hlhs foundations of care from fetus to fontan: fetal ... · texas birth defects registry atz am....
TRANSCRIPT

John M. Costello, MD, MPHProfessor of Pediatrics
Northwestern University Feinberg School of Medicine
Director, Inpatient Cardiology
Medical Director, Regenstein Cardiac Care Unit
Ann & Robert H. Lurie Children’s Hospital of Chicago
PCICS 12th Annual International Meeting
December 9, 2016
HLHS Foundations of Care From Fetus to Fontan:
Fetal Considerations & Delivery

Stage 1
Bidirectional Glenn
Fontan
Transplant?
HLHS Journey

HLHS Journey:Reality for some patients
Interstage mortality
Fontan takedown
Unplanned
reinterventions
Preoperative death
CNS injury
IUFD
NEC
PLE
Plastic
Bronchitis
Arrhythmia

HLHS Fetal Considerations & Delivery Outline:
• In-utero physiology:
• New data- enhance understanding
• Impact on end-organs
• Modifiable ?
• Prenatal dx- impact postnatal outcomes
• Timing & location of delivery

HLHS:Prenatal Diagnosis Rates
Multicenter Study Rate Population
Morris SA. Circ 2014
39%Texas Birth Defects
Registry
ATZ AM. JTCVS 2010
75% SVR trial
Van Velzen CL. BJOG 2016
97%Netherlands:
national screening

HLHS: Potential Benefits of Prenatal Dx
• Counseling
– Screening for non-cardiac anomalies
– TOP:
• 12-48% after seen in quaternary cardiac center
• Actual TOP rate for prenatal dx <24 weeks in community likely higher
• Planning for delivery
• Fetal therapies
Beruokhim RB Ultra Obst Gyn 2015; Rychik J Ultra Obst Gyn 2010; Kipps AK AJC 2011

Fetal PhysiologyNormal
Sun L. Circulation 2015
HLHS

Hypothesis: abnormalities related to ↓O2
and/or substrate deliveryLimperopoulos C. Circulation 2010
N-acetylaspartate / choline ratioTotal brain volume
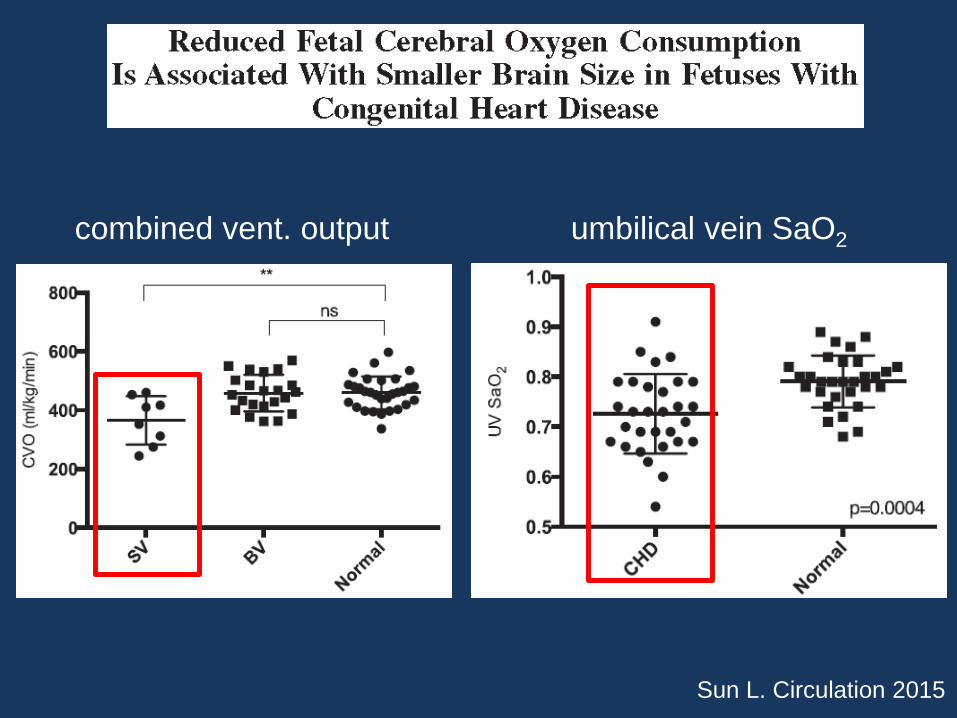
Sun L. Circulation 2015
umbilical vein SaO2combined vent. output
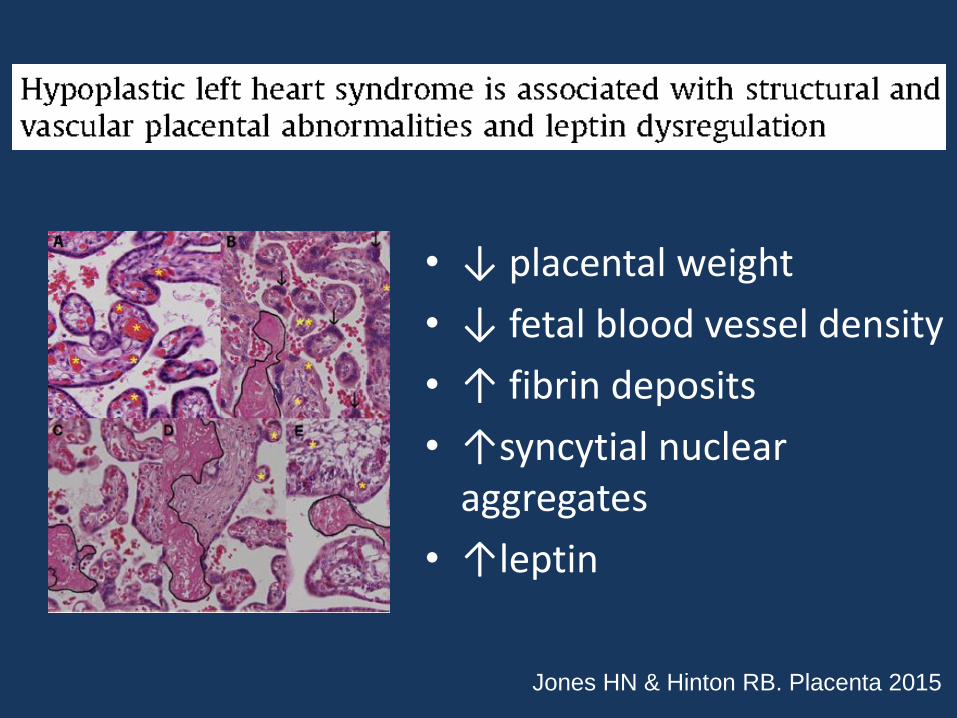
• ↓ placental weight
• ↓ fetal blood vessel density
• ↑ fibrin deposits
• ↑syncytial nuclear aggregates
• ↑leptin
Jones HN & Hinton RB. Placenta 2015
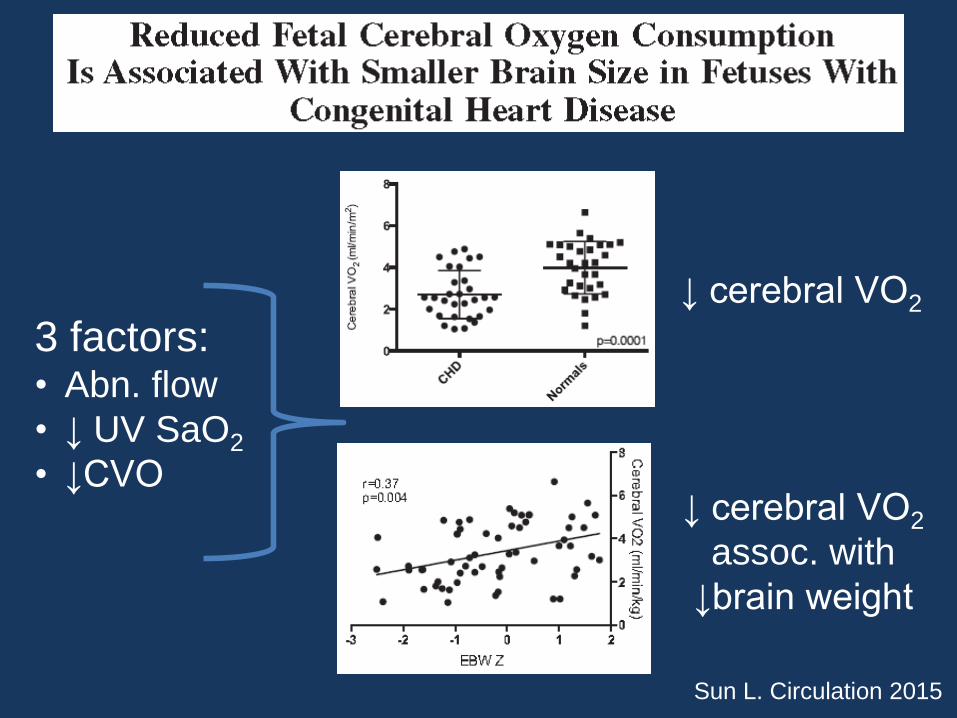
Sun L. Circulation 2015
↓ cerebral VO2
↓ cerebral VO2
assoc. with
↓brain weight
3 factors:• Abn. flow
• ↓ UV SaO2
• ↓CVO
Can maternal therapies improve outcomes in fetuses with HLHS?

Lara DA, Morris SA. US Ob Gyn 2016
ACUTE maternal
hyperoxygenation
CHRONIC maternal
hyperoxygenation

Trial of Maternal O2 Thpy in Fetal “Left Heart Hypoplasia”
• PI: Shane Morris (Baylor)
• RCT: 4L O2 vs. room air
• Primary outcomes: fetal MV & AoV growth
• Secondary outcomes:
– Brain maturation score & CNS injury (postnatal MRI)
– Neurodevelopmental outcomes
– Fetal neurosonogram & brain MRI indices
ClinicalTrails.gov NCT02965638

Fetal Echo at 24 weeks Fetal Echo at 36 weeks
Evolution to HLHS
L. Freud / W. Twortezky
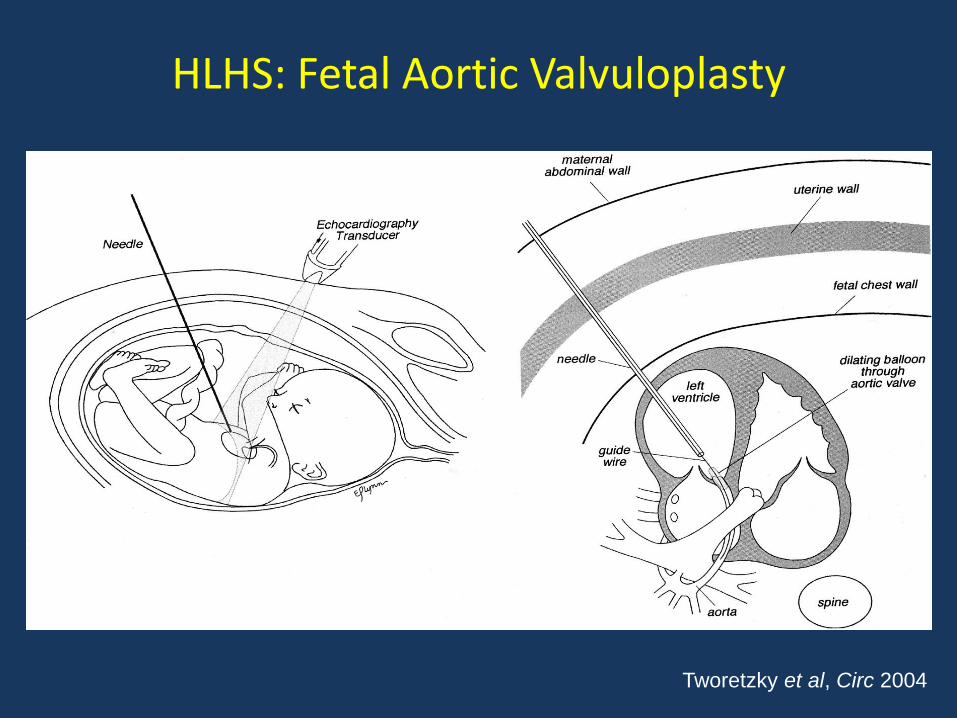
HLHS: Fetal Aortic Valvuloplasty
Tworetzky et al, Circ 2004

L. Freud / W. Twortezky

Circulation 2014

Moon-Grady AJ. JACC 2015

HLHS:Highly Restrictive or Intact Atrial Septum
• ~ 5% of HLHS
Frommelt MA. Clin Perinatal 2014
Atz AM AJC 1999
Vlahos AP. Circulation 2004
Vida VL . ATS 2007

• 21 attempts
• 19 technically successful
– 2 in-utero demise
• 12/19 required urgent postnatal intervention
– 58% stage 1 survival Prenat Diagn 2008

• 9 attempts:
– 4 successful stent placements
– 1 in-utero demise
– 4 of 8 live births died as neonates
Cath Cardiovasc Int 2014

Moon-Grady AJ. JACC 2015
Does prenatal diagnosis improve postnatal outcomes in
fetuses with HLHS?

Thakur V. Prenatal Diagnosis 2016
Pre-op
vasoactive
meds
Pre-op RV
dysfunction ≥
moderate

Thakur V. Prenatal Diagnosis 2016
Pre-op
mortality
Post-op
mortality


• 1999 – 2007: Texas Birth Defects Registry
• 463 births with isolated HLHS
• Prenatal diagnosis: 39%
• Driving time from delivery hospital to cardiac center varied based on prenatal diagnosis:
– Yes: median 3 min. (IQR 1-10)
– No: median 29 min. (IQR, 10-136)Circulation 2014

• Of 463 neonates, 123 (27%) died in first month of life
– 36% of deaths occurred prior to surgery
Circulation 2014

• Independent risk factors for mortality:
– Pre-transport: • Greater driving time to cardiac surgical center
• Low birth weight
• Earlier birth year
– Pre-stage 1:• Greater driving time to cardiac surgical center
• Low HLHS volume cardiac surgical center (trend)
– Surgical:• Low HLHS volume cardiac surgical center
• Earlier birth year
• To improve outcomes:
– Better fetal detection rates (only 39% in this study)
– Delivery near high HLHS volume center
Morris Circulation 2014

Fetus with HLHS:Timing of Delivery?
Fetal
Outcomes:↓ IUFD
Neonatal
Outcomes:↓early delivery
↓LBW

• IUFD 74/1,584 (4.6%)
• Independent risk factors:– Cardiomegaly
– Hydrops
– Pericardial effusion
– Extracardiac anomalies
– IUGRPediatr Cardiol 2014

HLHS: IUFD Rates
3 / 176 (1.7%)J Ultrasound Med 2005
US Obstet Gynecol 2010 3 / 240 (1.2%)
All IUFDs had
risk factors!

Fetus with HLHS:Timing of Delivery?
Fetal
Outcomes:↓ IUFD
Neonatal
Outcomes:↓early delivery
↓LBW
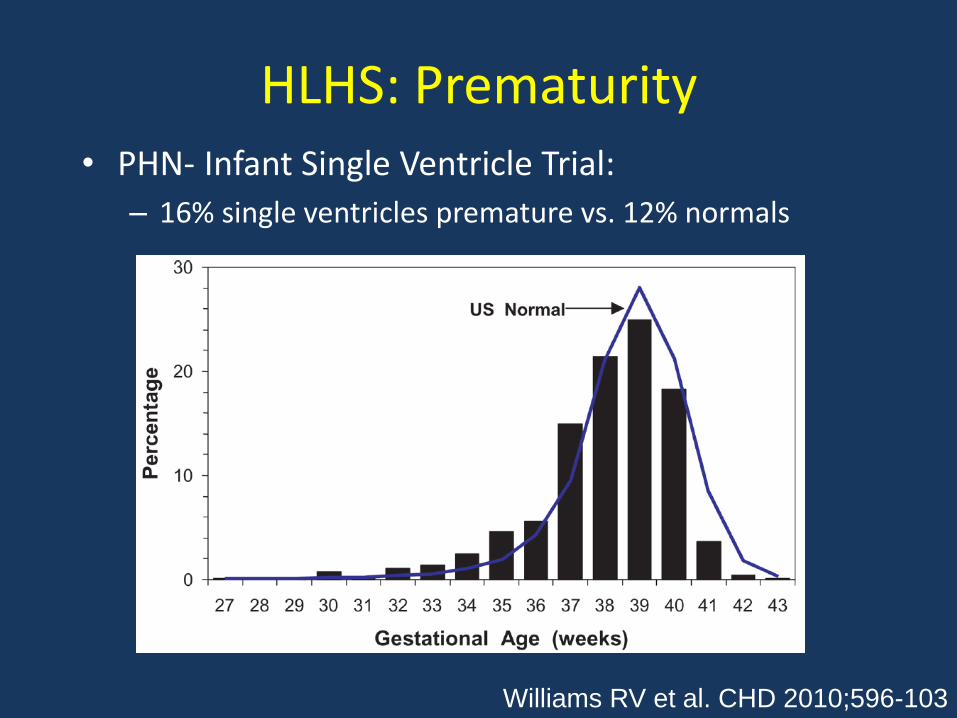
HLHS: Prematurity• PHN- Infant Single Ventricle Trial:
– 16% single ventricles premature vs. 12% normals
Williams RV et al. CHD 2010;596-103

Prematurity:Traditional Definition
PREMATURE
(PRETERM)TERM
POST
TERM
24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44
Weeks Gestational Age at Birth
Data???

Circulation 2014
• Early term birth assoc. with greater:
– Executive dysfunction
– ADHD
– Psychiatric problems
2016
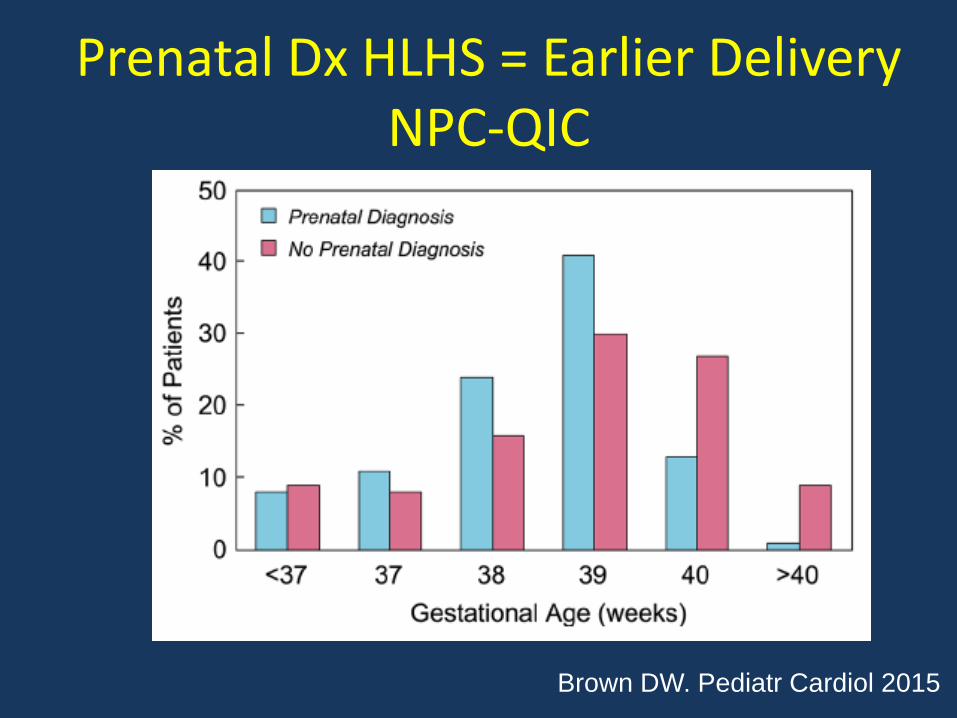
Prenatal Dx HLHS = Earlier DeliveryNPC-QIC
Brown DW. Pediatr Cardiol 2015

Donofrio MT Circulation 2014
“…. elective induction of fetuses with CHD before39 weeks is not recommended unless there arepatient-specific obstetric or logistical issues orfetus-specific concerns about well being.”
“The … management for other conditionsassociated with the evolution of fetal heart failureand sudden demise … has not, to date, been fullyevaluated”

Inferences
• Abnormal HLHS fetal physiology associated with delayed CNS maturation & development
– Likely contributes to ND outcomes
• Benefits of fetal therapies remain unproven
• Prenatal diagnosis a valuable tool
– Responsibility used for counseling & planning of delivery
Inferences
• Fetuses with HLHS at ↑ risk for early delivery
• Births <39 weeks gestation associated with– ↑ neonatal morbidity & mortality
– Adverse ND outcomes
• Fetal cohort studies:– Isolated HLHS may safely progress to 39 weeks
– Those with NCA, genetic anomalies, and/or severe AVVR: ↑ risk for IUFD; optimal monitoring & mgmt. unknown

Thank You