health dimensions group national summit - event management … · health dimensions group national...
TRANSCRIPT

1
Health Dimensions Group National Summit Accountable Care Organizations:
It’s More Than Acute Care
Catholic Health Initiatives A National System’s Approach to Building Accountable
Care Capability
Presented by: John DiCola
Senior Vice President, Strategy & Business Development
2
Catholic Health Initiatives: Overview • Profile: 73 hospitals; 40 long-term care, assisted living, and
residential facilities; two community-based health ministries; located across 19 states, including rural and urban communities
• More than 70,000 full- and part-time employees • More than 1,850 physicians and extenders • $13.9 billion in assets; • $9.6 billion in total operating revenues • Acute inpatient days: 1,763,378 • Acute inpatient revenues as a percentage of total: 47.6% • Long-term care days: 434,210 • Residential days: 682,470 • Home based visits: 701,439

3
MBO
JOA/JV
Top 15 MBOs/JOAs represent 95% of CHI’s NPSR in FY11 (JOA/JV revenues reflect only CHI portion)

4
CHI Strategic Plan: Priorities, Expectations and Resource Allocation in “The New Normal”
Maximize Clinical Operations “Highly effective delivery systems” (2010-2013)
Assume Performance Risk “Integrated health care delivery systems” (2012-2015)
Manage Population Health “Clinical and financial risk” (2014 +)
Move to integrated care capability and capitated models Establish insurance risk capability Manage and measure population health
Maximize performance to manage to Medicare rates Capitalize on payment incentives Relentless pursuit of value • Clinical excellence • Cost of care • Eliminate “waste” • Safety Reduce variation in performance across CHI Balance the portfolio through selective MBO and system growth
Develop interim models for risk assumption for defined payers, complex procedures, and disease states Manage episodes and systems of care across defined settings Translate current financial models to greater risk assumption capability Build physician alignment models to support integrated care delivery

5
• Market scale - Delivery system scale/access foundational to new, integrated care and financing models.
• Physician scale, organization, and alignment – Employed and “highly aligned” physician networks drive value-based care models.
• Post-Acute capability and scale – New financing models and improved care coordination requires lower acuity, lower cost settings via P/A network development.
• Information technology , decision support, and virtual technologies – Coordinated care requires advanced data and analytics on health status and health care utilization; virtual care platforms to extend access, enable care in less costly settings.
• “Reinvention” of core services and new businesses – New business requirements drive reorganization/redesign of old core services and development of new capabilities to support coordinated models of care.
• Higher quality, less costly, delivery models – Key challenge: staging market shift from volume-based to value-based delivery and financing models.
6
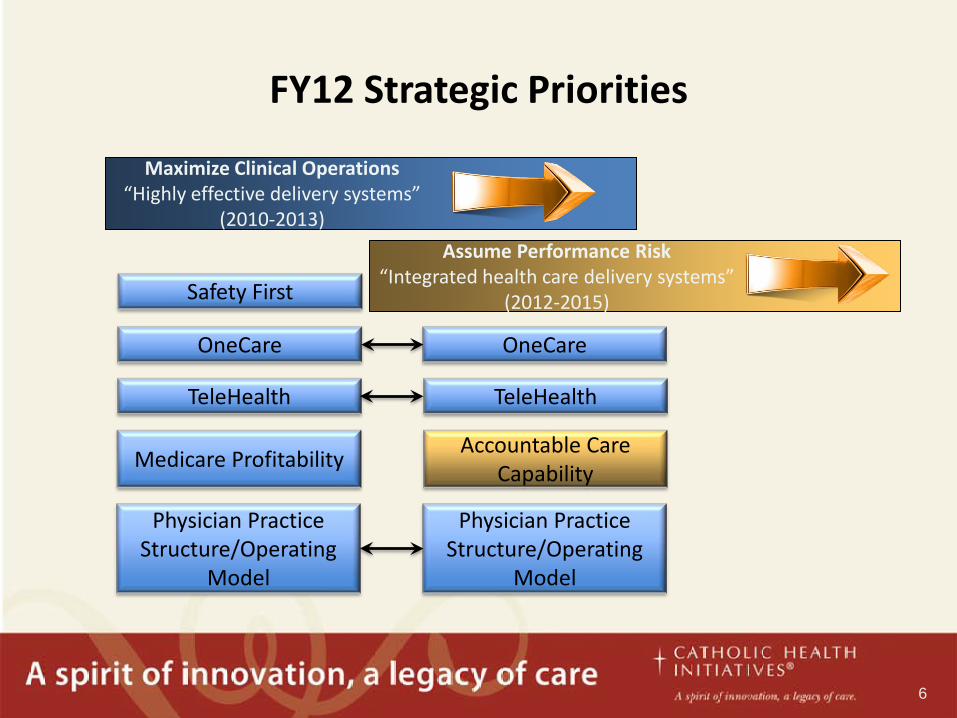
FY12 Strategic Priorities
OneCare OneCare
TeleHealth TeleHealth
Medicare Profitability Accountable Care
Capability
Physician Practice Structure/Operating
Model
Physician Practice Structure/Operating
Model
Safety First
Maximize Clinical Operations “Highly effective delivery systems”
(2010-2013)
Assume Performance Risk “Integrated health care delivery systems”
(2012-2015)

7
Risk Models
• Modeling tools to evaluate market populations for risk arrangements • Local market strategy for pace of payment shift, and risk product opportunities • Standardized, flexible processes for risk product development with selected
payers and major employers • Infrastructure to support risk models, including potential partners offering
required capabilities
• Seamless integration of care processes across delivery sites • High-functioning practice teams operating with clear protocols, using disease
registries and structured patient involvement • Effective (piloted) care management programs (eg. CTI, health coaches)
Care Management
• Contractually and clinically aligned physician enterprise • Distributed network of ambulatory assets through ownership or partnership • High performing, credentialed post acute network • Service line structures designed to provide high-value outcomes, and access
across the care continuum
Care Delivery System
Health Data Management
• Access to actionable data to drive improvements in quality and reductions in cost across delivery settings
• Point of care disease registry and other decision support capabilities • Data and analytic capabilities for management of population health
Building Accountable Care Capability

8
Current Scope of Activities CARE DELIVERY Ambulatory Development Physician Enterprise Development Post Acute Network Development CARE MANAGEMENT Accountable Care Pilots to Build Care Coordination Competencies Care Management Leader and Resources (inc. Third Parties) Care Transition Intervention model RISK MODELS CMMI Bundled Payment Initiative Commercial Payer Bundles Employee Health and Benefit Utilization and Management Investigate Opportunities in Insurance Arena (e.g., TPA, Health Plan) Roadmaps Navigating Economic Shift from Volume/FFS to Value HEALTH DATA MANAGEMENT Ambulatory Point of Care Population Mgt./Disease Registry Population Health Data Analysis and Infrastructure

9
Post Acute Care Network Development
• Post Acute Care Framework
– Assess post acute care capacity and capabilities with the intent to develop a preferred post acute care network of providers. Create a credentialing process with clear expectations around quality, cost and satisfaction.
– Include LTACH, SNF, Acute Rehabilitation, Home Health and Hospice (integrate CHI national home care program).
– Entity specific network options include ownership, management and contracting.
– Develop infrastructure options to connect all entities across the continuum.

10
Post Acute Care Network Development • Assessment Process
– Evaluate current and future post acute care needs– focus on Medicare, top DRGs, measuring utilization against norms and identify improvement opportunities.
– Inventory and assess capacity and capabilities of post acute care providers:
• Beds, census, discharge status, LOS
• 7 day and 30 day readmissions
• Functional Independence Measures (FIM) scores
• Patient and Family Satisfaction
• ED visit rates
• Infection rates
– Interviews – primary care, specialists, hospitalists.

11
Post Acute Network Development
• Implementation Process
– Create local PAC teams, inclusive of physicians, case management, nursing, post acute provider leaders to develop strategy and vision.
– Strategy to address network formation and structure, including post acute providers aligned through ownership, management, joint venture, and/or affiliation
– Strategy to identify key processes for clinical integration, network organization and management, metrics and reporting. Metrics to include financial, quality and outcome measures.

12
Post Acute Care Network Development • Additional Considerations
– Evaluate relationships outside of Medicare post acute care provider definition for further opportunities to coordinate care. (Examples include adult day care, Council on Aging, senior centers and assisted living.)
– Leverage Home Health and Telehealth capabilities and opportunities:
• Eg. Centura Health At Home – Initiated Program 7 years ago, started with 15 patients, now a census of 100, CHF/cardiac related disease:
– Low risk - monitored by telephone and self monitoring
– Moderate risk – 24/7 telemonitoring, phone calls for early intervention
– High risk – additionally have interactive video and home visits