hypertension - homepage | circulationcirc.ahajournals.org/content/121/20/2183.full.pdfthis analysis...
TRANSCRIPT

Hypertension
Acute Kidney Injury and Cardiovascular Outcomes in AcuteSevere Hypertension
Lynda A. Szczech, MD, MSCE; Christopher B. Granger, MD; Joseph F. Dasta, MSc, FCCM;Alpesh Amin, MD; W. Frank Peacock, MD; Peter A. McCullough, MD, MPH;
John W. Devlin, PharmD; Matthew R. Weir, MD, MS; Jason N. Katz, MD;Frederick A. Anderson, Jr, PhD; Allison Wyman, MS; Joseph Varon, MD; for the Studying the
Treatment of Acute Hypertension Investigators
Background—Little is known about the association of kidney dysfunction and outcome in acute severe hypertension. Thisstudy aimed to measure the association between baseline chronic kidney disease (estimated glomerular filtration rate),acute kidney injury (AKI, decrease in estimated glomerular filtration rate �25% from baseline) and outcome in patientshospitalized with acute severe hypertension.
Methods and Results—The Studying the Treatment of Acute Hypertension (STAT) registry enrolled patients with acutesevere hypertension, defined as �1 blood pressure measurement �180 mm Hg systolic and/or �110 mm Hg diastolicand treated with intravenous antihypertensive therapy. Data were compared across groups categorized by admissionestimated glomerular filtration rate and AKI during admission. On admission, 79% of the cohort (n�1566) had at leastmild chronic kidney disease (estimated glomerular filtration rate �60 mL/min in 46%, �30 mL/min in 22%). Chronickidney disease patients were more likely to develop heart failure (P�0.0001), non–ST-elevation myocardial infarction(P�0.003), and AKI (P�0.007). AKI patients were at greater risk of heart failure and cardiac arrest (P�0.0001 forboth). Subjects with AKI experienced higher mortality at 90 days (P�0.003). Any acute loss of estimated glomerularfiltration rate during hospitalization was independently associated with an increased risk of death (odds ratio, 1.05;P�0.03 per 10-mL/min decline). Other independent predictors of mortality included increasing age (P�0.0001), malegender (P�0.016), white versus black race (P�0.003), and worse baseline kidney function (P�0.003).
Conclusions—Chronic kidney disease is a common comorbidity among patients admitted with acute severe hypertension,and AKI is a frequent form of acute target organ dysfunction, particularly in those with baseline chronic kidney disease.Any degree of AKI is associated with a greater risk of morbidity and mortality. (Circulation. 2010;121:2183-2191.)
Key Words: epidemiology � hypertension � kidney � mortality
Both chronic kidney disease (CKD) and acute kidneyinjury (AKI) are associated with an increased risk of
mortality.1–3 The risks associated with abnormal kidneyfunction are underscored by the poor outcomes of patientswith end-stage renal disease (ESRD).4 With greater aware-ness of the methods by which both conditions can becategorized and compared across studies, it is becomingmore apparent that the risk associated with either abnormalserum creatinine or increases in serum creatinine manifestearly and increase directly with a decline in kidneyfunction.5–7
Editorial see p 2160Clinical Perspective on p 2191
Multiple studies further document the impact of chronichypertension on kidney function, with hypertension as a cause ofESRD among a significant proportion of patients requiringdialysis.2 However, the impact of acute severe hypertension onkidney function has not been explored fully. Knowledge of howoutcomes vary among patients with acute severe hypertensionand either CKD or AKI may enable us to identify high-riskgroups that warrant increased clinical surveillance.
Continuing medical education (CME) credit is available for this article. Go to http://cme.ahajournals.org to take the quiz.Received July 24, 2009; accepted March 23, 2010.From the Department of Medicine, Division of Nephrology, Duke University Medical Center, Durham, NC (L.A.S.); Duke Clinical Research
Institute, Durham, NC (C.B.G.); College of Pharmacy, University of Texas, Round Rock (J.F.D.); UCIMC, Orange, Calif (A.A.); EmergencyDepartment, The Cleveland Clinic, Cleveland, Ohio (W.F.P.); William Beaumont Hospital, Royal Oak, Mich (P.A.M.); School of Pharmacy,Northeastern University School of Pharmacy, Boston, Mass (J.W.D.); Division of Nephrology, University of Maryland School of Medicine,Baltimore (M.R.W.); Divisions of Cardiology and Pulmonary and Critical Care Medicine, University of North Carolina at Chapel Hill (J.N.K.);Center for Outcomes Research, University of Massachusetts Medical School, Worcester (F.A.A., A.W.); and University of Texas Health ScienceCenter and St Luke’s Episcopal Hospital, Houston (J.V.).
Correspondence to Lynda Anne Szczech, MD, MSCE, Duke University Medical Center, Box 3646, Durham, NC 27710. E-mail [email protected]
© 2010 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.109.896597
2183
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://circ.ahajournals.org/
Dow
nloaded from

This analysis is based on data from the Studying theTreatment of Acute Hypertension (STAT) registry, whichenrolled patients admitted to hospital for acute severe hyper-tension. The study was undertaken to define the risk amongpatients with acute severe hypertension and AKI and the riskassociated with both AKI and CKD on cardiovascular out-comes and mortality.
MethodsSTAT is a US, hospital-based, retrospective observational study ofthe routine management practices and outcomes of patients withacute severe hypertension managed in the emergency or critical caresettings (a setting with the capability of providing intravenousantihypertensive administration and arterial line blood pressure [BP]monitoring) and treated with intravenous antihypertensive therapy.Consecutive adults admitted with at least 1 BP measurement�180 mm Hg systolic and/or �110 mm Hg diastolic or �140/�90 mm Hg in patients with subarachnoid hemorrhage who wereadministered at least 2 antihypertensive boluses or were placed oncontinuous infusion therapy within 24 hours of hospitalization at 1 of25 centers were enrolled. Antihypertensives included diltiazem,enalapril, esmolol, fenoldopam, hydralazine, labetalol, metoprolol,nicardipine, nitroglycerin, phentolamine, sodium nitroprusside, andverapamil. Exclusion criteria included hypertension therapy in theperioperative setting or during the peripartum period, therapy de-layed �24 hours after hospitalization, nonintravenous administrationof antihypertensive drugs, and patients receiving “comfort caremeasures” only.
Data on demographics, medical history, admitting information,in-hospital management, 90-day outcomes (readmission, death, andrecurrent severe hypertension), and death up to 6 months after theindex hospitalization were collected by trained data abstractors. TheSocial Security Death Index was used to determine survival at 6months after presentation to hospital with the acute hypertensiveevent.
This study was conducted in accordance with the Health InsurancePortability and Accountability Act of 1996, with the approval of alllocal institutional review boards. It was done in compliance with theregulations of participating hospitals.
Definitions of VariablesData on serum creatinine concentrations were collected at 4 points:up to 12 months before admission (when available), at admission, atpeak creatinine, and at discharge when measured and available.Estimated glomerular filtration rate (eGFR) was calculated for eachavailable serum creatinine measure with the Modification of Diet inRenal Disease formula.8 For each patient, baseline kidney functionwas categorized according to the National Kidney FoundationDisease Outcomes Quality Initiative clinical practice guidelines9 of�90 mL/min (normal kidney function), 60 to 89 mL/min (mildkidney disease), 30 to 59 mL/min (moderate), �30 mL/min (severe),or dialysis dependent. The group categorized with kidney function�90 mL/min included patients with or without kidney disease basedon the presence or absence of proteinuria, respectively; no attemptwas made to divide this group because of the potential impact ofacute severe hypertension on the appearance of proteinuria atadmission.
For each patient, the relative change in GFR was calculated bysubtracting the lowest recorded eGFR from the earliest availableeGFR (before or on admission) and dividing that by the earliestavailable measure. The latter was used to minimize the impact of anadmission creatinine that is already elevated by early kidney injury.Change in kidney function from baseline to nadir GFR or severity ofAKI was analyzed continuously and categorically. Change in kidneyfunction was categorized with the RIFLE criteria (risk, injury,failure, loss, end-stage renal disease)10 based on GFR. A differenceof �25% from baseline to nadir was classified as no change inkidney function. As per the RIFLE criteria,10 risk was defined as aGFR decrease of 25% to 50%; injury was defined as a decrease of
50% to 75%; and failure and more severe categories were defined asa loss of �75% and were combined because of the limited numbersof subjects and information available on the chronicity of theirkidney injury. Patients with ESRD at baseline were not classifiedwith these criteria and were analyzed separately.
Description of Analyses PerformedPatients were categorized according to baseline eGFR initially intolevels of CKD and subsequently on the basis of loss of eGFR intolevels of AKI. Categorical variables are reported as frequencies.Nominal variables were compared by use of the �2 test; dichotomousand ordinal variables were compared by use of the Mantel-Haenszel�2 test. Continuous variables are displayed as medians with 25th and75th percentiles. To test for linear trends among continuous vari-ables, each category of CKD was assigned its median value. Aunivariate linear regression on these values was then performed foreach outcome; the P value for the slope is given in the tables.Similarly, each category of AKI was assigned its median value, againwith a linear regression performed on these values. For continuousvariables with nonnormal distributions, we performed linear trendtests on the untransformed variable and then a second time using arank transformation (a nonparametric test that ensures that extremevalues have no undue influence). In cases when results disagree, wereport both results. Logistic regression was used to estimate theassociation between AKI and mortality risk in adjusted analyses.Candidate variables included in this model were age, gender, race,Hispanic ethnicity, diabetes mellitus, baseline eGFR, peripheralvascular disease, greatest decrement in eGFR during AKI, protein-uria, and the interaction between baseline eGFR and proteinuria.
All P values are 2 sided, and all confidence intervals are 95%intervals. Analyses were performed with SAS (version 9.1, SASInstitute Inc, Cary, NC).
ResultsA total of 1566 patients were included in the STAT studybetween January 1, 2007, and April 6, 2008. Of these, 1542had sufficient creatinine measurements available to eval-uate the occurrence and severity of baseline CKD, and1369 had sufficient creatinine measurements available toevaluate the occurrence and severity of AKI during theperiod of observation.
CKD at BaselineMost of the patients (79%) had at least mild (stage II) CKDat baseline (Table 1), with the incidence of mild, moderate,and severe kidney disease being 32%, 23%, and 11%,respectively. A further 11% of patients were dialysis depen-dent on admission. In general, patients with more severeCKD at baseline presented with higher BP and were morelikely to be of black race and to have comorbidities such ascardiac disease, hypertension, diabetes mellitus, and periph-eral vascular disease (all P�0.0001).
During hospitalization, patients with worse baseline CKDwere more likely to experience complications such as acuteleft ventricular dysfunction (P�0.0001) and non–ST-segmentmyocardial infarction (P�0.003; Table 2) and were lesslikely to experience intracranial hemorrhage (intracerebral,P�0.001; subarachnoid, P�0.0001). Subjects in each cate-gory of CKD experienced AKI; however, patients with themost severe CKD on admission were more likely to experi-ence the greatest decrement in kidney function with AKI(P�0.007).
2184 Circulation May 25, 2010
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

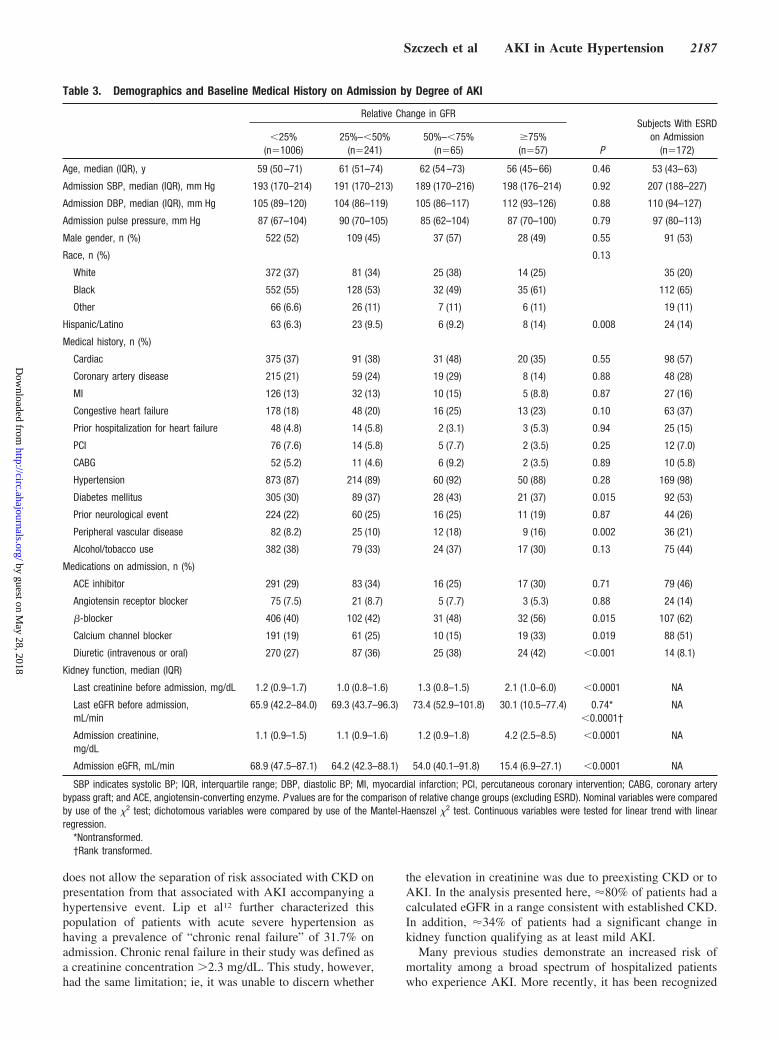
AKI During HospitalizationThe change in kidney function for all patients was assessedrelative to their own baseline value, and patients werecategorized by severity of decline (Table 3). Of the entirecohort, 64% had a �25% decline in kidney function; 15%had an acute decline in between 25% and �50%; 4.2%developed kidney injury; and 3.6% developed renal failure.
There were few differences in baseline characteristicsamong subjects in the different categories of AKI. Subjectswith the most severe kidney injury were slightly more likelyto be of Hispanic ethnicity compared with those with lesserdegrees of AKI (P�0.008). Other differences included agreater proportion of subjects with diabetes mellitus, periph-eral vascular disease, and CKD among those with any degreeof AKI compared with patients without a change in GFR(P�0.015, P�0.002, and P�0.0001, respectively). Onlypatients with severe AKI had a significantly different pread-mission eGFR (30.1 versus 65.9 to 73.4 mL/min; P�0.0001).Although the downward trend in eGFR calculated on admis-sion was more evident based on the degree of eventual AKI(68.9, 64.2, and 54.0 mL/min for �25%, 25% to �50%, and50% to �75%, respectively), the category of patients with themost severe degree of injury was decreased most dramaticallyat 15.4 mL/min. Otherwise, no differences were seen inadmission BP measurements, race, or presence of otherpreexisting comorbid conditions.
Few differences existed between types of antihypertensivestaken at admission among subjects based on category ofkidney injury. A greater proportion of patients with increas-ing severity of kidney injury received diuretics before admis-sion (P�0.001). However, no differences were seen among
categories of subjects with respect to the use of angiotensin-converting enzyme inhibitors or angiotensin receptor block-ers. Subjects with greater severity of kidney injury were morelikely to receive �-blockers (P�0.015). With calcium chan-nel blockers, a statistically significant difference existedamong categories of patients by severity of kidney injury(P�0.019); however, this difference did not appear clinicallymeaningful.
In general, patients who experienced greater degrees ofkidney injury also had a greater risk of other end-organ injuryor dysfunction (Table 4). This included a greater risk of acuteleft ventricular dysfunction and cardiac arrest (P�0.0001 forboth). Other adverse events that were more likely amongsubjects with AKI included the presence of moderate tosevere bleeding, recurrent severe acute hypertension, andneurological decline (P�0.001, P�0.001, and P�0.0001,respectively).
With respect to treatment of the acute hypertensive epi-sode, there were no differences among categories of subjectsbased on degree of kidney injury in the time to treatment withan intravenous agent or time to 10% decrease in systolic BP(Table 4). The duration of intravenous therapy and number ofintravenous agents, however, were significantly greateramong patients with greater degrees of AKI (bothP�0.0001). Subjects with a greater severity of AKI had ahigher in-hospital mortality rate and, among those dis-charged, a longer length of hospitalization (P�0.0001 forboth; Table 5). Patients with a greater severity of AKIexperienced an increased risk of rehospitalization for renalfailure (P�0.001) or heart failure (P�0.034). Subjects withany AKI experienced a higher risk of mortality at 90 days(P�0.003; Figure 1).
Table 1. Demographics and Baseline Medical History on Admission by CKD stage
All Patients(n�1566)
eGFR �90 mL/min(n�322)
eGFR 60–89 mL/min(n�503)
eGFR 30–59 mL/min(n�366)
eGFR �30 mL/min(n�179)
ESRD(n�172) P
Admission SBP, median(IQR), mm Hg
194 (172–216) 182 (157–204) 192 (170–212) 197 (175–220) 205 (190–224) 207 (188–227) �0.0001
Admission DBP, median(IQR), mm Hg
105 (88–121) 104 (87–115) 105 (88–120) 102 (87–122) 110 (93–126) 110 (94–127) 0.002
Admission pulse, median(IQR), bpm
87 (74–102) 86 (74–102) 85 (74–102) 88 (74–102) 86 (76–102) 91 (75–105) 0.94
Age, median (IQR), y 58 (49–70) 55 (48–61) 60 (50–73) 66 (52–79) 59 (49–70) 53 (43–63) �0.0001
Male gender, n (%) 800 (51) 190 (59) 249 (50) 173 (47) 84 (47) 91 (53) 0.07
Race, n (%) �0.0001
White 531 (34) 119 (37) 187 (37) 145 (40) 41 (23) 35 (20)
Black 878 (56) 165 (51) 272 (54) 190 (52) 121 (68) 112 (65)
Other 126 (8.1) 31 (9.6) 36 (7.2) 23 (6.3) 15 (8.4) 19 (11)
Hispanic/Latino 126 (8.1) 31 (9.6) 35 (7.0) 19 (5.2) 15 (8.4) 24 (14) 0.23
Medical history, n (%)
Cardiac 626 (40) 71 (22) 184 (37) 175 (48) 88 (49) 98 (57) �0.0001
Hypertension 1387 (89) 259 (80) 436 (87) 334 (91) 169 (94) 169 (98) �0.0001
Diabetes mellitus 542 (35) 83 (26) 137 (27) 141 (39) 83 (46) 92 (53) �0.0001
Peripheral vasculardisease
166 (11) 17 (5.3) 39 (7.8) 43 (12) 29 (16) 36 (21) �0.0001
DBP indicates diastolic BP; IQR, interquartile range; and SBP, systolic BP. P values are for the comparison of eGFR groups (excluding ESRD). Nominal variableswere compared by use of the �2 test; dichotomous variables were compared by use of the Mantel-Haenszel �2 test. Continuous variables were tested for linear trendusing linear regression.
Szczech et al AKI in Acute Hypertension 2185
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

Subjects with worsening degrees of both baseline kidneyfunction and severity of AKI experienced a greater risk ofmortality at 90 days (Figure 2). In the multivariable model,any acute loss of eGFR during hospitalization was indepen-dently associated with an increased risk of death (odds ratio,1.05; P�0.026 per 10-mL/min decline; Figure 3) whenclinical and demographic factors associated with severity ofAKI were controlled for. Other predictors of mortality in-cluded increasing age (P�0.0001), male gender (P�0.02),white versus black race (P�0.003), and poorer baselinekidney function (P�0.002).
DiscussionIn this large multicenter study of patients hospitalized withacute severe hypertension, the presence of either CKD or AKIwas associated with worse outcomes, including increasedlength of hospitalization. Even after accounting for baselinekidney dysfunction, the presence of AKI or an acute deteri-oration in kidney function during hospitalization is associatedwith morbidity and predicts mortality. This is the first study
to demonstrate that this increase in risk begins with only asubtle decline in kidney function and increases progressivelywith severity of AKI. Although the association with otherend-organ complications likely reflects the severity of thehypertensive episode, arguably AKI may have a more mech-anistic relationship to increased mortality. Importantly, be-cause kidney function was more severely impaired at base-line, there was a greater frequency and severity of subsequentAKI during the hospitalization. Finally, except for elevatedcreatinine concentration on admission, there were few iden-tifying clinical factors among patients who developed severeAKI to distinguish them from patients with no or lesserdegrees of kidney injury.
Although the association between CKD and outcomes inthe setting of acute systolic hypertension has not been fullydefined, these results are consistent with previous studies. Lipet al11 demonstrated that patients presenting with acceleratedhypertension whose blood urea nitrogen was �10 mmol/Land serum creatinine was �200 �mol/L had a worse survival.Although consistent with the results presented here, this study
Table 2. End-Organ Injury and Adverse Events During the Hospitalization for Accelerated Hypertension by CKD Stage
All Patients(n�1566),
n (%)
eGFR �90 mL/min(n�322),
n (%)
eGFR 60–89 mL/min(n�503),
n (%)
eGFR 30–59 mL/min(n�366),
n (%)
eGFR �30 mL/min(n�179),
n (%)
ESRD(n�172),
n (%) P
Cardiac
Acute LV dysfunction 228 (15) 22 (6.8) 49 (9.7) 72 (20) 33 (18) 50 (29) �0.0001
NSTEMI 88 (5.6) 11 (3.4) 19 (3.8) 32 (8.7) 13 (7.3) 13 (7.6) 0.003
STEMI 43 (2.8) 8 (2.5) 18 (3.6) 8 (2.2) 5 (2.8) 4 (2.3) 0.66
Unstable angina 50 (3.2) 7 (2.2) 19 (3.8) 17 (4.6) 1 (0.6) 5 (2.9) 0.80
Cardiac arrest/ventricularfibrillation
48 (3.1) 8 (2.5) 10 (2.0) 14 (3.8) 9 (5.0) 6 (3.5) 0.10
Cerebrovascular
Ischemic stroke 95 (6.1) 16 (5.0) 31 (6.2) 31 (8.5) 7 (3.9) 10 (5.8) 0.84
Intracerebral hemorrhage 179 (11) 47 (15) 64 (13) 42 (11) 16 (8.9) 8 (4.7) �0.001
Subarachnoid hemorrhage 186 (12) 78 (24) 67 (13) 28 (7.7) 11 (6.2) 1 (0.6) �0.0001
Septicemia 27 (1.7) 8 (2.5) 3 (0.6) 6 (1.6) 4 (2.2) 6 (3.5) 0.22
Moderate to severebleeding
69 (4.4) 15 (4.7) 20 (4.0) 11 (3.0) 13 (7.3) 10 (5.8) 0.28
AKI 0.007
No change in function(�25%)
1006 (64) 211 (66) 401 (80) 277 (76) 117 (65) NA
Decrement �25% and�50%
241 (15) 80 (25) 75 (15) 58 (16) 28 (16) NA
Decrement �50% and�75%
65 (4.2) 25 (7.8) 16 (3.2) 23 (6.3) 1 (0.6) NA
Decrement �75% 57 (3.6) 6 (1.9) 11 (2.2) 8 (2.2) 32 (18) NA
Mortality
During hospitalization 108 (6.9) 20 (6.2) 27 (5.4) 34 (9.3) 15 (8.4) 10 (5.8) 0.38
Between discharge and90 d
64 (4.7) 6 (2.2) 19 (4.2) 25 (7.8) 5 (3.3) 9 (5.8) 0.07
Mortality at 90 d (total) 172 (11) 26 (8.1) 46 (9.2) 59 (16) 20 (11) 19 (11) 0.07
Between 90 d and 6 mo* 40 (3.5) 10 (4.3) 7 (1.9) 9 (3.5) 5 (3.9) 9 (7.3) 0.11
LV indicates left ventricular; NSTEMI, non–ST-segment myocardial infarction. P values are for the comparison of eGFR groups (excluding ESRD) by use of theMantel-Haenszel �2 test.
*Among the 1139 patients alive at 90 days and with valid Social Security number.
2186 Circulation May 25, 2010
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from
does not allow the separation of risk associated with CKD onpresentation from that associated with AKI accompanying ahypertensive event. Lip et al12 further characterized thispopulation of patients with acute severe hypertension ashaving a prevalence of “chronic renal failure” of 31.7% onadmission. Chronic renal failure in their study was defined asa creatinine concentration �2.3 mg/dL. This study, however,had the same limitation; ie, it was unable to discern whether
the elevation in creatinine was due to preexisting CKD or toAKI. In the analysis presented here, �80% of patients had acalculated eGFR in a range consistent with established CKD.In addition, �34% of patients had a significant change inkidney function qualifying as at least mild AKI.
Many previous studies demonstrate an increased risk ofmortality among a broad spectrum of hospitalized patientswho experience AKI. More recently, it has been recognized
Table 3. Demographics and Baseline Medical History on Admission by Degree of AKI
Relative Change in GFR
P
Subjects With ESRDon Admission
(n�172)�25%
(n�1006)25%–�50%
(n�241)50%–�75%
(n�65)�75%(n�57)
Age, median (IQR), y 59 (50–71) 61 (51–74) 62 (54–73) 56 (45–66) 0.46 53 (43–63)
Admission SBP, median (IQR), mm Hg 193 (170–214) 191 (170–213) 189 (170–216) 198 (176–214) 0.92 207 (188–227)
Admission DBP, median (IQR), mm Hg 105 (89–120) 104 (86–119) 105 (86–117) 112 (93–126) 0.88 110 (94–127)
Admission pulse pressure, mm Hg 87 (67–104) 90 (70–105) 85 (62–104) 87 (70–100) 0.79 97 (80–113)
Male gender, n (%) 522 (52) 109 (45) 37 (57) 28 (49) 0.55 91 (53)
Race, n (%) 0.13
White 372 (37) 81 (34) 25 (38) 14 (25) 35 (20)
Black 552 (55) 128 (53) 32 (49) 35 (61) 112 (65)
Other 66 (6.6) 26 (11) 7 (11) 6 (11) 19 (11)
Hispanic/Latino 63 (6.3) 23 (9.5) 6 (9.2) 8 (14) 0.008 24 (14)
Medical history, n (%)
Cardiac 375 (37) 91 (38) 31 (48) 20 (35) 0.55 98 (57)
Coronary artery disease 215 (21) 59 (24) 19 (29) 8 (14) 0.88 48 (28)
MI 126 (13) 32 (13) 10 (15) 5 (8.8) 0.87 27 (16)
Congestive heart failure 178 (18) 48 (20) 16 (25) 13 (23) 0.10 63 (37)
Prior hospitalization for heart failure 48 (4.8) 14 (5.8) 2 (3.1) 3 (5.3) 0.94 25 (15)
PCI 76 (7.6) 14 (5.8) 5 (7.7) 2 (3.5) 0.25 12 (7.0)
CABG 52 (5.2) 11 (4.6) 6 (9.2) 2 (3.5) 0.89 10 (5.8)
Hypertension 873 (87) 214 (89) 60 (92) 50 (88) 0.28 169 (98)
Diabetes mellitus 305 (30) 89 (37) 28 (43) 21 (37) 0.015 92 (53)
Prior neurological event 224 (22) 60 (25) 16 (25) 11 (19) 0.87 44 (26)
Peripheral vascular disease 82 (8.2) 25 (10) 12 (18) 9 (16) 0.002 36 (21)
Alcohol/tobacco use 382 (38) 79 (33) 24 (37) 17 (30) 0.13 75 (44)
Medications on admission, n (%)
ACE inhibitor 291 (29) 83 (34) 16 (25) 17 (30) 0.71 79 (46)
Angiotensin receptor blocker 75 (7.5) 21 (8.7) 5 (7.7) 3 (5.3) 0.88 24 (14)
�-blocker 406 (40) 102 (42) 31 (48) 32 (56) 0.015 107 (62)
Calcium channel blocker 191 (19) 61 (25) 10 (15) 19 (33) 0.019 88 (51)
Diuretic (intravenous or oral) 270 (27) 87 (36) 25 (38) 24 (42) �0.001 14 (8.1)
Kidney function, median (IQR)
Last creatinine before admission, mg/dL 1.2 (0.9–1.7) 1.0 (0.8–1.6) 1.3 (0.8–1.5) 2.1 (1.0–6.0) �0.0001 NA
Last eGFR before admission,mL/min
65.9 (42.2–84.0) 69.3 (43.7–96.3) 73.4 (52.9–101.8) 30.1 (10.5–77.4) 0.74*�0.0001†
NA
Admission creatinine,mg/dL
1.1 (0.9–1.5) 1.1 (0.9–1.6) 1.2 (0.9–1.8) 4.2 (2.5–8.5) �0.0001 NA
Admission eGFR, mL/min 68.9 (47.5–87.1) 64.2 (42.3–88.1) 54.0 (40.1–91.8) 15.4 (6.9–27.1) �0.0001 NA
SBP indicates systolic BP; IQR, interquartile range; DBP, diastolic BP; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary arterybypass graft; and ACE, angiotensin-converting enzyme. P values are for the comparison of relative change groups (excluding ESRD). Nominal variables were comparedby use of the �2 test; dichotomous variables were compared by use of the Mantel-Haenszel �2 test. Continuous variables were tested for linear trend with linearregression.
*Nontransformed.†Rank transformed.
Szczech et al AKI in Acute Hypertension 2187
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

that even small reductions in kidney function are correlatedwith mortality.13–16 Among studies of patients with acutesevere hypertension, this study provides the first descriptionthat this risk begins to increase with more subtle relative
changes in GFR of between 25% and 50% of the baselinevalue. It is noteworthy that there were a few differences inbaseline clinical parameters on admission among patientscategorized by their subsequent severity of AKI. This indi-
Table 4. End-Organ Injury, Adverse Events, and Treatment Received During the Hospitalization for Accelerated Hypertension byDegree of AKI
Relative Change in GFR
P
Subjects With ESRDon Admission
(n�172)�25%
(n�1006)25%–�50%
(n�241)50%–�75%
(n�65)�75%(n�57)
Cardiac, n (%)
Acute left ventricular dysfunction/PE 105 (10) 33 (14) 18 (28) 20 (35) �0.0001 50 (29)
NSTEMI 53 (5.3) 10 (4.2) 5 (7.7) 7 (12) 0.08 13 (7.6)
STEMI 25 (2.5) 10 (4.2) 3 (4.6) 1 (1.8) 0.45 4 (2.3)
Unstable angina 28 (2.8) 11 (4.6) 3 (4.6) 2 (3.5) 0.26 5 (2.9)
Cardiac arrest/VF 18 (1.8) 13 (5.4) 3 (4.6) 7 (12) �0.0001 6 (3.5)
Cerebrovascular, n (%)
Ischemic stroke 67 (6.7) 11 (4.6) 4 (6.2) 3 (5.3) 0.41 10 (5.8)
Intracerebral hemorrhage 118 (12) 40 (17) 8 (12) 3 (5.3) 0.84 8 (4.7)
Subarachnoid hemorrhage 136 (14) 37 (15) 10 (15) 1 (1.8) 0.18 1 (0.6)
Septicemia, n (%) 8 (0.8) 5 (2.1) 5 (7.7) 3 (5.3) �0.0001 6 (3.5)
Moderate to severe bleeding, n (%) 34 (3.4) 13 (5.4) 4 (6.2) 8 (14) �0.001 10 (5.8)
Hypotension resulting from IV arterial hypertensiontreatment, n (%)
33 (3.3) 10 (4.2) 3 (4.6) 5 (8.8) 0.044 10 (5.8)
Recurrent severe acute hypertension, n (%) 268 (27) 86 (35) 26 (40) 21 (37) 0.001 42 (24)
Neurological decline, n (%) 43 (4.3) 20 (8.3) 8 (12) 8 (14) �0.0001 9 (5.2)
Time from qualifying BP to start of IV, median(IQR), h*
1.3 (0.5–3.0) 1.2 (0.4–3.7) 1.4 (0.6–2.8) 1.2 (0.4–2.9) 0.85 1.3 (0.6–3.6)
Time from qualifying BP to 10% SBP decrease,median (IQR), h*
3.6 (1.5–8.5) 3.3 (1.6–11) 4.4 (1.7–14) 3.6 (1.6–8.5) 0.12 3.9 (1.7–11)
Total time of IV treatment, median (IQR), h* 5.5 (1.6–16) 7.7 (2.5–20) 11 (4.3–40) 17 (7.0–33) �0.0001 7.0 (2.3–18)
IV drugs used, median (IQR), n* 2 (1–2) 2 (1–3) 2 (2–3) 2 (2–3) �0.0001 2 (1–3)
Discharge creatinine, median (IQR), md/dL† 1.1 (0.8–1.5) 1.2 (0.9–1.9) 1.6 (1.1–2.2) 3.5 (1.6–4.6) �0.0001 NA
Discharge eGFR, median (IQR), mL/min† 73.1 (50.5–95.2) 61.4 (36.4–84.7) 48.5 (30.7–78.8) 18.8 (11.7–39.4) �0.0001 NA
PE indicates pulmonary embolism; NSTEMI, non–ST-segment myocardial infarction; VF, ventricular fibrillation; SBP, systolic blood pressure; and IQR, interquartilerange. P values are for the comparison of relative change groups (excluding ESRD). Dichotomous variables were compared by use of the Mantel-Haenszel �2 test.Continuous variables were tested for linear trend with linear regression.
*Excludes patients with a presumptive primary admitting diagnosis of hemorrhagic stroke, subdural hematoma, or subarachnoid hemorrhage.†Excludes patients who were dialysis dependent at discharge (n�1 for �25%, n�1 for 25% to �50%, n�0 for 50% to �75%, and 23 for �75%).
Table 5. Discharge Findings and 90-Day Follow-Up Information by Degree of AKI
�25%(n�1006)
25%–�50%(n�241)
50%–�75%(n�65)
�75%(n�57) P
Subjects With ESRDon Admission
(n�172)
Length of stay, median (IQR), d 4 (2, 8) 7 (4, 14) 9 (5, 18) 9 (6, 20) �0.0001 3 (2, 7)
Mortality during hospitalization, n (%) 50 (5.0) 30 (12) 10 (15) 6 (11) �0.0001 10 (5.8)
Readmission (by cause), n (%)*
Any 270 (32) 65 (34) 20 (42) 16 (33) 0.26 81 (54)
Renal failure 23 (2.7) 4 (2.1) 2 (4.2) 7 (15) 0.001 35 (23)
Heart failure 28 (3.3) 5 (27) 6 (13) 3 (6.3) 0.034 13 (8.7)
Mortality between discharge and 90 d, n (%)† 32 (3.6) 14 (7.0) 4 (7.8) 5 (10) 0.003 9 (5.8)
Mortality between 90 d and 6 mo, n (%)‡ 22 (2.9) 6 (3.7) 3 (8.3) 0 (0.0) 0.78 9 (7.3)
IQR indicates interquartile range. P values are for the comparison of relative change groups (excluding ESRD). Dichotomous variables were compared by use ofthe Mantel-Haenszel �2 test. Continuous variables were tested for linear trend with linear regression.
*Among the 1313 patients discharged alive and not lost to readmission follow-up.†Among the 1369 patients discharged alive and whose vital status could be determined during follow-up.‡Among the 1219 patients alive at 90 days and with valid Social Security number.
2188 Circulation May 25, 2010
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

cates that vigilant surveillance of kidney function afteradmission is important to identify this higher-risk population.Furthermore, although the risk of mortality was increased, sowere the risks of other significant clinical events such as acuteheart failure, cardiac arrest, and bleeding episodes.
Our study has 2 important clinical implications. The first isthat there appears to be a critical mass of functioningnephrons at baseline in the setting of hypertensive urgencies.This is partially reflected in the baseline eGFR compensatingfor any degree of organ injury or dysfunction to keep serumcreatinine relatively unchanged in blood. In those withreduced eGFR at baseline, as a proxy for a reduced number ofremnant nephron units, there is a likely loss of compensatoryfiltration in the setting of acute hypertension and hence theexpression of AKI in terms of a rise in creatinine and fall ineGFR. The second is that markers of renal filtration such ascreatinine are crude reflections of AKI as a disease process.Our study highlights the need for novel markers of AKI thatgive rapid specificity to renovascular, glomerular, and tubularinjury before there is an elevation of filtered protein in theblood.17 It is hoped that the development of these markerswill lead to novel treatment strategies that not only lower BPbut also result in improved renal and cardiac outcomes.
Study LimitationsThe STAT registry is the largest observational cohort study tobe conducted to date and provides data on a heterogeneouspopulation of individuals presenting with acute severe hyper-tension. STAT is subject to certain inherent limitations andpotential biases, including the collection of nonrandomizeddata and missing or incomplete information. Participatingsites may not be representative of all US hospitals, andpatients with acute hypertension likely differ by region. Thestudy is subject to selection bias because the entry criteriarequired the physician to initiate intravenous antihypertensivetherapy. We do not have complete information on follow-up,and we may underestimate the degree to which follow-upoccurred. Although the enrollment of patients from multiplesites enhances power and generalizability compared with asingle-center study, it introduces the complexities of compar-ison of serum creatinine measurements from multiple labo-ratories. Although the bias associated with this was mini-mized through the use of changes in kidney function relativeto each individual’s baseline, the effect of this misclassifica-tion bias cannot be obviated in the categorization of CKDstage and would bias any association between CKD andmortality toward the null. Additionally, the timing of theassessment of serum creatinine must also be considered. Eventhough all patients had a serum creatinine measurement onadmission, those with elevated concentrations at that timepoint may reflect either the presence of preexisting CKD orthe occurrence of incident AKI. To minimize the misclassi-fication of these 2 different clinical scenarios, the earliestserum creatinine of either preadmission or admission wasused as baseline. However, this does not obviate the impact oftiming of changes in renal function on misclassification.Because both the Acute Kidney Injury Network and RIFLEcriteria provide time frames for the changes in creatinine (48hours and 7 days, respectively), our inability to fully definewhat changes occurred within those time frames likelyintroduced additional bias. This is compounded by the factthat a significant proportion of patients likely had CKD atbaseline, and the time to comparable relative changes increatinine among those with CKD is longer.18 Finally, interms of hospitalization, rehospitalizations at medical centersother than the participating sites would not be captured in thisstudy and could potentially bias the strength of the associa-tion between AKI and rehospitalization demonstrated heretoward the null.
ConclusionsThis study demonstrates that an alteration in kidney functionis associated with a greater risk of important outcomes,including mortality, additional end-organ injury, and in-creased length of stay, among patients admitted with acutesevere hypertension. Thus, renal dysfunction should promptcareful monitoring of this population, and effective treatmentmay be especially important. Specifically, this higher-riskpopulation who loses even small amounts of kidney functionafter admission is at greater risk of experiencing events suchas acute left ventricular failure and cardiac arrest. However,in terms of designing directed surveillance techniques toaddress the risk associated with these events, other than
Figure 2. Mortality risk at 90 days based on the presence ofCKD at baseline and AKI during hospitalization.
Figure 1. Mortality risk before discharge and at 90 days for sub-jects based on degree of AKI.
Szczech et al AKI in Acute Hypertension 2189
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

serum creatinine on admission, there are few clues availableto the clinician to identify the patients at higher risk for AKIand adverse events. Until the kidney equivalent of the cardiactroponin is available to predict on presentation the occurrenceof AKI, heightened awareness of AKI is required. Along withincreased surveillance of serum creatinine, knowledge of thesensitivity of creatinine at lower ranges of measurement tochanges in kidney function is needed to identify patients athighest risk for these poorer outcomes.
AppendixSTAT Steering Committee Members andPrincipal InvestigatorsSteering Committee: Alpesh Amin, Joseph F. Dasta, James Fergu-son, Joel Gore, Christopher B. Granger, Kurt Kleinschmidt, StephanA. Mayer, Alan S. Multz, W. Frank Peacock, Eric Peterson, CharlesPollack, Andrew F. Shorr, Gene Yong Sung, Joseph Varon, MatthewWeir.
Principal investigators: John Cienki, MD, Jackson MemorialHospital, Miami, Fla; Lala Dunbar, MD, Louisiana State UniversityHealth Sciences Center/University Hospital, New Orleans, La; JohnDevlin, PharmD, Tufts–New England Medical Center, Boston,Mass; Deborah Diercks, MD, University of California MedicalCenter Davis; Icilma Fergus, MD, Harlem Hospital Center, NewYork, NY; James Froehlich, MD, University of Michigan HealthSystem, Ann Arbor; Tony Gerlach, PharmD, Ohio State UniversityMedical Center, Columbus, Ohio; Marc LaPointe, MD, MedicalUniversity of South Carolina, Charleston; Phillip Levy, MD, DetroitReceiving Hospital and Sinai Grace Hospital, Detroit, Mich; Chad-wick Miller, MD, Wake Forest University Baptist Medical Center,Winston-Salem, NC; Richard Nowak, MD, Henry Ford Health System,Detroit, Mich; Brian O’Neil, MD, William Beaumont Hospital, RoyalOak, Mich; Noleen Ostapkovich, RN, Columbia University MedicalCenter, New York, NY; Namrata Patil, MD, Brigham and Women’sHospital, Boston, Mass; Jon Schrock, MD, MetroHealth MedicalCenter, Cleveland, Ohio; Adam Singer, MD, Stony Brook, StonyBrook, NY; Brian Tiffnay, MD, Chandler Regional Medical Center,Chandler, Ariz; Joseph Varon, MD, FACP, FCCP, FCCM, St Luke’sEpiscopal Hospital, Houston, Tex.
AcknowledgmentsWe thank the physicians and study coordinators participating inSTAT and the staff at the Center for Outcomes Research (Worcester,Mass). The data analysis was conducted by statisticians at the Centerfor Outcomes Research, University of Massachusetts MedicalSchool. Editorial support for the final version of this article,comprising language editing, content checking, formatting, andreferencing, was provided by Sophie Rushton-Smith, PhD (Centerfor Outcomes Research). STAT is overseen by a medical advisoryboard of clinicians. Further information about the registry can befound at http://www.outcomes.org/stat.
Source of FundingSTAT was supported by a research grant from The Medicines Co.The sponsors had no involvement in the collection, analysis, andinterpretation of data; in the writing of the report; or in the decisionto submit the paper for publication.
DisclosuresDr Szczech reports receiving consulting fees from Ortho BiotechClinical Affairs, Nabi Pharmaceuticals, Gilead, Fresenius MedicalCare, Kureha, Affymax, and Acologix; lecture fees from NabiBiopharmaceuticals, Fresenius Medical Care, GlaxoSmithKline,Gilead, Genzyme, Abbott, Amgen, and Ortho Biotech; and grantsupport from GlaxoSmithKline, Pfizer, and Genzyme. Dr Grangerhas received research grant support and honoraria from and is aconsultant/advisory board member for The Medicines Co. Dr Dastais on the speakers’ bureau for Hospira and is a consultant or advisoryboard member for The Medicines Co, VISICU, Keimar, and AbbottPoint of Care. Dr Peacock has received research grant support fromAbbott, BAS, Biosite, Brahms, CHF Solutions, Heartscape, Inovise,Inverness, PDL, and The Medicines Co; is a scientific advisory boardmember for Abbott, Beckman-Coulter, Biosite, Inovise, Inverness,Otsuka, Ortho Clinical Diagnostics, and The Medicines Co; is on thespeakers’ bureau for Abbott, Biosite, Otsuka, Ortho Clinical Diag-nostics, PDL, and Scios; and has ownership interest in Vital Sensors.Dr Devlin has received research grant support and honoraria fromand is a consultant/advisory board member for The Medicines Co. DrWeir is on the advisory board for Novartis, MSD, Wyeth, Daichi-Sankyo, and Boehringer-Ingelheim and is on the speakers’ bureaufor Novartis, Daichi-Sankyo, and Boehringer-Ingelheim. Dr Katzhas received an honorarium from The Medicines Co. Dr Andersonhas received research grants from The Medicines Co. Dr Varon hasreceived research grant support from The Medicines Co, is on thespeakers’ bureau for PDL Biopharma and The Medicines Co, and isa consultant/advisory board member for The Medicines Co. Theother authors report no conflicts.
References1. Collins AJ, Li S, Gilbertson DT, Liu J, Chen SC, Herzog CA. Chronic
kidney disease and cardiovascular disease in the Medicare population.Kidney Int Suppl. 2003:S24–S31.
2. U.S. Renal Data System UADR. Atlas of Chronic Kidney Disease andEnd-Stage Renal Disease in the United States, National Institutes ofHealth, National Institute of Diabetes and Digestive and KidneyDiseases. Bethesda, Md: National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases; 2008.
3. Dasta JF, Kane-Gill SK. Economics of acute kidney failure. In: Jorres A,Ronco C, Kellum JA, eds. Management of Acute Kidney Problems. NewYork, NY: Springer Publications; 2009.
4. Sarnak MJ, Levey AS. Epidemiology of Cardiac Disease in DialysisPatients. Seminars in Dialysis. 2002;12(2):69–76.
5. Reddan DN, Szczech LA, Tuttle RH, Shaw LK, Jones RH, Schwab SJ,Smith MS, Califf RM, Mark DB, Owen WF Jr. Chronic kidney disease,
Variable
Age
Male gender (vs female)
OR (95% CI) P value
1.05 (1.03, 1.06) <0.0001
1 52 (1 07 2 16) 0 02
Variable
Age
Race
Asian/other vs Black
White vs Black
Diabetes mellitus (vs no)
1.52 (1.07, 2.16) 0.02
0.0033
1.48 (0.80, 2.76) –
1.91 (1.31, 2.77) –
0.78 (0.53, 1.13) 0.19
Race
( )
Baseline eGFR*
Greatest decline in eGFR (baseline to nadir), per 10 ml/min/1.73 m2
( )
0.99 (0.99, 0.997) 0.002
1.05 (1.01, 1.09) 0.03
20 0.4 0.8 1.2 1.6 2.0 2.4 2.8 3.2
Lower risk of death Higher risk of death
Figure 3. Logistic regres-sion predicting death within90 days. OR indicates oddsratio.
2190 Circulation May 25, 2010
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

mortality, and treatment strategies among patients with clinically sig-nificant coronary artery disease. J Am Soc Nephrol. 2003;14:2373–2380.
6. Szczech LA, Reddan DN, Owen WF, Califf R, Racz M, Jones RH,Hannan EL. Differential survival after coronary revascularization pro-cedures among patients with renal insufficiency. Kidney Int. 2001;60:292–299.
7. Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J. Inde-pendent association between acute renal failure and mortality followingcardiac surgery. Am J Med. 1998;104:343–348.
8. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S,Kusek JW, Van Lente F. Using standardized serum creatinine values inthe modification of diet in renal disease study equation for estimatingglomerular filtration rate. Ann Intern Med. 2006;145:247–254.
9. The National Kidney Foundation Kidney Disease Outcomes Quality Ini-tiative (NKF KDOQI). New York, NY: National Kidney Foundation,2000.
10. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renalfailure: definition, outcome measures, animal models, fluid therapy andinformation technology needs: the Second International Consensus Con-ference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care.2004;8:R204–R212.
11. Lip GY, Beevers M, Beevers DG. Complications and survival of 315patients with malignant-phase hypertension. J Hypertens. 1995;13:915–924.
12. Lip GY, Beevers M, Beevers G. The failure of malignant hypertension todecline: a survey of 24 years’ experience in a multiracial population inEngland. J Hypertens. 1994;12:1297–1305.
13. Gottlieb SS, Abraham W, Butler J, Forman DE, Loh E, Massie BM,O’Connor CM, Rich MW, Stevenson LW, Young J, Krumholz HM. Theprognostic importance of different definitions of worsening renal functionin congestive heart failure. J Card Fail. 2002;8:136–141.
14. Smith GL, Vaccarino V, Kosiborod M, Lichtman JH, Cheng S, WatnickSG, Krumholz HM. Worsening renal function: what is a clinically mean-ingful change in creatinine during hospitalization with heart failure?J Card Fail. 2003;9:13–25.
15. Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W,Bauer P, Hiesmayr M. Minimal changes of serum creatinine predictprognosis in patients after cardiothoracic surgery: a prospective cohortstudy. J Am Soc Nephrol. 2004;15:1597–1605.
16. Loef BG, Epema AH, Smilde TD, Henning RH, Ebels T, Navis G,Stegeman CA. Immediate postoperative renal function deterioration incardiac surgical patients predicts in-hospital mortality and long-termsurvival. J Am Soc Nephrol. 2005;16:195–200.
17. Endre ZH. Acute kidney injury: definitions and new paradigms. AdvChronic Kidney Dis. 2008;15:213–221.
18. Waikar SS, Bonventre JV. Creatinine kinetics and the definition of acutekidney injury. J Am Soc Nephrol. 2009;20:672–679.
CLINICAL PERSPECTIVELittle is known about the association between kidney dysfunction and outcome in acute severe hypertension. Using datafrom the Studying the Treatment of Acute Hypertension (STAT) registry, this study examined the associations betweenboth acute kidney injury and chronic kidney disease among patients with acute severe hypertension. On admission, 79%of the cohort had at least mild chronic kidney disease and were subject to a greater risk of heart failure, non–ST-elevationmyocardial infarction, and acute kidney injury. Not surprisingly, acute kidney injury patients were also at greater risk ofheart failure, cardiac arrest, and mortality at 90 days. However, quite notable is the fact that any acute loss of estimatedglomerular filtration rate during hospitalization was independently associated with an increased risk of death (odds ratio,1.05; P�0.03 per 10-mL/min decline). This study strongly supports the clinical need for early and frequent monitoring ofkidney function to facilitate risk stratification among those admitted with acute severe hypertension. It also stronglysupports research on whether treatment aimed at preventing or mitigating the severity of the acute kidney injury will lowerthe risk. The clinician should therefore be aware that patients with even a subtle decline in kidney function after admissionare at higher risk for other cardiovascular events and tailor their therapy on a case-by-case basis.
Go to http://cme.ahajournals.org to take the CME quiz for this article.
Szczech et al AKI in Acute Hypertension 2191
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

for the Studying the Treatment of Acute Hypertension InvestigatorsAnderson, Jr, Allison Wyman and Joseph Varon
Peter A. McCullough, John W. Devlin, Matthew R. Weir, Jason N. Katz, Frederick A. Lynda A. Szczech, Christopher B. Granger, Joseph F. Dasta, Alpesh Amin, W. Frank Peacock,
Acute Kidney Injury and Cardiovascular Outcomes in Acute Severe Hypertension
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2010 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.109.896597
2010;121:2183-2191; originally published online May 10, 2010;Circulation.
http://circ.ahajournals.org/content/121/20/2183World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2013/10/17/CIRCULATIONAHA.109.896597.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 28, 2018
http://circ.ahajournals.org/D
ownloaded from

12:25:09:03:11
Page 77
Page 77
Hypertension artérielle
Lien entre l’insuffisance rénale aiguë et lesévénements cardiovasculaires dans
l’hypertension artérielle aiguë sévère
Lynda A. Szczech, MD, MSCE ; Christopher B. Granger, MD ; Joseph F. Dasta, MSc, FCCM ;Alpesh Amin, MD ; W. Frank Peacock, MD ; Peter A. McCullough, MD, MPH ;
John W. Devlin, PharmD ; Matthew R. Weir, MD, MS ; Jason N. Katz, MD ;Frederick A. Anderson, Jr, PhD ; Allison Wyman, MS ; Joseph Varon, MD ;
pour les investigateurs du registre Studying the Treatment of Acute Hypertension
Contexte—Nous ne possédons que peu de données sur l’influence pronostique exercée par l’insuffisance rénale dansl’hypertension artérielle aiguë sévère. Cette étude a donc été menée pour évaluer la relation entre la préexistence d’unenéphropathie chronique (établie sur la base de la filtration glomérulaire estimée), l’insuffisance rénale aiguë (IRA,diminution de la filtration glomérulaire estimée égale ou supérieure à 25 % par rapport à sa valeur initiale) et lesévénements cliniques chez les patients hospitalisés pour un épisode d’hypertension artérielle aiguë sévère.
Méthodes et résultats—Le registre STAT (Studying the Treatment of Acute Hypertension [étude sur le traitement del’hypertension artérielle aiguë]) a recensé les patients ayant présenté une poussée hypertensive aiguë sévère (définie par laconstatation d’une pression artérielle systolique supérieure à 180 mmHg et/ou d’une diastolique excédant 110 mmHglors d’au moins une mesure) et qui avaient reçu un traitement antihypertenseur intraveineux. Des comparaisons ontété effectuées entre les données recueillies dans les différents groupes constitués sur la base des valeurs de filtrationglomérulaire estimée mesurées à l’admission et sur la survenue d’une IRA pendant l’hospitalisation. A l’admission, 79 %des patients de la cohorte (n = 1 566) présentaient au minimum une insuffisance rénale chronique légère (filtrationglomérulaire estimée inférieure à 60 ml/min chez 46 % des sujets et à 30 ml/min chez 22 %). Les patients atteints d’uneinsuffisance rénale chronique ont été davantage susceptibles de développer une insuffisance cardiaque (p <0,0001), uninfarctus du myocarde sans sus-décalage de ST (p = 0,003) et une IRA (p <0,007). Les patients ayant présenté une IRAont été exposés à un risque plus important d’insuffisance cardiaque et d’arrêt cardiaque (p ≤0,0001 dans les deux cas). Ilsont également connu une mortalité plus élevée à 90 jours (p = 0,003). Quel qu’ait été son degré, la diminution aiguë de lafiltration glomérulaire estimée au cours de l’hospitalisation a été un facteur indépendant d’augmentation du risque dedécès (odds ratio : 1,05 ; p = 0,03 par tranche de diminution de 10 ml/min). Les autres facteurs indépendants prédictifs dudécès ont été l’avancement en âge (p <0,0001), le sexe masculin (p = 0,016), le fait d’être blanc plutôt que noir (p = 0,003)et le degré d’insuffisance rénale à l’entrée dans l’étude (p = 0,003).
Conclusion—L’insuffisance rénale chronique est une comorbidité couramment présente chez les patients hospitaliséspour un épisode d’hypertension artérielle aiguë sévère, l’IRA étant, par ailleurs, une forme fréquente de dysfonctionaiguë des organes cibles, notamment chez les sujets qui étaient déjà atteints d’une néphropathie chronique. Quelque soit son degré, la survenue d’une IRA contribue à augmenter le risque de morbidité et de mortalité. (Traduitde l’anglais : Acute Kidney Injury and Cardiovascular Outcomes in Acute Severe Hypertension. Circulation. 2010;121:2183–2191.)
Mots clés : épidémiologie � hypertension artérielle � rein � mortalité
Reçu le 24 juillet 2009 ; accepté le 23 mars 2010.Service de Médecine, Unité de Néphrologie, Centre Médical de l’Université Duke, Durham, Caroline du Nord, Etats-Unis (L.A.S.) ; Institut Duke de
Recherche Clinique, Durham, Caroline du Nord, Etats-Unis (C.B.G.) ; Faculté de Pharmacie, Université du Texas, Round Rock (J.F.D.) ; UCIMC, Orange,Californie, Etats-Unis (A.A.) ; Service des Urgences, Cleveland Clinic, Cleveland, Ohio, Etats-Unis (W.F.P.) ; William Beaumont Hospital, Royal Oak,Michigan, Etats-Unis (P.A.M.) ; Faculté de Pharmacie de la Northeastern University, Boston, Massachusetts, Etats-Unis (J.W.D.) ; Service de Néphrologie,Faculté de Médecine de l’Université du Maryland, Baltimore, Etats-Unis (M.R.W.) ; Services de Cardiologie, de Pneumologie et de Soins Intensifs,Université de Caroline du Nord à Chapel Hill, Etats-Unis (J.N.K.) ; Centre de Recherche en matière de résultats, Faculté de Médecine de l’Université duMassachusetts, Worcester, Etats-Unis (F.A.A., A.W.) ; et Centre des Sciences de la Santé de l’Université du Texas et St Luke’s Episcopal Hospital, Houston,Etats-Unis (J.V.).
Correspondance : Lynda Anne Szczech, MD, MSCE, Duke University Medical Center, Box 3646, Durham, NC 27710, Etats-Unis.E-mail : szcze001@ mc.duke.edu
© 2011 Lippincott, Williams & Wilkins
Circulation est disponible sur http://circ.ahajournals.org
77

12:25:09:03:11
Page 78
Page 78
Aussi bien l’insuffisance rénale chronique (IRC) quel’insuffisance rénale aiguë (IRA) contribuent à accroître
le risque de décès.1–3 Les risques liés à l’altération de lafonction rénale trouvent pleinement leur illustration dansl’évolution péjorative des patients en phase d’insuffisancerénale terminale (IRT).4 Grâce à une meilleure connaissancedes méthodes sur lesquelles s’appuyer pour classer etcomparer ces deux affections dans les études, nous avonsaujourd’hui davantage conscience que le risque associé à unecréatininémie anormale ou à l’élévation de ce paramètre semanifeste précocement et augmente de façon proportionnelleà la dégradation de la fonction rénale.5–7
De multiples études ont confirmé l’impact que l’hyper-tension artérielle chronique a sur la fonction rénale, cetteaffection étant la cause directe de l’IRT chez de nombreuxpatients relevant de l’hémodialyse.2 En revanche, on connaîtmoins bien l’influence exercée par l’hypertension artérielleaiguë sévère sur la fonction rénale. Or, si nous savionscomment les patients atteints d’un tel trouble évoluentselon qu’ils présentent une IRC ou une IRA, cela nouspermettrait d’identifier des groupes à haut risque méritant unesurveillance clinique accrue.
La présente analyse a été effectuée à partir des donnéesdu registre STAT (Studying the Treatment of Acute Hyper-tension [étude sur le traitement de l’hypertension artérielleaiguë]), qui a recensé les patients hospitalisés pour unepoussée hypertensive aiguë sévère. L’étude a été entreprise envue d’évaluer le risque encouru par les patients atteintsd’un tel trouble et ayant présenté une IRA ainsi que lescontributions respectives de l’IRA et de l’IRC aux risquesd’événement cardiovasculaire et de décès.
MéthodesSTAT est une étude observationnelle rétrospective menée en milieuhospitalier aux Etats-Unis pour évaluer les modalités courantesde prise en charge et le devenir clinique des patients admis dans unservice d’urgences ou de soins intensifs (deux structures où il estpossible d’administrer des antihypertenseurs par voie intraveineuseet de surveiller la pression artérielle [PA] par l’intermédiaire d’unevoie artérielle) pour un épisode hypertensif aigu sévère et ayant reçuun traitement antihypertenseur intraveineux. L’étude a porté surles adultes consécutifs qui, à leur admission, présentaient une PAsystolique supérieure à 180 mmHg et/ou une diastolique supérieureà 110 mmHg lors d’au moins une mesure, ou dont les chiffrestensionnels excédaient 140/90 mmHg s’ils avaient été victimes d’unehémorragie méningée, et qui avaient reçu au moins deux bolusantihypertenseurs ou avaient été placés sous perfusion continue dansles 24 heures ayant suivi leur hospitalisation dans l’un des 25 centresparticipants. Les antihypertenseurs administrés ont été le diltiazem,l’énalapril, l’esmolol, le fenoldopam, l’hydralazine, le labétalol, lemétoprolol, la nicardipine, la trinitrine, la phentolamine, le nitro-prussiate sodique et le vérapamil. Les critères d’exclusion étaientreprésentés par l’instauration du traitement antihypertenseur dans uncontexte périopératoire ou pendant le péripartum, son administrationplus de 24 heures après l’admission, le non-recours à la voie intra-veineuse pour administrer les antihypertenseurs et l’instauration dutraitement chez les patients en soins palliatifs.
Des collaborateurs rompus à la rédaction des résumés cliniques ontcolligé les informations relatives aux caractéristiques démographiquesdes patients, à leurs antécédents médicaux, au bilan pratiqué àl’admission, à la prise en charge hospitalière, aux événementscliniques survenus dans les 90 jours (réhospitalisation, décès, nouvellepoussée hypertensive sévère) ainsi que les décès intervenus au cours
des 6 mois ayant suivi l’hospitalisation initiale. Pour établir si lespatients étaient encore en vie 6 mois après avoir été hospitalisés pourun épisode d’hypertension artérielle aiguë, nous avons consulté leSocial Security Death Index (registre des décès du système américainde protection sociale).
L’étude a été menée dans le respect du Health Insurance Portabilityand Accountability Act de 1996 (équivalent de la loi Informatiqueet Libertés) et a été approuvée par les comités d’éthique de tousles établissements participants, dont elle a pleinement respecté lesrèglements.
Définitions des variablesLes valeurs de créatininémie ont été recueillies à quatre temps : dansles 12 mois ayant précédé l’hospitalisation (si la mesure avait étéeffectuée), à l’admission, lors du pic de créatininémie et à la sortied’hôpital si le taux avait été mesuré et était disponible. Le débit defiltration glomérulaire estimée (DFGe) a été calculée pour chaquevaleur de créatininémie disponible en appliquant la formule de l’étudeModification of Diet in Renal Disease (Modification du régimealimentaire dans l’insuffisance rénale, MDRD).8 Pour chaque patient,la fonction rénale à l’entrée dans l’étude a été définie conformémentaux recommandations de pratique clinique édictées par la NationalKidney Foundation Disease Outcomes Quality Initiative (comitéd’évaluation de la qualité des résultats cliniques de la FondationNationale de Néphrologie des Etats-Unis)9 : DFGe supérieur à90 ml/min (fonction rénale normale), compris entre 60 et 89 ml/min(insuffisance rénale légère), compris entre 30 et 59 ml/min(insuffisance rénale modérée), inférieur à 30 ml/min (insuffisancerénale sévère) ou recours nécessaire à l’hémodialyse. Le groupe depatients dont le DFGe excédait 90 ml/min comprenait aussi bien desindividus considérés comme insuffisants rénaux présentant uneprotéinurie que des sujets jugés normaux sans protéinurie ; aucunetentative n’a été faite pour subdiviser ce groupe de manière à prendreen compte l’influence potentiellement exercée par l’hypertensionartérielle aiguë sévère sur l’apparition d’une protéinurie à l’admission.
Chez chacun des patients, la modification relative du DFG a étécalculée en retranchant la plus faible valeur de DFGe recueilliede celle mesurée au temps le plus précoce (avant ou au moment del’admission) et en divisant le résultat par cette même valeur. Cetteapproche a été utilisée pour limiter au maximum l’impact d’unecréatininémie déjà élevée à l’admission du fait d’une atteinte rénalepréexistante. L’altération de la fonction rénale matérialisée parl’évolution du DFG depuis sa valeur initiale jusqu’à son point le plusbas (et reflétant par là même la sévérité de l’IRA) a été analysée sur unmode continu et en fonction de son grade. Pour ce faire, nous avonsutilisé la classification RIFLE (risk, injury, failure, loss, end-stagerenal disease [risque, lésion, insuffisance, insuffisance complète,IRT])10 qui repose sur le DFG. Lorsque la différence entre le DFGinitial et son point le plus bas était inférieure à 25 %, la fonctionrénale a été considérée comme non altérée. Conformément auxcritères RIFLE,10 le « risque » a été défini par une diminution du DFGcomprise entre 25 et 50 % et la « lésion » par une réduction compriseentre 50 et 75 % ; l’« insuffisance » et les deux derniers grades ont étédéfinis par une diminution excédant 75 % et regroupés en raisondes nombres réduits de patients formant ces groupes et du peud’informations disponibles sur la chronicité de leur atteinte rénale.Les patients qui étaient déjà en IRT à leur entrée dans l’étude n’ontpas été classés selon ces critères, car ils ont fait l’objet d’une analysedistincte.
Analyses statistiques effectuéesLes patients ont été classés tout d’abord par degrés d’IRC en fonctionde la valeur de leur DFGe à l’entrée dans l’étude, puis par gradesd’IRA d’après l’importance de la réduction de ce paramètre. Lesvariables catégorielles sont présentées sous forme de fréquences. Lesvariables continues ont été comparées au moyen d’un test du χ2 etles variables discontinues et ordinales à l’aide d’un test du χ2 deMantel-Haenszel. Les variables continues sont exprimées sous formede médianes assorties des 25ème et 75ème percentiles. Afin de rechercher
78 Circulation Mars 2011

12:25:09:03:11
Page 79
Page 79
Tableau 1. Caractéristiques démographiques et antécédents médicaux des patients à leur admission, en fonction du stade d’IRC
d’éventuelles tendances linéaires parmi les variables continues, chaqueclasse d’IRC a été analysée en prenant pour base la valeur médianede DFGe. Ces valeurs ont ensuite fait l’objet d’une analyse parrégression linéaire univariée pour chacun des événements cliniques ;les valeurs p obtenues sont indiquées dans les tableaux. De la mêmefaçon, pour chaque grade d’IRA, nous avons retenu la valeur médianede DFGe, les valeurs ainsi définies ayant, là encore, fait l’objet d’uneanalyse par régression linéaire. Pour les variables continues quin’étaient pas distribuées de façon normale, nous avons effectué destests de tendance linéaire portant d’abord sur les variables nontransformées, puis sur ces mêmes variables après leur transformationen rangs logarithmiques (ce test non paramétrique visant à éviter queles valeurs extrêmes n’aient une influence anormale). En cas dediscordance entre les résultats, nous rapportons chacun d’eux. Uneanalyse par régression logistique a été réalisée pour estimer le lienexistant entre l’IRA et le risque de décès dans les analyses ajustées.Les variables candidates incluses dans ce modèle ont été l’âge, le sexe,l’origine ethnique, l’appartenance à l’ethnie hispanique, le diabète, leDFGe à l’entrée dans l’étude, l’existence d’une artériopathiepériphérique, la plus forte diminution de DFGe survenue au cours del’IRA, la protéinurie et l’interaction entre le DFGe initial et cettedernière.
Les valeurs p sont toutes bidirectionnelles et les intervalles deconfiance ont été fixés à 95 %. Les analyses ont été effectuées à l’aided’un logiciel SAS (version 9.1, SAS Institute Inc, Cary, Caroline duNord, Etats-Unis).
RésultatsAu total, 1 566 patients ont été inclus dans l’étude STAT entrele 1er janvier 2007 et le 6 avril 2008. Parmi ces sujets, 1 542avaient fait l’objet de mesures de la créatininémie en nombresuffisant pour permettre d’évaluer l’incidence et la sévérité desIRC à l’entrée dans l’étude, alors que, pour 1 369 patients, ondisposait de suffisamment de mesures de ce paramètre pourpouvoir évaluer l’incidence et la sévérité des IRA au cours dela période d’observation.
IRC à l’entrée dans l’étudeLa plupart des patients (79 %) présentaient au minimum uneIRC légère (stade II) à leur admission (Tableau 1), les tauxd’insuffisances rénales légères, modérées et sévères ayant étéde, respectivement, 32, 23 et 11 %. A cela s’ajoutaient 11 %de patients qui relevaient de l’hémodialyse à leur entréedans l’étude. De façon générale, plus l’IRC des patients étaitsévère à leur admission et plus leur PA était élevée ; il existaitégalement un facteur de sévérité de l’IRC plus susceptiblede toucher les sujets noirs ou porteurs de pathologiesconcomitantes telles qu’une affection cardiaque, une hyper-tension artérielle, un diabète ou une artériopathie périphérique(p <0,0001 pour toutes les comparaisons).
Pendant leur hospitalisation, les patients se sont révélésd’autant plus exposés à présenter des complications tellesqu’une dysfonction ventriculaire gauche aiguë (p <0,0001) ouun infarctus du myocarde sans sus-décalage du segmentST (p = 0,003 ; Tableau 2) que leur IRC était plus sévèreà leur admission ; en revanche, ils ont été moins sujetsaux hémorragies intracrâniennes (intracérébrales, p <0,001 ;méningées, p <0,0001). Des patients ont développé une IRAdans chaque classe d’IRC ; toutefois, ceux qui étaientinitialement atteints des formes les plus sévères d’IRC ont étédavantage enclins à présenter les plus fortes altérations aiguësde leur fonction rénale (p = 0,007).
IRA pendant l’hospitalisationLa modification de la fonction rénale a été évaluée chezchaque patient en fonction de la valeur qu’elle avait chez luià l’admission, puis les patients ont été classés par degrésd’altération (Tableau 3). Sur l’ensemble de la cohorte, 64 %
Szczech et al L’insuffisance rénale aiguë dans l’hypertension artérielle aiguë 79
12:25:09:03:11
Page 80
Page 80
Tableau 2. Lésions des organes cibles et événements défavorables survenus pendant les hospitalisations pour hypertensionartérielle aiguë, en fonction du stade d’IRC
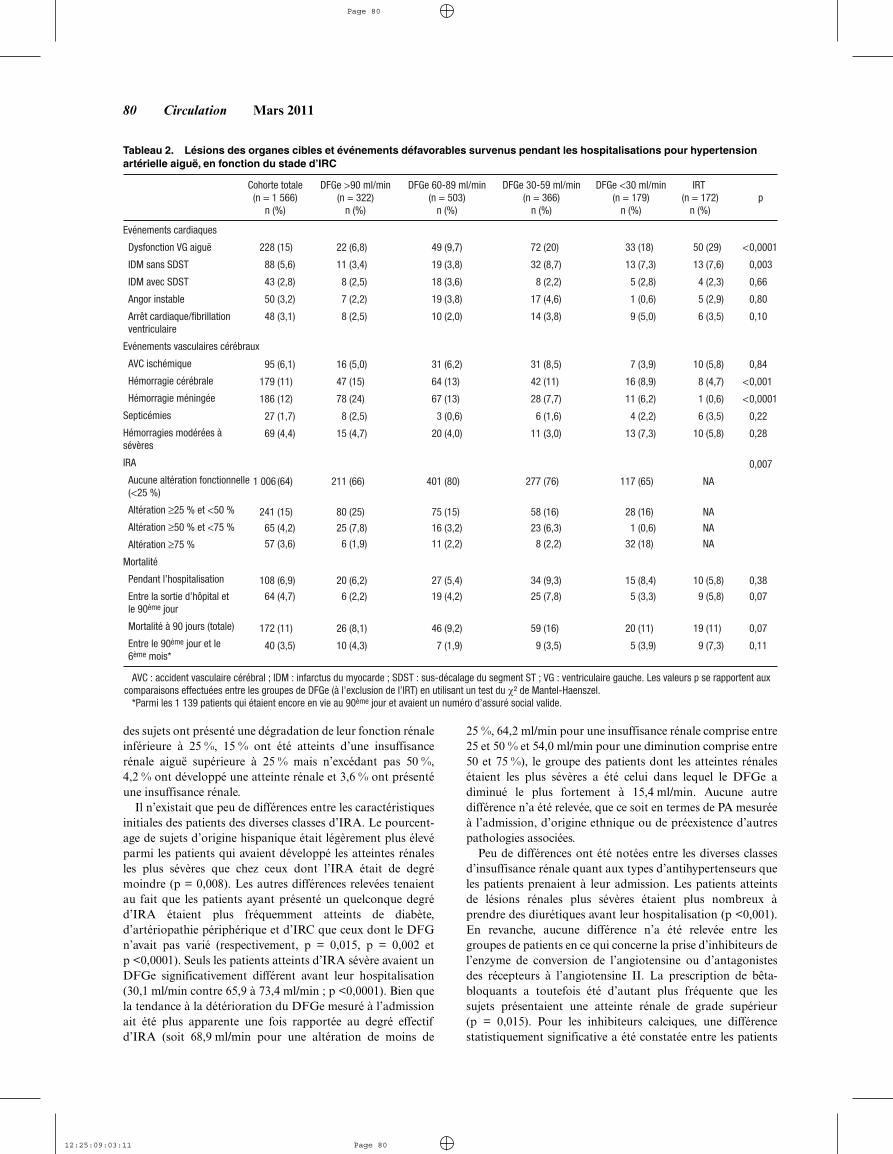
des sujets ont présenté une dégradation de leur fonction rénaleinférieure à 25 %, 15 % ont été atteints d’une insuffisancerénale aiguë supérieure à 25 % mais n’excédant pas 50 %,4,2 % ont développé une atteinte rénale et 3,6 % ont présentéune insuffisance rénale.
Il n’existait que peu de différences entre les caractéristiquesinitiales des patients des diverses classes d’IRA. Le pourcent-age de sujets d’origine hispanique était légèrement plus élevéparmi les patients qui avaient développé les atteintes rénalesles plus sévères que chez ceux dont l’IRA était de degrémoindre (p = 0,008). Les autres différences relevées tenaientau fait que les patients ayant présenté un quelconque degréd’IRA étaient plus fréquemment atteints de diabète,d’artériopathie périphérique et d’IRC que ceux dont le DFGn’avait pas varié (respectivement, p = 0,015, p = 0,002 etp <0,0001). Seuls les patients atteints d’IRA sévère avaient unDFGe significativement différent avant leur hospitalisation(30,1 ml/min contre 65,9 à 73,4 ml/min ; p <0,0001). Bien quela tendance à la détérioration du DFGe mesuré à l’admissionait été plus apparente une fois rapportée au degré effectifd’IRA (soit 68,9 ml/min pour une altération de moins de
25 %, 64,2 ml/min pour une insuffisance rénale comprise entre25 et 50 % et 54,0 ml/min pour une diminution comprise entre50 et 75 %), le groupe des patients dont les atteintes rénalesétaient les plus sévères a été celui dans lequel le DFGe adiminué le plus fortement à 15,4 ml/min. Aucune autredifférence n’a été relevée, que ce soit en termes de PA mesuréeà l’admission, d’origine ethnique ou de préexistence d’autrespathologies associées.
Peu de différences ont été notées entre les diverses classesd’insuffisance rénale quant aux types d’antihypertenseurs queles patients prenaient à leur admission. Les patients atteintsde lésions rénales plus sévères étaient plus nombreux àprendre des diurétiques avant leur hospitalisation (p <0,001).En revanche, aucune différence n’a été relevée entre lesgroupes de patients en ce qui concerne la prise d’inhibiteurs del’enzyme de conversion de l’angiotensine ou d’antagonistesdes récepteurs à l’angiotensine II. La prescription de bêta-bloquants a toutefois été d’autant plus fréquente que lessujets présentaient une atteinte rénale de grade supérieur(p = 0,015). Pour les inhibiteurs calciques, une différencestatistiquement significative a été constatée entre les patients
80 Circulation Mars 2011

12:25:09:03:11
Page 81
Page 81
Tableau 3. Caractéristiques démographiques et médicales initiales en fonction du degré d’IRA
selon la sévérité de leur atteinte rénale (p = 0,019) ; ladifférence n’a toutefois pas paru avoir d’incidence clinique.
En règle générale, le risque de lésion ou de dysfonction desautres organes cibles encouru par les patients a été d’autantplus élevé que leur atteinte rénale était sévère (Tableau 4).
Cela s’est notamment traduit par une augmentation desrisques de dysfonction ventriculaire gauche aiguë et d’arrêtcardiaque (p ≤0,0001 dans les deux cas). Les autres événe-ments pathologiques qui sont survenus plus fréquemmentparmi les patients atteints d’IRA ont été les hémorragies
Szczech et al L’insuffisance rénale aiguë dans l’hypertension artérielle aiguë 81

12:25:09:03:11
Page 82
Page 82
Tableau 4. Lésions des organes cibles, événements défavorables et traitements administrés pendant les hospitalisations pourhypertension artérielle aiguë, en fonction du degré d’IRA
modérées à sévères (p <0,001), les récidives hypertensivesaiguës sévères (p = 0,001) et les altérations neurologiques(p <0,0001).
S’agissant du traitement de l’épisode hypertensif aigu, iln’a pas été relevé de différence entre les groupes de patientsconstitués en fonction du degré de leur atteinte rénale tanten ce qui concerne le délai d’administration d’un anti-hypertenseur intraveineux que le temps ayant été nécessairepour obtenir une diminution de 10 % de la PA systolique(Tableau 4). En revanche, la durée du traitement intraveineuxet le nombre d’antihypertenseurs intraveineux ont été signifi-cativement supérieurs chez les patients dont l’IRA était plussévère (p <0,0001 dans les deux cas). Chez ces derniers, lamortalité intrahospitalière a également été plus élevée et, pourceux qui ont quitté l’hôpital en vie, la durée d’hospitalisationa été plus longue (p <0,0001 pour les deux comparaisons ;Tableau 5). Ces sujets atteints de formes d’IRA plus sévèresont, en outre, encouru un risque accru de réhospitalisationpour insuffisance rénale (p = 0,001) ou pour insuffisancecardiaque (p = 0,034). Enfin, les patients ayant présenté un
quelconque degré d’IRA se sont révélés exposés à un risqueplus important de décès dans les 90 jours (p = 0,003 ; Figure 1).
Les patients chez lesquels aussi bien la sévérité del’insuffisance rénale initiale que celle de l’épisode d’IRAétaient plus marquées ont présenté un risque supérieur dedécès à 90 jours (Figure 2). L’analyse multivariée a, parailleurs, montré que toute réduction aiguë du DFGependant l’hospitalisation avait été un facteur indépendantd’augmentation du risque de décès (odds ratio : 1,05 ;p = 0,026 par tranche de diminution de 10 ml/min ; Figure 3)après ajustement pour tenir compte des facteurs cliniques etdémographiques ayant pu influer sur la sévérité de l’IRA. Lesautres facteurs prédictifs du décès ont été l’avancée en âge(p <0,0001), le sexe masculin (p = 0,016), le fait d’être blancplutôt que noir (p = 0,003) et le degré d’insuffisance rénaleà l’entrée dans l’étude (p = 0,003).
DiscussionDans cette vaste étude multicentrique menée chez des patientshospitalisés pour un épisode hypertensif aigu sévère, la
82 Circulation Mars 2011

12:25:09:03:11
Page 83
Page 83
Tableau 5. Données relatives à l’hospitalisation et aux 90 jours ayant suivi la sortie d’hôpital, en fonction du degré d’IRA
Figure 1. Risques de décès des patients avant la sortie d’hôpital età 90 jours, en fonction de leur degré d’IRA.
Figure 2. Risques de décès à 90 jours liés à la préexistence d’uneIRC à l’entrée dans l’étude et à la survenue d’une IRA pendantl’hospitalisation.
présence d’une IRC ou d’une IRA a contribué à assombrirle pronostic clinique, notamment en allongeant la duréed’hospitalisation. Même après ajustement tenant compte de lapréexistence d’une insuffisance rénale à l’entrée dans l’étude,la survenue d’une IRA ou d’une détérioration aiguë de lafonction rénale pendant l’hospitalisation s’est montrée sourced’événements morbides et prédictive du risque de décès. Cetteétude est la première à avoir démontré qu’une dégradationminime de la fonction rénale suffit à majorer le risque et quecelui-ci augmente proportionnellement à la sévérité del’IRA. Bien que le lien mis en évidence avec l’atteinte desautres organes cibles reflète vraisemblablement la sévéritéde l’épisode hypertensif, il est permis de penser que l’aug-mentation de la mortalité associée à l’IRA répond à unprocessus plus mécaniste. Elément méritant d’être souligné,parce que la fonction rénale était plus sévèrement altérée àl’admission, les complications à type d’IRA survenues aucours de l’hospitalisation ont été à la fois plus fréquenteset plus sévères. Enfin, si l’on excepte la créatininémieinitialement augmentée, les patients qui ont développé uneIRA sévère ne présentaient que peu de caractéristiquescliniques permettant de les distinguer des sujets dont lafonction rénale était demeurée inchangée ou s’était moinsfortement dégradée.
Bien que le lien unissant l’IRC à l’évolution clinique lorsd’un épisode d’hypertension artérielle systolique aiguë n’aitpas été entièrement défini, ces résultats sont en accord avecceux de précédentes études. Lip et al11 ont démontré que lasurvie est amoindrie chez les patients ayant présenté unepoussée hypertensive et dont l’azotémie et la créatininémieexcèdent respectivement 10 mmol/l et 200 µmol/l. Bien que cesdonnées soient compatibles avec celles présentées ici, ce travailne permet pas de dissocier le risque lié à la préexistence d’uneIRC de celui découlant de l’IRA accompagnant l’épisodehypertensif. Lip et al12 ont précisé le profil de cette populationde patients hospitalisés pour une hypertension artérielle aiguësévère en montrant que la prévalence de l’« insuffisance rénalechronique » à l’admission atteignait 31,7 %. Dans leur étude,
Szczech et al L’insuffisance rénale aiguë dans l’hypertension artérielle aiguë 83

12:25:09:03:11
Page 84
Page 84
Figure 3. Estimation durisque de décès dans les 90jours selon la méthode parrégression logistique.OR : odds ratio.
l’insuffisance rénale chronique a été définie sur la based’une créatinine supérieure à 2,3 mg/dl. Cette seconde étudeprésentait toutefois le même défaut, car elle n’a pas permisd’établir si l’élévation de la créatininémie avait découléde l’IRC préexistante ou de l’IRA. Dans la présente analyse,près de 80 % des patients avaient un DFGe qui se situait dansdes limites compatibles avec la préexistence d’une IRC. Deplus, chez environ 34 % des patients, il a été observé unedégradation significative de la fonction rénale qui traduisaitau minimum la survenue d’une IRA légère.
De nombreuses études antérieures ont mis en évidenceune augmentation du risque de décès parmi de multiplescatégories de patients hospitalisés ayant présenté une IRA.Plus récemment, il a été établi qu’une altération même minimede la fonction rénale constitue un facteur de mortalité.13–16 Detous les travaux menés chez des patients ayant présenté unépisode hypertensif aigu sévère, cette étude est la premièreà montrer que ce risque commence à augmenter lors dediminutions du DFG encore plus modestes, c’est-à-diren’excédant pas 25 à 50 % de sa valeur initiale. Il y a lieude noter qu’il n’existait que peu de différences entre lesparamètres cliniques relevés à l’admission dans les diversgroupes de patients formés en fonction de la sévérité de l’IRAultérieure. Cela souligne combien il est important de surveillerétroitement la fonction rénale au cours de l’hospitalisationafin d’identifier les patients à haut risque. De plus, outre lerisque de décès, l’augmentation a également concerné lesrisques de survenue d’autres événements cliniques majeurs telsqu’une insuffisance cardiaque aiguë, un arrêt cardiaque ou unépisode hémorragique.
Notre étude a deux implications cliniques importantes. Lapremière est que, chez les patients admis en urgence pour unecrise hypertensive, il semble initialement exister une massecritique de néphrons fonctionnels. La démonstration en estpartiellement apportée par le fait que, dans un premiertemps, le DFGe compense l’atteinte et l’insuffisance rénales demanière à maintenir la créatininémie à un niveau relativementstable. Chez les individus dont le DFGe est d’emblée diminué,témoignant de la réduction du nombre d’unités néphroniquesencore fonctionnelles, ce phénomène de filtration compensa-toire est vraisemblablement aboli lors d’un épisode d’hyper-tension artérielle aiguë, cela donnant lieu à une IRA quis’exprime par l’élévation de la créatininémie et la diminutiondu DFGe. La seconde implication est que les marqueurs dela filtration rénale tels que la créatininémie ne rendent quegrossièrement compte de l’IRA en tant que processuspathologique. Notre étude montre qu’il est nécessaire de
disposer de nouveaux marqueurs de l’IRA permettant derapidement reconnaître la nature vasculaire, glomérulaireou tubulaire d’une lésion rénale avant même que celle-ci ne setraduise par une augmentation du taux de protéines extraitesdu sang.17 Il est permis d’espérer que la découverte de telsmarqueurs débouchera sur la survenue de stratégies thérapeu-tiques innovantes qui ne se limiteront plus à abaisser la PA,mais amélioreront également le pronostic rénal et cardiaque.
Limites de l’étudeLe registre de STAT, qui est la plus vaste étude observation-nelle de cohorte menée à ce jour, fournit des données sur unepopulation hétérogène d’individus ayant présenté une pousséehypertensive aiguë sévère. STAT est toutefois grevée decertaines limites propres à ce type d’étude ainsi que de biaispotentiels, tenant notamment au recueil de données nonrandomisées et aux informations manquantes ou incomplètes.Les centres participants ne sont pas nécessairementreprésentatifs de tous les hôpitaux des Etats-Unis, toutcomme les patients atteints d’hypertension artérielle aiguëdiffèrent probablement selon les régions géographiques.L’étude pourrait présenter un biais de sélection dans lamesure où les critères d’inclusion imposaient au médecin demettre en œuvre un traitement antihypertenseur intraveineux.Nous ne disposions pas d’informations complètes sur le suivi,de sorte que nous avons pu sous-estimer dans quelle propor-tion il avait été effectué. Le recrutement des patients dansplusieurs centres a, bien sûr, augmenté la puissance de l’étudeet la capacité de généralisation des résultats comparativementà une étude monocentrique, mais il a également rendu lacomparaison des valeurs de créatininémie plus difficile étantdonné que celles-ci ont été mesurées dans des laboratoiresdifférents. Bien que le biais résultant ait été minimisé enrapportant les modifications de la fonction rénale à son niveauinitial chez chaque individu, il n’était pas possible d’abolirl’effet de ce biais de classification lors de la qualification desdifférents stades d’IRC, de sorte qu’il existait un risque que lelien potentiel entre ce trouble et la mortalité soit faussementdéplacé vers l’hypothèse nulle. Il y a également lieu deconsidérer le moment où les mesures de créatininémie ont étépratiquées. Bien que, chez tous les patients, les dosages aientété effectués dès l’admission, le fait que la valeur ait été alorsaugmentée pouvait aussi bien témoigner de la préexistenced’une IRC que de la survenue d’une IRA. Pour limiterau maximum les erreurs de classification entre ces deuxéventualités cliniques différentes, nous avons retenu commevaleur initiale la toute première mesure de créatininémie
84 Circulation Mars 2011

12:25:09:03:11
Page 85
Page 85
disponible qui avait été effectuée avant ou pendant l’admis-sion. Toutefois, cela n’élimine pas l’influence exercée par lachronologie de survenue de l’altération de la fonction rénalesur le risque d’erreur de classification. Etant donné que tantles critères de l’Acute Kidney Injury Network (réseau d’étudede l’insuffisance rénale aiguë) que ceux de RIFLE définissentdes délais de modification de la créatininémie (respectivementfixés à 48 heures et à 7 jours), notre incapacité à parfaitementétablir quels changements s’étaient produits au cours de cesdélais a vraisemblablement introduit un biais supplémentaire.Cela a été aggravé par le fait qu’un pourcentage non néglige-able de patients était probablement atteint d’IRC à l’entréedans l’étude et que, chez de tels sujets, il s’écoule un tempsplus long avant que n’apparaissent des modifications relativesde la créatininémie de degré comparable.18 Pour terminer,s’agissant des hospitalisations, il ne nous a pas été possible derecenser les réhospitalisations intervenues dans des structuresmédicales autres que les centres participants, ces événementsétant susceptibles d’altérer la puissance de la relation object-ivée entre l’IRA et le risque de réhospitalisation en ladéplaçant vers l’hypothèse zéro.
ConclusionsCette étude démontre que, chez les patients hospitalisés pourun épisode hypertensif aigu sévère, toute altération de lafonction rénale contribue à accroître le risque de survenued’événements cliniques importants tels que le décès, l’atteinted’autres organes cibles et l’allongement de la duréed’hospitalisation. C’est pourquoi, chez ces patients, l’existenced’une insuffisance rénale justifie l’instauration d’unesurveillance étroite, la mise en œuvre d’un traitement efficacepouvant revêtir une importance toute particulière. Plusprécisément, même si elle ne perd qu’une faible partie de safonction rénale après son admission, cette population à hautrisque est davantage exposée à présenter des événements telsqu’une insuffisance ventriculaire gauche aiguë ou un arrêtcardiaque. Toutefois, s’agissant de mettre en œuvre desméthodes de surveillance spécifiquement destinées à gérer lerisque de survenue de tels événements autrement que parla mesure de la créatininémie à l’entrée, les médecins nepossèdent que peu de pistes pour identifier les patientsqui encourent un risque accru d’IRA et d’événementsdéfavorables. En attendant de disposer d’un équivalent rénalde la troponine cardiaque permettant d’anticiper dèsl’admission la survenue d’une IRA, il demeure nécessaired’être fortement sensibilisé à ce risque. Outre une surveillancerenforcée de la créatininémie, il importe d’être au fait de lasensibilité de ce paramètre en termes de modifications dela fonction rénale lorsque les valeurs se situent à de faiblesniveaux, cela afin de pouvoir identifier les patients exposés àun risque maximal de survenue de tels événements péjoratifs.
AnnexeMembres du comité exécutif et principauxinvestigateurs de STATComité exécutif : Alpesh Amin, Joseph F. Dasta, JamesFerguson, Joel Gore, Christopher B. Granger, Kurt Klein-schmidt, Stephan A. Mayer, Alan S. Multz, W. Frank
Peacock, Eric Peterson, Charles Pollack, Andrew F. Shorr,Gene Yong Sung, Joseph Varon, Matthew Weir.
Investigateurs principaux : John Cienki, MD, JacksonMemorial Hospital, Miami, Floride, Etats-Unis ; LalaDunbar, MD, Centre des Sciences de la Santé de l’Universitéd’Etat de Louisiane/Hôpital Universitaire, Nouvelle-Orléans,Louisiane, Etats-Unis ; John Devlin, PharmD, Centre Médi-cal Tufts de Nouvelle-Angleterre, Boston, Massachusetts,Etats-Unis ; Deborah Diercks, MD, Centre Médical Davis del’Université de Californie, Etats-Unis ; Icilma Fergus, MD,Centre Hospitalier de Harlem, New York, Etats-Unis ; JamesFroehlich, MD, Système de Santé de l’Université duMichigan, Ann Arbor, Etats-Unis ; Tony Gerlach, PharmD,Centre Médical de l’Université d’Etat de l’Ohio, Columbus,Ohio, Etats-Unis ; Marc LaPointe, MD, Faculté de Médecinede Caroline du Sud, Charleston, Etats-Unis ; Phillip Levy,MD, Detroit Receiving Hospital et Sinai Grace Hospital,Detroit, Michigan, Etats-Unis ; Chadwick Miller, MD,Centre Médical Baptiste de l’Université de Wake Forest,Winston-Salem, Caroline du Nord, Etats-Unis ; RichardNowak, MD, Système de Santé Henry Ford, Detroit,Michigan, Etats-Unis ; Brian O’Neil, MD, William BeaumontHospital, Royal Oak, Michigan, Etats-Unis ; NoleenOstapkovich, RN, Centre Médical de l’Université deColumbia, New York, Etats-Unis ; Namrata Patil, MD,Brigham and Women’s Hospital, Boston, Massachusetts,Etats-Unis ; Jon Schrock, MD, Centre Médical MetroHealth,Cleveland, Ohio, Etats-Unis ; Adam Singer, MD, StonyBrook, New York, Etats-Unis ; Brian Tiffnay, MD, CentreMédical Régional de Chandler, Chandler, Arizona, Etats-Unis ; Joseph Varon, MD, FACP, FCCP, FCCM, St Luke’sEpiscopal Hospital, Houston, Texas, Etats-Unis.
RemerciementsNous souhaitons remercier les médecins ayant participé à STAT,les coordonnateurs de l’étude ainsi que le personnel du centre derecherches en matière de résultats (Worcester, Massachusetts, Etats-Unis). L’analyse des données a été effectuée par les statisticiens de cecentre, à la Faculté de Médecine de l’Université du Massachusetts.Sophie Rushton-Smith, PhD (du Centre de recherches en matièrede résultats) a apporté son aide rédactionnelle à la version finale decet article, en assurant notamment la correction de la syntaxe, lavérification du contenu, la mise en page et l’élaboration de la biblio-graphie. L’étude STAT a été supervisée par un comité consultatifmédical constitué de cliniciens. Pour de plus amples informations surle registre, se reporter au site : http://www.outcomes.org/stat.
Source de financementSTAT a été financée par une bourse de recherche émanant de TheMedicines Co. Les promoteurs de l’étude n’ont pris aucune part dansle recueil des données, leur analyse et leur interprétation ; ils nesont pas non plus intervenus dans la rédaction du rapport ni dansla décision de soumettre l’article à publication.
DéclarationsLe Dr Szczech déclare être rémunéré en qualité de consultant par ledépartement des affaires médicales d’Ortho Biotech ainsi que parNabi Pharmaceuticals, Gilead, Fresenius Medical Care, Kureha,Affymax et Acologix ; il est également rémunéré en qualité deconférencier par Nabi Biopharmaceuticals, Fresenius Medical Care,GlaxoSmithKline, Gilead, Genzyme, Abbott, Amgen et OrthoBiotech et bénéficie de dotations émanant de GlaxoSmithKline, Pfizer
Szczech et al L’insuffisance rénale aiguë dans l’hypertension artérielle aiguë 85

12:25:09:03:11
Page 86
Page 86
et Genzyme. Le Dr Granger a bénéficié d’une bourse de rechercheoctroyée par The Medicines Co qui le rémunère par ailleurs en qualitéde consultant et de membre du comité consultatif. Le Dr Dasta exerceune fonction de conférencier pour le compte de Hospira et estrémunéré en qualité de consultant ou de membre de comitéconsultatif par The Medicines Co, VISICU, Keimar et Abbott Pointof Care. Le Dr Peacock a bénéficié de bourses de recherche émanantd’Abbott, BAS, Biosite, Brahms, CHF Solutions, Heartscape, Inovise,Inverness, PDL et The Medicines Co ; il est également membre descomités consultatifs scientifiques d’Abbott, Beckman-Coulter,Biosite, Inovise, Inverness, Otsuka, Ortho Clinical Diagnostics et TheMedicines Co ; il exerce des fonctions de conférencier pour le compted’Abbott, Biosite, Otsuka, Ortho Clinical Diagnostics, PDL et Scioset possède des parts dans Vital Sensors. Le Dr Devlin a bénéficiéd’une bourse de recherche octroyée par The Medicines Co qui lerémunère par ailleurs en qualité de consultant et de membre ducomité consultatif. Le Dr Weir est membre des comités consultatifs deNovartis, MSD, Wyeth, Daichi-Sankyo et Boehringer-Ingelheim etexerce des fonctions de conférencier pour le compte de Novartis,Daichi-Sankyo et Boehringer-Ingelheim. Le Dr Katz a perçu deshonoraires émanant de The Medicines Co. Le Dr Anderson abénéficié d’une bourse de recherche octroyée par The Medicines Co.Le Dr Varon a bénéficié d’une bourse de recherche émanant de TheMedicines Co, exerce des fonctions de conférencier pour le compte dePDL Biopharma et The Medicines Co et est rémunéré en qualité deconsultant et de membre du comité consultatif de The Medicines Co.Les autres auteurs n’ont aucun conflit d’intérêts à déclarer.
Références1. Collins AJ, Li S, Gilbertson DT, Liu J, Chen SC, Herzog CA. Chronic
kidney disease and cardiovascular disease in the Medicare population.Kidney Int Suppl. 2003:S24–S31.
2. U.S. Renal Data System UADR. Atlas of Chronic Kidney Disease andEnd-Stage Renal Disease in the United States, National Institutes ofHealth, National Institute of Diabetes and Digestive and Kidney Diseases.Bethesda, Md: National Institutes of Health, National Institute ofDiabetes and Digestive and Kidney Diseases; 2008.
3. Dasta JF, Kane-Gill SK. Economics of acute kidney failure. In: JorresA, Ronco C, Kellum JA, eds. Management of Acute Kidney Problems.New York, NY: Springer Publications; 2009.
4. Sarnak MJ, Levey AS. Epidemiology of Cardiac Disease in DialysisPatients. Seminars in Dialysis. 2002;12:69–76.
5. Reddan DN, Szczech LA, Tuttle RH, Shaw LK, Jones RH, SchwabSJ, Smith MS, Califf RM, Mark DB, Owen WF Jr. Chronic kidneydisease, mortality, and treatment strategies among patients with
clinically significant coronary artery disease. J Am Soc Nephrol.2003;14:2373–2380.
6. Szczech LA, Reddan DN, Owen WF, Califf R, Racz M, Jones RH,Hannan EL. Differential survival after coronary revascularizationprocedures among patients with renal insufficiency. Kidney Int. 2001;60:292–299.
7. Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J.Independent association between acute renal failure and mortalityfollowing cardiac surgery. Am J Med. 1998;104:343–348.
8. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S,Kusek JW, Van Lente F. Using standardized serum creatinine values inthe modification of diet in renal disease study equation for estimatingglomerular filtration rate. Ann Intern Med. 2006;145:247–254.
9. The National Kidney Foundation Kidney Disease Outcomes QualityInitiative (NKF KDOQI). New York, NY: National Kidney Foundation,2000.
10. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renalfailure: definition, outcome measures, animal models, fluid therapy andinformation technology needs: the Second International ConsensusConference of the Acute Dialysis Quality Initiative (ADQI) Group.Crit Care. 2004;8:R204–R212.
11. Lip GY, Beevers M, Beevers DG. Complications and survival of315 patients with malignant-phase hypertension. J Hypertens. 1995;13:915–924.
12. Lip GY, Beevers M, Beevers G. The failure of malignant hypertension todecline: a survey of 24 years’ experience in a multiracial populationin England. J Hypertens. 1994;12:1297–1305.
13. Gottlieb SS, Abraham W, Butler J, Forman DE, Loh E, Massie BM,O’Connor CM, Rich MW, Stevenson LW, Young J, Krumholz HM.The prognostic importance of different definitions of worsening renalfunction in congestive heart failure. J Card Fail. 2002;8:136–141.
14. Smith GL, Vaccarino V, Kosiborod M, Lichtman JH, Cheng S, WatnickSG, Krumholz HM. Worsening renal function: what is a clinicallymeaningful change in creatinine during hospitalization with heartfailure? J Card Fail. 2003;9:13–25.
15. Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W,Bauer P, Hiesmayr M. Minimal changes of serum creatinine predictprognosis in patients after cardiothoracic surgery: a prospective cohortstudy. J Am Soc Nephrol. 2004;15:1597–1605.
16. Loef BG, Epema AH, Smilde TD, Henning RH, Ebels T, Navis G,Stegeman CA. Immediate postoperative renal function deterioration incardiac surgical patients predicts in-hospital mortality and long-termsurvival. J Am Soc Nephrol. 2005;16:195–200.
17. Endre ZH. Acute kidney injury: definitions and new paradigms.Adv Chronic Kidney Dis. 2008;15:213–221.
18. Waikar SS, Bonventre JV. Creatinine kinetics and the definition of acutekidney injury. J Am Soc Nephrol. 2009;20:672–679.
PERSPECTIVE CLINIQUENous ne possédons que peu de données sur l’influence pronostique exercée par l’insuffisance rénale dans l’hypertension artérielle aiguë sévère. Dans cetravail, nous nous sommes appuyés sur les données de STAT (Studying the Treatment of Acute Hypertension [étude sur le traitement de l’hypertensionartérielle aiguë]) pour rechercher les liens existant avec l’insuffisance rénale aiguë et la néphropathie chronique chez les patients ayant présenté un épisodehypertensif aigu sévère. A l’admission, 79 % des patients de la cohorte présentaient au minimum une insuffisance rénale chronique légère et encouraient unrisque accru d’insuffisance cardiaque, d’infarctus du myocarde sans sus-décalage du segment ST et d’insuffisance rénale aiguë. Comme on pouvait s’yattendre, les patients ayant développé une telle insuffisance rénale aiguë étaient également exposés à un risque plus élevé d’insuffisance cardiaque, d’arrêtcardiaque et de décès dans les 90 jours. Il est toutefois intéressant de souligner que, quel qu’ait été son degré, la diminution aiguë du débit de filtrationglomérulaire estimée au cours de l’hospitalisation a été un facteur indépendant d’augmentation du risque de décès (odds ratio : 1,05 ; p = 0,03 par tranche dediminution de 10 ml/min). Cette étude démontre l’intérêt d’une surveillance précoce et régulière de la fonction rénale pour apprécier le risque encouru parles patients hospitalisés pour un épisode hypertensif aigu sévère. Elle constitue également une forte incitation à rechercher si l’instauration d’un traitementvisant à prévenir la survenue d’une insuffisance rénale aiguë ou à en atténuer la sévérité est à même de diminuer ce risque. Les médecins doivent donc avoir àl’esprit que, aussi minime que soit l’altération de la fonction rénale pouvant survenir chez un patient au cours de son hospitalisation, celui-ci encourt unrisque accru de survenue d’autres événements cardiovasculaires et qu’il y a donc lieu d’adapter le traitement au cas par cas.
86 Circulation Mars 2011