With Preeclampsia.
Chronic Hypertension:Systolic Pressure > Or =140 mmHg, Diastolic Pressure > Or =90 mmHg, Or Both, That Is Present Before The 20th Week Of Pregnancy.
Gestational Hypertension (Transient Hypertension Of Pregnancy):
Systolic Pressure ≥ Or =140 mmHg, Diastolic Pressure ≥ Or =90 mmHg, Or Both, That Develop ≥ 20th Week Of Pregnancy In A Previously Normotensive Woman, But With Out Proteinuria.
Definitions

Preeclampsia superimposed upon chronic hypertension:
• New onset proteinuria or greatly increases proteinuria
after 20 weeks of gestation.
• Sudden exacerbation of BP to the severe range (systolic > or =160 mmHg or diastolic > or =110 mmHg) in the last half of pregnancy.
• or other signs of multisystem involvement such as thrombocytopenia or transaminitis in a woman with prior hypertension.
Report of the National High Blood pressor Education program Working group on high blood pressure in pregnancy. Am J Obs gyn 2000;183:S1-22

(Special conditions)

INCIDENCE:
• Hypertensive disorders complicate 12 to 22 percent of pregnancies
• Preeclampsia occurs in approximately 3 to 14 percent of all pregnancies worldwide
3 and 7 percent in nulliparas
0.8 and 5.0 percent in multiparas
Preeclampsia and other Hypertensive Disorders in Pregnancy

Diagnosis: Systolic Blood Pressure Of 140 MMHg Or Diastolic Blood Pressure 90 MMHg And Proteinuria Of 0.3 Grams Or Greater In A 24-hour Urine Specimen. On Two Occasions At Least 6 Hours Apart.
Pre-eclampsiaPre-eclampsia
Severe Mild
Eclampsia Refers To The Development Of Grand Mal Seizures In A Woman With Gestational Hypertension Or Preeclampsia.

Symptoms of Central Nervous System Dysfunction
Blurred vision, Scotoma, Altered Mental Status, Severe Headache
Symptoms of liver capsule distension
Right upper quadrant or epigastric painNausea and vomiting
HepatocellularInjurty:
Serum transminase concentration at least twice normal
Severe blood pressure elevation:
Systolic blood pressure 160 mm Hg or diastolic 110 mm Hg on two occasions six hours apart
Thrombocytopenia:
Less than 100,000 platelets per cubic millimeter
Protenuria:
5 or more grams in 24 hours
Oligouria:
Severe fetal growth restriction
Criteria for Severe Pre-eclampsiaCriteria for Severe Pre-eclampsia

Pathogenesis

The Pathophysiology of preeclampsia
First Phase: Incomplete invasion of the trophoblast into the endometrium.
Second Phase: placental under-perfusion, hypoxia, and ischemia, which then leads to release of stress factors
Third Phase: Maternal pre-eclamptic systemic syndrome and endothelial adverse response.
PET begins early in pregnancy. It develop over three distinct phases.


Thromboxane: has a vaso-occlusive effect and increases platelets aggregation .
Prostacylin: has a vaso-relaxing effect and diminishes platelets aggregation.In normal pregnancy there is a positive balance in favor of Prostacyclin.

IMPAIRED TROPHOBLAST INVASION
ABNORMAL TROPHOBLAST DIFFERENTIATION
PLACENTAL ISCHEMIA
IMMUNOLOGIC FACTORS
GENETIC FACTORS
SYSTEMIC ENDOTHELIAL DYSFUNCTION
Pathogenesis of Preeclampsia

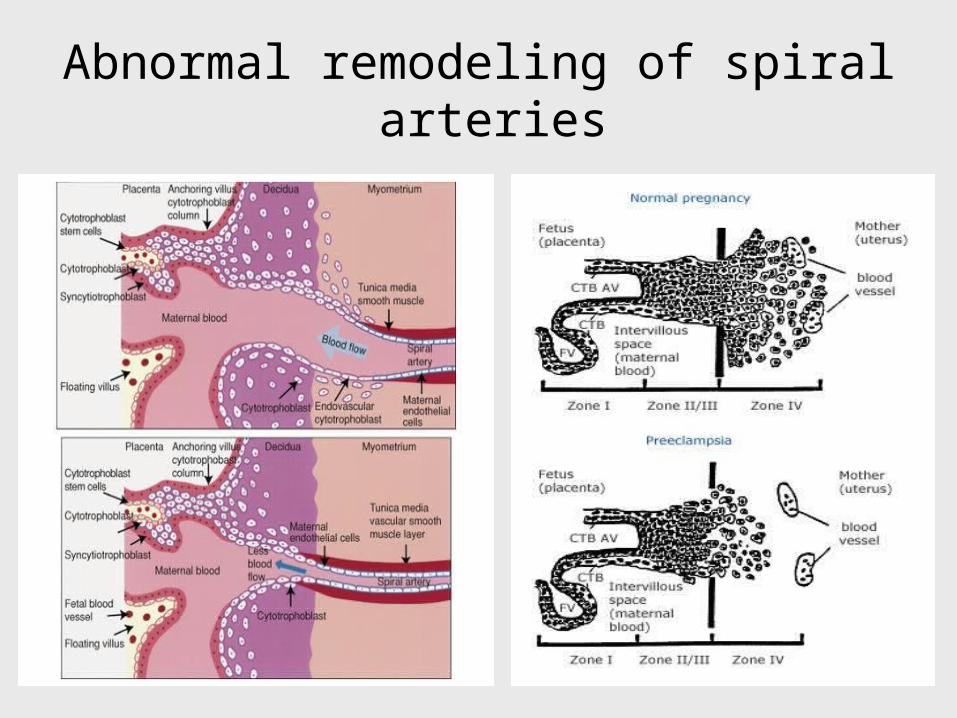
Abnormal remodeling of spiral arteries

Representation of Myometrial arteries and endometrial arteries

In normal pregnancyInvasive CTB invade maternal decidua and vasculature (zone v).



Clinical Manifestation of Preeclampsia
Preeclampsia is a systemic disease
characterized by generalized endothelial
dysfunction, vasospasm and and abnormal
endothelial expression of procoagulants
leads to coagulopathy.


Impaired Trophoblast invasionMedical conditions that predispose to vascular
insufficiencyObstetrical conditions that increase placental mass with a
relative decrease in placental blood flow
Placental hyperfusion/ischemia
Fetal Growth retardation Oligohydramnios
Imbalance of prostacyclin/ThromboxaneSystemic endothelial damage
Systemic Clinical Manifestations
CNS Renal Hematological Hepatic

Prevention of PET

High-protein and low-salt diet
Nutritional supplementation
Calcium
Magnesium
Zinc
Fish and evening primrose oil
Antihypertensive drugs including diuretics
Antithrombotic agents
Low-dose aspirin
Dipyridamole
Heparin
Vitamins E and C
Preventive Strategies
None of these interventions have proven to be effective.

19% decrease in the risk of preeclampsia (RR, 0.81; 95% CI, 0.75-0.88; number needed to treat [NNT], 69; 95% CI, 51-109),
7% decrease in the risk of preterm delivery (RR, 0.93; 95% CI, 0.89-0.98; NNT,83; 95% CI, 50-238),
16% decrease in the risk of fetal and neonatal death (RR, 0.84; 95% CI, 0.74-0.96; NNT, 227; 95%CI, 128-909 8% reduction in small for gestation age infants (RR 0.92; 95% CI 0.85-1.00)
No significant effects on the need for CS delivery or induction of labor
In more than 36 500 women aspirin use was associated with
Cochrane database meta-analysis of 41randomized controlled trials

Previous history of PET (RR 7.19, 95% CI 5.85 to 8.83) Antiphospholipids antibodies (9.72, 4.34 to 21.75), Pre-existing diabetes (3.56, 2.54 to 4.99), Multiple (twin) pregnancy (2.93, 2.04 to 4.21), Nulliparity (2.91, 1.28 to 6.61), family history (2.90, 1.70 to 4.93), Raised BP (diastolic > or = 80 mm Hg) at booking (1.38, 1.01 to 1.87), Raised BMI before pregnancy (2.47, 1.66 to 3.67) or at booking (1.55, 1.28 to 1.88), or Maternal age > or = 40 (1.96, 1.34 to 2.87, for multiparous women). Interval of >10 years since a previous pregnancy,
Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. Duckitt K; Harrington D BMJ 2005 12;330 .
Risk Factors of PE

Clinical Manifestations and Complications

Clinical Manifestation of Preeclampsia
Maternal:Hypertension:
Renal: Hepatic: Hematologic: Neurologic:
Fetal/Neonatal: IUGR:

Hypertension:Systolic BP ≥ 40 mmHg or Diastolic ≥ BP 90 mmHg in a woman who was normotensive prior to 20 weeks of gestation.
Renal:
• Proteinuria: ≥ 0.3 g protein in a 24-hour urine specimen (or 2+ on dipstick).
Proteinuria is due, in part, to impaired integrity of the glomerular barrier and altered tubular handling of filtered proteins (hypo filtration) leading to increased protein excretion.
• Creatinine clearance: Decline
• Uric acid: Reduced urinary excretion of uric acid (increase serum level of uric acid)
Clinical Manifestation of Preeclampsia

Edema and Intravascular volume: edema is no longer part of the diagnostic criteria. However, sudden and rapid weight gain and facial edema often occur in women who develop preeclampsia.
Hematologic changes:
Thrombocytopenia: Is the most common coagulation abnormality is due to formation of microthrombi.
The prothrombin time, partial thromboplastin time, and fibrinogen concentration:are affected with complications such as abruptio placentae or with severe liver involvement.
Microangiopathic hemolysis:Is detected by examination of a blood smear or elevation in the lactic dehydrogenase concentration.

Liver:Affected due to periportal hemorrhage, ischemic lesions, and microvesicular fat deposition.
Clinically: right upper quadrant or epigastric pain, elevated liver enzymes and, in severe cases, subcapsular hemorrhage or hepatic rupture.
Neurologic:
Eclampsia is the most severe complications.
Early signs may include headache, blurred vision, photophobia or mental state.Note: Only 50% of eclampsia cases have severe hypertension (> 160/110 mmHg)
No Reliable prediction for development of eclampsia in women with preeclampsia.

Pulmonary edema:
The etiology is multifactorial. Excessive elevations in pulmonary vascular hydrostatic pressure (PCWP).Capillary leak, left heart failure, and iatrogenic volume overload

Fetus and placenta:
IUGR:
The fetal consequences of chronic placental hypoperfusion are fetal growth restriction and oligohydramnios.
Severe or early onset preeclampsia results in the greatest decrements in birth weight compared to normotensive pregnancies.
Abruptio placenta:
Is infrequent (< 1 percent) in women with mild preeclampsia, but occurs in 3 percent of those with severe disease.

The HELLP Syndrome

HELLP syndrome is a group of symptoms that occur in pregnant women who have:
•H – Hemolytic anemia H•EL -- elevated liver enzymes •LP -- low Platelet count
The HELLP Syndrome

The HELLP Syndrome Incidence: ranged from 2 to 12 percent.
Classification: Class I: platelet nadir below 50,000/mmClass 2: platelet nadirs between 50,000 and 100,000/mm
Class 3: a platelet nadir between 100,000 and 150,000/mm
Severe hypertension is not a constant or even a frequent finding in HELLP syndrome.
Of 112 patients 66 percent had a diastolic BP of at least 110 mm Hg, 14.5 percent had a diastolic BP of less than 90 mm Hg.
The reported PNM has ranged from 7.7 to 60 percent. Maternal mortality from 0 to 24 percent. Maternal morbidity is
common.

Peripheral blood smear of normal case (Left) and patient with microangiopathic hemolytic anemia (right) note marked red cell fragmentation. The smear shows multiple helmet cells (small black arrows), other fragmented red cells (large black arrow); microspherocytes are also seen (blue arrows). The platelet number is reduced; the large platelet in the center (red arrow) suggests that the thrombocytopenia is due to enhanced destruction. In the normal (left) smear note the red cells are of relatively uniform size and shape, several platelets (black arrows) and a normal lymphocyte (blue arrow) can also be seen .

Criteria to Establish the Diagnosis of HELLP Syndrome
Hemolysis
Abnormal peripheral blood smear
Increased bilirubin <1.2 mg/dl
Increased lactic dehydrogenase >600 IU/L
Elevated liver enzymes
Increased SGOT ≥72 IU/L
Increased lactic dehydrogenase >600 IU/L
Thrombocytopenia
Platelet count <100,000/mm

It is important to emphasize that these patients may have a variety of unusual signs and symptoms, none of which are diagnostic of severe preeclampsia.
Pregnant women with probable preeclampsia presenting with atypical symptoms should have a complete blood count, a platelet count, and liver enzyme determinations irrespective of maternal blood pressure.
Clinical Manifestation and DiagnosisThe condition usually develops in the third trimester. It is more common if there are symptoms and sings of severe PET. However the final diagnosis is based on the result of the investigations. Symptoms and signs:. The most common clinical presentation is abdominal pain and tenderness in the midepigastrium, right upper quadrant, or below the sternum.Investigation :
Microangiopathic hemolytic anemia: with characteristic schistocytes (also called helmet cells) on blood smear .Other signs suggestive of hemolysis include:Elevated LDH (≥600 IU/L) or indirect bilirubin (≥1.2 mg/dL).Low serum haptoglobin concentration (≤25 mg/dL).Platelet count ≤100,000 cells/microL.Serum AST ≥70 IU/L.

Hypertension (blood pressure ≥140/90) and proteinuria are present in approximately 85 percent of cases, but it is important to remember that either or both may be absent in women with otherwise severe HELLP syndrome.

Medical and Surgical Disorders Confused with the HELLP Syndrome
Acute fatty liver of pregnancyAppendicitisDiabetes mellitusGallbladder diseaseGastroenteritisGlomerulonephritisHemolytic uremic syndromeHepatic encephalopathyHyperemesis gravidarumIdiopathic thrombocytopeniaKidney stonesPeptic ulcerPyelonephritisSystemic lupus erythematosus Thrombotic thrombocytopenic purpuraViral hepatitis

Test InterpretationBlood hematocrit. Hemoconcentration supports the diagnosis of
preeclampsia but hemolysis, if present, can decrease the hematocrit.
Platelet count Thrombocytopenia is a criterion of severe diseaseQuantification of protein excretion.
300 mg or more in 24 hours is necessary for diagnosis or at least 1+ protein on dipstick of two urine specimens collected at least four hours apart; 3+ or greater or 5 g or more per day is a criterion of severe disease.
Serum creatinine concentration.
An elevated or rising level suggests severe disease.
Serum alanine and aspartate amino transferase concentrations (ALT and AST).
Elevated or rising levels suggest hepatic dysfunction indicative of severe disease.
Tests for Microangiopathic hemolysis.
Elevated Serum lactate dehydrogenase (LDH) and red cell fragmentation (schistocytes or helmet cells) on peripheral blood smear.

Complications of PET
Long-term maternal risks

Long-term maternal risksCompared with women with no history of the disease, women with PET are at increased risk of :
hypertension (RR 3.70, 95% CI 2.70-5.05 at mean follow-up of 14 years),
IHD (RR 2.16, 95% CI 1.86-2.52 at mean follow-up of 11.7 years)
Stroke (RR 1.81, 95% CI 1.45-2.27 at mean follow-up of 10.4 years
VTE (RR 1.79, 95% CI 1.37-2.33 at mean follow-up of 4.7 years).
The absolute risk that a woman with or without a history of preeclampsia would develop one of these cardiovascular events at age 50 to 59 years was estimated to be 17.8 and 8.3 percent, respectively

DIAGNOSIS AND INITIAL EVALUATION


Management of PET
Confirm the diagnosis: by excluding other disorders characterized by hypertension and proteinuria.
Assess the severity of disease: whether mild or severe.
Fetal Assessment: by a non-stress test or biophysical profile, ultrasound to evaluate growth and amniotic fluid volume.

Powrie, R. O. JAMA 2007;298:1548-1558.
Quick Office Screen for Secondary Causes of Hypertension in Young Women

Laboratory evaluation to determine disease severity and characterize end organ involvement :
• Renal Function Evaluation: Quantification of protein excretion. Serum creatinine concentration Serum uric acid concentration• Hematological tests: Hematocrit Platelet count Lactic acid dehydrogenase concentration (LDH): RBCs smear may
indicate the presence of microangiopathic hemolysis.• Hepatic function: Serum alanine and aspartate aminotransferase concentrations
(ALT,AST)• Fetal well-being: Ultrasound to evaluate growth and amniotic fluid volume Non stress test and Biophysical profile

• Other causes of High Blood Pressure (renal, Vascular, Endocrinological)
• Preeclampsia versus essential hypertension:
o Onset: Hypertension occurring before the 20th. o Parity: Preeclampsia is far more common in primiparas.o Age: Preeclampsia is somewhat more common in both
young (<20 years) and older (>35 years) primigravidas.o Proteinuria: Proteinuria is present and increases with time
in preeclampsia, occasionally reaching the nephrotic range; by comparison, protein excretion is usually less than 1 g/day in hypertensive nephrosclerosis.
o Plasma uric acid concentration: Preeclampsia is typically associated with a rise in the plasma urate level to above 5.5 to 6 mg/dL (327 µmol/L).
Differential Diagnosis Of Preeclampsia

Symptoms of Central Nervous System Dysfunction
Blurred vision, Scotoma, Altered Mental Status, Severe Headache
Symptoms of liver capsule distension
Right upper quadrant or epigastric painNausea and vomiting
HepatocellularInjurty:
Serum transminase concentration at least twice normal
Severe blood pressure elevation:
Systolic blood pressure 160 mm Hg or diastolic 110 mm Hg on two occasions six hours apart
Thrombocytopenia:
Less than 100,000 platelets per cubic millimeter
Protenuria:
5 or more grams in 24 hours
Oligouria:
Severe fetal growth restriction
Criteria for Severe Pre-eclampsiaCriteria for Severe Pre-eclampsia

Treatment of PET

The Definitive Treatment Of Preeclampsia Is Delivery To Prevent Potential Maternal Complications.
Delivery Is Not Always In The Best Interests Of The Fetus.
In General, Intervention Is Based Upon:
- The Severity Of Preeclampsia.
- Maternal And Fetal Condition.
- Gestational Age.

At term ≥ 37 weeks: Induction of labour.
Remote from term: Expectant managemet
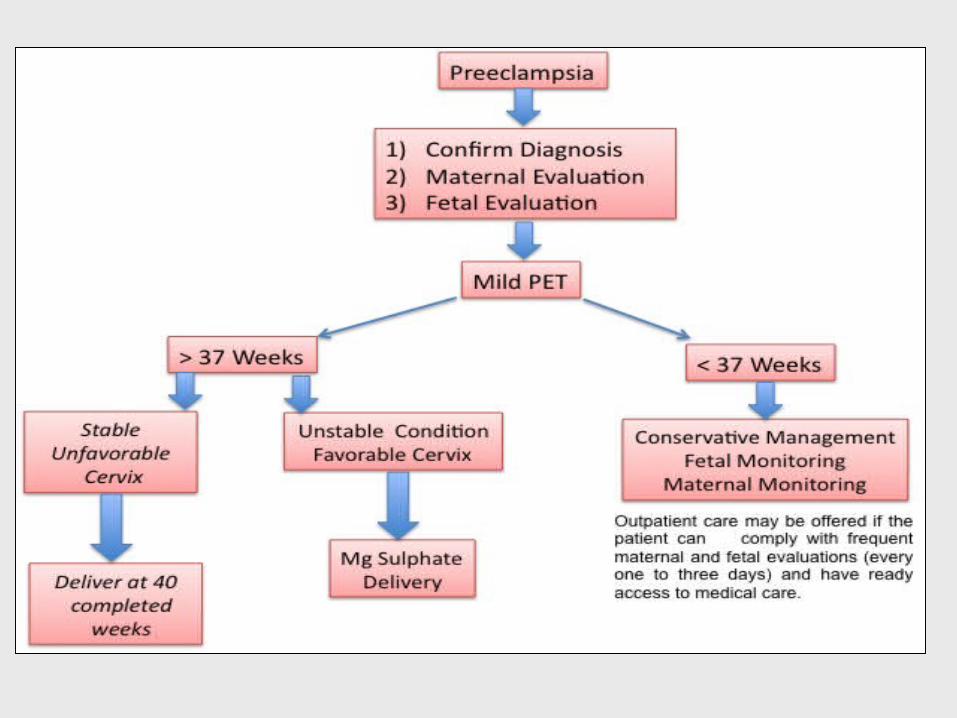
Treatment of Mild PET

Treatment of hypertension: antihypertensive drugs does not alter the course of the disease or diminish perinatal morbidity or mortality. The goal of therapy is a systolic pressure of 140 to 155 mmHg and diastolic pressure of 90 to 105 mmHg.
Assessment of fetal well-being: There are no data from randomized trials on which to base recommendations for the optimal type and frequency of fetal monitoring. Assessment of fetal growth: Early fetal growth restriction may be the first manifestation of preeclampsia or a sign of severe preeclampsia. Antenatal corticosteroids: Should be administered to women less than 34 weeks of gestation since preterm delivery is common. Indications for delivery: Mild preeclampsia may be delivered by 40 weeks of gestation.

Issues for Consideration
• Rest Vs. Restricted activity:
• Home Vs. Hospital Care:
• Laboratory follow-up: (once or twice weekly)
platelet count, creatinine, Quantification of urine protein, and liver enzymes
Lactic acid dehydrogenase (LDH) concentration is a better sign of hemolysis.

• Delivery, regardless of gestational age.
• Vaginal Delivery Should always be considered with cesarean delivery reserved for the usual obstetrical indications.
Treatment of Severe PET

• Anticonvulsant therapy:
• Control of Blood Pressure:
• Preparation for Delivery:
• Prevention of Complications:
Principle of Treatment of Severe PET

Anticonvulsant therapy: Magnesium Sulfate:
• Initiated at onset of labor or induction or prior to CS delivery and continued for 24 – 48 hours postpartum
• A loading dose of 4 to 6 g intravenously in 150 ml of
5% Dextrose Injection, at a rate not exceeding 3 ml per minute
followed by 1 to 2 g per hour as a continuous infusion. • Maintenance Dose:
- Patellar reflex is present (loss of reflexes being the first manifestation of symptomatic hypermagnesemia)
- Respirations exceed 12 per minute.- The urine output exceeds 100 mL per four
hours.

• It prevent eclampsia in part by selectively dilating the cerebral vasculature and relieving the cerebral vasospasm associated with preeclampsia It exerts this vasodilatory effect by:
• Decreasing the release of acetylcholine at motor end plates within the neuromuscular junction, thereby suppressing nerve transmission to vascular smooth muscle.
• Acting as a physiologic calcium antagonist to lower the intracellular calcium concentration within vascular smooth-muscle cells, which is necessary for activation of the myosin-actin contractile unit.
• Blocking excitatory amino acid receptors, including N-methyl-D-aspartate receptors, which have been implicated in the initiation and propagation of seizures .
Magnesium sulfate –Mechanism of action
Rapid infusion:Flushing, and warmth, probably related to peripheral vasodilation
and a drop in blood pressure. Nausea, vomiting, headache, muscle weakness, visual disturbances, and palpitations can also occur.
Dyspnea or chest pain may be symptoms of pulmonary edema, a rare side effect of magnesium sulfate administration.
Magnesium toxicity - loss of deep tendon reflexes occurs at 8 to 10 mEq/L- respiratory paralysis at 10 to 15 mEq/L, - cardiac arrest at 20 to 25 mEq/L.
Antidote:Calcium gluconate (1 g intravenously over at 5 to 10 minutes) may be administered to counteract magnesium toxicity.
Complication of magnesium: sulfate:
Labetalol (Normodyne):
Both Alpha and Beta Adrenerginc Blocker. Adult Dose20-30 mg IV initially; 40-60 mg IV q10-20 min; not to exceed 300 mg
Hydralazine (Apresoline):
direct vasodilatation of arterioles Adult Dose Initial: 5 mg IVMaintenance: 5-10 mg IV q20-30min
Antihypertensives

• INTRAPARTUM CARE:
Close, continuous maternal-fetal monitoring:
- worsening hypertension:
- deteriorating maternal hepatic:
- renal.
- cardiopulmonary
- hematologic function: - uteroplacental insufficiency or abruption (often manifested by nonreassuring fetal heart rate tracings, vaginal bleeding).


Gestation Hypertension
Gestation HypertensionElevated blood pressure first detected after 20 weeks of gestation in the absence of proteinuria.
The risks of gestational hypertension are mostly due to:
Development of preeclampsia: 50% among women who develop gestational hypertension before 30 weeks. Cases with severe symptoms and signs: severe hypertension: persistent headache, visual changes, growth restriction, oligohydramnios, epigastric or right upper abdominal pain, thrombocytopenia, or liver function abnormalities.

In these two situations, women with gestational
hypertension should be treated as though they have
preeclampsia (or HELLP syndrome), even in the
absence of proteinuria since they are high risk of
maternal and/or fetal morbidity .
The indications for and choice of antihypertensive
therapy in women with gestational hypertension are
the same as for women with preeclampsia.

Choice of drug and dose : (1) Acute management of severe hypertension, which may require parenteral therapy. (2) Longer-term blood pressure control during expectant management of severe preeclampsia.

Preexisting Hypertension

Preexisting HypertensionIncreased risk of adverse pregnancy outcome: “Superimposed preeclampsia” The most common risk is development of, two- to four-fold higher than in the general obstetric population.
Abruptio placentae (0.7 -1.5 percent).
Preterm birth <37 weeks (12 to 34 percent).
Fetal growth restriction (8-16 %). The risk is higher with severe preexisting BP in the first trimester

Women with uncomplicated preexisting hypertension who are normotensive or mildly hypertensive on medication may continue their therapy or have their antihypertensive agents tapered and/or stopped during pregnancy, with close monitoring of the maternal blood pressure response.
Neither the patient nor the fetus appears to be at risk from mild hypertension during pregnancy. More than 85 percent of hypertensive women will have uncomplicated pregnancies

Indications for initiating or reinstituting antihypertensive therapy are:
Persistent diastolic pressures of 95 to 99 mmHg, systolic pressures ≥ 150 mmHg.
Signs of hypertensive end-organ damage (e.g. ventricular dysfunction, retinopathy).
The goal of blood pressure control is systolic pressure between 140 and 150 mmHg and diastolic pressure between 90 and 100 mmHg

CONCLUSION: Pregnant women with chronic hypertension have significantly increased risks of maternal and perinatal morbidity and mortality.
Women with this condition should be treated as high risk with appropriate maternal and fetal surveillance

Eclampsia

Eclampsia• Eclampsia refers to the occurrence of one or more generalized
convulsions and/or coma in the setting of preeclampsia and in the absence of other neurologic conditions.
• The clinical manifestations appear anytime from the second trimester to the puerperium.
• INCIDENCE AND EPIDEMIOLOGY: 0.5 % of mildly PET
2 .0 % of severe PET
Antepartum (38 to 53 %)
Intrapartum (18 to 36 %)
< or =48 hours postpartum (5 to 39 %)
>48 hours postpartum (5 to 17 %)

CLINICAL MANIFESTATIONS AND DIAGNOSIS:
Maternal:
• Eclamptic seizures are almost always self-limiting and seldom last longer than 3 to 4 minutes.
• The diagnosis of preeclampsia/eclampsia sometimes may not be suspected prior to the development of seizures in women with relative hypertension (i.e. blood pressure elevated compared to patient's baseline, but less than 140/90 mmHg) and no proteinuria.
• Fifteen to 22 percent of eclamptic women have no evidence of proteinuria prior to their seizure.

• Cerebrovascular accident (hemorrhage, arterial or venous thrombosis).
• Hypertensive disease hypertensive encephalopathy pheochromocytoma
• Space-occupying lesions of the CNS (brain tumor, abscess).
• Metabolic disorders (hypoglycemia, uremia, inappropriate ADH secretion resulting in water intoxication).
• Infection (meningitis, encephalitis).
• Thrombotic thrombocytopenic purpura or thrombophilia
• Idiopathic epilepsy.
• Use of illicit drugs (e.g. methamphetamine, cocaine)
• Cerebral vasculitis.
DIFFERENTIAL DIAGNOSIS Of Eclampsia:

Maternal and Fetal complications of Eclampsia:
Eclampsia especially in developing countries and in absence of prenatal and intrapartum care is associated with high rate of maternal and fetal
mortality and morbidity .
The primary cause of maternal mortality is intracranial hemorrhage, which is also responsible for permanent brain damage and disabilities.

Outcome %
Abruption 7 to 10
Disseminated intravascular coagulation 7 to 11
Pulmonary edema 3 to 5
Acute renal failure 5 to 9
Aspiration pneumonia 2 to 3
Cardiopulmonary arrest 2 to 5
Liver hematoma 1
HELLP syndrome 10 to 15
Perinatal death 5.6 to 11.8
Preterm birth 50
Maternal and fetal outcome adopted of eclampsia from Sibai, BM. Obstet Gynecol 2005; 105:402.
.1Prevention of maternal hypoxia and trauma:
maintenance of airway patency and prevention of
aspiration in addition to protection of the patient from
injuring her tongue or mouth.
.2Management of severe hypertension
.3Prevention of recurrent seizures :
.4Evaluation for prompt delivery :
.5Close monitoring for maternal and fetal conditions :
Principles of Treatment of Eclampsia

Thanks