head injury management edited
TRANSCRIPT

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 1/49
Head injury managementHead injury management
Adapted from source Adapted from source
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 2/49
Traumatic Brain InjuryTraumatic Brain Injury
22,00022,000--25,000/yr pts Australian25,000/yr pts Australian
± ± 1,493 moderately TBI1,493 moderately TBI
± ± 1,000 severe cases of T
BI1,000 severe cases of T
BI ± ±
Qld incidence 200/100,000Qld incidence 200/100,000
National 140/100,000National 140/100,000
1/3 trauma deaths1/3 trauma deaths

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 3/49
Traumatic Brain InjuryTraumatic Brain Injury

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 4/49

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 5/49

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 6/49
Assessment History Assessment History
HistoryHistory Time & Mechanism InjuryTime & Mechanism Injury
Neuro statusNeuro status ± ± at scene (at scene (GCS Score and pupils)GCS Score and pupils)
± ± inin transporttransport ± ± After resuscitation After resuscitation
Vital signsVital signs Hypoxia and hypotensionHypoxia and hypotension
Time of intubation presence of apnoeaTime of intubation presence of apnoea
Associated injuries Associated injuries
Age Age
Alcohol / drugs/s intake Alcohol / drugs/s intakeBrain CTBrain CT

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 7/49
Traumatic Brain InjuryTraumatic Brain Injury
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 8/49
Traumatic Brain InjuryTraumatic Brain Injury
1515--1313 MildMild
99 ± ± 12 Moderate12 Moderate
<9<9 SevereSevere

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 9/49
Traumatic Brain InjuryTraumatic Brain Injury--GCSGCS
Eye openingEye opening ± ± SpontaneousSpontaneous 44
± ± To speechTo speech 33
± ± To painTo pain 22
± ± NONENONE 11
Verbal ResponseVerbal Response ± ± OrientatedOrientated 55
± ± Confused conversationConfused conversation 44
± ± Inappropriate wordsInappropriate words 33 ± ± IncomprehensibleIncomprehensible
soundssounds 22
± ± NoneNone 11
Best Motor Best Motor ResponseResponse ± ± ObeysObeys 66
± ± LocalisesLocalises 55
± ± WithdrawsWithdraws 44 ± ± Abnormal flexionAbnormal flexion 33
± ± Extensor responseExtensor response 22
± ± NoneNone 11
± ± After After ResuscitationResuscitation

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 10/49
Traumatic Brain InjuryTraumatic Brain Injury--GCSGCS
OutcomeOutcome
GCS 8GCS 8--15 = 0.3% mortality15 = 0.3% mortality
GCS 6GCS 6--77 = 24% mortality= 24% mortality
GCS 4GCS 4--55 = 49% mortality= 49% mortality
GCS 3GCS 3 = 83% mortality= 83% mortality
Klauber Klauber et al et al 1134 patients1134 patients

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 11/49
Pathophysiology TBIPathophysiology TBI
Primary insultPrimary insult
± ± Primary injuryPrimary injury ± ± Secondary injurySecondary injury
Secondary insultSecondary insult
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 12/49
Primary insultPrimary insult
Primary insultPrimary insult
± ± Primary injuryPrimary injury
± ± Direct damageDirect damage
involves mechanicalinvolves mechanical
forcesforces
Brain : contact energyBrain : contact energy
transfer and inertiatransfer and inertiaenergy transfer energy transfer
Vasculature: vesselVasculature: vessel
shear and disruptionshear and disruption

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 13/49
Secondary Brain injurySecondary Brain injury
Ischaemia (CBF)Ischaemia (CBF)
ExcitotoxicityExcitotoxicity
(CMRO2)(CMRO2)
Neuronal deathNeuronal death
cascades.cascades.
CerebralCerebral oedemaoedema
(vasogenic,(vasogenic,
cytotoxic).cytotoxic).
Inflammation.Inflammation.

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 14/49
Secondary insultsSecondary insults
Independently of the primary impactIndependently of the primary impact
Secondary insultsSecondary insults
Discrete processes, often iatrogenicDiscrete processes, often iatrogenic

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 15/49
Secondary injurySecondary injury

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 16/49
Traumatic brain injury managementTraumatic brain injury management
Primary injuryPrimary injury ± ± PreventionPrevention
Secondary injurySecondary injury ± ± attenuate secondary injury mechanismsattenuate secondary injury mechanisms
± ± manage raised ICPmanage raised ICP
Secondary insultSecondary insult ± ± Prevent and treat secondary insultsPrevent and treat secondary insults
± ± ABCD ABCD

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 17/49
Management Principles Secondary TBIManagement Principles Secondary TBI
Prevent further cerebral insultsPrevent further cerebral insultsHypoxiaHypoxia
HypotensionHypotension
HyperglycaemiaHyperglycaemiaDefend cerebral perfusionDefend cerebral perfusion
Limit intracranial pressure riseLimit intracranial pressure riseCerebral oedemaCerebral oedema
Cerebral blood volumeCerebral blood volumeCSF volumeCSF volume
Limit cerebral metabolic demandLimit cerebral metabolic demand

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 18/49
HypoxiaHypoxia ± ±Traumatic Brain InjuryTraumatic Brain Injury
Apnoea accompanies most head injuries. Apnoea accompanies most head injuries.
± ± Airway obstruction and aspiration major Airway obstruction and aspiration major
causes of death treatable head injuriescauses of death treatable head injuries
Hypoxia is commonHypoxia is common ± ± PaO2 60 mm Hg 46% admissions to the emergency departmentPaO2 60 mm Hg 46% admissions to the emergency department

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 19/49
Cerebral metabolic rate for oxygenCerebral metabolic rate for oxygen
(CMRO2)(CMRO2)
CMRO2CMRO2
± ± 3.5 ml/100g/min3.5 ml/100g/min
± ± 50 ml/min (20% of 50 ml/min (20% of
total basaltotal basalrequirements).requirements).
PaO2 minimal effectPaO2 minimal effect
on CBF until 50on CBF until 50mmHgmmHg

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 20/49
HypoxiaHypoxia ± ±Traumatic Brain InjuryTraumatic Brain Injury
Associated Associated
± ± 50% mortality rate50% mortality rate
± ± 50% severe disability50% severe disability
among survivorsamong survivors
Worse outcomes for Worse outcomes for
patients with TBI whopatients with TBI who
were intubated in thewere intubated in the
fieldfield
Why ?Why ?
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 21/49
IntubationIntubation ± ±TBITBI
Risk ICP, aspiration, and hypoxia.Risk ICP, aspiration, and hypoxia.
IPPV increases intra thoracic pressure,IPPV increases intra thoracic pressure, ± ± decrease venous return impair CPP.decrease venous return impair CPP.
Sedative agents can cause hypotensionSedative agents can cause hypotension
Risk of hyperventilationRisk of hyperventilation

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 22/49
Brain Trauma FoundationBrain Trauma Foundation
Prehospital guidelines recommendPrehospital guidelines recommend
intubationintubation
GCS scores 8GCS scores 8
Inadequate airwayInadequate airway
SaO2 < 90% with supplemental O2SaO2 < 90% with supplemental O2
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 23/49
PaCO2 TBIPaCO2 TBI
PaCO2 levels emergency departmentPaCO2 levels emergency department
± ± 17%, PCO2 < 3017%, PCO2 < 30
± ± 47%, PCO2 3047%, PCO2 30± ±3939
± ± 26%, PCO2 > 4026%, PCO2 > 40
Target PaCO2 range of 30Target PaCO2 range of 30± ±3939
± ± mortality 21%mortality 21%PaCO2 < 30 or >39PaCO2 < 30 or >39
± ± mortality 34%mortality 34%

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 24/49
PaCO2 CBFPaCO2 CBF
CO2 potent cerebralCO2 potent cerebralvasodilator vasodilator
1 mm Hg drop in1 mm Hg drop inPCO2 3% decreasePCO2 3% decreasein CBFin CBF
Hyperventilation canHyperventilation canlead to cerebrallead to cerebralischemiaischemia
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 25/49
Hypotension TBIHypotension TBI
Hypotension is common.Hypotension is common.
± ± 88± ±13% severe head injury pt.13% severe head injury pt.
Single episode of hypotension (SBP< 90Single episode of hypotension (SBP< 90
mm Hg) X2 mortality ratemm Hg) X2 mortality rate

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 26/49
Hypotension TBIHypotension TBI
HypotensionHypotension diff in adults to childrendiff in adults to children
Other injuryOther injurySpinal cord injurySpinal cord injury
Cardiac contusion/tamponadeCardiac contusion/tamponade
Tension pneumothoraxTension pneumothorax
Children may be hypotensive due to blood lossesChildren may be hypotensive due to blood lossesof head injuryof head injury

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 27/49
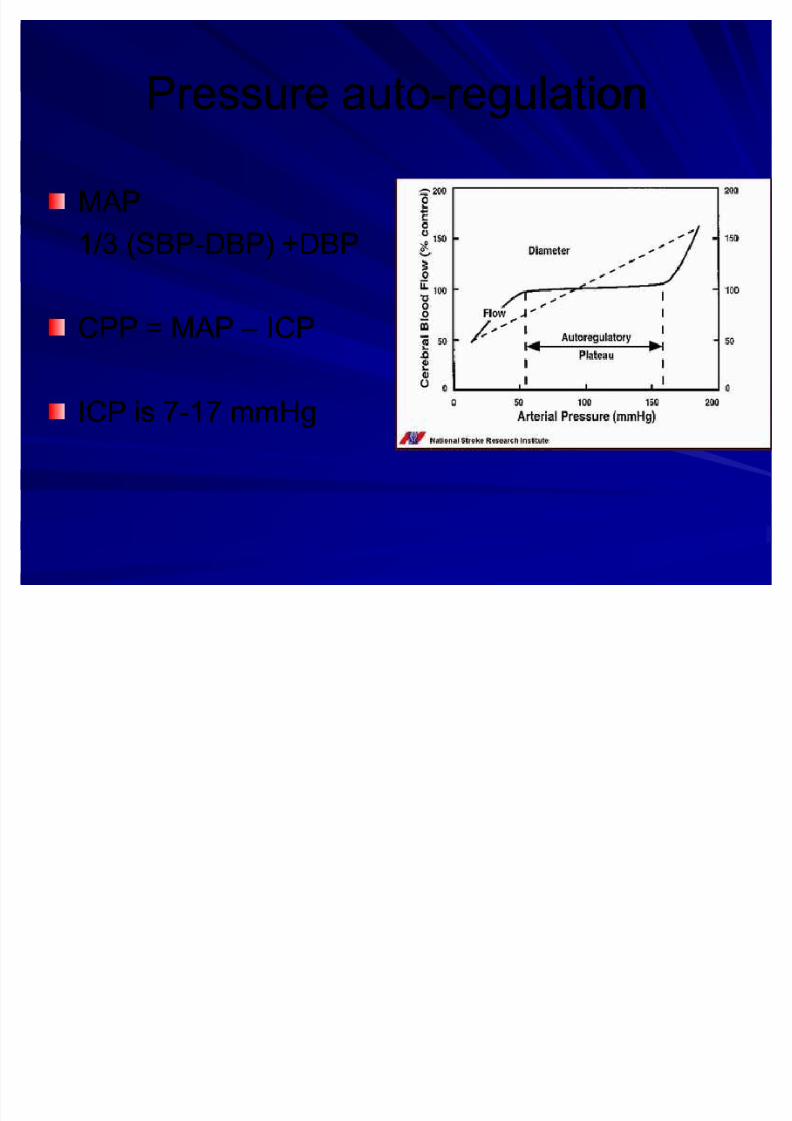
Pressure autoregulationPressure autoregulation
In normal brain CBFIn normal brain CBF
constant between MAP 50constant between MAP 50
mmHg and 150 mmHgmmHg and 150 mmHg
Nml CBFNml CBF
± ± 50ml/100g/min50ml/100g/min
± ± 700 ml/min700 ml/min
± ± 14 % of the cardiac output.14 % of the cardiac output.
Severe TBI CBF is bloodSevere TBI CBF is blood
pressure dependent.pressure dependent.

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 28/49
CBF TBICBF TBI
Severe TBI CBF is blood pressure dependent.Severe TBI CBF is blood pressure dependent.
Cerebral perfusion pressure (CPP)Cerebral perfusion pressure (CPP)
± ± CPP = MAP CPP = MAP ± ± ICPICP (or CVP, whichever is the highest)(or CVP, whichever is the highest)
Increase in mortality and poor outcome whenIncrease in mortality and poor outcome whenCPP < 70 mmHg for a sustained period.CPP < 70 mmHg for a sustained period.
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 29/49
Pressure autoPressure auto--regulationregulation
MAP MAP
1/3 (SBP1/3 (SBP--DBP) +DBPDBP) +DBP
CPP = MAP CPP = MAP ± ± ICPICP
ICP is 7ICP is 7--17 mmHg17 mmHg
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 30/49
Defend cerebral perfusionDefend cerebral perfusion
MABPMABP 90 mmHg90 mmHgCPP = MABP CPP = MABP ± ± (ICP or JVP)(ICP or JVP)
Avoid raised JVP or CVP Avoid raised JVP or CVP
± ± Blood volumeBlood volume
± ± JVP obstructionJVP obstruction
± ± Raised intrathoracic pressureRaised intrathoracic pressure
± ± Excessive PEEPExcessive PEEP
Inotropes NAdr or Adr Inotropes NAdr or Adr
PositionPosition
± ± Nurse head up 20Nurse head up 20--3030°°(if spine cleared)(if spine cleared)
± ± CC--spine collar spine collar
Avoid excessive ventilatory pressures Avoid excessive ventilatory pressures

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 31/49
PressurePressure--Volume CurveVolume Curve
Compensation
Point of n Decompensation
Herniation
Volume of Mass
ICP
(mm Hg)
5-
10-
15-
20-25-
30-35-
40-
45-50-
55-
60-

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 32/49

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 33/49
0 20 40 60 80 100 120
1
2
Intracranial tissue volume
Normal
Head injury
Brain
swelling
qCSF volume
Haematoma

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 34/49
Limit intracranial pressure riseLimit intracranial pressure rise
Cerebral blood volumeCerebral blood volume
Avoid Avoid hypertensionhypertension
± ± CVS responses to pain, stimulationCVS responses to pain, stimulation
± ± Analgesia & sedation associated injuries Analgesia & sedation associated injuriesTransfersTransfers
Procedures IntubationProcedures Intubation
Control PaCO2Control PaCO2 ± ± Ventilation to PaCOVentilation to PaCO22 = 34= 34 -- 36 mmHg36 mmHg

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 35/49
Limit intracranial pressure riseLimit intracranial pressure rise
Cerebral oedemaCerebral oedema
± ± Avoid hypo Na+ Avoid hypo Na+ ± ± Target Na+ >135 mmolTarget Na+ >135 mmol
0.9% saline0.9% saline

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 36/49
Signs of Impending HerniationSigns of Impending Herniation
Deteriorating LOC (GCS score)Deteriorating LOC (GCS score)
Pupillary asymmetry >1mmPupillary asymmetry >1mm
Motor asymmetryMotor asymmetry
Extensor (decerebrate) posturing (M2),Extensor (decerebrate) posturing (M2),
Cushing¶s response BP HRCushing¶s response BP HR
Respiratory arrestRespiratory arrest

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 37/49
Urgent measures to lower critical ICPUrgent measures to lower critical ICP
Mannitol AdministrationMannitol Administration
Hypertonic SalineHypertonic Saline

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 38/49
HyperventilationHyperventilation--ICPICP
Hyperventilation TherapyHyperventilation Therapy
PaCO2 < 25 mmHg noPaCO2 < 25 mmHg no
further reduction in CBFfurther reduction in CBF
HypoCO2HypoCO2
± ± shift the oxygenshift the oxygen
dissociation curve to leftdissociation curve to left
± ± oxygen less available tooxygen less available to
the tissues.the tissues.

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 39/49
Herniating patientsHerniating patients ± ± goal of PaCO2 30goal of PaCO2 30± ±35 mm Hg35 mm Hg
EndEnd--tidal PCO2 not reliable measure of PaCO2tidal PCO2 not reliable measure of PaCO2
Without cerebral herniationWithout cerebral herniation ± ± PaCO2 goal of 35PaCO2 goal of 35 -- 40 mm Hg40 mm Hg
± ± Vt 10 ml/kg and 10 bpmVt 10 ml/kg and 10 bpm
± ± Prophylactic hyperventilation worse prognosisProphylactic hyperventilation worse prognosis
HyperventilationHyperventilation--ICPICP
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 40/49
Hypothermia critical ICPHypothermia critical ICP
Admission temp (<35C) is a predictor of death in trauma Admission temp (<35C) is a predictor of death in traumapatientspatients
Hypothermia TBI controversialHypothermia TBI controversial
Induced therapeutic hypothermia vs accidentalInduced therapeutic hypothermia vs accidentalhypothermiahypothermia
66± ±7% decrease CMRO2 / 1C7% decrease CMRO2 / 1C decrease in tempdecrease in temp
RewarmingRewarming

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 41/49
TBI Management MinimiseTBI Management Minimise CMROCMRO22
SedationSedation ± ± no evidence regarding superiority of any particular sedativeno evidence regarding superiority of any particular sedative
use short acting agentsuse short acting agents
?role NMB?role NMB
Control temperatureControl temperature ± ± Brain in TBI temp 2 C degrees > core tempBrain in TBI temp 2 C degrees > core temp
± ± Mild hypothermia 34Mild hypothermia 34--35.5C35.5C
Prevent/treat seizuresPrevent/treat seizures ± ± minimize CMROminimize CMRO22
± ± Phenytoin (loading dose 15mg/kg, infuse 50mg/min)Phenytoin (loading dose 15mg/kg, infuse 50mg/min)

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 42/49
Trauma response TBITrauma response TBI
TBI with onTBI with on--scenescenestabilization in the fieldstabilization in the field ± ± better survival ratesbetter survival rates
± ± longlong--term outcomes incur term outcomes incur
longer medianlonger median
Independent of sceneIndependent of scenetimetime ± ± (113 vs 45 minutes,(113 vs 45 minutes,
respectively; p < 0.001)respectively; p < 0.001)
± ± Compared with other Compared with other traumatrauma

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 43/49
Trauma response TBITrauma response TBI
Neurosurgical expertiseNeurosurgical expertisesingle most importantsingle most importantdeterminant of outcome in ptsdeterminant of outcome in ptswith mass lesionswith mass lesions
Acute subdural hematomas Acute subdural hematomas
mortality ratemortality rate
30% if evacuation < 4hrs30% if evacuation < 4hrs90% if surgical evacuation > 490% if surgical evacuation > 4hrs.hrs.

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 44/49
Trauma response TBITrauma response TBI
Intervention of air Intervention of air medical and rapidmedical and rapid--response teamsresponse teams
Pts with minimalPts with minimalneurological functionsneurological functions(GCS 4)(GCS 4)
Greatest increase inGreatest increase insurvival.survival.

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 45/49
Maintain mean BP > 90 mm Hg
MaintainP
aCO2 approximately 35mm Hg
Use isotonic solution for euvolemia
Frequent neurologic examsReassess ABC if deterioration
Things to Do:

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 46/49
Things to Avoid:
Do Not Allow patient to become
hypotensive Do Not Allow patient to become hypoxic
Do Not hyperventilate
Do Not Use hypotonic IV fluids Do Not Paralyse before performing
complete exam (if possible )

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 47/49
PrognosisPrognosis
Very difficult to accurately predict prognosisVery difficult to accurately predict prognosiswithin the first 24 hrs of TBIwithin the first 24 hrs of TBI
Avoid assessments of medical futility and Avoid assessments of medical futility andpossible organ donationpossible organ donation
Allow the results of resuscitative efforts to be Allow the results of resuscitative efforts to beevaluatedevaluated

8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 48/49
?S?S
8/8/2019 Head Injury Management Edited
http://slidepdf.com/reader/full/head-injury-management-edited 49/49
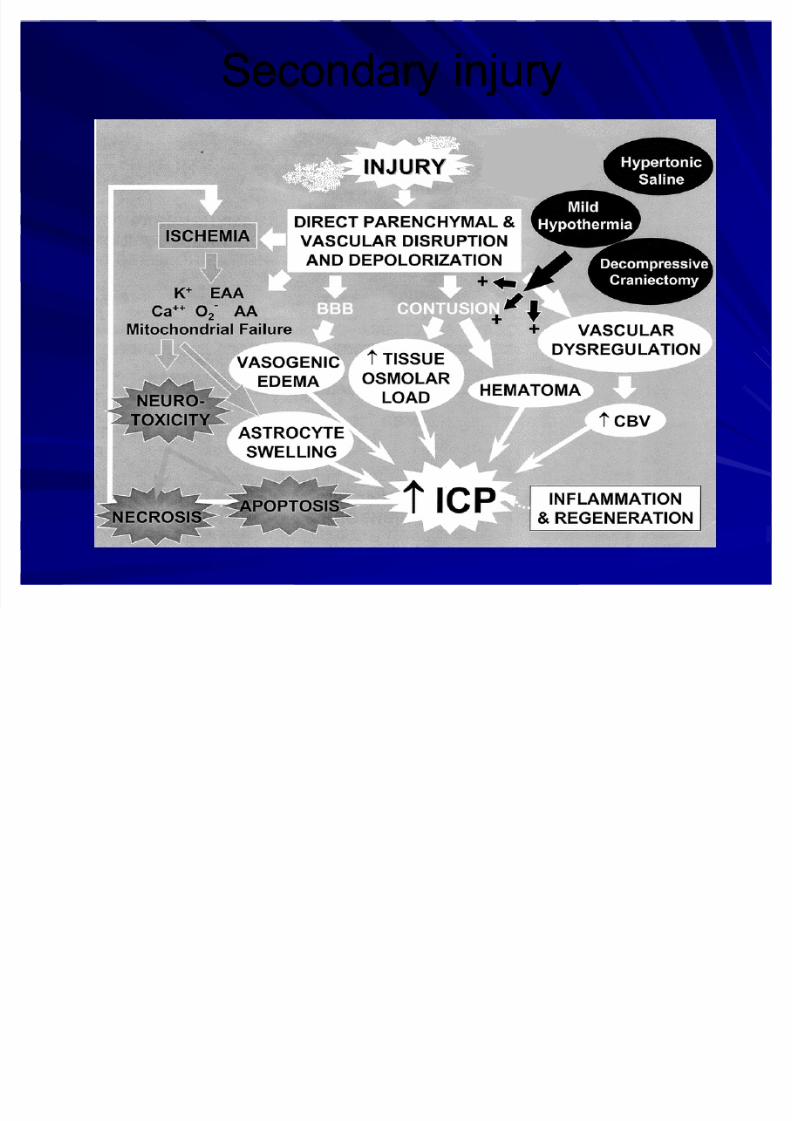
Secondary injurySecondary injury