hepatocellular carcinoma and pancreatic adenocarcinoma
TRANSCRIPT
(Continued on page 3)
CancerUpdateVolume 3 • Number 3 • Spring 2013
In This Issue 2 From the Medical Director 6 GI Cancer Conference 2013 7 New Directions in the Treatment of Hepatocellular Carcinoma10 Texas Cancer Vaccine Symposium 2013 11 New Directions in the Treatment of Pancreatic Adenocarcinoma14 Starving Cancer: Could This Be the Answer to Pancreatic Adenocarcinoma? 15 James W. Fleshman, Jr., MD, Joins Baylor Dallas as New Chief of Surgery 16 Welcome to New Members of the Medical Staff at Baylor Sammons Cancer Center 17 Ronald C. Jones, MD, FACS, Ends Distinguished Tenure as Chair of the Department of Surgery18 Development of the Oncology Evaluation and Treatment Center and the Infusion Center on the Baylor Dallas Campus20 Baylor Health Care System Foundation: Gathering Financial Support for Quality Cancer Care 24 New Clinical Trials at Baylor Charles A. Sammons Cancer Center at Dallas26 Site-specific Tumor Conferences27 Publications 28 Swim Across America 2013
Hepatocellular Carcinoma and Pancreatic Adenocarcinoma: Multidisciplinary Approaches for Complex CancersSince the National Cancer Act was signed in 1971, steady progress has been made to improve survival in many types of cancer. With earlier detection and innovative approaches for local and systemic therapy, there is the promise of transforming once-deadly diseases into chronic conditions that can be treated successfully over a long life span.
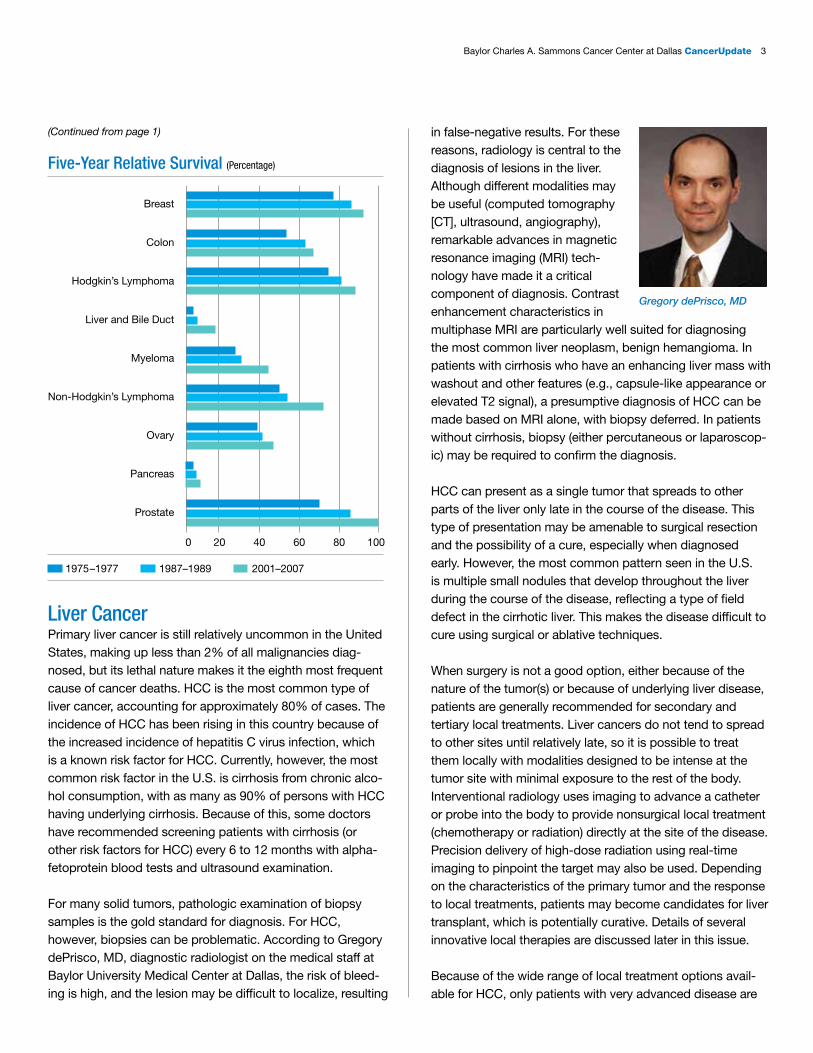
In two cases—hepatocellular carcinoma (HCC) and pancreatic adenocarcinoma (PA)—this optimistic possibility currently remains out of reach. Although small improvements have been made, outcomes continue to be grim for most patients, with 5-year survival rates of around 14% for patients with HCC and only 6% for patients with PA. For patients present-ing with distant metastases (22% in HCC and 53% in PA), those figures change to 4% and 2%, respectively. (See bar chart on page 3.)
What makes these cancers so resistant to treatment? In part, it is because both diseases tend to be asymptomatic or have only vague, nonspecific symptoms during their early stages. Thus, most cases of HCC and PA are fairly advanced by the time they are diagnosed. In addition, each disease develops and grows in a specific milieu that contributes to the difficulty in treating it effectively.
Charles A. Sammons Cancer Center at Dallas
2 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Volume 3 • Number 3 • Spring 2013
CancerUpdate is a publication of Baylor Charles A. Sammons Cancer Center at Dallas, Baylor University Medical Center at Dallas.
BaylorHealth.edu/Sammons214.820.3535
Editor in Chief: Alan M. Miller, MD, PhD Chief of Oncology, Baylor Health Care System Medical Director, Baylor Charles A. Sammons Cancer Center at DallasManaging Editor: Audrianne Schneider, FACHEWriters and Assistant Editors: Lorraine Cherry, PhD, Margaret Hinshelwood, PhD, and Jana Pope
To be removed from the mailing list, call 1.800.9BAYLOR.
Physicians are members of the medical staff at one of Baylor Health Care System’s subsidiary, community, or affiliated medical centers and are neither employees nor agents of those medical centers, Baylor University Medical Center at Dallas, or Baylor Health Care System.
Cancer research studies on the campus of Baylor University Medical Center at Dallas are conducted through Baylor Research Institute, Texas Oncology, and US Oncology. Each reviews, approves, and conducts clinical trials independently.
Copyright © 2013, Baylor Health Care System. All rights reserved. SAMMONS_000_2013 DH
From the Medical DirectorCancerUPDATE
Alan M. Miller, MD, PhDchief of oncology, Baylor Health Care System and medical director, Baylor Charles A. Sammons Cancer Center at Dallas
Hope for a Brighter Tomorrow
214.820.3535 or 1.800.9BAYLORBaylorHealth.edu/Sammons Our referral, consult, and information line offers easy access for:• Physician referrals • Follow-up on patients to referring
physicians • Medical records • Information on clinical trials • Specialized services • New patient information, maps, and
lodging information
Baylor Charles A. Sammons Cancer Center at Dallas
Progress has clearly been made in the war on cancer. Today, two out of every three people diagnosed with cancer survive 5 years or more. There are more than 12 million cancer survivors in the United States, and the number increases daily. The 5-year survival in prostate cancer is near 100%; in breast cancer and Hodgkin’s lymphoma, more than 80%; and in colon cancer and non-Hodgkin’s lymphoma, over 60%. In stark contrast to these figures is the 5-year survival in liver cancers (14%) and pancreatic cancer (6%).
Recent research provides glimmers of hope for improvement in the years to come. In this issue, articles describe new directions in the treatment of hepatocellular carcinoma (HCC) and pancreatic adenocarcinoma (PA). For HCC, several approaches are described for local therapies that can provide a bridge to curative liver transplantation. For PA, new understand-ing of the biology of this devastating malignancy is leading to treatments that may overcome the barriers that have prevented successful treatment.
At our institution, we are well positioned to continue to make strides in improving the outcome and survival for patients with cancers of the liver or pancreas. Our multidisciplinary teams meet regularly to discuss the best approach for individual patients, as well as designing new trials to find better approaches. Our liver transplant program, one of the first and largest in the country, offers many patients with HCC the chance for a cure. The Innovative Clinical Trials Center brings the newest in targeted therapies and phase I trials to patients with PA and HCC and is strengthened by our relationship with Dr. Daniel Von Hoff, who in his role as advisor to the center helps Baylor investigators access the most promising agents for trial in these diseases. Finally, through the generos-ity of our many donors we can leverage philanthropy to help support the research efforts that will lead to major improvements in the survival rates from these most difficult cancers.
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 3
(Continued from page 1)
Liver CancerPrimary liver cancer is still relatively uncommon in the United States, making up less than 2% of all malignancies diag- nosed, but its lethal nature makes it the eighth most frequent cause of cancer deaths. HCC is the most common type of liver cancer, accounting for approximately 80% of cases. The incidence of HCC has been rising in this country because of the increased incidence of hepatitis C virus infection, which is a known risk factor for HCC. Currently, however, the most common risk factor in the U.S. is cirrhosis from chronic alco-hol consumption, with as many as 90% of persons with HCC having underlying cirrhosis. Because of this, some doctors have recommended screening patients with cirrhosis (or other risk factors for HCC) every 6 to 12 months with alpha-fetoprotein blood tests and ultrasound examination.
For many solid tumors, pathologic examination of biopsy samples is the gold standard for diagnosis. For HCC, however, biopsies can be problematic. According to Gregory dePrisco, MD, diagnostic radiologist on the medical staff at Baylor University Medical Center at Dallas, the risk of bleed-ing is high, and the lesion may be difficult to localize, resulting
in false-negative results. For these reasons, radiology is central to the diagnosis of lesions in the liver. Although different modalities may be useful (computed tomography [CT], ultrasound, angiography), remarkable advances in magnetic resonance imaging (MRI) tech-nology have made it a critical component of diagnosis. Contrast enhancement characteristics in multiphase MRI are particularly well suited for diagnosing the most common liver neoplasm, benign hemangioma. In patients with cirrhosis who have an enhancing liver mass with washout and other features (e.g., capsule-like appearance or elevated T2 signal), a presumptive diagnosis of HCC can be made based on MRI alone, with biopsy deferred. In patients without cirrhosis, biopsy (either percutaneous or laparoscop-ic) may be required to confirm the diagnosis.
HCC can present as a single tumor that spreads to other parts of the liver only late in the course of the disease. This type of presentation may be amenable to surgical resection and the possibility of a cure, especially when diagnosed early. However, the most common pattern seen in the U.S. is multiple small nodules that develop throughout the liver during the course of the disease, reflecting a type of field defect in the cirrhotic liver. This makes the disease difficult to cure using surgical or ablative techniques.
When surgery is not a good option, either because of the nature of the tumor(s) or because of underlying liver disease, patients are generally recommended for secondary and tertiary local treatments. Liver cancers do not tend to spread to other sites until relatively late, so it is possible to treat them locally with modalities designed to be intense at the tumor site with minimal exposure to the rest of the body. Interventional radiology uses imaging to advance a catheter or probe into the body to provide nonsurgical local treatment (chemotherapy or radiation) directly at the site of the disease. Precision delivery of high-dose radiation using real-time imaging to pinpoint the target may also be used. Depending on the characteristics of the primary tumor and the response to local treatments, patients may become candidates for liver transplant, which is potentially curative. Details of several innovative local therapies are discussed later in this issue.
Because of the wide range of local treatment options avail-able for HCC, only patients with very advanced disease are
Five-Year Relative Survival (Percentage)
Breast
Colon
Hodgkin’s Lymphoma
Liver and Bile Duct
Myeloma
Non-Hodgkin’s Lymphoma
Ovary
Pancreas
Prostate
0 20 40 60 80 100
1975–1977 1987–1989 2001–2007
Gregory dePrisco, MD
4 Baylor Charles A. Charles A. Sammons Cancer Center at Dallas CancerUpdate
usually referred for systemic therapy. Unfortunately, HCC is highly resistant to most standard chemotherapy drugs. This resistance may stem in part from innate chemoresistance of the cells related to the expression of drug resistance genes. It may also be the result of hepatic dysfunction caused by cirrhosis, which results in poor drug uptake and metabolism. Fluid accumulation from cirrhosis can reduce effective drug concentrations. Doxorubicin, 5-fluorouracil, and cisplatin have shown some efficacy in reducing tumor size, but only in a small proportion of tumors, and typically only for a short time. The use of targeted therapies may hold more promise, although the field is still quite young. Sorafenib, an oral mul-tikinase inhibitor that suppresses tumor cell proliferation and angiogenesis, has shown promising results in several phase III trials, although hepatotoxicity may be dose-limiting in patients with reduced liver function. Based on these results, sorafenib is the only drug specifically recommended in the National Comprehensive Cancer Network treatment guidelines for patients with unresectable HCC who are not candidates for transplant.
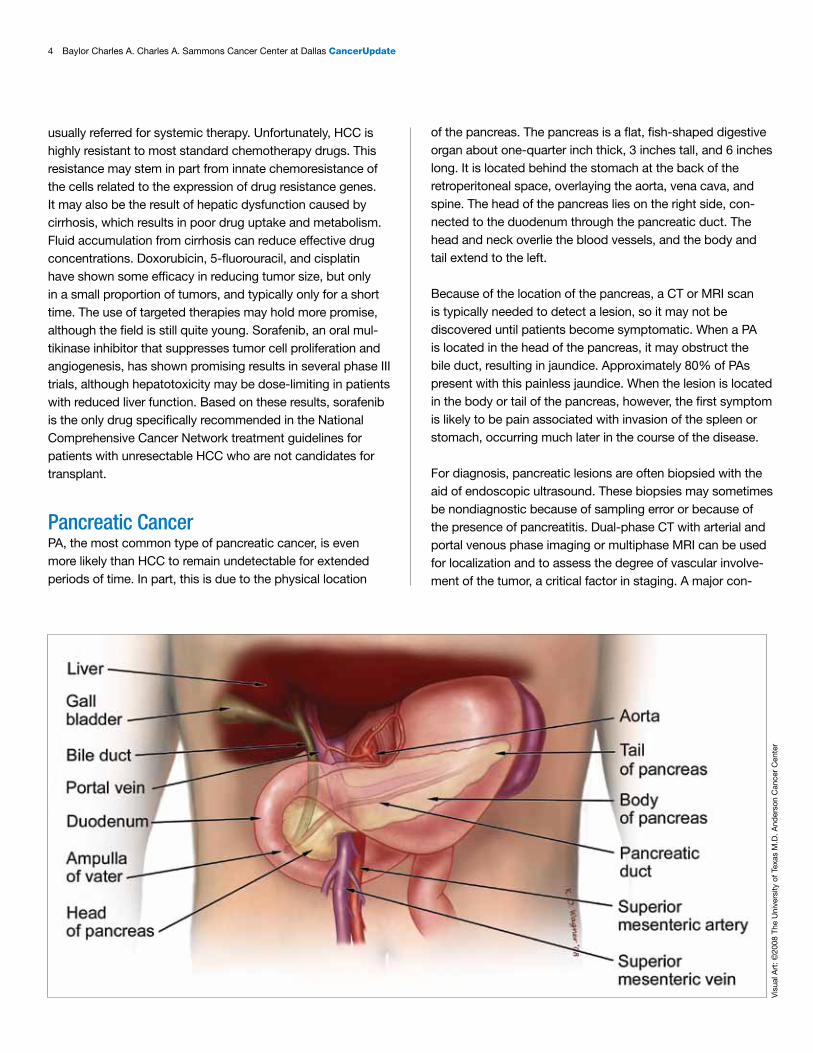
Pancreatic CancerPA, the most common type of pancreatic cancer, is even more likely than HCC to remain undetectable for extended periods of time. In part, this is due to the physical location
of the pancreas. The pancreas is a flat, fish-shaped digestive organ about one-quarter inch thick, 3 inches tall, and 6 inches long. It is located behind the stomach at the back of the retroperitoneal space, overlaying the aorta, vena cava, and spine. The head of the pancreas lies on the right side, con-nected to the duodenum through the pancreatic duct. The head and neck overlie the blood vessels, and the body and tail extend to the left.
Because of the location of the pancreas, a CT or MRI scan is typically needed to detect a lesion, so it may not be discovered until patients become symptomatic. When a PA is located in the head of the pancreas, it may obstruct the bile duct, resulting in jaundice. Approximately 80% of PAs present with this painless jaundice. When the lesion is located in the body or tail of the pancreas, however, the first symptom is likely to be pain associated with invasion of the spleen or stomach, occurring much later in the course of the disease.
For diagnosis, pancreatic lesions are often biopsied with the aid of endoscopic ultrasound. These biopsies may sometimes be nondiagnostic because of sampling error or because of the presence of pancreatitis. Dual-phase CT with arterial and portal venous phase imaging or multiphase MRI can be used for localization and to assess the degree of vascular involve-ment of the tumor, a critical factor in staging. A major con-
Vis
ual A
rt: ©
2008
The
Uni
vers
ity o
f Tex
as M
.D. A
nder
son
Can
cer
Cen
ter
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 5
founder in diagnosis is the presence of a pancreatic cystic lesion. MRI is useful in assessing pancreatic cystic lesions with regards to relationship to the pancreatic duct. If the lesion is small and clearly associated with the duct, it is likely to be a pseudocyst or intraductal papillary mucinous neoplasm (IPMN). Cyst aspiration under endoscopic ultra-sound can be useful to guide management. Serial surveil-lance exams are required for IPMN, preferably with MRI, in order to assess for evolution that would warrant resection. Surveillance is also advised for lesions that have undergone resection to evaluate for local recurrence and for new disease elsewhere in the gland, as IPMN confers an increased risk of PA in parts of the gland remote from the primary lesion via a field effect similar to that seen in cirrhotic livers.
Surgery is the only potentially curative treatment for pancre-atic cancer, but many patients will not be good candidates for surgery based on tumor stage and/or patient character-istics. Tumor staging, based on evidence of peritoneal or hepatic metastases and radiological findings of blood vessel involvement, classifies tumors as resectable, borderline resectable, or nonresectable. By these criteria, only 25% to 30% of tumors are considered operable at diagnosis. Patient characteristics that may affect suitability for surgery include age, comorbidities, performance status, and frailty. The type of surgery used will depend on the location of the tumor. For tumors located in the head of the pancreas, a pancreaticodu-odenectomy (Whipple procedure) is used, involving removal of the head, the duodenum, a portion of the common bile duct, gallbladder, and sometimes part of the stomach. For tumors located in the body or tail of the pancreas, a laparo-scopic procedure may be possible. Such procedures have outcomes as good as those seen with more radical surgery, and short-term recovery is easier.
Chemotherapy is commonly used for patients with PA, either for the treatment of unresectable disease or in the adjuvant setting. The standard treatment is gemcitabine, alone or in combination. Various chemotherapeutic and targeted agents have been used in combination with gemcitabine, but results have been largely disappointing. FOLFIRINOX, a combination of 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin, has
shown promise as first-line treatment for patients with meta-static disease. In addition, gemcitabine in combination with nab-paclitaxel has also shown an improvement in survival. With all of these efforts, however, most patients with PA still survive less than a year after diagnosis.
Why is chemotherapy so ineffective against PA? In HCC, the lack of effectiveness was tied to innate resistance in the cancer cells and hepatic dysfunction affecting drug uptake and metabolism. In PA, the answer may involve the dense tumor stroma around the tumor which can form a physical barrier to chemotherapy delivery. A number of new research approaches are aimed at disrupting the stromal barrier, with the hope of allowing increased accessibility of toxic agents to the tumor cells. Some of these approaches are being investigated by researchers at Baylor Charles A. Sammons Cancer Center at Dallas and are discussed in greater detail later in this issue.
Treating HCC and PA at BaylorOptimal treatment of patients with HCC or PA requires coor-dinated, multidisciplinary care, bringing together specialists in a variety of fields to design and implement treatment plans individualized for each patient.
At Baylor University Medical Center at Dallas, this quality of care is available through Baylor Liver and Pancreas Disease Center. This center started in 1998 as a center without walls, but is now consolidated as a single-site facility in Baylor Charles A. Sammons Cancer Center. It is associated with Baylor Annette C. and Harold C. Simmons Transplant Institute, one of the largest liver transplant programs in the world. It is designed to focus on the convenience and com-fort of the patient. For incoming patients, there is a single phone number to call, managed by a nurse who gathers all of the relevant information. The information is evaluated, consults are scheduled, and imaging and laboratory data are collected. A treatment plan is formulated, which can be presented to the patient on the day he or she comes to the center. According to Robert Goldstein, MD, surgical director of the center and assistant director of Baylor Annette C. and
“Through this multidisciplinary approach, new and innovative ways to treat the most difficult cancers can be discovered. Options that might not have been thought of by one specialist alone may come into focus when multiple treating and diagnostic physicians get together to look at the whole picture.”
Alan M. Miller, MD, PhD

6 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Harold C. Simmons Transplant Institute, “Very few institutions are as dedicated as Baylor in treating these very complex patients and staying at the forefront of treatment options.”
An integral part of the multidisciplinary program involves twice-monthly site-specific tumor conferences, usually held in the conference center at Baylor Charles A. Sammons Cancer Center. (Liver conferences are held on the second and fourth Tuesdays of each month; pancreas conferences are held on the first and third Fridays.) The conferences are attended by specialists on the medical staff who might be involved in the care of patients with that type of cancer, including diagnostic radiologists, interventional radiologists, surgeons, radiation oncologists, medical oncologists, and pathologists. These are true working conferences; the refer-ring clinician presents the case, then everyone interacts to make the best possible treatment decisions. A patient has the equivalent of three to five consultants evaluating the case, with the convenience of one visit, and receives recommendations that are truly personalized. The critical
importance of this multidisciplinary evaluation was empha-sized by Alan M. Miller, MD, PhD, chief of oncology, Baylor Health Care System, and medical director, Baylor Charles A. Sammons Cancer Center: “Through this multidisciplinary approach, new and innovative ways to treat the most difficult cancers can be discovered. Options that might not have been thought of by one specialist alone may come into focus when multiple treating and diagnostic physicians get together to look at the whole picture.”
The aggressive use of multidisciplinary care for patients with HCC and PA at Baylor Sammons Cancer Center brings high-quality, evidence-based, personalized diagnosis and treatment to patients with these extremely complex diseases. But clearly, new approaches are needed to improve the grim survival statistics still attached to these diseases. In the rest of this issue, we focus on new research directions that are being investigated to overcome the barriers that have pre-vented effective treatment of HCC and PA in the past.
The second annual GI Cancer Conference entitled “Liver Cancer—What Now?” was held on February 9, 2013. This event center-ed on the diagnosis, treatment, and management of liver cancers, but also featured a special lecture on the current treatment of colorectal cancer by the new chief of the Baylor University Medical Center Department of Surgery, James W. Fleshman, Jr., MD. The conference was attended by more than 90 medical professionals from across North Texas.
Expert faculty from Baylor lectured on treatment of hepatocellular carcinoma, an overview of the liver tumor, radiological caveats in liver tumors, liver metastasis from neuroendocrine carcinoma and other causes, surgical resection and ablative techniques for liver tumors, intraarterial therapies for liver cancer, and transplantation for liver tumors. The audience was able to put some of their new-found knowledge to work in a lively discussion of case presentations, with a panel of conference speakers providing their opinions and adding to the discussion. The speakers from Baylor were all part of the Baylor Liver and Pancreas Disease Center, a team of physicians who are dedicated to the treatment and management of these often difficult-to-treat tumors. This multidisciplinary group of physicians meets at bimonthly site-specific tumor conferences to discuss and establish the treatment plan needed for each patient with liver cancer.
In addition to talks and case presentations, participants were able to interact with the faculty at breaks and during a sit-down luncheon. General tours of Baylor Sammons Cancer Center were offered, along with an in-depth tour of the new Innovative Clinical Trials Center, which is located on the 7th floor of the cancer center.
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 7
A Bridge to Transplant: The Effectiveness of Local TherapiesThe grim overall prognosis for patients with hepatocellular carcinoma (HCC) tends to mask the fact that, for selected patients, the possibility of a cure and/or a dramatic improve-ment in quality of life is very real. These are patients who are not good candidates for surgery, but who are, or may become, good candidates for liver transplant. Because there is frequently an extensive waiting period before a liver is available for transplant, these patients may require one or more local therapies to treat new tumors that occur during that time. These therapies serve as a “bridge” to transplant.
A variety of local therapies are used for the treatment of HCC at Baylor Liver and Pancreas Disease Center at Baylor University Medical Center at Dallas:
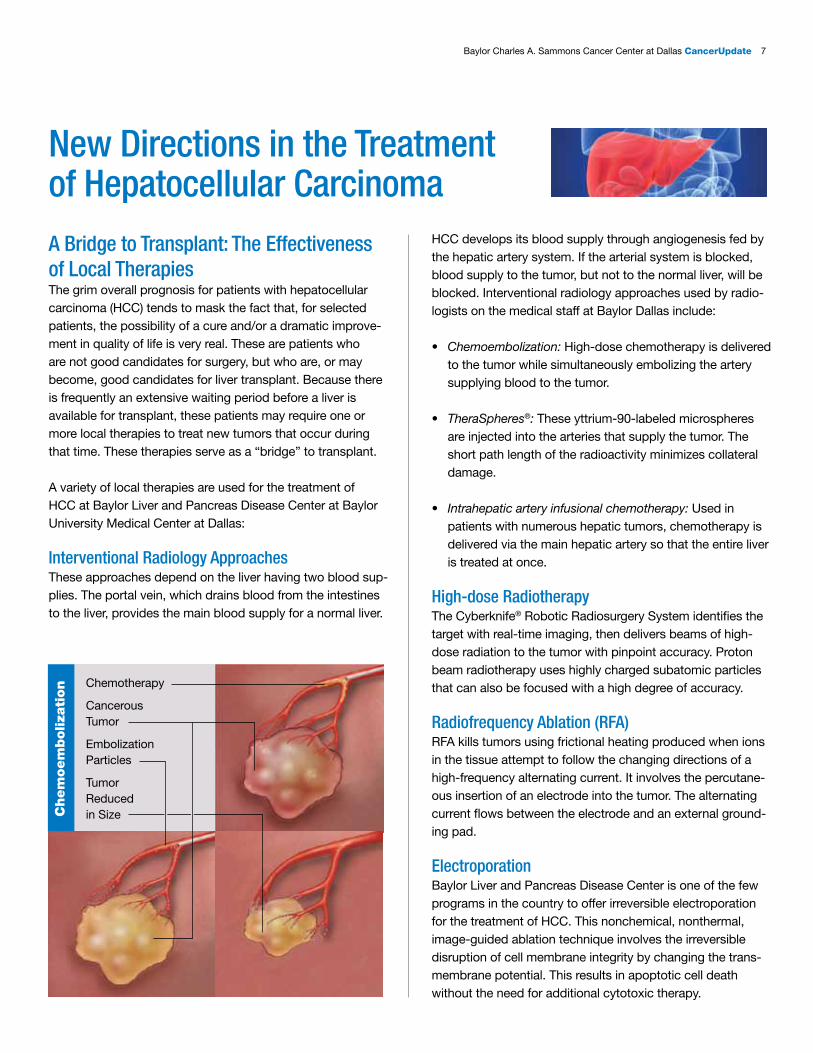
Interventional Radiology ApproachesThese approaches depend on the liver having two blood sup-plies. The portal vein, which drains blood from the intestines to the liver, provides the main blood supply for a normal liver.
New Directions in the Treatment of Hepatocellular Carcinoma
HCC develops its blood supply through angiogenesis fed by the hepatic artery system. If the arterial system is blocked, blood supply to the tumor, but not to the normal liver, will be blocked. Interventional radiology approaches used by radio-logists on the medical staff at Baylor Dallas include:
• Chemoembolization: High-dose chemotherapy is delivered to the tumor while simultaneously embolizing the artery supplying blood to the tumor.
• TheraSpheres®: These yttrium-90-labeled microspheres are injected into the arteries that supply the tumor. The short path length of the radioactivity minimizes collateral damage.
• Intrahepatic artery infusional chemotherapy: Used in patients with numerous hepatic tumors, chemotherapy is delivered via the main hepatic artery so that the entire liver is treated at once.
High-dose RadiotherapyThe Cyberknife® Robotic Radiosurgery System identifies the target with real-time imaging, then delivers beams of high-dose radiation to the tumor with pinpoint accuracy. Proton beam radiotherapy uses highly charged subatomic particles that can also be focused with a high degree of accuracy.
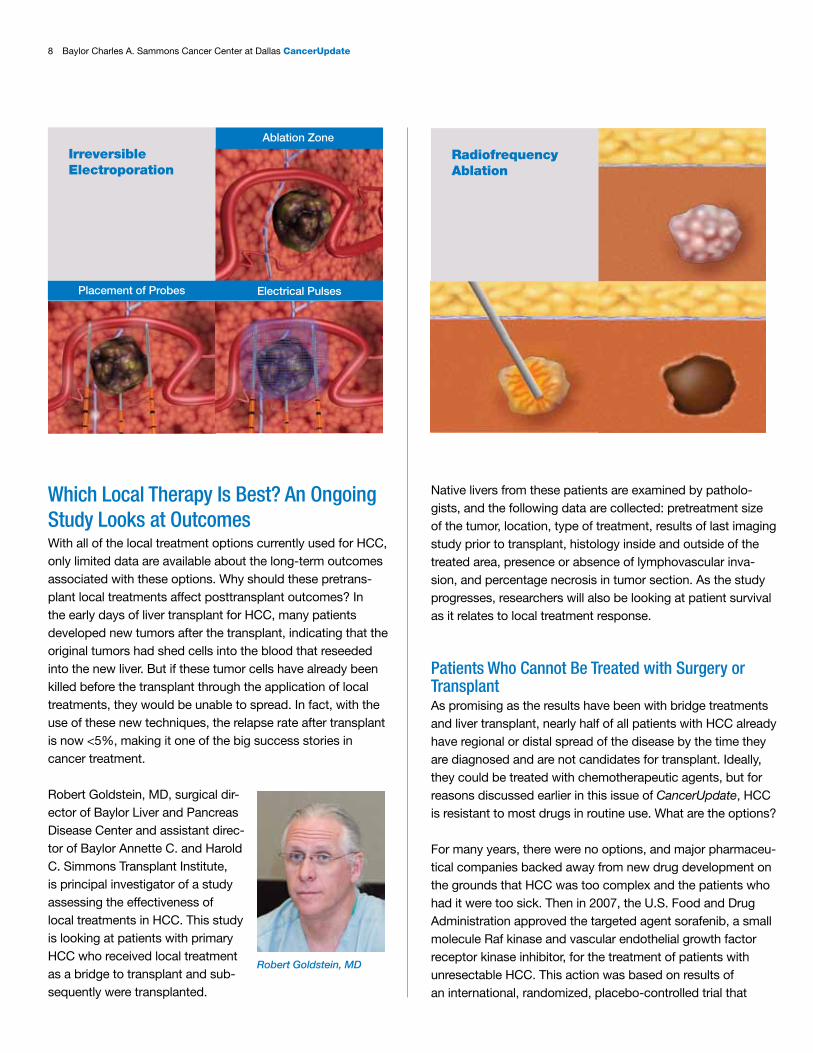
Radiofrequency Ablation (RFA)RFA kills tumors using frictional heating produced when ions in the tissue attempt to follow the changing directions of a high-frequency alternating current. It involves the percutane-ous insertion of an electrode into the tumor. The alternating current flows between the electrode and an external ground-ing pad.
ElectroporationBaylor Liver and Pancreas Disease Center is one of the few programs in the country to offer irreversible electroporation for the treatment of HCC. This nonchemical, nonthermal, image-guided ablation technique involves the irreversible disruption of cell membrane integrity by changing the trans-membrane potential. This results in apoptotic cell death without the need for additional cytotoxic therapy.
Chem
oem
boliza
tion Chemotherapy
Cancerous Tumor
Embolization Particles
Tumor Reduced in Size
8 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Which Local Therapy Is Best? An Ongoing Study Looks at OutcomesWith all of the local treatment options currently used for HCC, only limited data are available about the long-term outcomes associated with these options. Why should these pretrans-plant local treatments affect posttransplant outcomes? In the early days of liver transplant for HCC, many patients developed new tumors after the transplant, indicating that the original tumors had shed cells into the blood that reseeded into the new liver. But if these tumor cells have already been killed before the transplant through the application of local treatments, they would be unable to spread. In fact, with the use of these new techniques, the relapse rate after transplant is now <5%, making it one of the big success stories in cancer treatment.
Robert Goldstein, MD, surgical dir-ector of Baylor Liver and Pancreas Disease Center and assistant direc-tor of Baylor Annette C. and Harold C. Simmons Transplant Institute, is principal investigator of a study assessing the effectiveness of local treatments in HCC. This study is looking at patients with primary HCC who received local treatment as a bridge to transplant and sub-sequently were transplanted.
Native livers from these patients are examined by patholo-gists, and the following data are collected: pretreatment size of the tumor, location, type of treatment, results of last imaging study prior to transplant, histology inside and outside of the treated area, presence or absence of lymphovascular inva-sion, and percentage necrosis in tumor section. As the study progresses, researchers will also be looking at patient survival as it relates to local treatment response.
Patients Who Cannot Be Treated with Surgery or TransplantAs promising as the results have been with bridge treatments and liver transplant, nearly half of all patients with HCC already have regional or distal spread of the disease by the time they are diagnosed and are not candidates for transplant. Ideally, they could be treated with chemotherapeutic agents, but for reasons discussed earlier in this issue of CancerUpdate, HCC is resistant to most drugs in routine use. What are the options?
For many years, there were no options, and major pharmaceu-tical companies backed away from new drug development on the grounds that HCC was too complex and the patients who had it were too sick. Then in 2007, the U.S. Food and Drug Administration approved the targeted agent sorafenib, a small molecule Raf kinase and vascular endothelial growth factor receptor kinase inhibitor, for the treatment of patients with unresectable HCC. This action was based on results of an international, randomized, placebo-controlled trial that
Electrical Pulses
Ablation Zone
Placement of Probes
IrreversibleElectroporation
Radiofrequency Ablation
Robert Goldstein, MD
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 9
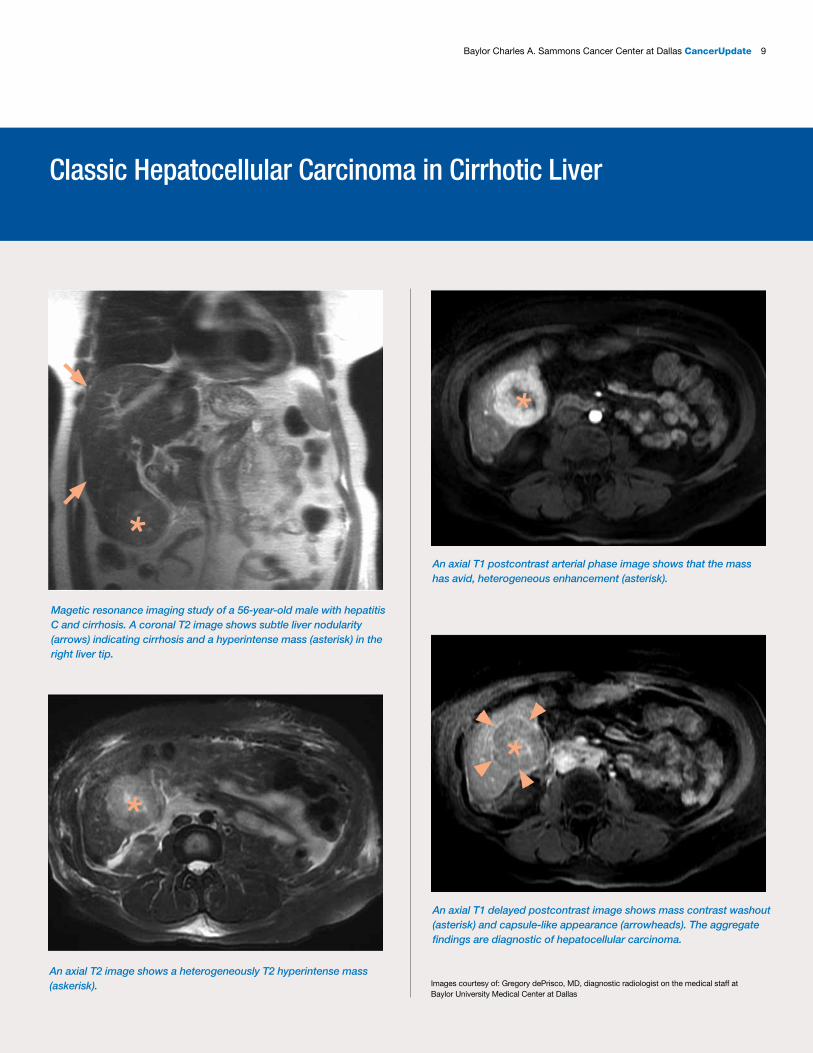
Magetic resonance imaging study of a 56-year-old male with hepatitis C and cirrhosis. A coronal T2 image shows subtle liver nodularity (arrows) indicating cirrhosis and a hyperintense mass (asterisk) in the right liver tip.
An axial T2 image shows a heterogeneously T2 hyperintense mass (askerisk).
An axial T1 postcontrast arterial phase image shows that the mass has avid, heterogeneous enhancement (asterisk).
An axial T1 delayed postcontrast image shows mass contrast washout (asterisk) and capsule-like appearance (arrowheads). The aggregate findings are diagnostic of hepatocellular carcinoma.
*
*
*
*
Classic Hepatocellular Carcinoma in Cirrhotic Liver
Images courtesy of: Gregory dePrisco, MD, diagnostic radiologist on the medical staff at Baylor University Medical Center at Dallas
10 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
found a significant advantage for sorafenib versus placebo in overall survival (10.7 vs. 7.9 months) and time to progression (5.5 vs. 2.8 months).
In the subsequent years, however, it has become clear that the benefits of sorafenib, either alone or in combination, are modest. In addition, studies using sorafenib as a control arm to test other targeted agents, including sunitinib, brivanib, and linifanib, have yielded disappointing results.
Nonetheless, interest has been reignited in finding more effective targeted agents to treat advanced HCC. Because HCC is a highly vascular tumor, agents that affect angiogen-esis are under active investigation. Multiple pathways thought to be involved in liver carcinogenesis are also being mined for new targets: insulin-like growth factor receptor, mammalian target of rapamycin (mTOR), the c-Met pathway, the Raf/MEK/ERK pathway, and the JAK/Stat pathway. Researchers are more excited now than at any recent time about the possibility of finding more effective treatments for this grim disease.
The first annual Texas Cancer Vaccine Symposium was held at Baylor Charles A. Sammons Cancer Center at Dallas on January 22, 2013. This symposium was jointly sponsored by Baylor Sammons Cancer Center, Baylor Institute for Immunology Research, and the University of Texas MD Anderson Cancer Center at Houston. This will be an annual meeting which will alternate between Dallas and Houston, with MD Anderson hosting next year’s symposium. More than 160 attendees participated from institutions across Texas. Speakers included faculty from both Baylor and MD Anderson, as well as featured speakers such as Bruce Beutler, MD, director of the Center for Genetics of Host Defense at the University of Texas Southwestern Medical Center at Dallas. Dr. Beutler received the Nobel Prize in Physiology or Medicine in 2011 for his work in the identification of the role for the Toll-like receptor 4 in infection.
Another guest speaker was Carl H. June, MD, director of translational research at the University of Pennsylvania’s Abramson Cancer Center. Dr. June was named the corecipient of the 2012 Ernst Beutler Lecture and Prize from the American Society of Hematology in December 2012, not only for his contributions to our understanding of the biology of the immune system, but for his progress in making a genetically engineered version of a patient’s own T cells to attack cancer in patients with chronic lymphocytic leukemia. The day was full of thought-provoking lectures on new advances in understanding the immune system and on the design of vaccines to treat cancer.
Texas Cancer Vaccine Symposium January 22, 2013 • 8aM to 6PM
Spea
kerS
10 th floor of the Charles A. Sammons Cancer Center, 3410 Worth St., Dallas, TX 75246
James Allison, PhD, Memorial Sloan-Kettering Cancer Center, New York, NYBruce Beutler, MD, University of Texas Southwestern Medical Center, Dallas, TXLaurence Cooper, MD, PhD, The University of Texas MD Anderson Cancer Center, Houston, TXMark Davis, PhD, Stanford University, Stanford, CAChen Dong, PhD, The University of Texas MD Anderson Cancer Center, Houston, TXRonald Germain, MD, PhD, National Institute of Allergy and Infectious Diseases, Bethesda, MDPatrick Hwu, MD, The University of Texas MD Anderson Cancer Center, Houston, TXCarl June, MD, University of Pennsylvania Perelman School of Medicine, Philadelphia, PALarry Kwak, MD, PhD, The University of Texas MD Anderson Cancer Center, Houston, TXYong-Jun Liu, MD, PhD, Baylor Institute for Immunology Research, Dallas, TXCornelius Melief, MD, PhD, ISA PharmaceuticalsJeff Molldrem, MD, The University of Texas MD Anderson Cancer Center, Houston, TXKarolina Palucka, MD, PhD, Baylor Institute for Immunology Research, Dallas, TXDrew Pardoll, MD, PhD, Sydney Kimmel Comprehensive Cancer Center, Johns Hopkins University, Baltimore, MDVirginia Pascual, MD, Baylor Institute for Immunology Research, Dallas, TX
OrGaNIZerSLarry Kwak, MD, PhD
Yong-Jun Liu, MD, PhDAlan Miller, MD, PhD
Jeff Molldrem, MDKarolina Palucka, MD, PhD
reGIStratION IS lImIted. reGISter tOday!Physicians are members of the medical staff at one of Baylor Health Care System’s subsidiary,
community, or affiliated medical centers and are neither employees nor agents of those medical centers or Baylor Health Care System. ©2012 Baylor Health Care System BRI_176_2012 RT
Free eventPre-registration is required.
To register or submit an abstract for a poster, email [email protected].
Daniel D. Von Hoff, MD, to Join the Fellows of the Amerian Association for Cancer Research Academy
We are proud to announce that Daniel D. Von Hoff, MD, an advisor to the Innovative Clinical Trials Center (ICTC) at Baylor Sammons Cancer Center and Physician-In-Chief of the Translational Genomics Research Institute in Phoenix, has been selected as an inaugural member of the recently formed Fellows of the American Association for Cancer Research Academy. A few of Dr. Von Hoff’s recent and continuing contributions to cancer research can be found on page 14 of this issue.

Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 11
Most of these patients will die from distant disease, not from recurrence at the surgery site. We don’t really need better surgery for pancreatic cancer; we need better chemother-apy to give our patients the best chance of a cure.”
Growing knowledge about the cellular and molecular biology of PA is identifying many new direc-tions for systemic treatment, but these new directions need to be tested in clinical trials. Such clinical trials bring new knowledge about PA and also may represent the best available care for these patients. John T. Preskitt, MD, medical director of the Division of Surgical Oncology at Baylor University Medical Center at Dallas, comment-ed: “Given the limited treatment options that are currently available, most of these patients need to be in clinical trials. That’s why it’s important to be at a place like Baylor Sammons Cancer Center, where the clinicians on our medical staff are closely integrated with the clinical scientists at Baylor Research Institute. Patients can be enrolled in novel clinical trials simultaneously with their initial treatment.”
FOLFIRINOX: Bringing It into the Neoadjuvant ArenaGemcitabine is a nucleoside analogue that was approved by the U.S. Food and Drug Administration in 1996 as a first-line treatment for patients with locally advanced (nonresectable Stage II or Stage III) or metastatic (Stage IV) PA who had been previously treated with 5-fluorouracil (5-FU). Used alone or in combination, gemcitabine remained the sole category 1 rec-ommendation for patients with PC until 2011, when results of a new clinical trial testing FOLFIRINOX (5-fluorouracil, leucovorin, irinotecan, and oxaliplatin) became available. In that trial, FOLFIRINOX produced significantly better rates of overall survival that gemcitabine when given as first-line treatment in patients with metastatic PA (11.1 months vs. 6.8 months, respectively). Based on this study, FOLFIRINOX has become the second category 1 recommendation for chemo-therapy in PA.
With the proven efficacy of FOLFIRINOX in the metastatic arena, Dr. Celinski and Carlos Becerra, MD, medical director of the Innovative Clinical Trials Center at Baylor Sammons Cancer Center, have initiated a clinical trial at Baylor University Medical Center evaluating a neoadjuvant FOLFIRI-NOX regimen in patients with nonmetastatic PA. Dr. Celinski said, “Our patients who die from pancreatic cancer after surgery die from metastasis: the cells were there when we operated, but not detectable. By giving FOLFIRINOX up front, we hope to get rid of those cells before we go after the pri-mary tumor.” Although the original studies in the metastatic arena had problems with toxicity, Dr. Celinski reported that patients in the current trial have tolerated the drug combina-
New Directions in the Treatment of Pancreatic AdenocarcinomaUnlike liver cancer, where innovative developments in localized therapy have significantly
improved patient outcomes, surgical techniques for pancreatic adenocarcinoma (PA) have not
changed a great deal over the last decade. In fact, as noted by Scott Celinski, MD, a surgical
oncologist on the medical staff at Baylor University Medical Center at Dallas, “When we do
surgery, our goal is to cure the patient. But realistically, the 5-year survival rates after surgery
for this disease are only about 25% to 30%.
Scott Celinski, MD
John T. Preskitt, MD
Daniel D. Von Hoff, MD, to Join the Fellows of the Amerian Association for Cancer Research Academy

12 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
tion very well. The study, which plans to enroll 100 patients, will measure progression-free survival as the primary outcome.
Attacking the Stroma PA is one of the most stroma-rich tumors. The stroma is characterized by an abundance of rigid desmoplasia that can compress blood vessels, impeding the delivery of cytotoxic drugs. A number of approaches to disrupting the stromal bar-rier have shown promise in preclinical trials, and researchers are now beginning to investigate those approaches in human clinical trials.
Hyaluronic acid (HA) is abundant in the stroma of PAs, and excess HA can lead to increased interstitial fluid pressure and compressed blood vessels. Preclinical trials have shown that enzymatically attacking HA with hyaluronidase can decrease the fluid pressure, resulting in better drug delivery. Dr. Becerra is initiating a study to assess the efficacy of hyaluronidase in combination with chemotherapy for the treatment of advanced PA.
A promising new approach for disruption of the stroma and delivery of cytotoxic drugs involves the use of ultrasound-targeted microbubble destruction (UTMD). Microbubbles are about the size of a red blood cell, with a gas core inside a stabilizing shell. The microbubbles are injected intravenously and destroyed by ultrasound within the microcirculation of the target organ. This process can cause mechanical disruption in the sur-rounding tissue and also allows the localized release of gene therapy or chemotherapeutic agents carried by the microbubbles. Paul Grayburn, MD, medical director of cardiology research at Baylor Heart and Vascular Institute, Dallas, has used UTMD in preclinical models of diabetes for delivery of the human insulin gene, with subse-quent expression of human insulin and C-peptide and lowering of blood glucose. Now, Dr. Grayburn is working with Dr. Becerra to design a phase I study investigating the usefulness of microbubbles for the treatment of patients with advanced PC. Initial studies will investigate
the effects of UTMD on the integrity and vascularization of the tumor stroma.
Nab-paclitaxel is an albumin-bonded formulation of paclitaxel that, unlike native paclitaxel, does not require a toxic carrier for administration. In various solid tumors, including breast cancer, it appears to be superior to paclitaxel, possibly due to enhanced permeability and retention. In PA, the albumin in nab-paclitaxel binds to SPARC proteins on stromal fibro-blasts. SPARC (secreted protein acidic and rich in cysteine) may have a role in tumor cell growth, differentiation, and metastasis. Its expression on stromal fibroblasts is inversely correlated with survival. When the albumin in nab-paclitaxel binds to the SPARC proteins, the stroma is disrupted and permeability of the tumor to chemotherapeutic agents increases. At the recent Gastrointestinal Cancers Symposium held in San Francisco, Daniel Von Hoff, MD, and associates presented the potentially practice-changing results of a phase III study of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic PA. Compared with gemcitabine alone, nab-paclitaxel plus gemcitabine showed statistically significant and clinically meaningful increases in overall survival, progression-free survival, time to treatment failure, and overall response rate.
Dr. Von Hoff, who is physician-in-chief and director of trans-lational research at the Translational Genomics Research Institute in Phoenix, Ariz., chief scientific officer of Scottsdale Healthcare, and chief scientific officer for US Oncology, serves as an advisor to the new Innovative Clinical Trials Center (ICTC) at Baylor Sammons Cancer Center. His research into the use of nab-paclitaxel for the treatment of advanced PA, carried out with support from the private fund-ing initiative Stand Up 2 Cancer, has revealed some interest-ing and unexpected new aspects of how this drug works to attack PA cells. Dr. Von Hoff is working with Dr. Becerra to bring related research to the ICTC (see article on page 14).
Early Screening A major factor in the lethality of PA is its silent nature during the early course of the disease. Although success has been limited in devising approaches for early screening, several ideas have promise, according to Michelle Shiller, DO, MPST, medical director of the Hereditary Cancer Risk Program and a pathologist on the medical staff at Baylor Dallas:
• A potential way to detect early stage PA is through metabolomics. Metabolomics is the rapid, high-throughput
Carlos Becerra, MD
Paul Grayburn, MD
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 13
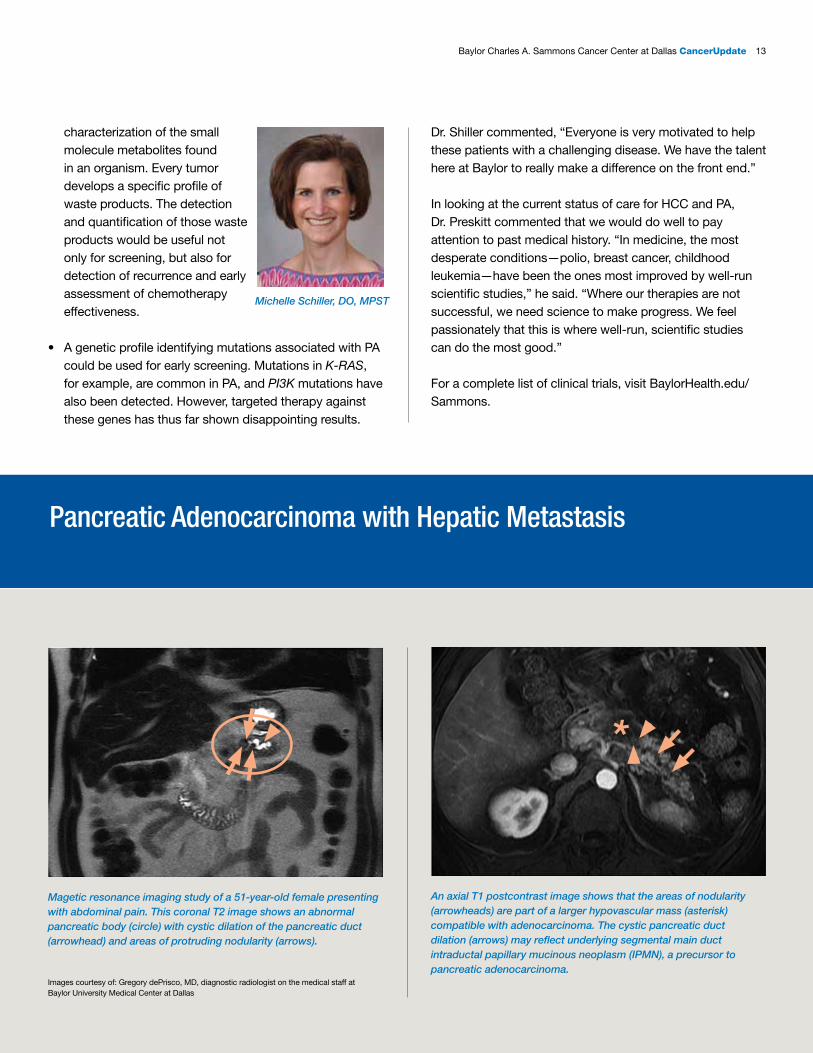
Magetic resonance imaging study of a 51-year-old female presenting with abdominal pain. This coronal T2 image shows an abnormal pancreatic body (circle) with cystic dilation of the pancreatic duct (arrowhead) and areas of protruding nodularity (arrows).
An axial T1 postcontrast image shows that the areas of nodularity (arrowheads) are part of a larger hypovascular mass (asterisk) compatible with adenocarcinoma. The cystic pancreatic duct dilation (arrows) may reflect underlying segmental main duct intraductal papillary mucinous neoplasm (IPMN), a precursor to pancreatic adenocarcinoma.
*
characterization of the small molecule metabolites found in an organism. Every tumor develops a specific profile of waste products. The detection and quantification of those waste products would be useful not only for screening, but also for detection of recurrence and early assessment of chemotherapy effectiveness.
• A genetic profile identifying mutations associated with PA could be used for early screening. Mutations in K-RAS, for example, are common in PA, and PI3K mutations have also been detected. However, targeted therapy against these genes has thus far shown disappointing results.
Dr. Shiller commented, “Everyone is very motivated to help these patients with a challenging disease. We have the talent here at Baylor to really make a difference on the front end.”
In looking at the current status of care for HCC and PA, Dr. Preskitt commented that we would do well to pay attention to past medical history. “In medicine, the most desperate conditions—polio, breast cancer, childhood leukemia—have been the ones most improved by well-run scientific studies,” he said. “Where our therapies are not successful, we need science to make progress. We feel passionately that this is where well-run, scientific studies can do the most good.”
For a complete list of clinical trials, visit BaylorHealth.edu/Sammons.
Pancreatic Adenocarcinoma with Hepatic Metastasis
Images courtesy of: Gregory dePrisco, MD, diagnostic radiologist on the medical staff at Baylor University Medical Center at Dallas
Michelle Schiller, DO, MPST
14 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
This coalition came about under the auspices of Stand Up 2 Cancer (SU2C). SU2C is a groundbreaking initiative created to accelerate innovative cancer research that will get new therapies to patients quickly. The privately funded program encourages col-laboration through the establish-ment of scientific “dream teams” that bring together researchers with diverse viewpoints to focus on a single problem. Dr. Von Hoff commented: “The progress we’ve witnessed in this program is at the level of incredible. I’ve been around cancer research a lot of years, and this is the most excited I’ve been about the genuine new ideas out there to target this disease.”
Through their work together, Drs. Von Hoff and Thompson have made two major discoveries. First, Dr. Von Hoff identified a stromal target for nab-paclitaxel, the SPARC protein, and found that it was present in 80% of PAs. This was the basis of a series of clinical trials, most recently the phase III trial reported in San Francisco, that demonstrated that nab-pacli-taxel was very active in PA, increasing 1-year overall survival from 22% to 35%, with minimal toxicity. Of 33 clinical trials since 1990 testing drugs for the treatment of PA, only three have previously shown positive results; this is the fourth. In addition, nab-paclitaxel can be used in the neoadjuvant setting to make inoperable tumors operable.
The second major finding had to do with the relatively new area of metabolic studies. PA tumors that had been removed from patients were analyzed to see what kind of food source the tumor cells used. There were two interesting observations. Amino acid levels were extremely low, indicating that the tumor cells were hanging on by a thread, very near the star-vation level. This means that relatively minor perturbations in their food source could actually starve the tumors. The second observation was about what the food source is. In general, tumor cells tend to preferentially use glucose. In the case of PA, the cells appeared to be engulfing and eating albumin, including the albumin coating the nab-paclitaxel. This means that nab-paclitaxel is not only disrupting the stroma, but also perhaps working through a Trojan horse mechanism. More importantly, it means that, if PA cells are near starvation and if their primary food source is albumin, stopping the utilization of that fuel should be an effective weapon against PA.
As advisor to the Innovative Clinical Trials Center (ICTC) at Baylor Sammons Cancer Center, Dr. Von Hoff is working to bring related research to the center. He and Carlos Becerra, MD, medical director of the ICTC, are putting together a study looking at the ability of 5-azacytidine to upregulate SPARC in PA tumors, making them more susceptible to nab-paclitaxel. He is also working with Karolina Palucka, MD, PhD, investiga-tor and Michael A.E. Ramsay Chair for Cancer Immunology Research at Baylor Institute for Immunology Research, on unmasking and upregulating immunogenic targets in PA tumors and tumor stroma to support development of a dendritic cell vaccine against pancreatic cancer.
Starving Cancer: Could This Be the Answer to Pancreatic Adenocarcinoma?As director of translational research at the Translational Genomics Research Institute in Phoenix,
Daniel Von Hoff, MD, has joined forces with Craig B. Thompson, MD, from Memorial Sloan-
Kettering Cancer Center in New York, to launch a multipronged attack against pancreatic cancer.
Daniel Von Hoff, MD
“The progress we’ve witnessed in this program is at the level of incredible. I’ve been around cancer research a lot of years, and this is the most excited I’ve been about the genuine new ideas out there to target this disease.” Daniel Von Hoff, MD
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 15
Dr. Fleshman’s area of expertise is colon and rectal surgery; he is especially well known for his innovations in the area of laparo-scopic resection. He has served as president of the American Board of Colon and Rectal Surgery, president of the Research Foundation of the American Society of Colon and Rectal Surgeons, and president of the American Society of Colon and Rectal Surgeons.
Dr. Fleshman noted that the Department of Surgery at Baylor Dallas is extremely strong in general surgery. His goal is to take this strong surgical department and turn it into an academic department of surgery, with greater emphasis on research. To help spearhead this effort, he is in the process of opening three studies on rectal cancer:
• A phase III prospective randomized trial comparing laparo-scopic-assisted resection versus open resection for rectal cancer. Laparoscopic-assisted resection is a less invasive type of surgery for rectal cancer that may have fewer side effects and an improved recovery compared with open resection. The primary goal of this study is to determine if laparoscopic-assisted resection is comparable to open resection in treating patients with stage IIA, stage IIIA, or stage IIIB rectal cancer, based on a composite primary endpoint of oncologic factors that are indicative of a safe and feasible operation.
• A phase II/III trial of neoadjuvant FOLFOX with selective use of combined modality chemoradiation versus preoperative combined modality chemoradiation for locally advanced rectal cancer patients undergoing low anterior resection with total mesorectal excision. A combination of surgery, chemotherapy, and radiation is normally used for the treat-ment of rectal cancer. The purpose of this randomized study is to find out how well chemotherapy alone with sur-gery compares with chemotherapy plus radiation therapy with surgery in treating patients with rectal cancer.
• RObotic versus LAparoscopic Resection for Rectal Cancer (ROLARR). Robotic-assisted laparoscopic surgery has been shown to be safe and effective in a number of differ-ent surgeries, but the data from robotic-assisted rectal cancer surgery are limited to small data sets. The goal of this international, multicenter, prospective study is to compare technical, functional, and oncologic outcomes in robotic-assisted versus laparoscopic surgery with curative intent for rectal cancer.
The results of these clinical trials will have major impacts on the type of surgical and treatment interventions practiced for treatment of rectal cancer.
Dr. Fleshman is working with John Preskitt, MD, medical director of the Division of Surgical Oncology, and C. Richard Boland, MD, chief of the Division of Gastroenterology, to establish a data registry on colorectal cancer patients at Baylor Dallas, as part of the Surgical Oncology Research Database (SOCRD). This registry will include patient data on pathology, surgical approach, treatment, genetics, follow up, and quality of life issues, and will be used to facilitate research in colorectal cancer.
James W. Fleshman, Jr., MD, Joins Baylor Dallas as New Chief of SurgeryBaylor Charles A. Sammons Cancer Center at Dallas welcomes James W. Fleshman, Jr., MD,
as the new chief of the Department of Surgery for Baylor University Medical Center at Dallas.
Dr. Fleshman comes to Baylor Dallas from Missouri, where he was chief of the section of colon
and rectal surgery at the Washington University School of Medicine, as well as chief of surgery
at the Barnes-Jewish West County Hospital in St. Louis.
James W. Fleshman, Jr., MD
16 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Young surgeons require support to start and develop an academic career. Such support is available through career development awards offered by a number of societies, includ-ing the Research Foundation of the Society of Colon and Rectal Surgeons, the Society for Surgery of the Alimentary Tract, and the Society of Surgical Oncology. Applicants are reviewed on their research proposal, their career development plan and letters of recommendation. Dr. Fleshman plans to assist young surgeons on the medical staff to obtain career development awards to aid them in developing a robust academic career.
Dr. Fleshman is creating a colorectal cancer multidisciplinary team with the goal of establishing a center of excellence in colorectal cancer. The team is composed of genetic counsel-ors, pathologists, medical oncologists, radiation oncologists, colon and rectal surgeons, surgical oncologists, and radiolo-gists. All of the members review the plan of care for every patient with colorectal cancer. Thus, patients receive a tailored treatment plan, which is in keeping with guidelines of the National Comprehensive Cancer Network and the American Society of Colon and Rectal Surgeons. Not only is the plan for a patient’s care vetted by the team, but the handling of the plan will be gauged by quality measures: Was the appropriate chemotherapy started in a timely manner? Were biologics used appropriately? Were the surgeons able to obtain a complete resection? Was the surgery done properly?
These are all questions that will be addressed. The goal is to create and adhere to a set of standards that will be used consistently for all patients, with checks to make sure quality is maintained. This multidisciplinary approach and standard-ization of treatment can then be created for other cancers, such as pancreas and breast cancers. Through standardiza-tion of treatments for a given type of cancer, a checklist can be developed to provide each patient who comes through the doors of Baylor Dallas quality care.
Finally, in another topic of extreme importance to Dr. Fleshman, an inherited colorectal cancer registry is being created, with help from Dr. Boland and Laura Panos, a genetic counselor at Baylor Dallas. The registry will include informa-tion on patients with Lynch syndrome, familial adenomatous polyposis, and young patients not classified in a specific syndrome. The purpose of this registry is to guide and support patients and their families with inherited colorectal cancers. With the registry, Baylor Dallas will have the ability to be in contact with patients and their families. They can send out letters and other information, as well as arrange support group meetings for patients and their families.
Dr. Fleshman brings to Baylor Dallas impressive expertise and exciting plans for the future. He commented: “I’m inspired by new challenges and I try to lead in a way that helps those around me to succeed and fulfill their dreams and goals.”
“I’m inspired by new challenges and I try to lead in a way that helps those around me to succeed and fulfill their dreams and goals.” James W. Fleshman, Jr., MD
Welcome to New Members of the Medical Staff at Baylor Charles A. Sammons Cancer Center at Dallas
Christine S. Landry, MD—Surgical Oncology
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 17
A native of Arkansas, Dr. Jones came to Dallas to do his general surgery residency at Parkland Memorial Hospital, and he has remained in the Dallas area since. He was a chief surgery resident on November 22, 1963, when President John F. Kennedy was brought to Parkland after being shot. Dr. Jones helped to treat the president until it was evident that he could not be saved. In another twist of fate, two days later, Dr. Jones was in the emergency room again to treat a second gunshot victim, Lee Harvey Oswald.
Dr. Jones joined the surgical faculty of the University of Texas Southwestern Medical Center at Dallas. During his tenure at UT Southwestern, he was in charge of the tumor service, the chemotherapy clinic, and the breast cancer clinic. His life-long areas of clinical interest include surgical infections and antibi-otics, breast surgical oncology, pancreaticoduodenal trauma, and thyroid cancer. Although he trained in general surgery, he has always had a special interest in surgical oncology.
He has contributed a great deal to the community, including being chairman of the medical advisory committee which established the citywide ambulance and emergency medical services in Dallas County in 1971. He received recognition for this service from the Mayor Pro-Tem and the City Council
of Dallas, the Dallas County Board of Commissioners, the Dallas-Fort Worth Hospital Council, and the North Central Texas Council of Governments. Dr. Jones has been very active in the American College of Surgeons (ACS) and was the vice chairman of the Commis-sion on Cancer (COC). He rose from state, to western area, and finally to national chairman of the Field Liaison Program of the COC. Additionally, he served as secretary of the Board of Governors of the ACS. During this time, he came to Baylor Dallas to lead the Department of Surgery. He believes that one of his biggest accomplishments here was directing the surgical residency program and more than doubling its size. Under his leadership, this 5-year program expanded from four to nine chief residents and from 20 to 45 general surgery residents per year. He has graduated 148 general surgery residents during his tenure at Baylor. Dr. Jones has found it very satisfying to work with the faculty and fellows over the years. He mentioned a quote that he shares with the surgical fellows and residents at the end of each year: “The road to success is always under construction.” These words reflect his belief that those in the practice of medicine and surgery must always be learning, always trying to become better at treating patients.
Dr. Jones is staying at Baylor as director of the surgical residency program, so he will be doing what he likes best—helping to train residents. He looks forward to the leadership of Dr. Fleshman and knows the department is in good hands.
Ronald C. Jones, MD, FACS, Ends Distinguished Tenure as Chair of the Department of SurgeryAfter more than 25 years of service, Ronald C. Jones, MD, FACS, is ending his tenure as chair
of the Department of Surgery at Baylor University Medical Center at Dallas. Dr. Jones will remain
as program director of the general surgery residency program, a post he has held concurrently
with his position as chair.
Ronald C. Jones, MD, FACS
18 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Oncologists in private practice, in collaboration with hospitals and insurers, are in a unique position to take the lead in defin-ing treatment and operational standards for the value-based delivery of cancer care.
Baylor Charles A. Sammons Cancer Center at Dallas opened a new facility in 2011 to provide outpatient services for cancer patients, and Baylor University Medical Center at Dallas opened Baylor T. Boone Pickens Cancer Hospital in January 2012 to provide inpatient services. Recognizing a further need to provide continuous quality care, Baylor Dallas, in collabo-ration with Texas Oncology, opened the Oncology Evaluation
and Treatment Center (OETC) and the Infusion Center in March of 2012. Yvonne M. Coyle, MD, is medical director of the OETC.
The OETC and the Infusion Center have a cooperative working relationship and are housed side-by-side in an outpatient facility located on the first floor of the cancer hospital. The OETC provides urgent care after office hours as well as scheduled procedures during office hours for adult oncology patients of all oncology physicians on the medical staff at Baylor Dallas, including Texas Oncology physicians. Diagnostic and therapeutic procedures are available, such as
Development of the Oncology Evaluation and Treatment Center and the Infusion Center on the Baylor Dallas CampusThe ideal cancer care delivery model is coordinated to provide comprehensive multidisciplinary
services, but this type of care can be costly. Therefore, government, employer groups, and
insurers are seeking models for the delivery of quality cancer care that are cost-efficient.
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 19
thoracentesis, paracentesis, and lumbar punctures for the administration of intrathecal chemotherapy. In addition, treat-ments are available outside of normal office hours to maintain adherence to prescheduled clinical research testing. All acute care can be provided at the OETC, with the exception of care required by patients who are transported by emergency medical services or care for patients with acute myocardial infarctions, cerebrovascular accidents, or trauma. If neces-sary, OETC patients may be transferred to the Emergency Department (ED) at Baylor Dallas, which is located near the cancer hospital and is accessible by an indoor connector.
A high percentage of patients who are seen at the OETC are bone marrow transplant recipients. Specialized care for these patients is extremely important, especially for those who have recently undergone a transplant procedure. Some patients must spend several months in the Dallas area after their transplant, and during this time before the new stem cells completely engraft, their immune systems remain weak. Sending these patients to a standard ED for their care during this period could place them at risk of infection. Thus, cre-ation of the OETC and Infusion Center has done much to protect these patients during vulnerable times in their lives.
The Infusion Center is open 24 hours a day, 7 days a week to provide oncology patients access to blood product transfu-sions, as well as hydrating, chemotherapy, and biological therapy infusions. Thus, interruptions in cancer care can be
prevented by administering infusions that are due on week-ends and holidays, when private practice offices are closed.
Analysis of data from the first quarter of operations (between April and July 2012) for the OETC and Infusion Center indi-cates success in reducing preventable health care utilization in a cost-efficient manner. During that quarter, 817 oncology patients received care in one of the facilities: 226 in the OETC and 591 in the Infusion Center. Eighty-nine percent of the oncology patients seen for urgent care at Baylor Dallas were referred by their oncologists to the OETC, instead of to the Baylor Dallas ED. The average time spent in the OETC was 46% shorter than the time spent for oncology patients in Baylor Dallas’ ED (3 hours 54 minutes versus 7 hours 38 minutes), as would be expected since the Baylor Dallas ED is a high-volume level I trauma center. Moreover, the hospital admission rate in the OETC was 36%, less than half the 63.2% rate recently reported for oncology patients in the ED. Furthermore, our new initiatives for conducting health service research within the OETC and Infusion Center hold promise for providing our cancer center and others with results that will assist in developing new methods for effectively organiz-ing, managing, financing, and delivering quality cancer care.
A new health care environment is developing that demands accountability for the cost and quality of care. Through the success of the OETC and the Infusion Center, we have taken another step in the delivery of quality and cost-efficient cancer care.
Quality Cancer Care and the Growing Need for Financial SupportFor more than 35 years, Baylor Charles A. Sammons Cancer Center at Dallas has provided quality clinical care and sup-port services to patients with cancer and their families. A high level of patient care is maintained through investments in technology as well as the training of clinical profession-als to provide an advanced level of care. New approaches that are needed for the detection, treatment, and prevention of diseases such as liver and pancreatic cancer are being tested in innovative research and clinical trials. Support ser-vices help to educate patients and families and guide them through the difficult journey of cancer treatment.
But this high level of service comes at a price. As part of Baylor Health Care System (BHCS), a private, not-for-profit organization, Baylor Sammons Cancer Center must look to multiple sources for the funding needed to maintain and expand its programs.
It has become especially challenging to obtain funds to sup-port research. Historically, most of the important advances in cancer research in the United States have been funded primarily by taxpayer dollars through highly competitive grants from the National Cancer Institute (NCI) to physicians and scientists at cancer centers and universities. Unfortu-nately, the NCI budget has remained essentially flat since 2003, leading to decreases in new awards, in noncompeting awards, and in support for cancer centers. Young research-ers and clinicians are frequently the hardest hit, and many may ultimately leave clinical research, jeopardizing progress for the future.
Addressing this situation, Alan M. Miller, MD, PhD, chief of oncology at BHCS and medical director of Baylor Sammons Cancer Center, commented: “Our greatest need right now is to obtain funds to support research. The number of federal dollars available is not increasing, yet the need for research is ever-increasing. In those cancers, like pancreatic cancer, where our progress has been limited to date, we need to
20 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Baylor Health Care System Foundation: Gathering Financial Support for Quality Cancer Care
At Swim Across America, more than 300 swimmers and volunteers helped raise $275,000 to support the Innovative Clinical Trials Center.
emphasize discovering new and better ways to approach the disease. Philanthropy has become one of the most im-portant ways that we can help innovative research to move the field forward.”
Working with the Baylor Health Care System Foundation: Finding Support for Cancer ProgramsBHCS Foundation, a separately incorporated not-for-profit organization, raises and manages charitable funds to sup-port BHCS and its charitable affiliates. Since the Foundation was established in 1978, it has distributed more than $440 million raised from more than 10,000 active donors.
Over the past year, BHCS Foundation has raised millions of dollars to support cancer initiatives at Baylor. Where does this money come from? Individual Donors Grateful patients and their family members are critical to the success of the fundraising mission of BHCS Foundation. Those who have recently sought to make a donation based on the quality care received at Baylor Sammons Cancer Center include:
• Don and Trudy Steen: Working with United Surgical Part-ners, they have made significant donations in support of leukemia research.
• The Boon Family: In 1992, E. K. Boon came to Baylor Sammons Cancer Center to be treated for renal cell carcinoma and participate in a genetics research program related to his disease. When he died in 1996, his family wanted to continue his legacy and launched a yearly ben-efit golf tournament that celebrated its 14th anniversary last September. To date, this tournament has raised more than $500,000 in support of cancer research.
• David and Karen Shuttee: In gratitude for the extraordi-nary care that Karen has received from Drs. Colin Koon and Lyndsey Harper and the nurses and staff of Baylor Sammons Cancer Center, Karen and David have made
a significant donation to BHCS Foundation by transfer-ring multiple life insurance policies to help fund ongoing operations and research at the Sammons Cancer Center.
• Bruce Selkirk: To honor the memory of his wife, Amy, who died of triple-negative breast cancer in her early 40s, Bruce instituted the Amy T. Selkirk Breast Cancer Vaccine Fund. The goal of the initiative is to raise funds for research and development of therapeutic vaccines for breast cancer patients with high-risk disease.
• Dale and Carolyn Dorin-Ballard: In 2012, professional bowler Dale Ballard was diagnosed with head and neck cancer. In gratitude for the care he received at Baylor Sammons Cancer Center, he and his wife Carolyn started Ballard vs. the Big “C.” This organization held its first bowling tournament in December 2012, raising $15,000 for the fight against cancer.
National and Statewide ProgramsMany organizations that operate at the national and state levels have established a presence in Dallas, where they raise money to support cancer initiatives at Baylor Sammons Cancer Center.
• “Swim Across America” (SAA) holds dozens of com-munity-oriented open-water swims from coast to coast, each used to raise funds for local beneficiaries supporting cancer research, prevention, and treatment. Beginning in 2011, SAA has sponsored an open-water swim at Lake
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 21
BHCS Foundation Director Amy McNabb, Alan Miller, MD, PhD, and SAA Dallas committee member Andrea Dickson
22 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
Ray Hubbard at the Harbor in Rockwall, Texas, to benefit the Innovative Clinical Trials Center (ICTC) at Baylor Sammons Cancer Center. To date, the event has raised more than $600,000.
• Golfers Against Cancer (GAC) was started in 1997 by members of the Deerwood Club in Kingwood, Texas, to show support to a Deerwood member and an assistant pro who both had been diagnosed with cancer at the time. Since then, the organization has spread to major cities including New York, Atlanta, and, now, Dallas. Their first event here in 2012 resulted in a $25,000 gift to support cancer initiatives.
• Young Texans Against Cancer (YTAC) was established in 2001 by a group of 44 young individuals in the Houston area to increase cancer awareness among the genera-tion of 22- to 40-year-olds. The organization is currently very active in Houston, Austin, and Dallas. Last year, the Dallas Chapter of YTAC gave a gift of $50,000 to support programs in gynecologic cancers at Baylor Dallas.
Celebrating Women: A BHCS Foundation EventWith one notable exception, BHCS Foundation is not an event-driven organization. That exception is Celebrating Women, a yearly luncheon to support breast cancer that has become one of the premiere charitable events in the Dallas-Fort Worth area. Over the past 13 years, Celebrating Women donors have raised more than $19 million to support educa-tion, research, technology, and patient-centered programs in the fight against breast cancer. The most recent luncheon, which featured actor and author Rob Lowe as a keynote speaker, had more than 1,350 attendees.
Campaign 2015: “Baylor Makes Us All Better”Additional funding for cancer initiatives at Baylor Sammons Cancer Center will be available from a major comprehensive campaign that was recently launched by BHCS Foundation. Campaign 2015 aims at raising $250 million over the next 2 years. With $165 million already raised, the campaign is focused on four priority areas:
“Through the generous support of philanthropic leaders in our community, Baylor has the opportunity to define the future of cancer care in North Texas. Philanthropy allows us to further our research and conduct clinical trials that offer potentially life-altering results for the patients we serve. In addition, we can make the necessary investments to maintain the qualities that make Baylor unique and special. And that makes us all better.” Rowland K. Robinson
Pam Perella, Rob Lowe and Pam Busbee, at Celebrating Women
At Celebrating Women: Joel Allison, president and CEO, Baylor Health Care System, Mary Anne Cree, Circle of Care Award winner, and Rowland K. Robinson, President of Baylor Health Care System Foundation.
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 23
1. Capital: Buildings and capital equipment2. Programmatic: Patient education and support services3. Research4. Education: Residencies, fellowships, undergraduate
medical education, and continuing medical education for advanced certification
The simple phrase “Baylor Makes Us All Better” expresses the bold vision of Joel Allison, president and CEO of BHCS: to take Baylor to national preeminence in areas of health care that have the power to transform individual lives and the communities we serve. In the drive to develop and support innovative models of care, technological advances, medical education, game-changing research, and effective community health initiatives, philanthropy has never been more important.
What Philanthropic Funding Supports at Baylor Sammons Cancer CenterPhilanthropic funding received at Baylor Sammons Cancer Center is not used primarily for bricks and mortar develop-ment. According to BHCS Foundation president Rowland K. Robinson, ”Through the generous support of philanthropic leaders in our community, Baylor has the opportunity to define the future of cancer care in North Texas. Philanthropy allows
us to further our research and conduct clinical trials that offer potentially life-altering results for the patients we serve. In addition, we can make the necessary investments to maintain the qualities that make Baylor unique and special. And that makes us all better.”
Funds raised at the annual Celebrating Women luncheon have had an impact in multiple areas affecting quality of care for women with breast cancer, including advanced digital imaging technology; funding for medical education; support for patient-centered programs, such as the patient navigation program and cancer center chaplains; and support of research studies looking at better ways to diagnose and treat breast cancer. These funds also support the Celebrating Women chair in Breast Cancer Research at Baylor Sammons Cancer Center currently held by Joyce O’Shaughnessy, MD, furthering Dr. O’Shaughnessy’s research looking for genetically based treatment options for aggressive forms of breast cancer.
Proceeds from the yearly SAA open-water swims support clinical trials at the new ICTC at Baylor Sammons Cancer Center. This center consolidates all phase I clinical trials from Baylor researchers and their academic and clinical research partners in one 6,376-square-foot center. These early trials are an essential component in bringing new treatments from the bench to the bedside.
Additional funding from private donors helps to support the Baylor Sammons Cancer Center’s research grant program. This internal program is designed to help investigators gener-ate the preliminary data needed to compete successfully for external funding. The program is currently funding grants in six categories: pilot projects, gap funding, supplemental funding, trainee cancer research awards, emerging technol-ogy access, and cancer clinical and translational patient trials. Grants submitted to this program are competitive and peer-reviewed. According to Dr. Miller, “We try to be very good stewards of the money that is donated to us. We want to make sure that it is used for things that have a reasonable chance of success.”
“Philanthropy has become one of the most important ways that we can help innovative research to move the field forward.” Alan M. Miller, MD, PhD
24 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
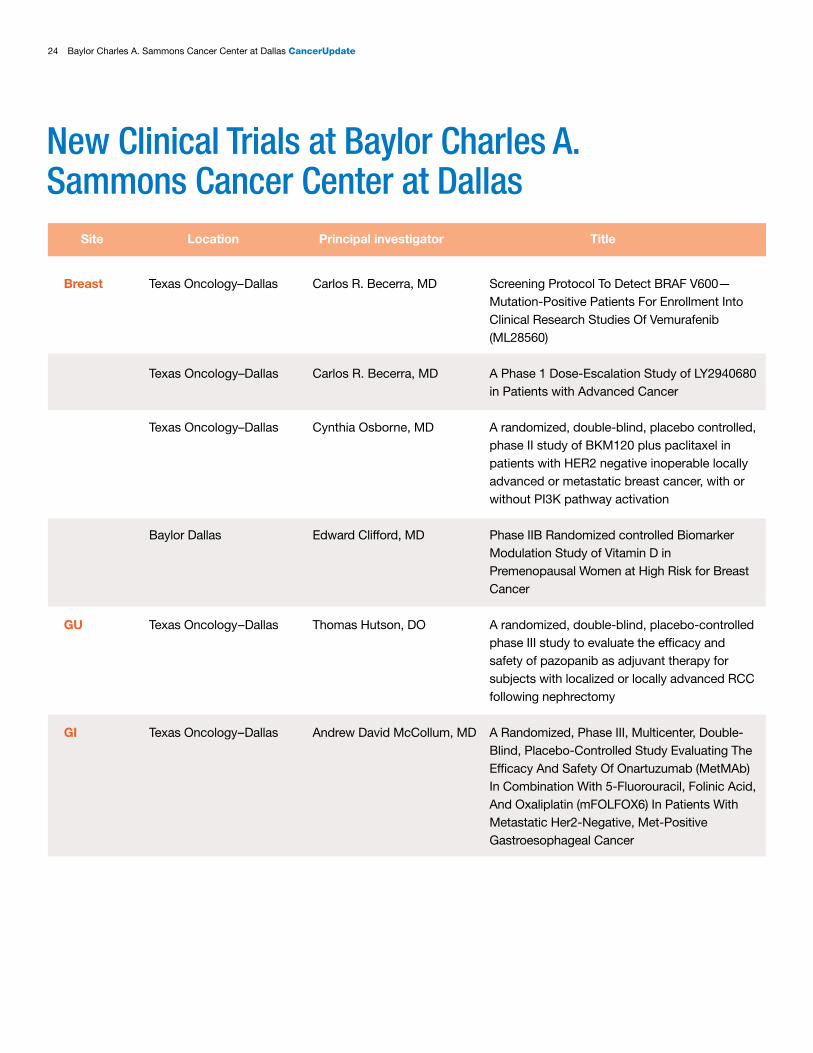
New Clinical Trials at Baylor Charles A. Sammons Cancer Center at Dallas
Site Location Principal investigator Title
Breast Texas Oncology–Dallas Carlos R. Becerra, MD Screening Protocol To Detect BRAF V600— Mutation-Positive Patients For Enrollment Into Clinical Research Studies Of Vemurafenib (ML28560) Texas Oncology–Dallas Carlos R. Becerra, MD A Phase 1 Dose-Escalation Study of LY2940680 in Patients with Advanced Cancer
Texas Oncology–Dallas Cynthia Osborne, MD A randomized, double-blind, placebo controlled, phase II study of BKM120 plus paclitaxel in patients with HER2 negative inoperable locally advanced or metastatic breast cancer, with or without PI3K pathway activation
Baylor Dallas Edward Clifford, MD Phase IIB Randomized controlled Biomarker Modulation Study of Vitamin D in Premenopausal Women at High Risk for Breast Cancer
GU Texas Oncology–Dallas Thomas Hutson, DO A randomized, double-blind, placebo-controlled phase III study to evaluate the efficacy and safety of pazopanib as adjuvant therapy for subjects with localized or locally advanced RCC following nephrectomy
GI Texas Oncology–Dallas Andrew David McCollum, MD A Randomized, Phase III, Multicenter, Double- Blind, Placebo-Controlled Study Evaluating The Efficacy And Safety Of Onartuzumab (MetMAb) In Combination With 5-Fluorouracil, Folinic Acid, And Oxaliplatin (mFOLFOX6) In Patients With Metastatic Her2-Negative, Met-Positive Gastroesophageal Cancer
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 25
Site Location Principal investigator Title
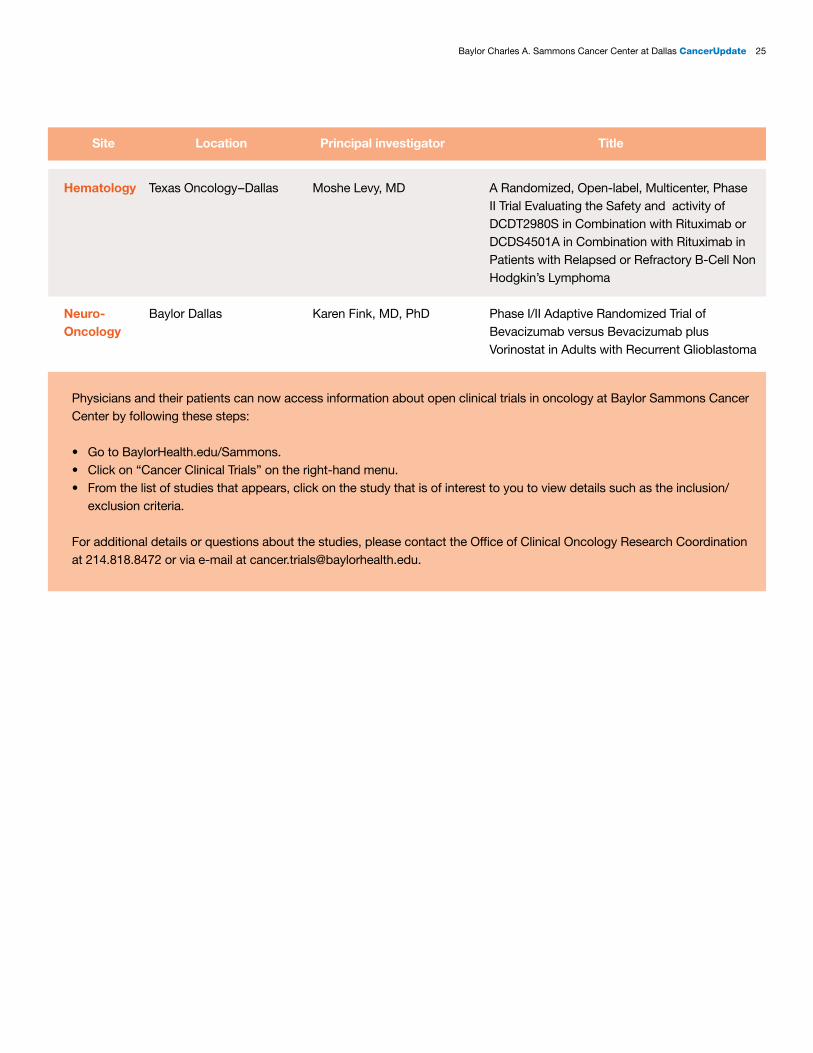
Hematology Texas Oncology–Dallas Moshe Levy, MD A Randomized, Open-label, Multicenter, Phase II Trial Evaluating the Safety and activity of DCDT2980S in Combination with Rituximab or DCDS4501A in Combination with Rituximab in Patients with Relapsed or Refractory B-Cell Non Hodgkin’s Lymphoma
Neuro- Baylor Dallas Karen Fink, MD, PhD Phase I/II Adaptive Randomized Trial of Oncology Bevacizumab versus Bevacizumab plus Vorinostat in Adults with Recurrent Glioblastoma
Physicians and their patients can now access information about open clinical trials in oncology at Baylor Sammons Cancer Center by following these steps:
• Go to BaylorHealth.edu/Sammons.• Click on “Cancer Clinical Trials” on the right-hand menu.• From the list of studies that appears, click on the study that is of interest to you to view details such as the inclusion/
exclusion criteria.
For additional details or questions about the studies, please contact the Office of Clinical Oncology Research Coordination at 214.818.8472 or via e-mail at [email protected].
26 Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate
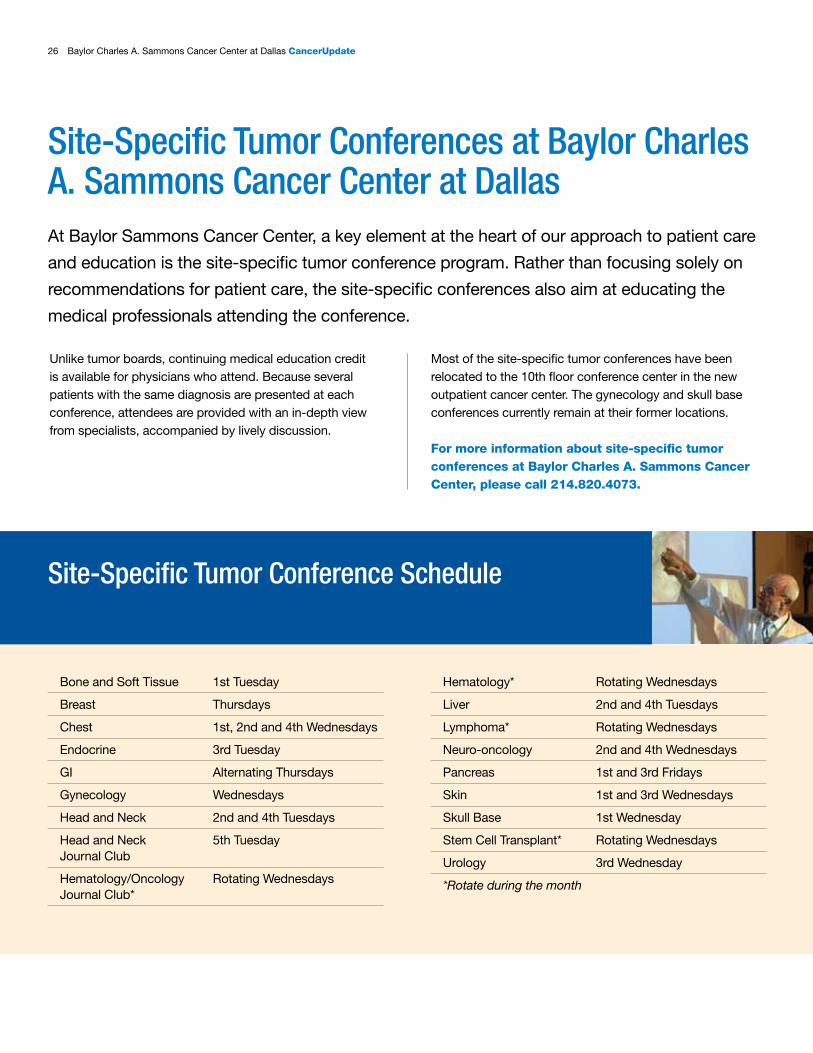
Site-Specific Tumor Conferences at Baylor Charles A. Sammons Cancer Center at Dallas
Unlike tumor boards, continuing medical education credit is available for physicians who attend. Because several patients with the same diagnosis are presented at each conference, attendees are provided with an in-depth view from specialists, accompanied by lively discussion.
Bone and Soft Tissue 1st Tuesday
Breast Thursdays
Chest 1st, 2nd and 4th Wednesdays
Endocrine 3rd Tuesday
GI Alternating Thursdays
Gynecology Wednesdays
Head and Neck 2nd and 4th Tuesdays
Head and Neck 5th Tuesday Journal Club
Hematology/Oncology Rotating Wednesdays Journal Club*
At Baylor Sammons Cancer Center, a key element at the heart of our approach to patient care
and education is the site-specific tumor conference program. Rather than focusing solely on
recommendations for patient care, the site-specific conferences also aim at educating the
medical professionals attending the conference.
Most of the site-specific tumor conferences have been relocated to the 10th floor conference center in the new outpatient cancer center. The gynecology and skull base conferences currently remain at their former locations.
For more information about site-specific tumor conferences at Baylor Charles A. Sammons Cancer Center, please call 214.820.4073.
Site-Specific Tumor Conference Schedule
Hematology* Rotating Wednesdays
Liver 2nd and 4th Tuesdays
Lymphoma* Rotating Wednesdays
Neuro-oncology 2nd and 4th Wednesdays
Pancreas 1st and 3rd Fridays
Skin 1st and 3rd Wednesdays
Skull Base 1st Wednesday
Stem Cell Transplant* Rotating Wednesdays
Urology 3rd Wednesday
*Rotate during the month
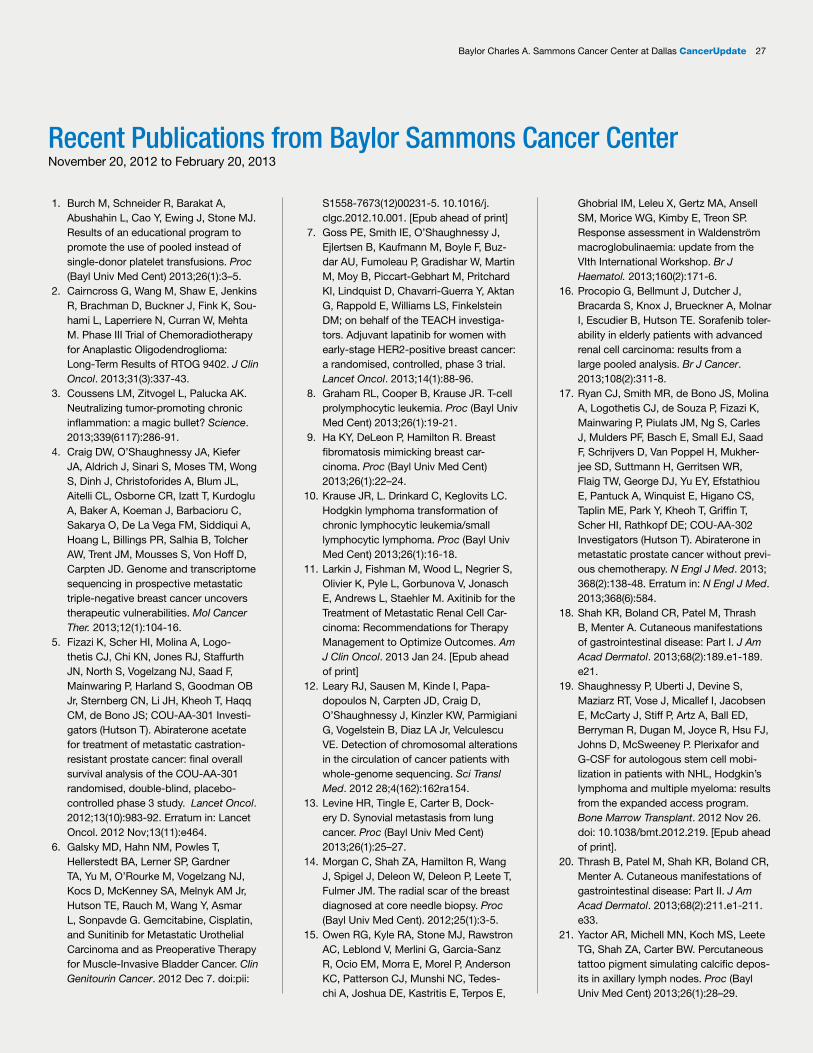
Baylor Charles A. Sammons Cancer Center at Dallas CancerUpdate 27
Recent Publications from Baylor Sammons Cancer CenterNovember 20, 2012 to February 20, 2013
1. Burch M, Schneider R, Barakat A, Abushahin L, Cao Y, Ewing J, Stone MJ. Results of an educational program to promote the use of pooled instead of single-donor platelet transfusions. Proc (Bayl Univ Med Cent) 2013;26(1):3–5.
2. Cairncross G, Wang M, Shaw E, Jenkins R, Brachman D, Buckner J, Fink K, Sou-hami L, Laperriere N, Curran W, Mehta M. Phase III Trial of Chemoradiotherapy for Anaplastic Oligodendroglioma: Long-Term Results of RTOG 9402. J Clin Oncol. 2013;31(3):337-43.
3. Coussens LM, Zitvogel L, Palucka AK. Neutralizing tumor-promoting chronic inflammation: a magic bullet? Science. 2013;339(6117):286-91.
4. Craig DW, O’Shaughnessy JA, Kiefer JA, Aldrich J, Sinari S, Moses TM, Wong S, Dinh J, Christoforides A, Blum JL, Aitelli CL, Osborne CR, Izatt T, Kurdoglu A, Baker A, Koeman J, Barbacioru C, Sakarya O, De La Vega FM, Siddiqui A, Hoang L, Billings PR, Salhia B, Tolcher AW, Trent JM, Mousses S, Von Hoff D, Carpten JD. Genome and transcriptome sequencing in prospective metastatic triple-negative breast cancer uncovers therapeutic vulnerabilities. Mol Cancer Ther. 2013;12(1):104-16.
5. Fizazi K, Scher HI, Molina A, Logo-thetis CJ, Chi KN, Jones RJ, Staffurth JN, North S, Vogelzang NJ, Saad F, Mainwaring P, Harland S, Goodman OB Jr, Sternberg CN, Li JH, Kheoh T, Haqq CM, de Bono JS; COU-AA-301 Investi-gators (Hutson T). Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012;13(10):983-92. Erratum in: Lancet Oncol. 2012 Nov;13(11):e464.
6. Galsky MD, Hahn NM, Powles T, Hellerstedt BA, Lerner SP, Gardner TA, Yu M, O’Rourke M, Vogelzang NJ, Kocs D, McKenney SA, Melnyk AM Jr, Hutson TE, Rauch M, Wang Y, Asmar L, Sonpavde G. Gemcitabine, Cisplatin, and Sunitinib for Metastatic Urothelial Carcinoma and as Preoperative Therapy for Muscle-Invasive Bladder Cancer. Clin Genitourin Cancer. 2012 Dec 7. doi:pii:
S1558-7673(12)00231-5. 10.1016/j.clgc.2012.10.001. [Epub ahead of print]
7. Goss PE, Smith IE, O’Shaughnessy J, Ejlertsen B, Kaufmann M, Boyle F, Buz-dar AU, Fumoleau P, Gradishar W, Martin M, Moy B, Piccart-Gebhart M, Pritchard KI, Lindquist D, Chavarri-Guerra Y, Aktan G, Rappold E, Williams LS, Finkelstein DM; on behalf of the TEACH investiga-tors. Adjuvant lapatinib for women with early-stage HER2-positive breast cancer: a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14(1):88-96.
8. Graham RL, Cooper B, Krause JR. T-cell prolymphocytic leukemia. Proc (Bayl Univ Med Cent) 2013;26(1):19-21.
9. Ha KY, DeLeon P, Hamilton R. Breast fibromatosis mimicking breast car-cinoma. Proc (Bayl Univ Med Cent) 2013;26(1):22–24.
10. Krause JR, L. Drinkard C, Keglovits LC. Hodgkin lymphoma transformation of chronic lymphocytic leukemia/small lymphocytic lymphoma. Proc (Bayl Univ Med Cent) 2013;26(1):16-18.
11. Larkin J, Fishman M, Wood L, Negrier S, Olivier K, Pyle L, Gorbunova V, Jonasch E, Andrews L, Staehler M. Axitinib for the Treatment of Metastatic Renal Cell Car-cinoma: Recommendations for Therapy Management to Optimize Outcomes. Am J Clin Oncol. 2013 Jan 24. [Epub ahead of print]
12. Leary RJ, Sausen M, Kinde I, Papa-dopoulos N, Carpten JD, Craig D, O’Shaughnessy J, Kinzler KW, Parmigiani G, Vogelstein B, Diaz LA Jr, Velculescu VE. Detection of chromosomal alterations in the circulation of cancer patients with whole-genome sequencing. Sci Transl Med. 2012 28;4(162):162ra154.
13. Levine HR, Tingle E, Carter B, Dock-ery D. Synovial metastasis from lung cancer. Proc (Bayl Univ Med Cent) 2013;26(1):25–27.
14. Morgan C, Shah ZA, Hamilton R, Wang J, Spigel J, Deleon W, Deleon P, Leete T, Fulmer JM. The radial scar of the breast diagnosed at core needle biopsy. Proc (Bayl Univ Med Cent). 2012;25(1):3-5.
15. Owen RG, Kyle RA, Stone MJ, Rawstron AC, Leblond V, Merlini G, Garcia-Sanz R, Ocio EM, Morra E, Morel P, Anderson KC, Patterson CJ, Munshi NC, Tedes-chi A, Joshua DE, Kastritis E, Terpos E,
Ghobrial IM, Leleu X, Gertz MA, Ansell SM, Morice WG, Kimby E, Treon SP. Response assessment in Waldenström macroglobulinaemia: update from the VIth International Workshop. Br J Haematol. 2013;160(2):171-6.
16. Procopio G, Bellmunt J, Dutcher J, Bracarda S, Knox J, Brueckner A, Molnar I, Escudier B, Hutson TE. Sorafenib toler-ability in elderly patients with advanced renal cell carcinoma: results from a large pooled analysis. Br J Cancer. 2013;108(2):311-8.
17. Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, Fizazi K, Mainwaring P, Piulats JM, Ng S, Carles J, Mulders PF, Basch E, Small EJ, Saad F, Schrijvers D, Van Poppel H, Mukher-jee SD, Suttmann H, Gerritsen WR, Flaig TW, George DJ, Yu EY, Efstathiou E, Pantuck A, Winquist E, Higano CS, Taplin ME, Park Y, Kheoh T, Griffin T, Scher HI, Rathkopf DE; COU-AA-302 Investigators (Hutson T). Abiraterone in metastatic prostate cancer without previ-ous chemotherapy. N Engl J Med. 2013; 368(2):138-48. Erratum in: N Engl J Med. 2013;368(6):584.
18. Shah KR, Boland CR, Patel M, Thrash B, Menter A. Cutaneous manifestations of gastrointestinal disease: Part I. J Am Acad Dermatol. 2013;68(2):189.e1-189.e21.
19. Shaughnessy P, Uberti J, Devine S, Maziarz RT, Vose J, Micallef I, Jacobsen E, McCarty J, Stiff P, Artz A, Ball ED, Berryman R, Dugan M, Joyce R, Hsu FJ, Johns D, McSweeney P. Plerixafor and G-CSF for autologous stem cell mobi-lization in patients with NHL, Hodgkin’s lymphoma and multiple myeloma: results from the expanded access program. Bone Marrow Transplant. 2012 Nov 26. doi: 10.1038/bmt.2012.219. [Epub ahead of print].
20. Thrash B, Patel M, Shah KR, Boland CR, Menter A. Cutaneous manifestations of gastrointestinal disease: Part II. J Am Acad Dermatol. 2013;68(2):211.e1-211.e33.
21. Yactor AR, Michell MN, Koch MS, Leete TG, Shah ZA, Carter BW. Percutaneous tattoo pigment simulating calcific depos-its in axillary lymph nodes. Proc (Bayl Univ Med Cent) 2013;26(1):28–29.

PRESORTED FIRST CLASS
US POSTAGE PAID DALLAS, TX
PERMIT #777
Multiple MyelomaResearch Consortium
Powerful Collaboration Accelerates Results
8:00 am1/2 mile, 1 mile, 2 mileThe Harbor at Lake Ray Hubbard
JUNE 8, 2013swimacrossamerica.org/dallas
Open Water Swim to Fight Cancer
3410 Worth StreetSuite 550Dallas, Texas 75246214.820.3535BaylorHealth.edu/Sammons