head injury
TRANSCRIPT
HEAD INJURY.
1
IntroductionEpidemiologyAetiologyClassificationManagementComplicationsTake home points
2
Head injury can be defined as trauma to the brain and/or its coverings from an externally
applied mechanical force.
The terms head injury and traumatic brain injury are used interchangeably in literature.
3
• Head injury data are difficult to compare internationally for multiple reasons, including inconsistencies and complexities of diagnostic coding and inclusion criteria.
• However, it is generally found that trauma is the fourth most common cause of death in Nigeria (CDC-2011)
4
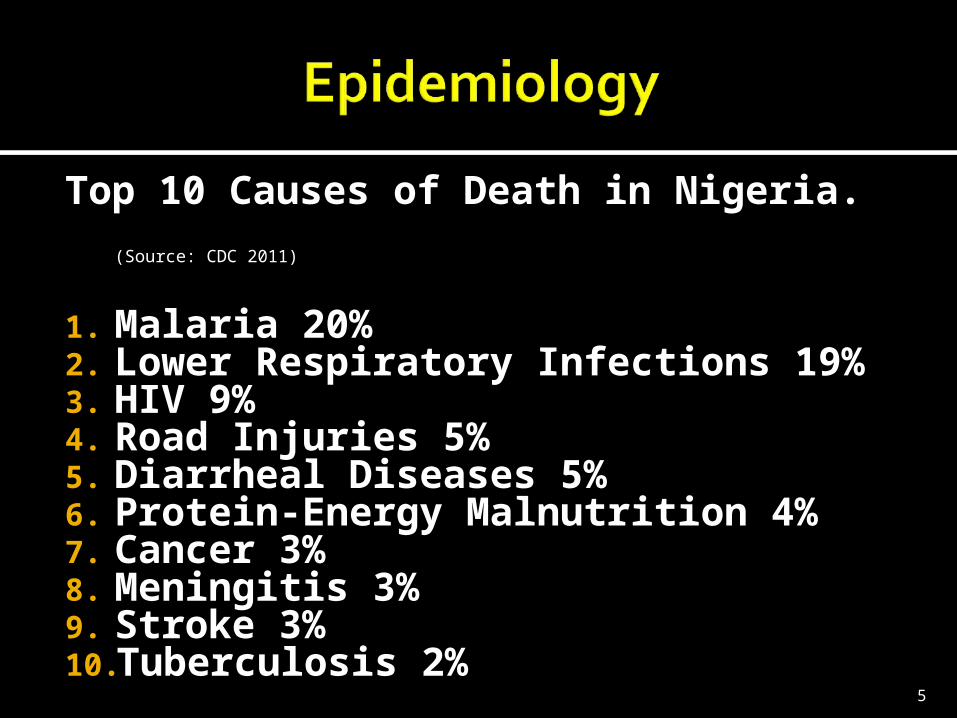
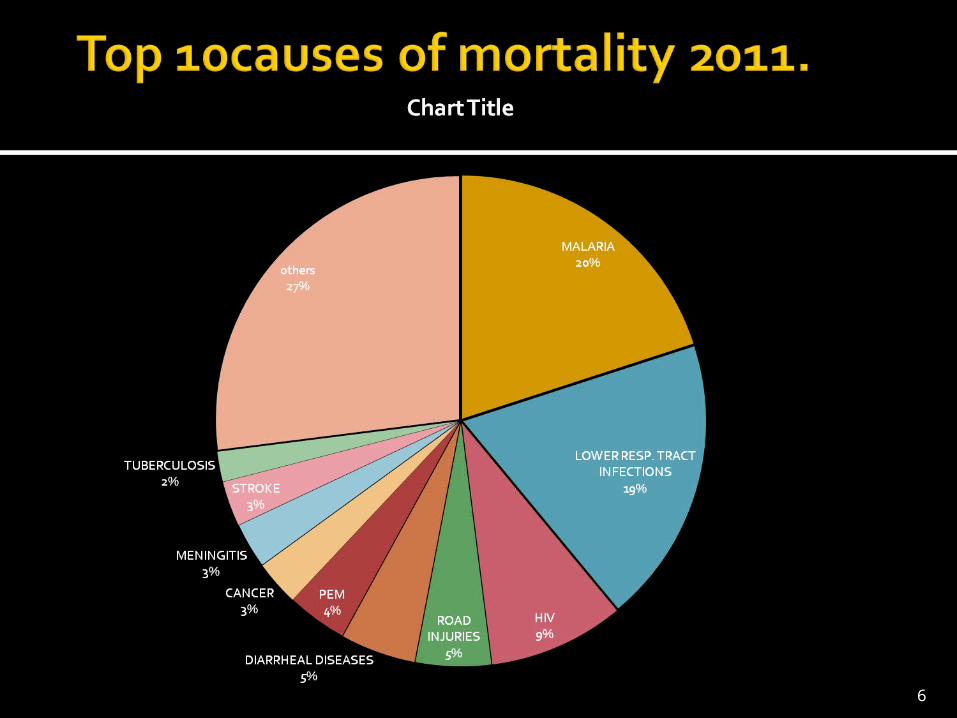
Top 10 Causes of Death in Nigeria. (Source: CDC 2011)
1. Malaria 20%2. Lower Respiratory Infections 19%3. HIV 9%4. Road Injuries 5%5. Diarrheal Diseases 5%6. Protein-Energy Malnutrition 4%7. Cancer 3%8. Meningitis 3%9. Stroke 3%10.Tuberculosis 2%
5
6

• AGE: The Incidence is highest in active males in the third decade of life (i.e. btw ages 21-30)
Approximately half of the patients admitted to a hospital for head injury are aged 24 years or younger.
• SEX: Men are nearly twice as likely to be hospitalized with a brain injury than women.
7

8
Road traffic AccidentsFalls Outside or inside the home,
this is common with those that are above 50 years.
Missile or Gun shot injuries.Assaults or Civilian violenceSport injuries- Foot ball, polo
games, base ball, skating. Industrial accidents-Mishaps
while operating machines.9

• Motor vehicle and motorcycle-related accidents account for almost half of the cases of head injuries, and deserve special mention in this regard.
10
• Anatomical (Scalp, Skull and Brain)• Closed or Open.• Diffuse or Focal.• Coup or contrecoup.• Mild, Moderate or Severe.• Non-haemorrhagic or Haemorrhagic
(extradural,subdural,subarachnoid ,intraparenchymal or intraventricular).
• Concussion,Contusion or Diffuse axonal
• Primary or Secondary 11
SCALP INJURY: Highly vascularised and bleeds
profusely
SKULL INJURY: Fractures to cranium and the
face may be severe enough as to cause injury to the brain.
BRAIN INJURY: Coup and contrecoup 12
13
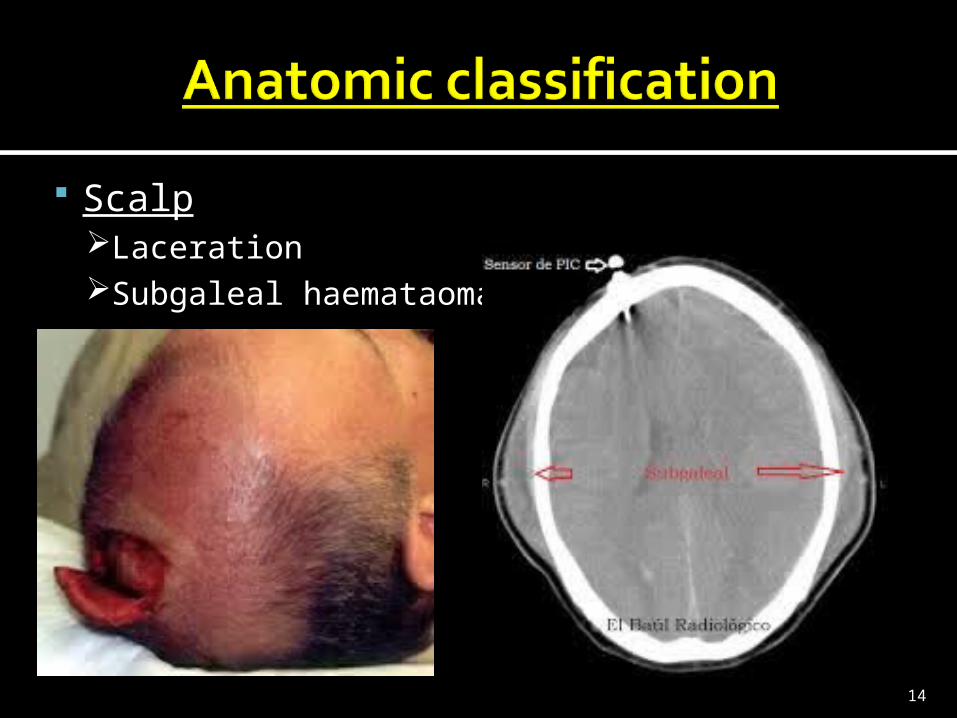
ScalpLacerationSubgaleal haemataoma.
14

SkullFracture:
• Simple or Compound.• Linear or Comminuted.•Depressed.• Base of Skull.
15

16
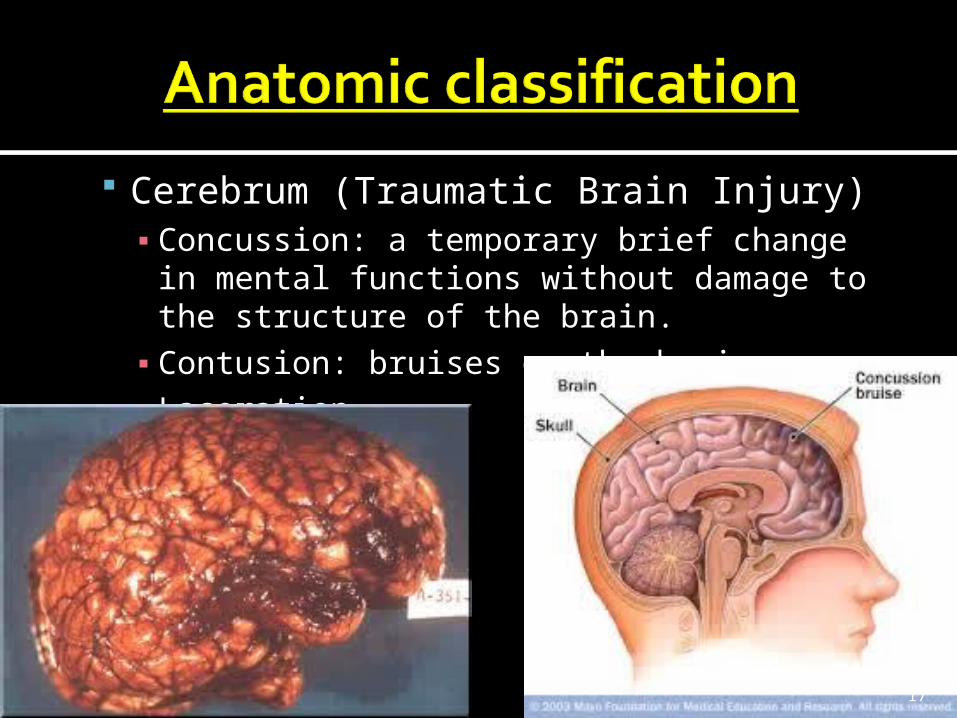
Cerebrum (Traumatic Brain Injury)▪ Concussion: a temporary brief change in
mental functions without damage to the structure of the brain.▪ Contusion: bruises on the brain▪ Laceration
17
The Glasgow Coma Scale
Has a minimum score of 3 and a maximum of 15 Mild head injury------------------- (GCS 13-15)
Moderate head injury-------------(GCS 9-12)
Severe head injury-----------------(GCS 3-8)
The scale was published in 1974 by Graham Teasdale and Bryan J. Jennett, professors of neurosurgery at the University of Glasgow's Institute of Neurological Sciences
18
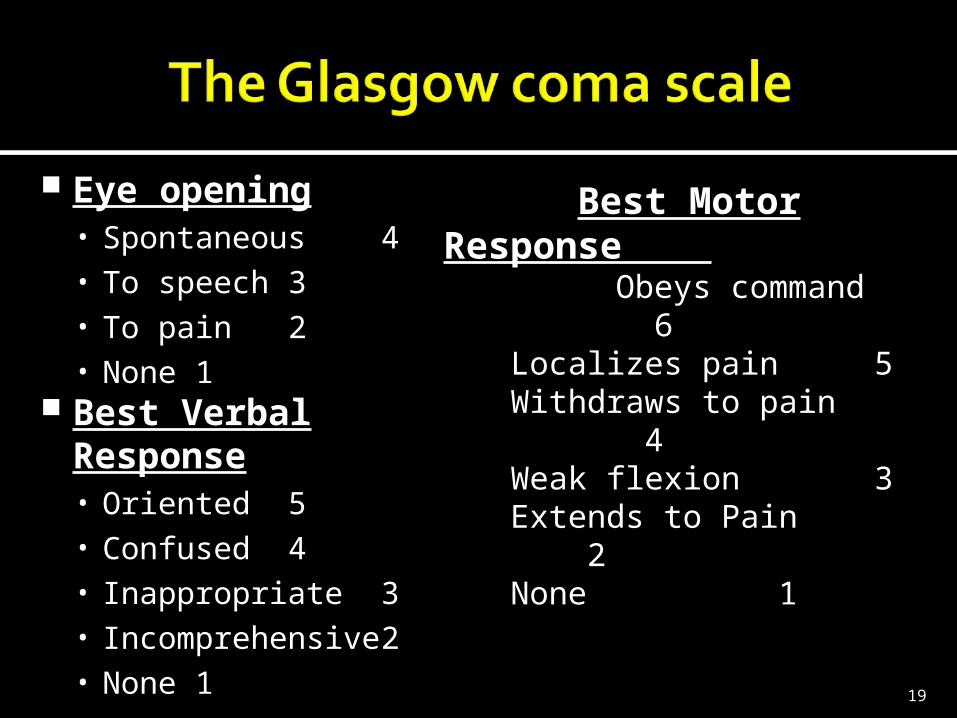
Eye opening• Spontaneous 4• To speech 3• To pain 2• None 1
Best Verbal Response• Oriented 5• Confused 4• Inappropriate 3• Incomprehensive 2• None 1
Best Motor Response • Obeys command 6•Localizes pain 5•Withdraws to pain 4•Weak flexion 3•Extends to Pain 2•None 1
19
Primary TBI- is due to direct impact of trauma to the brain. They include;
Concussion :- a temporary brief change in mental functions without damage to the structure of the brain.
Contusion :- bruises on the brain
Lacerations :- when the tissue of the brain is mechanically cut or torn.
20
These result as a consequence of the complications of the primary injury.
Secondary brain injury results from: Systemic hypotension, Hypoxia, Biochemical changes. Elevated Intracranial Pressure
(pressure effect of intracranial
haematomas or brain swelling),
21
Cranial compartment is rigid and has no room for expansion
Cranium and its constituents (blood, brain tissue and CSF) are at a state of volume equilibrium.
Thus an increase in the volume of one constituent must be accompanied by a decrease in the volume of the other two.
Normal ICP can only be maintained via these compensatory mechanism for volume less than 100-120mls
22
Before arrival at the hospital. On arrival at the hospital.
• Initial clinical evaluation and resuscitation: involves a thorough systemic trauma evaluation and stabilization process referred to as the advanced trauma life support (ATLS) guidelines.
• After patient has been resuscitated and stabilized, patient is then transported to an adequately equipped hospital where attention may then be directed to a focused head injury evaluation.
23
General preventive measures are the only way to avoid initial head injury.
Hence the major concern in managing head injury patients is the early detection of the primary head injury and prevention of secondary brain injuries.
Quick history of the mechanism of injury Proper classification of the injury Find out if it is an isolated head injury
case or if patient has multiple injuries.
24
First responders should immediately institute the ATLS Protocols.
Avoid moving the patient if at all possible
A--------secure and preserving the AIRWAY, B------- maintain and supporting
BREATHINGC------- maintain the CIRCULATIOND------- Assess level of DISABILITYE---------EXPOSURE
25
Airway Remove any Foreign bodies in the
airways▪ Finger sweep
Jaw thrust and chin lift Oropharyngeal airways, LMA Surgical cricothyroidectomy Endotracheal intubation
26
Breathing Check for life threateninig conditions Tension pneumothorax Massive haemothorax Open pneumothorax Cardiac tamponade
Resuscitation with supplemental oxygen
27
Control haemorrhage Manual pressure Haemostats
2 large-caliber iv catheterUse of Crystalloids/Blood
28
Semi rigid/rigid collars, Side head supports and strappingsWhole spine is immobilized in a
neutral position on a firm surface and the patients whole body is transported as in one unit without flexing the spinal column.LOG ROLLING!!!!
29

30
Assessment of the level of consciousness in the AVPU scale Alert Voice----------elicits response Pain-----------elicits response Unresponsive
GCSPupils size, equality and reaction
31
Unclothe patientPrevent hypothermia
Warm blanket Warm iv fluids
32
Promptly transport people with suspected TBI directly to a centre with a trauma team.
Ideally in all cases, stand-by calls should be made to the destination emergency department (ED) for all patients particularly those with GCS<8 and/or polytraumatization.
33
Care of patients with CNS injuries is a multidisciplinary endeavor.
Paramedics, emergency medicine specialists, trauma specialists, neurosurgeons, neurointensivists,
neuroradiologists, and an array of highly specialized nursing and technical staff are all integral to succesful management.
34
The trauma team leader Coordinates life support (directs primary &
secondary survey) Assures priorities of diagnosis and defines
order of therapies Makes decisions regarding appropriate
consultations, medications, investigations and the need for surgical intervention
Ensures the trauma documentation is complete.
It is essential that the team leader stands back from the resucitation to coordinate and should NOT be involved in clinical procedures
35
GENERAL PRIORITIES: Maintain Airway Assess integrity of C-spine & immobilise Arrest Haemorrhage in scalp lacerations Assess Glasgow Coma Scale Assess Pupillary size Assess muscle tone, power and reflexes Assess sensation Do relevant X-Rays, CT scan
36
Things a quick history should elicit include:-
Mechanism of injury Loss of consciousness Presence of lucid intervals Altered consciousness Bleeding from lacerations Bleeding from orifices
Rhinorrhea/Otorrhea Seizures Vomiting
37

Inability to remember the cause of the injury or events that occurred Immediately before or up to 24 hours after
Confusion and disorientation Difficulty remembering new information Headache Dizziness Blurry vision Nausea and vomiting Ringing in the ears Trouble speaking coherently Changes in emotions or sleep patterns
38
The Glasgow Coma Scale (GCS) is the mainstay for rapid neurologic assessment in acute head injury. (Recall slides 17 & 18)
Next a quick but thorough general examination which should also include all obvious injuries
39
Examine for signs of external trauma. Bruising or bleeding on the head and scalp and blood in the ear canal or behind the tympanic membranes may be clues to occult brain injuries.
Also consider coexistent cervical spine and other systemic injuries.
40
41
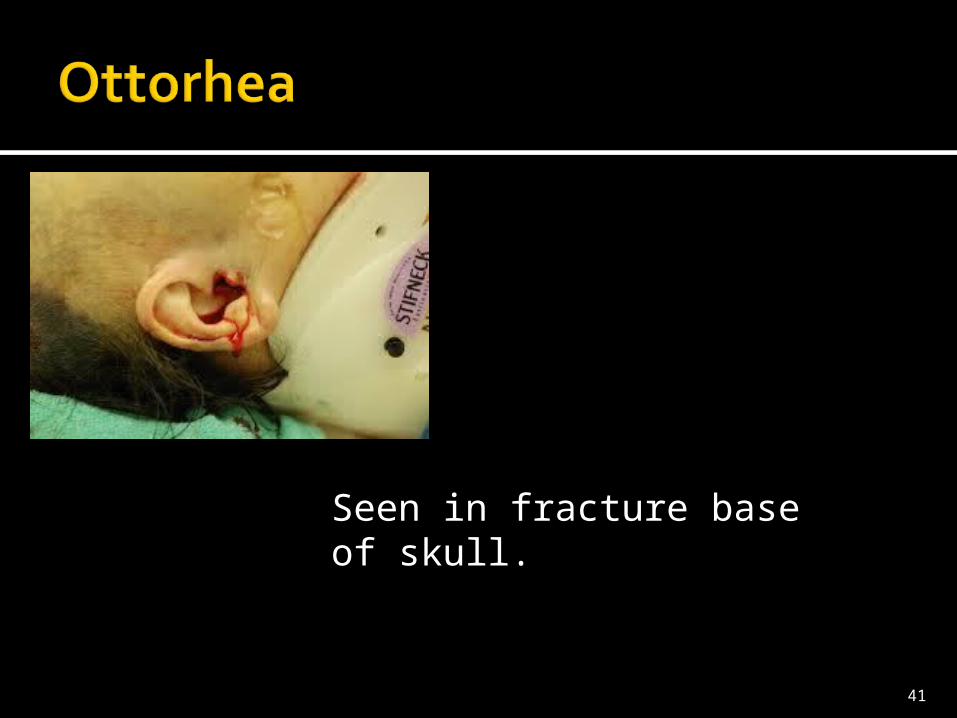
Seen in fracture base of skull.

42
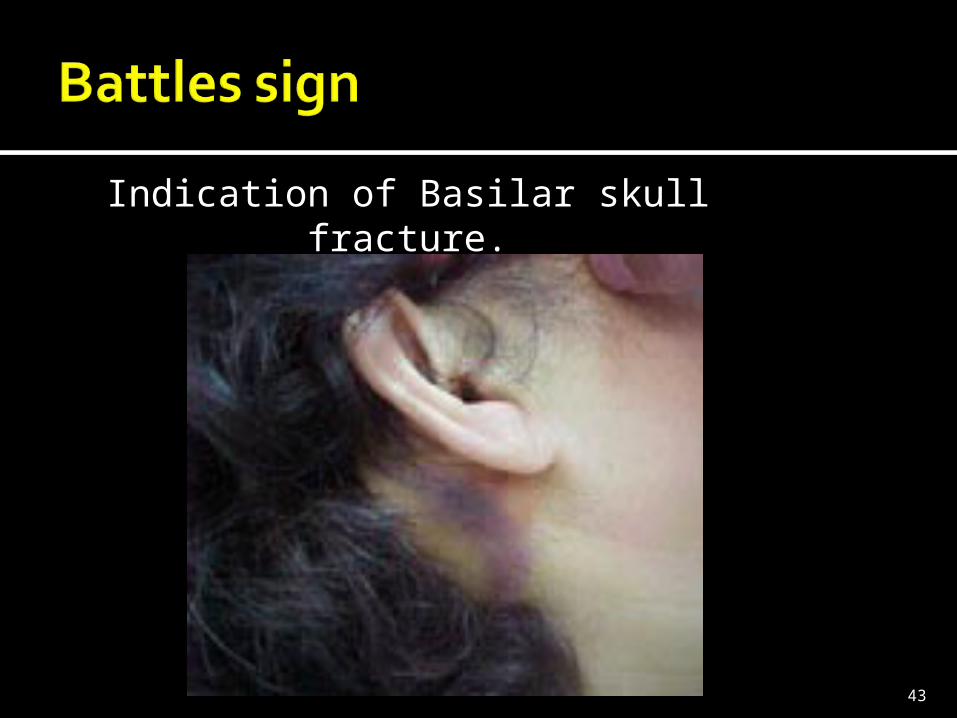
Indication of Basilar skull fracture.
43

44
Anosmia (caused by the shearing of the olfactory (CN I) nerves at the cribriform plate.
Pupillary reactivity +/-Anisocoria▪ A unilaterally dilated pupil with or without
evidence of ipsilateral cranial nerve (CN) III paralysis, such as ptosis or impaired ocular motility, may indicate impending herniation.
CN VI (abducens) palsies may indicate raised intracranial pressure.
CN VII (facial)palsy, particularly in association with decreased hearing, may indicate a fracture of the temporal bone. 45

Focal motor findings may be manifestations of a localized contusion or, more ominously, an early herniation syndrome. Flexor or extensor posturing ▪ extensive intracranial pathology or▪ raised intracranial pressure. In the chronic
phase, Spasticity, akinesia rigidity, tremors and
dystonia may also be present.46
Aphasia no ability to retain new information.
▪ Anterograde amnesia
47
Laboratory Studies PCV/FBC E/U/Cr Arterial blood Gases Alcohol level Drug screens O2 Spirometry
Imaging Studies Skull and cervical spineXrays: CT scanning. Skull and c- spine
48
• Computerized Tomography Scanning:
• The standard CT scan for the evaluation of acute head injury is a non contrast scan that spans from the base of the occiput to the top of the vertex in 5-mm increments.
49
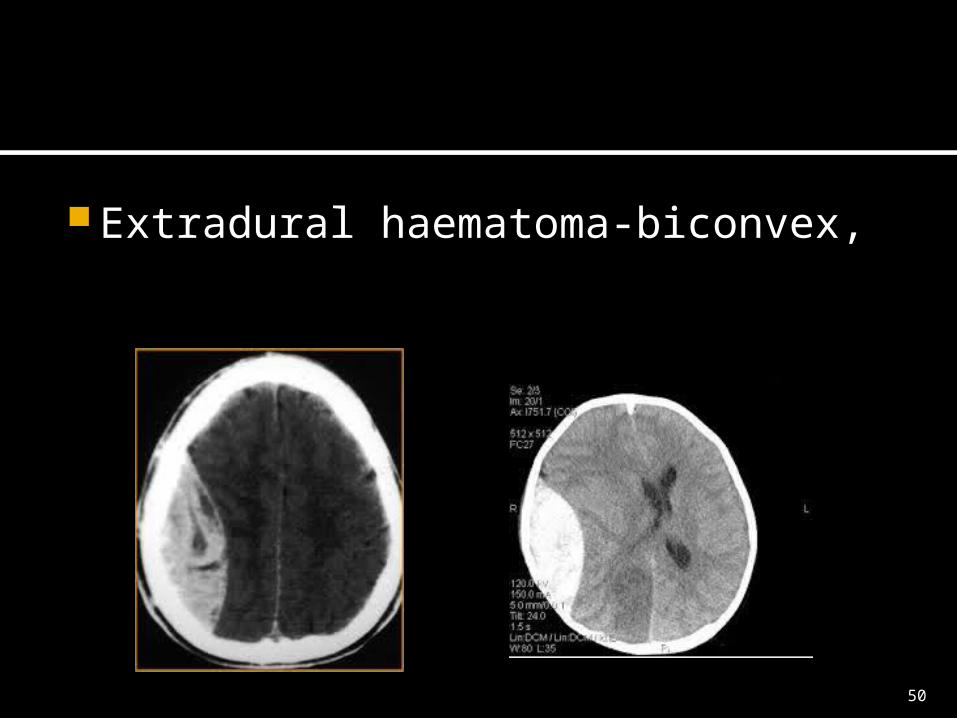
Extradural haematoma-biconvex,
50
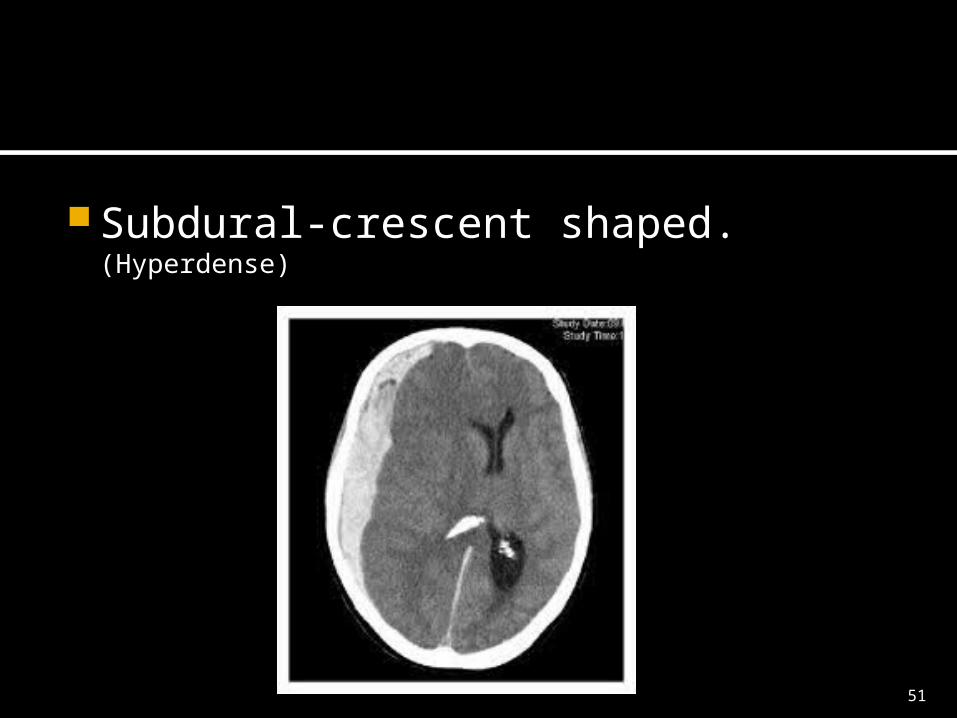
Subdural-crescent shaped. (Hyperdense)
51

Subarachnoid-filling of gyri over convex brain surfaces. (hyperintense lesion)
52
Wide bore intravenous accessNeed to Catheterise patientsOxygen therapy
53
Mild head injuries :analgesics and close monitoring for potential complications such as intracranial bleeding.
Moderate and Severe head injuries:There is significant secondary injury : Prevention of hypoxia: Oxygen therapy Maintenance of perfusion: Ringer’s lactate
Normal saline, blood transfusions when indicated.
Control of elevated intracranial pressure. Mannitol, hyperventilation
54
Monitoring of blood pressure: vassopressors
Seizures: anticonvulsants Agitation:Paralytics,sedation. Nutrition:Enteral or parenteral
feeding. Correction of dyselectrolytaemia:
Hyponatramia, Hypomagnesaesemia.
55
InsomniaCognitive declinePosttraumatic headachePosttraumatic depressionPosttraumatic seizuresHydrocephalusDeep vein thrombosis
56

Posttraumatic seizuresHydrocephalusSpasticityGastrointestinal complications:
Cushing’s ulcers.Gait abnormalities
57
A putative diagnosis of mild head injury does not necessarily mean a favourable outcome.
80% of patients with mild head injury recover completely.
Patients could develop Alzheimer’s disease subsequently.
Adequate follow up is essential.
58

Head injured patients need not die at the site of accident
Head injured patients should be carefully assessed in order to categorise them. The more severely injured should be stabilised and referred as soon as possible.
Multidisciplinary approach is key in the management of the head injured patient.
Improved medical facilities coupled with skilled first contact physician and appropriate public awareness will improve prognosis.
59

60
THANK YOU.
61
Orledge JD, Pepe PE. Out-of-hospital spinal immobilization: is it really necessary?. Acad Emerg Med. 1998 Mar. 5(3):203-4. [Medline].
Hadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, et al. Guidelines for the management of acute cervical spine and spinal cord injuries. Clin Neurosurg. 2002. 49:407-98. [Medline].
Lockey D, Davies G, Coats T. Survival of trauma patients who have prehospital tracheal intubation without anaesthesia or muscle relaxants: observational study. BMJ. 2001 Jul 21. 323(7305):141. [Medline].
Cooper A, DiScala C, Foltin G, Tunik M, Markenson D, Welborn C. Prehospital endotracheal intubation for severe head injury in children: a reappraisal. Semin Pediatr Surg. 2001 Feb. 10(1):3-6. [Medline].
Winchell RJ, Hoyt DB. Endotracheal intubation in the field improves survival in patients with severe head injury. Trauma Research and Education Foundation of San Diego. Arch Surg. 1997 Jun. 132(6):592-7. [Medline].
Gabriel EJ, Ghajar J, Jagoda A, Pons PT, Scalea T, Walters BC. Guidelines for prehospital management of traumatic brain injury. J Neurotrauma. 2002 Jan. 19(1):111-74. [Medline].
Stern SA, Zink BJ, Mertz M, Wang X, Dronen SC. Effect of initially limited resuscitation in a combined model of fluid-percussion brain injury and severe uncontrolled hemorrhagic shock. J Neurosurg. 2000 Aug. 93(2):305-14. [Medline].
Rotstein OD. Novel strategies for immunomodulation after trauma: revisiting hypertonic saline as a resuscitation strategy for hemorrhagic shock.
62
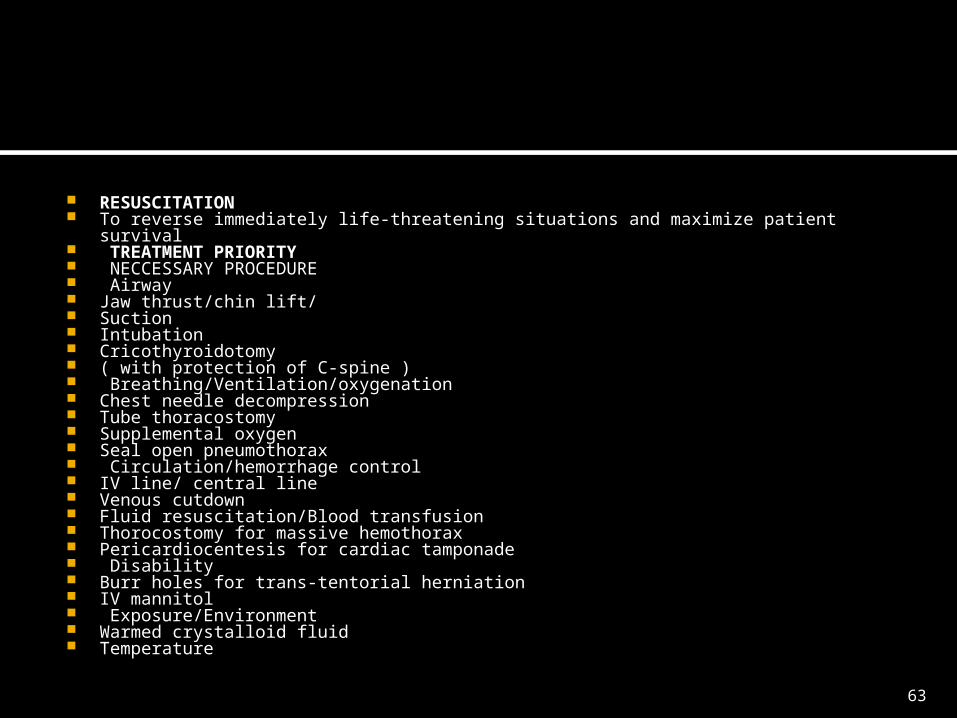
RESUSCITATION To reverse immediately life-threatening situations and maximize patient survival TREATMENT PRIORITY NECCESSARY PROCEDURE Airway Jaw thrust/chin lift/ Suction Intubation Cricothyroidotomy ( with protection of C-spine ) Breathing/Ventilation/oxygenation Chest needle decompression Tube thoracostomy Supplemental oxygen Seal open pneumothorax Circulation/hemorrhage control IV line/ central line Venous cutdown Fluid resuscitation/Blood transfusion Thorocostomy for massive hemothorax Pericardiocentesis for cardiac tamponade Disability Burr holes for trans-tentorial herniation IV mannitol Exposure/Environment Warmed crystalloid fluid Temperature
63