how to handle common eye problems in your practice shuan dai, franzco eye doctors ascot hospital...
TRANSCRIPT

How to Handle Common Eye How to Handle Common Eye ProblemsProblems
in Your Practicein Your Practice
Shuan Dai, FRANZCO
Eye Doctors
Ascot Hospital

The Red EyeThe Red Eye• A “Red Eye” may be due to an abnormality of the
ocular structures including:• Adnexa
• Lid Disorders• Lacrimal System• Orbital Disease
• Globe• Conjunctival / Scleral Disorders• Corneal Disease• Uveitis• Glaucoma

Adnexal RednessAdnexal Redness
• Lids• Blepharitis• Stye • Chalazion• Topical Allergic
• Lacrimal System• Dacryocystitis• Canaliculitis• Dacryoadenitis
• Orbit• Cellulitis
• Preseptal• Orbital
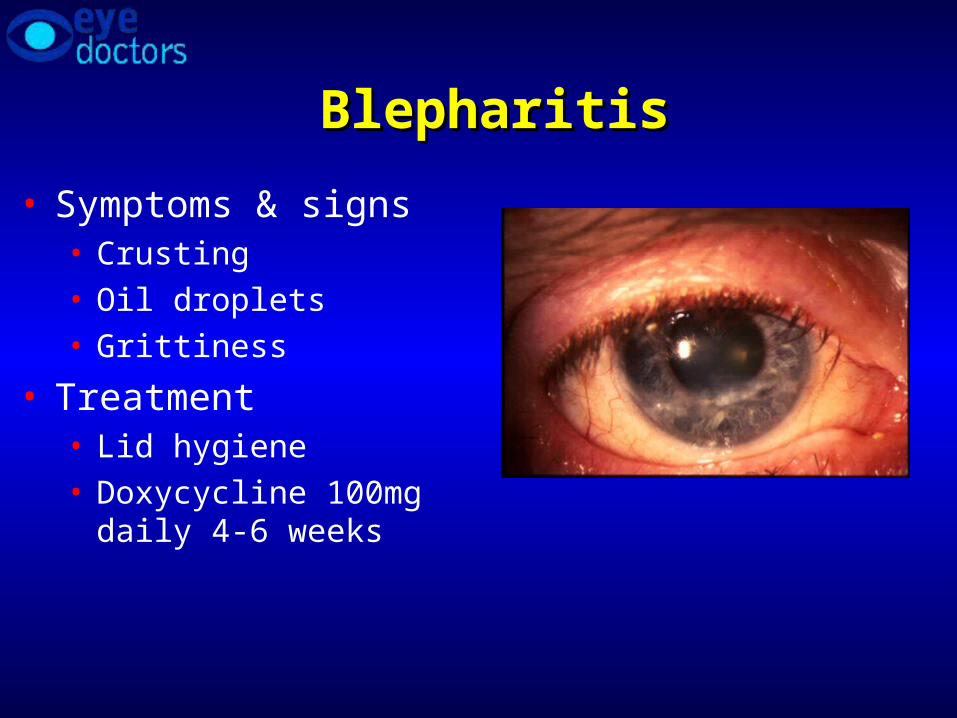
BlepharitisBlepharitis
• Symptoms & signs • Crusting • Oil droplets• Grittiness
• Treatment• Lid hygiene • Doxycycline 100mg daily
4-6 weeks

StyeStye & Chalazion & Chalazion

DacryocystitisDacryocystitis
• Recurrent watering eye
• Mucous/purulent discharge
• Abscess /lump over lacrimal sac
• Blocked tear duct

Ophthalmia NeonatorumOphthalmia Neonatorum
• Infantile purulent conjunctivitis• Chemical from antibiotic
drops/silver nitrate• Chlamydia• Gonorrhea
• An ocular emergency as GC can invade the intact cornea and perforate the globe

Lacrimal sac mucoceleLacrimal sac mucocele
• An uncommon variant• Look for an elevated
mass extending medially
• Life threatening if infected – refer for intravenous antibiotics

DacryoadenitisDacryoadenitis
• Acute painful
• Swelling lateral upper lid
• Viral/bacteria infection
• Oral/iv antibiotics

OrbitalOrbital CellulitisCellulitis
• Proptosis
• Limited eye movement
• Reduced vision

Redness Confined to the Redness Confined to the GlobeGlobe
• Conjunctiva / Sclera• Subconjunctival
hemorrhage• Ocular injection –
conjunctivitis• Pingueculum /
Pterygium• Episcleritis• Scleritis
• Cornea• Keratitis• Corneal abrasion• Corneal ulcer
• Anterior chamber• Iritis• Endophthalmitis
ConjunctivitisConjunctivitis
• Bacterial• Purulent discharge• Papillary reaction• Associated blepharitis
• Viral• Mucoid discharge• Follicular reaction• Associated URTI,
epidemic
• Allergic• Seasonal• Papillary reaction• Associated rhinitis,
itching

Bacterial ConjunctivitisBacterial Conjunctivitis• Symptoms: discharge,
irritation• Signs: papillary
conjunctivitis, perilimbal injection if associated keratitis
• Treatment: chloramphenicol/fucithalmic
• Danger: if hyperpurulent (gonococcal) or recent intraocular surgery REFER!

Viral ConjunctivitisViral Conjunctivitis
• Highly contagious, epidemics• Symptoms: previous URTI,
previous contacts, mucoid discharge, often photophobia
• Signs: preauricular node, pseudoptosis, follicular conjunctivitis ,conjunctival injection, punctate keratitis
• Treatment: cool compresses, ocular lubricants. Referal
• Warning: extreme infectivity, second eye at one week, lasts 10 – 14 days

Allergy -Allergy -Papillary conjunctival Papillary conjunctival reactionreaction

Allergic ConjunctivitisAllergic Conjunctivitis
• Symptoms: itching, seasonal, atopic history, rhinitis
• Signs: papillary reaction, mucus
• Treatment: cool compresses, ocular lubricants, anti-histamines - topical (Vasocon A) or systemic, Opticrom (Na chromoglycate) prophylaxis
• Possible history of contact lens wear with giant papillary conjunctivitis
• Treatment:• Lomide • Patanol• Steroid, i.e. FML

Pingueculum & PterygiumPingueculum & Pterygium
Pingueculum is degenerative collagen within the interpalbebral fissure
Pterygium extends onto the cornea

Episcleritis & ScleritisEpiscleritis & Scleritis
Episcleritis
Less painful
Younger age
No systemic association
Diffuse Scleritis
Extremely painful
Elderly,
RA, systemic vasculitis
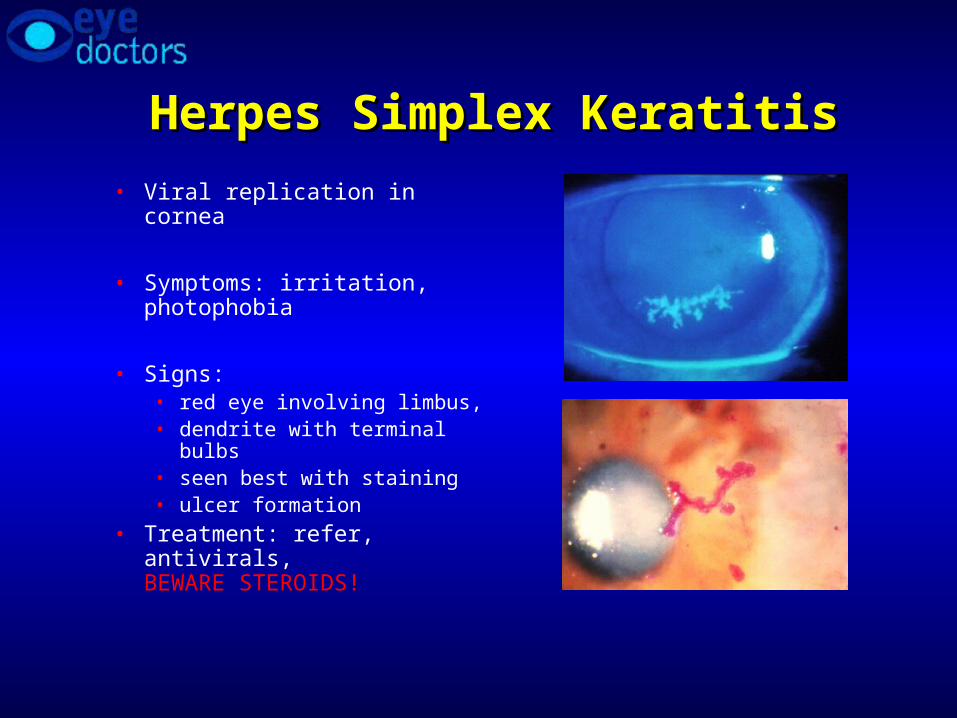
Herpes Simplex KeratitisHerpes Simplex Keratitis
• Viral replication in cornea
• Symptoms: irritation, photophobia
• Signs:• red eye involving limbus, • dendrite with terminal bulbs• seen best with staining • ulcer formation
• Treatment: refer, antivirals, BEWARE STEROIDS!
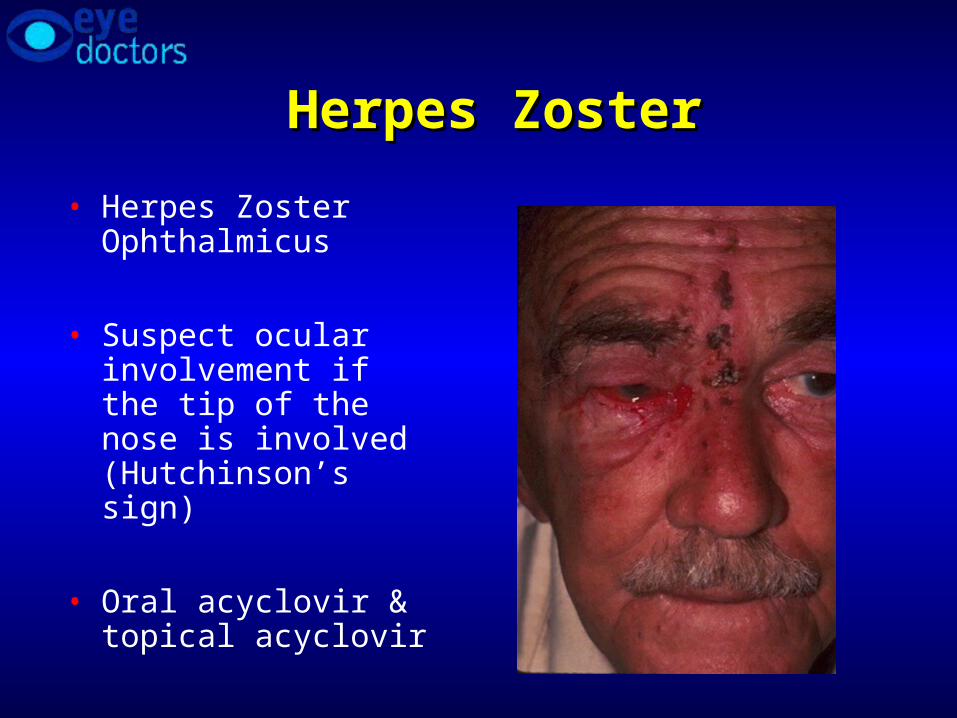
Herpes ZosterHerpes Zoster
• Herpes Zoster Ophthalmicus
• Suspect ocular involvement if the tip of the nose is involved (Hutchinson’s sign)
• Oral acyclovir & topical acyclovir
IritisIritis
• Etiology• 50% idiopathic, unknown
• Ocular disease• Large abrasion• HSV, HZV• Primary disease in young
patients
• Systemic disease• JRA – pauciarticular disease• Ankylosing spondylitis
• Symptoms• Extreme photophobia
• Reduced vision
• Signs• Miosis• Red eye to limbus• Flare with cell
• Treatment• Cycloplegia• Topical steroids
REFER

Acute iritis Acute iritis
• Light sensitivity • Deep dull ache • Smaller/ irregular
pupil• Often idiopathic

Angle Closure GlaucomaAngle Closure Glaucoma
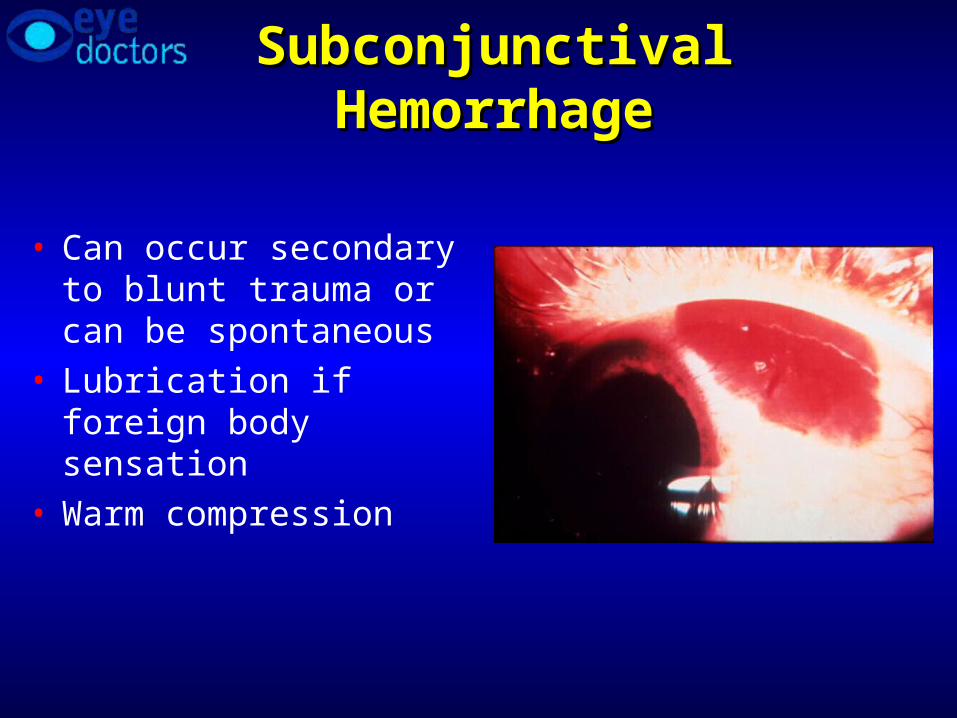
Subconjunctival HemorrhageSubconjunctival Hemorrhage
• Can occur secondary to blunt trauma or can be spontaneous
• Lubrication if foreign body sensation
• Warm compression

Corneal AbrasionCorneal Abrasion
• Management• Non-contact lens wearer
• Antibiotic ointment and patch
• Follow-up one day
• Contact lens wearer• DO NOT PATCH• Antibiotic ointment or
drops• Follow up daily until
healed• Treat abrasions
created with organic material in this manner

Corneal UlcerCorneal Ulcer
• Risk of corneal ulcer when epithelium compromised, especially in contact lens wearers• Contact lens wearers
have a higher rate of colonization with Pseudomonas

Abrasion versus UlcerAbrasion versus Ulcer
Abrasion Ulcer
Fluorescein Stain Stain
Transparency Transparent Opaque
Corneal contour Unchanged Uneven
Level Epithelial only Involves stroma

Superficial Corneal Foreign BodySuperficial Corneal Foreign Body• Removed under
topical anesthetic• With burr or 25
gauge needle
• Manage same as corneal erosion
• Encourage safety glasses• Polycarbonate
lenses

Anterior SegmentAnterior Segment
• Linear epithelial defects is suggestive of a foreign body under the eye lid

Ultraviolet Radiation(arc eye)Ultraviolet Radiation(arc eye)
• Sources• Sunlamps, welding
arcs
• Management• Cycloplegics, antibiotic
ointment, patch
• Avoid long term topical anaethetic drop !!!
Chemical InjuryChemical Injury
• Acid precipitates quickly• Alkali continues to penetrate
• Therefore can progress over an extended period of time
• Management• Continuous irrigation with saline until neutral pH
• Test fornices with Litmus paper
• Sweep fornices to remove retain debris• Antibiotic ointment, cycloplegics

Chemical InjuryChemical Injury
Thorough irrigation before referral !!!

Blunt TraumaBlunt Trauma
• Hyphema• Indicates damage to
angle and/or to the iris
• Management• Vertical position• No anti-coagulants• Cycloplegics

Blunt TraumaBlunt Trauma
• Damage to Iris and Lens• Iridodialysis, cataract• Dislocation

Blunt Trauma - SequelaeBlunt Trauma - Sequelae
• Angle damage which can lead to glaucoma: can develop days to years after injury

Blunt Trauma - SequelaeBlunt Trauma - Sequelae
• A retinal tear which can progress to a retinal detachment

Open Globe InjuriesOpen Globe Injuries
• Blunt trauma – rupture
• Sharp trauma – laceration
• Projectile trauma• Penetrating – in and out• Perforating ± intra ocular foreign body –
just in
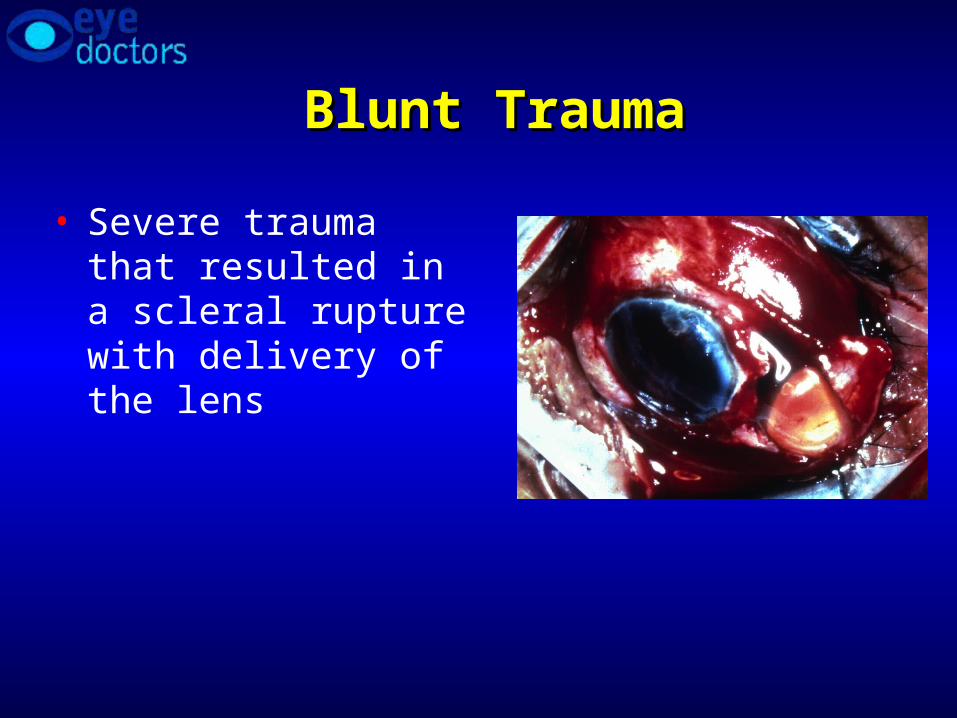
Blunt TraumaBlunt Trauma
• Severe trauma that resulted in a scleral rupture with delivery of the lens

Sharp TraumaSharp Trauma
• Corneal laceration and traumatic cataract from a thrown beer bottle

Penetrating Eye InjuriesPenetrating Eye Injuries
• Intraocular foreign bodies generally have to be removed, unlike orbital (extraocular) foreign bodies
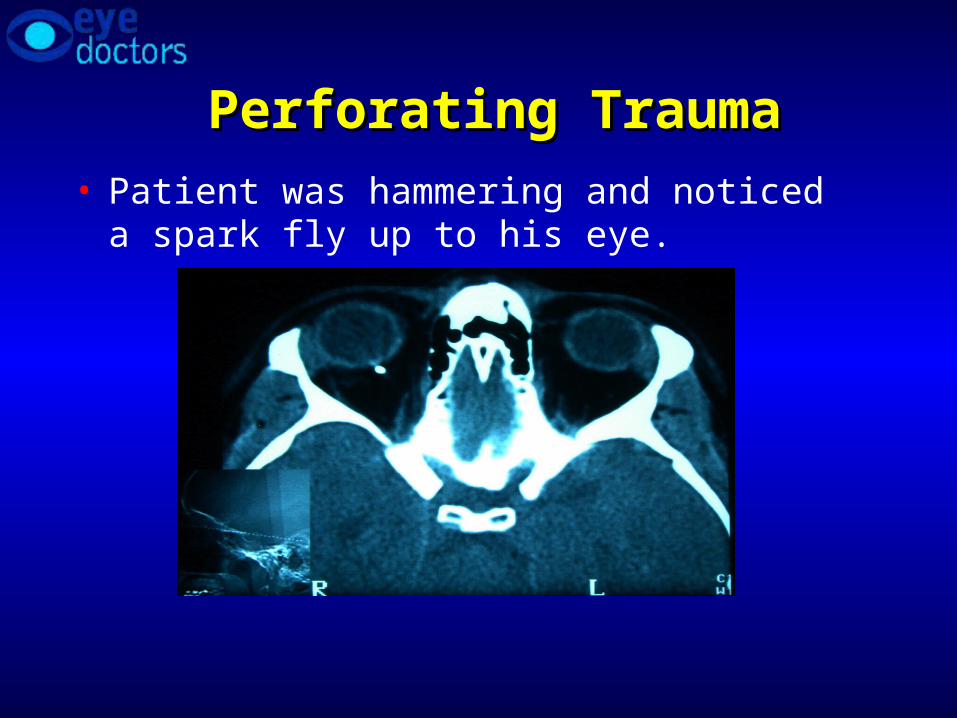
Perforating TraumaPerforating Trauma
• Patient was hammering and noticed a spark fly up to his eye.

Child with poor red reflexChild with poor red reflex
