how to understand and implement health literacy conference/health literacy mdhhs... · how to...
TRANSCRIPT
How to Understand and
Implement Health Literacy
Presented by: Dr. Nickell M. Dixon
HEALTH DISPARITIES REDUCTION/ MINORITY HEALTH SECTION
OFFICE OF HEALTH POLICY AND INNOVATION
Objectives
•List barriers to good communication in public health
•Provide an example for each barrier
•List techniques to improve health communication.
•Define plain language
•Describe communication strategies you can apply in
your daily work
2
OUTLINE
What is literacy
Health literacy
framework
Identifying and
Assessing Health
Literacy
Who is responsible
for improving health
literacy
What can you do
Strategic Planning
Patient/Physician
communication
Patient Centered
Approach
Follow Up
3
WHAT IS HEALTH
LITERACY?
4

Consider Patricia Olsen, the 42-year-old woman who was asked if she had taken her
antibiotic premedication and responded:
Patient: “Yes…well actually, No, I didn’t. Tell me again why I’m supposed to take that
medication.”
Dental Hygienist: “Pat, when I saw you last year you told me that you had had an
artificial heart valve placed in your heart. Do you remember our discussion about that?”
Patient: “I remember my doctor telling me about my heart valve but I also remember her
saying that I don’t have to worry about it.”
Dental Hygienist: “I know; and, most of the time that’s true. However, the mouth is a
warm and moist environment and many germs live and grow in our mouths. When we
clean your teeth it’s common for some of these germs to get into your bloodstream and
travel through your body. Normally, your body’s defense mechanisms remove these
germs within a short amount of time. However, when a person has an artificial heart
valve, like you do, there is a risk that the bacteria might attach themselves to that valve
and begin to grow. This can cause an infection around the blood vessel that could
become serious. That is why we want you take an antibiotic before you have dental
procedures done. That way, if any bacteria do get into your bloodstream, the medication
will be waiting there to destroy them before they can attach to your blood vessel and
cause a problem.”
Patient: “Now that you say that, I do remember my doctor telling me that I would have to
take antibiotics if I ever have surgery. I guess I just didn’t think getting my teeth cleaned
was such a big deal. Now that you’ve explained it to me it makes more sense.”
Dental Hygienist: “Pat, just so that I know I’ve explained it clearly to you, would you
please tell me why we want you to take antibiotics before your dental appointments?”
5
What is Health Literacy?
A set of skills that people need to function
effectively in the health care environment
Degree to which individuals have the capacity
to obtain, process, and understand basic health
information and services needed to make
appropriate health decisions.
6
Source: Berkman et al (2011). Health literacy interventions and outcomes: an updated systematic review, pg. ES1. 1Institute of Medicine

7
Why is it important?
Better health outcomes
• health-related decisions should be based on clear and
correct understanding of relevant health information and
services.
People who have low literacy are most likely not health
literate.
People with limited health literacy may not be able to
navigate the health care system and to find the right
resources.
Over 70 millions adults in our country with limited
health literacy cannot fully benefit from medical care
and the health care system.
8 (Howard, Gazmararian, & Parker, The impact of low health literacy on medical costs of medicare
managed care enrollees, 2005)
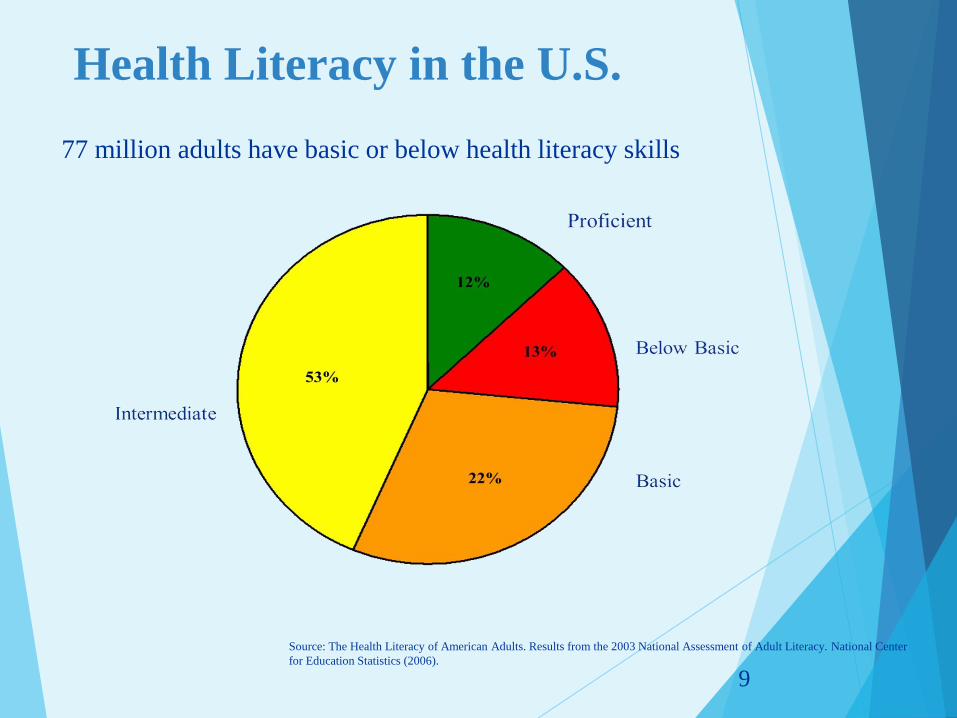
Health Literacy in the U.S.
77 million adults have basic or below health literacy skills
9
Source: The Health Literacy of American Adults. Results from the 2003 National Assessment of Adult Literacy. National Center
for Education Statistics (2006).
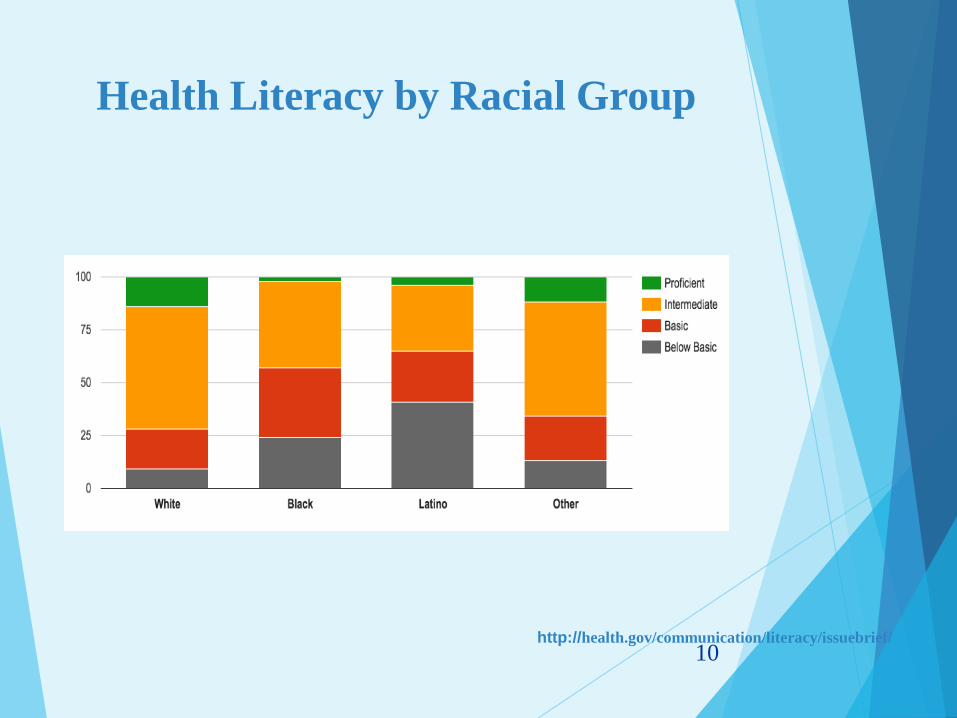
Health Literacy by Racial Group
10 http://health.gov/communication/literacy/issuebrief/
Economic Impact
It is estimated that limited health literacy
costs the U.S. health care system
between $50 and $73 billion per year
11
Source: American Medical Association Foundation (2009). Health literacy and patient safety: manual for clinicians, pg. 7.
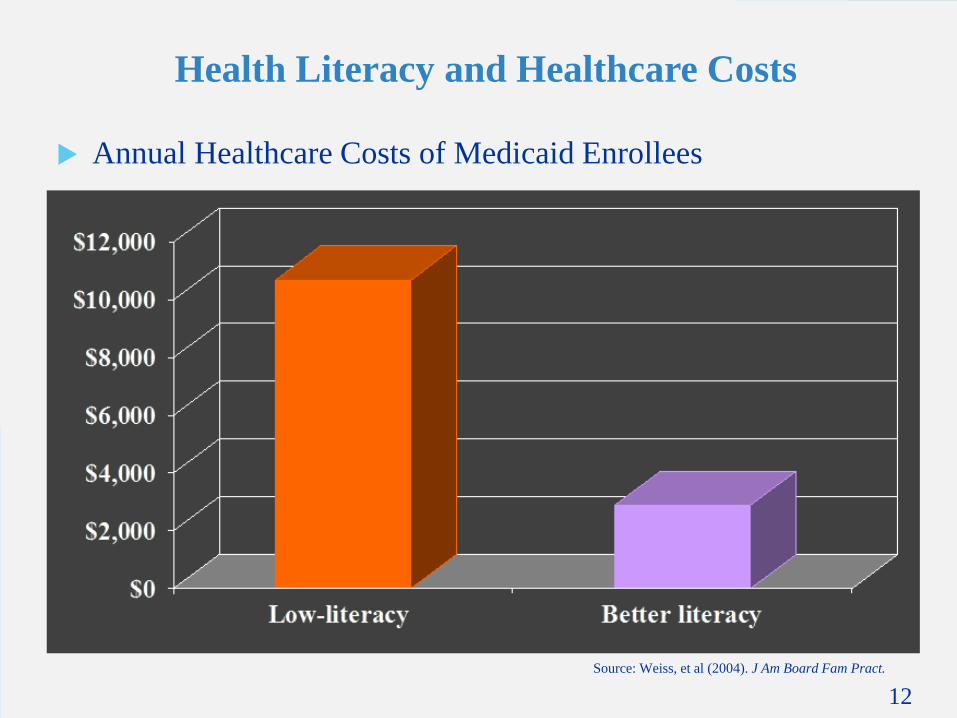
Health Literacy and Healthcare Costs
Annual Healthcare Costs of Medicaid Enrollees
12
Source: Weiss, et al (2004). J Am Board Fam Pract.
(<3rd-grade reading level) (>4th-grade reading level)

Increased Healthcare Costs
Annual health costs for individuals with low health literacy skills are four times higher than for people with higher skills.
(Howard, Gazmararian, & Parker, The impact of low health literacy on medical costs of medicare managed care enrollees, 2005)
13

Pop Quiz
Health Literacy develops over a
lifetime?
True
False
14

Pop Quiz
1. Health Literacy develops over a
lifetime?
True
False
15

HEALTH LITERACY
FRAMEWORK
16
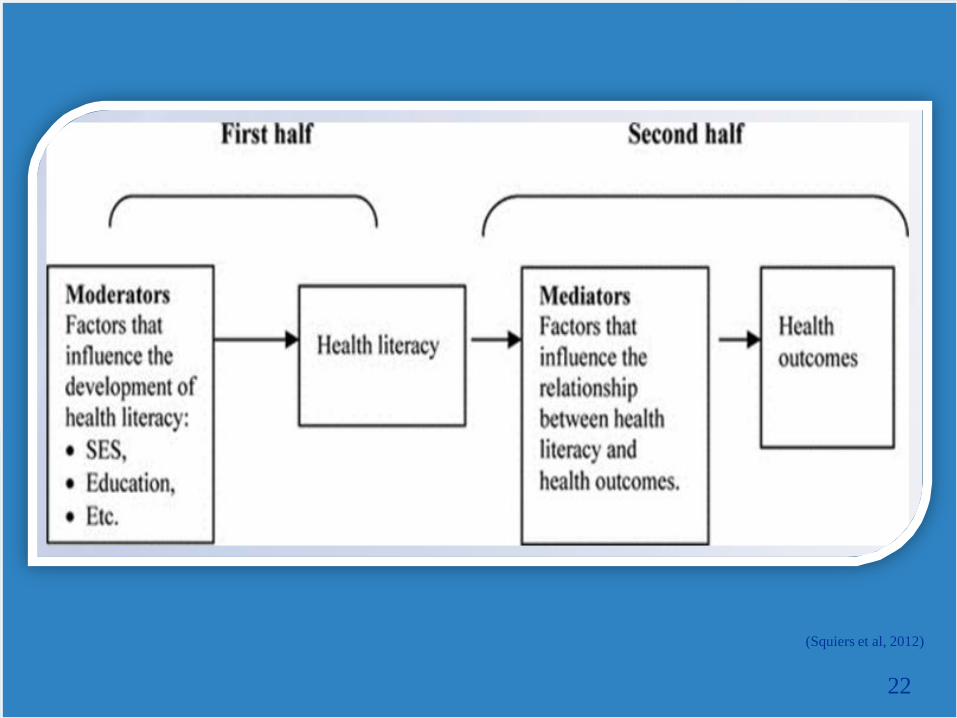
(Squiers et al, 2012)
22

18
MODERATORS
Health Literacy and Health
Disparities
There is a strong correlation between health literacy and health
disparities.
o Health disparities: “Differences in health that occur by gender,
race or ethnicity, income or education, disability, living in a rural
locality, or sexual orientation.
HHS reports that the cultural and linguistic differences among
patients directly impact their health literacy levels, which, in
turn, contributes to an increased prevalence of health
disparities among minorities.
19
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2966655/
Health Literacy and Health
Disparities
Studies show that when controlling for health literacy, racial
and ethnic disparities in health care quality and outcomes often
disappear.
20
http://www.chcs.org/media/CHCS_Health_Literacy_Fact_Sheets_2013.pdf

High-Risk Groups
Elderly
Minorities
Limited English Proficiency (LEP)
patients
Low income
Homeless
Prisoners
Persons with limited education
Learning Disabled
(Berkman, Sheridan, Donahue, Halpern, & Crotty, 2011)
21
26
MEDIATORS
22
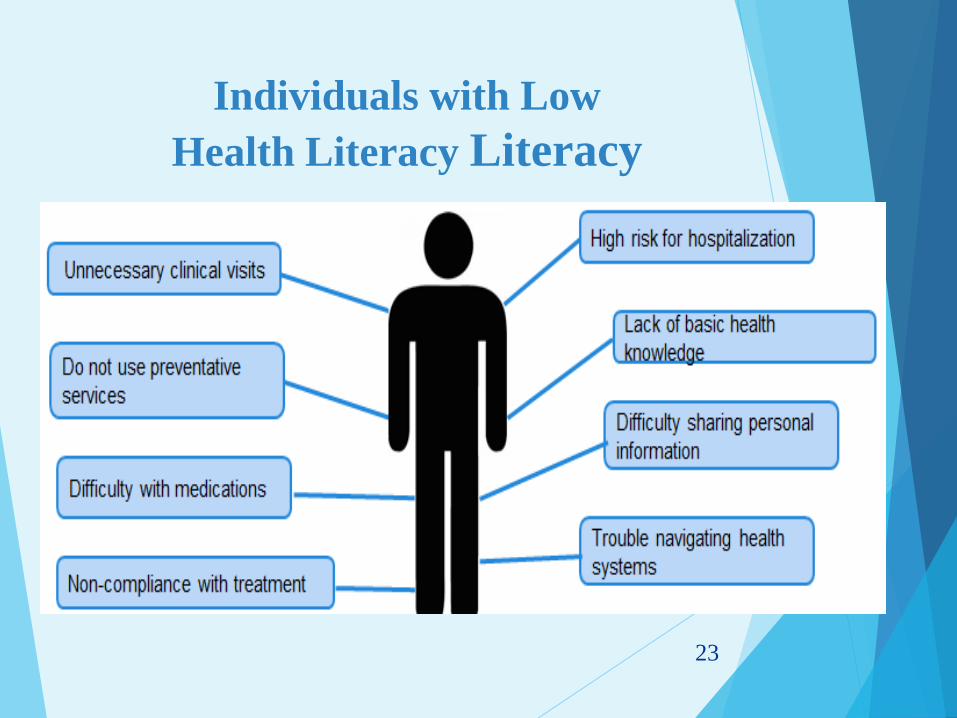
Individuals with Low
Health Literacy Literacy
23
Poor compliance with medical treatment
Often appear to be noncompliant with medical
treatment.
may miss appointments
forget to take medications
fail to follow self-treatment regimens
24 Brown, M. T., & Bussell, J. K. (2011). Medication Adherence: WHO Cares? Mayo Clinic Proceedings, 86(4), 304–314.
doi:10.4065/mcp.2010.0575

POOR HEALTH OUTCOMES
25

Poor Health Outcomes
Poor literacy skills often result in poor health outcomes for individuals.
• Diabetes
• Hypertension
• Cancer
Fail to seek preventive care and are at more than double the risk for hospitalization
Report poorer health status than people with better literacy skills.
Adult patients with low health literacy in primary care clinics were less able to describe how they would take 5 medications and had a greater probability of misunderstanding instructions on 1 or more labels.
Higher all cause mortality
26
http://health.gov/communication/literacy/quickguide/factsbasic.htm
IDENTIFYING AND
ASSESSING HEALTH
LITERACY
27

POSSIBLE SIGNS OF
LOW HEALTH LITERACY
Your patients’ may
frequently say:
• I forgot my glasses
• My eyes are tired
• I’ll take this home for
my family to read
• What does this say? I
don’t understand this
Your patients’ behavior
may include:
• Not getting their
prescriptions filled, or not
taking their medications as
prescribed
• Consistently arriving late to
appointments
• Returning forms without
completing them
• Requiring several calls
between appointments to
clarify instructions
28
Testing for Health Literacy
There are several test that can be used to measure
Health Literacy in patients:
Test of Functional Health Literacy in Adults
(TOFHLA)
Newest Vital Sign (NVS)
The Short Assessment of Health Literacy-Spanish
and English (SAHL-S & E)
Rapid Estimate of Adult Literacy in Medicine-Short
Form (REALM-SF)
Short Assessment of Health Literacy for Adults
Spanish(SAHLSA-50)
29

Oral Health Literacy
Questions
1) How often do you have somebody help you read hospital materials?
2) How confident are you filling out medical forms by yourself?
3) How often do you have problems learning about your medical condition because of difficulty understanding written information?
30

PATIENT/PHYSICIAN
COMMUNICATION
31
Patient-physician relationship
Patients ’ most common complaint is the lack
of information provided by physicians
Majority of malpractice suits arise from
communication errors; not incompetence
32 Silverman, Kurtz and Draper: Skills for communicating with patients 2005
The Seven Learning Styles
1. Visual (spatial):You prefer using pictures, images, and spatial understanding.
2. Aural (auditory-musical): You prefer using sound and music.
3. Verbal (linguistic): You prefer using words, both in speech and writing.
4. Physical (kinesthetic): You prefer using your body, hands and sense of touch.
5. Logical (mathematical): You prefer using logic, reasoning and systems.
6. Social (interpersonal): You prefer to learn in groups or with other people.
7. Solitary (intrapersonal): You prefer to work alone and use self-study.

Medical
Hypertension
Insomnia
Benign
Hazardous
Disorder
Option
Routinely
Adverse
Plain Language
High blood pressure
Can’t sleep
NOT cancer
Dangerous
Problem
Choice
Often
Bad
Plain Language
34
http://www.plainlanguage.gov/
Instead of saying Periodontal disease, you might say:
“The gum tissue and jaw bone surrounds and supports the teeth,
just like the foundation of a house surrounds and supports our
homes. If we don’t take care of problems in the foundation of the
home, it doesn’t matter how good the condition of the home might
be, a weak foundation won’t be able to support it. The same is true
of your gum tissue, no matter how healthy your teeth are, if the
gum tissue and bone that support your teeth aren’t healthy, you
might still lose your teeth.”
35

Tips to Identify a Patient’s
Preferred Language
Ask the patient for their preferred spoken and
written language.
• Display a poster of common languages spoken by
patients
• Ask them to point to their language of preference.
Make available and encourage patients to
carry “I speak….” or “Language ID” cards.
• Many phone interpreter companies provide
language posters and cards at no charge.
36
Interpreter
Individuals who are not trained to be an interpreter
make more clinically significant mistakes.
Unacceptable language assistance:
• Untrained/Uncertified clinicians or staff
• The patient’s family and friends
• Minor children
37 http://khn.org/news/trained-interpreters-help-avoid-medical-mishaps-michelle-andrews-052212/

Trained health care interpreters can reduce liability, help
ensure appropriate utilization, and increase client
adherence and satisfaction with services.
Trained interpreters help to assure effective
communication between the client and provider, support
effective use of time during the clinical encounter, and
improve outcomes.
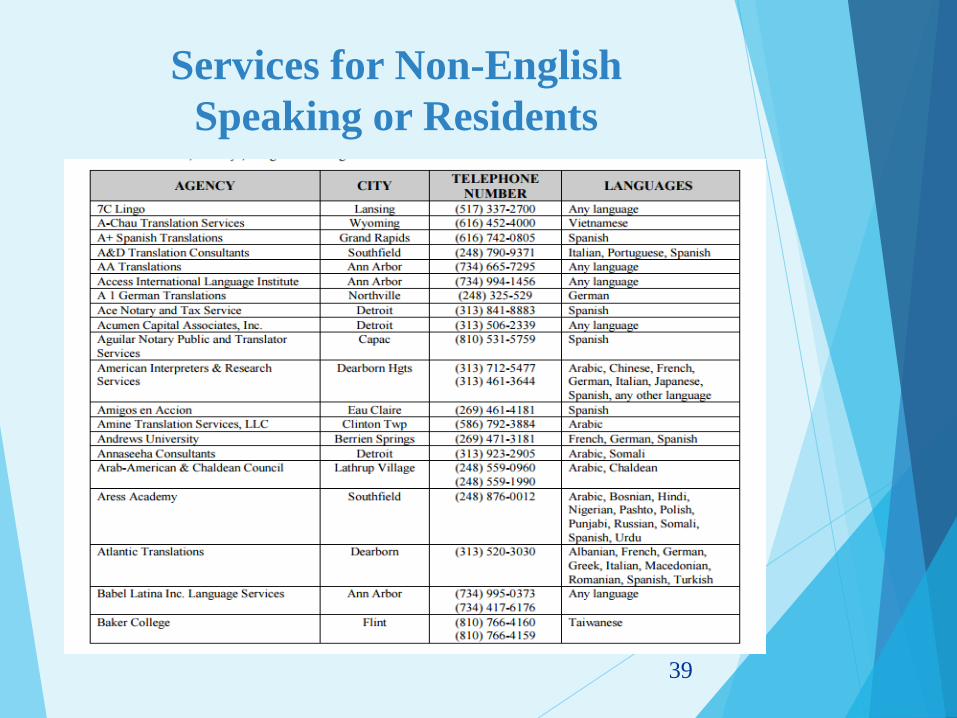
Services for Non-English
Speaking or Residents
39

Don’t Assume
► If the information is critical, make sure you or someone in your office reviews the information with your patient and/or the patient’s caregiver.
When reviewing a handout:
► Circle or highlight the most important points as you talk about them.
► Personalize the material by adding the patient’s name, medicines, and/or specific care instructions.
► Use teach-back to confirm understanding.
► Emphasize the importance of the material by referring to it during follow up phone calls, emails, and future office visits. You may need to give the material to the patient more than once.
40
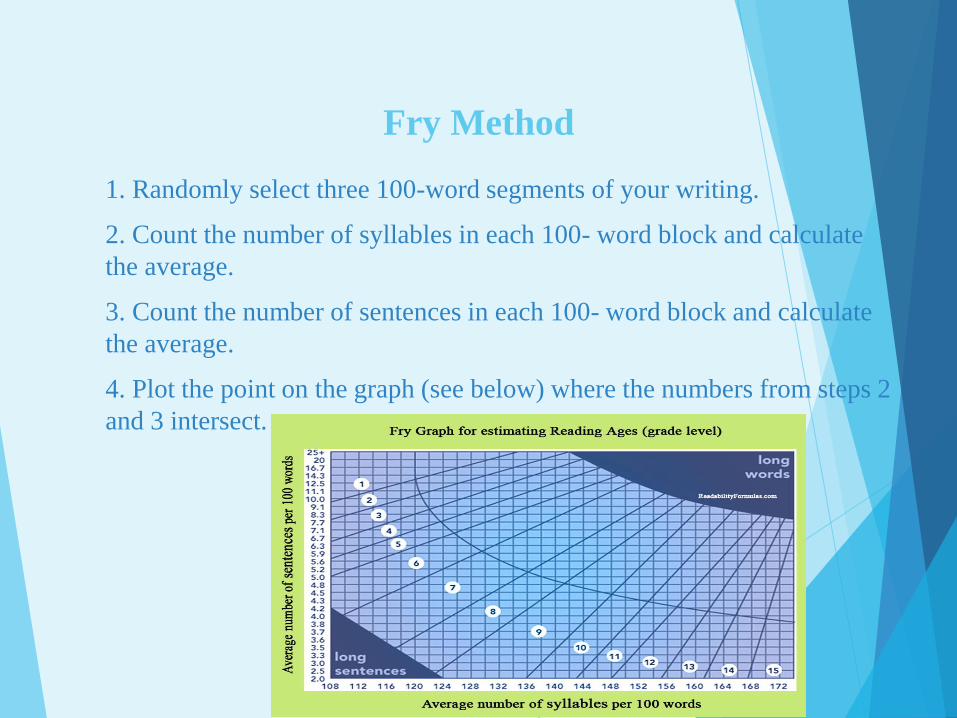
Fry Method
1. Randomly select three 100-word segments of your writing.
2. Count the number of syllables in each 100- word block and calculate
the average.
3. Count the number of sentences in each 100- word block and calculate
the average.
4. Plot the point on the graph (see below) where the numbers from steps 2
and 3 intersect.
Are you pregnant? Do you get health coverage from an Iowa
program? If you do, your baby will also be covered. Coverage
will last until the end of the month of your baby’s first
birthday. The baby must live with you in Iowa.
Grade 3, according to Fry’s Readability Graph
Health Literacy and Culture
The Institute of Medicine has called for the need to view
health literacy in the context of language and culture.
43
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2910560/
Consider Culture, Customs,
and Beliefs Tool
Religion, culture, beliefs, and ethnic
customs can influence
how patients understand health concepts
how they take care of their health
how they make decisions related to their
health
44 http://www.med.unc.edu/tarc/files/HLUPTRheum.pdf
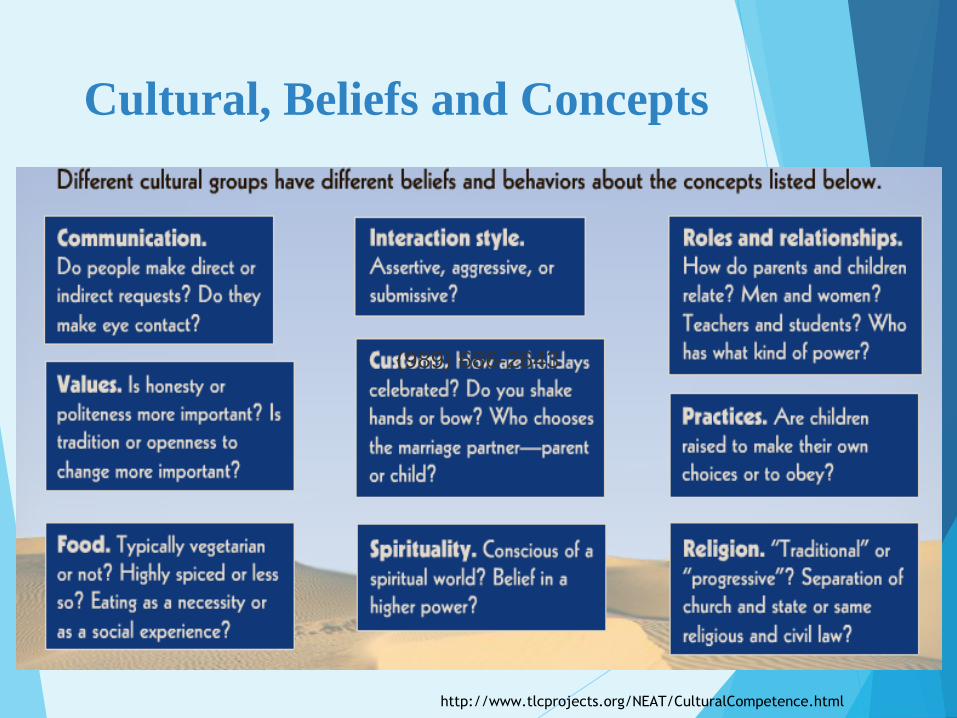
Cultural, Beliefs and Concepts
(989) 686-2643
http://www.tlcprojects.org/NEAT/CulturalCompetence.html
Teach Back Method
Studies have shown that 40-80 percent of the medical information
patients receive is forgotten immediately and nearly half of the
information retained is incorrect.
One of the easiest ways to close the gap of communication
between clinician and patient is to employ the “teach-back”
method, also known as the “show-me” method or “closing the
loop.”
Teach-back is a way to confirm that you have explained to the
patient what they need to know in a manner that the patient
understands.
Patient understanding is confirmed when they explain it back to
you. It can also help the clinic staff members identify explanations
and communication strategies that are most commonly understood
by patients
46
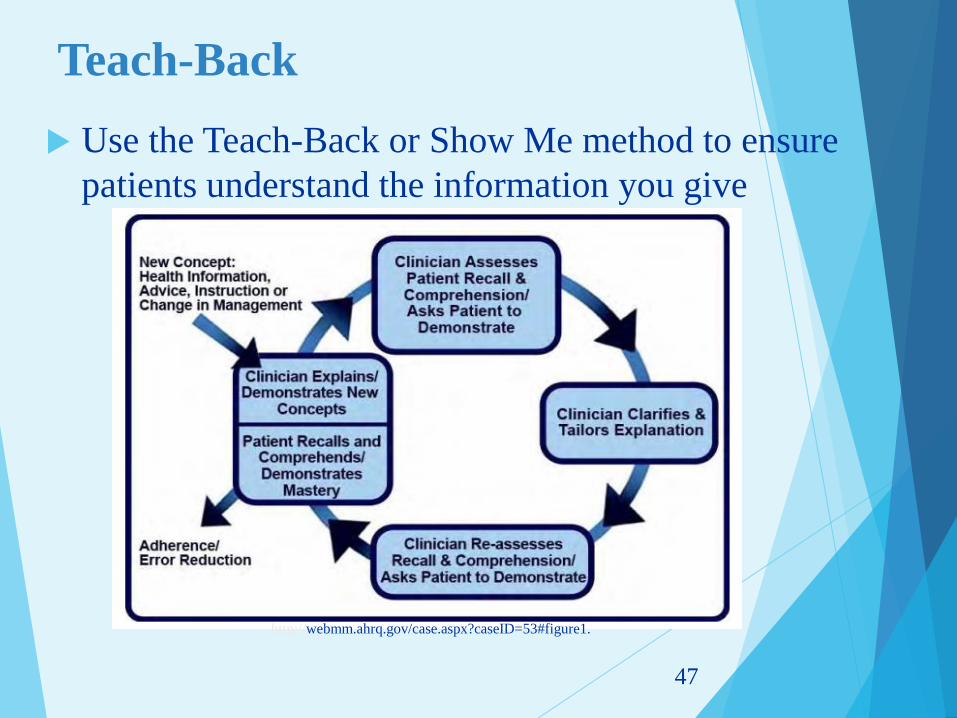
Teach-Back
Use the Teach-Back or Show Me method to ensure
patients understand the information you give
47
http://webmm.ahrq.gov/case.aspx?caseID=53#figure1.
Use Teach Back Method when discussing
brushing teeth, flossing etc.
Dental Hygienist: “Let’s review the most effective way to floss
your teeth. I’ll have you watch me floss your teeth first and then,
just to make certain that I’ve explained this clearly, I’ll have you
demonstrate the technique back for me.”
48

WHO IS RESPONSIBLE
FOR IMPROVING
HEALTH LITERACY?
49
Who is responsible for
improving health literacy?
Public health professionals, health care
providers, and the health care and public health
systems have primary responsibility.
Health literacy has direct impact on the three
pillars of medical and health services
provision:
• Increased quality
• Improved patient/consumer experience and
patient outcomes
• Reduced costs
50
Making Changes
The Institute of Medicine stated in order to address the
challenge of health literacy requires system-level
changes for both health professionals and organizations.
Systems change include using the universal health
literacy precaution methods which include:
Form changes,
Sending forms before appointments,
No heavy use of patient portal, better
communication with patients,
Uses of decision aids to help with patient
understanding
51
(Easton, Entwistle, & Williams, 2013; Weiss, 2014)
NIDCR Work Group on Functional
Health Literacy (2004)
The National Institute of Dental and Craniofacial Research
(NIDCR) convened a Working Group on Functional Oral
Health Literacy in January 2004.
The workgroup used existing health literacy knowledge from
the medical field to begin building an understanding of oral
health literacy.
The workgroup was interested in the ways in which the issue
of health literacy affected the adoption of effective disease
prevention methods, patient adherence to treatment regimens,
and ultimately, improved oral health status.
In addition, the potential impact of oral health literacy on
clinical research was also acknowledged.
52

The ADA’s House of Delegates
meeting in 2006 The delegates adopted the following six oral health literacy-related resolutions:
Res. 14H-2006: “The ADA recognizes that limited oral health literacy is a potential barrier to effective prevention, diagnosis and treatment of oral disease.”
Res. 16H-2006: Directed the ADA’s Council on Access, Prevention and Inter-professional Relations (CAPIR) to work with the Council on Government Affairs and other appropriate ADA agencies to develop and implement an advocacy strategy, based on the 2006 School Health Policies and Programs Study (SHPPS) data, to increase the number of school districts requiring oral health education for K-12 students.
Res. 17H-2006: Authorized the ADA President to appoint a three-year National Oral Health Literacy Advisory Committee (NOHLAC) of 12 national health literacy experts from dentistry, public health, literacy and other advocacy organizations.
Res. 18H-2006: Directed the CAPIR to design and execute a comprehensive oral health literacy awareness and education strategy targeting the entire dental team. The NOHLAC is will provide recommendations for this plan.
Res. 19H-2006: Instructed CDEL and other appropriate ADA agencies to encourage the development of undergraduate, graduate and continuing education programs to train dentists and allied dental team members to effectively communicate with patients with limited literacy skills.
Res. 23H-2006: Requested ADA agencies to develop guidelines for the creation of educational products to meet the needs of patients with limited literacy skills, including the involvement of targeted audiences in materials development.
53

WHAT CAN YOU DO?
54

Dental practice-related malpractice
statistics for the years 1990-2004:
The National Practitioner Data Bank Public Use File (NPDB) Summary Report:
34,691 malpractice reports regarding dentist
137 malpractice reports regarding dental residents
17 malpractice reports regarding dental hygienists
19 malpractice reports regarding denturists
8 malpractice reports regarding dental assistants
The reasons for these Patient-Clinician Related Malpractice Lawsuits were categorized as follows:
Inadequate explanation of diagnoses
Inadequate explanation of treatment
Patient feels ignored
Clinician fails to understand the perspective of patient
Clinician discounts or devalues views of patients or relatives
Patient feels rushed
55
CLAS
Enhanced in April 2013
Focuses on health equity
For use by both health
care and health service
organizations
CLAS Standards
Eliminate Health/care Inequities
Improve Quality of Services
Advance Health Equity

CLAS
CLAS standards require health care providers to:
Provide free language assistance to individuals who are not
proficient in English
Notify individuals in their preferred language, verbally and in
writing, of the availability of language assistance
Establish competence of individuals who provide language
assistance rather than using untrained interpreters minors
Provide easy-to-read handouts and posters in common
languages other than English
Include Health Literacy in
Staff Training and Orientation
Training staff will increase awareness of the need for addressing health literacy and improve their skills for communicating with the public.
Include information on health literacy in staff orientation.
Make a presentation on health literacy at your next staff meeting.
Circulate relevant research and reports on health literacy to colleagues.
Post and share health literacy resources.
58

A Health Literate Healthcare Organization 1. Has leadership that makes health literacy integral to its mission, structure, and operations.
2. Integrates health literacy into planning, evaluation measures, patient safety, and quality
improvement.
3. Prepares the workforce to be health literate and monitors progress.
4. Includes populations served in the design, implementation, and evaluation of health information
and services.
5. Meets the needs of populations with a range of health literacy skills while avoiding
stigmatization.
6. Uses health literacy strategies in interpersonal communications and confirms understanding at
all points of contact.
7. Provides easy access to health information and services and navigation assistance.
8. Designs and distributes print, audiovisual, and social media content that is easy to understand
and act on.
9. Addresses health literacy in high-risk situations, including care transitions and communications
about medicines.
10. Communicates clearly what health plans cover and what individuals will have to pay for
services.
Roundtable on Health Literacy; Board on Population Health and Public Health Practice; Institute of Medicine. How Can Health Care Organizations Become
More Health Literate: Workshop Summary. Washington (DC): National Academies Press (US); 2012 Jul 18. 2, Attributes of a Health Literate Health Care
Organization. Available from: http://www.ncbi.nlm.nih.gov/books/NBK201212/
59
Has leadership that makes health
literacy integral to its mission,
structure, and operations.
Is health literacy apart of your mission?
How does health literacy impact the
structure of your office?
What operations are in place to address
health literacy in your office?
Does your office leadership have
training in health literacy?
60
Integrates health literacy into planning,
evaluation measures, patient safety, and
quality improvement.
Are patients with low health literacy
giving extra time in appointments?
What evaluations measures are in place
to assess health literacy in your office?
How is information delivered to
patients?
How are medication instructions
written?
61
Prepares the workforce to be health
literate and monitors progress.
Are there trainings in place for staff to
stay abreast on health literacy yearly?
Have all physicians and nurses take
CME and CNE offered on health
literacy and cultural competency?
Are behavior changes toward being
better with low health literate patients on
the staff performance evaluation?
62
Includes populations served in the design,
implementation, and evaluation of health
information and services.
* Are there audits on medical records to
determine all languages of patients in
the office?
* Are patients literacy/health literacy
levels tested?
* Is there a survey that asks the patients to
grade how the office is doing on various
areas of health literacy?
63
Meets the needs of populations
with a range of health literacy
skills while avoiding stigmatization. * How do patients get linked to non-medical
support?
* Are their less than five steps in getting a patient
a referral?
* How has the staff taking time to understand the
diverse cultures, religions and sexual
backgrounds of your patients?
* Have you used an interpreter service for all
clients who are ESL even if family member
interprets?
64

Uses health literacy strategies in
interpersonal communications and
confirms understanding at all points of
contact * Have written materials in patients’
spoken language?
* Use the Teach Back method with
all patients?
* How does your physician or office
encourage patients to ask
questions?
65
Provides easy access to health
information and services and
navigation assistance.
* Do you have patient navigators in
place?
* Are patients who do not have
computer access able to get their
results and questions easy?
66

Designs and distributes print,
audiovisual, and social media content
that is easy to understand and act on.
* Are patient materials tested for
readability and understandability?
* Is all information giving to patients on a
5th grade reading level?
* Are there any usage of decision aids to
help with decision making between the
patient and physician?
67
Addresses health literacy in high-risk
situations, including care transitions and
communications about medicines.
* Are there measures to help those with
low health literacy lessen injuries due to
medication and or treatment adherence?
68
Communicates clearly what health
plans cover and what individuals will
have to pay for services.
* Does the staff have a cheat sheet for
patients to understand their insurance
plan before seeing the physician?
* Is the physician knowledgeable of health
plans and order treatment accordingly as
not to increase fees to the patient?
* Are all services and fees are written
down for the patient and explained
thoroughly for the client to agree or
disagree with.?
69

STRATEGIC
PLANNING
70
Your Strategic Plan is to plan the best way to implement the
Health Literacy Universal Precautions rules, the toolkit is here to
help with the implementation.
71
Use Health Literacy Universal
Precautions Toolkit
Agency for Healthcare Research and Quality created the Universal
Precaution Health Literacy Toolkit
Because limited health literacy is common and is hard to recognize,
experts recommend using health literacy universal precautions.
Practices should assume that all patients and caregivers may have
difficulty comprehending health information and should
communicate in ways that anyone can understand.
Health literacy universal precautions are aimed at:
■ simplifying communication with and confirming comprehension for all
patients, so that the risk of
miscommunication is minimized8
■ making the office environment and health care system easier to navigate
■ supporting patients’ efforts to improve their health
72
Steps to Implementing
Universal Precaution
1. Raise Awareness
2. Form a Group
3. Bring Team Members together
4. Create a Health Literacy Improvement Plan
73

PATIENT CENTERED
APPROACH
74
Patient Advocacy
Part of health literacy is getting the patient to become better
advocates for their health.
This usually takes skill building of the patient.
Most hospitals, health departments, and clinics used
community health workers, health educators , volunteers and
other staff to spend some time with patients to help build these
skills including:
• Asking physician questions
• Shared decision making
• Medication Awareness
• Numeracy
75
Ask Me 3
Ask Me 3 is a patient education program designed to improve
communication between patients and health care providers,
encourage patients to become active members of their health care
team, and promote improved health outcomes.
The program encourages patients to ask their health care providers
three questions:
1. What is my main problem?
2. What do I need to do?
3. Why is it important for me to do this?
https://youtu.be/B3EB-icaNKQ
76
http://www.npsf.org/?page=askme3

“Don’t Ask, Don’t Tell”
Not revealing information due to the patient not asking about it does not work in the medical community especially for those who aren’t health literate
Those with low health literacy sometimes do not know what to ask or how to ask a question
Example of this are immunizations and testing.
• It is the physician's jobs to stress the importance of immunization and treatment options
http://sph.umich.edu/richmedia/sph/ophp/08.25.11_GrandRounds/08.25.11_GrandRounds.html
77
Decision Making
Not all patients agree on the same way of making decision about their
health.
Some believe :
The doctors should make all their decisions
The doctor and patient should make the decision together
The patient should make the decision with their families
The patient should make the decision alone
The patient will not make any decision.
78
Use Decision Aids in every situation
Patient decision aids are tools that help people
become involved in decision making.
making explicit the decision that needs to be made
providing information about the options and outcomes
clarifying personal values
Complement, rather than replace
Help those with low literacy make better decisions
and lessen decisional regret while also gaining
knowledge
There are numerous decisions aids already in
existence
http://shareddecisions.mayoclinic.org/decision-aid-information/decision-aids-for-chronic-disease 79

80

Shared Decision Making
Shared decision making (SDM) has been defined as: ‘an
approach where clinicians and patients share the best available
evidence when faced with the task of making decisions, and
where patients are supported to consider options, to achieve
informed preferences
81 Implementing shared decision making in the NHS.
Elwyn G, Laitner S, Coulter A, Walker E, Watson P, Thomson R
BMJ. 2010 Oct 14; 341():c5146.
6 steps to SDM
1) Invite Patient to participate
2) Present Options
3) Provide information on benefits and risks
4) Assist patients in evaluating options based on their goals and
concerns
5) Facilitate deliberation and decision making
6) Assist with implementation
82

NUMERACY AND
MEDICATION
83
What is Numeracy?
Numeracy is the type of math skills needed to function in
everyday life, in the home, workplace, and community
(Withnall 1995).
When applied to health behaviors, it describes the degree to
which individuals have the capacity to access, process,
interpret, and act on graphical and probabilistic health
information.
As a cognitive and functional skill, low numeracy correlates
with poor outcomes in the management of chronic diseases;
Numeracy is therefore an essential component of patients'
capacity to adhere to medication regimens.
84
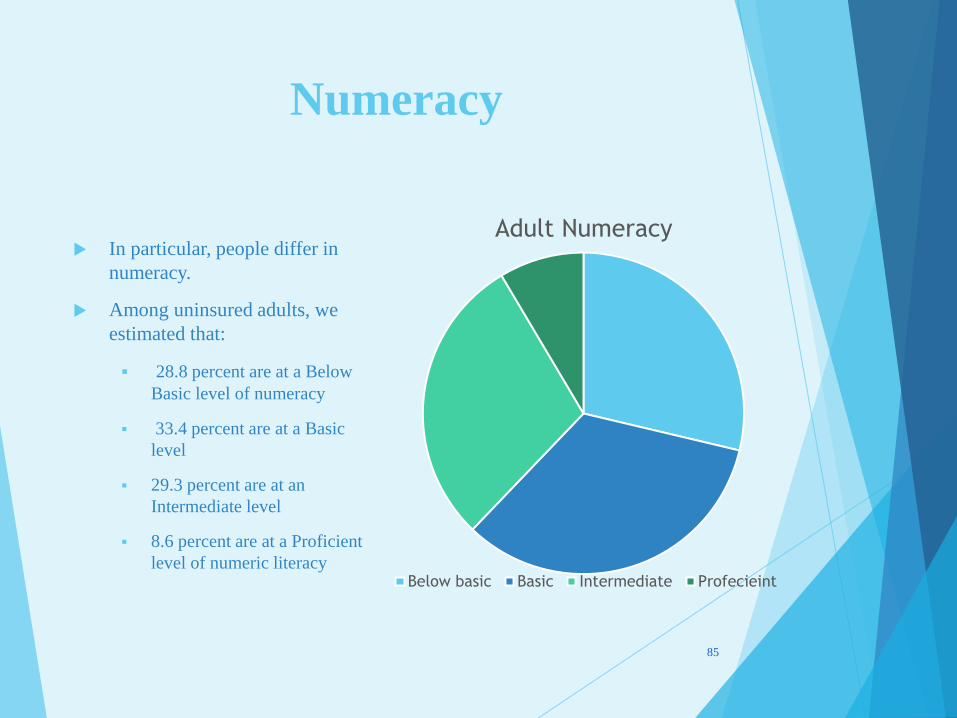
Numeracy
In particular, people differ in
numeracy.
Among uninsured adults, we
estimated that:
28.8 percent are at a Below
Basic level of numeracy
33.4 percent are at a Basic
level
29.3 percent are at an
Intermediate level
8.6 percent are at a Proficient
level of numeric literacy
85
Adult Numeracy
Below basic Basic Intermediate Profecieint

Numeracy
Numeracy skills are needed to :
select a health plan
choose treatments
understand medication instructions include education-based skills
and emergent decision-based abilities
We estimate that the skills needed to make many complex,
informed health decisions (e.g., management of chronic diseases)
require a Proficient level of numeric literacy, given how numeric
information is often provided.
86

CREATE A CHEAT SHEET
FOR NUMERACY
Create a cheat sheet to
help those with low
numeracy understand
basic measurements they
will use when taking
medication.
IE. difference
between MG and
MM and cup vs
ounces.
Maybe your clinic would
want to create this and
give it out to your
patients.
87
Summary of Recommendations for
Presenting Numerical Concepts
Recommendation
Use the fewest and simplest mathematical constructs
Remove nonessential information
Order information from most to least important or along a discernible hierarchy
Use several formats for presentation, e.g., verbal, quantitative, visual
Consider using constructive framing or anecdotes
Present benefits and risks, loss and gains, negative and positive
Realize positive is more likely to be chosen
Consider the best time frame for presenting risk
When using graphs, use most appropriate format and explain it to the patient
When applicable, show full denominator or full range of scale and explain both the numerator and denominator
Tailor information to the patient
Make communication interactive
Reinforce important messages with repeat instruction
Confirm comprehension
88

FOLLOW UP
89
Follow Up With Patients
Follow-up is the act of making contact with a patient or caregiver at a later, specified date to check on the patient’s progress since his or her last appointment.
Appropriate follow-up can help you to identify misunderstandings and answer questions, or make further assessments and adjust treatments.
Choose the ways your office will follow up.
Phone.
Secure email.
Texting.
Postal mail.
Automated calling system
Note Patient Portal isn't an option
Summary
Understanding and implementing Health Literacy
is beneficial for the patient, the healthcare
community and economically the nation.
Health Literacy changes start with understanding
the patient, training staff, updating materials, and
continuing education amongst health care
workers.
Decisions aids are a great tool to help those with
low literacy.
91
Health Literacy Communication
Checklist
Plain Language
Proper Use of Interpreters
Making Patient Materials readable for a 4th grade level
Consider Culture of the Patient
Use teach Back Method
Tell even IF they don’t ASK
Use Decision Aids
Medication Brown Bag
Follow up with patients ( less Patient Portal)
92
Questions & Comments
Dr. NICKELL M. DIXON, DrPH, MPH
HEALTH EQUITY INITIATIVE COORDINATOR
HEALTH DISPARITIES REDUCTION AND MINORITY HEALTH SECTION
PHONE: 517-373-6865
FAX: 517-241-1200
CAPITOL VIEW BLDG., 7th Floor 201 TOWNSEND STREET
LANSING, MI 48913
E-MAIL:[email protected]
www.michigan.gov/mdch
93