how do we re-tool ontario’s health care system for chronic disease management and prevention? inet...
TRANSCRIPT
How do we Re-tool Ontario’s Health Care System for
Chronic Disease Management and Prevention?
INET International
Michael M. Rachlis MD MSc FRCPC
www.michaelrachlis.com
Toronto June 20, 2007

Outline• Chronic disease has a major impact on our
health and health system
• Our health system doesn’t deal with chronic diseases very well
• Some examples of chronic disease management excellence
• How will Ontario’s health reforms affect chronic disease management and prevention
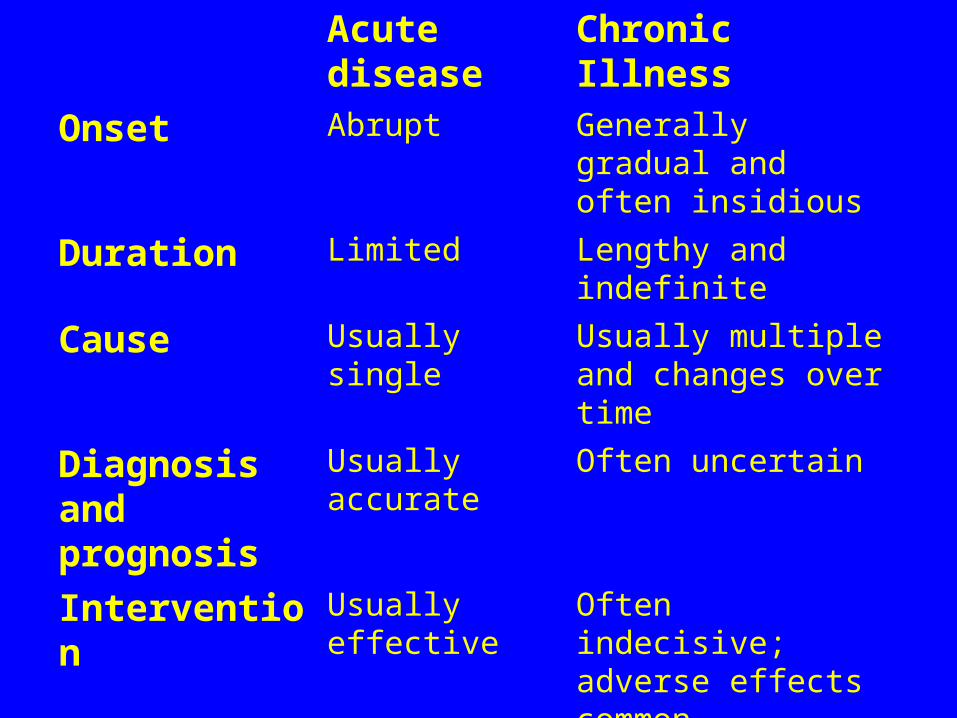
Acute disease Chronic Illness
Onset Abrupt Generally gradual and often insidious
Duration Limited Lengthy and indefinite
Cause Usually single Usually multiple and changes over time
Diagnosis and prognosis
Usually accurate Often uncertain
Intervention Usually effective Often indecisive; adverse effects common
Outcome Cure possible No cure
Uncertainty Minimal Pervasive
Knowledge Prof’s know Patients don’t
Prof’s and patients have complementary knowledge

Chronic disease has a major impact on our health and health system
• Chronic diseases account for 70% of all deaths.
• Chronic diseases account for more than 60% of health care costs.
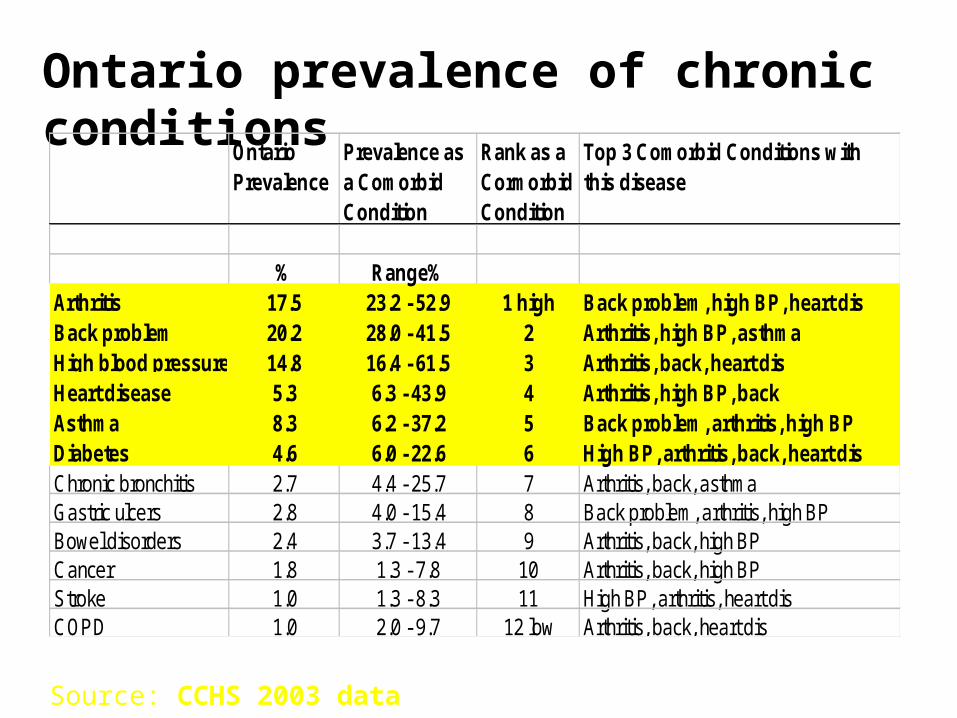
Ontario prevalence of chronic conditions
Ontario Prevalence
Prevalence as a Comorbid Condition
Rank as a Cormorbid Condition
Top 3 Comorbid Conditions with this disease
% Range%Arthritis 17.5 23.2 - 52.9 1 high Back problem, high BP, heart disBack problem 20.2 28.0 - 41.5 2 Arthritis, high BP, asthmaHigh blood pressure 14.8 16.4 - 61.5 3 Arthritis, back, heart disHeart disease 5.3 6.3 - 43.9 4 Arthritis, high BP, backAsthma 8.3 6.2 - 37.2 5 Back problem, arthritis, high BPDiabetes 4.6 6.0 - 22.6 6 High BP, arthritis, back, heart disChronic bronchitis 2.7 4.4 - 25.7 7 Arthritis, back, asthmaGastric ulcers 2.8 4.0 - 15.4 8 Back problem, arthritis, high BPBowel disorders 2.4 3.7 - 13.4 9 Arthritis, back, high BPCancer 1.8 1.3 - 7.8 10 Arthritis, back, high BPStroke 1.0 1.3 - 8.3 11 High BP, arthritis, heart disCOPD 1.0 2.0 - 9.7 12 low Arthritis, back, heart dis
Source: CCHS 2003 data

Ontarians with chronic conditions
Source: CCHS 2000/01
Number of Chronic Conditions
Popn12+
Selected Health-Related Problems/Needs None 1 2 3+
Ontarians reporting chronic conditions (millions) 3.4 2.6 1.7 2.1
% % % %
Consulted an MD in past 12 months 73 83 90 95 83
Number of MD visits in past 12 months 2 4 5 9
Overnight Patient in past 12 months 3 7 8 14 7
Activities limited due to a health problem 5 16 30 55 23
One or more disability days in past two weeks 9 14 18 30 16
Pain prevents a few, some or most activities 2 6 15 34 12
Moderate or Severe Pain or Discomfort 2 6 13 31 11
Self-perceived unmet health care needs 7 11 14 20 12

Chronic diseases: Common Risk Factors
• The Social Determinants of Health, especially work and life strain
• Unhealthy behaviours– Smoking, other drugs
– Diet
– Physical Exercise

Disparities in health between different groups are responsible for 20% of health care costs
Health Disparities Task Group of the Federal Provincial Territorial Advisory Committee on Population Health and
Health Security. Health Disparities: Roles of the Health Sector. 2004.
http://www.phac-aspc.gc.ca/ph-sp/disparities/pdf06/disparities_discussion_paper_e.pdf
Outline• Chronic disease has a major impact on our
health and health system
• Our health system doesn’t deal with chronic diseases very well
• Some examples of chronic disease management excellence
• How will Ontario’s health reforms affect chronic disease management and prevention
Evidence of Ontario’s performance in Chronic Care
• Fewer than 60% of Ontarians with diabetes have had a HgbA1c within the past year.
• Only 50% of Ontarians with diabetes have an eye examination within one year of diagnosis.
• 1 in 7 Ontario patients newly diagnosed with heart failure are re-admitted to hospital within 90 days of discharge and nearly one-quarter are re-admitted within one year.

Evidence of Canada’s performance in Chronic Care
• Nearly 60% of Canadians with asthma had an uncontrolled outbreak in the previous year
• 59% of Canadians who were depressed in the previous year did not receive mental health services despite over 90% having seen a family doctor
• A study in Ottawa reported that one in six seniors was re-admitted to hospital within 30 days of discharge

If you can’t measure it, you can’t manage it: Registries are
fundamental for chronic disease management and few Ontario doctors have them.

Canadian MDs don’t have registries
Percent reporting very difficult or cannot generate
14
43
10 7 61
33
0
25
50
75
AUS CAN GER NETH NZ UK US
Source: Schoen 2006

Canadian MDs don’t give care plans
Percent giving written plan
2914
63
2518 21
33
0
25
50
75
100
Source: Schoen 2006
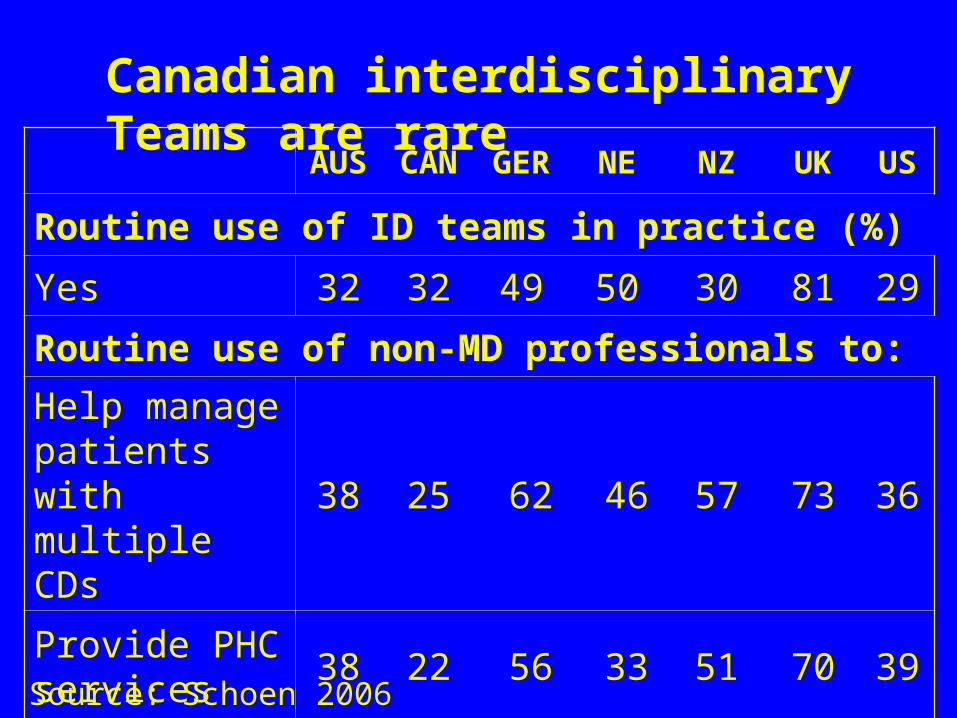
Canadian interdisciplinary Teams are rare
AUS CAN GER NE NZ UK US
Routine use of ID teams in practice (%)
Yes 32 32 49 50 30 81 29
Routine use of non-MD professionals to:
Help manage patients with multiple CDs
38 25 62 46 57 73 36
Provide PHC services
38 22 56 33 51 70 39
Source: Schoen 2006
We could prevent most chronic diseases
• > 80% of ischemic heart disease, lung cancer, chronic lung disease, and diabetes cases could be prevented with what we know
• This would free up over 2900 acute hospital beds Ontario

Each System is Perfectly Designed to get the Results it
Achieves.
We designed our health system to manage acute illnesses, not manage (much less prevent)
chronic ones.

Commonwealth Fund Rankings
AUS CA DEU NZ UK USOverall Rank 2007 3.5 5 2 3.5 1 6
Quality of Care 4 6 2.5 2.5 1 5
Right care 5 6 3 4 2 1
Safe care 4 5 1 3 2 6
Coordinated care 3 6 4 2 1 5
Patient-centered care 3 6 2 1 4 5
Access 3 5 1 2 4 6
Efficiency 4 5 3 2 1 6
Equity 2 5 4 3 1 6
Healthy Lives 1 3 2 4.5 4.5 6
US$/Capita (PPP) $2876 $3165 $3005 $2083 $2546 $6102
K. Davis et al Commonwealth Fund pub no 1027 May 2007
High Med Low

Trying to deliver health services without adequate primary health care is like pulling
your goalie in the first period!

Outline• Chronic disease has a major impact on our
health and health system
• Our health system doesn’t deal with chronic diseases very well
• Some examples of chronic disease management excellence
• How will Ontario’s health reforms affect chronic disease management and prevention

Informed,ActivatedPatient and Family
Productive InteractionsPrepared,ProactivePracticeTeam
DeliverySystemDesign
DecisionSupport
ClinicalInformation
SystemsSelf-
Management Support
Health SystemResources and Policies
CommunityHealth Care Organization
Chronic Care Model
Improved Outcomes
http://www.improvingchroniccare.org
Patient-centredTimely
Efficient
CoordinatedSafe
Evidence-based

INDIVIDUALS AND FAMILIES
Improved clinical, functionaland population health outcomes
HEALTH CAREORGANIZATIONS
Informed, activatedindividuals & families
Prepared, proactivepracticeteams
Activated communities &
prepared, proactivecommunity
partners
HealthyPublicPolicy
SupportiveEnvironments
CommunityAction
DeliverySystemDesign
ProviderDecisionSupport
InformationSystems
Ontario’s CDPM Framework
Productive interactions and relationships
PersonalSkills & Self-Management
Support

Assessing your Readiness for Chonic Disease careAssessment of Chronic Illness Care (ACIC) Version 3.5Http://www.improvingchroniccare.org/ACIC%20docs/ACIC_V3.5.doc
Assessment of Chronic Illness Care
• Health care organization • Community linkages• Self management support• Decision support• Delivery system design• Clinical information systems• Integration of Chronic Care Model Components• Prevention• Public Policy

Organization of the Health Care System: Think of the US Veteran’s Health Services
• Replaced 173 autonomous hospitals with 22 integrated regional networks .
• Decreased hospital utilization by 62%• Increased overall number of patients by 18%• Increased ambulatory visits by 35% • Decreased costs by 18%• Increased colorectal cancer screening from
34% to 74%• 93% of diabetics have had a recent HgbA1C,
70% have had a recent foot exam• Discontinued 72% of forms

Veterans Administration bibliography
Armstrong B, Levesque O, Perlin JB, et al. Reinventing Veteran’s Health Administration: Focus on Primary Care. Journal of Healthcare Management. 2005;50(6):399-408.
Arnst C. The best medical care in the US: How Veterans Affairs transformed itself and what it means for the rest of us. Business Week Online. June 2006. Found at: www.businessweek.com/print/magazine/content/06_29/b3993061.htm?chan=gl. Accessed November 7, 2006.
Asch SM, EA, Hogan MM, et al. Comparison of quality of care for patients in the Veterans Health Administration and Patients in a National Sample. Annals of Internal Medicine. 2004;141:938-945.

Community Linkages: Think of the London InterCommunity Health Centre Latin American Diabetes Program
• Adult Saturday screening program• IGT intensive risk management and prevention
program• Children’s diabetes risk assessment program• Children’s intensive risk management program• Diabetes complication prevention program• Diabetes specialist satellite clinic.

London InterCommunity Health Centre Latin American Diabetes Program
• Multiple entry points, Flexible hours• Multi-lingual, culturally appropriate care
– Community health workers– International health professionals
• Integrated with primary health care– Dietician, Foot Nurse, Nurse Practitioner, Social
Worker
• Self-management support• IT support
Self-management support: Think of the McMaster Stonechurch Family Health Centre rehab project
• Patients > 45 with chronic illness and > 4 visits to the practice during the previous year
• Assessed by an OT and PT
• Individual care programs integrated goals for exercise, nutrition, and stress management into their care plans
• After 2 years, the rehabilitation patients had fewer falls and their caregivers reported less stress. Rehab patient used ~ $450 less hospital care

Decision Support: Think of the Hamilton Shared Care mental health project
• The Hamilton HSO Mental Health Program increased access for mental health patients by 1100% while decreasing referrals to the psychiatry outpatients’ clinic by 70%.– 145 MDs, 85 mental health counsellors, 17
psychiatrists, 340,000 patients
Delivery System design: Think of the Sault Ste Marie Group Health Centre
• 30 family doctors
• 30 specialists
• 120 nurses
• 50 other professionals
• Electronic records

Clinical Information Systems: Think of the Sault and OSCAR (www.oscarmcmaster.ca)
• Registries
• Reminders to providers
• Feedback
• Information about relevant subgroups of patients needing services
• Patient treatment plans

Prevention: Think of Kahnewake and Sandy Lake
• Community-based action• Community-based research• Healthy Public Policy
– Walking trails– Healthy food

Public Policy: Think of Cigarette Smoking and seat belts
• Thousands of Canadians won’t die this year because smoking rates are less than one-half what they were in 1970
• Thousands of Canadians will avoid lifelong disability and chronic pain because of seat belt laws

Outline• Chronic disease has a major impact on our
health and health system
• Our health system doesn’t deal with chronic diseases very well
• Some examples of chronic disease management excellence
• How will Ontario’s health reforms affect chronic disease management and prevention
Ontario 2007• The government made its own fiscal box
• A first ever Ministry Strategic Plan
• Local Health Integration Networks
• Family Health Teams, CHCs, and primary health care reform
• Chronic disease management
• Wait list management

Ontario 2007• New CCAC boundaries
• Health Human Resources
• Public Health Reform
• Ontario Health Quality Council (ohqc.ca)
• The Social Determinants of Health
• Take a breath!

LHINs 2007

LHINs: Ontario’s Bold Step Forward?
• With integrated models, the devil is in the details. What are the details?
• The LHINs are due to get $ authority but will the Ministry let them have it?
• Future of CCACs and hospitals? CHCs?• Will the LHINs put ALL services out to
tender?• How will the LHINs be funded? History?
Population? Needs?
LHINs: Ontario’s Bold Step Forward?
• Relationships with physicians?
• Relationships with public health?
• Relationships with family health teams?
• Will there be protected budgets for services to vulnerable groups?
• Labour transition strategy?
Primary health care reform
• Will the family health teams be able to achieve excellence in care?– The funding encourages and discourages care
for chronic disease
• Will the province use the network of > 70 community health centres to stimulate innovation in service design
• The use electronic systems?

Facilitating Solutions
• Fully integrated funding• True primary health care reform• Electronic health records• ↑↑↑ resources for training for staff and
boards• Integrated planning for prevention by Public
Health, LHINs, FHTS, CCACs, CHCs et al• Provincial government strategy for health
care AND health

Attributes of High Performing Health Systems Ontario Health Quality Council. April 2006. (www.ohqc.ca)
1. Safe2. Effective3. Patient-Centred4. Accessible5. Efficient6. Equitable7. Integrated8. Appropriately resourced9. Focused on Population Health

Summary:• Chronic disease has a major impact on
Ontario’s health and health system
• Ontario deals poorly with chronic diseases
• There are examples of Ontario chronic disease excellence but spread is hard
• We need to change the way we deliver care
• The Ontario CDMP Framework and Ontario Health Quality Council's Attributes for a high performing heath system can help us plan

“Courage my Friends, ‘Tis Not Too Late to Make a Better World!”
Tommy Douglas
(per Tennyson)