history and growth of health economics associations · history and growth of health economics...
TRANSCRIPT

1
History and Growth of Health Economics Associations Thomas E. Getzen, iHEA and Temple University (emeritus) getzen@ temple.edu draft 02 June 2014 6604 words
Emergence of Health Economics as a Sub-Discipline …..1
Table 1 Timeline Size: Estimating the number of Health Economists …..3 Scale: From Departmental Seminar to World Congress .....5 Scope: Economics, Health Econ and Health Services Research .....5 The History of iHEA …..7
Table 2 Growth of iHEA Past as prelude: (iHEA 2020) …..9 Notes & References ....10 -------------------------------------------------------------------------------------------------------------------------- Health economics has achieved a level of growth and maturity barely imagined a generation ago. There are textbooks, journals, conferences, research units and occasionally distinct academic departments. Forget (2004) laments the lack of historical consciousness among health economists. This report attempts to fill parts of that gap by describing the development of academic associations in health economics. It estimates the growth in the number of participants and briefly considers changes in scope and disciplinary boundaries, then examines the establishment of iHEA, the International Health Economics Association in somewhat greater depth. Its primary purpose is to serve as background for planning the future of iHEA and related association in the field of health economics. Examples are taken mainly from developments in the US and UK, with limited references to Europe and the rest of the world since there are no comprehensive intellectual histories for health economics as a field of study or set of academic organizations, and the author is most familiar with experiences and grey literature within that narrower scope. As can be expected of a mature field, the greatest expansion is now occurring in emerging markets in Asia, Latin America, Africa and Eastern Europe. The field has changed immensely in this process, and it is no longer exactly what the prime movers imagined it to be.
Some health economists set the “start date” at the publication of Kenneth Arrow’s “Uncertainty and the Welfare Economics of Medical Care” in 1963. To do so is to ignore the development of national health accounting (Committee on the Cost of Medical Care, 1933; Guillebaud Report 1952), cross-national comparisons (Dublin, 1928; various ILO reports) and hundreds of cost-benefit studies carried out in public health and clinical diseases over the prior fifty years (Weisbrod, 1961) . Hebert Klarman’s (1979) review essay begins “Economists were working on health care long before there was a sub-discipline called health economics,” and goes on to describe the activities of the CCMC researchers starting in 1926, the formation of a bureau of Medical Economics within the AMA in the 1930s, Friedman and Kuznets’ research on physician incomes (part of the national income accounting effort and empirical basis for the permanent income hypothesis), organized sessions on medicine an health at the AEA meetings in 1950 and 1955, and other activities before “a watershed period (1961-1962), when the newly renamed sub-discipline of health economics emerged as a visible entity.”
Almost all of the efforts described by Klarman were within the U.S., and a similar parochialism seems characteristic of early work in other nations. The first international health

2
economics congress was organized by the IEA in 1973, but a far more important driver of international collaboration was development of health accounts by J-P Poullier in the 1970s (OECD 1977, 1986). Even though cross-national studies had previously been undertaken by Brian Abel-Smith in 1963 and 1967, and replicated by Joseph Newhouse (1977) and others, making a large database publicly available that compiled comparable information on multiple variables in many nations facilitated international collaborations among scores of researchers.
The growth of health economics was accompanied by, and amplified by, the formation of health economics associations and publications (HESG, Journal of Health Economics, iHEA, etc.). Government research and data gathering activities were ongoing by 1960 in Ministries of Health, Ministries of Finance, the World Bank and WHO, and numerous economic studies were carried out by medical and insurance societies, yet none of the voluntary associations specifically for health economics that are currently active were organized until later, and in some cases, much later. However, it is evident that gatherings of economists to discuss health issues and review each other’s research in national and international settings were taking place long before any formal organization for “health economists” had been created even where documentation of such meetings is thin and not readily accessible.
Graduate training in the 1960s and 1970s was strongly influenced by two universities, York in the UK and Harvard in the USA. Allan Williams, Tony Culyer and others established the Health Economics Study Group (HESG) before 1975 as a means of training students and reaching out to other universities. Its history is detailed in a lengthy study published by Bronwyn Croxson (1998) for their 25th Anniversary. Offspring from that seminal group include the Nordic, Canadian and Australian associations, all of which were ongoing by the 1980s.
A heath research section affiliate (HERO) of the American Economic Association was begun by Donald Yett in the 1963, and a health economics committee was created as part of the medical care section within the American Public Health Association in the 1970s, but neither of these American entities developed organizationally to become membership associations. There was an annual American “workshop” organized by Ted Stefos and Jim Burgess from the VA Management Science Group, but it was by invitation only and included relatively few (20 to 50) people.
The Journal of Health Economics was started in 1981 by Joe Newhouse and Tony Culyer, followed ten years later by Health Economics under the direction of Alan Maynard, which shared the distinctive yellow color of reports from York’s Centre for Health Economics. These two became the lead journals of a field expanded to encompass a plethora of publications.1 Several articles discuss the development of health economics in the US and UK (Blaug 1998; Forget 2004) but none of them touch or more than a few aspects. Although no comprehensive review of the intellectual and organizational history of the field has been published, a limited perspective can be gained from the various compendiums that collated articles and topic reviews (Cooper and Culyer, Handbook) or, more recently, formal bibliometric studies of health economics publications (Rubin and Change 2004, Wagstaff and Culyer 2010)
Health economics (H.E.), as a distinct sub-field of study, grew and prospered from 1960 to 2000 (see Table 1: TIMELINE below). By 2010 it was well established—and indeed after 50 years was perhaps no longer the epitome of a interdisciplinary field at the cutting edge, but beginning to split and fray as various sub-sub-fields (addictions, risk-adjustment, hospital management, behavioral change, quality of life) became more important and independent. Health economics in 2014 is mature sub-discipline, seeking some new directions, and perhaps even new terminology or changes in scope.
3
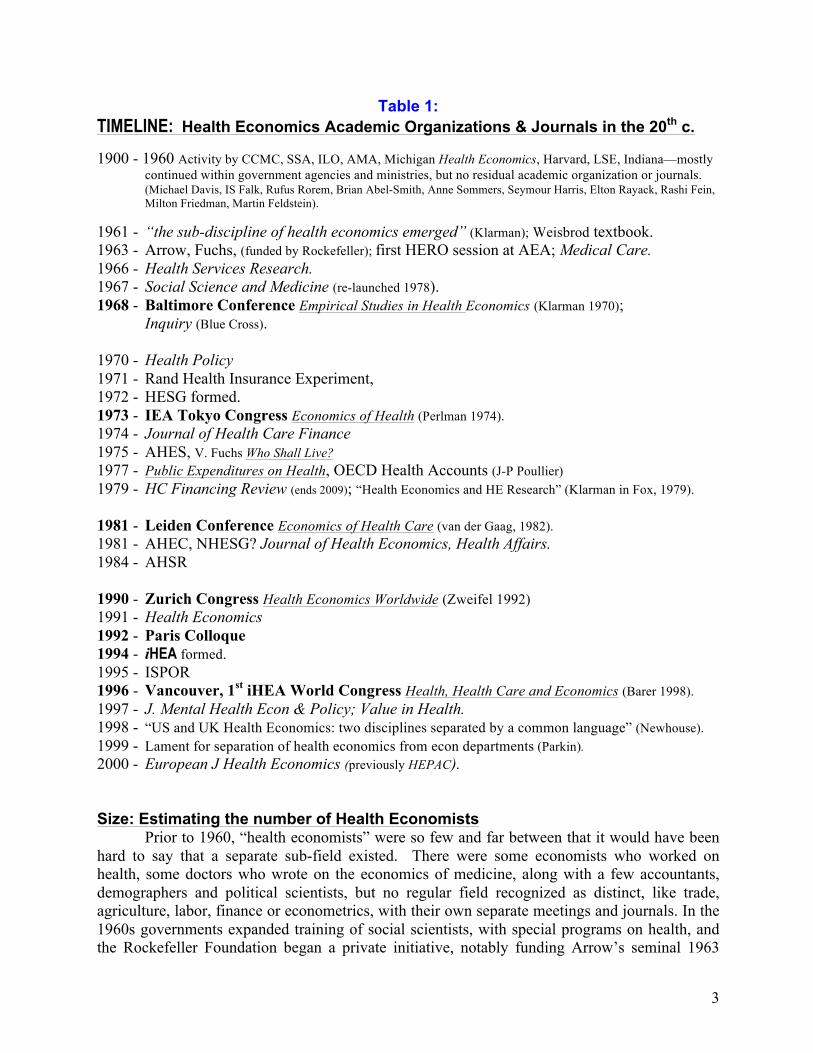
Table 1: TIMELINE: Health Economics Academic Organizations & Journals in the 20th c. 1900 - 1960 Activity by CCMC, SSA, ILO, AMA, Michigan Health Economics, Harvard, LSE, Indiana—mostly
continued within government agencies and ministries, but no residual academic organization or journals. (Michael Davis, IS Falk, Rufus Rorem, Brian Abel-Smith, Anne Sommers, Seymour Harris, Elton Rayack, Rashi Fein, Milton Friedman, Martin Feldstein).
1961 - “the sub-discipline of health economics emerged” (Klarman); Weisbrod textbook. 1963 - Arrow, Fuchs, (funded by Rockefeller); first HERO session at AEA; Medical Care. 1966 - Health Services Research. 1967 - Social Science and Medicine (re-launched 1978). 1968 - Baltimore Conference Empirical Studies in Health Economics (Klarman 1970);
Inquiry (Blue Cross). 1970 - Health Policy 1971 - Rand Health Insurance Experiment, 1972 - HESG formed. 1973 - IEA Tokyo Congress Economics of Health (Perlman 1974). 1974 - Journal of Health Care Finance 1975 - AHES, V. Fuchs Who Shall Live? 1977 - Public Expenditures on Health, OECD Health Accounts (J-P Poullier) 1979 - HC Financing Review (ends 2009); “Health Economics and HE Research” (Klarman in Fox, 1979). 1981 - Leiden Conference Economics of Health Care (van der Gaag, 1982). 1981 - AHEC, NHESG? Journal of Health Economics, Health Affairs. 1984 - AHSR 1990 - Zurich Congress Health Economics Worldwide (Zweifel 1992) 1991 - Health Economics 1992 - Paris Colloque 1994 - iHEA formed. 1995 - ISPOR 1996 - Vancouver, 1st iHEA World Congress Health, Health Care and Economics (Barer 1998). 1997 - J. Mental Health Econ & Policy; Value in Health. 1998 - “US and UK Health Economics: two disciplines separated by a common language” (Newhouse). 1999 - Lament for separation of health economics from econ departments (Parkin). 2000 - European J Health Economics (previously HEPAC). Size: Estimating the number of Health Economists
Prior to 1960, “health economists” were so few and far between that it would have been hard to say that a separate sub-field existed. There were some economists who worked on health, some doctors who wrote on the economics of medicine, along with a few accountants, demographers and political scientists, but no regular field recognized as distinct, like trade, agriculture, labor, finance or econometrics, with their own separate meetings and journals. In the 1960s governments expanded training of social scientists, with special programs on health, and the Rockefeller Foundation began a private initiative, notably funding Arrow’s seminal 1963
4
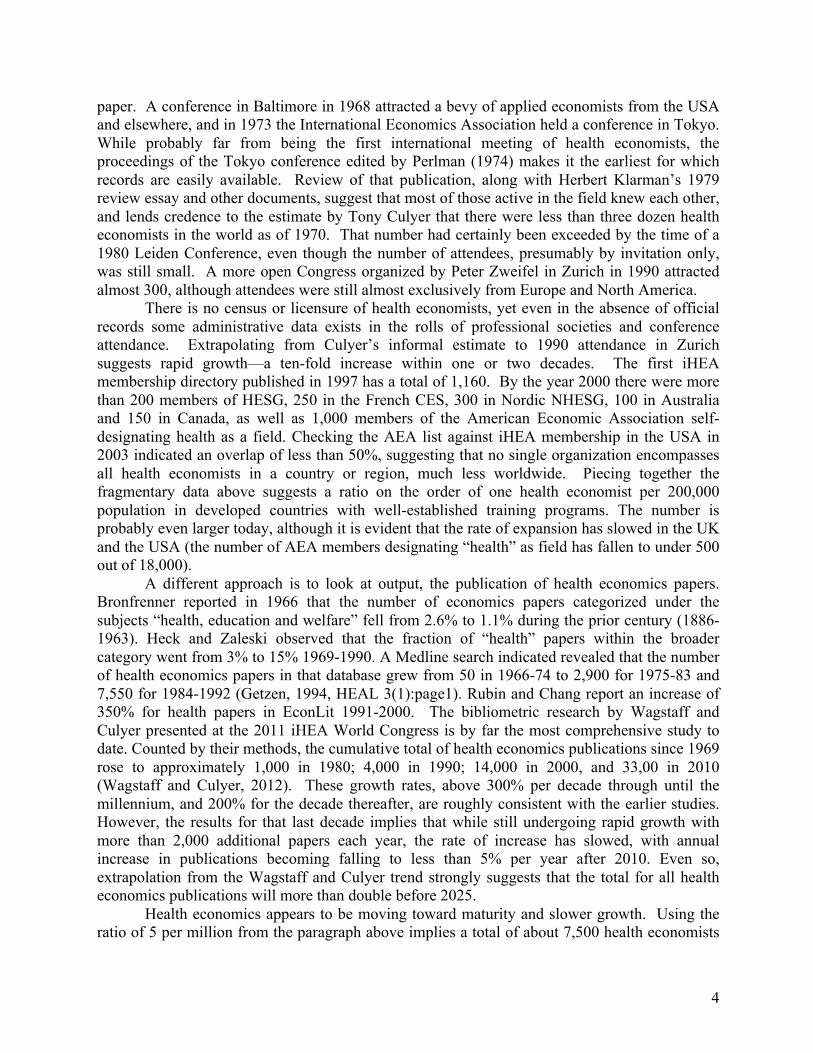
paper. A conference in Baltimore in 1968 attracted a bevy of applied economists from the USA and elsewhere, and in 1973 the International Economics Association held a conference in Tokyo. While probably far from being the first international meeting of health economists, the proceedings of the Tokyo conference edited by Perlman (1974) makes it the earliest for which records are easily available. Review of that publication, along with Herbert Klarman’s 1979 review essay and other documents, suggest that most of those active in the field knew each other, and lends credence to the estimate by Tony Culyer that there were less than three dozen health economists in the world as of 1970. That number had certainly been exceeded by the time of a 1980 Leiden Conference, even though the number of attendees, presumably by invitation only, was still small. A more open Congress organized by Peter Zweifel in Zurich in 1990 attracted almost 300, although attendees were still almost exclusively from Europe and North America.
There is no census or licensure of health economists, yet even in the absence of official records some administrative data exists in the rolls of professional societies and conference attendance. Extrapolating from Culyer’s informal estimate to 1990 attendance in Zurich suggests rapid growth—a ten-fold increase within one or two decades. The first iHEA membership directory published in 1997 has a total of 1,160. By the year 2000 there were more than 200 members of HESG, 250 in the French CES, 300 in Nordic NHESG, 100 in Australia and 150 in Canada, as well as 1,000 members of the American Economic Association self-designating health as a field. Checking the AEA list against iHEA membership in the USA in 2003 indicated an overlap of less than 50%, suggesting that no single organization encompasses all health economists in a country or region, much less worldwide. Piecing together the fragmentary data above suggests a ratio on the order of one health economist per 200,000 population in developed countries with well-established training programs. The number is probably even larger today, although it is evident that the rate of expansion has slowed in the UK and the USA (the number of AEA members designating “health” as field has fallen to under 500 out of 18,000).
A different approach is to look at output, the publication of health economics papers. Bronfrenner reported in 1966 that the number of economics papers categorized under the subjects “health, education and welfare” fell from 2.6% to 1.1% during the prior century (1886-1963). Heck and Zaleski observed that the fraction of “health” papers within the broader category went from 3% to 15% 1969-1990. A Medline search indicated revealed that the number of health economics papers in that database grew from 50 in 1966-74 to 2,900 for 1975-83 and 7,550 for 1984-1992 (Getzen, 1994, HEAL 3(1):page1). Rubin and Chang report an increase of 350% for health papers in EconLit 1991-2000. The bibliometric research by Wagstaff and Culyer presented at the 2011 iHEA World Congress is by far the most comprehensive study to date. Counted by their methods, the cumulative total of health economics publications since 1969 rose to approximately 1,000 in 1980; 4,000 in 1990; 14,000 in 2000, and 33,00 in 2010 (Wagstaff and Culyer, 2012). These growth rates, above 300% per decade through until the millennium, and 200% for the decade thereafter, are roughly consistent with the earlier studies. However, the results for that last decade implies that while still undergoing rapid growth with more than 2,000 additional papers each year, the rate of increase has slowed, with annual increase in publications becoming falling to less than 5% per year after 2010. Even so, extrapolation from the Wagstaff and Culyer trend strongly suggests that the total for all health economics publications will more than double before 2025.
Health economics appears to be moving toward maturity and slower growth. Using the ratio of 5 per million from the paragraph above implies a total of about 7,500 health economists

5
serving the established OECD countries, with the worldwide numbers rising toward 25,000 – 40,000 as training expands in developing countries and new topical niches (risk adjustment, quality-of-life measurement, AIDS, tobacco, addiction, clinical trial design). Even with slower internal growth in coming years, the potential size of the global demand for trained health economists is substantial. Scale: From Departmental Seminar to International Congress Academic “meetings” vary from local university seminars where one person presents a single paper with perhaps a dozen health economists and others making comments, to an international congress where hundreds of papers are presented with over a thousand health economists in attendance. The classic example of peer review was once the “royal society” but is now more commonly a “seminar” or “workshop,” a small group meeting regularly to critically review just one (or perhaps a few) pieces of research at each meeting. The format varies, but it is usual to devote 1 to 2 hours to the presentation and discussion of a piece of research in progress. There is a social networking element at such a small meeting, but it is limited. A regional group (e.g., London, Boston, Midwestern Pharmacoeconomists) has a larger networking component, and proportionately less time devoted to presentation and discussion. By the time the scale approaches that of a major national meeting in the US or a Continental meeting in Europe or Latin America, the opportunity for academic presentation is limited, critical commentary is mostly provided outside the formal program (i.e., discussions in the hall or over lunch), and networking benefits outweigh the feedback on one’s own paper. Many national meetings (AEA, MLA, APHA) also act as “job fairs” for a significant number of participants, a rite of passage from student status to member of the profession.
While the purpose of a “meeting” has some constancies across the span from university to global, it is quite different at the two ends. Meetings do not simply “scale up,” with seminars being piled on top of each other to make a local meeting, and piled higher to make a national one. The use of time and goals differ as one moves along the span university – regional – national – global. Scope: Economics, Health Economics and Health Services Research. The boundaries of “health economics” are apt to undergo continuous change, and have never been entirely clear or fixed. Economists were studying health before Malthus, and examples of economic analysis made by doctors can be found dating back for centuries. What was once “natural philosophy” has divided and subdivided many times over. The transactions of the Royal Society in the 17th century provide common sources for both medicine and economics in the work of Sir William Petty and John Graunt. The American Economics Association was spun off from the existing Historical Society in 1885, and in turn spun out a number of allied social science organizations. By 1960 there were societies for statistics, sociology, finance, public finance, policy analysis and so on. Interdisciplinary hybrids such as medical anthropology, survey research and mathematical biology were becoming increasingly common. By 1980 HESG, AHES, and other national health economics associations were well established, as was the health section (HERO) among the allied social science associations meeting within the AEA. However, rather than unifying in a tightly bonded theoretical structure or body of empirical results, health economics was increasingly driven by centrifugal strains that stretched research topics and methods beyond any simple definition.
6
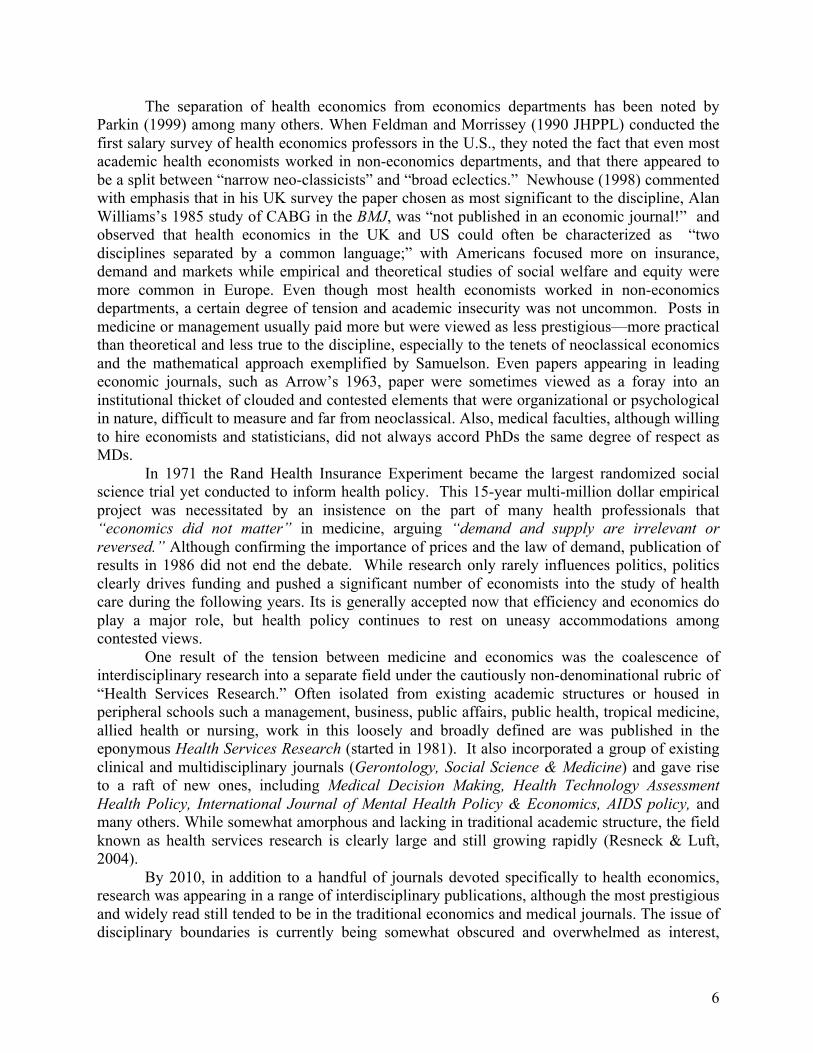
The separation of health economics from economics departments has been noted by Parkin (1999) among many others. When Feldman and Morrissey (1990 JHPPL) conducted the first salary survey of health economics professors in the U.S., they noted the fact that even most academic health economists worked in non-economics departments, and that there appeared to be a split between “narrow neo-classicists” and “broad eclectics.” Newhouse (1998) commented with emphasis that in his UK survey the paper chosen as most significant to the discipline, Alan Williams’s 1985 study of CABG in the BMJ, was “not published in an economic journal!” and observed that health economics in the UK and US could often be characterized as “two disciplines separated by a common language;” with Americans focused more on insurance, demand and markets while empirical and theoretical studies of social welfare and equity were more common in Europe. Even though most health economists worked in non-economics departments, a certain degree of tension and academic insecurity was not uncommon. Posts in medicine or management usually paid more but were viewed as less prestigious—more practical than theoretical and less true to the discipline, especially to the tenets of neoclassical economics and the mathematical approach exemplified by Samuelson. Even papers appearing in leading economic journals, such as Arrow’s 1963, paper were sometimes viewed as a foray into an institutional thicket of clouded and contested elements that were organizational or psychological in nature, difficult to measure and far from neoclassical. Also, medical faculties, although willing to hire economists and statisticians, did not always accord PhDs the same degree of respect as MDs.
In 1971 the Rand Health Insurance Experiment became the largest randomized social science trial yet conducted to inform health policy. This 15-year multi-million dollar empirical project was necessitated by an insistence on the part of many health professionals that “economics did not matter” in medicine, arguing “demand and supply are irrelevant or reversed.” Although confirming the importance of prices and the law of demand, publication of results in 1986 did not end the debate. While research only rarely influences politics, politics clearly drives funding and pushed a significant number of economists into the study of health care during the following years. Its is generally accepted now that efficiency and economics do play a major role, but health policy continues to rest on uneasy accommodations among contested views.
One result of the tension between medicine and economics was the coalescence of interdisciplinary research into a separate field under the cautiously non-denominational rubric of “Health Services Research.” Often isolated from existing academic structures or housed in peripheral schools such a management, business, public affairs, public health, tropical medicine, allied health or nursing, work in this loosely and broadly defined are was published in the eponymous Health Services Research (started in 1981). It also incorporated a group of existing clinical and multidisciplinary journals (Gerontology, Social Science & Medicine) and gave rise to a raft of new ones, including Medical Decision Making, Health Technology Assessment Health Policy, International Journal of Mental Health Policy & Economics, AIDS policy, and many others. While somewhat amorphous and lacking in traditional academic structure, the field known as health services research is clearly large and still growing rapidly (Resneck & Luft, 2004).
By 2010, in addition to a handful of journals devoted specifically to health economics, research was appearing in a range of interdisciplinary publications, although the most prestigious and widely read still tended to be in the traditional economics and medical journals. The issue of disciplinary boundaries is currently being somewhat obscured and overwhelmed as interest,

7
excitement and resources shift toward emerging research centers devoted to cognitive science, genomics, decision theory, gaming, population studies, behavioral finance, complexity, algorithms, simulation and IT. Hence it is not inappropriate to suggest that the boundaries of health economics are still in flux as of 2014, and will remain so for the foreseeable future.
The History of iHEA The creation of iHEA as an international health economics association rests on a congruence of several trends and events. The chair of the health economics committee for the American Public Health Association, Tom Getzen, decided to follow the example of the existing Viseltear Prize for work in medical history by creating a new award for health economics. He asked Kenneth Arrow, who had agreed to write a forward for his textbook, to lend his name to this award. At the same time he was also in the process of producing a newsletter, HEAL, which was an outgrowth from a session on cross-national spending comparisons at the 1990 Zurich Congress organized by Peter Zweifel.
A number of junior professors attending the US VA workshops in 1990 and 1992 had expressed dissatisfaction, saying there were insufficient opportunities to present their work, especially since the existing HERO sessions of the American Economic Association were too restrictive, obscure in their selection process, and with great excess demand. It was suggested that a new association was needed, and that making explicitly international rather than American or British would help to avoid overlap and conflict with the established HESG and HERO. Getzen was able to obtain the support of Joe Newhouse, Mark Pauly and other leading health economists in the U.S. After participating in the health econometrics workshop organized by Andrew Jones and Owen O’Donnell, he was on sabbatical at York in 1993 and able to enlist the support of Tony Culyer, Alan Maynard and Cam Donaldson (then head at Aberdeen and president of HESG), as well as Nordics such as Bengt Jonsson, Jan Olson, Haari Sintonen and Jes Sogaard. In 1994 iHEA was incorporated as a non-profit educational charity recognized as a 501©3 tax-exempt corporation. There was a consensus that the existing journals, JHE and HE, were sufficient and the new association should cooperate with them and continue the newsletter rather than creating a new journal. Memberships were set at $25 and promised a subscription to the HEAL newsletter as well as discounts on JHE and HE. Over 300 persons signed up in 1995, and each was provided with a “charter member” certificate.
During the 1990 Zurich Congress, Morris Barer had agreed to edit a special issue of Social Science and Medicine for selected papers and offered to organize another international meeting within a few years. Getzen’s paper was among those being edited, and in 1994 Barer suggested to him that this upcoming Congress take on the name and sponsorship of the newly organized association iHEA. Despite an early oath to keep the operation small and never to have it run meetings, this was agreed and in 1996 the Vancouver meetings organized under the auspices of UBC became the first iHEA World Congress. Soon thereafter Bill Swan, graduate student and part-time director of the Canadian association, came on board to run operations and logistics. In 1999 the Rotterdam Congress was held under the leadership of Frans Rutten, and a 2001 Congress was planned for York under Alan Maynard. When Maynard left for the Nuffield Trust Mike Drummond graciously took over. However, the scramble to cover the gap in leadership and other operational difficulties were making it obvious that iHEA needed more formal structure and staff resources if planning and operation of future Congresses were to be successful. Bill Swan became full-time deputy CEO and head of operations while Patrick Taylor, who had worked for several years as a consultant, took over the IT function.

8
Table 2: Growth of iHEA
Year MEMBERS Countries CONGRESS Attendance
founded 1994
420
21
1995 575 28
1996 900 35 Vancouver 661
1997 1,160 47
1999 1,561 60 Rotterdam 852
2001 1,915 62 York 1,250
2003 2,483 65 San Francisco 1,456
2005 2,536 Barcelona 1,912
2007 2,548 76 Copenhagen 1,667
2009 1,739 Beijing 1,228* *plus 870 in China Forum
2011 2,232 Toronto 1,844
2013 1,830 89 Sydney 1,263
2014 2,570 90 Dublin 1,000** **estimated
The first iHEA Board election was held in 1999, with a daylong governance meeting at
York in 2001. The York Congress had been a sort of joint venture, with split responsibility. In 2003 HEA itself, rather than a private company or host university, became legally responsible for the Congress as lead organizer and financial guarantor. In part, the decision was forced by the inability of UC Berkeley to legally take on such a role, but primarily it reflected the evolution of iHEA as a professional association. Such a leap would not have been possible without the experience and financial reserves gained from earlier years. Voluntary contributions had been made by local organizers following the Vancouver and Rotterdam conferences, and a sizable financial boost had come from the joint ventureship with York. From 2003 on, iHEA was no longer a junior partner. It was now the lead organizer for each iHEA World Congress, with all of the responsibilities and obligations that entailed (see “OWNERSHIP” appendix). Among those responsibilities was fostering the growth of affiliated health economics associations. Seeing a mismatch between the restricted activity of HERO and the large number of U.S. health economists, iHEA created ASHE as a sub-committee with a budget of $100,000, appointed a board and executive director, and ran those meetings for 2006, 2008 and 2010 before ASHEcon became a separate organization. In 2005 as part of the Barcelona Congress iHEA held a meeting for its European Committee on Health Economics (ECHE), hoping to formalize European efforts. ECHE subsequently held meetings in Budapest, Rome, Helsinki and Zurich but was not able to create a permanent secretariat of it own before morphing into EUHEA (European Union of Health Economics Associations) in 2014. In Africa, iHEA partnered with the Gates foundation and AfHEA to help that association become a more organized and enduring entity, with meetings in Accra (2009), Dakar (2011) and Nairobi (2013). In 2010 iHEA assisted the WHO in the formation of Health Systems Global (HSG) in 2010 and prepared the abstracted and program review for their second Symposium in Beijing (2012). Technical assistance of more

9
limited nature has been provided to associations in China, India and Turkey, and indirect support for organizing activity has come from hundreds of iHEA scholarships to delegates from developing countries over the last decade.
Journal subscriptions were a major activity of iHEA at its formation, and contributed the majority of majority of revenues until 1999. iHEA expanded its co-operative distribution agreements from the original 2 to as many as 8 journals. Journal revenues began to fall as the business model of scientific publication shifted to the internet and bulk academic contracts rather than personal sales to individual scholars. As the costs of servicing a dwindling number of individual subscriptions became unsustainable, iHEA’s decided to exit this line of activity and the last journal co-marketing contract was phased out in 2010. Past as Prelude: (iHEA 2020)
The creation of iHEA was driven from the demand side – the desire of junior professors to find more and better outlets for presentation of their work in progress. Unlike HESG at York, or JHE at Harvard, there was no pull (or pool of available resources) from the supply side. Major changes in information technology that facilitated worldwide communications were also a factor. iHEA took root and grew as an individual membership organization with a congruence of conditions that did not exist until about 1990: a deep pool of excess demand, technological change and independent social entrepreneurship.
Rapid growth in the latter half of the 20th century caused a surge in demand for conferences and other places where these new researchers could present their work to colleagues and advance their careers. While senior health economists were swamped with opportunities in 1990, students and junior professors struggled in a crowd to find open slots. The few HERO sessions at the American Economic Association could accept only a fraction of the papers submitted, with a selection process that was obscure and sometimes felt to be dominated by an established group of insiders, unreceptive to newcomers. Organizing within the U.K., Australia and the Nordic countries had proceeded successfully along the “study group” lines –volunteer leadership that was largely informal and borrowed staff support from university research centers running medium or small meetings characterized by extensive discussion of papers with a few plenary addresses—a format ideally suited to complement and extend existing university research seminars at the next level, but not so well suited for very large numbers or extensive international growth outside of national boundaries and collegial networks.
International commercial and scientific communications were revolutionized by two technological changes in the 1980s – first fax and then email. Mailing of letters, journals or brochures across national boundaries was slow and expensive (early 4 to 8 page iHEA newsletters and programs cost one to two dollars per piece, in addition to printing and paper). In 1996, although still a relatively small association, processing communications, invoicing and payments caused the small corner office housing iHEA to have the second highest long distance charges among all the thousands of telephones at Temple University. Fortunately, advances in technology rapidly lowered costs as email and scanning replaced paper and fax. The new association also was beginning to accumulate revenues and could afford to cover more overhead.
iHEA grew to fill a perceived gap in the organizational environment. Medical and economic societies were old and established. Indeed, medical the medical establishment had grown so large and fragmented that some specialty societies were more powerful than the “main” national medical association. Social sciences had blossomed in the 1960s and 1970s, but the organizational niches within the overlapping fields of economics, policy, statistics, financing, management, biology and medicine were hardly distinct or clear. Interdisciplinary blurring and

10
splintering have continued, although a few congealed groupings are becoming more apparent, such as “health services research” and “cognitive science.” The atomistic individualism of rational actors in economics is yielding ground to behavioral analyses, but the group and public aspects of economics and decision theory are still vague and indistinct. Health care, with its admixture of social, biological, psychological and ethical or even religious elements is a particularly tangled knot, but one that occupies a larger and larger portion of a developed and aging economy.
Prior to 1990 there was probably not enough demand to make an independent self-supporting international health economics association possible, nor was the technology available. Note that HESG and JHE benefitted substantially from the prestige and support of York and Harvard, and provided commensurate returns on human and financial capital invested by those institutions. iHEA was able to grow from scratch without major external support because there was excess demand and a way to monetize a small but sufficient reserve in the tens of thousands of dollars (not hundreds or millions) that replaced the start-up funding contributed personally by the founder. Mailing costs alone would have made the HEAL newsletter unsustainable without the shift to the internet (where now ambitious and sophisticated blogs flourish with little funding). The fact that HERO had not expanded beyond its original format created a deep pool of unmet need among junior professors in the USA, a need that adequate grant and university funding translated into effective demand. However, it still required a spark or catalyst to convert this confluence of favorable forces into a functioning organization with lasting structure.
In private enterprise, such gathering of forces is commonly termed entrepreneurship, and lately a similar process in the non-profit arena has become known as social entrepreneurship. It might also be called start-up, initial organization, genesis or founding, but whatever term is used some person or small group must take action in order for an organization to form. This step may be brief and seem slight, yet is far from trivial and not to be ignored. The rapid growth of ASHEcon in the US suggests that significant excess demand for a national association existed there prior to 2005, but no organization spontaneously arose —it was created when iHEA provided initial funding, hired a director, and organized logistical support until ASHEcon could effectively operate independently in 2010. Similarly a European health economics association had been discussed and planned since 1980—and was still being discussed and planned 30 years later. ECHE was established as a committee within iHEA to further the European efforts, and hopefully EUHEA, formally organized in 2013, will now take hold. Four different pharmacoeconomics associations were started in the 1990s, and only one, ISPOR, remains. Entrepreneurship and a risky period of initial growth and formal structuring is required before a group of scholars can become an enduring professional association such as the Royal Statistical Society, AEA, MLA, Geophysical Union---or iHEA.
Every organization is to greater or lesser extent both path dependent and conditioned by historical context—yet must also be nimble enough to grow and prosper as conditions change. iHEA grabbed a moment favorable to its formation. Given the great number of changes in the environment (globalization and ascendance of emerging markets, bifurcating demand for skills with vast expansion of university education, competition for research resources, decline of paper scientific journals, changing disciplinary boundaries, new regional, national and topical associations growing,) and changes within the organization (initial growth spurt slowing, shift from journals to conferences as business model, turnover of the old guard), it is evident that iHEA is at something of a turning point.

11
1 Several other serial publications, including one called Health Economics published by the University of Michigan, came and went during the 20th century. The most international of these was Cahiers de Sociology et de Demographie Medicales published in Paris under Bui van Ho Dong from 1961 to 2010.
Abel-Smith B. (1963) Paying for Health Services, Public Health Papers No. 17, WHO: Geneva. Abel-Smith B. (1967) An International Study of Health Expenditure. Public Health Papers No. 32, WHO: Geneva. Arrow, KJ (1963). Uncertainty and the Welfare Economics of Medical Care. American Economic Review. 53: 941-973. Barer M, Getzen T, Stoddart G. (1998) Health, Health Care and Economics: perspectives on distribution. Wiley: NY.
(selected papers from the First iHEA World Congress in Vancouver, BC July 1996). Blades CA, Culyer AJ, Wiseman J and Walker A (1986) The International Bibliography of Health Economics: A
comprehensive annotated guide to English Language Sources since 1914. Brighton, Sussex: Wheatsheaf Books. Blaug, M. (1998) Where are we now in British health economics? Health Economics 7:S63-S78 (special supplement). Bronfenbrenner M. Trends, cycles and fads in economic writing. American Economics Review 1966; 56(2): 538–552 Cawley J Morrisey M. (2007) The earnings of U.S. health economists. Journal of Health Economics 26:358-372. Croxson, Bronwyn (1998). From private club to professional network: an economic history of the Health Economists’ Study
Group, 1972 - 1997 Health Economics (Special Issue) 7(S1): S9-S45; also appears in C.Donaldson and A.Maynard, eds. Twenty Five Years of Health Economics in the UK. Nuffield Provincial Hospitals Trust, 1998.
Cooper MH, Culyer AJ (1973) Health Economics London: Penguin. Culyer AJ, Wiseman J, Walker A. (1977) Annotated Bibliography of Health Economics. Oxford: Martin Robinson. Culyer, A. (1986) Health Economics: The Topic and the Discipline. in J.M Horne, ed. Proceedings of the Third Canadian
Conference on Health Economics. Davis, MM. (1931) New Plans of Medical Service. Chicago: Rosenwald Fund. Dublin LI. (1928) Health and Wealth: A Survey of the Economics of World Health. New York: Harper. Fama EF and MC Jensen. (1983) “Separation of Ownership and Control.” Journal of Law and Economics 26(2):301-325. Feldman R, Morrisey M. (1990) Health Economics: A Report on the Field. J Health Politics Policy & Law 15(3): 627-646. Feldstein, M. (1967) Economic Analysis for Health Service Efficiency Amsterdam: Elsevier. Falk, IS. (1933) The Incidence of Illness and the receipt and costs of medical care among representative families.
(Publication #26 of the Committee on the Costs of Medical Care) Chicago: University of Chicago Press. Fox Daniel M (1979) Economists and Health Care NY: Prodist. RA410.f69 Forget EL. (2004) Contested Histories of an Applied Field: The Case of Health Economics. History of Political Economy
36(4): 613-637. Fuchs VR. (1972) Essays in the economics of health and medical care. NBER. Fuchs VR (1975) Who Shall Live? New York: Basic Books. Fuchs VR (1996) Economics, Values and health care reform. AER 86:1-24. Fuchs VR (1986b) editorial J. Health Econ 5:367 Fuchs VR (2000) The Future of Health Economics (keynote address to iHEA 2nd World Congress of Health Economists)
Journal of Health Economics 19(2):141-157. Getzen, TE (2009), History of iHEA (and other Health Economics Organizations) in R. Mullner (ed), Encyclopedia of Health
Services Research. Sage: NY. Grossman, M. (1972) The Demand for Health. NBER Hauser MM. (1972) The Economics of Medical Care (proceedings of a conference at University of York, UK) Allen &Unwin Klarman HE (1965). The Economics of Health NY: Columbia U Press. Klarman HE. (1968) Empirical Studies in Health Economics Baltimore: Johns Hopkins. Klarman, HE (1977). “Health Economics and Health Economics Research” in Fox (1979) pp:80-89. Lee, K. and Mills, A. The role of economists and economics in health service planning: a general overview. in: Lee, K. (Eds)
Economics and Health Planning. London: Croom Helm, 1979. Lopez-Casasnopvas, G. ed. (1991) Incentives in Health Systems (selected papers from the First European Conference on
Health Economics, Barcelona, September 1989). Springer-Verlag. Morrisey MA, Cawley J. (2004)Health Economists’ Views of Health Policy. J Health Politics Policy & Law. 2004. Morrisey MA, Cawley J. (2008) US Health Economists: What we are and what we do. Health Economics. 17:535-543. Mushkin, S.J., (1958). Toward a definition of health economics. Public Health Reports 73: 785–793. Mushkin, S.J., (1962). Health as investment. Journal of Political Economy 80: 223–255 Newhouse, JP (1987). Health Economics and Econometrics. American Economic Review 77(2): 269-274. Newhouse, JP (1998) US and UK Health Economics: two disciplines separated by a common language. Health Economics
7:S79-S92. OECD (1977) Public Expenditure on Health. Organization for Economic Co-operation and Development, Paris.

12
Perlman M, ed. (1974) The Economics of Health and Medical Care. Proceedings of a 1973 Tokyo IEA Conference. London: Macmillian.
Poullier, J-P (see OECD) Parkin, D. (1999) The Health Economists’ Study Group and the Royal Economic Society. Newsletter of the Royal Economic
Society, issue 104, January 1999. Resneck J, Luft H. (2004) How Health Policy and Health Services Researchers are Compensated: Analysis of a Nationwide
Salary Survey. Medical Care Research and Review. 2004 61: 392-408 Rorem, CR (1940). Non-profit Hospital Service Plans; Historical and critical analysis. Chicago: American Hospital
Association. Rorem, CR (1982). A Quest for Certainty: Essays on Health Care Economics, 1930-1970. Ann Arbor: U Michigan Press. Rubin, RM and CF. Chang (2003) A bibliometric analysis of health economics articles in the economics literature: 1991-
2000. Health Economics 12:403-414. Van der Gaag, J. Neenan WB, Tsukahara T. (1982) Health, Economics, and Health Economics. Proceedings of the World
Congress on Health Economics. New York: Praeger. Wagstaff A, Culyer, AJ (2012) Four decades of health economics through a bibliometric lens. Journal of Health Economics
31:406-439. Weisbrod, BA. (1961a) Economics of Public Health: Measuring the economic Impact of Diseases. U Pennsylvania Press. Weisbrod, BA. (1961b). The valuation of human capital. Journal of Political Economy 69, 425–436. Williams, A. (1985) Economics of coronary artery bypass grafting. British Medical Journal 1985; 291: 326-329. Williams, A. (1987) Health Economics: The cheerful Face of the Dismal Science? In: Williams, A. (Eds) Health and
Economics: proceedings of Section F (Economics) of the British Association for the Advancement of Science, Bristol, 1986. Basingstoke: MacMillan, 1987
Zweiffel P, Frech HE (1992) Health Economics Worldwide. (proceedings of the Second World Congress Zurich September 10-14 1990). Kluwer: Dordecht.