hospitalist/internal medicine/family practice
TRANSCRIPT

1 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Hospitalist/Internal Medicine/Family Practice
INSTEAD OF PLEASE CONSIDER
Low or No Severity Diagnosis—NO
High Severity Diagnosis---YES
ICD 10 Themes: e.g. Acute on Chronic Systolic Heart Failure
Acuity/Severity/Type/Staging
Acute/Chronic/Acute on Chronic
Mild, Moderate, Severe
Systolic, Diastolic, Combined
Stage I, II, III, IV
e.g. Malignant neoplasm of lower lobe right bronchus
Anatomy/Site Specificity
Location of tumor
Bone/Joint/Muscle involved
e.g. Decubitus Ulcer, Stage 3, Right Buttocks, Present on Admission
Laterality
Right/Left/Bilateral/Overlapping (see Neoplasm re overlaps two or more contiguous (next to each other) sites)
e.g. Hypertensive heart disease with chronic systolic heart failure
Manifestations – LINK IT!
Associated or Related Conditions
‘With’/‘Secondary’ to/’Due to’
‘Evidence of’ and causative organism
Use ‘no organism isolated’, instead of ‘negative culture’
e.g. Likely Sepsis secondary to UTI; Evidence of Bacterial Pneumonia (‘Evidence of’ in outpt setting can be captured as a diagnosis)
Etiology – ‘DUE TO’ WhAt?
‘LIKELY’ suspects….Who dun it?
Possible, Probable, Suspected (Inpt Only)
Evidence of, As Evidenced by (Outpt Setting and Inpt Setting)
e.g. Drug Poisoning/Adverse Effect Episode of Care/Incidence of Encounter (Trauma/Fractures/Medication.Chemical Event(Drug Poisoning))
Initial/Subsequent/Sequela
Top Diagnosis Codes by Specialty:
Pneumonia Type: Healthcare Associated/Aspiration/Ventilator Associated/Radiation Induced
CAUTION: CAP-Community Acquired PNA- defaults to a ‘simple pna’ with low severity; if documented, please also include if it is Viral or Bacterial (and other items listed from list on right, as applicable) to capture the true severity.
Causative Agent: Viral or Bacterial
Causative Organism (if known)
Associated Illnesses: influenza/ lung abscess/Sepsis

2 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Common Secondary Conditions: Acute Respiratory Failure; Exacerbation of COPD, etc.
Clinically significant diagnostic results from Lab and Radiology in the medical record. i.e. if elevated white count; infiltrate on CXR
History of Tobacco Use, Present or Past
COPD Acute Exacerbation or Decompensated
(Chronic RF is very common in pt with severe COPD) CAUTION: ‘Respiratory Distress’ and ‘Respiratory Insufficiency’ are vague and symptomatic of underlying condition – is the intended diagnosis Respiratory Failure OR what is other underlying condition?
If with acute lower respiratory infection, as applicable (also include causative organism, if known)
IF Oxygen Dependent
Common Secondary Conditions: Acute, Chronic, Acute on Chronic Respiratory Failure; Pneumonia, etc.
History of Tobacco Use, Present or Past
Respiratory Failure Acuity: Acute/Chronic/Acute on Chronic
(Chronic RF is very common in pt with severe COPD) CAUTION: ‘Respiratory Distress’ and ‘Respiratory Insufficiency’ are vague and symptomatic of underlying condition – is the intended diagnosis Respiratory Failure OR what is other underlying condition?
Manifestation: With Hypoxia or With Hypercapnia, or both
Etiology: if known (i.e. due to COPD Exacerbation; Pneumonia; Surgery, Trauma, etc)
Pleural Effusion Type: Malignant (Specify site and morphology of tumor if possible); Influenzal; Tuberculosis; In heart failure
Pancreatitis Acuity: Acute vs. Chronic
Etiology/Cause and Effect: Idiopathic, Biliary, Alcohol induced, Drug Induced, Other
Urinary Tract Infection Acuity: Acute or Chronic
e.g. ‘Chronic Cystitis with hematuria’; ‘Acute Urethritis due to E.Coli’; ‘Acute on Chronic Pyelonephritis due to foley catheter with Candida’
Specific Site: Bladder (Cystitis)/Urethra (Urethritis)/Kidney (Pyelonephritis)
Manifestations: Hematuria etc.
Causative Organism i.e. E Coli or Candida
IF related to a device i.e. foley catheter, state ‘due to’ or ‘secondary to’

3 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Sepsis Type: Sepsis/Severe Sepsis/Septic Shock
(fyi: negative or inconclusive blood cultures do not preclude a diagnosis of sepsis in patients with clinical evidence of the condition)
Causative Organism (if known)
(fyi: Bacteremia is a non specific diagnosis and indicates the presence of bacteria in the blood, but does not indicate the bacteria are pathological or has any resulting systemic illness needing treatment.)
Underlying Systemic Infection (the source of infection) i.e. Sepsis due to UTI
(fyi: Urosepsis is non descriptive term and is NOT synonymous with sepsis and there is no default for coders…please .use ‘Sepsis due to UTI’ instead) (fyi: Sepsis Syndrome is a non specific term..avoid using it)
Any Associated Organ Dysfunction i.e. Acute Renal Failure; Acute Respiratory Failure; Encephalopathy
SIRS Infectious or Non-infectious (If ‘non-infectious’ specify what ‘due to’, i.e. ‘SIRS due to Burn’)—These DONOT code to Sepsis unless Sepsis specifically stated.
Always document the Etiology!! With severe Sepsis or Without Sepsis
With or Without Organ Dysfunction
‘SIRS’ Does NOT code to Sepsis, unless stated ‘with sepsis’)
Defaults to the underlying infectious process i.e. Pneumonia
Atrial Fibrillation Type: Paroxysmal/Persistent/Chronic
CVA/Cerebral Infarction Etiology: Thrombus or Embolism
When you don’t specify side affected as dominant or nondominant: Rt Side defaults to dominant/Lt side defaults to nondominant
Artery Site: Precerebral – Vertebral, basilar, carotid, or other Cerebral – Middle, anterior, or posterior Cerebellar arteries
Laterality, When Appropriate
Dominant or Non-Dominant Side Affected
Associated Conditions i.e. aphasia, hemiplegia, dysphasia
Diverticulitis Location: Small, Large or Both Intestines
With or Without Bleeding
With or Without Perforation/Abscess
Diabetes Type: Type 1 or Type 2 ; Drug or Chemical Induced; or Gestational
Terms i.e. ‘uncontrolled’ or ‘inadequately controlled’ code to ‘hyperglycemia’…even if recent ‘hypoglycemia’…..specifically use Hypoglycemia or
Control Status (Insulin):
With: Hypoglycemia/Hyperglycemia
4 | P a g e R e v . 9 . 2 9 . 2 0 1 5
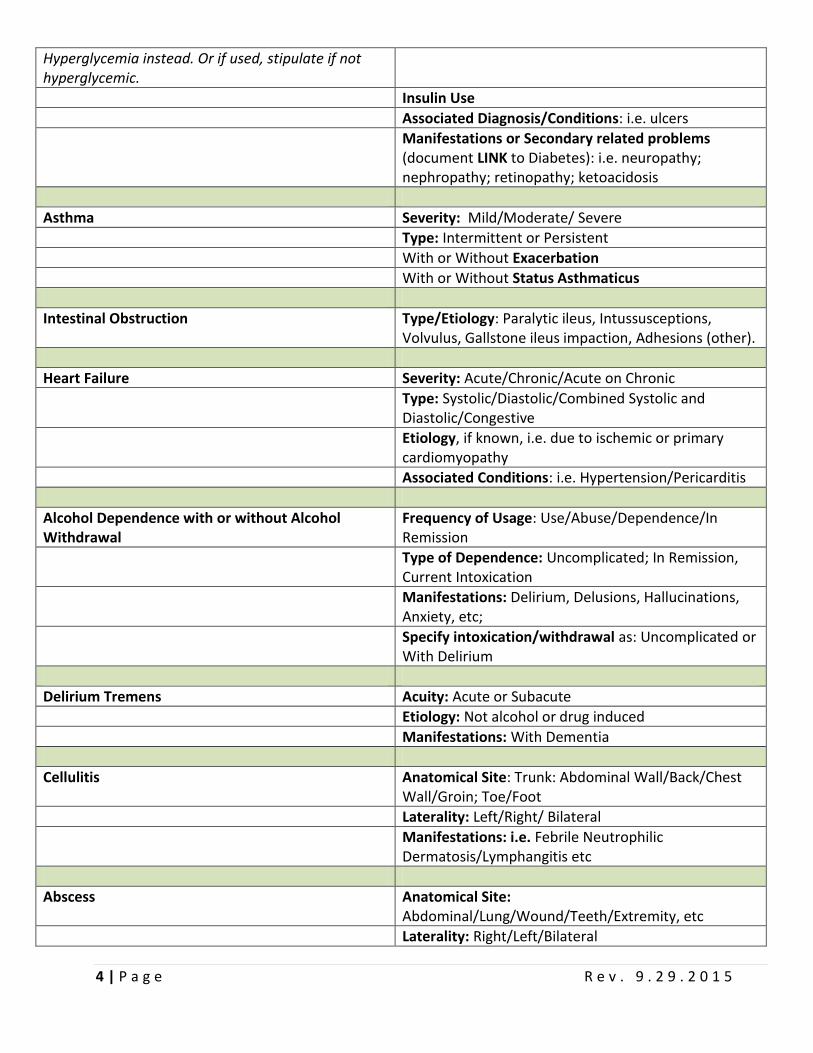
Hyperglycemia instead. Or if used, stipulate if not hyperglycemic.
Insulin Use
Associated Diagnosis/Conditions: i.e. ulcers
Manifestations or Secondary related problems (document LINK to Diabetes): i.e. neuropathy; nephropathy; retinopathy; ketoacidosis
Asthma Severity: Mild/Moderate/ Severe
Type: Intermittent or Persistent
With or Without Exacerbation
With or Without Status Asthmaticus
Intestinal Obstruction Type/Etiology: Paralytic ileus, Intussusceptions, Volvulus, Gallstone ileus impaction, Adhesions (other).
Heart Failure Severity: Acute/Chronic/Acute on Chronic
Type: Systolic/Diastolic/Combined Systolic and Diastolic/Congestive
Etiology, if known, i.e. due to ischemic or primary cardiomyopathy
Associated Conditions: i.e. Hypertension/Pericarditis
Alcohol Dependence with or without Alcohol Withdrawal
Frequency of Usage: Use/Abuse/Dependence/In Remission
Type of Dependence: Uncomplicated; In Remission, Current Intoxication
Manifestations: Delirium, Delusions, Hallucinations, Anxiety, etc;
Specify intoxication/withdrawal as: Uncomplicated or With Delirium
Delirium Tremens Acuity: Acute or Subacute
Etiology: Not alcohol or drug induced
Manifestations: With Dementia
Cellulitis Anatomical Site: Trunk: Abdominal Wall/Back/Chest Wall/Groin; Toe/Foot
Laterality: Left/Right/ Bilateral
Manifestations: i.e. Febrile Neutrophilic Dermatosis/Lymphangitis etc
Abscess Anatomical Site: Abdominal/Lung/Wound/Teeth/Extremity, etc
Laterality: Right/Left/Bilateral

5 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Manifestations: i.e. Febrile Neutrophilic Dermatosis/Lymphangitis
Causative Agent: Viral or Bacterial
Causative Organism (if known)
Episode of Care: Initial/Subsequent/Sequela (if ‘Wound’ related)
Pathological Fracture/Fragility Fracture (fyi: any ground level fall of 50 yr old or greater is usually a pathological fracture) -When the fracture is out of proportion to the degree of the trauma (weakening of the bone structure by pathologic processes i.e. Osteoporosis)
Site and Laterality Etiology:
Age related
Osteoporosis or Osteopenia
Neoplastic
Some other disease Episode of Care: Initial/Subsequent/Sequela For Subsequent: Routine or Delayed Healing; Non union or Malunion Current Fracture and/or personal history
Traumatic Fractures (Fracture Tib/Fib, Femur, Hip) Location: Specific Part of Body - Name of specific bone and specific site on bone
Laterality: Right/Left/Bilateral
LEO C. FAUR
(acronym to remember elements of fracture documentation)
Zupko and Associates
Episode of Care:
Initial (receiving active treatment);
Subsequent (encounters AFTER the patient
has received active treatment of the condition
and is receiving routine care):
o Routine Healing or Delayed Healing
o Non-Union or Mal-union:
If non union: State if delayed
Tx, (it’s Initial Encounter,
otherwise it’s ‘Subsequent’)
Sequela (Use for complications or conditions
that arise as a direct result of a condition…no
time limit….i.e. Neuropathy of lower leg, ankle
and foot due to previous crush injury
Open or Closed
Classifications: Open use Gustilo Classification: Type I, II, IIIA, IIIB, or IIIC (used for soft tissue classification); Salter; Physeal etc

6 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Fracture Pattern/Type/Orientation, i.e.:
Greenstick Comminuted Torus
Spiral Segmental
Transverse Avulsed
Oblique Torus
Alignment: Displaced or Nondisplaced
Underlying Bone Diseases: i.e. Fragility (Pathologic), Stress, Traumatic in healthy etc
Results: Routine or Delayed Healing; Non union or Malunion
Pulmonary Embolism Severity: Acute/Chronic (still present) vs. Healed (Old)
Type: Saddle/Septic
Manifestations: With or Without Acute Cor Pulmonale
DVT Acuity: Acute or Chronic
Laterality: Right/Left/Bilateral
Dementia Etiology: Alzheimers/with Lewy Bodies/Epilepsy/Hypercalcemia/Parkinson’s Disease
Manifestations: With behavioral disturbance or Without Behavioral disturbance
Cholecystitis with or without Cholelithiasis Acuity: Acute/Chronic/Acute on Chronic
Location: Gallbladder/Bile Duct/Gallbladder & Bile Duct
With Obstruction/Without Obstruction
Atrial Flutter Type: Typical (Type 1) or Atypical (Type 2)
Obesity BMI 19 or less = Indicates Malnutrition
BMI 25 – 29.9 = Overweight
(BMI can be taken from Nursing Documentation; MD needs to document the diagnosis and etiology/manifestation correlating to BMI)
BMI 30.0 – 39.9 = Obesity
BMI ≥ 40 = Morbid Obesity (state Etiology: Excess Calories ; Other and Manifestation: Alveolar Hypoventilation, as applicable)
Etiology: Excess Calories (for Morbid Obesity); Drug Induced; Endocrine; Familial; Constitutional; etc
Manifestation: Alveolar Hypoventilation (for Morbid Obesity)
7 | P a g e R e v . 9 . 2 9 . 2 0 1 5
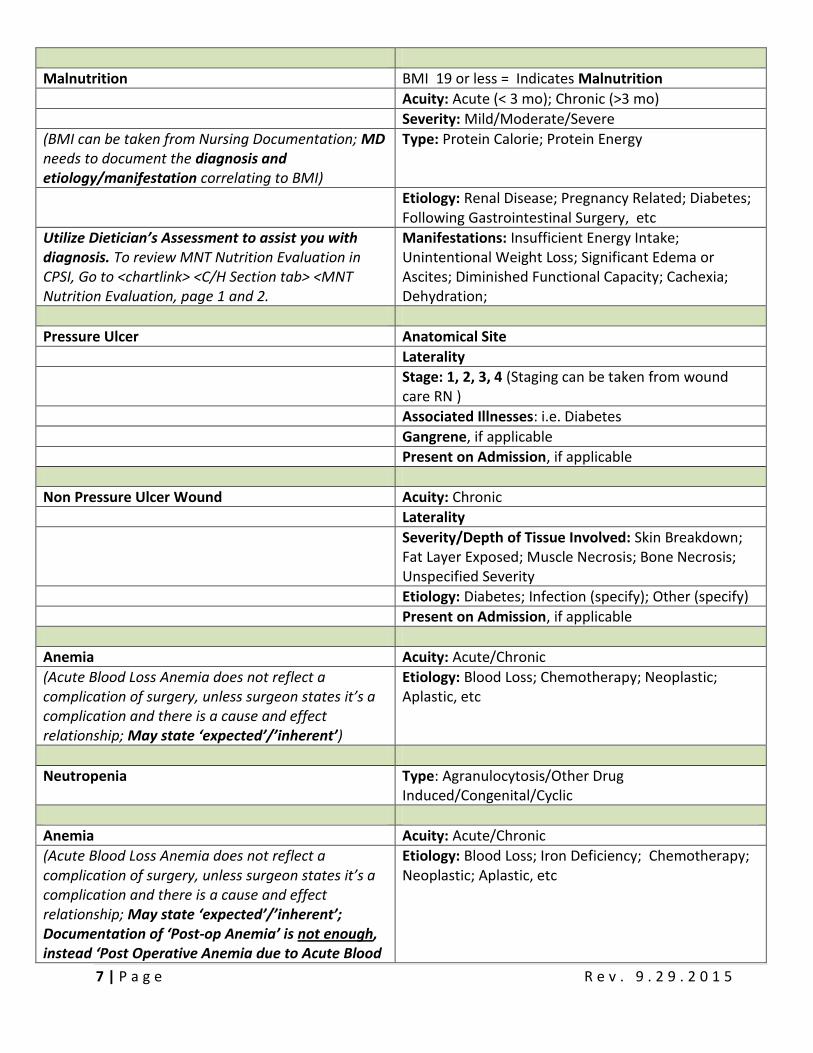
Malnutrition BMI 19 or less = Indicates Malnutrition
Acuity: Acute (< 3 mo); Chronic (>3 mo)
Severity: Mild/Moderate/Severe
(BMI can be taken from Nursing Documentation; MD needs to document the diagnosis and etiology/manifestation correlating to BMI)
Type: Protein Calorie; Protein Energy
Etiology: Renal Disease; Pregnancy Related; Diabetes; Following Gastrointestinal Surgery, etc
Utilize Dietician’s Assessment to assist you with diagnosis. To review MNT Nutrition Evaluation in CPSI, Go to <chartlink> <C/H Section tab> <MNT Nutrition Evaluation, page 1 and 2.
Manifestations: Insufficient Energy Intake; Unintentional Weight Loss; Significant Edema or Ascites; Diminished Functional Capacity; Cachexia; Dehydration;
Pressure Ulcer Anatomical Site
Laterality
Stage: 1, 2, 3, 4 (Staging can be taken from wound care RN )
Associated Illnesses: i.e. Diabetes
Gangrene, if applicable
Present on Admission, if applicable
Non Pressure Ulcer Wound Acuity: Chronic
Laterality
Severity/Depth of Tissue Involved: Skin Breakdown; Fat Layer Exposed; Muscle Necrosis; Bone Necrosis; Unspecified Severity
Etiology: Diabetes; Infection (specify); Other (specify)
Present on Admission, if applicable
Anemia Acuity: Acute/Chronic
(Acute Blood Loss Anemia does not reflect a complication of surgery, unless surgeon states it’s a complication and there is a cause and effect relationship; May state ‘expected’/’inherent’)
Etiology: Blood Loss; Chemotherapy; Neoplastic; Aplastic, etc
Neutropenia Type: Agranulocytosis/Other Drug Induced/Congenital/Cyclic
Anemia Acuity: Acute/Chronic
(Acute Blood Loss Anemia does not reflect a complication of surgery, unless surgeon states it’s a complication and there is a cause and effect relationship; May state ‘expected’/’inherent’; Documentation of ‘Post-op Anemia’ is not enough, instead ‘Post Operative Anemia due to Acute Blood
Etiology: Blood Loss; Iron Deficiency; Chemotherapy; Neoplastic; Aplastic, etc

8 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Loss’)
Nutritional Anemia Type: i.e. if nutritional due to iron deficiency: Sideropenic iron deficiency anemia; Iron deficiency due to inadequate dietary iron intake
Vitamin B12 type i.e. Due to intrinsic factor deficiency; Vitamin B12 malabsorption
Folate Deficiency type: i.e. Due to diet; Drug induced
Other Nutritional Types: i.e. Protein deficiency
Anemia in Chronic Disease Link to Chronic Disease i.e. -Anemia due to chronic kidney disease -Anemia due to colon cancer
Neutropenia Type: Agranulocytosis/Other Drug Induced/Congenital/Cyclic
Etiology: Cancer Chemotherapy/Infection etc.
If Drug-induced: - Specify Drug - Purpose of drug’s use (e.g. chemotherapy) - Specify the malignancy (e.g. Cytoxan for primary
malignancy upper-inner quadrant of left breast
Associated Conditions (e.g. infection)
Adverse Effect (e.g. fever or mucositis)
Thrombocytopenia Classification: -Idiopathic -Primary -Secondary -Congenital or Hereditary -Heparin Induced
Secondary Thrombocytopenia: - Underlying Condition (e.g. alcohol induced)
Specify Hemorrhagic Conditions (e.g. qualitative platelet defects)
Pancytopenia Definition - Anemia (e.g. Hct < 32%); and, - Thrombocytopenia (e.g. PPC < 150K); and, - Neutropenia (e.g. ANC < 1,500)
–
Physician must describe underlying cause and what individual component has been treated
- e.g. Platelets for thrombocytopenia - PRBC transfusion for acute blood loss anemia
Etiology

9 | P a g e R e v . 9 . 2 9 . 2 0 1 5
- Malignancy (Specify Malignancy) - Drug induced (Specify specific drug) - ‘Pancytopenia due to antineoplastic
chemotherapy’ or - ‘Pancytopenia secondary to Cisplatin and
disease’ , Or - ‘Pancytopenia due to HIV disease.’
Pain Acuity: Acute/ Chronic
Anatomic Site: Cervical/Lumbar/Thoracic/Ankle/Elbow/Buttock,etc
Laterality: Right/Left
‘Chronic back pain due to spinal stenosis and difficulty sleeping due to the pain.’
Etiology: i.e. Device, implant, graft; Pyschogenic (list type)
Manifestations: With: Myelopathy; Radiculopathy; Neuritis; Radiculitis; etc
Episode of Care/Incidence of Encounter: Initial/Subsequent/Sequela
Kidney Failure Note: Re Chronic: ‘insufficiency’ and no ‘stage’ codes to ‘unspecified’ code and does not reflect the severity of the patient
Acuity: Acute/Chronic/Acute on Chronic If Chronic:
Stage 1 (GFR ≥ 90) – Kidney Damage with normal or ↑ GFR
Stage 2 (mild) (GFR 60 – 90) + Kidney Damage
Stage 3 (moderate) (GFR 30-59)
Stage 4 (severe) (GFR 15-29)
Stage 5 (GFR ‹ 15)
End Stage Renal Disease Above per KDIGO 2012 Clinical Practice Guidelines
Re Acute: ‘insufficiency’ and ‘kidney disease’ do not report ‘failure, acute renal’
If Acute: due to traumatic injury or non trauma event
Manifestations: With-Acute Tubular Necrosis (ATN)/Acute Cortical Necrosis/Medullary Necrosis
Etiology: Pre-renal AKI/ ATN/Post-Renal Obstructive AKI/Diabetic/Hypertensive
Hypotension Etiology: Postural; Orthostatic (chronic); Neurogenic (Orthostatic); Postoperative; Drug-induced; Cardiogenic; Idiopathic; etc
Atelectasis Etiology: i.e. Morbid Obesity/Pleural Effusion/Malignancy etc
Associated Conditions: i.e. Apnea
Present on Admission, if applicable

10 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Alzheimers Type: Early Onset (presenile dementia); Late Onset (senile dementia)
“Early onset Alzheimers with dementia. Pt wandered into snow with bathing suit on and sustained a hand laceration of unknown mechanism”—link it.
Manifestations: With ‘Behavioral’ Disturbances (i.e. Aggressive; Combative; Violent, Wandering); With ‘Mind’ Disturbances (i.e. Dementia/Delirium)
- Dementia with Wandering
-With Associated Delirium
Osteomyelitis Acuity: Acute/Subacute/Chronic
Anatomic Site: Body part (i.e. thigh); Specific bone (i.e. femur); Joint (i.e. shoulder)
Laterality: Right/Left/Bilateral
Causative Agent: Viral or Bacterial
Causative Organism (if known)
Etiology/’Due to’: i.e. Acute osteomyelitis, left humerus, ‘due to’ infect hip
Complications: Abscess/Amputation/Avascular necrosis/Gangrene/Meningitis etc.
Acute Myocardial Infarction (AMI) Indicate exact date of initial MI, if unavailable, report in weeks, NOT months.
Acuity: Acute; Subsequent (Acute MI occurring within 28 days (4 weeks) of previous acute MI, regardless of site; Old (> 28 days of current encounter)
Type: STEMI/NSTEMI
Anatomical Site: For STEMI: Wall involved; also include artery involved; NSTEMI – no add’l documentation needed
Neoplasm Type: Malignant (Primary; Secondary/Metastatic); Benign; In-Situ; Uncertain Behavior (include cell type) (Uncertain behavior is a specific pathologic diagnosis indicating behavior that cannot be predicted, as opposed to a diagnosis of unknown pathology)
Morphology: Adenocarcinoma; Sarcoma; Lymphoma etc
Note: A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified 'overlapping lesion', unless the combination is specifically indexed elsewhere. For multiple neoplasms of the same site that are not contiguous, such as tumors in different quadrants of the same breast, codes for each site should be assigned.
Behavior: Primary or Secondary Site; Designate if Overlapping For Secondary Site…document if primary site still exists
Gender: Male or Female
11 | P a g e R e v . 9 . 2 9 . 2 0 1 5
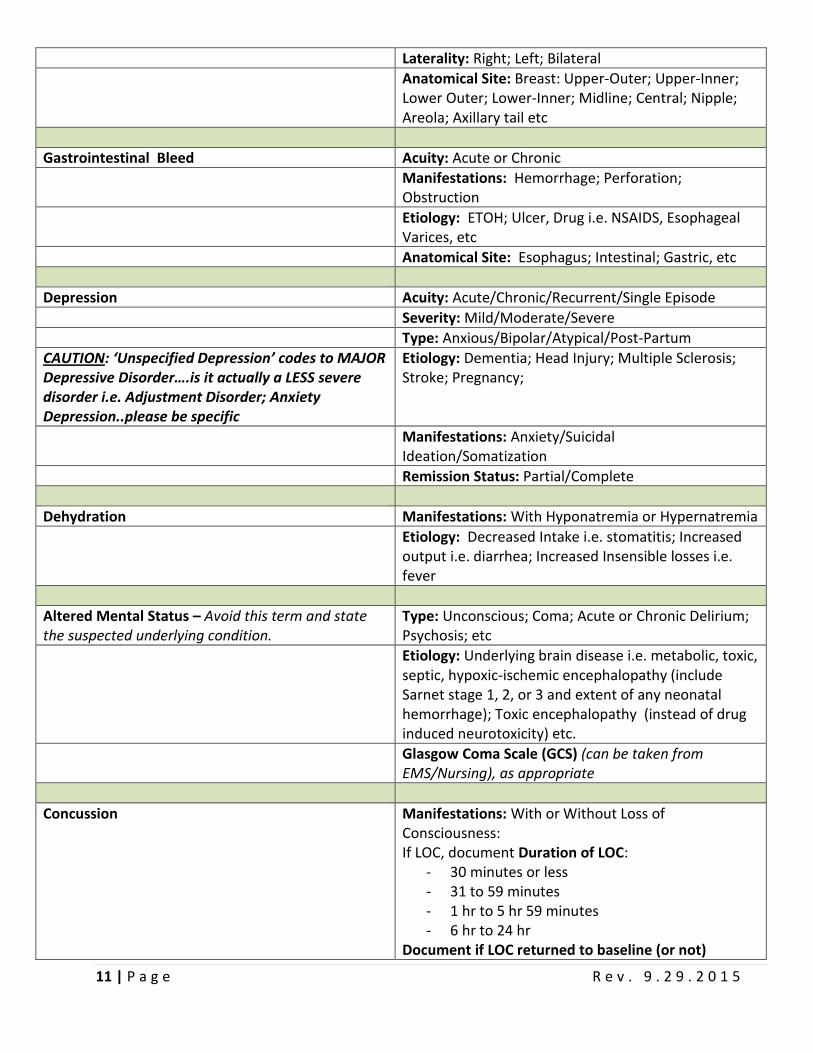
Laterality: Right; Left; Bilateral
Anatomical Site: Breast: Upper-Outer; Upper-Inner; Lower Outer; Lower-Inner; Midline; Central; Nipple; Areola; Axillary tail etc
Gastrointestinal Bleed Acuity: Acute or Chronic
Manifestations: Hemorrhage; Perforation; Obstruction
Etiology: ETOH; Ulcer, Drug i.e. NSAIDS, Esophageal Varices, etc
Anatomical Site: Esophagus; Intestinal; Gastric, etc
Depression Acuity: Acute/Chronic/Recurrent/Single Episode
Severity: Mild/Moderate/Severe
Type: Anxious/Bipolar/Atypical/Post-Partum
CAUTION: ‘Unspecified Depression’ codes to MAJOR Depressive Disorder….is it actually a LESS severe disorder i.e. Adjustment Disorder; Anxiety Depression..please be specific
Etiology: Dementia; Head Injury; Multiple Sclerosis; Stroke; Pregnancy;
Manifestations: Anxiety/Suicidal Ideation/Somatization
Remission Status: Partial/Complete
Dehydration Manifestations: With Hyponatremia or Hypernatremia
Etiology: Decreased Intake i.e. stomatitis; Increased output i.e. diarrhea; Increased Insensible losses i.e. fever
Altered Mental Status – Avoid this term and state the suspected underlying condition.
Type: Unconscious; Coma; Acute or Chronic Delirium; Psychosis; etc
Etiology: Underlying brain disease i.e. metabolic, toxic, septic, hypoxic-ischemic encephalopathy (include Sarnet stage 1, 2, or 3 and extent of any neonatal hemorrhage); Toxic encephalopathy (instead of drug induced neurotoxicity) etc.
Glasgow Coma Scale (GCS) (can be taken from EMS/Nursing), as appropriate
Concussion Manifestations: With or Without Loss of Consciousness: If LOC, document Duration of LOC:
- 30 minutes or less - 31 to 59 minutes - 1 hr to 5 hr 59 minutes - 6 hr to 24 hr
Document if LOC returned to baseline (or not)

12 | P a g e R e v . 9 . 2 9 . 2 0 1 5
Episode of Care: Initial/Subsequent/Sequela
Coma Manifestations: Unconscious; Stupor; Somnolence
“Unconscious codes to coma” Etiology: Identify the cause of unconscious state, if possible
Document any associated skull fracture or intracranial injury
Coma Assessment Areas: Eye opening/Verbal Response/Motor Response
Glasgow Coma Scale (GCS) (can be taken from EMS/Nursing), as appropriate
Document if there is a ‘Persistent vegetative state’ or ‘Transient alteration of awareness’
Incidental to Pregnant State vs. Impacting Pregnancy
State “Does not affect or complicate the pregnancy” if incidental, otherwise will code as ‘impacting the pregnancy’
e.g. Pregnant patient with burn of hand, “Burn of hand does not affect or complicate the pregnancy”
Newborn Themes Preterm or Term; # weeks gestation
Birth Weight in Grams
Single Live born Vaginal/C Section
In Hospital/Outside of Hospital
Single, Twin, Triplet, Other
Maternal Conditions affecting the newborn
Congenital vs. Acquired conditions
Associated Diagnoses/conditions
Infectious Otitis Externa Site and Laterality Type: Abscess, Cellulitis, Diffuse, Hemorrhagic, Swimmer’s, Other
Underdosing Intentional vs. Unintentional
Reason for Underdosing i.e. financial hardship or Age related dementia
Episode of Care: Initial/Subsequent/Sequela
Tobacco Use Use/Dependence/Contact with Second Hand Exposure (Acute or Chronic)
Caution: ‘History of smoking’ can be an ambiguous statement.
Current/No longer Use Tobacco/Never
Type of Tobacco Product: Cigarette/Chewing Tobacco/Nicotine

13 | P a g e R e v . 9 . 2 9 . 2 0 1 5
If Dependence: Uncomplicated/In remission/With withdrawal/With other Nicotine induced disorder
ADDITIONAL DOCUMENTATION TIPS
Radiology Tests Ordered
‘Better info given →Better outcome on Report’
Reason for Exam –Be Specific as to what looking for - Anatomical Site Specificity/Where specifically the
problem is…i.e. ‘tender over T9’ instead of ‘back pain’
- Indication for Xray, i.e. Lt Pleuritic Chest Pain; Orthopnea; SOB at rest
- Why doing exam/What are you looking for? i.e. re Cancer…’Looking for Metastasis
- AVOID: R/O, Pre –Op, Vague terms i.e. cough, dizzy. Instead state, fever, shakes, chills so Radiologist can help you capture Pneumonia if present.
- Example of Reason for Exam: ‘Pt fell of ladder, pain medial aspect Lt ankle x 3 days’ instead of ‘ankle pain’; OR, ‘Pt with fever, chills, productive cough green sputum x 2 days’ instead of, ‘cough’.
Chronic Conditions/Secondary Diagnosis Capture the Severity!!!
Avoid stating ‘History of’ ……Instead document what you are doing for Chronic Conditions now! Examples of documentation showing link between the additional disease and this admission’s evaluation, treatment, or monitoring:
Hypertensive Heart Disease and Chronic Kidney Disease (CKD), stage 3 (Strict I & O, Monitor BP)
Chronic Systolic Heart Failure (Echo, Lasix 40 mg)
Hypokalemia (K+ repleted)
Acute Blood Loss Anemia (2 U PRBC’s)
Indicate “Present on Admission” (POA) status, as applicable
A diagnosis without documentation of being present on admission could be inadvertently considered a hospital-acquired condition (HAC). Example: Pneumonia not definitively diagnosed until hospital day two but suspected, probable, or likely on admission should be noted as such. This allows coders to most accurately report the condition as being POA as opposed to hospital-acquired.

14 | P a g e R e v . 9 . 2 9 . 2 0 1 5
AVOID Signs and Symptoms as Diagnosis Definitive diagnoses are preferred in the inpatient setting and support a higher evaluation and management (E/M) fee. In the inpatient setting, coders can capture ‘probable’, ‘likely’, ‘suspected’, or presumed diagnoses when patients present with the signs and symptoms of the diagnoses being ruled out…. as long as those diagnoses are restated in the discharge summary and have not been ruled out during the stay.
Discharge Summary Wrap it all up!!
For all ‘Rule Out’ situations: Rule it in!/ Rule it Out!/or state ‘Resolved’!
Avoid Conflicting with previous documentation substantiated in the record……Caution: If primary physician subsequent dictation conflicts with previous ‘consult’ note, the primary physician’s diagnosis is taken.
INCLUDE: Reason for hospitalization: Chief Complaint; including description of the initial diagnostic evaluation Significant Findings: -Admitting Diagnosis - reason for hospitalization -Discharge Diagnosis - significant findings/diagnoses -As well as those conditions resolved during hospitalization -List all possible and probable diagnoses as well -Hospital Course - procedures performed and findings/surgical findings/test results/treatment rendered/consults -Discharge Disposition – pt condition at discharge -Education -Follow up needed -Diet -Medications – discharge meds; changes; discontinued meds -Discharge Instructions - instructions to patient and family, including follow up
References: 3M physician video; CMS Road to 10; Coding Guidelines; 3M Doc tips; AHIMA ACDIS ICD 10 Webinar 12.2014; ACDIS ICD 10 CDI Bootcamp 2014; ICD 10 CM for Hospitals; Precyse Doc Talks
Check out www.tfhd.com/icd10