home hemodialysis have you ever considered home dialysis?
TRANSCRIPT
A N E W LO O K AT H O M E D I A LY S I S
Read aboutTeadora Mendezand her successfulexercise program.
—Page 13
Home dialysis canpsychologicallyimprove the livesof those with kid-ney disease.
—Page 10
Home peritonealdialysis can be agood treatmentfor your childwith CKD.
—Page 5
Have You Ever Considered Home Dialysis?By Bobbie Knotek, RN, BSN, CNN
Would you like to:� Have more control over
how chronic kidney disease(CKD) affects your life?
� Spend more time at homewith your family?
� Schedule your dialysistreatments around work,school or other activities?
If you answered yes to thesequestions, you might want toconsider learning how to dohemodialysis or peritoneal dial-ysis at home.
There are three types ofhemodialysis (HD) treatmentsand two types of peritonealdialysis (PD) treatments thatcan be done at home. All HDand PD treatments removewaste products and extra fluidthat build up in kidney failure,but the number of hours pertreatment and the number oftreatments per week will be dif-
ferent for each type of dialysisbecause each removes wasteproducts and extra fluid fromthe blood at a different speed.
The three types of home hemodiaylsis are:• Standard hemodialysis—four
to five hour treatments, threetimes per week
• Nocturnal hemodialysis—eight to 10 hour treatments,three to five times per week
• Short, daily hemodialysis—two to three hour treatments,five to seven nights per week
The two types of home peritonealdialysis are:• CAPD—four to five fluid
exchanges during the day• CCPD—four to 10 fluid
exchanges during the night(using a machine)
What are the advantages ofhome dialysis?
1) Fewer trips to the dialysisclinic. Unless you have aspecial problem that has tobe watched closely, you willprobably only need to makemonthly visits to the clinicfor checkups.
2) You can arrange dialysistreatments around your life.You still need to dialyze theprescribed number of daysand hours, but you get topick the days and times.
3) You can dialyze in the priva-cy of your home. You decidesuch things as if and whenyou want visitors duringdialysis and when you eatyour meals.
4) Many people feel better onhome dialysis because theyhave more control over theirlife and their treatment.
This publication is a part of the National Kidney Foundation’s Kidney Learning System (KLS)™
and is made possible through an educational grant from .
Inside this issue:
30 East 33rd
StreetN
ew Yo
rk, NY
10016
NO
N-P
RO
FIT O
RG
.U
.S. P
OS
TAG
E
PA
ID
Shakopee,MN
Permit No.211
H O M E H E M O D I A L Y S I SH O M E P D F O R C H I L D R E N
K E E P I N G F I T
A publication of the National Kidney
Foundation
Vol 14, No 2Spring 2005
NEXTISSUE
MENTAL HEALTH
Continued on page 3
Your training
nurse will review
all aspects of
home hemodialy-
sis with you.
This issue of Family Focuswill highlight several dif-
ferent modes of treatment thathave at least one thing in common—each of them can bedone in the comfort of yourown home. You will learnabout the different ways youcould perform either hemodial-ysis or peritoneal dialysiswithout visiting the dialysiscenter except for regular clinic visits.
When first faced with theprospect of beginning dialysis,it is not unusual to be fright-ened. The fear of the unknownis a very natural and logicalreaction. This fear applies tothe concept of dialyzing any-where, including the dialysiscenter where trained staff isavailable to you. When ahealth care professional offersthe option of performing dialy-sis either alone or with the assistance of a helper, usually afamily member, it is again avery common response to feeleven more frightened by theidea of dialyzing at home.However, after exploring thisoption with the staff, one real-izes that a person must be thor-oughly trained by the facility’shome dialysis staff and willnot dialyze at home until boththe person requiring dialysis,their helper, if appropriate,and the staff feel that the indi-vidual(s) is absolutely compe-tent and comfortable withwhatever form of home dialysishas been selected. It also helps
to know thatthe staff willbe available24 hours aday to all whodialyze intheir homes.
There was atime whenmany morepeople wereon home dial-ysis. In the earlier days of dial-ysis, there were fewer dialysisfacilities. As a result, if some-one lived far from a facility,and most were located inurban areas, the only otherdialysis option was to performit at home. Home hemodialysiswas the only form of hometreatment available until the1980’s. When peritoneal dialy-sis was first available, the onlyform of chronic treatmentoffered to most people wasContinuous AmbulatoryPeritoneal Dialysis (CAPD).Although home treatmentoptions have continued toincrease over time, the numberof people who chose any form ofhome dialysis began to go downas more and more dialysis facil-ities opened throughout allareas of the country.
Home dialysis offers manyadvantages, although—as withall things— it may also havedisadvantages. All people whoare either facing dialysis or arealready on dialysis have aresponsibility to look at all of
the advan-tages and disadvantagesfrom theirown personalperspectives.What is a pos-itive treat-ment optionfor one personmay not bethe best foranother.
It is the right of all individualswith chronic kidney disease(CKD) to have every treatmentoption for which they are med-ically suitable offered to them.Family Focus conducted a sur-vey of its readers in 1995 tolearn about the factors affect-ing their treatment choices. Ofthe 844 who responded, 83.6percent reported that centerhemodialysis had been pre-sented to them as an optionbefore they began dialysistreatments.
However, only 49 percent ofthem were offered CAPD, 27percent were offered homehemodialysis and 23 percentwere offered automated peri-toneal dialysis. If those find-ings are an accurate reflectionof what is happening in theUnited States, it should not besurprising that only a smallpercentage of those with CKDactually dialyze at home.
It is our hope that this issueon home dialysis will beenlightening and informationalwhether someone is just begin-ning to consider dialysisoptions or has been receivingdialysis for many years. It isnever too late to learn, as wellas make changes should youdecide that a form of hometreatment is for you!
Karren King, MSW, ACSW, LCSW
For the Editorial Board
EDITOR-IN-CHIEF: Karren King, MSW, ACSW, LCSWKansas City, MO
FITNESS EDITOR: Pedro Recalde, MS, ACSMDowney, CA
MEDICAL EDITOR: Wendy W. Brown, MD, Nashville, TNNURSING EDITOR: Bobbie Knotek, RN, BSN, Plano, TX
NUTRITION EDITOR: Lori Fedje, RD, LD, Portland, ORPATIENT EDITOR: David Jones, Glen Ellyn, IL
PEDIATRIC EDITOR: Barbara Fivush, MD, Baltimore, MDSOCIAL WORK EDITOR: Mary Beth Callahan, ACSW/LMSW-ACP
Dallas, TXTRANSPLANT EDITOR: Nancy Swick, RN, BSN, CCTC
Santa Rosa, CAESRD NETWORK LIAISON: Roberta Bachelder, MA
Woodbridge, CT
EDITORIAL OFFICE: NATIONAL KIDNEY FOUNDATION30 E. 33rd Street, New York, NY 10016800-622-9010 • 212-889-2210www.kidney.orgE-mail: [email protected]
EDITORIAL DIRECTOR: Gigi Politoski
EDITORIAL MANAGER: Sheila Weiner, MSW, LCSW
VICE PRESIDENT OF HEALTH POLICY
AND RESEARCH: Dolph Chianchiano, JD,MPA
EXECUTIVE EDITOR: Sara Kosowsky
MANAGING EDITOR: Helen Packard
PRODUCTION DIRECTOR: Sunil Vyas
DESIGN DIRECTOR: Oumaya Abi Saab
2 FAMILY FOCUS • Volume 14, Number 2
NKF Family Focus is published quarterlyby the National Kidney Foundation.
Opinions expressed in this newspaper donot necessarily represent the position of
the National Kidney Foundation.
F R O M T H E E D I T O R
Karren King
CORRECTION
In the Winter 2005 issue, the byline for the article entitled“Speaking Up For Your Good Health” was printed as beingauthored by Mary Beth Callahan, ACSW, LICSW. This wasan editorial error and the article was actually authored byMark Meier, MSW, LICSW. We apologize to Mr. Meier for
the error.
Mark Meier, MSW, LICSW is the ConsumerServices Coordinator for the Renal Network ofthe Upper Midwest, Inc., of St. Paul, MN.
FAMILY FOCUS • Volume 14, Number 2 3
They learn how to assess and/or prevent health or dialysis-related problems (for example, people on homehemodialysis tend to have fewer bloodpressure drops during their treatmentsbecause they are watching their bloodpressure closely).
5) People on nocturnal hemodialysis orshort daily hemodialysis often havefewer diet restrictions. When your kid-neys are healthy, they clean waste prod-ucts from your blood 24 hours a day,seven days per week (for a total of 168hours of “cleaning time” per week).Unlike healthy kidneys, however, stan-dard dialysis only gives 15 hours of“cleaning time” every week. This is whypeople on standard hemodialysis havestrict diet and fluid restrictions. Peopleon nocturnal hemodialysis, however, get24–48 hours of “cleaning time” per week and those on short daily hemodialysisget 2 1/2–3 hours of “cleaning time” on adaily basis.
6) There are usually fewer problems withyour fistula or graft because the sameperson inserts needles every time andknows your access.
7) There is more freedom to travel with peritoneal dialysis.
What would I learn during home dialysistraining?That depends on the type of home dialysisyou choose, although everyone on homedialysis learns to:• Take blood pressure and pulse• Set up a safe dialysis treatment room
(or area)
• Control fluid and diet • Care for the dialysis access • Order and store dialysis
supplies• Keep treatment records• Learn how to fix dialysis problems,
including machine alarms (for CCPD andHD), low blood pressure and gaining toomuch fluid.
How many people in the United States dohome dialysis?Most of the people in the United Stateswith CKD go to dialysis clinics for theirdialysis treatments. Less than 10 percent ofthe people do peritoneal dialysis and only 1percent do home hemodialysis.
Why don’t more people choose home dialysis?• Many people never get education from
their doctor about the full range of treat-ments available for people with CKD.Because they are never told about any-thing besides in-center hemodialysis,they do not know it is possible to do dial-ysis at home.
• Not every dialysis facility has a homedialysis program. Facilities that do nothave home dialysis programs may notencourage home dialysis.
• At the current time, Medicare does notreimburse dialysis facilities for the costof daily dialysis. Medicare will only payfor three HD treatments per week.Sometimes Medicare will approve payment for a fourth treatment.
• People are often nervous about doingdialysis at home. When talking abouthome dialysis, people with CKD oftensay:• “I am afraid to put needles in my
fistula or graft for hemodialysis.”
• “There is too much to learn— I am notsmart enough to learn home dialysis.”
• “What happens when I have problemsduring a home dialysis treatment?”
It is normal to have concerns and fearswhen starting home dialysis training. Bythe time home dialysis training is done,however, people are almost as good at put-ting in needles and handling machine prob-lems as the dialysis staff. It is alsoreassuring to know that home dialysis clin-ics provide these services to those who areon home treatment: a) a treatment teamthat consists of the kidney doctor, socialworker, dietitian and home dialysis nurse;b) home dialysis staff available or on call 24hours a day for dialysis medical problemsand c) back-up dialysis at the outpatientdialysis center in case you have machineproblems or get too sick to do dialysis athome.
How can I find out more about home dialysis?• Tell your kidney doctor, nurse or social
worker you are interested in home dialysis and ask for more information.
• Go to www.kidney.org (National KidneyFoundation Web site)
• Go to www.homedialysis.org (HomeDialysis Central Web site)
• To find home dialysis clinics that areMedicare certified to offer training, go toMedicare’s Dialysis Facility Compare atwww.medicare.gov and follow thesesteps:1) Look for “Search Tools,” then, click
“Compare Dialysis Facilities In YourArea.”
2) Search for dialysis clinics near yourcity. Type in the name of the city andstate and how many miles outside thecity you wish to look.
3) Choose home hemodialysis or peri-toneal dialysis.
You will get the names, addresses andphone numbers of the home dialysis train-ing facilities in your area.
Home Dialysis…Continued from page 1
Dear Editor,
Kudos to Family Focus for the themesyou are choosing to highlight in your publication. Patient empowerment andhome dialysis are two concepts that,when implemented, have the ability tosignificantly shape people’s lives for thebetter. This year, I celebrate 30 years ofdialysis. Half of that time has been athome; first on CAPD and for the past twoyears on nocturnal home hemodialysis.From those first few months as a teenag-er, I understood that I must take respon-sibility for the management of my healthcare needs. I learned very quickly that Ihave the most invested in the quality ofmy care, thus the imperative to takeaction. This seemingly obvious statementis highly challenging to communicate toboth patients and professionals.
Thank you for doing your part to enlightenothers.
Best regards,Judy Weintraub, MS EdLos Angeles, CA
Dear Editor,
I am on peritoneal dialysis and neededto find a way to hold the peritonealcatheter in place. I bought ladies’ tube topsand wear one around my stomach. It sitsnice and snug over the catheter. I do nothave to worry about the exit site beingexposed or having something pull on thecatheter. I thought this idea might helpothers. My dialysis nurse has passed thistip on to several other people in her care.
Julie Murphy
Julie Murphy receives her dialysis care in Ardmore, OK.
letters tothe editor
DID YOU KNOW that if you have CKD, youhave the right to:
• BE TOLD about ALL treatment options forCKD, including kidney transplant, peritonealdialysis, in-center hemodialysis and homehemodialysis? (This is a Medicare law.)
• BE EVALUATED for home dialysis?• BE GIVEN the names and phone numbers of
clinics that offer home hemodialysis or peri-toneal dialysis training (if your clinic does notoffer this service)?
• TRANSFER to another clinic for home dialysistraining and follow-up if your clinic does notoffer the kind of home dialysis you choose?
Continued on page 16

4 FAMILY FOCUS • Volume 14, Number 2
H O M E H E M O O P T I O N S
WHEN CHRONICHEMODIALYSIS first
began in the late 1950’spatients were treated for 24hours at a time a few days aweek. Over the next severalyears treatments were short-ened, so by the 1970’s mostwere on dialysis for four hoursthree times a week. Eventhough the original, longertreatments were very effective,they were inconvenient forboth those on dialysis andcaregivers and were veryexpensive. In the late 1970’sand 1980’s a few kidney doc-tors in Europe tried to restartmore frequent, longer dialysis.These trials were usually prac-ticed as part of a research trialor were paid for by privatefunding. Dialysis was per-formed at home or in-center foreight to 10 hours, three to fivetimes a week. These programswere all eventually discontin-ued either for financial practi-cal, or social reasons. This typeof therapy was more expensivedue to the greater use of thedialysis machine and use ofmore dialysate, and the thera-py was more labor intensiveeither for the in-center staff orfor the caregiver if the treat-ment was practiced at home.Success came in the early1990’s when Dr. Uldall and Dr. Pierratos from Canadastarted their nocturnal dialysis(dialysis at night) program.They are currently the mostexperienced in the world withthis therapy and have beenproviding it for over 10 yearsto more than 90 individualswith kidney failure.
SINCE NATIVE KIDNEYSFUNCTION 24 hours a day,seven days a week, Drs. Uldalland Pierratos felt that morefrequent, longer dialysis wouldallow people on dialysis to feelhealthier and live more normallives. However, those on dialy-sis also needed free time forsuch things as work and beingwith their families. Thus, theidea of long-time overnightdialysis was born.
ALTHOUGH MORE ANDMORE CENTERS in theUnited States—approximately50—now offer nocturnal dialy-sis, there are usually only afew individuals using it ineach center. There are current-ly about 140 patients inCanada on nocturnal dialysisand about 200 in the UnitedStates. There is no nationalregistry for this type of thera-py, so the actual numbers are
not known. Since nocturnalhemodialysis is performedwhile the person is asleep, thisconstitutes an entirely differ-ent kind of therapy than regu-lar in-center dialysis.Extensive training of the per-son on dialysis and thenephrologist are required,careful attention to safety isnecessary and the cost is high-er than standard hemodialysisand Medicare does not reim-burse for the extra treatmentsperformed per week. Manypeople with chronic kidney dis-ease are not interested in thetherapy because of the exten-sive training required.
NOCTURNAL HEMODIALY-SIS is usually done six orseven nights a week for abouteight hours each night whilethe person sleeps. The dialysismachine is usually in the
home, but some centers prac-tice in-center nocturnalhemodialysis. If it is done athome, it is helpful to have apartner there. The partnerusually does not participate inthe therapy, but if there is anemergency where the individ-ual on dialysis is unable to getto a phone, the partner couldperform that task. Althoughsome programs require that apartner be present, it is notrequired by all programs.Some programs also monitorthe dialysis session over theInternet, but this is becomingincreasingly less common.Several centers have shownthat remote monitoring is notnecessary because people areso stable during the treatmentthey do not need to be moni-tored. Practicing dialysis sixdays a week for eight to 10hours per treatment providesfor very slow fluid removal.Therefore, there is minimal, ifany, hypotension (low bloodpressure) and no need for con-tinued monitoring duringtreatment.Also, if thereare anymachine orflow prob-lems themachine willstop andalarm.Finally,remote moni-toring is anadditionalexpense notcovered by Medicare. The indi-vidual who will do nocturnaldialysis follows an extensivesix-week training program forabout five or six hours a dayduring their chronic dialysistreatments three times a week.All aspects of dialysis therapyare taught, including cannula-tion (putting needles in your
access), setting up and takingdown the machine and trou-bleshooting when problemsarise. All aspects of the watersystem, which provides thedialysis solution to the dialysismachine, are also explained.
BLOOD PRESSURE is onlyrecorded at the beginning andend of treatment by the personon dialysis. Weight or fluidgains between treatments areusually small so there are typi-cally not problems with lowblood pressure. In addition,low blood pressure is oftenavoided with longer treat-ments and slower fluidremoval in nocturnal dialysis.For these reasons, there is noneed to check blood pressureduring treatment.
INDIVIDUALS WHO PRAC-TICE nocturnal therapy usual-ly eat a regular diet withoutfluid restriction. Since noctur-nal dialysis treatments aremuch longer and much morefrequent than traditional dial-ysis, more fluid and wasteproducts are removed perweek, allowing for a very liber-al diet. Most people on thisform of treatment no longertake phosphate binders, sincethere is adequate phosphate
removal with dialy-sis. Many patientsstop their bloodpressure medicinesbecause of betterfluid control.Restless leg syn-drome, that constantjumping and invol-untary contractionof the leg muscles,also often goes awaydue to better control
of uremia. Quality of life isoften much improved, withmore energy and better sleepbecause the patient’s bloodpressure is more stable. Peopleon nocturnal dialysis have moretime for other activities sincedialysis is only at night.
Nocturnal HemodialysisBy Mary Gellens, MD
Nocturnal hemodialysis can be an ideal dialysis option for some.
Although more and
more centers in the United
States now offer nocturnal
dialysis, there are usually
only a few individuals using
it in each center.
Quality of life is often much
improved, withmore energy and better
sleep.
Continued on page 14

FAMILY FOCUS • Volume 14, Number 2 5
F O R Y O U R C H I L D
THE DECISION TO BEGINKIDNEY REPLACEMENT
THERAPY for a child with kid-ney failure is a clinical decisionmade by the health care team.However, the type of kidneyreplacement therapy to use is ateam decision that includesinput from the child and his orher family. The available treat-ment options are hemodialysis,peritoneal dialysis and trans-plant. This article will focus onhome peritoneal dialysis (PD)as kidney replacement treat-ment for children with kidneyfailure (CKD Stage 5).
PD became available as a hometherapy for children with kid-ney failure in the early 1980’s.Since that time, because ofimproved technology, PD hasbecome more user-friendly. PDis managed by the child withCKD and his or her family athome. This type of dialysistakes place inside the abdomi-nal cavity (belly) using the peri-toneal membrane, which linesthe abdomen, as a filter. Thedialysis process consists of sev-eral “exchanges.” The exchangebegins with dialysis fluid enter-ing the abdominal cavitythrough a small plastic tube (aPD catheter), which has beensurgically placed, usually as anoutpatient procedure. The “fill”process only lasts a few min-utes and is followed by a“dwell” phase, during whichtime the fluid stays in the cavi-ty. It is during this “dwell”phase that the filtering processtakes place, clearing the bloodof waste products and extrafluid. Once the dwell period iscomplete, the fluid is “drained”from the cavity through thesame PD catheter into a drainbag. The exchange process isrepeated many times over 24hours to imitate some of thefunctions of a normal kidney.
There are two types of PD:Continuous AmbulatoryPeritoneal Dialysis (CAPD) andAutomated Peritoneal Dialysis(APD), which includes continu-
ous cycling peritoneal dialysis(CCPD). CAPD consists of fourexchanges (draining “old” fluidfrom the peritoneal cavity fol-lowed by draining new fluid in)done manually over 24 hoursfrom the time the child wakesup until the time he or she goesto sleep. There is usually a sixhour dwell time betweenexchanges. Each new exchangetakes about 20 to 30 minutes.APD uses a small cyclermachine about the size of aVCR to do the exchanges,approximately four to sixexchanges over eight to 10hours while the child sleeps.
There are many advantagesover center hemodialysis toeither CAPD or APD for chil-dren and their families. Thetwo main advantages are free-dom from a set schedule andthe ability to do dialysis athome rather than traveling toand from a dialysis center.CAPD and APD may be doneon a flexible daily schedule,making it possible for the childto attend school on a regularbasis and participate in every-day activities. Children on PD
are able to bike, swim andenjoy non-contact sports. Inaddition, PD requires few if anydietary restrictions, a plus inoptimizing caloric intake toachieve optimal growth. Thishome therapy is free of needlesand pain. Therefore, the fearelement is quickly removedonce the child understands thatPD is a painless procedure, andif using APD, that it typicallyoccurs while he or she is asleep.Since PD equipment isportable, traveling is easier.From a clinical standpoint, PDis a good kidney replacementtherapy because it occurs 24hours a day, seven days a week,and therefore works in a waythat is similar to the body’s ownkidneys.
Once the decision is made tobegin PD, outpatient surgerywill be scheduled to place thePD catheter. In most cases aftersurgery, dialysis is not done forone week to allow healing andto begin PD training. Familyeducation for home
PD covers all of the necessaryinformation to ensure that thecaregiver(s) is comfortable man-aging the treatment at home.Programs may vary from onecenter to another, but trainingusually includes five to 10 ses-sions with the PD nurse. Thechild is assigned age appropri-ate jobs to help, and is encour-aged to take an active role inhis or her treatment.
In conclusion, it is important toremember that home peritonealdialysis is a great treatmentoption for children with kidneyfailure. The most importantfeature is that it allows thechild to remain at home withhis or her family and be part ofthe family environment on aday-to-day basis.
Barbara Case, RN,CNN, hasbeen a pediatric nephrologynurse at the Johns HopkinsHospital in Baltimore,Maryland for 20 years.
PATIENT & FAMILY COUNCIL’S MESSAGE BOARD!
If you have chronic kidney disease, are on dialysis, have akidney transplant, or are a family member, friend or healthcare professional, we invite you to share your stories andexperiences, network and get support from others.
Follow the simple instructions below and you will be there in no time:
Home Peritoneal DialysisFor Children
By Barbara Case, RN, CNN
Learn the facts about home PD for
your child with CKD.
Family educationfor home PD
covers all of thenecessary infor-mation to ensure
that the caregiver(s)is comfortable managing the
treatment at home.
Advantages of PeritonealDialysis:
Flexible scheduleLiberal dietNeedle-freeCan attend school regularlyEasier travelParticipation in non-contact
sports and other activities
Go to: www.kidney.org
Select a topic:MessageBoards andChats
Click on: Peoplewith kidneydisease andtheir families

6 FAMILY FOCUS • Volume 14, Number 2
E A T I N G R I G H T
IF YOU ARE CONSIDERINGHOME DIALYSIS, one of the
things you might want to thinkabout is diet. This article willbriefly review the types of homedialysis and the best diet foreach type. There are two typesof peritoneal dialysis (PD): con-tinuous ambulatory peritonealdialysis (CAPD) and continuouscycling peritoneal dialysis(CCPD) or automated peri-toneal dialysis (APD). There are also three types of homehemodialysis: conventionalhome hemodialysis, daily homehemodialysis and nocturnalhome hemodialysis (1).
PD uses the lining of yourabdomen, called the peri-toneum, to filter fluid andwastes out of your blood. Abouttwo liters of fluid, calleddialysate, is placed into theperitoneal cavity (belly) throughan abdominal catheter andallowed to remain for a period of time. During this timewastes and extra fluids travelfrom the body into thedialysis solution and are thenremoved when the solution isdrained. This process, calledan exchange, is done severaltimes a day. It can be donemanually using gravity (CAPD)or with a machine (CCPD orAPD) called a cycler that typi-cally does the exchanges whileyou sleep (2).
Both CAPD and CCPD have thesame diet restrictions. DuringPD, protein and waste productsare lost with each exchange, soprotein needs to be replaced.The high protein diet is neededto build, maintain and repairbody tissues. High-quality pro-tein such as eggs, chicken, fishand lean red meats should beeaten at each meal (3).
Potassium, a mineral in manyfoods, is more liberal or lessstrict in PD compared to in-center hemodialysis (HD). InPD, potassium leaves the bodyand needs to be replaced daily.Too much or too little potassiumin your body can be dangerous
and harmful to your heart.Although potassium is found insalt substitutes, fruits and veg-etables, milk, meat, chocolateand nuts, fruits and vegetablesare the best choices for keepingpotassium in the normal range.Many on PD are able to eat anorange, half of a banana or onetomato daily to keep theirpotassium in normal range.Milk, chocolate and nuts arehigh in phosphorus and saltsubstitutes are not recom-mended. (3).
For people onPD, fluidsand sodiumrestrictionsare more liberal.Moderateintake of fluidcan helpimprove dial-ysis andflush outwastes.Sodium, a mineral that canaffect your blood pressure, isfound in table salt, canned foodsand processed, pickled andcured foods. It is usually best tolimit table salt and salty foodsto prevent too much fluidweight gain, which can causehigh blood pressure and hearttrouble.
Phosphorus, a mineral found inmilk, cheese, nuts, dried beans,lentils, peas and corn products,is limited in PD. You need totake phosphate binders witheach meal to remove phospho-rus from foods eaten. Caloriesgive your body energy. Most ofyour calories come from thefoods you eat, but with PD thesugar in the dialysate gives youmore calories. Your body takesin the sugar and can causeweight gain (3).
Conventional home HD, similarto in-center HD, is done threetimes a week but at home. Thediet, equivalent to in-center HD,is limited in terms of one’sintake of sodium, potassium,phosphorus and fluids (1).
Daily home HD consists of two-to three-hour treatments donefive to six days a week totalingabout 12 hours of dialysis perweek. Since daily home HD isdone more often, more toxinsand fluid are removed. Those on
daily homeHD haveincreasedenergy levelsanddecreaseduse of bloodpressuremedications.Phosphorus,potassium,sodium andfluid restric-
tions are moreliberal than in-center HD (4).
In nocturnal home HD, treat-ment is done eight to 10 hoursduring the night, six to sevennights a week. One of the bene-fits of nocturnal home HD isthere are almost no dietaryrestrictions. Because phospho-rus removal is improved, manypeople can stop taking phos-phate binders and are encour-aged to eat more phosphate anddairy products. Since dialysis isdone nightly, there is usually nofluid, sodium and potassiumrestriction. Appetite is alsoimproved due to better and fre-quent removal of toxins andwastes. (5, 6, 7) Daily home HDand nocturnal home HD areoffered in limited clinics in theUnited States, Canada andEurope. Studies have shown
many benefits and few disad-vantages (6, 7, 8). Currently, theFederal Government reimburs-es dialysis facilities for threetreatments per week. Some pri-vate insurance companies maycover extra treatments. For noc-turnal and daily HD treatmentsto be used on a larger scale, theFederal Government andCongress need to develop reimbursement methods that support them.(8)
The five types of home dialysishave different dietary consider-ations to think about. Whatevertype of home dialysis youchoose, your health care teamwill continue to be availableand serve as a valuable asset to you.
Valerie Wong, RD, has been apracticing dietitian for 17 years.She currently works as a renaldietitian specializing in PD at an outpatient facility inFresno, CA.
References1. Types of home dialysis.
www.homedialysis.org/v1/types/index.shtml
2. Kidney Directions: Choices.www.kidneydirectins.com/us/patients/choices/periton/twotypes.htm
3. National Kidney Foundation A to ZHealth Guide, Nutrition andPeritoneal Dialysis. www.kid-ney.org/atoz/atozprint.cfm?id=97
4. Curtis, J: Daily short and nightlynocturnal home hemodialysis: stateof the art. Dialysis &Transplantation 33:2:64-71, 2004.
5. Hartwell, L. Nocturnal HomeHemodialysis. 2001 <www.ikid-ney.com/ikidney/Community/Pro2Pro/Clinicians/Printer/NocturnalHomeH
6. Frequently asked questions aboutnocturnal Home Hemodialysis,2000.www.renalweb.com/guest/lit/mwilliams/FAQs.htm
7. Pierratos, A. Nocturnal homehemodialysis: An update on a 5-year experience. Nephrol DialTransplant 14:2835-2840, 1999.
8. Pederson, ML: Discussing finalwishes: nightly home hemodialysis.
9. Aakp. RENALIFE 18:6, 2003.www.aakp.org/AAKP/renalifeArt/2003/finalwighes.htm
Diet Comparisons in Home DialysisBy Valerie Wong, RD
One of the keys to successful home dialysis is following the proper diet.
Many on PD are able to eat anorange, half of a banana or one
tomato daily to keep their potassiumin normal range.

FAMILY FOCUS • Volume 14, Number 2 7
S P O T L I G H T O N M E D I C A R E
IN SPITE OF ALL THATIS SAID AND WRITTENabout its limitations, the
Social Security and Medicaresystems in this country benefitmany people. In fact, ESRD(End Stage Renal Disease) orkidney failure is the only spe-cific disease that allows a per-son to receive Medicarecoverage regardless of age orreceipt of Social SecurityDisability Insurance (SSDI) aslong as he or she is a citizen orpermanent legal resident andhas worked enough to qualifyor can qualify under a spouse’swork record. A child can quali-fy at any age under a parent’swork record. When someonefirst learns they have kidneyfailure and is facing dialysis ora transplant, they are oftenworried about how much treat-ment will cost. It is reassuringto know Medicare will pay formuch of the cost of dialysis or transplant.
When starting treatment forkidney failure, doctors shouldoffer all treatment optionsmedically suited to each per-son’s unique health situationand psychosocial needs, includ-ing center hemodialysis, trans-plantation and home treat-ments—hemodialysis (HD) andperitoneal dialysis (PD). Whenyou are deciding the best treat-ment choice for you and yourfamily, you may be interestedin learning how Medicare paysfor self-care dialysis in a clinicor at home.
If you need dialysis or a trans-plant, you may qualify forESRD Medicare by havingpaid into Social Security andearning enough credits. Howmany credits you need to qual-ify for Medicare based on yourwork depends on your age. Youearn work credits based onhow much you earn in eachcalendar quarter. Every yearthe amount you need to earnto equal one credit goes up.You can read more about earn-ing credits and how many youneed to get Medicare in the
booklet How You Earn Credits.There are two parts toMedicare—Part A and Part B.Part A covers in-patient hospi-tal stays for a certain amountof days after a deductible ismet. Part B covers 80 percentof allowable expenses, aftermeeting a deductible, for avariety of outpatient services,such as dialysis, and physi-cians’ fees if Medicare isresponsible for paying first.You or your secondary insur-ance, such as Medicaid,Medigap or individual healthinsurance, will be responsiblefor the remaining 20 percent. If you are covered by anemployer group insurance, itmust pay first for 30 monthsthat you could have Medicare(whether you chose to takeMedicare or not). If you haveMedicare during this 30months, Medicare may paysome charges left after yourgroup insurance pays. Whenyou have Medicare, your dialy-sis clinic or transplant pro-gram must accept whatMedicare allows as payment infull and cannot bill you for anycharges over that amount forMedicare covered services.
If you qualify for but do notalready have Medicare whenyou start in-center dialysis,your Medicare coverage willnot start until the first day ofthe third full month of dialy-sis. During those first months,if you have other health insur-ance, it will be billed. If youhave no other insurance, yourdialysis clinic will make pay-ment arrangements with you.
However, if you choose to starta self-care in-center or homedialysis training program foreither PD or HD in those firstmonths, your Medicare cover-age can be backdated to start
the first of the month thatyour dialysis began. Medicarecovers home training charges,the dialysis machine (if need-ed) and supplies and minorhome changes to hook amachine into existing plumb-ing and electricity. You mayhave to pay some charges forother changes if needed.
If you choose to do home dialy-sis (HD or PD), you will beasked to choose one of twoMedicare billing options,Method 1 or Method 2. Youreceive all home dialysis serv-ices, equipment and suppliesdirectly from a dialysis facilityunder Method 1. UnderMethod 2, all equipment andsupplies are delivered to yourhome directly from the suppli-er who bills Medicare for them.Your dialysis clinic bills forsupport services from yournurse, social worker, and dieti-tian. If you need help under-standing these options, askyour home training nurse toexplain them to you. Regard-less of whether you chooseMethod 1 or 2, training andongoing clinical support fromyour doctors, nurses, socialworkers and dietitians must beprovided by a Medicare certi-fied ESRD facility.
Whether you have chronic kid-ney disease (CKD) and are noton dialysis or have a trans-plant or have kidney failureand are already having treat-ment, you should talk with thesocial worker at the dialysiscenter about Medicare cover-age of home dialysis. You canalso call or e-mail the PatientServices Professional from theESRD Network in your stateto get more information.
NETWORK 1(CT, ME, MA, NH, RI, VT)Phone: (203) 387-9332
NETWORK 2(NY)ESRD Network of New York, Inc.Phone: (212) [email protected]
NETWORK 3(NJ, PR, VI) Phone: (609) [email protected]
NETWORK 4(DE, PA)Phone: (412) [email protected]
NETWORK 5(DC, MD, VA, WV)Phone: (804) [email protected]
NETWORK 6(GA, NC, SC)Phone: (919) [email protected]
NETWORK 7(FL)Phone: (813) [email protected]
NETWORK 8(AL, MS, TN)(601) [email protected]
NETWORK 9/10(IL, IN, KY, OH)Phone: (317) [email protected]
NETWORK 11(MI, MN, ND, SD, WI)Phone: (651) [email protected]
NETWORK 12(IA, KS, MO, NE)Phone: (816) [email protected]
NETWORK 13(AR, LA, OK)Phone: (405) [email protected]
NETWORK 14(TX)Phone: (972) [email protected]
NETWORK 15(AZ, CO, NV, NM, UT, WY)Phone: (303) [email protected]
NETWORK 16(AK, ID, MT, OR, WA)Phone: (206) [email protected]
NETWORK 17(AS, Guam, HI, Mariana Islands, N. CA)Phone: (415) [email protected]@nw17.esrd.net
Self-Care Dialysis—What Medicare PaysBy Roberta Bachelder, MA
What does Medicare cover? For how long? Your questions are answered here.
Continued on page 11

8 FAMILY FOCUS • Volume 14, Number 2
P E R S O N A L S T O R I E S
AS I LOOK BACK ON 21 YEARS OF HOME
HEMODIALYSIS (HHD), Ihave to say that I believe it isthe dialysis therapy that hasthe potential to give thehealthiest and longest life.Also, I chose HHD because Ido not believe dialysis is some-thing I want to outsource toothers. Who has the greatestinterest in the quality of mydialysis care? I do—thepatient. So keeping control ofmy own treatment has beenmy goal.
When my kidneys failed in1980 at age 34 from heredi-tary kidney disease, I wasvery glad chronic dialysistreatments were available. Iwanted to take full advantageof the opportunity to survive—something my brothers werenot able to do because theirkidney failure occurred at anearlier time when neither thetechnology nor the MedicareEnd Stage Renal Disease(ESRD) program to help payfor dialysis was available. Ichose HHD primarily becauseit allowed me to keep working;I had control of my treatmentschedule, which accommodat-ed my job as a school coun-selor. I considered peritonealdialysis, but inevitably reject-ed it due to often high peri-tonitis (infection) rates. I alsoconsidered transplant, butrejected it as well due to thehigh failure rates of kidneygrafts in the early 1980’s.
After initially choosing HHDin order to keep working, Ilater realized it had other ben-efits. I found that I was betterable to control the quality ofthe treatment I got. I couldavoid infections that can beacquired in a dialysis facility,and I was able to avoid the
psychological toll that some-times happens at an institu-tional environment. I could domy own needle “sticks,” thusbetter preserving my fistula(the original one is now 24years old). I could enjoy usingthe time on dialysis to eat din-ner, read mail and the news-paper and hold my dog in mylap, all in the comfort of myown home. After a couple ofyears my wife and I even fit-ted out an RV for dialysis andtraveled the country while Idialyzed on the campgrounds.
Another important advantageof HHD was the ability to dia-lyze longer and more oftenthan was offered in most dial-ysis facilities. As soon as Ilearned that it is difficult toget too much dialysis andlearned of the high mortalityrate with too little dialysis, Ilengthened my dialysis ses-sions. I did as much as fivehours per session at one time.Later I abandoned the tradi-tional schedule of three timesper week and began dialyzingevery other day for four hoursper session. This schedule notonly gave me more total dialy-sis time, but I also had loweruremic peaks and valleys—Ifelt less washed out after eachtreatment. This regimen alsoallowed me to eat a little moreprotein and my fluid intakewas a little more liberal.
One of the essential keys tomost HHD (an exception maybe nocturnal hemodialysis) isthe availability of a reliablepartner to assist with treat-ments. I am very lucky tohave a wonderful wife whodevoted herself to helping allthese years. Learning to takeover the dialysis treatment athome was pretty scary forboth of us at first, but master-ing it gave us confidence and
allowed us to go onwith a good life togeth-er. We were fortunateto have a trainingnurse who was bothknowledgeable andsupportive. We trainedfor about eight weeksand learned how toperform safe dialysis.We also learned how tomanage emergencies.We were both taughthow to stick the access.At first my wife woulddo one stick and Iwould do the other, butlater I took over all myown sticks.
The first 15 years were prettymuch smooth sailing, and Icontinued working full timewhile maintaining our yardand doing basic home repairs.After 15 years I started toexperience some of theinevitable long-term complica-tions of hemodialysis. I hadjoint pain and had to havecarpal tunnel surgery. I beganto feel the wear and tear of somany years of dialysis, but Iwas getting older too. I was sosuccessful with HHD that oldage finally caught up with me!
Three years ago the advancesin transplantation, coupledwith my long-term complica-tions of dialysis, led me todecide to have a transplant. Ihave done very well and thejoint pain has pretty muchresolved. I am certainly enjoy-ing the freedom of wider trav-el options, and the moreliberal diet is also quite enjoy-able. But, considering therisks involved with a trans-plant, and though I believe Iam doing better with thetransplant, I do not think the difference between goodHHD and a transplant is allthat drastic.
Transplant recipients alwayslive with the possibility of los-ing the graft. But, if I had togo back to dialysis, there is noquestion in my mind that Iwould want to go back to theroad less traveled that leadsback home—back home tocomfort, security, quality, safe-ty and a long survival on dial-ysis: all the things that HHDcan provide. Looking back onit after three years with a suc-cessful transplant, it was agood life. We worked, we vaca-tioned in the RV or on dialysiscruises and we led what weconsidered to be a more regu-lar lifestyle than the otherdialysis options offered us. Forus, choosing the road less traveled HAS made all the difference.
A retired high school counselorfrom Rome, Georgia, GeorgeHarper currently works as acivil mediator. He was onhome hemodialysis for 21years and has had a trans-plant for three years. Hefounded the GeorgiaAssociation of Kidney Patients,Inc., and serves on the editorial advisory board of Nephrology News and Issues.
Good Years on Home HemodialysisBy George Harper, MEd, EdS
21
George and wife Irene hike in Sequoia National Park.

P E R S O N A L S T O R I E S
FAMILY FOCUS • Volume 14, Number 2 9
IT WAS A LITTLE OVERTWO YEARS AGO WHEN
MY DOCTOR TOLD ME thatmy kidney function was so poorI would need dialysis. I criedbecause my health had beensteadily deteriorating for sometime, and this marked a longfeared milestone. The doctordescribed the types of dialysisavailable at my center at thattime, which were in-centerhemodialysis or peritoneal dialysis (PD).
I LIKED THE FREEDOM andpersonal control that PDoffered, so I selected PD. Thereare two types of PD: continuousambulatory peritoneal dialysis(CAPD), which requiresexchanges of fluid a number oftimes during the day, andAutomated Peritoneal Dialysis(APD), which includes continu-ous cycling peritoneal dialysis(CCPD), and involves a numberof exchanges done continuouslyand automatically by a “cycler”machine, usually at night. Theflexibility and freedom of CCPD
appealed to me, so I chose it. Acatheter, through which theexchanges of fluid take place,was placed in my abdomenwithin just a few weeks. Myactual dialysis was started soonthereafter. The therapy was notonly painless but it was hard toeven notice that fluid was flow-ing in and out of my peri-toneum, or abdominal cavity.
I STARTED WITH TREAT-MENTS of 10 hours a day,seven days a week, with sixcycles of the machine occurringduring the 10 hour period. Eachcycle consists of a “fill” ofdialysate into the abdominalarea, a “dwell” time for the fluidin the abdominal cavity of one
to one and a half hours, andthen a drain cycle. Fortunately,I have not had any infections ofmy exit site or abdominal cavityover the past two years.
AS I GAINED EXPERIENCEwith PD, I discovered that Icould control my blood pressureby managing the concentration
of dextrose in the dialysate. Ihave had high blood pressurefor the past 20 years, treatedfirst with one medication, thenfinally with a combination ofdrugs. Now, whenever my bloodpressure goes up, I raise thedextrose concentration, whicheffectively dehydrates me with-out side effects. Of course, anyadjustments that you makeshould be discussed with yourdoctor first.
CCPD GIVES ME A SENSE ofwell-being, improves myappetite and gives me moreenergy. Another benefit is the flexibility of my diet: I have almost no dietary restric-tions (I am not diabetic). For
example, as long as I take myphosphate binders, I can occa-sionally eat moderate amountsof dairy products, tomatoes andnuts. Again, each person’s dietvaries and should be discussedwith your doctor and dietitian.
THE ADEQUACY OF MY PDTREATMENTS is easy to moni-tor, like hemodialysis, with peri-odic blood tests such aspotassium, creatinine andB.U.N. If they are not consid-ered to be in the normal levelsfor me, the doctor makeschanges in my dialysate formu-la or in my number ofexchanges. I visit my kidneydoctor every month to monitormy blood and kidney function.
ANOTHER ADVANTAGE OFPD is the portability of thetreatment. I can travel andbring my dialysis machine,
which is comparable in size toan early-model VCR. When youtravel with your PD machine, be sure to tell your clinic staffabout your plans. If you will beaway for a short time, you cantake the supplies you will needfor treatment with you. If youwill be gone for a longer periodof time, you can alert yourdialysate supplier of the placesyou will visit and they can havethe dialysate solution shippedto your destinations. It is oftena good idea to have the solutiondelivered prior to your visit sothat you can assure it hasarrived prior to departing onyour travels.
GENERALLY, CCPD IS DONEat night while you sleep, so thatcan be a disadvantage for some.In my case, I am an amateurastronomer, and my therapyhas eaten into my availablenighttime observation hours.However, PD is an evolvingprocess and I hope improvedmachines and dialysate willshorten the time required foreach exchange. Already I have a new machine that is muchquieter, making it much easierand more comfortable to sleepwhile dialyzing.
TODAY I REGARD PD as ablessing, which makes my longwait for a transplant quite bear-able. Some people have chosento stay on dialysis, as opposedto being on the waiting list for atransplant, and now I canunderstand why.
Eduardo Colmenares is aretired vice president of amajor national bank. He has aBS from the University ofCalifornia-Berkeley and aMBA from University ofChicago. He currently lives in Chicago.
Eduardo Speaks Out About Peritoneal Dialysis
By Eduardo Colmenares
Eduardo Colmenares
Some people have chosen to stay on dialysis, asopposed to being on the waiting list for a transplant,
and now I can understand why.
To find out about themany services andactivities offered in
your community or tojoin the Patient andFamily Council at no
cost, contact us at
800-622-9010or visit us at
www.nkfkidneypatient.org
MEMBERS GET FAMILY
FOCUS DELIVERED
DIRECTLY TO
THEIR HOMES

IN 2002, 91 PERCENT OFPEOPLE with kidney failure
in the United States did in-center hemodialysis. Only 8percent did peritoneal dialysis(PD), while less than 1 percentdid home hemodialysis (HHD).Most nephrologists (kidneydoctors) say they would choosehome dialysis if their kidneysfailed—and not just becausethey have medical training.(1)Nephrologists are aware of thepositive impact that home dial-ysis can have on people whochoose it, and many believethat home dialysis is used toolittle. In fact, nephrologists saythat survival rates wouldimprove if 25 percent of peopleon dialysis in the UnitedStates did PD and 11 percentdid HHD.(3)
Life Options RehabilitationProgram research has lookedat why some patients live fordecades on dialysis, while oth-ers die earlier. In a study ofpeople who lived for 15 yearsor longer on any type ofhemodialysis, all of the partici-pants were active self-man-agers of their disease and theirtreatment. They learned howthe treatment worked and howto speak up if something waswrong, how to track their labtests, what each of their med-ications was for and how to fol-low their treatment plans.How did they learn so much?Most had done home dialysisat some point in their lives.
Although any type of dialysisyou choose will have a majoreffect on many areas of yourlife, taking charge of yourtreatment is one way to feel ingreater control. You may findthat the benefits of home dial-ysis outweigh its burdens foryou and your family. This arti-cle may help you decide.
TECHNICIANS LEARN DIALYSIS. YOU CAN TOO!Fear of medical tasks scaressome people away from home
dialysis. But most dialysistechnicians have no medicalbackground before they learndialysis. If technicians canlearn to do dialysis, so can you.Dialysis is their job, but it isyour life! You will be able todialyze at home only after yourtraining nurse knows you canhandle it. Once home, you willhave phone back-up andmonthly visits with your doc-tor, nurse, dietitian and socialworker.
SELF-MANAGEMENT ANDSURVIVALEven if you do in-centerhemodialysis and spend 14hours each week at the clinic,the other 154 hours—92 per-cent of your time—you are onyour own to self-manage yourkidney failure. You are self-managing every time you do atreatment, take your medica-tions, follow your diet andfluid limits and report symp-toms. Research shows that ifyou learn a lot about dialysisand take an active role in yourown care, you will be morelikely to feel better and livelonger. Home dialysis is the
highest level of self-manage-ment, which may be one rea-son why people who do homedialysis often live longer.
THE IMPORTANCE OF CONTROLIndependence is a core valuein American culture, but one ofthe first things people feelwhen their kidneys fail is aloss of control over their lives.Home dialysis gives you con-trol over when and where todialyze, room temperature,who is present, whether to eator drink during treatment,how to spend your time whiledialyzing and even whether tolengthen your treatment tofeel better. You can changeyour schedule to fit dialysisinto your life—and you mayhave more energy, so it is easi-er to work full-time. With PD,traveling is easier: you canbring your supplies or havethem shipped. People who doPD or longer or more frequenthemodialysis have a much eas-ier diet and fewer fluid limits.In fact, people on daily HHDor nocturnal HHD may evenbe able to eat a normal diet.Instead of spending time in aclinic, you can spend dialysistime with your own family andfriends.
On the other hand, home dial-ysis has its burdens. Most clin-ics require HHD patients tohave a helper in the homewhen they dialyze, which canlimit a helper’s activities.Needing to cope with emergen-cies, taking deliveries, storingsupplies and dealing withmachine problems are extratasks that people on PD orHHD or their helpers need to
do. Some home dialysis helperseven place hemodialysis nee-dles or do PD exchanges fortheir loved one. Worried aboutthe burden of home dialysis onyour helper? The more you doyourself, the less of a burdenyour helper will feel. If youchoose HHD, you can do back-up dialysis in-center if yourhelper needs a break.
AVAILABILITY OF HOME DIALYSISIn 2004, the nonprofit MedicalEducation Institute launched anew Web site called HomeDialysis Central (www.home-dialysis.org), with the goal ofraising awareness and anincreased use of home thera-pies. As of March 2005, the“Find a Center” database onthe site lists 1,515 clinics withCAPD; 1,485 with CCPD; 319with conventional HHD; 46with daily HHD; and 81 withnocturnal HHD. As new clin-ics open and others add newhome treatments, they add oredit their listing. The growthin clinics offering home treat-ment provides more choices.
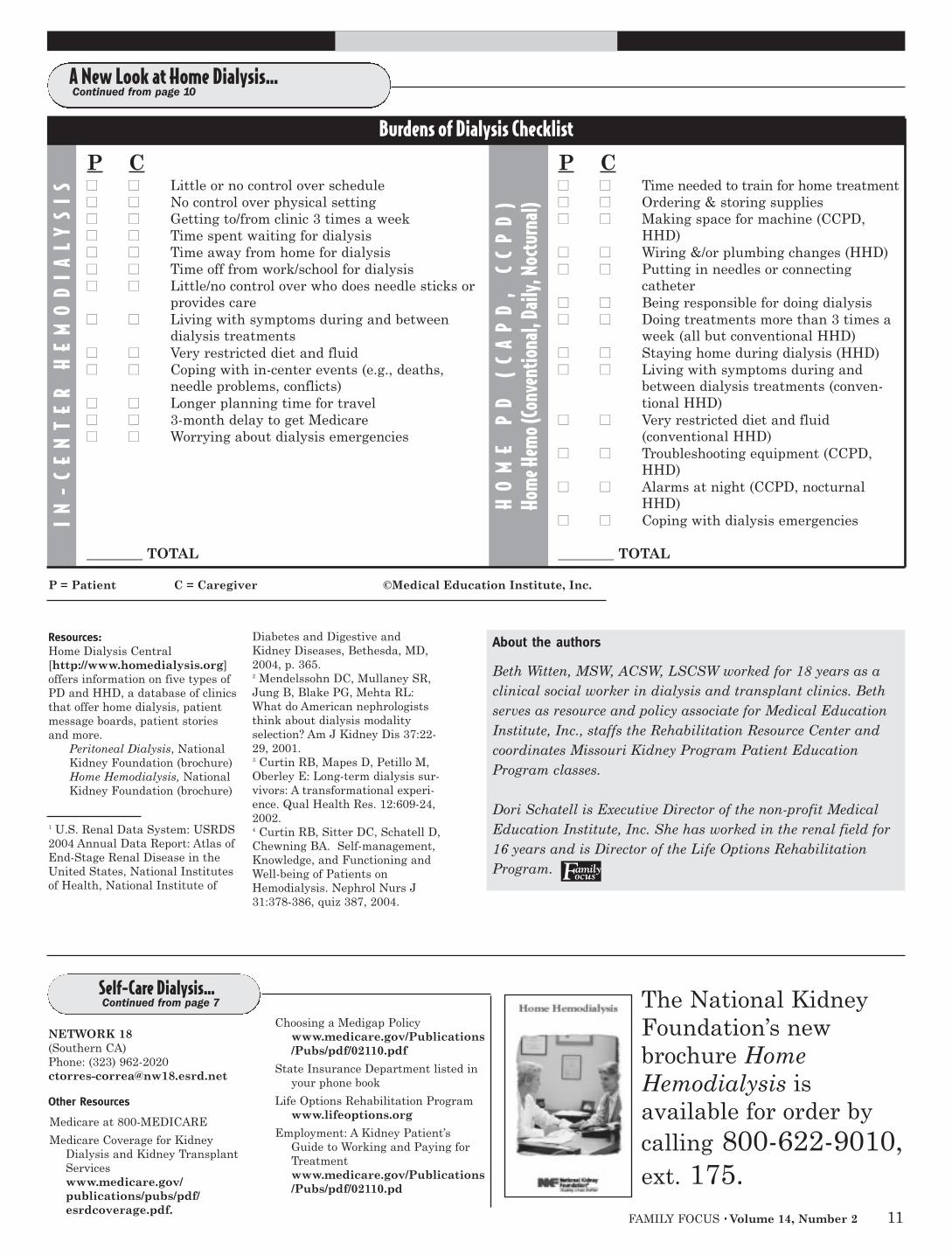
ASSESSING YOUR OWN NEEDSSee if home dialysis would fitinto your life. Use thePatients (P) and Caregivers(C) Checklist on the nextpage. The patient and caregiv-er should each assign 0 (noburden at all) to 10 points(heavy burden) to each item.Add up the points to see whichtype of dialysis is the best fit
10 FAMILY FOCUS • Volume 14, Number 2
A New Look at Home Dialysis:A Psychosocial Perspective
By Dori Schatell, MS and Beth Witten, MSW, ACSW, LSCSW
Choosing home hemodialysis can have positive
psychological results for you. Read on.
T A K I N G C H A R G E O F Y O U R T R E A T M E N T
You are self-managing everytime you do a
treatment, takeyour medications,follow your dietand fluid limits
and report symptoms.
Technicians learn dialysis. You can too!
Continued on page 11
FAMILY FOCUS • Volume 14, Number 2 11
P C�� �� Little or no control over schedule�� �� No control over physical setting�� �� Getting to/from clinic 3 times a week�� �� Time spent waiting for dialysis�� �� Time away from home for dialysis�� �� Time off from work/school for dialysis�� �� Little/no control over who does needle sticks or
provides care�� �� Living with symptoms during and between
dialysis treatments�� �� Very restricted diet and fluid�� �� Coping with in-center events (e.g., deaths,
needle problems, conflicts)�� �� Longer planning time for travel�� �� 3-month delay to get Medicare�� �� Worrying about dialysis emergencies
________ TOTAL
A New Look at Home Dialysis…Continued from page 10
P = Patient C = Caregiver ©Medical Education Institute, Inc.
IN-
CE
NT
ER
HE
MO
DIA
LY
SIS
HO
ME
PD
(C
AP
D,
CC
PD
)Ho
me H
emo (
Conv
entio
nal,
Daily
, Noc
turn
al)
Burdens of Dialysis Checklist
P C�� �� Time needed to train for home treatment�� �� Ordering & storing supplies�� �� Making space for machine (CCPD,
HHD)�� �� Wiring &/or plumbing changes (HHD)�� �� Putting in needles or connecting
catheter�� �� Being responsible for doing dialysis�� �� Doing treatments more than 3 times a
week (all but conventional HHD)�� �� Staying home during dialysis (HHD)�� �� Living with symptoms during and
between dialysis treatments (conven-tional HHD)
�� �� Very restricted diet and fluid (conventional HHD)
�� �� Troubleshooting equipment (CCPD,HHD)
�� �� Alarms at night (CCPD, nocturnal HHD)
�� �� Coping with dialysis emergencies
________ TOTAL
Resources:Home Dialysis Central[http://www.homedialysis.org]offers information on five types ofPD and HHD, a database of clinicsthat offer home dialysis, patientmessage boards, patient storiesand more.
Peritoneal Dialysis, NationalKidney Foundation (brochure)Home Hemodialysis, NationalKidney Foundation (brochure)
1 U.S. Renal Data System: USRDS2004 Annual Data Report: Atlas ofEnd-Stage Renal Disease in theUnited States, National Institutesof Health, National Institute of
Diabetes and Digestive andKidney Diseases, Bethesda, MD,2004, p. 365.2 Mendelssohn DC, Mullaney SR,Jung B, Blake PG, Mehta RL:What do American nephrologiststhink about dialysis modalityselection? Am J Kidney Dis 37:22-29, 2001.3 Curtin RB, Mapes D, Petillo M,Oberley E: Long-term dialysis sur-vivors: A transformational experi-ence. Qual Health Res. 12:609-24,2002.4 Curtin RB, Sitter DC, Schatell D,Chewning BA. Self-management,Knowledge, and Functioning andWell-being of Patients onHemodialysis. Nephrol Nurs J31:378-386, quiz 387, 2004.
About the authors
Beth Witten, MSW, ACSW, LSCSW worked for 18 years as aclinical social worker in dialysis and transplant clinics. Bethserves as resource and policy associate for Medical EducationInstitute, Inc., staffs the Rehabilitation Resource Center andcoordinates Missouri Kidney Program Patient EducationProgram classes.
Dori Schatell is Executive Director of the non-profit MedicalEducation Institute, Inc. She has worked in the renal field for 16 years and is Director of the Life Options Rehabilitation Program.
NETWORK 18(Southern CA)Phone: (323) [email protected]
Other Resources
Medicare at 800-MEDICARE
Medicare Coverage for KidneyDialysis and Kidney TransplantServices www.medicare.gov/publications/pubs/pdf/esrdcoverage.pdf.
Choosing a Medigap Policywww.medicare.gov/Publications/Pubs/pdf/02110.pdf
State Insurance Department listed inyour phone book
Life Options Rehabilitation Program www.lifeoptions.org
Employment: A Kidney Patient’sGuide to Working and Paying forTreatmentwww.medicare.gov/Publications/Pubs/pdf/02110.pd
Self-Care Dialysis…Continued from page 7 The National Kidney
Foundation’s newbrochure HomeHemodialysis is available for order bycalling 800-622-9010,ext. 175.

12 FAMILY FOCUS • Volume 14, Number 2
F A M I L Y F O C U S V O I C E S
Once again, Family FocusVoices featured questions
that related to this issue’stheme, Home Dialysis.Respondents were asked toshare why they had or had notselected a form of home dialy-sis, as well as if this type oftreatment had been offered asa treatment option.
There were 34 total respon-dents, 20 males and 14females. Twenty-five of the 34were offered some form ofhome dialysis with threeinformed only about peritonealdialysis and one told only ofhome hemodialysis. Eight ofthe 25 who were educatedabout a form of home treat-ment being available to themchose to start treatment oncenter hemodialysis, while 15of them selected a home dialy-sis modality. Eight of thosewho responded stated theywere not given the option ofhome hemodialysis. One ofthese individuals sought outinformation independently,however, and is now on homehemodialysis. Three individu-als initially were not offeredany form of home dialysis buttwo of them subsequently haveutilized some form of hometreatment.
The respondents’ reasons forselecting their particular treat-ments varied greatly. As oneindividual stated, “I have beentaught ‘To each their own.’What is right for one may notbe right for another.” That isthe key thing to remember asyou read about the factors that
influenced treatment decisions.Keep an open but criticalmind, and remember that youknow best if any of them arerelevant for you and yourunique situation.
Those who selected centerhemodialysis often referred tothe desire to have a separationbetween dialysis treatmentsand their home environment.One individual who respondedshared, “I liked coming homeand leaving all of the smells,needles, solutions andmachines at the unit.” Anothersaid, “My treatment and myhome were to be kept sepa-rate.” One person voiced con-cern about the emotionalstrain performing homehemodialysis might place onhis family. Storage space fordialysis supplies and equip-ment was a negative factor forothers. Another reason givenfor selecting center dialysiswas that it afforded the oppor-tunity to slow down and relaxafter a busy workday. This per-son preferred to have the cen-ter staff perform the treatment,with the exception of the nee-dle stick, which she chose todo. Hemodialysis needles werethe reason another individualelected to remain in-center.Her particular access proved tobe a challenge even for thedialysis nurses. The ability tohave a closer working relation-ship with the dialysis staff was
why one respondent elected toremain in-center. In addition,several individuals stressedthe importance of having med-ical assistance available shouldan emergency arise. Severalpeople pointed out that havingno one to assist with treat-ments prevented homehemodialysis for them. Oneperson shared that, initially,while seeing people with vari-ous medical situations at the center frightened her, onceshe began dialyzing in the cen-ter those same individualsbecame like family to herthrough their mutual support.Lastly, it was pointed out thatmedical issues can result infewer treatment options.Peritoneal dialysis was not anoption for one individual due to abdominal adhesions.
Several people shared whythey had selected centerhemodialysis over peritonealdialysis. A teenager was con-cerned about how a peritonealcatheter would affect his bodyimage. Another respondentpreferred going to the centerthree days per week, leavingthe rest of his week free fromdialysis.
Some people also expressedwhy they selected peritonealdialysis. Using the cyclerallowed several individuals todialyze at night and work full-time during the day. Someoneelse pointed out that whilebeing on hemodialysis does notprevent full-time employment,it proved problematic for himbecause he frequently did notfeel well following treatment. Aperson who began on continu-ous ambulatory peritonealdialysis (CAPD) but changed toa cycler form of peritoneal dial-ysis shared that not only didthe extra freedom of dialyzing
at night allow her to work full-time, she also attends collegepart time, is active with herchurch and family and exercis-es regularly. She also enjoysbeing in control of her treat-ment. Another reason forselecting peritoneal dialysiswas to avoid the hemodialysisneedles. A woman who oftentraveled preferred the ease ofperitoneal dialysis compared tothe need to arrange hemodialy-sis treatments. Another personexplained how peritoneal dialy-sis allowed her to maintaininterests like fishing andexploring. If an exchange isneeded during those times, shesimply does it in her car (usingsterile technique to avoid infec-tion!) and then resumes heractivity. She also views thetime spent doing an exchangeas a time to relax and taketime for herself. A mother of afour year old with chronic kid-ney disease was directed toperitoneal dialysis because herdaughter retained some kidneyfunction. They were able toperform dialysis while sheslept, thus not restricting heractivity during the day. Theyalso enjoy peritoneal dialysis’fewer dietary restrictions.
A common reason that homehemodialysis was chosen wasthat it offers the ability tomaintain control over one’shealth. Several people chose tolengthen their treatment timeand dialyze more often, result-ing in feeling better physically.Being on home hemodialysisalso means that one does nothave to worry about trans-portation problems. Severalindividuals credited homehemodialysis for allowing themto remain employed full timedue to its scheduling flexibility.Dialyzing in the comfort ofone’s home was another reasongiven for selecting this form oftreatment. One individualdealt with the issue of needingsomeone to assist with treat-ment by hiring a nurse to
Home Dialysis: Is It Right For Me?
By Karren King, MSW, ACSW, LCSW
Family Focus VOICESWE LOVE TO HEAR FROM OUR READERS,so every issue of Family Focus includes a special question.
Read the question below, also posted online at www.familyfocusvoices.org, and let us know what you think.
How do you cope with the mental health challenges related to having CKD?
You may visit the Web site above to share your thoughts, or send your response in writing to:
Family Focus Voices30 East 33rd StreetNew York, NY 10016 Continued on page 13

QUESTIONS THAT AREOFTEN ASKED by people
who are starting an exerciseprogram are “What is the dif-ference between walking, run-ning, swimming or using abicycle, and which one is bestfor me?” There are obvious dif-ferences between them, but theeffect on your heart is just thesame: They are good for you!The specificity training princi-ple states that your body’sshort-term and long-term ben-efits from exercise are specificto the muscles that are beingused during your exercise ses-sion. For example, the musclesin your legs grow stronger asyou run, the muscles in yourback grow stronger when youswim, the muscles in yourarms grow stronger if you usean arm cycle and the musclesin your thighs grow strongerwhen you ride a bike.
Although it is true that specif-ic muscle groups benefit fromexercises that involve thosemuscle groups, there is onemuscle that will always benefitfrom exercise: your heart. Your
heart gets its exercise by beat-ing faster to supply energy tothose working muscles. It doesnot matter which exercise youchoose, as long as you enjoy itand do it safely.
Teadora Mendez is an exampleof someone who is in an activeexercise program while alsobalancing the responsibility oftaking care of her home dialy-sis needs. She is 57 years oldand the proud mother of five
children and grandmother ofsix children. Teadora starteddialysis treatments at her localdialysis center in 2002, butlater switched to home hemo-dialysis. She was trained by a
home training nurse;little by little shelearned how to do home hemodialysis by herself.
When asked about themain reasons for choos-ing home hemodialysisand the impact it hashad on her life, Teadorasays that her doctorrecommended it, so she
did it. She feels that thedoctor’s recommendation wasmade in her best interest, soshe followed his suggestion.Teadora also likes the freedomof not having to go to the dial-ysis center three times a week.“I don’t have to deal with thedialysis center environment,”she says. “At home, my mind iscalm and tranquil, while thegrandkids help me with choresaround the house.”
Teadora underwent coronaryartery bypass surgery in2004. Since the sur-gery, she participatesin a hospital basedrehabilitation programthree times a weeknear her home in LosAngeles. In addition,she takes occasionalwalks outdoors whenCalifornia weather per-mits. When askedabout her attitude andenergy level for exer-cise, she says “Sometimes Ifeel good, sometimes not sogood, but I always put in aneffort to go to the exerciseclass. Sometimes it is difficult
because of the pain in my legsand in my bones, or becausemy blood pressure drops afterthe exercise. I usually justdrink a little bit of soup and Ifeel better. When the pain inmy legs and feet is too high, Itry different exercises that areless painful.
“My legs have problems, pri-marily due to my diabetes, andI know that exercising helpskeep my circulation up and mylegs strong. Also, I’m on thetransplant list and if they callme, I want to be in the bestshape that I can possibly be.”
Finally, I asked Teadora if shehad any advice for others whomight be in a position tochoose among treatmentoptions. “Most importantly iswhat the doctor orders. Iwouldn’t want to change myoption because it is practicalfor me, but I still speak withthe nurse on the phone when Ihave questions. It’s importantto remember that conservingyour body is of primary con-cern and the exercise is a largepercentage of the rehabilita-tion. Every time I speak toany doctor, they always recommend exercise, exercise,exercise!”
Thank you, Teadora!
FAMILY FOCUS • Volume 14, Number 2 13
K E E P I N G F I T
Which Type of Exercise Is Best For You? By Pedro Recalde, MS
Teadora Mendez has learned the key to good CKD health: Exercise!
perform dialysis. She felt homehemodialysis was idealbecause it afforded minimaldisruption in the lives of herthree young children. Severalof those who responded hadput considerable effort intomaking home hemodialysis areality. Since home hemodialy-sis is not offered at every dial-ysis facility, one respondentfaced a lengthy waiting periodto be trained. Another personwas forced to transfer to a newdoctor and dialysis facilitywhere home hemodialysis wasavailable. While researchingtreatment options, one individ-ual arranged to meet withsomeone who was on homehemodialysis. After the meet-ing, not only did this personbegin home hemodialysis,
which allowed her to care fortwo children, work full timeand complete a graduatedegree, she also married thegentleman who had shared hishome dialysis experiences withher! A mother of a nine yearold girl on home hemodialysissummed up her feelings aboutthis form of treatment by say-ing that it had been a “blessingsent from heaven.”
Many of those who answeredour questions had been on sev-eral, if not all, of the availabletreatment options, selectingthem based on their needs andparticular circumstances atthat time. Remember that you,too, have a choice. Make it aninformed one!
Family Focus VoicesContinued from page 12
Teadora works her leg muscles on the stationary bicycle.
Teadora uses an arm ergometer to build upper
body strength.
14 FAMILY FOCUS • Volume 14, Number 2
THE NATIONAL KIDNEYFOUNDATION (NKF) has
joined the two dozen memberorganizations that comprisethe “Kidney Care Partners”coalition to advocate the enact-ment of the Kidney CareQuality and Improvement Actof 2005. The draft legislationwas introduced by SenatorRick Santorum (R. PA) asS.635. The bill number in theU. S. House of Representat-ives is H. R. 1298. The Housebill was introduced byRepresentative Dave Camp (R.MI). Two provisions of theKidney Care Quality andImprovement Act are of particular interest.
Section 401, “Improving theHome Dialysis Benefit,” callsupon the Secretary of Healthand Human Services (HHS) toprovide incentives to improvethe home dialysis benefit forMedicare beneficiaries.Section 402 requires theInstitute of Medicine (IOM) toconduct an evaluation of thebarriers that exist to increas-ing the number of individualswith chronic kidney disease(CKD) who elect to receivehome dialysis services underthe Medicare program. In con-ducting that evaluation theInstitute shall:
Medicare pays dialysis clinicssuch a small fee for home dial-ysis training that many believeit is a disincentive or discour-
ages centers from referring peo-ple to home dialysis. NKF plansto bring that to the attention ofthe IOM panel that will under-take this analysis if and whenthe legislation passes.
Looking at home dialysis fromanother viewpoint, the NationalInstitute of Diabetes and
Digestive and Kidney Diseases (NIDDK) has announced a newresearch study that will be thefirst step towards comparinglong nocturnal (nighttime) dial-ysis at home with conventionalin-center dialysis. This isknown as the “FrequentHemodialysis Clinical Trial.”The research will provide pre-liminary data on the impact oflong nocturnal dialysis on ane-mia, nutritional status, bloodpressure, left ventricular hyper-trophy (enlargement of theheart related to anemia), exer-cise tolerance, medication useand hospitalizations. The fol-lowing Coordinating ClinicalCenters will begin recruitingpatients for this study late inthe summer of 2005:
� The Renal ResearchInstitute in New York City,led by Dr. Nathan W. Levin.
� The University of California,San Francisco, led by Dr.Glenn Chertow.
� Wake Forest University, inWinston-Salem, N.C. led byDr. Michael Rocco.
Finally, Representative JimMcDermott, (D. WA) will bereintroducing the KidneyPatient Daily Dialysis QualityAct in the 109th Congress. Hisproposal would require theSecretary of HHS to publishregulations to establish a pay-ment rate for more frequenthemodialysis done at home. TheSecretary would also need todocument (1) Medicare savingsresulting from more frequenthemodialysis due to fewer med-ications, hospitalizations anddoctor’s visits being needed; and(2) the improved quality of careand improved outcomes thatmore frequent hemodialysismay bring to individuals.
The National KidneyFoundation has advocated fund-ing for the NIDDK FrequentHemodialysis Clinical Trial intestimony to the U. S. House ofRepresentatives and sent a letter of support for Represent-ative McDermott’s bill.
Advocacy Stimulates GovernmentInterest in the Option of Home Dialysis
By Dolph Chianchiano, JD, MPH
The House of Representatives is actively working towards improvements in
home hemodialysis.
L E G I S L A T I V E U P D A T E
Dolph Chianchiano, JD, MPH
(A) Compare current Medicarehome dialysis costs andpayments with current in-center and hospital dialy-sis costs and payments;
(B) Catalogue and evaluate theincentives and disincen-tives in the current reim-bursement system thatinfluence whether individu-als with CKD receive homedialysis services;
(C) Evaluate patient educa-tion services and how suchservices impact treatmentchoices.
Nocturnal HemodialysisContinued from page 4
INDIVIDUALS WHO WANTto do nocturnal dialysis mustbe very interested in takingan active role in their care.One of the biggest problems isfinding a center that offersnocturnal dialysis. In addi-tion, Medicare does not coverall of the extra costs of thistherapy. Supplemental insur-ance may cover some of thecosts not covered byMedicare. Individual unitshave different policies regard-ing coverage of extra costs.
Some centers will absorb thecost, some will only offer the
therapy if there is supplemen-tal insurance and some maybill the patient. A large studysponsored by the federal gov-ernment is now underwaywhich looks at the effective-ness of daily dialysis. If thestudy proves that outcomesare better for people usingdaily dialysis, it is hoped thatMedicare may then pay forthe extra cost. The studybegan in 2004 with someresults hopefully available by2006. This still-preliminary study will compare shortdaily dialysis, nocturnal
dialysis and conventionaldialysis with regards to effica-cy and benefits for those ondialysis. Once these issuesare established, then a largerstudy will be undertaken; itsresults will not be availableuntil about 2008.
About the author:Mary Gellens, MD is Director of Dialysis Servicesand Associate Professor ofInternal Medicine at SaintLouis University in Saint Louis, MO.
FAMILY FOCUS • Volume 14, Number 2 15
JOYCE AND I HAVEENJOYED MANY TRIPS
AND VACATIONS in our 54years together—all of theUnited States and Canada,Europe and Mexico. We hadplans to keep it up until weheard that dreaded word,“dialysis.” We thought thatmeant the end of extendedtravel for sure. NOT SO!
Since we found that it could bedone, we have taken four tripsof three weeks or longer.Actually, I am writing this nowon the balcony of a resort inFort Myers Beach, Florida atthe beginning of a four-weekstay. We have learned a lot,and I would like to share myexperience with other peoplewho are on dialysis.
SUPPLIESPlanning and double-checkingis the key to a no problem trip.Make a checklist! Talk withyour dialysis supplier aboutshipping the solution bags andsome accessories to your desti-nation. When you call, theywill explain the requirements.You will need a confirmationnumber and a person to con-tact at your destination, andyou should speak to the personwho will receive the shipmentto confirm they will accept thesupplies. You will need a sepa-rate bag for your own acces-sories. Among those toconsider are: a flashlight, a 1/4inch piece of plywood (I willexplain why later), an 18 x 24heavy duty extension cord,duct tape, scissors and a penknife.
BY AIR:Plan on checking the accessorybag at the airport and ask fora PRIORITY sticker so it willbe sure to go with you. Expectthis bag to be opened forinspection, so do not lock it.Include a laminated letter byyour doctor explaining the contents.
If you use a cycler machine, itshould always be a carry-on.Have a letter from your doctorexplaining that this is medicalequipment. Your nurse may beable to get a custom case forthe cycler, or you can use anysturdy case and fill out anyspace with foam blocks. Thecycler should be well paddedand protected. You do not wantit to get damaged.
Tell the airline in advance thatyou are traveling with a pieceof medical equipment, andthey will flag your name forspecial attention.
BY CARYou have more flexibility withcar travel. You may need totake the solution bags that youwill need to use on the way;they fit nicely out of the car-tons on your back seat floor.That is the best place for thecycler too. Request a first flooror “Handicapped” room if youstop at a hotel or motel.
IMPROVISINGI mentioned a piece of ply-wood. When the cycler is in anightstand, you need to sup-port the solution bags. If thereis a folding luggage rack, theplywood makes a solid surfacefor this purpose. You can alsoput the plywood on a chair oruse the cardboard insert fromthe cassette carton to bridgebetween two chairs. The cartonitself makes a useful platform.I have even used a motel ironing board. My programrequires one manual exchangeat the end of the cycle.Hauling an IV pole is out ofthe question. You can use thehook on the back of a door. Abathroom hook works well. Youcan use a wire hanger to posi-tion the desired height of thebag. I have used the sectionedpole from a spiral Christmas
tree. Tape an “S” hook to thetop and tape the pole to a chairback or floor lamp. The buttsection of a bait-chasing rodwould work too.
CRUISESUnless you are on hemodialy-sis, the specialized cruises arenot needed. Almost any linewill accept delivery from yourdialysis supplier and willaccommodate you. You must
have very specific deliveryinstructions from the ship per-sonnel to relay to the supplier.The ship should store the sup-plies and bring them to yourcabin as needed.
I do not want to minimize theseriousness of kidney failure. A“normal” life is history for us.But if you are in reasonablygood health otherwise, travel-ing with dialysis is more of anuisance than a handicap. Donot miss out on the funbecause of the inconvenience.
I work out four times per weekat a gym and, when I can,while on the road. It keeps meable to handle the 30-poundcycler. I just turned 80 yearsold in January 2005. If I cando it, you can too!
Richard Hagen has been on PD for 2 1/2 years. He lives inNew Jersey.
Traveling with Peritoneal DialysisBy Richard A. Hagen
Living Donors Web Site
If you are a transplant candidate, you may already knowthat you can receive a transplant in two ways: from adeceased donor (through the national waiting list) or from
a living donor. Living donation is when a living persondonates a kidney, or part of a liver or lung, to another person.Potential donors can find extensive information, support andother resources on the National Kidney Foundation’s Web siteon living donation at www.livingdonors.org
The Web site includes a detailed Q&A section featuring com-monly-asked questions about the process, risks, evaluation,making the decision, the surgery and recovery. Living andpotential donors, as well as their families and friends, canconnect with one another in many different ways through theWeb site. These include a message board, regular onlinechats, an e-mail group and a pen pal program where partici-pants can ask questions, seek support and encouragement orshare their experiences with one another.
Site visitors can also find ways to honor those who havealready donated, learn more about professional conferenceson living donation, sign up for free newsletters and learnabout upcoming events related to donation and transplanta-tion. Please visit www.livingdonors.org to learn more! Formore information about transplantation, visit us atwww.transplantrecipients.org
16 FAMILY FOCUS • Volume 14, Number 2 01-65-1402
* Number of treatment days, hours and exchange times described in this chart represent the average prescription.
Quick Guide to Home Dialysis (cont’d from page 3)
Quick Guide to Home DialysisStandard Short Daily Nocturnal
Home Hemodialysis HemodialysisHemodialysis
CAPD CCPD
*Treatment days (or nights) per week 3 days/week 5-6 days/week 4-6 nights/week 7 days/week 7 nights/week
*Hours per treatment (including average set-uptime before the treatment and clean-up time
after the treatment; set-up time varies with eachmachine)
Machine(s) needed to do treatment Yes No Yes
Water system needed to do treatment Yes No
Type of dialysis access Fistula, graft, or catheter PD Catheter
Needles inserted for the treatment Yes (unless a catheter is used for dialysis) No
Back-up (helper) neededMost home dialysis clinics require that you train with a helper who will stay close by during home treatment. If
you do nocturnal dialysis, you may not need to have a helper.
A helper is not needed for peritoneal dialysisunless the person getting dialysis cannot do the
treatment steps independently.
Maximum training days paid by Medicare.(Payment policies may vary depending on your
Medicare payer or fiscal intermediary)
Medicare pays for approximately 3 training treatments perweek for a month. If more days are needed, an exception
request can be submitted,
15 days (If more days are needed, an exceptionrequest can be submitted to Medicare.)
Space and storage needs Machine, water system and supplies Supplies Machine and supplies
Plumbing/electrical changes May be necessary for home hemodialysis (Ask the home dialy-sis unit that is responsible about minor changes that may be
needed to accommodate home dialysis.)No Grounded electrical
outlet
Utilities neededHome hemodialysis requires water, plumbing and electricity. Peritoneal dialysis requires running
water for hand washing.
Possible increase in water or electrical bills Yes No Yes
4-6 hours Set-up=30-45 min. After=30-45 min.
21/2-3 hours Set-up=30-45 min. After=30-45 min.
6-8 hoursSet-up=30-45 min. After=30-45 min.
4-5 bag exchangesspaced evenly
throughout the day (About 30-45
min./exchange).
7-10 hoursSet-up=30-45 min.After=30-45 min.