hands-on session: skin tightening w006...hands-on session: skin tightening anthony m. rossi, md...
TRANSCRIPT
Hands-on Session: Skin Tightening
Anthony M. Rossi, MD
Assistant Attending Memorial Sloan Kettering Cancer Center
Assistant Professor
Weill Cornell Medical College
DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY
DISCLOSURES
Allergan: Advisory Board
Cutera: Consultant
Non Invasive Skin Tightening � Therapies Skin spare the epidermis
and melanocytes � Immediate collagen contraction and
collagen denaturation � Neocollagenesis and remodeling of
collagen in 4-6 months Zelickson BD, Kist D, Bernstein D, et al. Histological and ultrastructual evaluation of the effects of a radiofrequency based nonablative dermal remodeling device: a pilot study. Arch Dermatol 2004;140:204-209
Multiple Energy and Light Based Devices Available
� Thermal energy � Electrical source such as radiofrequency
� Light based � Ultrasound (focused and non-focused)
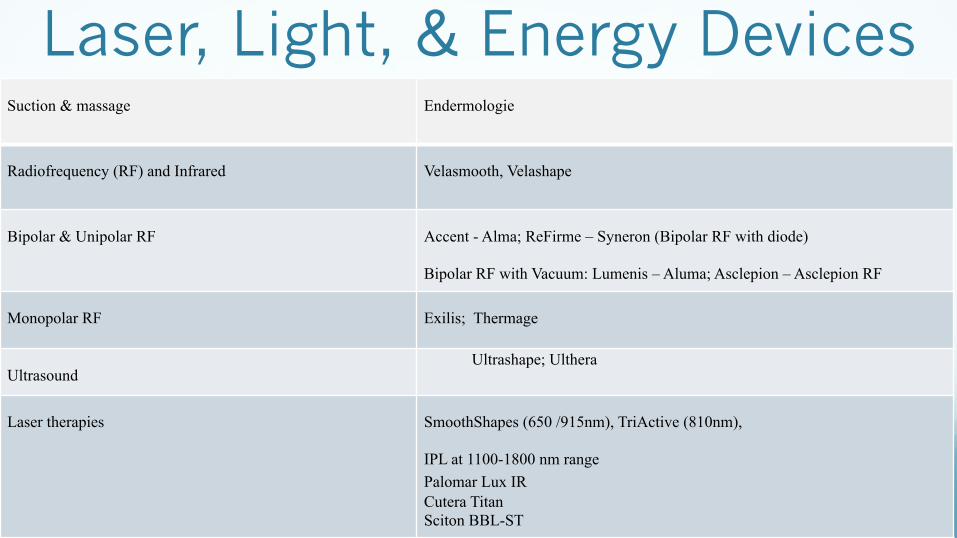
Laser, Light, & Energy Devices Suction & massage Endermologie
Radiofrequency (RF) and Infrared Velasmooth, Velashape
Bipolar & Unipolar RF Accent - Alma; ReFirme – Syneron (Bipolar RF with diode)
Bipolar RF with Vacuum: Lumenis – Aluma; Asclepion – Asclepion RF
Monopolar RF Exilis; Thermage
Ultrasound Ultrashape; Ulthera
Laser therapies SmoothShapes (650 /915nm), TriActive (810nm),
IPL at 1100-1800 nm range Palomar Lux IR Cutera Titan Sciton BBL-ST
Radiofrequency - Basics � Utilizes an electrical source
� Electrical energy becomes heat energy to the dermis at a relative low temperature
� Induces thermal damage to dermal collagen – leads to remodeling
Hollmig ST, Hantash BM. Radiofrequency in cosmetic dermatology: recent and future developments. J Cosmetic Dermatol. Dec. 2011;24:565-574
Radiofrequency � Impedance dictates where majority of
the current will flow � Lower impedance = conductivity � Impedance feedback systems are help
regulate the degree of energy and heat transferred

Monopolar radiofrequency � Volumetric bulk heating of the epidermis and dermis
� Heating is generated by innate tissue resistance to flow of electrical current
� Depends on the electrical properties of the target tissue � Most devices have cooling to protect the epidermis
� Heat → damage → subsequent inflammation alters collagen (remodeling) → produces tightening effect
� Immediate reaction � Collagen fibrils incur denaturation which shortens the fibril length � Inflammation for the initial heat
� Delayed reaction � New collagen formation
Radiofrequency technology � Monopolar
� Examples: Solta Thermage CPT®; Ellman Pelleve; BTL Exilis
� Energy is delivered to the tissues through a single electrode and hand piece.
� Requires a grounding plate and energies at 2.2-6.0 MHz
� Energy penetrates up to 20 mm � Dermal layer � Fat layer

Monopolar vs. Bipolar
Monopolar Electrode Deeper penetration of heat - Monopolar devices have one “active” electrode and a “passive” return electrode - current runs from the active electrode, through the body, and is returned at the return pad
Bipolar Electrode -More Superficial heating - the current flows back and forth between the two electrodes, and tissue is heated below and between both.
� Combined IR with bipolar RF and mechanical massage
� RF to target septa and fat; IR thought to promote collagen production, vascular flow
� Sadick et al: 35 female patients (20 treated biweekly for 4 weeks; 15 treated biweekly for 8 weeks)
� All patients: reduction in thigh circumference, skin texture, and appearance of cellulite
� Those treated for 8 weeks saw higher levels of improvement
� No statistical testing; NO DIFFERENCE B/W TREATED & UNTREATED SIDE ON HISTOLOGY
� Alster et al: 20 adult women with moderate cellulite treated biweekly for 4 weeks to inner thigh & buttock area
� Patients presented for follow-up treatments at 1, 3 and 6 months after the completion
� 18 out of 20 patients reported seeing an improvement in the appearance of their cellulite, with the average graded score being 1.82 (0-3) one month after the completion of treatment.
� However, when they were reassessed at follow-up appointments, their graded score dropped from 1.82 to approximately 1.4 at the 3 month visit and to about 1.1 at the 6 month visit
� Possible need for treatment in intervals in order to maintain results
VelaSmooth™
a) Sadick NS1, Mulholland RSA prospective clinical study to evaluate the efficacy and safety of cellulite treatment using the combination of optical and RF energies for subcutaneous tissue heating. J Cosmet Laser Ther. 2004 Dec;6(4):187-90. b) Alster TS1, Tanzi EL. Cellulite treatment using a novel combination radiofrequency, infrared light, and mechanical tissue manipulation device. J Cosmet Laser Ther. 2005 Jun;7(2):81-5.

VelaSmooth™
over 8 years. Three months after a series of eight twice-weekly VelaSmooth treatments (20 W RF, 20 W IR,200 mbar vacuum), significant improvement of her condi-tion was observed (Fig. 1B).
CASE 2
A25-year-oldwomanwithahistory of diabetes presentedwith moderate thigh and buttock cellulite (Fig. 2A). Noprior treatments had been received. One month after aseries of eight twice-weekly VelaSmooth treatments (20 WRF, 20W IR, 200mbar vacuum),mild clinical improvementwas evident (Fig. 2B). Note: Similar clinical results wouldbe expected from the TriActive device.
SUMMARY
The focus of this discussionwas to outline the treatmentsthat have a positive effect on cellulite in a clinical setting,given the systems currently available. Despite the pre-
valence of cellulite and the popularity of various cellulitetreatments, there remains a relative lack of basic andclinical research in the area. In an ideal world, prolongedor even permanent improvement of cellulite would bepossible. Unfortunately, the transient nature and signifi-cant variations in clinical efficacy from the use of over-the-counter products and massage-based therapies arethe norm. Even the two FDA-approved combinationlaser systems have their limitations, but at least yieldbetter and more prolonged clinical results than othertherapies.
In practice, a series (eight or more) combined IRlight!RF and mechanical negative tissue massage treat-ments are recommended on a twice-weekly basis, followedby monthly treatments thereafter to maintain and furtherenhance the clinical effect. Adherence to this protocol,along with a healthy sense of realism, keeps patient(and physician) expectations in check. In addition, areasonable diet and exercise plan facilitates and enhancesthe process.
Fig. 1. Posterior thigh and buttock cellulite before (A) andthree months after a series of eight twice weekly VelaSmoothtreatments (B).
Fig. 2. Posterior thigh and buttock cellulite before (A) and onemonth after a series of eight twice-weekly VelaSmoothtreatments (B).
TREATMENT OF CELLULITE WITH OPTICAL DEVICES 729
Alster et al: 30 minute treatment session 20 W RF 20 W IR (700-1,500nm) light 200 mbar vacuum mild erythema / edema Retreated 2x per week 8 Sessions Monthly maintenance treatments
over 8 years. Three months after a series of eight twice-weekly VelaSmooth treatments (20 W RF, 20 W IR,200 mbar vacuum), significant improvement of her condi-tion was observed (Fig. 1B).
CASE 2
A25-year-oldwomanwithahistory of diabetes presentedwith moderate thigh and buttock cellulite (Fig. 2A). Noprior treatments had been received. One month after aseries of eight twice-weekly VelaSmooth treatments (20 WRF, 20W IR, 200mbar vacuum),mild clinical improvementwas evident (Fig. 2B). Note: Similar clinical results wouldbe expected from the TriActive device.
SUMMARY
The focus of this discussionwas to outline the treatmentsthat have a positive effect on cellulite in a clinical setting,given the systems currently available. Despite the pre-
valence of cellulite and the popularity of various cellulitetreatments, there remains a relative lack of basic andclinical research in the area. In an ideal world, prolongedor even permanent improvement of cellulite would bepossible. Unfortunately, the transient nature and signifi-cant variations in clinical efficacy from the use of over-the-counter products and massage-based therapies arethe norm. Even the two FDA-approved combinationlaser systems have their limitations, but at least yieldbetter and more prolonged clinical results than othertherapies.
In practice, a series (eight or more) combined IRlight!RF and mechanical negative tissue massage treat-ments are recommended on a twice-weekly basis, followedby monthly treatments thereafter to maintain and furtherenhance the clinical effect. Adherence to this protocol,along with a healthy sense of realism, keeps patient(and physician) expectations in check. In addition, areasonable diet and exercise plan facilitates and enhancesthe process.
Fig. 1. Posterior thigh and buttock cellulite before (A) andthree months after a series of eight twice weekly VelaSmoothtreatments (B).
Fig. 2. Posterior thigh and buttock cellulite before (A) and onemonth after a series of eight twice-weekly VelaSmoothtreatments (B).
TREATMENT OF CELLULITE WITH OPTICAL DEVICES 729
� Combined IR, bipolar RF, vacuum & mechanical massage
� Brightman et al: 19 individuals underwent 5 weekly treatments to the upper arms; 10 had 4 weekly treatments to abdomen and flanks
� Change in arm circumference was significant at 5 weeks (-0.625cm) � At follow-up of 1 month (-0.71cm) and 3 months (-0.597cm) � Reduction of abdominal circumference was significant at 3 weeks (-1.25cm) and
at follow-up of 1 month (-1.43cm) and 3 months (-1.82cm)
� Winter: 20 postpartum women underwent 5 weekly treatments to the abdomen, buttocks, and thighs
� Mean circumference reduction 5.4 cm � Improvement in skin laxity and tightening per physician and patient � No major side effects or safety concerns
Velashape™
a) Brightman L1, Weiss E, Chapas AM, Karen J, Hale E, Bernstein L, Geronemus RG.Improvement in arm and post-partum abdominal and flank subcutaneous fat deposits and skin laxity using a bipolar radiofrequency, infrared, vacuum and mechanical massage device. Lasers Surg Med. 2009 Dec;41(10):791-8. doi: 10.1002/lsm.20872. b) Winter ML1.Post-pregnancy body contouring using a combined radiofrequency, infrared light and tissue manipulation device. J Cosmet Laser Ther. 2009 Dec;11(4):229-35. doi: 10.3109/14764170903134334.
� Low-level, dual-wavelength (650/915) laser energy and massage
� Lach: 74 patients completed the study in which one thigh was randomized to SmoothShapes vs. massage alone (control). Average 14.3 treatments over 4-6 weeks. Response assessed with MRI.
� Fat thickness decreased by 1.19cm2 with SmoothShapes, and increased by 3.82cm2 in the control leg
� Overall ~82% responded to treatment
� Gold et al: Multicenter study of 83 patients with mild to moderate cellulite who received 8 treatments to one leg with SmoothShapes, with the opposite leg serving as a control.
� Reduction in thigh circumference was noted for all treatment areas (upper, middle, and lower thigh)
� Greatest reduction (-0.82cm) seen in upper thigh at 1 month follow-up � Statistically significant mean reduction seen in the treated thigh (-0.64cm) as compared to
the untreated thighs (-0.20cm) (p < 0.0001).
SmoothShapes™
a) Lach E1Reduction of subcutaneous fat and improvement in cellulite appearance by dual-wavelength, low-level laser energy combined with vacuum and massage. J Cosmet Laser Ther. 2008 Dec;10(4):202-9. doi: 10.1080/14764170802516680. b) Gold MH1, Khatri KA, Hails K, Weiss RA, Fournier N. Reduction in thigh circumference and improvement in the appearance of cellulite with dual-wavelength, low-level laser energy and massage. J Cosmet Laser Ther. 2011 Feb;13(1):13-20. doi: 10.3109/14764172.2011.552608.

Lach: MRI analysis
20.07 cm2 and 4.10 cm2, respectively. The differencein the change over time between the laser-massagetreated leg and the massage-alone treated leg wasstatistically significant (pv0.001). Among the indivi-duals, changes in fat pad thickness of the laser-massagethighs ranged from no change to up to 36.79%compared with the massage-only (control) thighs.
Among the 71 individuals who had both pre- andpost-treatment thigh circumference (tape) measure-ments, changes over time between the laser-massageand massage-alone treated legs (0.09¡1.819 vs0.11¡1.628, mean¡SD) did not differ significantly(p50.968). The inherent variability in manual tapemeasurements may have obscured differences (ifpresent) in the actual thigh circumferences.
Responders to treatment comprised 80.26% ofindividuals. Responders were those in whom (i) areduction in fat thickness on the laser-massage thighwas greater than the corresponding change in fatthickness on the massage thigh or (ii) an increase infat thickness in the laser-massage thigh was less thana corresponding increase in the massage thigh. Allother individuals were considered unresponsive totreatment. A Student’s t-test showed that amongresponders, the mean incremental increase in fatthickness of the laser-massage thighs compared to
the massage thighs was significantly greater(pv0.001) than the corresponding mean increaseamong non-responders.
Among the 74 individuals who completed the study,56.2% definitely exercised, 26% may have exercisedsomewhat, and 17.8% did not exercise during thestudy period. The effects of exercise are controlledfor by treating one thigh with laser and massage andthe contralateral thigh with massage alone.
Figure 1. Axial views (24 horizontal slices) that included both
coronal (A) and sagittal (B) images were prescribed to quantify fat
deposits in the study participants. A high degree of reproducibilitywas obtained by orienting the individual along a tangent drawn
from the superior cortex of the right femoral head to the left
femoral head.
Figure 2. Horizontal images of the laser-massage and massage-only
thighs of an individual treated in this study. The volume of each leg
was measured by pixel densitometry. Pixel counts of the entire thighexclusive of the fat layer were subtracted from the pixel counts of the
entire thigh to obtain pixel counts of the fat layer.
204 E. Lach
J Cos
met L
aser T
her D
ownlo
aded
from
infor
mahe
althc
are.co
m by
Corn
ell U
nivers
ity on
04/23
/15Fo
r pers
onal
use o
nly.
friend; and 80.3% would continue maintenancetreatments if available. One individual noted transientsacroiliac tingling during treatment.
Discussion
This study confirms that the combination of low-level,dual-wavelength laser with massage safely providessignificantly greater reduction in subcutaneous fatthan massage alone and that participant satisfactionwith the treatment and results is generally high.
Fat pad thicknesses in the treated thighs wereobjectively measured by (i) scanning MRI images at3000 and 5000 Hz to arrive at pixel counts for theentire thigh and each anatomic constituent, and then(ii) subtracting the pixel count of the entire thighexclusive of the fat layer from the pixel counts of theentire thigh. MRI scans yield a more objective valuethan a tape measure or ultrasound transducerbecause they are very reproducible and free ofoperator bias (25). Such measurements can also berandomized to the treated side to eliminate bias ofthe image interpreter.
Table II summarizes the physical modalities forimproving the appearance of cellulite, including thepresent device.
Subcision is associated with high patient satisfac-tion (6), but it is also invasive; has adverse effectssuch as pain, bruising, hyperpigmentation, and skinpuckering (4,32); and the duration of clinical effectsare not known (17). Liposuction, though potentiallyeffective for body contouring (7), is not recom-mended for cellulite because treatment may result in
increased skin dimpling (26). The relatively newminimally invasive operative procedure of laser-assisted lipolysis requires surgical anesthesia andmay have some benefit for cellulite-afflicted skin butthere are no controlled studies to confirm that.
Endermologie LPG has been suggested as amethod to rapidly reduce edema and ecchymosisafter liposuction (33). The device is designed todisorganize adipose tissue and smooth it out over aseries of treatments by sucking up the skin androlling the soft tissues between two rotating rollers(12,33). The technique is based on the assumptionthat cellulite is partly due to impaired circulation andlymphatic drainage (32). Endermologie is an FDA-approved device for a temporary reduction in theappearance of cellulite.
Other devices for cellulite have combined lightand/or RF with mechanical massage, but still havedrawbacks. The TriActive device (Cynosure,Chelmsford, MA, USA) delivering 810-nm diodelaser light (13) requires a multitude of treatments toachieve clinical effects (29,34). The 700–2000-nminfrared light with bi-polar RF and suction-basedmassage combination can initiate collagen remodel-ing (17), but the 700–2000-nm wavelength producesnon-specific heating and RF energy provides non-selective and potentially destructive bulk tissueheating. Clinical effects persist for a few months,but long-term improvements are not documented.Monopolar RF devices such as ThermaCool(Thermage, Hayward, CA, USA) and the AccentRF system (Alma Lasers, Inc., Israel) claim to havelonger-lasting results (18). The latter may be
Figure 4. Participant before treatment (left) and 2 weeks after nine treatments with the SmoothShapes device (right). In the post-treatment
photograph, the skin of the upper thigh and lower buttocks is smoother and tighter and the circumference of both treated areas is noticeablyreduced.
Table I. Changes in fat thickness (cm2) of thighs before and after treatment.
Laser-massage Massage
Pre-Tx End of Tx Change over time Pre-Tx End of Tx Change over time
Mean 136.57 135.37 21.19 133.98 137.80 3.82
SD 34.718 34.147 12.710 34.389 34.233 14.960
Tx5treatment; SD5standard deviation.
206 E. Lach
J Cos
met L
aser T
her D
ownlo
aded
from
infor
mahe
althc
are.co
m by
Corn
ell U
nivers
ity on
04/23
/15Fo
r pers
onal
use o
nly.
2 weeks post 9 treatments; SmoothShapes: 650 nm at 0.5 W and 915 nm at 1 W
MRI shows decrease circumference of treated thigh
� FDA-approved (wrinkles / rhytids) radiofrequency device - unipolar head - Heats up to 20 mm depth
� Bipolar RF – superficial heating & Unipolar RF – deeper heating
� Alexiades et al: 10 female patients each had one leg randomized to treatment every other week for an average of 4.22 treatments. � At 3 month follow-up, there was improvement in cellulite dimple density (11.25%), distribution
(10.75%), and depth (~2%). � Overall improvement of 7.83% in the appearance of cellulite
� Goldberg et al: 30 patients with upper thigh cellulite were treated every other week for 6 treatments � Evaluation before and 6 months after treatment
� 27 subjects showed clinical improvement with mean decrease in leg circumference -2.45cm � Histologic examination showed dermal fibrosis of the upper dermis
Accent XL™
a) Alexiades-Armenakas M1, Dover JS, Arndt KA. Unipolar radiofrequency treatment to improve the appearance of cellulite. J Cosmet Laser Ther. 2008 Sep;10(3):148-53. doi: 10.1080/14764170802279651. b) Goldberg DJ1, Fazeli A, Berlin AL. Clinical, laboratory, and MRI analysis of cellulite treatment with a unipolar radiofrequency device. Dermatol Surg. 2008 Feb;34(2):204-9; discussion 209. Epub 2007 Dec 17.
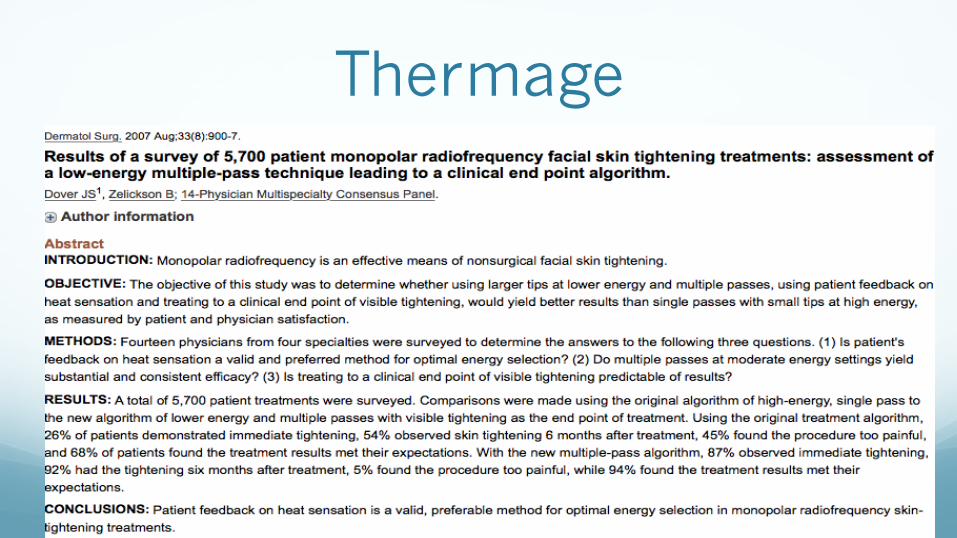
Thermage
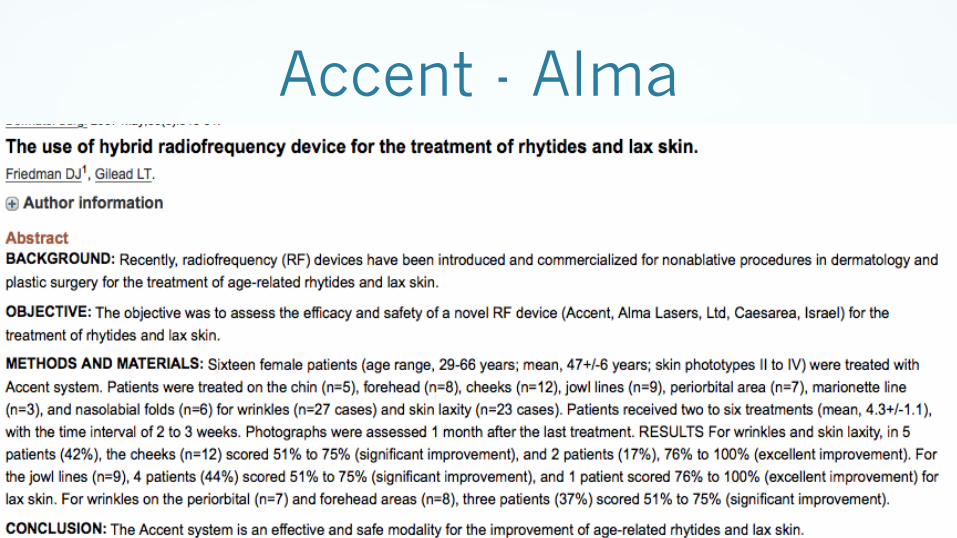
Accent - Alma
BTL: Exilis ULTRA™ FDA CLEARANCE
� The Exilis is indicated for the primary treatment of dermatologic and general surgical procedures for non-invasive treatment of wrinkles and rhytids. The massage device is intended to provide a temporary reduction in the appearance of cellulite.

MonoPolar RF with Precise Depth of Penetration
n Exilis ULTRA
n Monopolar Radiofrequency and Ultrasound
n Focused Thermal Effect with Advanced Controlled Cooling
n No Disposable Costs
n Total Body Applications

Body Applicator To Enhance Safety
� Exilis Infrared thermal sensor on applicator gives real time skin temperature readings
� All treatment controls on applicator
� Visual warning on screen and audible alarm if skin contact is compromised
Fractional Radiofrequency � Examples: Primaeva Medical Renesis, Syneron
eMatrix � Improvement in skin texture and reduced
wrinkles � Erythema post procedure � Painful � Increases type I and III collagen and decreased
elastin at 3 months post treatment
Ultrasound � Ultrasound (focused and non-focused) � low energy non-focused ultrasound and low energy electrical
stimuation and suction � Examples: Ultera® (focused), Bella Contour® (non-focused)
� Initially developed micro-focused ultrasound for non-invasive treatment of liver cancer
� Visualization of tissue, fat and bone � Imaging 8 mm below the epidermis � Painful. Tissue temperature
65-70° C � 86% response rate. Patient selection is important and critical
Laser: Infrared Wavelength � Example: Cutera Titan®
� light source generates energy from 1100 to 1800 nm for safe and effective volumetric heating of the dermis.
� Safe for all skin types
� Requires several sessions
Conclusion: Many Options
-A variety of energy and light based devices available
-Baseline severity matters
Non-invasive devices
• Least invasive • Short follow-up studies • Results may be shorter in duration • Possible need need for maintenance treatments - ? DURABILITY
Invasive laser delivery
• More invasive • Longer follow-up shows lasting results • Possibility of a single treatment
MUST MANAGE EXPECTATIONS
