hypertension: cardiac hypertrophy as a target of antihypertensive therapy
TRANSCRIPT

66 | FEBRUARY 2010 | volUmE 7 www.nature.com/nrcardio
nEws & viEws
HypErTEnsion
Cardiac hypertrophy as a target of antihypertensive therapyAlberto Zanchetti
Two large trials were conducted to evaluate the effects of an angiotensin-converting-enzyme inhibitor, an angiotensin-receptor blocker or a combination of both in high cardiovascular risk patients. a decrease in the prevalence of left ventricular hypertrophy (lvH) was reported, but this did not translate into a prognostic benefit. new-onset lvH was associated with an increase in cardiovascular events.
verdecchia et al.1 present post hoc analyses of data from the large ontarGet2 and transCenD3 trials that were carried out to determine the effects of an angiotensin- converting-enzyme inhibitor (ramipril) and an angiotensin-receptor blocker (telmi-sartan) on a composite of major cardio-vascular events. the analyses by verdecchia et al. focus on left ventricular hypertrophy (lvH) detected by electrocardiography (a combination of voltage and strain cri teria).
there is mounting interest in the value of assessing lvH as an intermediate step in the cardiovascular continuum. a re appraisal of guidelines on the management of hyper tension by the european society of Hypertension task Force4 describes lvH as a powerful indicator of cardiovascular risk. the development of lvH, evaluated by electro cardiography or echocardiography when more sensitive detection is required, places hypertensive patients in the high-risk category where more than 20% of cardio-vascular outcomes are expected in 10 years (Figure 1). antihypertensive therapy, parti-cularly targeting the renin-angiotensin system, leads to the regression of lvH and cardiovascular protection.4
in the two trials presented by verdecchia et al.,1 31,546 patients with a history of cardio vascular disease or with compli-cated dia betes were treated for a median of 56 months with ramipril, telmi sartan or a combination of both in the ontarGet trial,2 and with telmi sartan or placebo in transCenD.3 lvH prevalence was reduced by telmisartan (from 12.7% to 9.8%) in the transCenD trial and left unchanged by placebo (12.8%, odds ratio 0.79, 95% Ci 0.68 to 0.91; P = 0.0017) owing to similar lvH regression in the two groups, but less fre-quent new-onset lvH with tel misartan (37% lower risk). in ontarGet, lvH prevalence decreased to a similar extent (from 12.5% to 10%) on the three treatments.
lvH regression has important prognostic value, as shown by the randomized, con-trolled liFe trial that was conducted in over 9,000 hypertensive patients with electro-cardiographic evidence of lvH.5 a com-parison of the regimens, which were based either on an angiotensin-receptor blocker (losartan) or a β-adrenoceptor antagonist (atenolol), revealed that both of these blood pressure-lowering treatments reduced lvH prevalence, but more so when losartan was used. lvH regression had clear survival ben-efits as less severe lvH was associated with a lower likelihood of cardiovascular events, independent of changes in blood pressure.6
the results presented by verdecchia et al.1
support the findings of the liFe trial; active antihypertensive treatment over several years is indeed accompanied by a regression of baseline lvH in a proportion of patients. the study also shows that despite active treat-ment, new-onset lvH can occur, though to a significantly lower extent than in placebo-treated patients. the findings by verdecchia and colleagues also differ, however, from those of the liFe study in a clinically rele-vant way. in transCenD, the lower prev-alence of lvH during active treatment did not translate into a reduction in outcomes, parti cularly heart failure, which is a compli-cation considered to be heavily dependent on lvH and was reduced in liFe patients with lvH regression.7 only the small number of patients who developed new-onset lvH during treatment had a higher incidence of major cardiovascular events accompanied by a smaller reduction in blood pressure.
similarities and differences between the liFe trial5-7 and the ontarGet2 and transCenD3 trials must be considered. First, there are methodological differences in the evaluation of electrocardiographic lvH. the liFe trial used electrocardiographic criteria as continuous variables,6 whereas verdecchia et al.1 defined lvH according to
binary yes or no criteria. as a consequence, a limitation of the latter study is that even small changes in values close to the arbitrary cut-off for lvH definition could have placed patients into or outside the lvH category.
more importantly, the inclusion cri-teria for the trials were dif ferent. liFe5 enrolled patients with hypertension and electro cardiographic lvH, and excluded individuals with recent cardio vascular events. in contrast, the ontarGet2 and transCenD3 protocols only included high-risk patients who had experienced previous events or had complicated diabe-tes. accordingly, only 16% of liFe patients reported a previous myocardial infarction and 8% reported a previous stroke, whereas nearly all patients included in ontarGet and transCenD had a history of cardio-vascular disease. Furthermore, in the liFe trial,5 preceding antihypertensive therapy was withdrawn and substituted by rando-mized regimens, and concurrent lipid-lowering and antiplatelet agents were only occasionally administered. By comparison, rando mized regimens were assigned in addi-tion to previous anti hypertensive agents in the two high-risk trials,2,3 and lipid-lowering and antiplatelet therapies were given con-currently to a large number of patients (66% and over 80%, respectively).
not surprisingly, therefore, the liFe trial showed that lowering of blood pressure and lvH regression—the two factors con-trolled by the therapies—markedly reduced cardiovascular events.6,7 By contrast, the patients enrolled in the ontarGet and transCenD trials already had advanced cardiovascular disease, which was under the control of pre-existing antihyper tensive therapy and other medications such as statins and aspirin. i have recently argued that in high-risk patients, even aggres-sive therapy cannot reduce cardiovascular events below a relatively high level of resi-dual, irreversible risk.8 the ontarGet and transCenD trials, where randomized study drugs were added on top of multiple background therapies, could show only a limited benefit as patients had already been brought close to the achievable level of risk before the study commenced.8 this could explain why regression of organ damage, such as lvH, is prognostically important in patients who have asymptomatic cardio-vascular disease and are subjected to less intense background therapies, whereas ben-e fits of lvH regression might not be seen in patients who have advanced disease and are already subjected to aggressive background
nrcardio_NV_FEB10.indd 66 11/1/10 16:29:32
© 20 Macmillan Publishers Limited. All rights reserved10
nature reviews | cardiology volume 7 | FeBruarY 2010 | 67
nEws & viEws
treatment. this is consistent with another finding from the ontarGet trial, where combination treatment had a greater effect on proteinuria than monotherapies, but the differences in proteinuria, like those in lvH, did not translate into different rates of cardio vascular events.9 By contrast, more effective correction of proteinuria was regularly accompanied by greater outcome benefit in many other trials.4
By comparing the benefits of lvH regres-sion in the liFe trial and in the ontarGet and transCenD trials, it is possible to con-clude that cardiovascular therapies should be tailored according to the different stages of the cardiovascular disease continuum (Figure 1). intervention trials indicate that therapies are capable of reducing outcomes by approximately 25–30% independent of the risk level at which treatment is started.10 this means that when cardio vascular disease is more advanced and the initial risk is higher, the residual level of risk will also be higher even after all possible treatment benefits have been achieved.8 aiming to correct sub-clinical organ damage might be more bene-ficial when the progress of cardio vascular disease is moderate, such as in the liFe trial, and in contrast to the ontarGet and transCenD trials where cardio vascular outcomes had already occurred.
in con clusion, cardiovascular inter vention at a late stage of the disease is undoubtedly beneficial, but it cannot reverse the disease process entirely. addressing the early stages of the cardiovascular continuum allows
regression to a low-level of risk and pro-vides the possibility of arresting disease pro-gression, which can only be obtained and maintained by early intervention.Center for Clinical Physiology and Hypertension, University of Milan, Via F. Sforza 35, Milan 20122, Italy [email protected]
doi:10.1038/nrcardio.2009.229
acknowledgments This manuscript has been prepared as one of the activities of the eC network of excellence inGenious HyperCare (contract LsHM-CT-2006-037093). The author would like to thank Mrs Donatella Mihalich and Mrs Cinzia Tiberi for their invaluable assistance.
competing interests The author declares no competing interests.
1. verdecchia, P. et al. effects of telmisartan, ramipril, and their combination on left ventricular hypertrophy in individuals at high vascular risk in the Ongoing Telmisartan Alone and in Combination with Ramipril Global end Point Trial and the Telmisartan Randomized Assessment study in ACe intolerant subjects with Cardiovascular Disease. Circulation 120, 1380–1389 (2009).
2. Yusuf, s. et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N. Engl. J. Med. 358, 1547–1559 (2008).
3. Yusuf, s. et al. effects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trial. Lancet 372, 1174–1183 (2008).
4. Mancia, G. et al. Reappraisal of european guidelines on hypertension management: a european society of Hypertension Task Force document. J. Hypertens. 27, 2121–2157 (2009).
5. Dahlöf, B. et al. Cardiovascular morbidity and mortality in patients with diabetes in the Losartan intervention For endpoint reduction in hypertension study (LiFe): a randomised trial against atenolol. Lancet 359, 995–1003 (2002).
6. Okin, P. M. et al. Regression of electrocardiographic left ventricular hypertrophy during antihypertensive treatment and the prediction of major cardiovascular events. JAMA 292, 2343–2349 (2004).
7. Okin, P. M. et al. Regression of electrocardiographic left ventricular hypertrophy is associated with less hospitalization for heart failure in hypertensive patients. Ann. Intern. Med. 147, 311–319 (2007).
8. Zanchetti, A. Bottom blood pressure or bottom cardiovascular risk? How far can cardiovascular risk be reduced? J. Hypertens. 27, 1509–1520 (2009).
9. Mann, J. F. et al. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the OnTARGeT study): a multicentre, randomised, double-blind, controlled trial. Lancet 372, 547–553 (2008).
10. Law, M. R., Morris, J. K. & wald, n. J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 338, 1665–1683 (2009).
pHarMacoTHErapy
Intracoronary streptokinase in acute myocardial infarctionPaul W. Armstrong
despite angiographically successful primary percutaneous coronary intervention (pci) in patients with sT-segment elevation myocardial infarction, microcirculatory failure is common and leads to an increased risk of morbidity and mortality. The administration of intracoronary streptokinase immediately after pci may improve outcomes and provides a promising potential therapy for the future.
a pioneering study by rentrop et al.1 showed that intracoronary infusion of s t repto k inase could achieve rapid
recanalization following acute myocardial infarction. the seminal work by Dewood et al.2 that demonstrated the role of
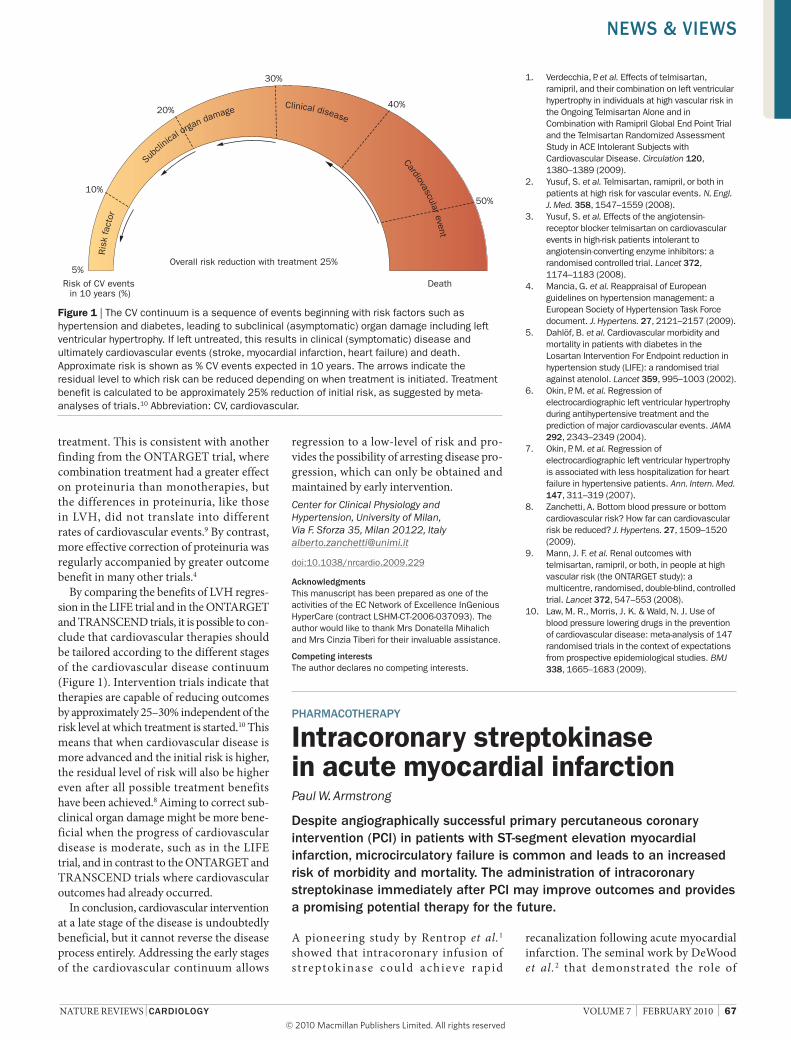
Figure 1 | The Cv continuum is a sequence of events beginning with risk factors such as hypertension and diabetes, leading to subclinical (asymptomatic) organ damage including left ventricular hypertrophy. if left untreated, this results in clinical (symptomatic) disease and ultimately cardiovascular events (stroke, myocardial infarction, heart failure) and death. Approximate risk is shown as % Cv events expected in 10 years. The arrows indicate the residual level to which risk can be reduced depending on when treatment is initiated. Treatment benefit is calculated to be approximately 25% reduction of initial risk, as suggested by meta-analyses of trials.10 Abbreviation: Cv, cardiovascular.
Risk of CV events in 10 years (%)
Death
Overall risk reduction with treatment 25%5%
10%
20%
30%
40%
50%
Ris
k fa
ctor
Su
bclin
ical orga
n damage Clinical disease Cardiovascular event
nrcardio_NV_FEB10.indd 67 11/1/10 16:29:33
© 20 Macmillan Publishers Limited. All rights reserved10