haemoglobin tissues need oxygen for respiration 4 polypeptides (see protein notes) –each contains...
TRANSCRIPT

Haemoglobin
• Tissues need oxygen for respiration
• 4 polypeptides (see protein notes)– Each contains 1 haem group– Each haem group combines with 1 molecule
O2
– Hb + 4O2 ↔ HbO8
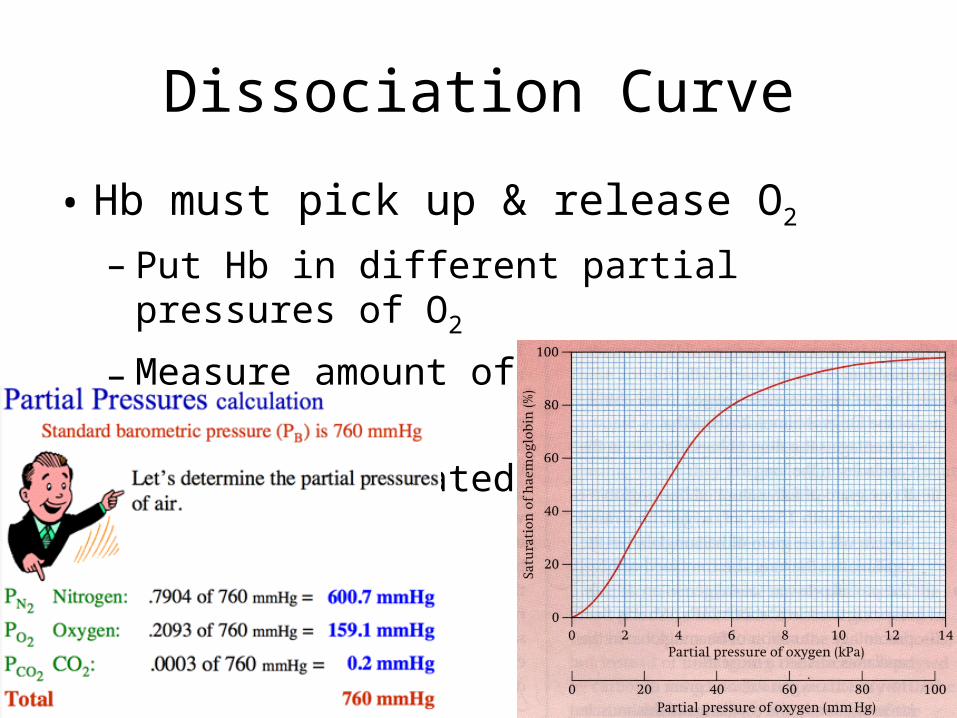
Dissociation Curve
• Hb must pick up & release O2
– Put Hb in different partial pressures of O2
– Measure amount of O2 retained by Hb
– 100% is saturated Hb
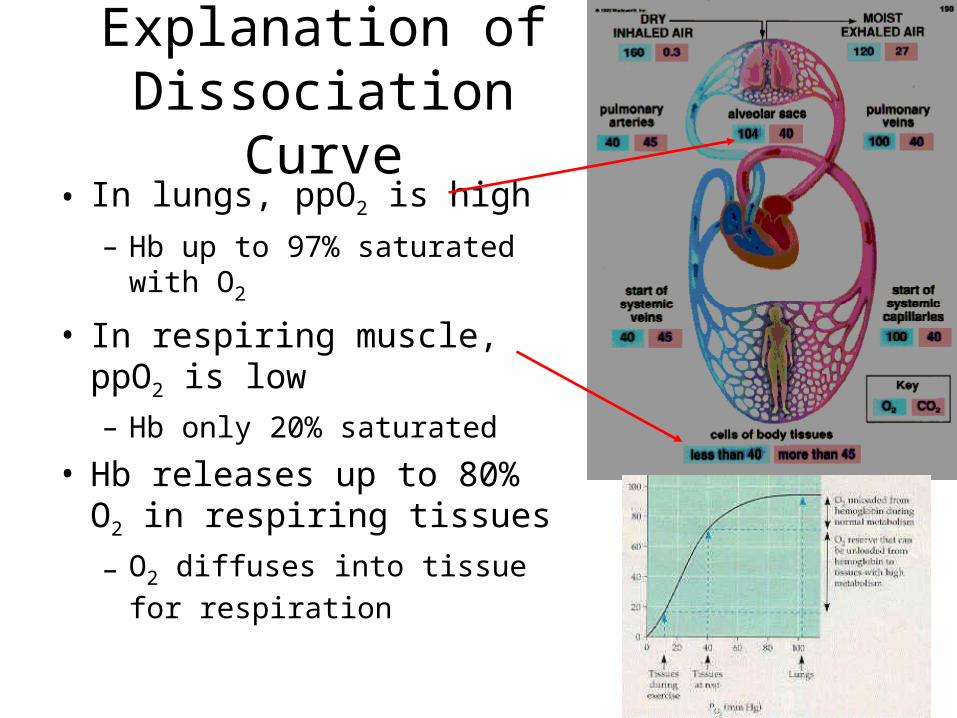
Explanation of Dissociation Curve
• In lungs, ppO2 is high
– Hb up to 97% saturated with O2
• In respiring muscle, ppO2 is low– Hb only 20% saturated
• Hb releases up to 80% O2 in respiring tissues– O2 diffuses into tissue for
respiration
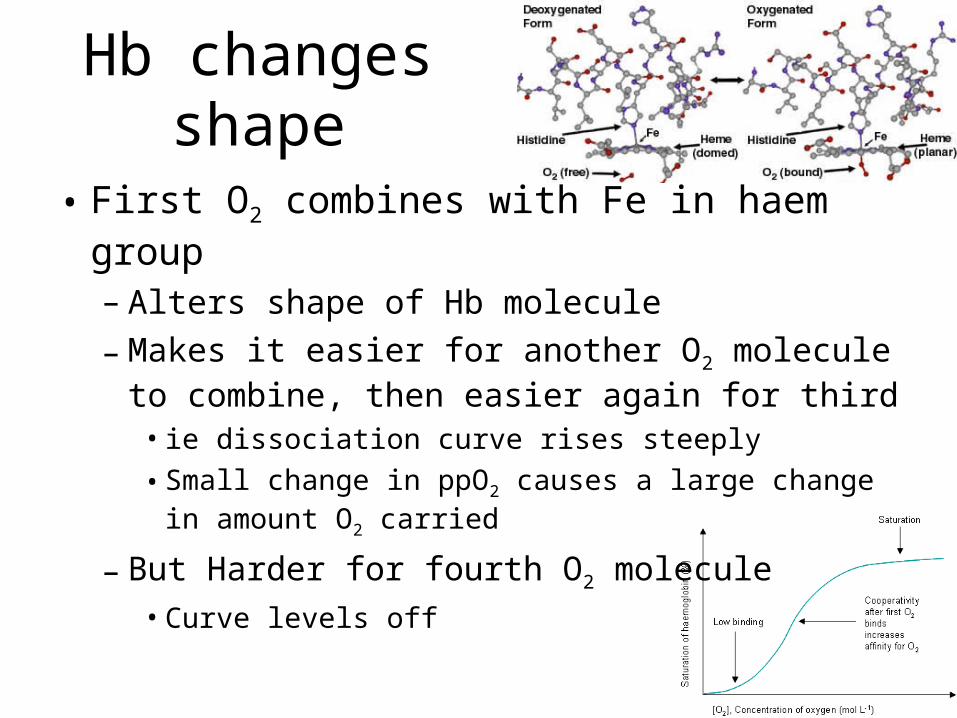
Hb changes shape
• First O2 combines with Fe in haem group
– Alters shape of Hb molecule
– Makes it easier for another O2 molecule to combine, then easier again for third
• ie dissociation curve rises steeply
• Small change in ppO2 causes a large change in amount O2 carried
– But Harder for fourth O2 molecule• Curve levels off

Effect of CO2 on Hb
• CO2 produced by respiring cells– Diffuses into RBCs– Converted to carbonic acid by carbonic
anhydrase:• CO2 + H2O ↔ H2CO3 (H+ + HCO3
-)
– Haemoglobin combines with H+, forming haemoglobinic acid (HHb)
– HHb releases O2

Bohr Shift (Bohr Effect)
• High ppCO2 causes release of O2
– When tissues very active, O2 is
required
– Dissociation curve shows release of O2 at lower ppO2
due to high ppCO2

Hb as a Buffer
• Mops up H+ from carbonic acid– Otherwise acidic conditions (low pH)– Hb maintains neutral pH
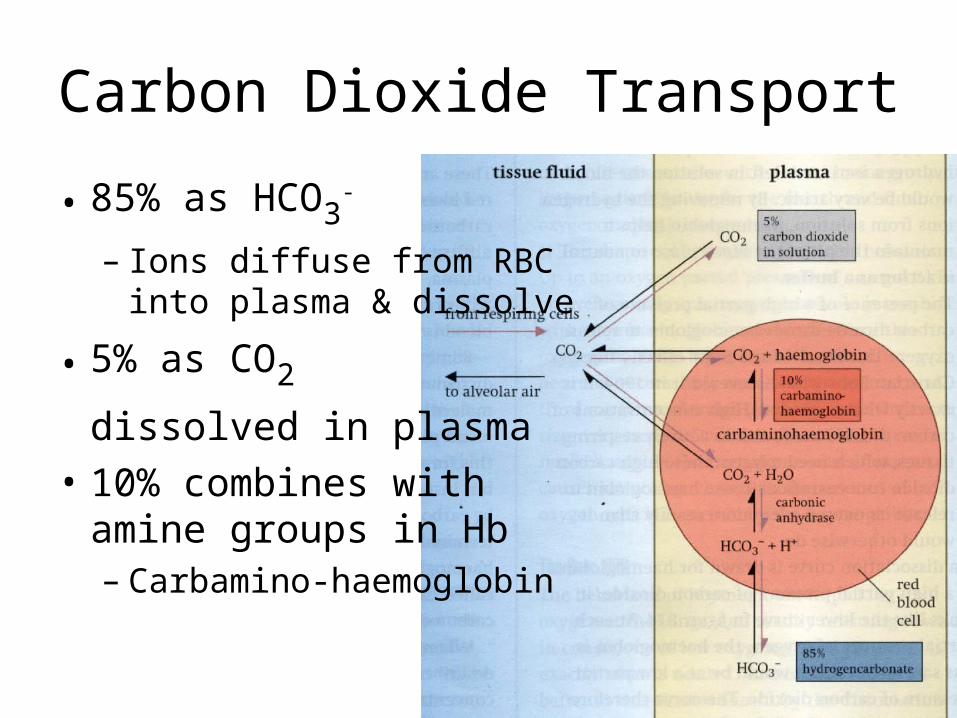
Carbon Dioxide Transport
• 85% as HCO3-
– Ions diffuse from RBC into plasma & dissolve
• 5% as CO2
dissolved in plasma
• 10% combines with amine groups in Hb– Carbamino-haemoglobin
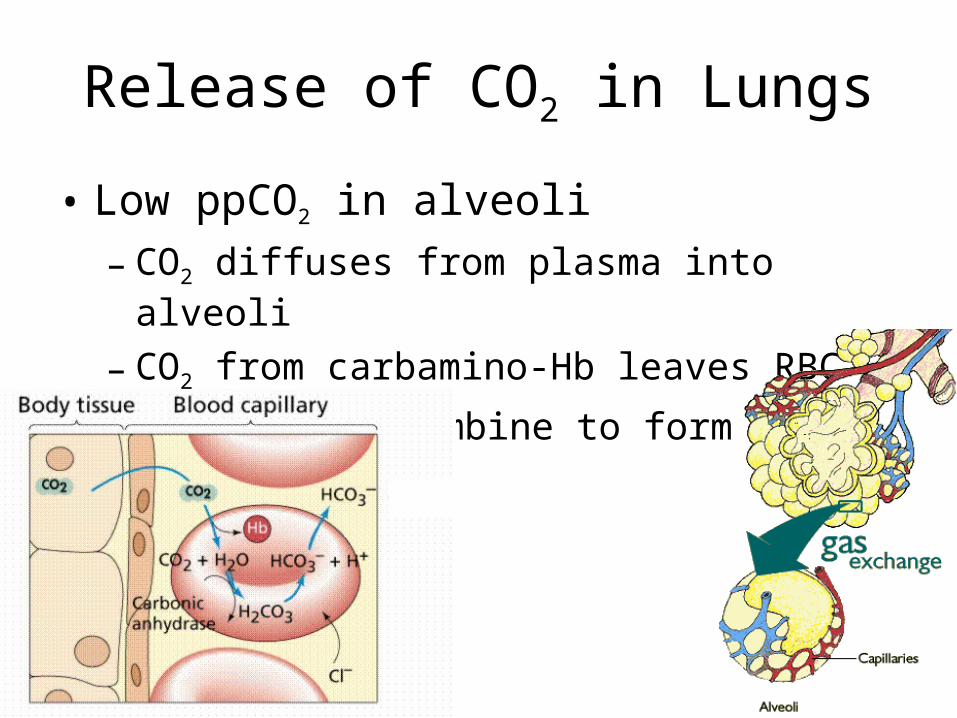
Release of CO2 in Lungs
• Low ppCO2 in alveoli
– CO2 diffuses from plasma into alveoli
– CO2 from carbamino-Hb leaves RBC
– H+ + HCO3- recombine to form CO2

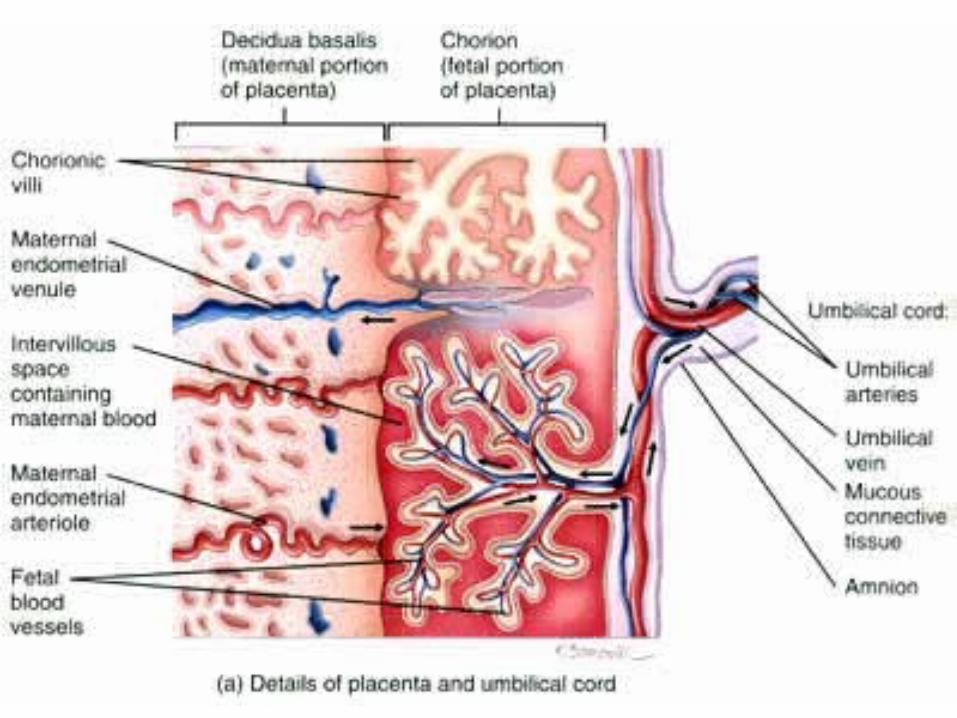
Foetal Haemoglobin• Diffusion of O2 from mothers
blood into foetus blood in placenta– Low ppO2 in placenta as foetus
is respiring– O2 passes from mother’s blood
to foetus
• Foetal Hb combines with O2 more readily than mother’s– Higher affinity– ‘Rips’ O2 away from mother’s Hb

Myoglobin
• Red pigment, in muscle cells– 1 polypeptide; 1 haem group
– Combines with 1 O2 molecule
– When combined it is very stable
– Does not release O2 until ppO2
is very low
– At each ppO2, it has higher
saturation than Hb
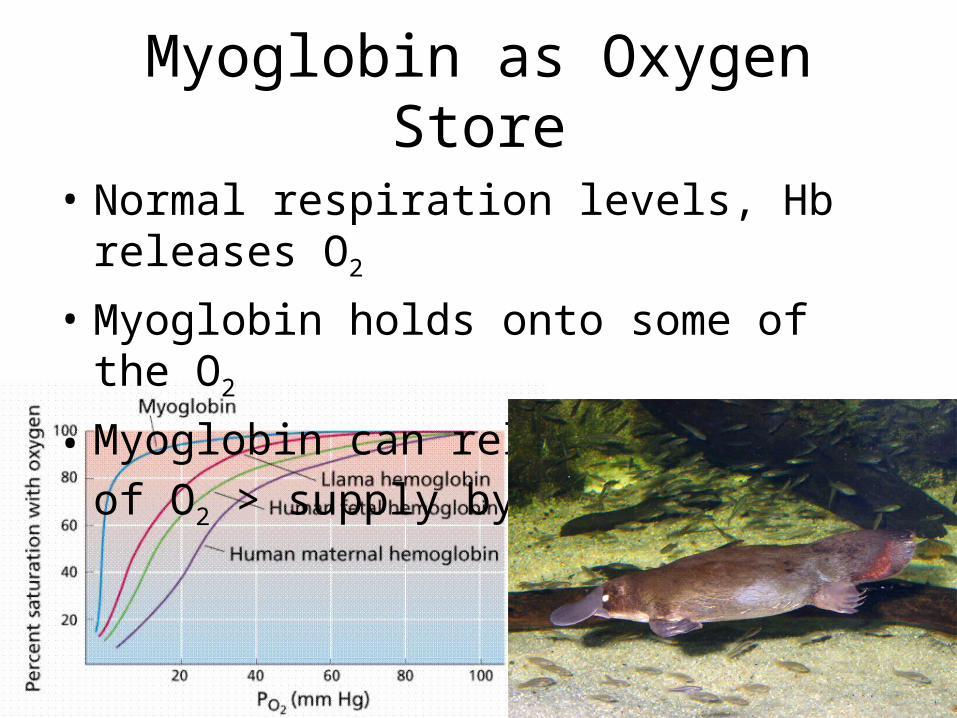
Myoglobin as Oxygen Store
• Normal respiration levels, Hb releases O2
• Myoglobin holds onto some of the O2
• Myoglobin can release O2 if use of O2 >
supply by Hb
Problems with O2 Transport
1. CO
2. High Altitude

CO
• CO combines strongly with Hb• Formed when fuels burn incompletely
– Exhaust fumes, cigarette smoke
• CO diffuses from alveoli into RBCs– Readily combines with Haem group in Hb– Forms carboxyhaemoglobin at very low ppCO– CarboxyHb* is very stable; remains in blood
• Death by asphyxiation can be caused by 0.1% CO in air
Bright red colouration*
Treatment of CO Poisoning
• Administer O2 & CO2
– O2 replaces CO
– CO2 stimulates breathing
• Note:– Cigarette smoke contains up to 5% CO– Approx 5% Hb in smokers is permanently
combined with CO• Reduces O2 carrying capacity
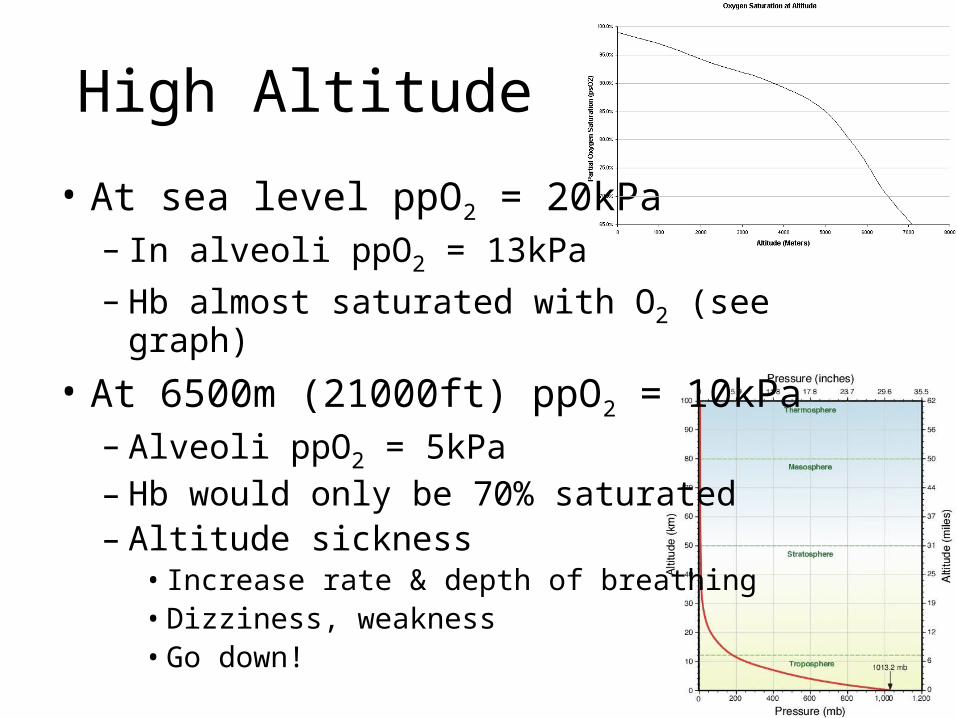
High Altitude
• At sea level ppO2 = 20kPa– In alveoli ppO2 = 13kPa
– Hb almost saturated with O2 (see graph)
• At 6500m (21000ft) ppO2 = 10kPa– Alveoli ppO2 = 5kPa– Hb would only be 70% saturated– Altitude sickness
• Increase rate & depth of breathing• Dizziness, weakness• Go down!

Acute Altitude Sickness
• Arterioles in brain dilate– Increases blood flow in capillaries– Fluid leaks into brain tissue
• Disorientation
• Fluid leaks into lungs
• May be fatal– Go down / take O2

Acclimatisation
• Body can adapt, especially up to 5000m
• 1979 climbers topped Everest without O2
– Suffered hallucinations
• Number of RBCs increases over 3 weeks– Normally 50% of blood– Up to 70% after
acclimatisation

Permanent High Altitude
• Natives in Andes or Himalayas– Not genetically different– Environmental adaptations
• Broader chests– larger lung capacity
• Larger heart– especially the right side which
pumps to lungs
• More Hb in blood– more efficient O2 transport