hit policy committee consumer empowerment workgroup – kickoff meeting march 19, 2013 3:00 – 4:00...
TRANSCRIPT

HIT Policy Committee
Consumer Empowerment Workgroup – Kickoff Meeting March 19, 20133:00 – 4:00 PM Eastern
2
Agenda
• Welcome • Introductions• Charter and Scope• Process and Procedures for Federal Advisory Committee
Workgroups• Review Initial Task• Context:
– Patient/family engagement in Meaningful Use – Standards work on shared care plan
• Outlining a Work Plan• Public Comment
3
Welcome & Introductions
• Christine Bechtel, Chair, Consumer Empowerment WG
• Leslie Kelly Hall, Chair, Consumer Technology WG
• Lygeia Ricciardi, Director, Office of Consumer eHealth, ONC
• Introductions by WG members – (<1 min each)
Consumer Empowerment Workgroup (WG)Members
WG Members • Christine Bechtel, National Partnership for
Women & Families (Chair)• Korey Capozza, HealthInsight• James Cartreine, Brigham and Women's
Hospital/Harvard Medical School• Scott Fannin, Greenway Medical
Technologies• Leslie Kelly Hall, Healthwise• Katherine Kim, San Francisco State
University• Sarah Krug, Society for Participatory
Medicine • Rita Kukafka, Columbia University• Patricia MacTaggart, George Washington
University
• Beth Morrow, Children’s Partnership• Jan Oldenburg, Aetna• Casey Quinlan, Mighty Casey Media LLC• Clarke Ross, Consortium for Citizens with
Disabilities • Mark Savage, Consumers Union • MaryAnne Sterling, Sterling Health IT
Consulting, LLC • Ann Waldo, Wittie, Letsche & Waldo LLP• Ryan Witt, drchrono inc
Ex Officio Members • Terry Adirim, HRSA• Cynthia Baur, CDC• Bradford Hesse, NIH• Kim Nazi, Veterans Health Administration• Danielle Tarino, SAMHSA• Teresa Zayas Caban, AHRQ
4

5
Charge & Scope
• Charge: Provide recommendations on policy issues and opportunities for strengthening the ability of consumers, patients, and lay caregivers to manage health and health care.
• Scope: – Examples of policy issues the WG may engage in include patient generation
of their health data, co-managing and sharing care plans, patient reconciliation of medical records from various sources, and new types & sources of patient data.
– Important touch points with other workgroups:• HITPC Meaningful Use WG• HITPC Privacy & Security Tiger Team WG• HITPC Quality Measures WG• HITSC Consumer Technology WG

6
Process & Procedures for FACAs and Workgroups
• HIT Policy Committee gives advice to the National Coordinator for Health Information Technology, the recommendations are not binding.
• HIT Policy Committee is a Federal advisory Committee subject to the Federal Advisory Committee Act (FACA).
• Workgroups cannot provide advice or recommendations directly to ONC, they only report to the parent Committee
• All Workgroup meetings are open to the public, and the public may make comments at the close of the meeting
• Majority of the Workgroup calls are held virtually with possible in person meetings, listening sessions or hearings
• Detailed minutes are kept for each meeting and are posted on the ONC website along with all meeting materials
• All official calendar appointments and meeting materials are distributed from the ONC FACA Meetings email account
HIT Policy Committee & Workgroups
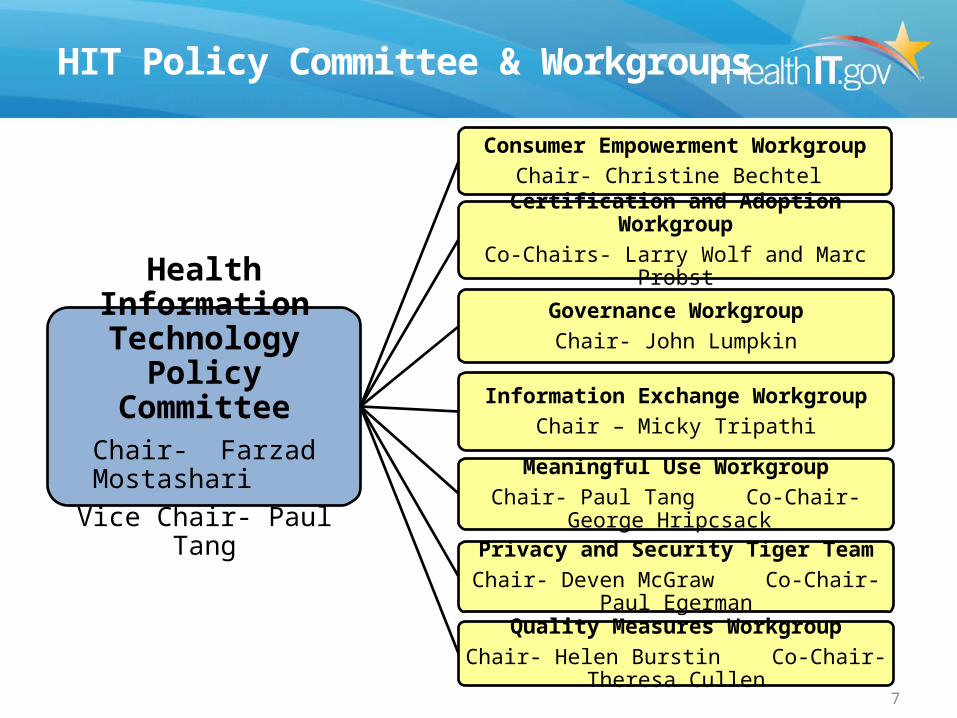
Health Information Technology Policy
CommitteeChair- Farzad Mostashari
Vice Chair- Paul Tang
Consumer Empowerment WorkgroupChair- Christine Bechtel
Certification and Adoption WorkgroupCo-Chairs- Larry Wolf and Marc Probst
Governance WorkgroupChair- John Lumpkin
Information Exchange WorkgroupChair – Micky Tripathi
Meaningful Use WorkgroupChair- Paul Tang Co-Chair- George Hripcsack
Privacy and Security Tiger TeamChair- Deven McGraw Co-Chair- Paul Egerman
Quality Measures WorkgroupChair- Helen Burstin Co-Chair- Theresa Cullen
7
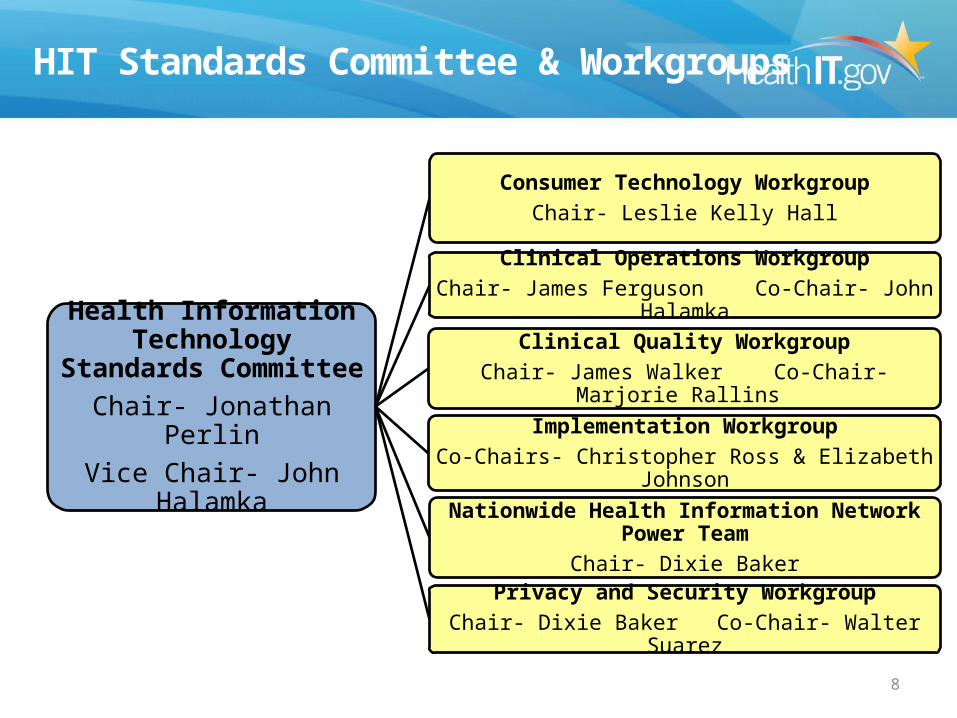
HIT Standards Committee & Workgroups
Health Information Technology Standards
CommitteeChair- Jonathan Perlin
Vice Chair- John Halamka
Consumer Technology WorkgroupChair- Leslie Kelly Hall
Clinical Operations WorkgroupChair- James Ferguson Co-Chair- John Halamka
Clinical Quality WorkgroupChair- James Walker Co-Chair- Marjorie Rallins
Implementation WorkgroupCo-Chairs- Christopher Ross & Elizabeth Johnson
Nationwide Health Information Network Power TeamChair- Dixie Baker
Privacy and Security WorkgroupChair- Dixie Baker Co-Chair- Walter Suarez
8
9
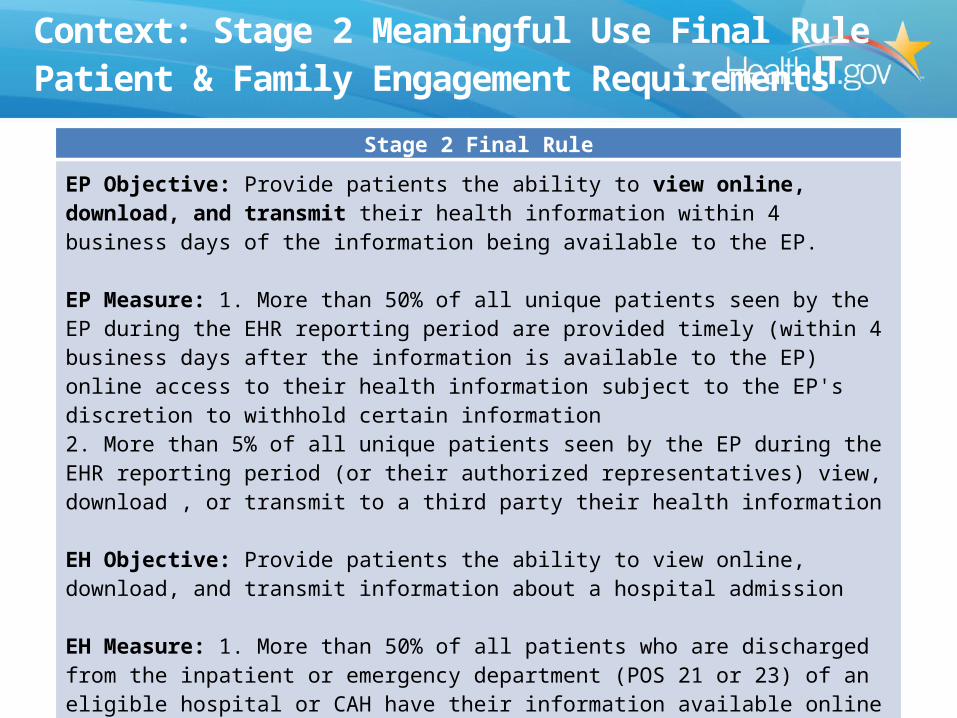
Stage 2 Final Rule
EP Objective: Provide patients the ability to view online, download, and transmit their health information within 4 business days of the information being available to the EP.
EP Measure: 1. More than 50% of all unique patients seen by the EP during the EHR reporting period are provided timely (within 4 business days after the information is available to the EP) online access to their health information subject to the EP's discretion to withhold certain information2. More than 5% of all unique patients seen by the EP during the EHR reporting period (or their authorized representatives) view, download , or transmit to a third party their health information
EH Objective: Provide patients the ability to view online, download, and transmit information about a hospital admission
EH Measure: 1. More than 50% of all patients who are discharged from the inpatient or emergency department (POS 21 or 23) of an eligible hospital or CAH have their information available online within 36 hours of discharge2. More than 5% of all patients (or their authorized representatives) who are discharged from the inpatient or emergency department (POS 21 or 23) of an eligible hospital or CAH view, download or transmit to a third party their information during the reporting period
Context: Stage 2 Meaningful Use Final RulePatient & Family Engagement Requirements
10
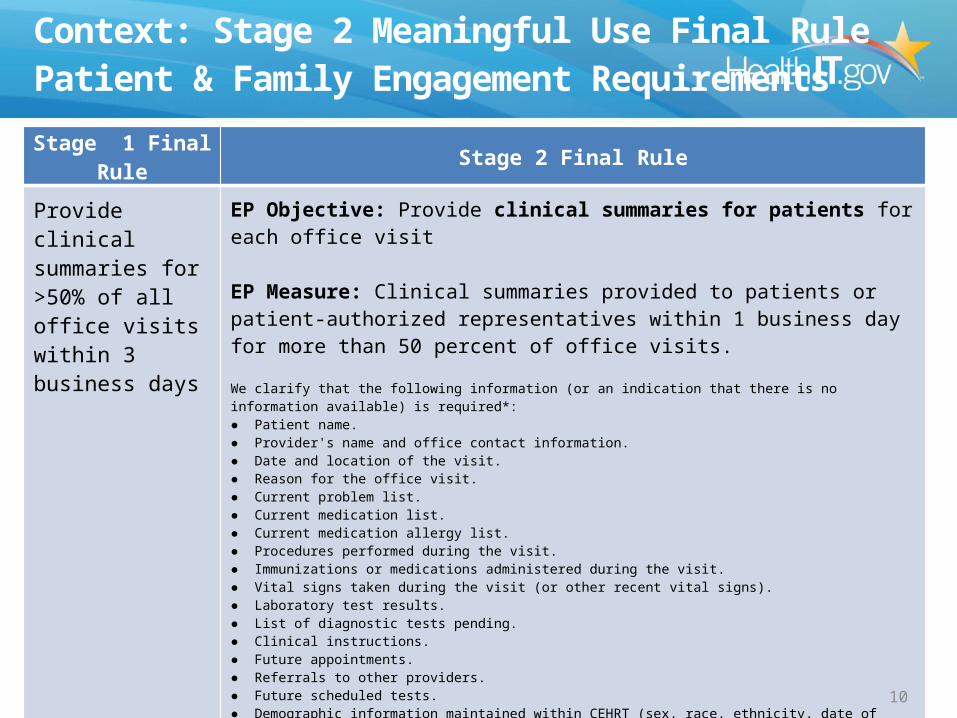
Stage 1 Final Rule Stage 2 Final RuleProvide clinical summaries for >50% of all office visits within 3 business days
EP Objective: Provide clinical summaries for patients for each office visit
EP Measure: Clinical summaries provided to patients or patient-authorized representatives within 1 business day for more than 50 percent of office visits.We clarify that the following information (or an indication that there is no information available) is required*:● Patient name.● Provider's name and office contact information.● Date and location of the visit.● Reason for the office visit.● Current problem list.● Current medication list.● Current medication allergy list.● Procedures performed during the visit.● Immunizations or medications administered during the visit.● Vital signs taken during the visit (or other recent vital signs). ● Laboratory test results.● List of diagnostic tests pending.● Clinical instructions.● Future appointments.● Referrals to other providers.● Future scheduled tests. ● Demographic information maintained within CEHRT (sex, race, ethnicity, date of birth, preferred language).● Smoking status ● Care plan field(s), including goals and instructions. ● Recommended patient decision aids (if applicable to the visit).
*an EP could withhold information from the clinical summary if they believe substantial harm may arise from its disclosure through an after-visit clinical summary
Context: Stage 2 Meaningful Use Final RulePatient & Family Engagement Requirements
10
11
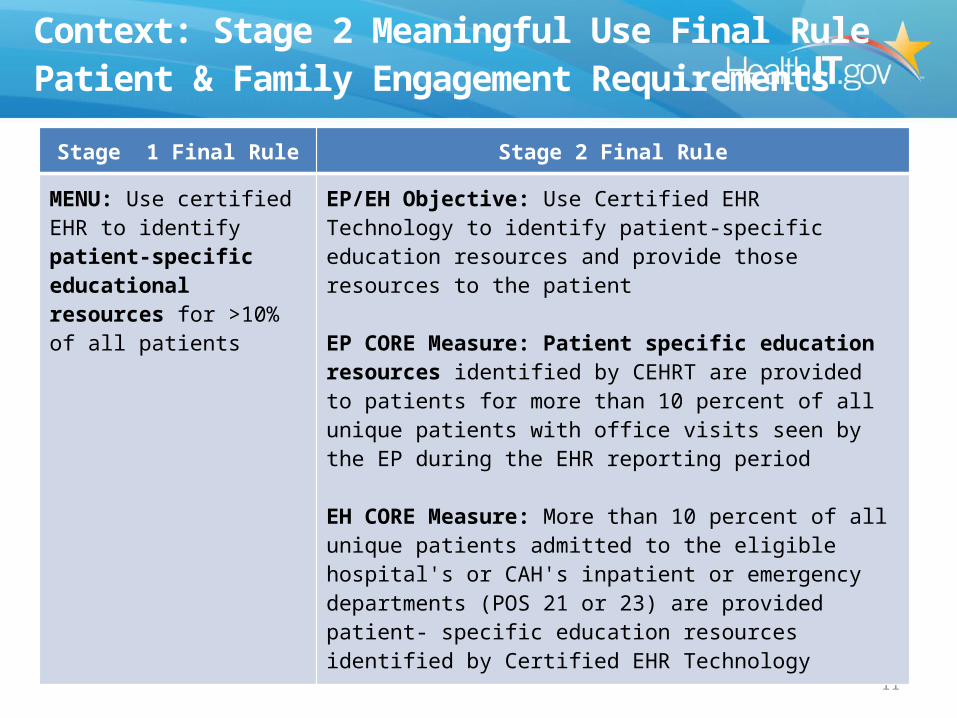
Stage 1 Final Rule Stage 2 Final Rule
MENU: Use certified EHR to identify patient-specific educational resources for >10% of all patients
EP/EH Objective: Use Certified EHR Technology to identify patient-specific education resources and provide those resources to the patient
EP CORE Measure: Patient specific education resources identified by CEHRT are provided to patients for more than 10 percent of all unique patients with office visits seen by the EP during the EHR reporting period
EH CORE Measure: More than 10 percent of all unique patients admitted to the eligible hospital's or CAH's inpatient or emergency departments (POS 21 or 23) are provided patient- specific education resources identified by Certified EHR Technology
Context: Stage 2 Meaningful Use Final RulePatient & Family Engagement Requirements
12
Stage 2 Final RuleEP Objective: Use secure electronic messaging to communicate with patients on relevant health information
EP Measure: A secure message was sent using the electronic messaging function of Certified EHR Technology by more than 5 percent of unique patients (or their authorized representatives) seen by the EP during the EHR reporting period
Context: Stage 2 Meaningful Use Final RulePatient & Family Engagement Requirements
13
Shared Care Plan: Proposed for Future Stage
Stage 3 Request for Comment (Proposed for Future Stage)EP/ EH / CAH Objective: EP/ EH/CAH who transitions their patient to another site of care or refers their patient to another provider of care
For each transition of site of care, provide the care plan information, including the following elements as applicable:
•Medical diagnoses and stages •Functional status, including ADLs •Relevant social and financial information (free text) •Relevant environmental factors impacting patient’s health (free text) •Most likely course of illness or condition, in broad terms (free text) •Cross-setting care team member list, including the primary contact from each active provider setting, including primary care, relevant specialists, and caregiver •The patient’s long-term goal(s) for care, including time frame (not specific to setting) and initial steps toward meeting these goals •Specific advance care plan (Physician Orders for Life-Sustaining Treatment (POLST)) and the care setting in which it was executed. For each referral, provide a care plan if one exists
Measure: The EP, eligible hospital, or CAH that transitions or refers their patient to another site of care or provider of care provides the electronic care plan information for 10% of transitions of care to receiving provider and patient/caregiver.
Certification Criteria: Develop standards for a shared care plan, as being defined by S&I Longitudinal Coordination of Care WG. Some of the data elements in the shared care plan overlap content represented in the CDA. Adopt standards for the structured recording of other data elements, such as patient goals and related interventions
14
Initial Task: Shared Care Plans
• Elements of a care plan in clinical summaries for stage 2:– Care plan field, including goals and instructions. – Care team including the primary care provider of record and any
additional known care team members beyond the referring or transitioning provider and the receiving provider.
• Growing demand for EHRs to support Shared Care Plans– Raises a host of issues, including what is a care plan? How
should consumers and caregivers update these plans, share them, author or co-author, etc.?
– S&I Framework has a significant focus on care plans

15
Context: Standards Activities on Shared Care Plans
•Parsimony is a common theme for standards; many complement each other• VDT, publish and subscribe: C-CDA DIRECT• Longitudinal Care Plan: C-CDA• Patient generated health data HL-7: C-CDA• CDISC; roles team members: PGHD C-CDA• HL7 CDISC: enroll in trials and research• DIRECT: provider to/from consumer and team• IOM: shared decision making interoperability HL7
16
Outlining a Work Plan and Next Steps
• Identify issues related to care plans that WG will tackle– Next WG meeting will dive into care plans
• Briefing from ONC on projects that may raise policy issues for WG to address
• Identify and prioritize other topics that WG would address in the future