hormonal regulation of plasma calcium and calcium metabolism
DESCRIPTION
Hormonal Regulation Of Plasma Calcium And Calcium Metabolism. Guo Xiaosun [email protected] Shandong University. 1. The significance of maintaining plasma calcium levels. I The normal value and source of plasma calcium; II The structure, functions and endocrinology of bone; - PowerPoint PPT PresentationTRANSCRIPT

Hormonal Regulation Of Plasma Calcium And Calcium Metabolism
Guo Xiaosun
Shandong University
1

• 1. The significance of maintaining plasma calcium levels.
• I The normal value and source of plasma calcium;
• II The structure, functions and endocrinology of bone;
• 2. The hormonal regulation of plasma calcium:
• I Parathyroid hormone: parathyroid glands; secretion of parathyroid hormone; actions of parathyroid hormone; parathyroid hormone related peptide.
• II Calcitriol: source and activation of vitamin D; vitamin D and calcitriol in blood ; action of calcitriol.
• III other hormones.
• 3. Disorders of calcium metabolism and metabolic bone disease:
• I Disorders of hypocalcaemia: vitamin D deficiency; parathyroid hormone deficiency.
• II Diseases of bone: osteoporosis; osteomalacia and rickets; Paget’s disease.
• 4. Regulation of serum phosphate. 2

1.The significance of maintaining plasma calcium levels.
3

CALCIUM
•2% of body weight 99% in bones 1% in body fluids
•Plasma (Extracellular fluid)
▫2.25 – 2.75 mmol/l
•Cell (Intracellular fluid)
▫10-8 – 10-7 mol/l = 10-5 – 10-4 mmol/l
4

5

PLASMA CALCIUM diffusible
• 48% (50%) Ca2+ ionized
• 6% (10%) combined with anions
(citrate, phosphate) – non-
dissociated
nondiffusible
• 46% (40%) combined with plasma
proteins
• combination with proteins depends
on pH 0.2 mmol/l Ca2+ on each pH
unit
6

Plasma Calcium Regulation
•Free calcium is tightly regulated (5%)
▫Too low = neuronal hyper-excitability
▫Too high = neuronal depression
•Control points for calcium
▫Absorption – Via intestines
▫Excretion – Via urine
▫Temporary storage – Via bones
7

Calcium Balance• Intake = output•Negative calcium
balance: Output > intake▫Neg Ca2+ balance
leads to osteoporosis•Positive calcium
balance: Intake > output▫Occurs during growth
•Calcium is essential, we can’t synthesize it
8

Calcium and the Cell
• Translocation across the plasma membrane• Translocation across the ER and mitochondrion;
Ca2+ ATPase in ER and plasma membrane 9

ROLE OF CALCIUM
• excitability of cell membranes
• neuromuscular transmission and muscle contraction
• releasing of transmitters from synapses
• “second messenger”
• stimulates secretory activity of exocrine glands and
releasing of hormones
• contractility of myocard
• blood coagulation
10
Changes in Ca2+ plasma levelHypocalcemia
• Muscle tetany carpopedal spasm
• Na+ inflow ↑→myocardium excitability and conductibility ↑ ;Ca2+ inflow ↓→plateau phase of action potential↑
• Increased cell membrane permeability
• Impaired blood clotting
Hypercalcemia
• Depression of nervous system, reflex activity,
• Increased heart contractility
• Formation of calcium phosphate crystalls ( Kidney stones, and
ectopic calcification)
11

Bones – reservoir of calcium• 99% of skeletal calcium forms stable bone (not
exchangeable with the Ca in extracellular fluid)
• 1% is in the form of releasable pool of Ca
• Balance of deposition and resorption
• Osteoblasts – bone-forming cells responsible for
bone deposition
▫Secrete type I collagen
▫Differentiate into osteosytes
• Osteoclasts – “bone-eating” cells that resorb the
previously formed bone12

Osteoblast and Osteoclast Function
• Osteoblasts
• Bone formation
• Synthesis of matrix
proteins
▫ Type I collagen
▫ Osteocalcin
▫ Others
• Mineralization
• Activation of osteoclasts
via RANKL production
• Osteoclasts
• Bone resorption
▫ Degradation of proteins by
enzymes
▫ Acidification
• RANK is activated by
RANKL, and this leads to
cells differentiation to
osteoclasts
13


Regulation of osteoblasts function
• Stimulation▫PTH (fast reaction - activation of calcium pump ? –
pumping Ca to ECF)▫1,25 Dihydrocholecalciferol▫ IL-1▫T3, T4▫hGH, IGF-1 (insuline-like growth factor)▫PGE2 (prostaglandine)
▫TNF (tumor necrosis factor)▫Estrogens
• Inhibition▫Corticosteroids
15

Regulation of osteoclasts function• Stimulation
▫PTH (not directly – through stimulation of osteoblasts)
▫1,25 Dihydrocholecalciferol (not directly – through stimulation of osteoblasts)
▫ IL-6, IL-11• Inhibition
▫Calcitonin (directly – receptors)▫Estrogens (by inhibiting production of certain
cytokines)▫TGF-β (tranforming growth factor)▫PGE2(prostaglandine)
16

2. The hormonal regulation of plasma calcium
17

Regulation of calcium metabolism
1. Parathyroid hormone
2. Calcitonin
3. Vitamin D
18

Parathormon
19
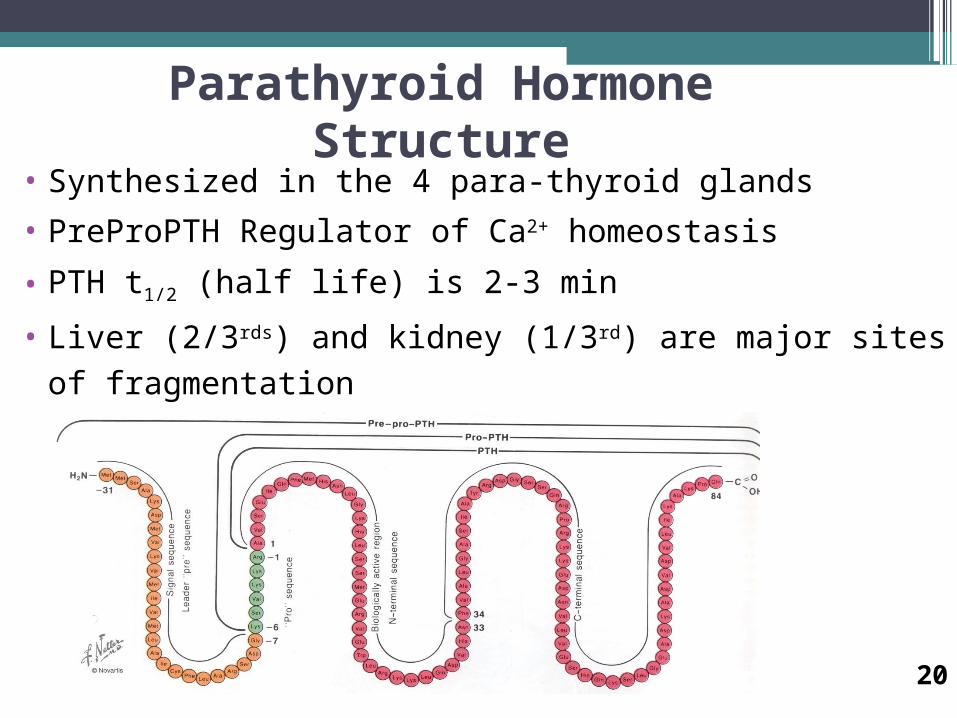
Parathyroid Hormone Structure• Synthesized in the 4 para-thyroid glands
• PreProPTH Regulator of Ca2+ homeostasis
• PTH t1/2 (half life) is 2-3 min
• Liver (2/3rds) and kidney (1/3rd) are major sites of fragmentation
20
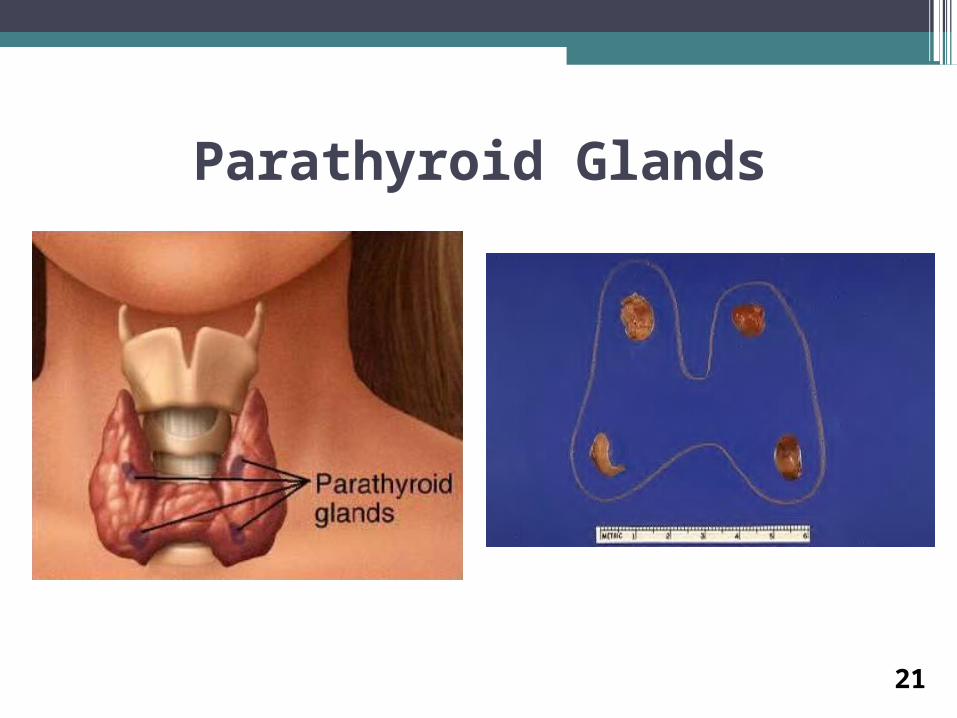
Parathyroid Glands
21
22

28W.F.Ganong: Review of Medical Physiology 2003 20th Ed. #188 fig.21-10

Mechanism of Action of PTH
• PTH binds to a G protein-coupled receptor.
• Binding of PTH to its receptor activates 2 signaling
pathways:
- increased cyclic AMP
- increased phospholipase C
• Activation of PKA appears to be sufficient to decrease
bone mineralization
• Both PKA and PKC activity appear to be required for
increased resorption of calcium by the kidneys
24

Actions of PTH: Bone
• PTH acts to increase degradation of bone (release of calcium).
--Rapid action
--Delayed action
- causes osteoblasts to release cytokines, which stimulate
osteoclast activity
- stimulates bone stem cells to develop into osteoclasts
-- net result: increased release of calcium from bone
-- effects on bone are dependent upon presence of vitamin D
25

Actions of PTH: Kidney• PTH acts on the kidney → the reabsorption of calcium ↑
(excretion↓).
• excretion of phosphate ↑ excretion of H +↓ (more acidic
environment favors demineralization of bone)
• ALSO, Stimulates transcription of 1-alpha hydroxylase for
Vitamin D activation in kidney→the active metabolite of
vitamin D3↑ (required for calcium absorption from the small
intestine, bone demineralization).
• NET RESULT: increased plasma calcium levels
26

27

Regulation of PTH Secretion
• PTH is released in response to changes in plasma calcium
levels (negative feedback).
• PTH cells contain a receptor for calcium, coupled to a G
protein.
• calcium ↑→ Gq →PLC→IP3 →calcium inflow↑ , ER
calcium release↑→ PTH ↓
• Also, vitamin D↑ , Mg2+↑, P↓ , somatostatin→PTH↓
28

29

PTH, Calcium & Phosphate
30

Vitamin D
31

32
Vitamin D Metabolism

Effects of Active Form of Vit D3• Promotes intestinal absorption of calcium
• promotes bone mobilization (stimulate osteoclasts’ precursor
mature and turnover
→Ca2+↑Pi ↑)mainly
• promotes bone deposition ( stimulate osteoblasts →
osteocalcin↑other protein↑→ deposition ↑ calcification ↑ )• Has slight effect to increase calcium re-absorption in kidneys
• Works with PTH to cause calcium absorption from bone
• PTH↓
33

Proposed Mechanism of Action of 1,25-DihydroxyD3 in Intestine
34
Regulation of Vitamin D Metabolism• PTH → 1-hydroxylase activity↑→ production of active form↑
• PTH→ 24-hydroxylase transcription↓→1,24,25 ( OH ) 3D 3↓
• phosphate ↓→ 1-hydroxylase activity↑
• Ca↓→PTH→…………
• 1,25 ( OH ) 2D 3↑→ 1-hydroxylase activity ↓
• 1,25 ( OH ) 2D 3↑→ 24-hydroxylase transcription↑→ 1,24,25 ( O
H ) 3D 3↑
• Growth hormone, prolactin, estrogen, calcitonin→ 1,25 ( OH ) 2D 3↑
• cortisol → 1,25 ( OH ) 2D 3 ↓
35

Changes in vitamine D plasma levelHypovitaminosis
• RICKETS (rachitis)– children
• OSTEOMALACIA - adults
▫Attention! – Osteoporosis is decrease of bone
mass (matrix and minerals)
Hypervitaminosis
• Tissue and organs calcification
• Lost of body weight
• Kidney function failure
36

Calcitonin
37

•Product of parafollicular C cells of the thyroid•32 aa
Calcitonin
38

• The target cell for calcitonin is the osteoclast.
--Calcitonin acts via increased cAMP concentrations to inhibit
osteoclast motility and cell shape and inactivates them.
( 15min ↓70% , mainly in children but not in adult)--The major effect of calcitonin administration is a rapid fall in
Ca2+ caused by inhibition of bone resorption.
• osteoblastic activity ↑→Ca P deposition ↑ ( 1h)• Ca, P , Mg, Na and Cl resorption in kidney tubules ↓(weak)
Actions of Calcitonin
39

40
Comparison of Calcitonin Effects with PTH Effects
(1) PTH ---- slowly, need several hrs.
CT ----- rapidly, less than 1 hr.
(2) PTH ---- long-term regulation
CT ----- short-term regulation
PS Wang/2004.0
5
What is the Role of Calcitonin in Humans?
• Removal of the thyroid gland has no effect on
plasma Ca levels!
• Excessive calcitonin release does not affect bone
metabolism!
• Other mechanisms are more important in regulating
calcium metabolism (i.e., PTH and vitamin D).
41

Calcitonin• Role of calcitonin in normal Ca2+ control is not
understood—may be more important in control of bone remodeling.
• Used clinically in treatment of hypercalcelmia and in certain bone diseases in which sustained reduction of osteoclastic resorption is therapeutically advantageous.
• May be more important in regulating bone remodeling than in Ca2+ homeostasis.
42
Regulation of Calcitonin Release
• Calcitonin release is stimulated by increased circulating
plasma calcium levels.
• Calcitonin release is also caused by the gastrointestinal
hormones gastrin and cholecystokinin (CCK), whose
levels increase during digestion of food.
Food (high calcium )
gastrin, CCK, glucagon, secretin
increasedcalcitonin
decreased boneresorption 43

Factors affecting bone turnover
44

Factors affecting bone turnover • Other hormones
• Glucocorticoids▫ gut - decrease absorption▫ bone - increased re-absorption/decreased formation▫ Kidney-excretion of both calcium and phosphate ↑
• Thyroxine▫ stimulates formation/resorption▫ net resorption▫ Kidney-excretion of calcium↑
• Growth hormone▫ Stimulate bone formation▫ renal calcium excretion ↑▫ gastrointestinal absorption of calcium ↑
• Oestrogen▫ gut - increased absorption▫ bone - decreased re-absorption
45

•Estrogens and Androgens: both stimulate bone
formation during childhood and puberty.
•Estrogen inhibits PTH-stimulated bone resorption.
•Estrogen increases calcitonin levels
•Osteoblasts have estrogen receptors, respond to
estrogen with bone growth.
•Postmenopausal women (low estrogen) have an
increased incidence of osteoporosis and bone
fractures.
46

47W.F.Ganong:Review of Medical Physiology 2003 20th Ed. fig.21-6 #1441

Factors affecting bone turnover•Local factors• I-LGF 1 (somatomedin C)
▫ increased osteoblast prolifn• TGF
▫ increased osteoblast activity
• IL-1/OAF▫ increased osteoclast activity (myeloma)
• PG’s▫ increased bone turnover (#’s/inflammn)
• BMP▫bone formation
48

Factors affecting bone turnover
•Other factors
•Local stresses
•Electrical stimuli
•Environmental
▫temp
▫oxygen levels
▫acid/base balance
49

Nutrition and Calcium
50

Nutrition and Calcium
Heaney RP, Refferty K Am J. Clin Nutr 200174:343-7
▫ Excess calciuria associated with consumption of
carbonated beverages is confined to caffeinated
beverages.
▫Acidulant type (phosphoric vs. citric acid) has no acute
effect.
▫The skeletal effects of carbonated beverage consumption
are due primarily to milk displacement.
51

Nutrition and CalciumSee Nutrition 2000 Vol 16 (7/8) in particular:
• Calvo MS “Dietary considerations to prevent loss of bone
and renal function”▫ “overall trend in food consumption in the US is to drink less
milk and more carbonated soft drinks.”
▫ “High phosphorus intake relative to low calcium intake”
▫ Changes in calcium homeostasis and PTH regulation that
promote bone loss in children and post-menopausal women.
▫ High sodium associated with fast-food consumption competes
for renal reabsorption of calcium and PTH secretion.
52

Nutrition and CalciumSee Nutrition 2000 Vol 16 (7/8) in particular:
• Harland BF “Caffeine and Nutrition”
▫ Caffeine is most popular drug consumed world-wide.
▫ 75% comes from coffee
▫ Deleterious effects associated with pregnancy and osteoporosis.
▫ Low birth-rate and spontaneous abortion with excessive
consumption
▫ For every 6 oz cup of coffee consumed there was a net loss of 4.6
mg of calcium
▫ However, if you add milk to your coffee, you can replace the
calcium that is lost.
53

Effects of soft drinks
• Intake of carbonated beverages has been associated
with increased excretion and loss of calcium
• 25 years ago teenagers drank twice as much milk as
soda pop. Today they drink more than twice as much
soda pop as milk.
• Another significant consideration is obesity and
increased risk for diabetes.
• For complete consideration of ill effects of soft drinks on
health and environment see:▫ http://www.saveharry.com/bythenumbers.html
54

Excessive sodium intake• Excessive intake of Na may cause renal hypercalciuria
by impairing Ca reabsorption resulting in compensatory
increase in PTH secretion.
• Stimulation of intestinal Ca absorption by PTH-induced
1,25-(OH)2-D production compensates for excessive Ca
excretion
• Post-menopausal women at greater risk for bone loss
due to excessive Na intake due to impaired vitamin D
synthesis which accompanies estrogen deficiency.
55

Effects of Exercise•Bone cells respond to pressure gradients in laying down bone.
•Lack of weight-bearing exercise decreases bone formation, while increased
exercise helps form bone.
� Increased bone resorption during immobilization may result in hypercalcemia
56

Exercise and Calcium
•Normal bone function requires weight-bearing
exercise
•Total bed-rest causes bone loss and negative
calcium balance
57

58

3. Disorders of calcium metabolism and metabolic bone disease
59

Hypercalcaemia
60

physiological response of hypercalcaemia
• ↑plasma calcium→↓PTH
• →bone:↓ breakdown of bone; formation of bone
• → gut:↓ formation of calcitrol→less Ca2+uptake from gut
• →kidney:↓ Ca2+absorption→excess Ca2+ lost in urine
• →→↓ plasma calcium
61

Causes of Hypercalcemia
Common Uncommon
Malignant disease, e.g. some lung cancers
Renal failure
Hyperparathyroidism Sarcoidosis
Vitamin D toxicity (excessive intake)
Multiple myeloma
62

PTHrP; Parathyroid Hormone related Protein
• It is synthesized as 3 isoforms as a result of alternative splicing (139, 141, 173 aa)
• Can activate the PTH receptor• Plays a physiological role in lactation, possibly as a hormone
for the mobilization and/or transfer of calcium to the milk• May be important in fetal development• May play a role in the development of hypercalcemia of
malignancy▫Some lung cancers are associated with hypercalcemia▫Other cancers can be associated with hypercalcemia
63

PTHrP; Parathyroid Related Protein
64

Symptoms: They are classically summarized by the mnemonic "stones, bones,
abdominal groans and psychic moans”
• "Stones" refers to kidney stones, nephrocalcinosis, and diabetes insipidus (polyuria and polydipsia).
• "Bones" refers to bone-related complications, osteitis fibrosa cystica, which results in pain and sometimes pathological fractures, osteoporosis, osteomalacia, and arthritis.
• “Abdominal Groans” refers to gastric related symptoms such as Abdominal pain, vomiting, constipation and anorexia .
• "Psychic moans” which includes depression, memory loss, psychosis, ataxia, delirium, and coma.
65

66

67

• Left: Giant Cell Granuloma
• Right: Loss of lamina dura, pathognomonic oral change in
hyperparathyroidism68

Signs
•Proximal muscle weakness
•Signs of Dehydration
•Altered mental state.
69

Investigations:• Serum calcium and phosphate: phosphate is low in primary
hyperparathyroidism and some cases of malignancy, normal or
inappropriately high in other causes of hypercalceamia.
• PTH level: high in hyperparathyroidism.
• Radiology (lytic lesions, subperiosteal erosions in the
phalanges).
70

Investigation
If PTH is undetectable the following tests should be
done:
• -protein electrophoresis for myeloma.
• -TSH to exclude hyperthyroidism.
• -synacthen test to exclude Addison’s disease.
• -hydrocortisone suppression test, +ve in sarcoidosis, vitamin
D-mediated hypercalceamia and some malignancies.
71

Treatment
- Fluids:
- parathyroidectomy
-removing the source of vit D and treating with
glucocorticoids(excess vit D)
72

Hypocalcaemia
73

physiological response of hypocalcaemia
• ↓ plasma calcium→↑PTH
• → bone:↑ breakdown of bone; formation of bone↓
• → gut:↑ formation of calcitrol→↑Ca2+uptake from gut
• → kidney:↑ Ca2+absorption→↓ Ca2+ lost in urine
• →→↑ plasma calcium
84

Sequence of Adjustments to Hypocalcemia
75

Causes of Hypocalcemia
Hypoparathyroid
Nonparathyroid PTH Resistance
Postoperative Vitamin D deficiency
Pseudo-hypoparathyroidism
Idiopathic Malabsorption
Post radiation Liver disease
Kidney disease
Vitamin D resistance
76
Vitamin D Deficiency• Inadequate intake and absence of sunlight
• The most prominent clinical effect of Vitamin D
deficiency is osteomalacia, or the defective
mineralization of the bone matrix
• Osteoblasts contain the vitamin D receptor
• Vitamin D deficiency in children produces rickets
• A deficiency of renal 1α-hydroxylase produces
vitamin D-resistant rickets
▫Sex linked gene on the X chromosome
▫Renal tubular defect of phosphate resorption
▫Teeth may be hypoplastic and eruption may be
retarded 77

Rickets
78

Vitamin D-Resistant Rickets
• Above: Hypoplastic teeth
• Below: Minimal caries can produce pulpitis; periapical abscesses are thus common
• Lack 1-hydroxylase in kidney
• Rx: Respond well to 1, 25-
dihydroxyD3
79
Pseudohypoparathyroidism• Symptoms and signs
▫ Hypocalcemia▫ Hyperphosphatemia▫ Characteristic physical appearance: short stature, round face,
short thick neck, obesity, shortening of the metacarpals▫ Autosomal dominant
• Resistance to parathyroid hormone• The patients have normal parathyroid glands, but they fail to respond
to parathyroid hormone or PTH injections• Symptoms begin in children of about 8 years
▫ Tetany and seizures▫ Hypoplasia of dentin or enamel and delay or absence of eruption
occurs in 50% of people with the disorder• Rx: vitamin D and calcium
80

Pseudohypoparathyroidism
Elfin facies, short stature, enamel hypoplasia
81

Congenital Hypoparathyroidism
• Hypoplasia of the teeth, shortened roots, and retarded eruption82

Calcium, Bones and Osteoporosis
• The total bone mass of humans peaks at 25-35 years of
age.
• Men have more bone mass than women.
• A gradual decline occurs in both genders with aging, but
women undergo an accelerated loss of bone due to
increased resorption during perimenopause.
• Bone resorption exceeds formation.
83

Calcium, Bones and Osteoporosis
•Reduced bone density and mass: osteoporosis
•Susceptibility to fracture.
•Earlier in life for women than men but eventually
both genders succumb.
•Reduced risk: ▫Calcium in the diet
▫habitual exercise
▫avoidance of smoking and alcohol intake
▫avoid drinking carbonated soft drinks
84

Factors that Affect Peak Bone Mass• Gender (M>F), males have greater PBM than females• Race (Blacks >Whites)• Genetics (osteoporosis runs in families and this may be the
predominant factor)
▫Estrogen receptor gene▫Type I collagen gene▫Vitamin D receptor gene
• Gonadal steroids (estrogen and testosterone increase bone mass)
• Growth hormone (increases bone mass)• Calcium intake (supplements work)• Exercise (increases bone mass)
85

Vertebrae of 40- vs. 92-year-old women Note the marked loss of trabeculae with preservation of cortex.
86

Normal and Osteoporotic Bone
87

Sequelae of Osteoporosis
88

Osteo-porosis
89

Bone Density as a Function of Age
90

Treatments (Continued)• Exercise, activity• Calcium intake should be 1000-1500 mg/day
▫ Postmenapausal women take in less than 500 mg/day▫ Males and females should take in 1000-1500 mg/day▫ All adults greater than 65 years should take 1500 mg/day▫ Three glasses of milk or three cups of yogurt per day provide 1000-1500
mg/day• Estrogen treatment
▫ Estrogen inhibits osteoclastic activity▫ Bone density increases 3-5% per year for the first three years after
menopause▫ This therapy needs to be individualized
Estrogen may increase the incidence of breast cancer, heart attacks, stroke, blood clots
That it may exacerbate cardiovascular disease is controversial
▫ All the data are not in yet, and estrogen treatment is under review; for more information go to http://www.fda.gov/bbs/topics/NEWS/2003/NEW00863.html
91

Treatments (Continued)• Raloxifene (Brand name Evista) is a selective estrogen receptor modulator
• Decreases in estrogen levels after menopause lead to increases in bone
resorption and bone loss. Bone is initially lost rapidly because the
compensatory increase in bone formation is inadequate to offset resorptive
losses. This imbalance between resorption and formation is related to loss
of estrogen, and may also involve age-related impairment of osteoblasts or
their precursors
• Raloxifene reduces resorption of bone and decreases overall bone turnover.
These effects on bone are manifested as increases in bone mineral density
(BMD)
• Raloxifene’s biological actions, like those of estrogen, are mediated through
binding to estrogen receptors. This binding results in the modulation of
expression of multiple estrogen-regulated genes in different tissues
92

Treatments (Continued)
• Bisphosphonates inhibit osteroclasts▫ Alendronate (Brand name Fosamax)
▫ Risedronate (Brand name Actonel)
• Calcitonin (Brand name Miacalcin )
▫From salmon
▫Given intranasaly
▫Probably least effective Rx
• Vitamin D
▫Most Americans consume less than recommended amount
▫800 IU per day seems safe and not enough to cause vitamin
D toxicity93

Treatments (Continued)• Parathyroid hormone (Brand name Forteo)
▫ Teriparatide, a form of parathyroid hormone, is approved for the treatment of osteoporosis in postmenopausal women and men who are at high risk for a fracture
▫ Chronically elevated PTH leads to bone loss; however, intermittent PTH (once daily bolus injection) leads to new bone synthesis
▫ Must be injected daily, a major disadvantage▫ Cost about $7000 per year
• Future Rx’s Sodium fluoride
Considered a possibility for years Adoption seems unlikely
Strontium ranelate NEJM 350 (2004) 459-468.
94

Calcium Content of Foods
• http://www.nal.usda.gov/fnic/foodcomp/Data/SR16/wtrank/wt_rank.html 95

4. Regulation of serum phosphate.
96

PHOSPHATES
• 80% bones and teeth
• 10% blood and muscles
• 10% different chemical complexes
• Plasma (ECF) 0.65 – 1.62 mmol/l
• Cell (ICF) 65 mmol/l (including organic P)
97

Phosphate Turnover
98

99