guidelines for the echocardiographic assessment of atrial...
TRANSCRIPT

10/9/2016NYU Leon H. Charney Division of Cardiology
1
2016 ASE Echo Florida, Orlando, FL
Guidelines for the Echocardiographic Assessment of Atrial Septal Defect and Patent Foramen Ovale
Sunday, October 9, 2016 | 2:30 – 2:45 PM | 15 min
M U H A M E D S A R I Ć , M D , P H D
D i r e c t o r o f E c h o c a r d i o g r a p h y L a b
A s s o c i a t e P r o f e s s o r o f M e d i c i n e
N e w Y o r k U n i v e r s i t y L a n g o n e M e d i c a l C e n t e r

M e d t r o n ic & P h i l i p s S p e a k e r s ’ B u r e a u s
10/9/2016NYU Division of Cardiology
2
Disclosures

10/9/2016NYU Division of Cardiology 3
Frank SilvestryUniversity of Pennsylvania
Guidelines Chair

10/9/2016NYU Division of Cardiology 4
ANATOMY & EMBRYOLOGY
Atrial septum & septal defects
1
ECHO IMAGING
2D/3D TTE & TEE
2
SHUNT ASSESSMENT
Color Doppler & contrast
3
PERCUTANEOUS CLOSURE
Echo guidance
4

Anatomy & Embryology of Atrial Septum
NYU Leon H. Charney Division of Cardiology 10/9/2016
5

10/9/2016NYU Division of Cardiology 6
Septum primum
Ostium primum
Ostium secundum
Ostium secundum
Development of septum secundum Foramen ovale
Septum primum
EMBRYOLOGY OF ATRIAL SEPTUM

10/9/2016NYU Division of Cardiology 7
ATRIAL SEPTAL DEFECTS

Common atrium
10/9/2016NYU Division of Cardiology 8
Secundum ASD(Fossa ovalis ASD)
Primum ASD(AV canal spectrum)
Sinus venosus ASD(SVC-type)
ATRIAL SEPTAL
DEFECTS

Amenable to percutaneous closure
10/9/2016NYU Division of Cardiology 9
*SVC
AV
FO
SVC-TYPE SINUS VENOSUS ASD(Right atrial perspective)*
LV
MV
AV
PRIMUM ASD(Left atrial perspective)
SECUNDUM ASD(Left atrial perspective)
*
SVC
AV~15% of ASDs
~80% of ASDs
~5% of ASDs
ATRIAL SEPTAL DEFECTS

10/9/2016NYU Leon H. Charney Division of Cardiology 10
SECUNDUM ASDsSeen from RA
perspective
SVC
AV
Circular
Ovoid
Triangular
Fenestrated
Multiple holes(< Lat. fenestra
– window)
ATRIAL SEPTAL DEFECTS | SHAPE & SIZE VARIABILITY

Echocardiographic Imagingof Atrial Septum
NYU Leon H. Charney Division of Cardiology 10/9/2016
11

10/9/2016NYU Division of Cardiology 12
ECHO IMAGING OF ATRIAL SEPTUM
For best imaging of atrial septum, insonation angle should be as perpendicular as possible to the septal plane.
TTE | Subcostal View

10/9/2016NYU Leon H. Charney Division of Cardiology 13
ECHO IMAGING OF ATRIAL SEPTUM
As perpendicular as possible to the septal plane >>> Coaxial with Doppler flow.
Large Secundum
ASD

10/9/2016NYU Division of Cardiology 14
ECHO IMAGING OF ATRIAL SEPTUM
For insonation angle is parallel (coaxial) with the septal plane,image dropouts must be differentiated from true atrial septal defects.
TTE | Apical 4-Chamber View
No ASD Secundum ASD

10/9/2016NYU Leon H. Charney Division of Cardiology 15
TEE | ATRIOVENTRICULAR & POSTERIOR ASD RIM
1
2
A
*
RA
RV
LA

3
4
B
*
RA
RV
LA
AV
10/9/2016NYU Leon H. Charney Division of Cardiology 16
TEE | AORTIC & POSTERIOR ASD RIM

C
56
*
RA
LA
SVC
10/9/2016NYU Leon H. Charney Division of Cardiology 17
TEE | SUPERIOR & INFERIOR ASD RIM

10/9/2016NYU Leon H. Charney Division of Cardiology 18
3D TEE | SECUNDUM ASD RIMS
LA Perspective
MV
AV
SVC RUPV
RA Perspective
SVC
AV
IVCTV

Atrial Septum: Associated Findings
NYU Leon H. Charney Division of Cardiology 10/9/2016
19

10/9/2016NYU Leon H. Charney Division of Cardiology 20
ATRIAL SEPTUM MASQUERADERS
• Eustachian valve• Chiari network • Thebesian valve
HEART TUBE
SINUS VENOSUS VALVE

10/9/2016NYU Leon H. Charney Division of Cardiology 21
EUSTACHIAN VALVE | PARTIAL VALVE OF IVC
BARTOLOMEO EUSTACHI
Latinized as Eustachius (1514 -1574)
Italian anatomist
RA
LA
SVCIVC

10/9/2016NYU Leon H. Charney Division of Cardiology 22
EUSTACHIAN VALVE | PARTIAL VALVE OF IVC
BARTOLOMEO EUSTACHI
Latinized as Eustachius (1514 -1574)
Italian anatomist

10/9/2016NYU Leon H. Charney Division of Cardiology 23
EUSTACHIAN VALVE | PARTIAL VALVE OF IVC
BARTOLOMEO EUSTACHI
Latinized as Eustachius (1514 -1574)
Italian anatomist

10/9/2016NYU Leon H. Charney Division of Cardiology 24
CHIARI NETWORK| REMNANT OF SINUS VENOSUS VALVE
RA
LA
RA
LA
HANS CHIARI
(1851 − 1916)Austro-Hungarian
anatomist

10/9/2016NYU Leon H. Charney Division of Cardiology 25
ATRIAL SEPTAL ANEURYSM
DEFINITION• Redundancy or saccular
deformity of the atrial septum• Increased mobility of the atrial
septal tissue. • Excursion of the septal tissue
(typically the fossa ovalis) of > 10 mm from the plane of the atrial septum into the RA or LA, or
• A combined total excursion right and left of > 15 mm
RA
LA
PREVALENCE• 2%–3% of humans
ASSOCIATIONS• Increase prevalence of PFO• Increased size of a PFO• Increased prevalence of
cryptogenic stroke• Multiple septal fenestrations
(fenestrated ASD)

10/9/2016NYU Leon H. Charney Division of Cardiology 26
ATRIAL SEPTAL ANEURYSM
M mode

Shunt Assessment
NYU Leon H. Charney Division of Cardiology 10/9/2016
27

10/9/2016NYU Leon H. Charney Division of Cardiology 28
ATRIAL SEPTAL ANEURYSM | PFO SHUNT WITH SALINE CONTRAST

10/9/2016NYU Leon H. Charney Division of Cardiology 29
INTRACARDIAC VS. INTRAPULMONARY SHUNT
• PROVOCATIVE MANEUVERS
Agitated saline injections should be performed at rest and provocative maneuvers to increase the right atrial pressure, such as cough and the Valsalva maneuver.
• PFOWithin 3 cardiac cyclesThe presence of PFO is presumed when agitated saline contrast is noted in the left atrium within 3 cardiac cycles after complete opacification of the right atrium.
• INTRAPULMONARY SHUNT
After 5 cardiac cyclesIf the agitated saline contrast is noted after 5 cardiac cycles after complete opacification of the right atrium, pulmonary arteriovenous malformations (AVMs) must be considered.
• LARGE SHUNT
> 20 bubblesVarious classification schemes have been proposed to assess the sizes of shunts, though none have been universally accepted yet. However, >20 bubbles crossing the PFO from the right to left atrium is considered to be a large shunt

10/9/2016NYU Leon H. Charney Division of Cardiology 30
PFO VS. INTRAPULMONARY SHUNT
Intrapulmonary Shunt
Intracardiac Shunt (PFO)

Percutaneous Closure of Secundum ASD
NYU Leon H. Charney Division of Cardiology 10/9/2016
31

2D/3D Echocardiography in ASD Closure
10/9/2016NYU Leon H. Charney Division of Cardiology
32
BeforeASD Closure
DuringASD Closure
AfterASD Closure
Appropriateness criteria for ASD closure (whether surgical or percutaneous)
ASD details relevant to percutaneous ASD closure
Visualization of guide catheters and ASD closure device as it is being deployed
Assessment of device seatedness and residual shunt
Perk, G, Ruiz, C, Saric, M and Kronzon, I. Current Cardiovascular Imaging Reports 2009;2:363-374.

Pre-procedural Imaging
NYU Leon H. Charney Division of Cardiology 10/9/2016
33

10/9/2016NYU Leon H. Charney Division of Cardiology 34
CASE PRESENTATION
49-year-0ld woman with progressive dyspnea on exertion over the past year
• History of hypertension
• An atrial septal defect (ASD) and no pulmonary hypertensionwere seen on a transthoracic echocardiograph (TTE)
• Now referred for transesophageal echocardiogram (TEE)

10/9/2016NYU Leon H. Charney Division of Cardiology 35
PREPROCEDURAL TEE | VIEW AT 99°

10/9/2016NYU Leon H. Charney Division of Cardiology 36
PREPROCEDURAL TEE | BIPLANE VIEW
10/9/2016NYU Leon H. Charney Division of Cardiology 37
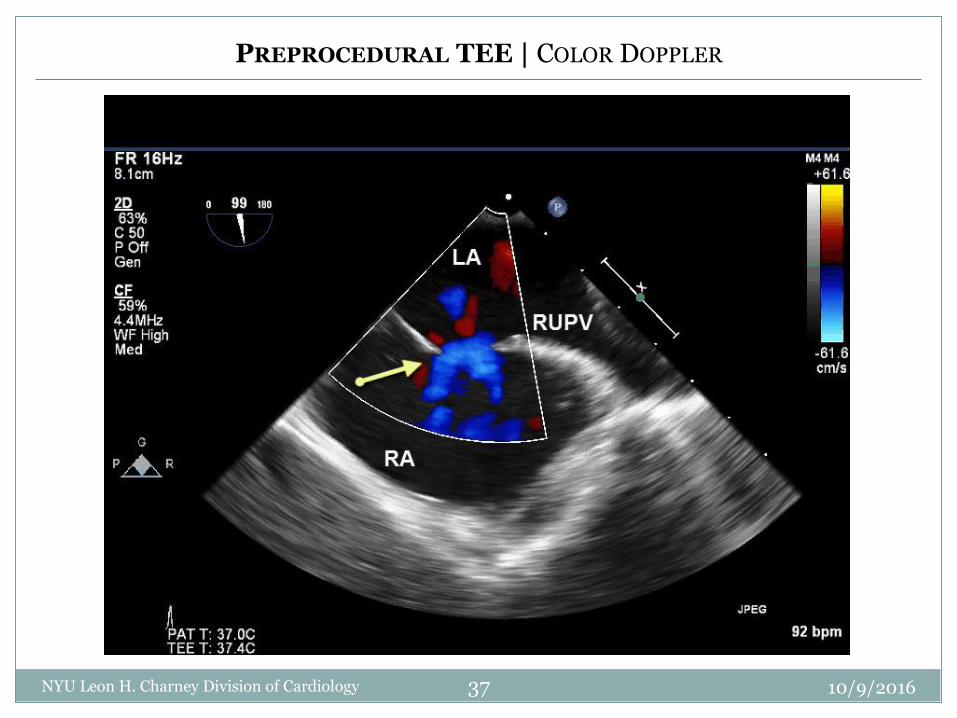
PREPROCEDURAL TEE | COLOR DOPPLER

10/9/2016NYU Leon H. Charney Division of Cardiology 38
PREPROCEDURAL TEE | 4-CHAMBER VIEW

10/9/2016NYU Leon H. Charney Division of Cardiology 39
DIAGNOSIS
• Secundum ASD with left-to-right shunt
• Dilated right heart
• No pulmonary hypertension
• Progressive dyspnea on exertion

10/9/2016NYU Leon H. Charney Division of Cardiology 40
QUESTION
Has the patient met the clinical & hemodynamic criteria for ASD closure?

10/9/2016NYU Leon H. Charney Division of Cardiology 41

10/9/2016NYU Leon H. Charney Division of Cardiology 42
QUESTION
Has the patient met the anatomic criteria for percutaneous ASD closure?

10/9/2016NYU Leon H. Charney Division of Cardiology 43
PREPROCEDURAL TEE | ATRIOVENTRICULAR & POSTERIOR RIM
1
2
A
*
RA
RV
LA

3
4
B
*
RA
RV
LA
AV
10/9/2016NYU Leon H. Charney Division of Cardiology 44
PREPROCEDURAL TEE | AORTIC & POSTERIOR RIM

C
56
*
RA
LA
SVC
10/9/2016NYU Leon H. Charney Division of Cardiology 45
PREPROCEDURAL TEE | SUPERIOR & INFERIOR RIM

10/9/2016NYU Leon H. Charney Division of Cardiology 46
PREPROCEDURAL 3D TEE | SECUNDUM ASD RIMS
LA Perspective
MV
AV
SVC RUPV
RA Perspective
SVC
AV
IVCTV

10/9/2016NYU Leon H. Charney Division of Cardiology 47
PREPROCEDURAL 3D TEE | TUPLE MANEUVER
Saric, M, Perk, G, Purgess, JR, Kronzon, I. J Am Soc Echocardiogr 2010;23:1128-35.

10/9/2016NYU Leon H. Charney Division of Cardiology 48
PREPROCEDURAL 3D TEE | RA PERSPECTIVE | ASD SIZING

10/9/2016NYU Leon H. Charney Division of Cardiology 49
DIAGNOSIS
• Secundum ASD with left-to-right shunt
• ASD Size: 1.85 x 1.25 cm
• Sufficient ASD rims

10/9/2016NYU Leon H. Charney Division of Cardiology 50
AMPLATZER
For ASDs up to 38-mm in diameter
LA Disc > RA Disc
Gore-HelexFor ASDs up to
18-mm in diameter
RA Disc = LA Disc
PERCUTANEOUS ASD OCCLUDERS

10/9/2016NYU Leon H. Charney Division of Cardiology 51
PERCUTANEOUS ASD CLOSURE PEARLS

A S D B A L L O O N S I Z I N G
Intra-procedural Imaging
NYU Leon H. Charney Division of Cardiology 10/9/2016
52

10/9/2016NYU Leon H. Charney Division of Cardiology 53
FLUOROSCOPY | ASD SIZING
After obtaining a peripheral venous access, a sizing balloon is inflated inside the ASD
Balloon waist at ASD level

10/9/2016NYU Leon H. Charney Division of Cardiology 54
INTRAPROCEDURAL TEE | ASD BALLOON SIZING

10/9/2016NYU Leon H. Charney Division of Cardiology 55
INTRAPROCEDURAL TEE | ASD BALLOON SIZING

10/9/2016NYU Leon H. Charney Division of Cardiology 56
ASD SIZING | STOP-FLOW DIAMETER

10/9/2016NYU Leon H. Charney Division of Cardiology 57
ASD OCCLUDER SIZING
19-mm Amplatzer ASD occluder was chosen

A S D O C C L U D E R D E P L O Y M E N T
Intra-procedural Imaging
NYU Leon H. Charney Division of Cardiology 10/9/2016
58

10/9/2016NYU Division of Cardiology 59
INTRAPROCEDURAL 3D TEE | DEPLOYMENT OF LA DISC

10/9/2016NYU Division of Cardiology 60
INTRAPROCEDURAL 3D TEE | DEPLOYMENT OF LA DISC

10/9/2016NYU Division of Cardiology 61
INTRAPROCEDURAL 3D TEE | DEPLOYMENT OF LA DISC

10/9/2016NYU Division of Cardiology 62
INTRAPROCEDURAL 2D TEE | AMPLATZER OCCLUDER DEPLOYMENT

10/9/2016NYU Division of Cardiology 63
INTRAPROCEDURAL ICE| AMPLATZER OCCLUDER DEPLOYMENT

10/9/2016NYU Division of Cardiology 64
INTRAPROCEDURAL ICE| AMPLATZER OCCLUDER DEPLOYMENT

10/9/2016NYU Division of Cardiology 65
INTRAPROCEDURAL FLUOROSCOPY | AMPLATZER OCCLUDER DEPLOYMENT

A S D O C C L U D E R D E P L O Y M E N T
Post-procedural Imaging
NYU Leon H. Charney Division of Cardiology 10/9/2016
66

10/9/2016NYU Division of Cardiology 67
POST-PROCEDURAL 3D TEE | AMPLATZER DEPLOYED
RA Perspective LA Perspective

10/9/2016NYU Division of Cardiology 68
POST-PROCEDURAL 2D TEE | AMPLATZER DEPLOYED
Check for para-device leak.

10/9/2016NYU Leon H. Charney Division of Cardiology 69
POST PERCUTANEOUS ASD OCCLUDER
Complications are rare……but you must check for them proactively!

10/9/2016NYU Division of Cardiology 70
POST-PROCEDURAL 2D TTE | ASD OCCLUDER EMBOLIZED
Check for complications.

10/9/2016NYU Division of Cardiology 71
POST-PROCEDURAL CATH| RETRIEVAL OF ASD OCCLUDER

Thank You!
10/9/2016NYU Leon H. Charney Division of Cardiology
72
New York University Medical Center

A S D B A L L O O N S I Z I N G
Bonus Slides
NYU Leon H. Charney Division of Cardiology 10/9/2016
73

Before ASD Closure
10/9/2016NYU Division of Cardiology
74
Part 1

Before ASD Closure: Guidelines for ASD Closure
Class I Recommendations RA or RV enlargement with or without symptoms
Sinus venosus, coronary sinus or primum ASDs should be repaired surgically rather than percutaneously
10/9/2016NYU Leon H. Charney Division of Cardiology
75
Class II Recommendations Paradoxical embolism Orthodeoxia-platypnea Net left-to-right shunt
when PVR < 2/3 SVR and PAP < 2/3 systemic BP
Class III Recommendations Patients with severe irreversible pulmonary
arterial hypertension and no evidence of a left-to-right shunt should NOT undergo ASD closure
ACC/AHA Guidelines for Adult Congenital Heart Disease, Circulation 2008;118:e714-833.
1. Establish the diagnosis of SECUNDUM ASD
2. Assess for RIGHT HEART DILATATION
3. Document the presence of a net LEFT-to-RIGHT SHUNT
4. Measure pulmonary artery PRESSURE and RESISTANCE

Assessment Before ASD Closure
10/9/2016NYU Leon H. Charney Division of Cardiology
76
RIGHT HEART DILATATION NET LEFT-to-RIGHT SHUNT
Apical 4-Chamber ViewSECUNDUM ASD
ASE/EAE/CSE Guidelines for Right Heart AssessmentJ Am Soc Echocardiogr 2010;23:685-713.
Left-to-Right ShuntSECUNDUM ASD

Secundum ASD: Left-to-Right Shunt
10/9/2016NYU Leon H. Charney Division of Cardiology
77
Spectral DopplerASD Flow in Sinus Rhythm
Color Doppler2D TEE at 30 Degrees
PEAK 1-----------------------------------
End-ventricular systole
PEAK 2-------------Atrial kick

Before ASD Closure: Right Heart Pressures
10/9/2016NYU Leon H. Charney Division of Cardiology
78
TR Jet
TR Jet
3 m/s
PI Jet
1.5 m/s
IVC
RAP=3 mm Hg
PASP = 4 * (3 m/sec)2 + RAP = 39 mm Hg PADP = 4 * (1.5 m/sec)2 + RAP = 12 mm Hg

Before ASD Closure: Pulmonary Vascular Resistance
10/9/2016NYU Leon H. Charney Division of Cardiology
79
PVR = 0.16 + 10 * (3 m/sec) / (17 cm)
PVR = 1.8 Wood units [or, 1.8 * 80 = 144 SI units]
TR Jet
3 m/sSystolic RVOT VTI = 17 cm
RVOT
RVOT
jetTR
VTI
VPVR
max*1016.0
Abbas MethodJ Am Coll Cardiol 2003;41:1021-7.
Flow
ΔPResistance

PVR and ASD Closure
10/9/2016NYU Leon H. Charney Division of Cardiology
80
Closure of ASD is usually NOT done when:--------------------------------------PVR > 2/3 * SVR
Normal Resistance Values-------------------------------------PVR = 1-2 Wood unitsSVR = 11-16 Wood units
Paul WoodBritish invasive cardiologist
(1907–1962)Died of acute LAD infarct

10/9/2016NYU Division of Cardiology
82
Diagnosis of ASD Per Se
ASD Shape*
ASD Orifice and Rim Size*
Relationship of ASD to surrounding structures

10/9/2016NYU Leon H. Charney Division of Cardiology 83
Secundum ASDs: Variety of Shapes
SECUNDUM ASDsSeen from RA
perspective
SVC
AV
Circular
Ovoid
Triangular
Fenestrated
Multiple holes(< Lat. fenestra
– window)

Relationships of Secundum ASDs
10/9/2016NYU Leon H. Charney Division of Cardiology
84
SVC
AV
*
A B
AV
*
SVC
RA Perspective LA Perspective
SUFFICEINT ASD RIMS Aortic rim > 3 mmOther rims > 7 mm

Orienting 3D TEE Images of Atrial Septum
10/9/2016NYU Leon H. Charney Division of Cardiology
85TUPLE Maneuver: Tilt Up Then Left
Saric, M, Perk, G, Purgess, JR, Kronzon, I. J Am Soc Echocardiogr 2010;23:1128-35.
Acquisition at 0 Degrees Acquisition at 120 Degrees

Orienting 3D TEE Images of Atrial Septum
10/9/2016NYU Leon H. Charney Division of Cardiology
86
TUPLE maneuver is now featured in the latest edition of Braunwald textbook of cardiology.
Acquisition at 0 Degrees

Sizing Secundum ASDs: The OLD Way
10/9/2016NYU Leon H. Charney Division of Cardiology
89
Method #1: Rectangular Grid (2 mm) Method #2: Multiplane Reconstruction (MPR)
ASD 1.6 x 1.4 cm

Sizing Secundum ASDs: The NEW Way
10/9/2016NYU Leon H. Charney Division of Cardiology
90
Method #3: ASD Sizing Directly on 3D TEE Image
ASD Diameters: 1.6 x 1.4 cmASD Area : 1.8 cm2
ASD Circumference: 5.0 cm

Diameter
Diameter
3D TEEMPR = Multi Plane Reconstruction
Sizing Secundum ASDs: 2D vs. 3D
10/9/2016NYU Leon H. Charney Division of Cardiology
91
2D TEETends to UNDERESTIMATE the size of
ASD-----------------------------------------Often geometric chord rather than
true diameter is measured.
Chord
RA
LAASD
AV
χορδή = gut, string of a musical instrument (made of gut)

ASD Occluders
Approved for use in the United States
92
10/9/2016NYU Leon H. Charney Division of Cardiology
Device #1:Amplatzer
LA Disc > RA Disc
Device #2:Gore-Helex
RA Disc = LA Disc

10/9/2016NYU Leon H. Charney Division of Cardiology 93
St. Jude Amplatzer ASD Occluder: Sizing based on WAIST size
Kurt Amplatz(b. 1925)
Austrian-born American radiologist

10/9/2016NYU Leon H. Charney Division of Cardiology 94
Gore-Helex: Sizing based on DISC size

During ASD Closure
10/9/2016NYU Division of Cardiology
95
Part 2

Percutaneous ASD Closure
10/9/2016NYU Division of Cardiology
96
STEP 1
Femoral venous access
STEP 2
RA
LAASD
Passage of wires & catheters across ASD
Sizing of ASD with balloon
Deployment of ASD closure device
STEP 3
ASD
RA
LA
RA
LA
ASD
VIDEO

Percutaneous ASD Closure
Balloon Sizing(Stop-flow diameter)
99
10/9/2016NYU Leon H. Charney Division of Cardiology

Percutaneous ASD Closure
ASD Closure Device Deployment
Amplatzer Device Still Attached to Delivery
Catheter
100
10/9/2016NYU Leon H. Charney Division of Cardiology
RA Perspective
LA Perspective

Percutaneous ASD Closure
ASD Closure Device Deployment
Tugging the device
101
10/9/2016NYU Leon H. Charney Division of Cardiology
Residual Leak

ASD Closure Device: LA Perspective
10/9/2016NYU Leon H. Charney Division of Cardiology
102
Gore-Helex ASD OccluderResidual Leak
Repositioned Gore-Helex Device: No Leak

ASD Closure: Intracardiac Echo (ICE)
10/9/2016NYU Leon H. Charney Division of Cardiology
103

Post ASD Closure
10/9/2016NYU Division of Cardiology
104
Part 3

ASD Occluders Seen From LA Side
10/9/2016NYU Leon H. Charney Division of Cardiology
106
After percutaneous ASD closure, check for complications (e.g. pericardial effusion).
Amplatzer Gore-Helex

Primum ASD
NYU Leon H. Charney Division of Cardiology 10/9/2016
113

10/9/2016NYU Division of Cardiology 114
PRIMUM ASD
Part of the endocardial cushion
(AV canal) disease spectrum
Associated withDown syndrome
(trisomy 21) disease spectrum
John Langdon Down(1828-1896)
British physician

10/9/2016NYU Leon H. Charney Division of Cardiology 115
ENDOCARDIAL CUSHION DISEASE SPECTRUM
NormalAV Canal
Complete AV Canal
PartialAV Canal

10/9/2016NYU Leon H. Charney Division of Cardiology 116
PRIMUM ASD | AV CANAL

10/9/2016NYU Leon H. Charney Division of Cardiology 117
PRIMUM ASD

10/9/2016NYU Leon H. Charney Division of Cardiology 118
PRIMUM ASD + SOMETHING ELSE
PeculiarMitral Regurgitation

10/9/2016NYU Leon H. Charney Division of Cardiology 119
Cleft Mitral Valve(LV perspective)
PRIMUM ASD + CLEFT MITRAL VALVE
Relationship between cleft mitral valve and primum ASD

10/9/2016NYU Leon H. Charney Division of Cardiology 120
CLEFT MITRAL VALVE: LA PERSPECTIVE

10/9/2016NYU Leon H. Charney Division of Cardiology 121
TEACHING POINTS
• Primum ASD is located near the atrioventricular valves
• Rarely an isolated lesion
• Typically associated with elements of endocardial cushion defect disease spectrum• Cleft mitral valve• Inlet VSD

Sinus Venosus ASD
NYU Leon H. Charney Division of Cardiology 10/9/2016
122

10/9/2016NYU Division of Cardiology 123
SINUS VENOSUS ASDS
IVC-typeSinus venosus ASD
SVC-typeSinus venosus ASD
Sinus venosus is an embryologic venous reservoir proximal to the right atrium.

10/9/2016NYU Leon H. Charney Division of Cardiology 124
SVC-TYPE SINUS VENOSUS ASD
Markedly dilated right heart without apparent septal defect

10/9/2016NYU Leon H. Charney Division of Cardiology 125
SVC-TYPE SINUS VENOSUS ASD

10/9/2016NYU Leon H. Charney Division of Cardiology 126
SVC-TYPE SINUS VENOSUS ASD | ANOMALOUS PULMONARY VENOUS RETURN
RUPV
SVC

10/9/2016NYU Leon H. Charney Division of Cardiology 127
True Atrial Septum
Aortic Valve
SVC
ASD
RA Aspect
SVC-TYPE SINUS VENOSUS ASD

10/9/2016NYU Leon H. Charney Division of Cardiology 128
SVC-TYPE SINUS VENOSUS ASD + PAPVR

Thank You!
10/9/2016NYU Leon H. Charney Division of Cardiology
129
New York University Medical Center