guidelines for initiating and monitoring ketogenic therapy
TRANSCRIPT

GUIDELINES FOR INITIATING AND MONITORING KETOGENIC THERAPY FOR
PATIENTS WITH EPILEPSY
By
MANDY HAMMOND LAYMAN
A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE
UNIVERSITY OF FLORIDA
2004

Copyright 2005
by
Mandy Hammond Layman

iii
ACKNOWLEDGMENTS
I would like to thank Dr. Peggy Borum for her guidance, support, and patience with
this study. Her compassion for the patients is truly inspirational.
I would also like express my appreciation to Dr. Gail Kauwell for the guidance and
advice she offered throughout the program. I learned a lot from her passion for helping
others and her commitment to her work.
I would also like to thank Dr. Paul Carney for his leadership in the ketogenic
program at the University of Florida. His expertise in this field has been an invaluable
resource.
I thank my fellow lab members for the time and hard work they put into this study.
Sheron Wen is appreciated for analyzing valuable statistical data used in this study.
I thank my husband, Zack Layman, for always having confidence in me and for his
continuous encouragement.
Finally, I would like to thank my parents, Randy and Carolyn Hammond, for
making it possible for me to be here and for uplifting me with their endless love.

iv
TABLE OF CONTENTS page ACKNOWLEDGMENTS ................................................................................................. iii
LIST OF TABLES............................................................................................................. vi
LIST OF FIGURES ......................................................................................................... viii
ABSTRACT.........................................................................................................................x
CHAPTER 1 INTRODUCTION ........................................................................................................1
Background...................................................................................................................1 Purpose .........................................................................................................................2
2 METHODS...................................................................................................................4
3 DEVELOPMENT OF KETOGATOR (KG) GUIDELINES.......................................7
Patient Selection ...........................................................................................................7 Inborn Errors of Metabolism.................................................................................7 Age ........................................................................................................................8 Efficacy for All Age Groups ...............................................................................11 Effects of AEDs...................................................................................................15
Use of Ketogenic Therapy Combined with Other Treatments ...................................20 AEDs ...................................................................................................................20 VNS and Surgery.................................................................................................26
Initiation......................................................................................................................33 Schedule Protocol................................................................................................33 Fasting .................................................................................................................37 Laboratory Values ...............................................................................................43 Patient/Parent Education .....................................................................................45
Diet Prescription at Initiation and During Fine-Tuning .............................................48 Ratio ....................................................................................................................48 Calories................................................................................................................52 Fluids ...................................................................................................................59
Monitoring Potential Adverse Effects ........................................................................63 Growth and Development....................................................................................63
v
High Lipid Profiles ..............................................................................................69 Other Adverse Effects .........................................................................................83
4 DISCUSSION OF KETOGATOR GUIDELINES ....................................................88
Pre-Initiation ...............................................................................................................88 Patient Selection ..................................................................................................88 Use of Ketogenic Therapy Combined with Other Treatments ............................89 Patient/Parent Education .....................................................................................89
Initiation......................................................................................................................90 Schedule Protocol................................................................................................90 Fasting .................................................................................................................90 Laboratory Values ...............................................................................................91 Patient/Parent Education .....................................................................................91 Diet Prescription..................................................................................................91
Post-Initiation .............................................................................................................92 Laboratory Values ...............................................................................................92 Growth and Development....................................................................................92 Potential Adverse Effects ....................................................................................92 Surgery ................................................................................................................93
Chapter Summary .......................................................................................................93 5 SUMMARY................................................................................................................98
APPENDIX A DATABASE PARAMETERS..................................................................................100
B DATABASE QUERIES ...........................................................................................105
C WORKING HYPOTHESES ....................................................................................117
D TOLERANCE AND COMPLIANCE FORMS .......................................................118
E DIET PRESCRIPTION FORM................................................................................127
F PATIENT/PARENT EDUCATION FORM ............................................................130
LIST OF REFERENCES.................................................................................................132
BIOGRAPHICAL SKETCH ...........................................................................................138

vi
LIST OF TABLES
Table page 2-1 Evidence Grading System* ..........................................................................................5
3-1 Basis of KetoGator Guidelines. Patient Selection: Inborn Errors ...............................9
3-2 Basis of KetoGator Guidelines. Patient Selection: Age ............................................16
3-3 Basis of KetoGator Guidelines. Patient Selection: Effects of AEDs ........................21
3-4 Basis of KetoGator Guidelines. Use of Combined Treatments: AEDs.....................27
3-5 Basis of KetoGator Guidelines. Use of Combined Treatments: VNS.......................30
3-6 Basis of KetoGator Guidelines. Use of Combined Treatments: Surgery ..................31
3-7 Ketogenic Diet Protocol at Johns Hopkins Hospital ..................................................34
3-8 Ketogenic Diet Protocol at the University of Florida.................................................35
3-9 Basis of KetoGator Guidelines. Initiation: Schedule Protocol ..................................38
3-10 Basis of KetoGator Guidelines. Initiation: Fasting .................................................41
3-11 Suggested lab values* ...............................................................................................44
3-12 Basis of KetoGator Guidelines. Initiation: Lab Values...........................................45
3-13 Basis of KetoGator Guidelines. Initiation: Patient/Parent Education......................49
3-14 Recommended Age-Based Initiation Ratios (Fat: Protein + Carbohydrate) for Ketogenic Therapy ...................................................................................................51
3-15 Basis of KetoGator Guidelines. Diet Prescription: Ratio ........................................53
3-16 Estimated Energy Requirement (EER) Related to Age and Gender ........................54
3-17 Guidelines for Calculating Energy Needs for Patients on Ketogenic Therapy ........54
3-18 Basis of KetoGator Guidelines. Diet Prescription: Calories ...................................57

vii
3-19 Holiday-Segar Method for Determining Maintenance Fluid Needs ........................60
3-20 Basis of KetoGator Guidelines. Diet Prescription: Fluids.......................................61
3-21 Basis of KetoGator Guidelines. Diet Prescription...................................................64
3-22 Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: Growth and Development ............................................................................................................67
3-23 Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: High Lipid Profiles .....................................................................................................................80
3-24 Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: Other Adverse Effects ........................................................................................................84
4-1 KetoGator (KG) Guidelines........................................................................................94
A-1 Population Database Parameters* ............................................................................100
C-1 Working Hypotheses................................................................................................117

viii
LIST OF FIGURES
Figure page 3-1 Algorithm for choosing the appropriate treatment(s) for patients with epilepsy .......32
3-2 Recommended energy intake: DRI versus ADA ketogenic therapy ...........................55
3-3 Triglyceride concentrations of individual patients on ketogenic therapy over time ..72
3-4 Triglyceride concentrations of individual patients at baseline and 1 to 3 months post-initiation of ketogenic therapy..................................................................................72
3-5 Total cholesterol concentrations of individual patients on ketogenic therapy over time...........................................................................................................................73
3-6 Total cholesterol concentrations of individual patients at baseline and 1 to 3 months post-initiation of ketogenic therapy..........................................................................73
3-7 LDL cholesterol concentrations of individual patients on ketogenic therapy over time74
3-8 LDL cholesterol concentrations of individual patients at baseline and 1 to 3 months post-initiation of ketogenic therapy..........................................................................74
3-9 HDL cholesterol concentrations of individual patients on ketogenic therapy over time...........................................................................................................................75
3-10 HDL cholesterol concentrations of individual patients at baseline and 1 to 3 months post-initiation of ketogenic therapy..........................................................................75
3-11 Non-HDL cholesterol concentrations of individual patients on ketogenic therapy over time...................................................................................................................76
3-12 Non-HDL cholesterol concentrations of individual patients at baseline and 1 to 3 months post-initiation of ketogenic therapy.............................................................76
3-13 Triglyceride concentrations of individual patients ...................................................77
3-14 Total cholesterol concentrations of individual patients............................................77
3-15 LDL cholesterol concentrations of individual patients.............................................78
3-16 HDL cholesterol concentrations of individual patients ............................................78

ix
3-17 Non-HDL cholesterol concentrations of individual patients....................................79

x
Abstract of Thesis Presented to the Graduate School
of the University of Florida in Partial Fulfillment of the Requirements for the Degree of Master of Science
GUIDELINES FOR INITIATING AND MONITORING KETOGENIC THERAPY FOR PATIENTS WITH EPILEPSY
By
Mandy Hammond Layman
December 2004
Chair: Peggy R. Borum Major Department: Food Science and Human Nutrition
Ketogenic therapy has proven to be an effective treatment for epilepsy. It was
developed to mimic fasting by providing fat as the primary energy source with minimal
carbohydrate intake. There is limited published research regarding how clinicians should
carry out specific aspects of ketogenic therapy. The purpose of this study was to prepare
evidence-based guidelines, called KetoGator (KG) Guidelines, for developing a course of
action for initiating and monitoring ketogenic therapy for patients who have epilepsy.
A search was performed on the Web of Science and PubMed for published research
articles containing the key phrase “ketogenic diet” from the year 1995 through July 2004.
Queries were developed, and published research articles were reviewed and evaluated.
An evidence grading system was used to rank the strength of the evidence presented in
each of the articles with regard to various aspects of ketogenic therapy in the treatment of
patients with epilepsy. There were 325 hits from the search, and 57 articles met the
inclusion criteria: publication date of 1995 or later, full-text article, human study, English

xi
language, and content addressing one or more of the topics covered in the KG guidelines.
Topics include patient selection, use of ketogenic therapy combined with other
treatments, initiation of ketogenic therapy, diet prescription at initiation and during fine-
tuning, and potential adverse effects to monitor. Data from these research studies were
used to prepare the KG Guidelines for each topic listed above.
A database has been designed and created to provide a mechanism for ongoing
development and evaluation of care. The database contains data from patients previously
and currently treated with ketogenic therapy at the University of Florida (UF) from 1995
through May 2004. Potential techniques for analyzing the database were described as an
example of how clinics can retrieve and use patient data to evaluate current practice.
The ultimate goal of this study was to move toward the standardization of care for
ketogenic therapy, which to our knowledge is something that has never been done. The
process used in this study included reviewing published research on clinical care
practices; retrieving data from medical and other records; compiling the data into a usable
database; analyzing the data to determine trends and outcomes; and formulating
recommendations with the goal of improving the overall consistency of initiating and
monitoring ketogenic therapy. The outcome of this process has resulted in the first
edition of the KG Guidelines, which are presented in this thesis.

1
CHAPTER 1 INTRODUCTION
Background
Searching for a cure for seizures dates back to Biblical times when fasting was
found to reduce the frequency of seizures. In the 1920’s the ketogenic diet was
developed to mimic fasting and the biochemical changes associated with starvation.
Ketogenic therapy advocates the use of fat as the primary energy source with minimal
carbohydrate intake. The total amount of fat and carbohydrate to be consumed is based
on a ratio of grams of fat to grams of carbohydrates plus grams of protein. With the
development of anti-epileptic drugs (AEDs), the use of ketogenic therapy decreased over
time. However, in the 1990’s there was a resurgence of interest in ketogenic therapy as a
means of treatment for the 20 to 30% of patients with epilepsy who do not respond to
AEDs.
Ketogenic therapy has been proven to be an effective treatment for epilepsy (1-9).
In fact, a survey used to document the long-term outcomes of ketogenic therapy proved
that it was effective in controlling seizures in children 3 to 6 years after initiation (4).
Yet, due to the dietary restrictions and the demands of weighing and measuring all foods,
it is typically not used as the first treatment option (10). Today, physicians typically
prescribe ketogenic therapy only after the patient has responded poorly to AEDs or if the
adverse effects associated with the medications are unacceptable to the patient and/or
parent.

2
The effectiveness of ketogenic therapy lies in its potential to reduce seizure
frequency and severity, reduce dosage or need for medications, and increase the attention
and alertness of patients. Studies have repeatedly shown that, in general, ketogenic
therapy is effective in reducing seizures in approximately 30 to 60% of patients (1-8). In
a study of 55 children suffering from epilepsy, ketogenic therapy was associated with
more than a 50% reduction in seizure frequency in 81% of the subjects, and none of the
subjects had an increase in seizure frequency (11).
Much of the available published research focuses on providing evidence that
ketogenic therapy is efficacious for patients with epilepsy. However, there is limited
published research regarding how clinicians should implement specific aspects of
ketogenic therapy, especially when dealing with the diet prescription. If evidence-based
standards of care were available and followed, except for things that must be managed on
an individual basis, it would improve the quality of care provided to patients, as well as
provide guidance to dietitians and other clinicians involved with the medical care of
individuals on ketogenic therapy.
Purpose
The purpose of this study was to develop evidence-based guidelines for initiating
and monitoring ketogenic therapy for patients who have epilepsy. The guidelines
developed as a result of this study are referred to as KetoGator (KG) Guidelines. The
intent of these guidelines is to provide the healthcare team with evidence-based
recommendations that can be used in conjunction with current practice and clinical
judgment in an attempt to optimize treatment outcomes. It is anticipated that the
healthcare team will refer to the KG Guidelines as they consider options for managing
patients with epilepsy.

3
An additional purpose of this study was to make recommendations for appropriate
measures to be taken by clinicians and future studies to be conducted in order to provide
data for establishing or supporting guidelines for which sufficient evidence is lacking. To
accomplish this, the basis of current practices used for treating patients on ketogenic
therapy is reviewed.
Each procedure listed in the KG Guidelines is supported by evidence from
published research studies. The following topics are addressed in the KG Guidelines:
• Patient selection
• Use of ketogenic therapy combined with other treatments
• Initiation of ketogenic therapy
• Diet prescription at initiation and during fine-tuning
• Potential adverse effects to monitor
An important aspect of the development of standards of care is the ongoing
evaluation of the safety and efficacy of these standards. To accomplish this, it is
recommended that data related to patient responses and outcomes to therapy be
documented systematically. Identifying the types and frequency of data to be collected
and establishing a database system that can be used to retrieve and analyze data are
important steps in this process. With this in mind, a database of patients previously and
currently treated with ketogenic therapy at the University of Florida (UF) from 1995
through May 2004 was designed and created. Potential techniques for analyzing the
database are described as an example of how clinics can retrieve and use patient data to
evaluate current practices.

4
CHAPTER 2 METHODS
A search was performed on the Web of Science and PubMed for published research
articles containing the key phrase “ketogenic diet” from the year 1995 through July 2004.
Three hundred twenty-five citations were identified. The inclusion criteria for selection
of articles to be used in establishing the KG Guidelines were publication date of 1995 or
later, full-text article, human study, English language, and content addresses one or more
of the topics to be covered in the KG guidelines. Topics included patient selection, use of
ketogenic therapy combined with other treatments, initiation of ketogenic therapy, diet
prescription at initiation and during fine-tuning, and potential adverse effects to monitor.
Of the 325 citations, 57 articles met the inclusion criteria.
Queries about initiation and monitoring of ketogenic therapy were developed, and
published research articles were reviewed and evaluated. An evidence grading system
(Table 2-1) was used to rank the strength of the evidence presented in each of the articles
with regard to various aspects of ketogenic therapy. An article received an “A” ranking if
it was conducted as a randomized, double blind, placebo controlled trial. A “B” ranking
was given if the study was a cohort or case-control study. A “C” ranking was given to
studies that were poorly controlled or uncontrolled (C1 for a systematic review and C2
for an individual study). A “D” ranking was given if the study was a case series or case
report. An “E” ranking was given if the study was based on expert consensus or clinical
experience. KG Guidelines were developed based on the literature review, and the level
of evidence for each guideline is indicated.

5
Table 2-1. Evidence Grading System* Level of Evidence Description A Randomized, double-blind, placebo controlled studies B Cohort or case-control studies C1 Systematic review of several poorly controlled or uncontrolled studies C2 Poorly controlled or uncontrolled studies D Case series or case reports E Expert consensus or clinical experience
* Each research article received a letter grade according to the level of evidence description.
A database containing information from patients previously and currently treated
with ketogenic therapy at the University of Florida (UF) from 1995 through May 2004
was designed and created. Institutional Review Board (IRB) approval was obtained prior
to using these data. Lab members who are students at UF previously had entered patient
data from medical records into Microsoft Excel files as part of continuing care for each
patient. The data for 73 patients were audited by the lab members to ensure all
information was present and accurate. The audited patient data were entered into a
database using Microsoft Access. Each patient was assigned a KetoGator identification
(KG ID) number so the patients only can be identified by a code.
There were 146 database parameters for each patient. The parameters were divided
into the following categories: demographics, blood lipids, complete blood count,
gastrointestinal (GI) issues, height and weight, beta-hydroxybutyrate,
alertness/development, metabolic panel, seizures, diet prescription, ketones and specific
gravity, antiepileptic drugs (AEDs) [17 types], medications excluding AEDs [68 types],
supplements [32 types], medication scores, and arm anthropometrics. See Appendix A
for a list of parameters for each category. Similar to the manner in which published
research articles were used to address queries about ketogenic therapy, queries were
developed specific to the database (Appendix B). Procedures also were developed to

6
explain the steps for combining different parameters to answer each query (Appendix B).
The database and the procedures for answering the queries were created to provide a
mechanism for ongoing development and evaluation of evidence-based standardized care.
Some of the queries could not be answered using the database because the
appropriate patient data were not available for entry into the database. For queries that
can be answered using existing data in the database, recommendations were made for
future database analysis. For queries that could not be answered due to the lack of data in
the database and the lack of data in the literature, recommendations were made including
appropriate measures that need to be taken by clinicians (i.e., documentation of particular
patient information) in order to adequately analyze the effects of ketogenic therapy for
each patient, and future studies regarding important issues not addressed in the reviewed
literature or in the database.

7
CHAPTER 3 DEVELOPMENT OF KETOGATOR (KG) GUIDELINES
The KetoGator (KG) Guidelines were developed based on an evaluation of
published research that met pre-established inclusion criteria and addressed topics such
as: patient selection, use of ketogenic therapy combined with other treatments, initiation
of ketogenic therapy, diet prescription at initiation and during fine-tuning, and potential
adverse effects to monitor. A system for organizing and analyzing information
addressing these topics was designed and created using data obtained from patients with
epilepsy who were treated with ketogenic therapy at UF from 1995 through May 2004.
Procedures for using the database to answer future queries (Appendix B) were created so
that the KG Guidelines can be expanded and revised as new data become available. For
situations in which insufficient data are available in the literature and database to address
a query, recommendations regarding the specific patient information to be documented
and analyzed were made. The evidence used for the development of the KG Guidelines
is discussed in detail in the following sections.
Patient Selection
Patient selection criteria for initiating ketogenic therapy are based on screening for
inborn errors of metabolism, patient age, and the effects of anti-epileptic drugs (AEDs)
on social skills and seizure control.
Inborn Errors of Metabolism
A patient must have a negative screen for fatty acid oxidation deficiency in order to
avoid complications from a high fat diet (12-14). Ketogenic therapy could be dangerous

8
for patients who have porphyria, pyruvate carboxylase deficiency, unrecognized carnitine
deficiency, defects in fatty acid oxidation, or mitochondrial disorders (12). Screening for
urine organic acids (13) and amino acids, serum amino acids, lactate, pyruvate, and
carnitine should be done prior to ketogenic therapy initiation (12,14). Screening prior to
initiation is necessary for determining if the patient may be at risk for metabolic
complications due to high fat consumption.
The database developed by the research team in the current study did not include
information that addressed the question of whether patients were screened for metabolic
disorders by measuring urinary organic acid and amino acid, serum amino acid, lactate,
pyruvate, and carnitine prior to initiation (Table 3-1). Based on the strength of the
evidence from the studies evaluated, screening for certain metabolic disorders should be
conducted prior to starting ketogenic therapy (Table 3-1). For this reason, it is
recommended that a policy be instituted identifying the types of disorders for which
screening should be conducted and where the results are to be documented (Table 3-1).
Age
It has been suggested that ketogenic therapy works best in children because of the
limited food selections of the diet (15,16). However, our working hypothesis (Appendix
C) is that it is effective in all age groups. The belief among some clinicians is that
ketogenic therapy is not an appropriate therapy for infants. Reasons cited for excluding
the use of ketogenic therapy with infants include the potential for adverse effects of the
diet (17) and the belief that ketosis is difficult to achieve and maintain and that infants are
susceptible to severe hypoglycemia (18). Evidence to the contrary was demonstrated in a
study by Klepper et al. Based on the tolerance to ketogenic therapy and seizure control,
Klepper et al. reportedly introduced ketogenic therapy to 4 infants under 1 year of age

9
safely and successfully (17). In fact, Nordli et al. found the effectiveness of controlling
seizures with ketogenic therapy in 32 infants to be similar to the rates reported in the
literature for older children (19). Klepper et al. reported on 2 patients with seizures and
hypoglycorrachia who were placed on ketogenic therapy. One patient began ketogenic
therapy at 4 weeks of age and discontinued it at 19 weeks of age; at 21 months of age, she
remained seizure-free and her neurodevelopment was entirely age appropriate. The other
patient began ketogenic therapy at 4 weeks of age and discontinued it at 2.2 years of age;
he remained seizure-free at 2.5 years of age and his muscle tone and development were
almost normal (20). Nordli and De Vivo stated, “Our own experience using the
ketogenic therapy in this age group has been quite favorable” (21:p.746). Ketogenic
therapy has been suggested as an early treatment in children with infantile spasms, and
the risk-benefit ratio for ketogenic therapy is favorable (22).
Table 3-1. Basis of KetoGator Guidelines. Patient Selection: Inborn Errors Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Is there a need for a negative screen of inborn errors?
Yes E (3) Is there documentation that screening for inborn errors has occurred?
No data available
What should be screened?
- Urinary organic acids and amino acids - Serum amino acids, lactate, pyruvate, and carnitine.
E (2) What should be screened?
No data available
Document the screening results of: - Urinary organic acids and amino acids - Serum amino acids, lactate, pyruvate, and carnitine.

10
Seizures are detrimental and may cause brain damage as early as infancy. Our
working hypothesis (Appendix C) is that ketogenic therapy may be a favorable treatment
for infants with epilepsy. Our database contains only 4 patients who were infants (<12
months old) at the time of initiation of ketogenic therapy, so there is not sufficient
information to analyze this age group (Table 3-2). Systematic investigation of the
effectiveness and safety of ketogenic therapy in infants less than 12 months old is
recommended (Table 3-2).
Research on the efficacy and compliance of adolescents with ketogenic therapy is
limited. Mady et al. conducted a retrospective study of 45 patients, ages 12 to19 years on
ketogenic therapy. Of the patients remaining on ketogenic therapy at 6 months (62%),
21% had a 50 to 90% seizure reduction and 29% had more than a 90% reduction. Of the
patients remaining on ketogenic therapy at 12 months (44%), 35% had a 50 to 90%
reduction and 30% had more than a 90% reduction. No evidence was found to support
the belief that ketogenic therapy was too restrictive or lacked efficacy for adolescents.
The authors suggest “family support and personal motivation are the primary factors in
achieving success on the diet” (7:p.850). They go on to say that ketogenic therapy should
be considered as an option for treating adolescents since it is not more restrictive and has
similar efficacy for this age group compared to younger children (7).
Adults with refractory epilepsy usually are not treated with ketogenic therapy.
Schwartz et al. studied the clinical effects of 3 different types of ketogenic therapies in 59
patients, 4 of whom were adults. They reported that evidence of the effectiveness of the
therapy was less encouraging in adults than in children, although a statistical analysis was
not possible because of the small sample size (23). The authors did not provide an

11
explanation for concluding that this therapy is less encouraging in adults. Maydell et al.
reported a trend of patients older than 12 years of age less frequently having ≥50%
reduction in seizures in comparison to the younger age group; however, the differences
were not significant (8). On the other hand, a study conducted with 11 adults (median
age of 32.2 years) on ketogenic therapy for 8 months reported a 50% seizure reduction in
6 subjects, no change in 2 subjects, and poor compliance in 2 subjects. The results for 1
subject were not reported. The authors concluded that persistent ketosis is possible in
adults and well-motivated adults can comply with the diet for long periods of time (24).
Fifty-six patients between the ages of 1 and 23 years (mean age of 10.4 years) were
started on ketogenic therapy. There were no statistically significant differences in
outcome related to age; however, poor compliance was slightly more prevalent in older
age groups (25). In a literature review, Freeman and Vining et al. reportedly showed no
significant difference in outcome related to age (26).
Although our working hypothesis (Appendix C) related to the use of ketogenic
therapy in adults with epilepsy is consistent with other researchers (27), there is
insufficient data in our database (4 adolescents; 2 adults) upon which to make any
conclusions at this time (Table 3-2). Future investigation in this area is warranted based
on the positive results achieved in the small number of subjects followed by other
research groups (Table 3-2).
Efficacy for All Age Groups
The measurement of the success of ketogenic therapy lies in the efficacy and
tolerance to ketogenic therapy and patient compliance. Efficacy is the ability of a therapy
to control or cure an illness (28) and includes improvement in seizures, a decrease in the
12
amount of medications prescribed, and improvement in alertness. Tolerance is the ability
of a patient to endure unusually large doses of a therapy (28). Compliance is the
willingness of a patient to follow a prescribed course of treatment (29). Efficacy,
tolerance, and compliance can often be subjective measurements. The database contains
no data on alertness or compliance, and therefore, cannot be analyzed. Database
information on seizures is limited to the number of seizures per week for each patient.
These data are insufficient to determine improvement or regression of seizures, since the
type, severity, and frequency of seizures must be taken into account.
Changes in medications, a measure of efficacy, can be analyzed using a parameter
called “medication score.” Medication scores have been proposed to quantitatively
measure the effects of AEDs, which may be used as a comparison tool among and within
patients. It is calculated by dividing the patient’s daily dose of a particular medication by
the recommended minimum daily dose for that patient’s age and body size [Daily dosage
÷ (recommended minimum daily dose × patient’s weight in kilograms)]. An individual
score is calculated for the amount of each medication the patient is taking, and the
individual scores are added together for the total medication score. By calculating and
recording medication scores, clinicians can determine whether or not an attempt to wean
the patient from a medication(s), one of the goals of ketogenic therapy, is occurring
successfully and if so, the rate at which the patient is being weaned. Medication scores
provide quantifiable data that can be documented and evaluated in conjunction with other
changes in ketogenic therapy.
Similar to the medication score, a seizure score has been proposed as an objective
measurement for efficacy. The proposed scoring system will take into account the

13
seizure type, severity, and frequency, information that is necessary for determining
seizure improvement or regression. The use of video-monitoring of seizure activity or
regular electroencephalograms (EEG) to test for changes in brain activity provide the
most objective data for seizure analysis.
Since the seizure score has not been put into practice yet, our database cannot be
analyzed for changes in seizures. An alertness score also has been proposed and may be
another beneficial objective measurement of efficacy in the future. The details for
determining alertness scores have not been developed yet.
In order to determine the efficacy of ketogenic therapy in each age group, it is
important to record the change in seizures, medications, and alertness. However, seizure
number and alertness are often recorded in a subjective manner, and the number of
medications a patient takes may not account for the increase or decrease in the total
dosage of the medications. This makes it difficult to provide evidence-based care. The
development and use of seizure scores may allow clinicians to objectively document
improvement or worsening of seizures by calculating the seizure score at each clinic visit
and each time there is a major change in seizures (Table 3-2). It also is important to
document the occurrences of illnesses or other stressors that may affect seizures.
Medication scores can be used as an objective measure for the increase or decrease in
total medications, specifically AEDs, by documenting the type and amount of
medications prescribed at each clinic visit and each time there is a major change in
medication type and/or dosage (Table 3-2). Once alertness scores have been developed,
clinicians may be able to better identify improvements in the patients’ behavior by

14
calculating and documenting alertness scores at each clinic visit and each time there is a
major change in alertness (Table 3-2).
Patient tolerance can be analyzed using our database, by determining whether or
not the patient suffered from gastrointestinal (GI) disturbances (i.e., vomiting, nausea,
diarrhea, constipation). In order to better document tolerance and compliance, forms
were developed for future use to determine how well the patient tolerates and complies
with ketogenic therapy during initiation (Appendix D). Three separate forms were
developed to evaluate tolerance. One can be used to document the following factors
about vomiting: number of times the patient vomits per hour, how long after the meal the
patient vomited, the estimated percent of the meal that was vomited, and the presence of
nausea with gagging or retching. A second form can be used to document the following
about diarrhea: number of times the patient has diarrhea per hour, the volume output,
consistency, color, and the presence of gas with or without pain/cramping. A third form
can be used to document the following about constipation: number of bowel movements
during initiation, consistency of the stool, color of the stool, and the presence of gas with
or without pain/cramping. The compliance form can be used to document the amount of
meal consumed as a percentage, a ranking of the refusal to eat food throughout the meal,
and the length of time in minutes to complete the meal; each measure is compared to the
patients’ normal eating habits before beginning ketogenic meals. After analysis of these
forms, it may be possible to suggest better guidelines for adjusting ketogenic therapy
during the initiation process.
By using the proposed seizure score, medication score, alertness score, tolerance
forms, and compliance form, the progress of each patient may be easier to track and may

15
provide a means for conducting studies related to the success of particular dietary
changes throughout ketogenic therapy. By documenting the above information in a
database for patients in every age group, comparisons can be made among different age
groups. This may help determine whether or not age is a contributing factor to success or
failure of ketogenic therapy (Table 3-2).
Effects of AEDs
AEDs may control seizures, but can have undesirable side effects, (i.e., loss of
personality; decreased social skills). In children, taking a large number of medications
was associated with a significantly diminished health-related quality of life (30). In fact,
one reason for initiating patients on ketogenic therapy is to wean them off of AEDs
because of the associated potential adverse effects. Many patients and/or caregivers are
disappointed to discover that after a patient has experienced failure with one AED, it is
highly probable all other AEDs will fail (2,13). If the use of AEDs does not control
seizures or has effects that are unacceptable to the patient and/or parent, ketogenic
therapy may be an appropriate choice for treating epilepsy. Since seizure scores have not
been implemented yet, our database does not include sufficient data for analyzing the
impact of changes in AEDs on the seizures (Table 3-3).
It is not surprising that the cost of treatment significantly decreases as AEDs are
weaned (31,32). Mandel et al. reported that for 15 patients treated with ketogenic
therapy, the total cost of treatment was $352,821 during the pre-initiation period, $41,223
during ketogenic therapy initiation, and $149,438 during the post-initiation period. Pre-
initiation costs were significantly higher than post-initiation costs (p=0.038). The authors
suggest that “as the cost of the pre-diet care increased, the cost-effectiveness of the

16
Table 3-2. Basis of KetoGator Guidelines. Patient Selection: Age Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Is there a change in seizure scores at different durations of ketogenic therapy for infants and young children (0 to 3 yrs)?
No seizure scores available
Is there a change in medications scores for AEDs at different durations of ketogenic therapy for infants and young children (0 to 3 yrs)?
Data available for future analysis (Appendix B)
Develop seizure scores (or something similar) and calculate and document at each clinic visit and each time there is a major change in seizures for all ages. Document occurrences of illnesses or other stressors that may affect seizures for all ages.
Is ketogenic therapy effective in infants?
Yes C2 D E
(2) (2) (1)
Is there a change in alertness scores for AEDs at different durations of ketogenic therapy for infants and young children (0 to 3 yrs)?
No alertness scores available
Monitor seizure activity with video-monitoring, EEGs, etc. for all ages.

17
Table 3-2. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Is ketogenic therapy safe to use in infants?
Yes C2 D E
(1) (2) (1)
No C2 D E
(3) (4) (2)
Should ketogenic therapy be discouraged in infants? Yes C1 (1)
How did infants and young children (0 to3 yrs) tolerate ketogenic therapy? How frequent did GI disturbances occur in those age groups?
Data available for future analysis (Appendix B)
Is there a change in seizure scores at different durations of ketogenic therapy for adolescents (14 to 18 yrs)?
No seizure scores available
Is there a change in medications scores for AEDs at different durations of ketogenic therapy for adolescents (14 to 18 yrs)?
Insufficient data available for adolescents
Is ketogenic therapy effective for adolescents?
Yes C2 (1)
Is there a change in alertness scores for AEDs at different durations of ketogenic therapy for adolescents (14 to 18 yrs)?
No alertness scores available
Calculate medication scores and document at each clinic visit and each time there is a major change in medication dosage for all ages.

18
Table 3-2. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Is ketogenic therapy safe to use in adolescents?
Yes C2 (1)
Should ketogenic therapy be discouraged in adolescents?
No C2 (1)
How did adolescents (14 to 18 yrs) tolerate ketogenic therapy? How frequent did GI disturbances occur for that age group?
Insufficient data available for adolescents
Is there a change in seizure scores at different durations of ketogenic therapy for adults (≥19 yrs)?
No seizure scores available
Is there a change in medications scores for AEDs at different durations of ketogenic therapy for adults (≥19 yrs)?
Insufficient data available for adults
Is ketogenic therapy effective for adults?
Yes C1 C2
(1) (2)
Is there a change in alertness scores for AEDs at different durations of ketogenic therapy for adults (≥19 yrs)?
No alertness scores available
Develop alertness scores (or something similar) and calculate and document at each clinic visit and each time there is a major change in alertness for all ages.

19
Table 3-2. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Is ketogenic therapy safe to use in adults?
No evidence that it is unsafe.
-- How did adults (≥19 yrs) tolerate ketogenic therapy? How frequent did GI disturbances occur for that age group?
Insufficient data available for adults
Fill out tolerance forms at initiation for all ages.
Should ketogenic therapy be discouraged in adults?
No C1 C2 E
(1) (2) (1)
What is the correlation between compliance and age?
No data available
Fill out compliance forms at initiation for all ages.

20
ketogenic diet also increased” (31:p.397). Gilbert et al. reports that the daily medication
costs after diet initiation can be reduced by 70% (32).
Efficacy, tolerance, and compliance to ketogenic therapy may be affected by
treatment with AEDs. Because some AEDs show a stronger negative interaction with
ketogenic therapy, it may be important to wean patients from those particular AEDs
before they are weaned from others. The database can be analyzed to identify the order
in which AEDs were weaned by comparing the individual medication scores and
identifying which decreased first (Table 3-3).
The order in which AEDs are weaned, including the medication score, needs to be
documented in the medical record and entered into the database. It also would be
interesting to look at the results of starting a patient on ketogenic therapy before other
treatments (i.e., AEDs) are prescribed. A study could be conducted to determine the
efficacy, tolerance, and compliance of ketogenic therapy when administered as the first
line of treatment compared to those patients who started AEDs prior to ketogenic therapy
(Table 3-3).
Use of Ketogenic Therapy Combined with Other Treatments
The University of Florida Pediatric Comprehensive Epilepsy Center uses ketogenic
therapy, AEDs, surgery, and the vagus nerve stimulator (VNS) to treat patients with
epilepsy. Since all four treatments are used regularly, it is valuable to understand
potential interactions with ketogenic therapy.
AEDs
Research suggests that valproic acid (VPA), a type of AED, should not be given in
combination with ketogenic therapy (18,33). Ballaban-Gil reported a study of 52

21
Table 3-3. Basis of KetoGator Guidelines. Patient Selection: Effects of AEDs Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Which AEDs were taken and what was the medication score for each AED prior to initiation of ketogenic therapy?
No data available
Calculate medication scores prior to initiation and document.
Which AEDs were taken and what was the medication score for each AED taken at different durations of ketogenic therapy?
Data available for future analysis (Appendix B)
Document each AED that is taken. Calculate medication scores of each AED and document at each clinic visit and each time there is a major change in the type of AED and the dosage.
What evidence supports: Use ketogenic therapy ONLY IF seizures are uncontrolled by AEDs, or use ketogenic therapy AFTER unacceptable side effects from AEDs?
No evidence --
What were the seizure scores at different durations of ketogenic therapy?
No seizure scores available
Develop seizure scores (or something similar) and calculate and document at each clinic visit and each time there is a major change in seizures. Document occurrences of illnesses or other stressors that may affect seizures.

22
Table 3-3. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
How many patients started ketogenic therapy without previous use of AEDs?
0 Conduct a study to determine the efficacy, tolerance, and compliance of ketogenic therapy when administered as the first line of treatment compared to those patients started on AEDs prior to ketogenic therapy.
Can ketogenic therapy be used before trials of medications and/or surgeries?
No evidence --
How many patients started ketogenic therapy without previous use of surgery?
No data available
Conduct a study to determine the efficacy, tolerance, and compliance of KT when administered as the first line of treatment compared to patients who had surgery prior to ketogenic therapy.

23
Table 3-3. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
What is the order in which AEDs were weaned? What is the order in which the medication score for each AED decreased?
Data available for future analysis (Appendix B)
Is the order of weaning from AEDs important for efficacy, tolerance, compliance, and safety of ketogenic therapy?
No evidence --
What is the change in efficacy, tolerance, and compliance with the weaning of each AED?
No data available
Document the order in which AEDs are weaned, including the medication score.
What is the importance of weaning AEDs?
A large number of medications have been associated with a significantly diminished health-related quality of life in children.
B (1) N/A N/A N/A
24
children on the classic 4:1 ketogenic therapy. Four out of 5 (80%) children who
experienced adverse effects were taking VPA in addition to ketogenic therapy. When
VPA was discontinued from their treatment, the adverse effects resolved in 3 of the
children in a matter of a few weeks (33). Tallian et al. stated that VPA reportedly
interferes with the production of ketone bodies, which serve as an alternative energy
source to the brain (18). The adverse effects listed in our database are limited, so adverse
effects potentially caused by VPA could not be analyzed (Table 3-4).
There have been reports of increased risk of kidney stones when ketogenic therapy
is used in combination with carbonic anhydrase inhibitors, a type of AED that includes
drugs such as topiramate (TPM), zonisamide (ZNS), and acetazolamide (AZM) (34,35).
Carbonic anhydrase inhibitors decrease serum bicarbonate, which may result in metabolic
acidosis (34). Patients on ketogenic therapy are predisposed to metabolic acidosis due to
their ketotic state, and the mixture with carbonic anhydrase inhibitors carries the potential
risk for severe secondary metabolic acidosis and nephrolithiasis (34,36). Wilner reported
that using TPM and ketogenic therapy in combination may increase the risk of metabolic
acidosis. Additionally, if water intake is restricted as part of the treatment, the water
restriction and acidosis may increase the incidence of nephrolithiasis (35). However,
Kossoff et al. reported that the combination of ketogenic therapy and TPM or ZNS used
in 80 patients did not increase the risk of kidney stones (36). They recommended
increasing fluid intake to 100% of daily needs and using urine alkalinizing agents (i.e.,
potassium citrate, sodium citrate, sodium bicarbonate) to help prevent kidney stone
formation (36). Takeoka et al. reviewed the medical charts of 14 children co-treated with
TPM and ketogenic therapy, and TPM was reported to possibly cause metabolic acidosis

25
during initiation of ketogenic therapy. The authors report that the co-treatment of TPM
and ketogenic therapy may lead to better efficacy, and weaning TPM before ketogenic
therapy initiation carries a risk of increasing seizure activity. They concluded that the
two treatments can be used together with careful monitoring of serum bicarbonate
concentrations, but the risks must be assessed in each case (34).
Our working hypothesis (Appendix C) is that one carbonic anhydrase inhibitor can
be given in addition to ketogenic therapy as long as adequate fluids are consumed. There
is no record of any patients taking AZM, nor is there any record of kidney stones or the
amount of fluid consumed/prescribed for each patient in our database. Therefore, the
database could not be analyzed for the potential relationship between carbonic anhydrase
inhibitors and kidney stones (Table 3-4).
Phenobarbital is another AED for which adverse effects have been reported in the
literature when used in combination with ketogenic therapy. Tallian et al. reported that
drowsiness and in some cases encephalopathy may develop when phenobarbital is
administered in conjunction with ketogenic therapy. The underlying cause of this
response is thought to be related to the acidotic state produced by ketogenic therapy,
which enhances the uptake of phenobarbital by the brain (18). There is no record of
encephalopathy in our database, and the lack of alertness scores prevents any type of
analysis of this interaction at this time (Table 3-4). This warrants further research on the
effects of the combination treatment of phenobarbital and ketogenic therapy.
More research is needed to understand the potential adverse reactions that can
occur due to the interaction of ketogenic therapy and AEDs, specifically VPA, carbonic
anhydrase inhibitors, and phenobarbital. In order to study this, the following data need to

26
be documented in the medical record and entered into the database: medication scores for
VPA, carbonic anhydrase inhibitors, and phenobarbital at each clinic visit and each time
there is a change in dosage, adverse effects experienced with each of those medications,
the occurrence of kidney stones along with the medication scores for each of the carbonic
anhydrase inhibitors and the amount of fluid consumed, and the occurrence of
encephalopathy along with the medication scores for phenobarbital (Table 3-4).
VNS and Surgery
The vagus nerve stimulator, or VNS, is a generator surgically implanted into the
chest. The physician programs it to give a prescribed dose of electrical stimulation.
Additional stimulation can be self-administered by swiping a magnet over the generator
(37). Surgery is another therapy used for seizure management. Surgery is performed on
the region of the brain where there is an electrochemical abnormality.
Using ketogenic therapy in combination with VNS and/or brain surgery may affect
the success of the treatment. There are no published data related to the use of VNS and
ketogenic therapy as co-treatments or on the effectiveness of using ketogenic therapy for
patients treated with brain surgery. There is no data in our database to evaluate the
number of patients who received VNS and ketogenic therapy in combination or the
number of patients who received brain surgery prior to or during ketogenic therapy.
Therefore, the effect of combined treatments on seizure control cannot be determined at
this time (Tables 3-5 and 3-6).
It would be interesting to explore the idea of using ketogenic therapy with VNS
and/or surgery. On a related issue, it may be beneficial to take precautions for patients
undergoing any type of surgery while on ketogenic therapy. McNeely suggests using
“Anaesthetic Guidelines for Paediatric Patients on the Ketogenic Diet” in order to avoid

27
Table 3-4. Basis of KetoGator Guidelines. Use of Combined Treatments: AEDs Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Calculate medication score of VPA and document at each clinic visit and each time there is a change in VPA dosage.
Can VPA and ketogenic therapy be safely used in combination?
No C1 C2
(1) (1)
How many patients who used VPA experienced adverse effects?
Limited data available
Document the adverse effects experienced while on VPA.
How many of those that used TPM experienced kidney stones?
No data available
Yes. It is recommended to give fluid as estimated maintenance needs and to use urine alkalinization to avoid kidney stones.
C2 (1)
How many of those that used ZNS experienced kidney stones?
No data available
Can carbonic anhydrase inhibitors and ketogenic therapy be safely used in combination?
Yes. Close monitoring of serum bicarbonate is recommended.
C2 (1) How many of those that used AZM experienced kidney stones?
No data available
Document the occurrence of kidney stones. Identify the medication score of TPM, ZNS, and AZM when kidney stones were developed.

28
Table 3-4. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
It may decrease serum bicarbonate and increase the risk of metabolic acidosis. (Acidosis and fluid restriction may increase the risk of kidney stones.)
C2 D
(2) (1)
What was the amount of fluid consumed/prescribed for those taking TPM, ZNS, and AZM?
No data available
Document the fluid prescription and consumption at each clinic visit and each time there is a major change in fluid prescription and consumption. Identify the fluid prescription and consumption while taking TPM, ZNS, or AZM.
What other AEDs are discouraged from being used in combination with ketogenic therapy?
Phenobarbital in combination with ketogenic therapy may increase serum phenobarbital and may cause drowsiness and/or encephalopathy.
C1 (1) How many of those that used phenobarbital experienced encephalopathy?
No data available
Document the occurrence of encephalopathy. Identify the medication score of phenobarbital when encephalopathy is experienced.
29
Table 3-4. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
How many patients that took AEDs (other than VPA, carbonic anhydrase inhibitors, and phenobarbital) experienced adverse effects?
Limited data available
Document the adverse effects experienced. Calculate medications scores of all AEDs taken and document at each clinic visit and each time there is a change in AED dosage.

30
Table 3-5. Basis of KetoGator Guidelines. Use of Combined Treatments: VNS Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
How many patients had VNS and were on the ketogenic therapy in combination?
No data available
Document the date the VNS was placed.
Identify the efficacy (seizure score, medication score, and alertness score) of ketogenic therapy prior to VNS placement and compare to the efficacy of ketogenic therapy after VNS placement.
What are the results of using VNS and ketogenic therapy in combination?
No evidence --
How did the combination of VNS and ketogenic therapy affect seizure control?
No data available
Conduct a study using the flow chart in figure 3-1 to determine if co-treatment of ketogenic therapy and VNS is appropriate.
disrupting ketogenic therapy during any type of surgery (38). A study could be
conducted to determine the effectiveness of ketogenic therapy and VNS as a combination
treatment. Comparisons of efficacy (using seizure scores, medication scores, and
alertness scores) could be made for individuals on ketogenic therapy prior to VNS
placement to those receiving ketogenic therapy after VNS placement (Table 3-5). Figure

31
3-1 depicts a potential algorithm for choosing the appropriate treatment for epilepsy that
includes circumstances under which VNS and/or brain surgery may be applied. It also
shows how clinicians can use the process of elimination to determine the most
appropriate type of treatment for their patients. It may be beneficial to identify the results
of using combined treatments of AEDs, surgery, or VNS with ketogenic therapy.
Table 3-6. Basis of KetoGator Guidelines. Use of Combined Treatments: Surgery Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for
Database
Database Assessment
Future Documentation/ Studies Needed
Document the date and the type of surgery performed on the brain.
How many patients had surgery and were on the ketogenic therapy?
No data available
What is the effectiveness of using ketogenic therapy for patients previously treated with brain surgery?
No evidence --
How did the use of brain surgery during ketogenic therapy affect seizure control?
No data available
Conduct a study using the flow chart in Figure 3-1 to determine if use of ketogenic therapy is appropriate after surgery.
Should special precautions be taken in order to perform surgery on a patient on ketogenic therapy?
Refer to McNeely’s “Anaesthetic Guidelines for Paediatric Patients on the Ketogenic Diet.”
D/ E
(1) N/A N/A N/A

32
Figure 3-1. Algorithm for choosing the appropriate treatment(s) for patients with sy
Start KT
Success Failure
KT only Add VNS
Success Failure
Wean KT Add surge
Success Failure Success Failure
VNS only KT and VNS Discontinue Increase other treatments
Success Failure
Wean KT
Success Failure
No KT, no VNS KT and new AEDs
Add VNS, wean KT
Success Failure
VNS only KT, VNS, and new AEDs
AEDs fail
AEDs: antiepileptic drugs, KT: ketogenic therapy, VNS: erve stimulator
epilep
ry
VNS
Vagus n

33
Appropriate levels of each treatment could be prescribed to provide a suitable treatment
for seizures.
Initiation
The initiation process of ketogenic therapy includes the schedule protocol, the issue
of fasting, establishment of laboratory values that need to be monitored, and patient
and/or parent education.
Schedule Protocol
Although many clinics use similar procedures for initiating ketogenic therapy, there
is no consensus protocol. Initiation is traditionally scheduled as a 5-day process. Patients
are fasted in the hospital for two days, start consuming ketogenic meals at 1/3 the caloric
prescription on the third day, receive 2/3 the caloric prescription on the fourth day, and
increase to the full caloric prescription on the fifth day (39). Table 3-7 outlines the 5-day
protocol currently used at the Johns Hopkins Medical Institute (40). UF, as well as other
clinics, currently uses a 3- to 4-day schedule in order to reduce the hospital stay (41).
Table 3-8 outlines the protocol used at Shands Hospital at the University of Florida (41).
Patients are fasted overnight before admission, start ketogenic meals at 1/3 the caloric
prescription on the day of admission, and increase to full caloric prescription on the
second or third day as tolerated by the patient.
Orally fed patients typically do not consume any other foods while ketogenic meals
are increased at initiation. Conversely, patients fed with enteral tube feedings and bottle
fed infants typically are not deprived of energy during initiation. One-third of the
ketogenic formula and two-thirds of the normal formula and are mixed together on the
first day of initiation. The ketogenic formula is gradually increased to full strength by the

34
Table 3-7. Ketogenic Diet Protocol at Johns Hopkins Hospital Day before admission Low carbohydrate consumption for 24 h. Children examined in clinic the afternoon before admission. Fasting starts in the evening.
Day 1 Admitted to the hospital. Fasting continues. Fluids restricted to 60 to 70 ml/kg. Blood glucose monitored every 6 h. Use carbohydrate-free drugs. Parents begin educational program.
Day 2 Dinner given as one third of calculated diet meal as “eggnog”. Blood glucose checks discontinued after dinner. Parents begin to check urine ketones periodically.
Day 3 Breakfast and lunch given as one third of diet. Dinner increased to two-thirds (still eggnog). Education program completed.
Day 4 Breakfast and lunch given as two-thirds of diet allowance. Dinner is first full ketogenic meal (not eggnog).
Day 5 Full ketogenic diet breakfast given. Prescription reviewed and follow-up arranged. Child discharged to home. Taken from Kossoff, E. H. More fat and fewer seizures: dietary therapies for epilepsy (2004) The Lancet Neurology 3:415-420. third day while the normal formula is reduced by equal volume (14). This raises the
question of the importance of restricting energy for any patient at initiation.
In fact, Wirrell et al. used an initiation protocol that excluded the traditional energy
restriction. Fourteen children were started on ketogenic therapy without a fast.
Ketogenic therapy was initiated as a 1:1 ratio of fat to carbohydrates plus protein and
advanced to a 3:1 or 4:1 ratio over 3 to 4 days. Thirteen of the 14 patients were
successfully initiated on ketogenic therapy, with 1 developing vomiting and food refusal
after ketosis was established. The authors concluded that good ketosis can be established

35
Table 3-8. Ketogenic Diet Protocol at the University of Florida Pre-Admission • Dietitian will assess patient, review hospitalization, and determine admission date. • Dietitian will give family fluid and carbohydrate restriction guidelines for day prior to
admission. • Dietitian or practitioner will review admission plans so that patient/family are prepared for
admission with lab slip of serum lab work, complete medication evaluation, gram scale, ketogenic diet book, and required groceries.
• Obtain height and weight. • Tests/labs: EEG, lipid panel, comprehensive metabolic panel, magnesium, phosphorous, beta-
hydroxybutyrate, uric acid, ALT, AED levels, complete blood count. • Neurologist will assess seizure frequency, intensity, duration, type, etc.
Day 1 • Admitted to the hospital. • Maintain fluid/volume restriction. • Complete nutritional assessment, including diet history and anthropometric measurements by
dietitian. • Begin diet at 1/3 total calories once patient reaches 160 ketones in urine. • If the patient has been on home care, contact the agency. • Education: meal preparation instruction, how to check urine for ketones and specific gravity,
and how to monitor daily input and output. • Assessment: check urine ketones and specific gravity every void and blood glucose every 6
hours. • Specific gravity should remain between 1.015 and 1.025; blood glucose should remain ≥50.
Day 2 • If patient has tolerated 2 meals then advance as directed by dietitian. (If diet has not been
initiated, begin at 1/3 total calories once patient reaches 160 ketones in urine or fasts for 48 hours.)
• Maintain fluid restriction. • Family receives prescription for calcium carbonate and Multistix 9 SG. • Education: meal preparation instruction, ketogenic therapy for home, symptoms of excessive
ketosis, hypoglycemia, and dehydration, and how to check all labels for carbohydrate content. • Assessment: Check urine ketones and specific gravity every void, blood glucose every 6 hours
or three times daily if patient on diet x 24 hours, and weight in the morning after void. • Specific gravity should remain between 1.015 and 1.025; blood glucose should remain ≥50.
Day 3 • If patient has tolerated at least 2 meals then advanced as directed by dietitian. • Caregiver will complete nutrition discharge quiz. • Make arrangements with home care if indicated. • If patient is tolerating full calorie diet x 2 meals, then discharge. • Maintain fluid restriction. • Obtain AED levels and electrolytes, if indicated. • Assessment: Check urine ketones and specific gravity three times daily, blood glucose, and
weight in morning after void. • Specific gravity should remain between 1.015 and 1.025; blood glucose should remain ≥50;
ketosis should remain between 80 and 160 (reading on multistix).

36
Table 3-8. Continued Day 4 (If necessary) • Advance diet as directed by dietitian. • Review nutrition discharge quiz. • Dietitian will remain in frequent contact with family. • Discharge family home with gram scale and Multistix 9 SG. • Family will need copies of their written meal plans, formula prescription if appropriate,
prescription for CaCO3 and Multistix 9 SG. • Return to clinic in the outpatient setting in 3 to 4 weeks as scheduled by dietitian. • Monitor patient’s ketosis (multistix reading should be 80 to 160). • Maintain fluid restriction. • Assessment: Check urine ketones and specific gravity twice daily, blood glucose (must be ≥50
to be discharged), and weight in morning after void. • Specific gravity should remain between 1.015 and 1.025; blood glucose should remain ≥50;
ketosis should remain between 80 and 160 (reading on multistix).
Post-Discharge • Dietitian will meet with family and assess diet tolerance and anthropometric measurments at
follow-up visits. • Dietitian will remain in frequent contact with the family. • Neurologist will see patient and assess seizure history and/or medication adjustment/wean. Taken from Ketogenic Treatment Program/Intractable Epilepsy Clinical Pathway. Shands Children’s Hospital at the University of Florida, 1999. with this protocol, and the mean time (58 hours) for achieving good ketosis is comparable
to the traditional protocol (42).
Unfortunately, no available protocols specific to adjusting the dietary aspect of
ketogenic therapy were found in the research studies reviewed. MacCracken and Scalisi
stated, “Lack of diet standardization and method for evaluation of diet efficacy makes the
decision to implement this diet therapy problematic for dietetics practitioners”
(43:p.1554). The American Dietetic Association’s (ADA) Pediatric Manual for Clinical
Dietetics discusses the basic nutrition care for patients on ketogenic therapy (44).
However, no discussion is provided on problem-solving for things such as an appropriate
ratio to recommend if the patient experiences problems or how many calories should be
added or deleted from the diet prescription when a child experiences growth, lack of
growth, weight loss, or weight gain. The American Academy of Pediatrics has at least 70

37
contributors to the nutrition recommendations made for infants, children, and
adolescents. A detailed background about ketogenic therapy is discussed, but specific
information is lacking similar to the ADA manual (45). Even The Florida Dietetic
Association Diet Manual notes that “information on the calculation of the ketogenic diet
is beyond the scope of this discussion” (46:p.K14.2). The reader is referred to The
Epilepsy Diet Treatment: An Introduction to the Ketogenic Diet, 2nd ed., a book written
by Freeman, Kelly, and Freeman, which introduces ketogenic therapy to clinicians as
well as to patients and parents/caregivers. Thus, it appears that there are very few
references available to dietitians and other clinicians that provide details about initiating
and adjusting ketogenic diets.
Different initiation protocols are used among ketogenic therapy clinics, including
outpatient. There does not appear to be a standardized protocol for initiating ketogenic
therapy. Schedule protocols and the outcomes of treatment at different clinics (inpatient
and outpatient) need to be compared to each other in order to develop a standardized
evidence-based protocol. A study could be conducted that compares the protocols of
ketogenic therapy initiation at different clinics and the outcomes of efficacy, tolerance,
and compliance (Table 3-9).
Fasting
There is no evidence to support the schedule protocols described in Tables 3-7 and
3-8. In fact, there is no evidence to support fasting as a necessary step in initiating
ketogenic therapy. It has been thought that a fast is needed to bring the patient into a
state of ketosis before starting ketogenic therapy. However, Wirrell et al. reported that 17
children initiated on ketogenic therapy achieved ketosis without fasting (42). Fasting,

38
Table 3-9. Basis of KetoGator Guidelines. Initiation: Schedule Protocol Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
Initial fast until ketosis is induced, then provide ketogenic meals as 1/3 of caloric prescription. Increase by thirds until full caloric prescription is reached.
C2 E
(1) (2)
What initiation protocols are currently used by different clinics?
Provide ketogenic meals at full caloric prescription. Start with a 1:1 ratio and increase ratio until full ratio prescription is reached.
C2 (1)
N/A N/A Conduct a study that compares the protocols of ketogenic therapy initiation at different clinics. Compare the outcomes of ketogenic therapy at those different clinics.

39
Table 3-9. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
How many patients were initiated as in-patient?
No data available
How many patients were initiated as out-patient?
No data available
What are the pros and cons of in-patient vs. out-patient?
Financially, initiation as inpatient tends to have higher reimbursement rates for the hospital than initiation as outpatient.
C2 (1)
What was the efficacy, tolerance, and compliance of those initiated as in-patient versus those initiated as out-patient.
No data available
Document the efficacy (seizure scores, medication scores, and alertness scores), tolerance, and compliance of each patient initiated in-patient and out-patient. Compare the efficacy, tolerance, and compliance of ketogenic therapy among patients that are initiated as in-patient verses out-patient.
What is the traditional initiation protocol (increase caloric prescription by thirds over 3 days) based on?
No evidence -- N/A N/A Run a study that compares different initiation protocols. For example, compare an initiation protocol that increases the calories of ketogenic therapy by thirds verses a protocol that gradually increases the ratio of ketogenic therapy to the prescribed ratio.

40
perhaps, places added stress on patients, especially children, and may increase the risk for
vomiting, making it more difficult to introduce ketogenic meals. Avoiding a fast may be
beneficial by decreasing psychological stress on the patient and family, decreasing the
risk of hypoglycemia, and decreasing the hospital stay and cost (42). Only a few patients
treated at UF were initiated on ketogenic therapy without a fast, so database queries could
not be analyzed (Table 3-10).
Our working hypothesis (Appendix C) is that the length of time between the last
meal eaten and the first ketogenic meal eaten affects tolerance and compliance.
However, this hypothesis cannot be tested using our current database because the data
needed for analysis were not recorded. Initiation without a fast needs to be investigated
more thoroughly. A study could be conducted that compares the efficacy, tolerance, and
compliance of patients initiated with a fast versus patients initiated without a fast (Table
3-10). Another working hypothesis (Appendix C) is that the length of time between the
last meal consumed and the first ketogenic meal consumed affects tolerance and
compliance. A study could be conducted that compares the efficacy, tolerance, and
compliance of patients fasted for varying amounts of time prior to initiation of ketogenic
therapy (Table 3-10).
In order to test this, a newly created diet prescription form (Appendix E) can be
used in conjunction with the tolerance and compliance forms (Appendix D) to track
patient initiation progress. The diet prescription form was developed to document the
time of the patient’s last pre-treatment meal, the time of the first ketogenic meal actually
received, and changes in calories, ratio, and fluids throughout the initiation process.
Evaluating these data could provide information that could lead to the development of an

41
Table 3-10. Basis of KetoGator Guidelines. Initiation: Fasting Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Database Assessment
Future Documentation/ Studies Needed
How many patients fasted prior to ketogenic meal?
No data available
How many patients were not fasted prior to ketogenic meal?
No data available
Is a fast necessary? No C2 (1)
What are the pros of fasting?
No evidence --
What are the cons of fasting?
1) Fasting can put a child at high risk for hypoglycemia, 2) parents find the concept of fasting their child very difficult psychologically, and 3) avoidance of a fast may decrease hospitalization time and the cost.
C2 (1)
Of those who fasted, how did their results compare to those who did not fast?
No data available
Conduct a study that compares the efficacy, tolerance, and compliance of patients initiated with a fast versus patients initiated without a fast.

42
Table 3-10. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database Answers from
Database
Future Documentation/ Studies Needed
Is a certain length of time too long for patients/children/ infants to fast?
No evidence -- What time was the last pre-treatment meal eaten? What time was the first ketogenic meal actually eaten?
No data available
Conduct a study that compares the efficacy, tolerance, and compliance of patients fasted for different durations at initiation. Fill out the die prescription form.

43
evidence-based ketogenic therapy initiation protocol associated with the most favorable
outcomes and limited adverse effects (Table 3-10).
Laboratory Values
Laboratory (lab) values are checked during the initiation process and at most clinic
visits throughout ketogenic therapy. It is important to establish which values are
necessary to monitor and how frequently. Baseline lab values should be collected to use
as a reference point for the patient’s nutrition and neurological evaluations (14). The labs
that are normally checked at initiation and follow-up clinic visits at UF include but are
not limited to blood lipid concentrations, complete blood count, serum beta-
hydroxybutyrate concentrations, metabolic panel, urinary ketone bodies, and urinary
specific gravity (41). A complete list of labs is found in Table 3-11. In addition, it has
been recommended that urinary excretion of calcium and uric acid be monitored (47).
Urinary ketone bodies and urinary specific gravity are checked by the patient’s caregiver
on a regular basis between clinic visits (41). One study suggests monitoring serum beta-
hydroxybutyrate concentrations on a regular basis similarly to how a person with diabetes
checks his/her blood glucose concentrations (48). This suggestion requires further
investigation to determine the cost-effectiveness and impact on outcomes achieved from
this type of testing.
Published research does not focus on the frequency that certain lab values should
be monitored. No information is provided for determining which lab tests are most
useful in adjusting treatment to improve outcomes. It may be beneficial to analyze the
database to identify which lab values are tested more often and which ones tend to be
abnormal during ketogenic therapy (Table 3-12). The labs monitored at initiation and at
each clinic visit need to be documented in the medical record and entered into the

44
Table 3-11. Suggested lab values* Lab Value Category Lab Value Blood Lipids Triglycerides (TG) High Density Lipoprotein (HDL) Low Density Lipoprotein (LDL) Total/HDL Cholesterol Total Cholesterol Complete Blood Count Red Blood Cell (RBC) Count Hemoglobin (Hgb) Hematocrit (Hct) Platelet Count Mean Cell Volume (MCV) Mean Cell Hemoglobin (MCH) Mean Cell Hemoglobin Concentration (MCHC) Mean Platelet Volume (MPV) Red Blood Cell Distribution (RBC Dist) White Blood Count (WBC) Beta-Hydroxybutyrate Serum Beta-Hydroxybutyrate Metabolic Panel Sodium (Na) Potassium (K+) Chloride (Cl-) Carbon Dioxide (CO2) Blood Urea Nitrogen (BUN) Creatinine Glucose (Glu) Calcium (Ca+2) Magnesium (Mg+2) Inorganic Phosphate (PO4) Uric Acid Total Protein Albumin Bilirubin Total Bilirubin Direct Alkaline Phosphatase Aspartate Aminotransferase (AST) Alanine Transaminase (ALT) Lactate Dehydrogenase (LDH) Total Urinary Ketones and Specific Gravity
Ketone Body Level (Ketones)
Specific Gravity *Suggested lab values to be monitored at initiation and follow-up clinic visits. database. It is obvious that any lab values that are repeatedly abnormal require regular
monitoring, and clinicians should work toward correcting those lab values. On the other

45
hand, if a particular lab value never seems to be abnormal, it may not be necessary to
continue monitoring it (Table 3-12).
Table 3-12. Basis of KetoGator Guidelines. Initiation: Lab Values Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for
Database
Database Assessment
Future Documentation/ Studies Needed
*Serum lipid concentrations
C2E
(1) (1)
*Complete blood count
E (1)
*Serum beta- hydroxybutyrate
C2E
(1) (1)
*Metabolic Panel
E (1)
*Urinary ketone bodies
E (1)
*Urinary specific gravity
E (1)
Which labs are tested and appear to be abnormal at initiation?
Data available for future analysis (Appendix B)
Document which labs are monitored during initiation. Identify the labs that are abnormal at initiation.
Urinary excretion of calcium
C2 (1)
Which lab values should be monitored during initiation and at follow-up clinic visits?
Uric acid C2 (1) Urinary ketones and specific gravity
E (1) Which labs should be monitored between follow-up clinic visits?
Serum beta- hydroxy- butyrate
C2 (1)
Which labs are tested and appear to be abnormal at different durations of ketogenic therapy?
Data available for future analysis (Appendix B)
Document which labs are monitored during ketogenic therapy at each clinic visit. Identify which ones are regularly abnormal at clinic visits.
*See Table 3-11 for complete list of labs. Patient/Parent Education
The patient and/or parent are typically educated on calculating, measuring, and
preparing ketogenic meals during the initiation process. There are no official lesson
plans for educating the patient and/or parent. A questionnaire conducted with
patients/caregivers and health care providers found that patients/caregivers view their
educational needs differently than health care providers, and tailored educational

46
programs are needed to accommodate the specific characteristics of the patient (49). It
appears that many patients/parents participate in ketogenic therapy listservs, suggesting
that there is a need for more caregiver education.
Meeting with the patient and parent/caregiver prior to initiation is important.
Things to consider discussing in a pre-ketogenic diet session include the process of food
preparation and food weighing, information about purchasing a scale that weighs in
tenths of a gram, a description of meals and beverages that will be eaten, requirements for
the omission of carbohydrate-rich foods, appropriate foods and nutritional supplements,
the required follow-up appointments, the possible adverse effects, the expected length of
ketogenic therapy, and alternative foods to enjoy at holidays and major events (14). This
session may aid in the success of the diet.
A 3-year trial using a protocol for patient care was developed by a team of inpatient
and outpatient registered dietitians (RD). Before patients were hospitalized, orally fed
patients met with the outpatient RD twice and tube fed patients met once. The focus of
the preadmission appointments included nutrition assessment, overview of the ketogenic
therapy, calculation methods, and discussions of goals and expectations. During
initiation, the inpatient RD focused on reinforcing the principles introduced before
admission, strategies for problem solving, and facilitating accuracy and creativity in
menu development. All participating parents/caregivers (n=13) received a survey, and 11
of them completed and returned the survey (85% return rate). On a scale of 1 to 5, the
average ranking of diet efficacy was 4.4, compliance was 3.8, and program evaluation
was 4.5. Limitations associated with this survey include that it was based on the
caregivers’ impression of the patients’ improvement. In addition, it is unclear at which

47
point during ketogenic therapy (i.e., immediately following initiation, 1 month after
initiation, 6 months after initiation, etc.) these surveys were distributed and returned,
which may have affected the results. Nonetheless, meeting with the families of patients
prior to hospital admission may be an efficient way of educating caregivers about
ketogenic therapy (43). Several individuals, including family members, teachers, and
pharmacists, play a role in the success of ketogenic therapy for each patient. It is
important to educate each individual about ketogenic therapy and the importance of
complying with the patients’ strict carbohydrate intake. Small amounts of carbohydrates
provided through meals, snacks, medications, toothpaste, etc. could disrupt the patients’
ketogenic therapy regimen and possibly lead to break out seizures. Properly educating
these individuals may help to avoid such disruptions and perpetuate seizure control.
The patient and/or parent are typically educated on calculating, measuring, and
preparing ketogenic meals during the initiation process. There are no set lesson plans for
educating the patient and/or parent. Studies designed and conducted to determine the
type of training sessions that are most useful to the patients/caregivers and yield the best
results in terms of adherence and acceptability would provide valuable information
(Table 3-13). The establishment of good take-home material could be useful for
caregivers.
In order to make suggestions for consistency of the education process, a
patient/parent education evaluation form (Appendix F) that lists everything patients
and/or parents need to know before leaving the hospital was developed to determine how
well the patient and/or parent feels they understand each aspect of ketogenic therapy.
Specifically, the patient/parent will be asked to rank their understanding of each

48
technique (i.e., calculations, measurements) using a scale of 1 to 4 (1 = Not comfortable
doing this on my own; 2 = Feel somewhat comfortable doing this on my own but still
need hands-on help; 3 = Feel mostly comfortable doing this on my own but still need
verbal help; 4 = Feel completely comfortable doing this on my own). If a 1, 2, or 3 is
ranked for any technique, the patient and/or parent will be asked to specify where they
need assistance so appropriate follow-up assistance can be provided. A member of the
healthcare team should record the patient’s and/or parent’s responses on the evaluation
form. The dietitian may use this as a tool for determining if the patient/parent needs
more education. Thorough education may increase compliance, and the proposed
Patient/Parent Education Evaluation Form may aid in that success (Table 3-13).
Diet Prescription at Initiation and During Fine-Tuning
The diet prescription is based on ratio of fat to carbohydrates plus protein, calories,
fluid allowance, protein, and number of meals and snacks. Protein and the number of
meals and snacks are not discussed because there is little published research that focuses
on the protein content of the diet or on the number of meals and snacks that could impact
the success of the diet. More research focusing on these factors could provide
information that would assist clinicians with clinical decisions regarding the diet
prescription.
Ratio
Ketogenic therapy uses a ratio based on grams of fat to grams of carbohydrates plus
grams of protein [grams of fat:(grams of carbohydrates + grams of protein)]. It originally
was based on the ketogenic/anti-ketogenic potential of the diet, as calculated by (90% fat
+ 46% protein)/(100% carbohydrates + 10% fat + 58% protein) (18). This ratio was
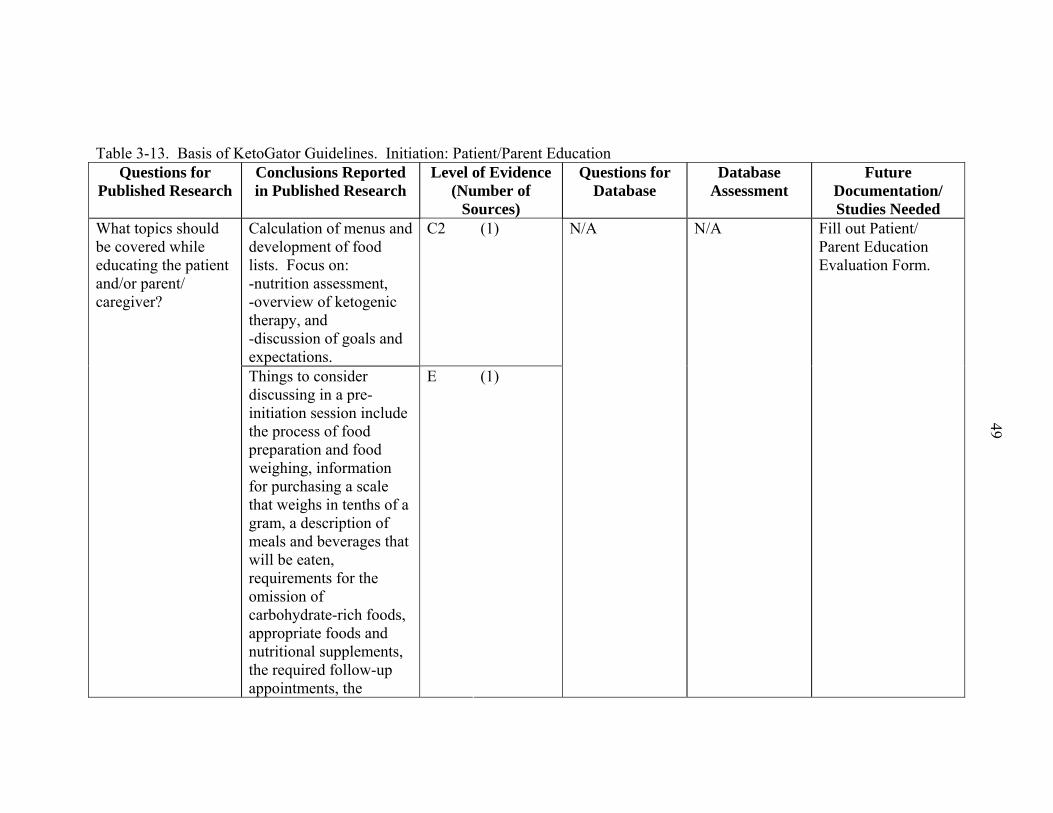
49
Table 3-13. Basis of KetoGator Guidelines. Initiation: Patient/Parent Education Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence (Number of
Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Calculation of menus and development of food lists. Focus on: -nutrition assessment, -overview of ketogenic therapy, and -discussion of goals and expectations.
C2 (1) What topics should be covered while educating the patient and/or parent/ caregiver?
Things to consider discussing in a pre-initiation session include the process of food preparation and food weighing, information for purchasing a scale that weighs in tenths of a gram, a description of meals and beverages that will be eaten, requirements for the omission of carbohydrate-rich foods, appropriate foods and nutritional supplements, the required follow-up appointments, the
E (1)
N/A N/A Fill out Patient/ Parent Education Evaluation Form.
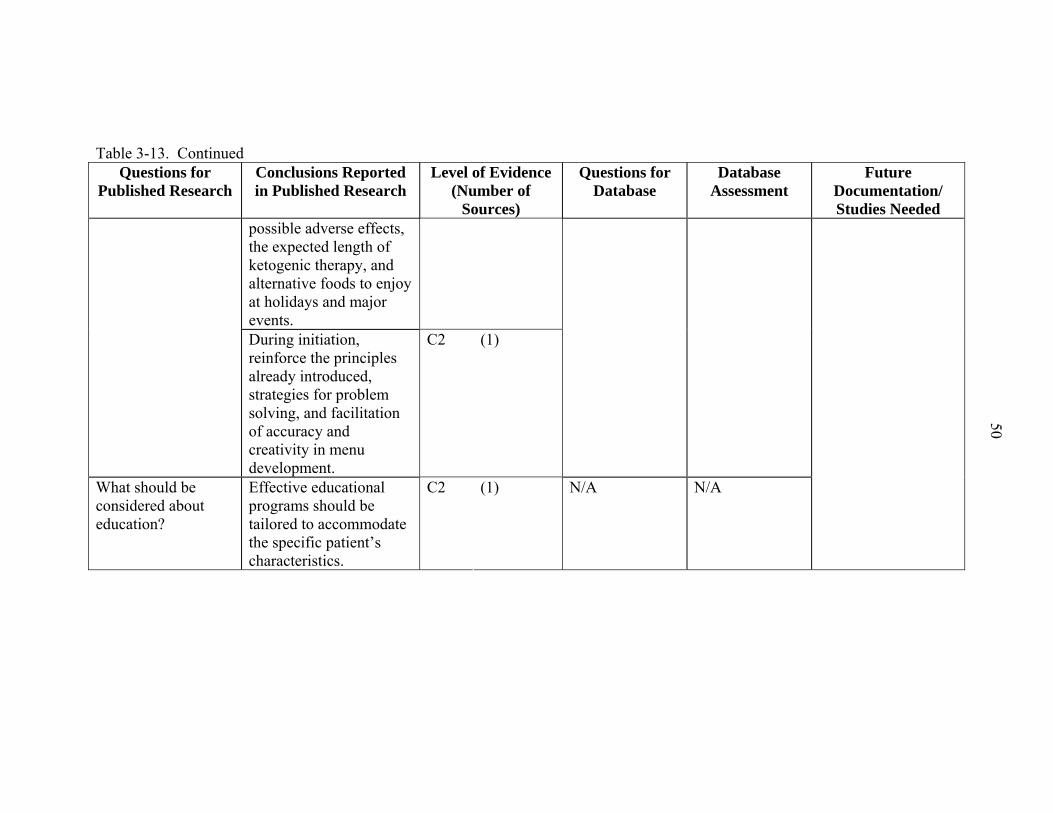
50
Table 3-13. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence (Number of
Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
possible adverse effects, the expected length of ketogenic therapy, and alternative foods to enjoy at holidays and major events.
During initiation, reinforce the principles already introduced, strategies for problem solving, and facilitation of accuracy and creativity in menu development.
C2 (1)
What should be considered about education?
Effective educational programs should be tailored to accommodate the specific patient’s characteristics.
C2 (1) N/A N/A

51
based on the idea that 90% of fat and 46% of protein contribute to the formation of
ketone bodies (i.e., ketogenic effect), and 100% of carbohydrates, 10% of fat, and 58% of
protein contribute to the formation of glucose (i.e., anti-ketogenic effect). Some amino
acids produce ketone bodies as well as glucose, so there is a slight overlap in the
ketogenic/anti-ketogenic effect of protein.
Traditionally, ketogenic therapy is given at a ratio of 3:1 or 4:1 at initiation, and
adjustments are made to the ratio according to seizure control and palatability/compliance
to the diet. Unfortunately, the ratio at initiation and the appropriate adjustments are
estimated, and there is no evidence on which to base an appropriate ratio for each patient.
Initiation ratios have been suggested by Zupec-Kania et al. (Table 3-14).
Table 3-14. Recommended Age-Based Initiation Ratios (Fat: Protein + Carbohydrate) for Ketogenic Therapy
Age Ratio ≤ 18 months 3:1
19 months to 12 years 4:1
> 12 years 3:1
Obesity 3:1
Taken from Zupec-Kania, B., Werner, R. R. & Zupanc, M. L. (2004) Clinical Use of the Ketogenic Diet: The Dietitian's Role. In: Epilepsy and the Ketogenic Diet (Stafstrom, C. E. & Rho, J. M., eds.), pp. 63-81. Humana Press, Totowa, New Jersey.
Ketogenic therapy generally provides 80% of calories from fat, 15% from protein,
and 5% from carbohydrates (3.5:1 ratio). In contrast, the Atkins diet provides 60% of
calories from fat, 30% from protein, and 10% from carbohydrates (2:1 ratio). In a study
designed to evaluate the use of the Atkins diet instead of the traditional ketogenic therapy
as a treatment for seizures, six patients, ages 7 to 52 years, were enrolled on the induction
phase (<10 grams carbohydrates per day) of the Atkins diet as an open trial over a 2-year
period. The calorie prescriptions were not reported. Of the three cases presented in

52
detail, two of the patients became seizure-free and one had a reduction in seizures. The
authors concluded that the Atkins diet should not be used as a substitute for ketogenic
therapy but that additional research is warranted to determine if the restrictions of
calories traditionally imposed by ketogenic therapy are necessary (50). In a review of
this study, Kossoff recommended that diet therapy for the treatment of epilepsy should be
given only if both a neurologist and dietitian monitor the patients closely due to potential
risks of dyslipidemia, renal stones, etc. (40).
Our database contains data that can be analyzed to identify the changes in ratio
prescription that occurred from initiation throughout ketogenic therapy (Table 3-15).
Additional research is needed to determine an appropriate ratio to prescribe at initiation
and throughout the fine-tuning process. The data that need to be documented in the
medical record and entered into the database include the starting ratio prescription and
the reason for prescribing that ratio (i.e., ratio is in agreement with the Zupec-Kania et al.
recommendations) and the ratio each time it is changed and the reason for the change
(i.e., poor seizure control, weight gain) (Table 3-15). Comparisons can be made among
patients and clinics to determine what changes in ratio prescription aid in the success of
ketogenic therapy.
Calories
In the 2002 Dietary Reference Intake (DRI) report, the Institute of Medicine (IOM)
recommends appropriate calorie intake using the Estimated Energy Requirement (EER).
The EER “represents the average dietary energy intake that will maintain energy balance
in a healthy person of a given gender, age, weight, height, and physical activity level”
(51:p.93). Table 3-16 shows the EER for all ages.

53
Table 3-15. Basis of KetoGator Guidelines. Diet Prescription: Ratio Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for
Database
Database Assessment
Future Documentation/ Studies Needed
What is the starting ratio dependent on?
No evidence -- N/A N/A Document the starting ratio prescription. Document reason for prescribing that ratio (i.e., ratio is in accordance to Zupec-Kania et al. recommenda-tions).
What is the appropriate ratio to prescribe?
No evidence -- What was the ratio prescript-ion at different durations of ketogenic therapy?
Data available for future analysis (Appendix B)
Document each time the ratio is changed. Document the reason for the change (i.e., poor seizure control, weight gain).
Ketogenic therapy was originally developed to provide calories at 75% of the RDA.
Table 3-17 shows the American Dietetic Association’s (ADA) guidelines for calculating
energy needs of patients on ketogenic therapy. The ADA also advise adjusting the
energy intake to achieve modified growth goals, which are not defined (44). Figure 3-2
compares the DRI for energy to the ADA’s recommended energy intake for ketogenic
therapy.
Couch et al. reported that approximately 75 kilocalories per kilogram of body
weight per day (kcal/kg/d) is an adequate amount of energy for children after finding
normal growth in children on ketogenic therapy for 6 months (52). Some references

54
Table 3-16. Estimated Energy Requirement (EER) Related to Age and Gender
Age (years) Reference
BMI, kg/m2
Reference height, cm
(in)
Reference weight, kg
(lb)
Energy (EER),
kcal/day Energy,
kcal/kg/day Males 0-0.5 - 62 (24) 6 (13) 570 95 0.5-1 - 71 (28) 9 (20) 743 82.6 1-2 - 86 (34) 12 (27) 1046 87.2 3-8 15.3 115 (45) 20 (44) 1742 87.1 9-13 17.2 144 (57) 36 (79) 2279 63.3 14-18 20.5 174 (68) 61 (134) 3152 51.7 19-30 22.5 177 (70) 70 (154) 3067a 43.8 >31 3067 a Females 0-0.5 - 62 (24) 6 (13) 520 63 0.5-1 - 71 (28) 9 (20) 676 75.1 1-2 - 86 (34) 12 (27) 992 82.7 3-8 15 115 (45) 20 (44) 1642 82.1 9-13 17.4 144 (57) 37 (81) 2071 56 14-18 20.4 163 (64) 54 (119) 2369 43.9 19-30 21.5 163 (64) 57 (126) 2403b 42.2 >31 2403 b Pregnancy 1st trimester +0 2nd trimester +340 3rd trimester +452 Lactation 1st 6 months +330 2nd 6 months +400 a For males, subtract 10 calories per day for each year of age above 19. b For females, subtract 7 calories per day for each year of age above 19. Taken from Food and Nutrition Board. (2002) Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Institute of Medicine, National Academy of Sciences, Washington, DC. Table 3-17. Guidelines for Calculating Energy Needs for Patients on Ketogenic Therapy
Age (years) Calories/kg/day 0-1 90-100
1-1.5 75-80 1.5-3 70-75 3-6 65-68
7-10 55-60 11-18 30-40 >18 20-30
Taken from Nevin-Folino, N., ed. (1998) The American Dietetic Association Pediatric Manual for Clinical Dietetics. The American Dietetic Association, Chicago.

55
suggest that caloric restriction is important because weight gain on the diet often
correlates with lack of seizure control; in such cases, caloric restriction often improves
control (53). Dietary restriction to promote weight loss is often used by Mady et al. for
adolescent patients. The rationale is that the patients need to be as near to his or her ideal
body weight as possible in order to mimic starvation effectively (7). No studies were
found to support this reasoning or to further test the mechanism of weight gain or obesity
in reducing seizure control.
Recommended Energy Intake: DRI vs. ADA Ketogenic Therapy
0102030405060708090
100
0 1 1.5 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Age (years)
Kca
ls/k
g/da
y
DRI ADA Ketogenic Therapy
DRI: Dietary Reference Intake, ADA: American Dietetic Association, kcals: kilocalories, kg: kilograms
Figure 3-2. Recommended energy intake: DRI versus ADA ketogenic therapy
Contrary to those beliefs, Vining et al. suggested that an energy restriction may not
be necessary, based on the fact that a continuous decline in height z-score was found in
children on ketogenic therapy for 2 years. Patients received 25 to 116 kcal/kg/d with an
average of 64 kcal/kg/d (54). In fact, Kossoff et al. calculated energy as basal metabolic

56
needs plus activity for 23 patients on ketogenic therapy and found improvement in
seizure control and growth (22). Nordli said, “We know of no methodologically sound
studies that demonstrate the need for dehydration or severe calorie restriction when the
ketogenic diet is started” (21:p.746).
It has been suggested that the thermic effect of a high-fat diet is higher than a high-
carbohydrate diet; therefore, the energy level of ketogenic therapy can be lowered to be
80 to 90% of the DRI (14). However, there is no evidence to support this. In addition,
the factors affecting energy expenditure should be taken into account, for example,
immobility (low energy expenditure) or muscle spasticity (increased energy expenditure)
(14).
Our database can be used to identify how much of an energy restriction the patients
were prescribed at initiation and throughout ketogenic therapy compared to the DRI
standards. It also can be used to compare the calorie prescriptions according to weight
(Table 3-18).
Research is needed to determine the energy intake (restricted or unrestricted) that
should be prescribed at initiation of ketogenic therapy and throughout the fine-tuning
process. A study could be conducted comparing patients receiving 100% of the DRI for
energy versus patients receiving <100% of the DRI (i.e., 90-99%, 80-89%, and 70-79%
of the DRI) for energy. The data that need to be documented in the medical record and
entered into the database include the patients’ growth and development patterns, the
starting energy prescription (including kcals/kg/d) and the rationale for the level of
energy intake prescribed, and each time the calorie prescription is changed and the reason
for the change (i.e., weight gain, weight loss, growth, hunger) (Table 3-18). Comparisons
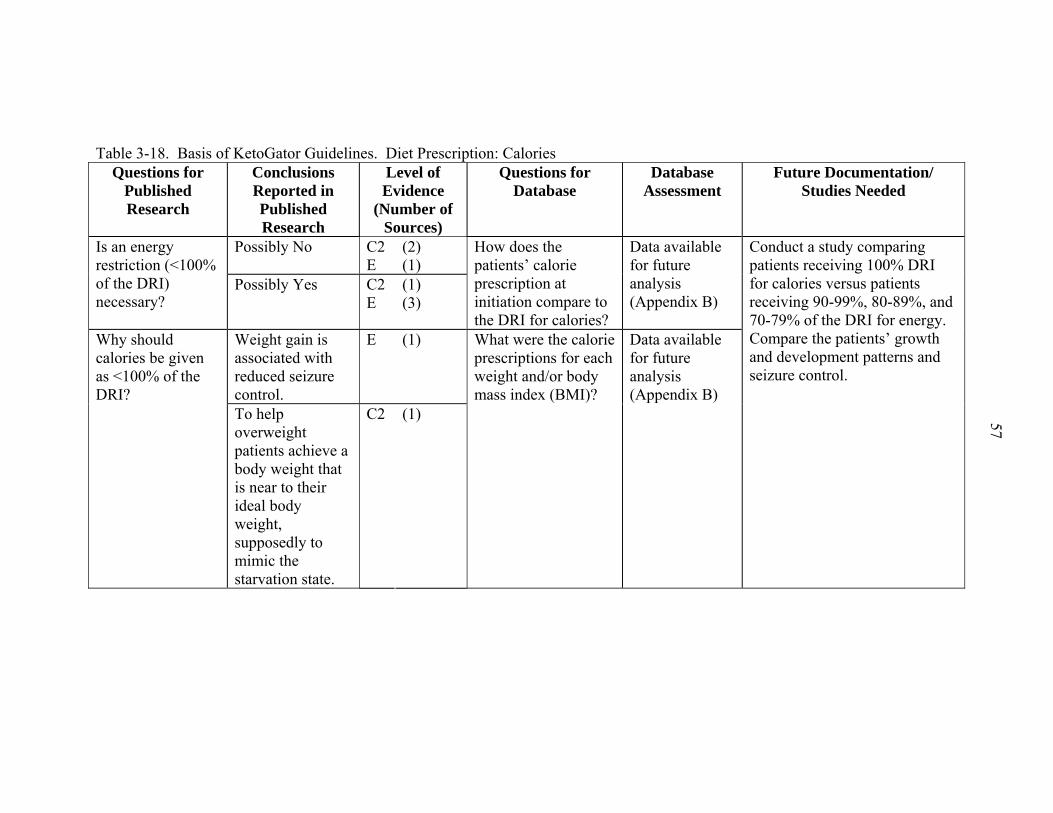
57
Table 3-18. Basis of KetoGator Guidelines. Diet Prescription: Calories Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Possibly No C2 E
(2) (1)
Is an energy restriction (<100% of the DRI) necessary?
Possibly Yes C2 E
(1) (3)
How does the patients’ calorie prescription at initiation compare to the DRI for calories?
Data available for future analysis (Appendix B)
Weight gain is associated with reduced seizure control.
E (1) Why should calories be given as <100% of the DRI?
To help overweight patients achieve a body weight that is near to their ideal body weight, supposedly to mimic the starvation state.
C2 (1)
What were the calorie prescriptions for each weight and/or body mass index (BMI)?
Data available for future analysis (Appendix B)
Conduct a study comparing patients receiving 100% DRI for calories versus patients receiving 90-99%, 80-89%, and 70-79% of the DRI for energy. Compare the patients’ growth and development patterns and seizure control.

58
Table 3-18. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
What is the appropriate energy intake for patients on ketogenic therapy?
Approximately 75 kcal/kg/d is adequate for a significant increase in height and weight for 6 months on ketogenic therapy.
C2 (1) What was the energy prescription at initiation and throughout ketogenic therapy?
Data available for future analysis (Appendix B)
Document the starting calorie prescription (including kcals/kg/d). Document rationale for prescribing that amount of calories.
What are the criteria for adjusting the energy prescription?
No evidence -- N/A N/A Document each time the calorie prescription is changed. Document the reason for the change (i.e., weight gain, weight loss, growth, hunger).

59
can be made among patients and clinics to determine what changes in calorie prescription
aid in the success of ketogenic therapy.
Fluids
Traditionally, ketogenic therapy includes a fluid prescription. Fluids are
traditionally given at 80% of maintenance for healthy, active children (27). Fluid
recommendations are typically set at 60 milliliters per kilogram of body weight, or 1
milliliter per calorie of the diet prescription (27). However, some report that the role of
dehydration in seizure control is uncertain, and there may, in fact, be no relationship
between the two (18,27). As mentioned previously, Nordli went on to say, “We know of
no methodologically sound studies that demonstrate the need for dehydration or severe
calorie restriction when the ketogenic diet is started” (21:p.746).
Furth et al. recommended that fluid intake should be maximized since ketosis may
alter the normal thirst mechanism causing an unintentional decrease in fluid intake (55).
After a team of dietitians tested their protocol for patients on ketogenic therapy, they
decided to discontinue the mild restriction of fluid intake since it appeared to offer no
benefits (43). A recent recommendation with regard to fluid intake is to base it on
maintenance needs (Table 3-19); however, a large volume of fluid at one time is not
recommended because “this may upset internal fluid balance and ketosis” (14:p.73). In
addition, “a fluid ‘schedule’ should be outlined with reasonable quantities of calorie-free,
caffeine-free fluids to be consumed daily based on the child’s maintenance fluid goals”
(14:p.75). In 1998, Freeman and Vining said, “The necessity of fluid restriction has not
been tested” (53:p.450), which is still true today. There are no data available in the
database regarding the amount of fluids consumed or prescribed, so the effects fluid
consumption cannot be analyzed at this time (Table 3-20).

60
Table 3-19. Holiday-Segar Method for Determining Maintenance Fluid Needs Body Weight Water (mL/kg/d) 1st 10 kg 100
2nd 10 kg 50
Each additional kilogram 20
Taken from Zupec-Kania, B., Werner, R. R. & Zupanc, M. L. (2004) Clinical Use of the Ketogenic Diet: The Dietitian's Role. In: Epilepsy and the Ketogenic Diet (Stafstrom, C. E. & Rho, J. M., eds.), pp. 63-81. Humana Press, Totowa, New Jersey.
It has become apparent that restricting the fluid intake of patients on ketogenic
therapy has become unpopular (Table 3-20). Adequate fluids must be consumed to avoid
complications such as kidney stone formation. To compare the effects of restricted and
unrestricted fluid consumption, a study could be conducted comparing patients receiving
100% DRI for fluids, or unrestricted fluids, versus patients receiving <100% DRI for
fluids. The data that need to be documented in the medical record and entered into the
database include the starting fluid prescription and the reason for prescribing that amount
of fluid (i.e., amount is in agreement with the Holiday-Segar recommendations), the
amount of fluid actually consumed by the patient with comparisons to the DRI, and each
time the fluid prescription changes and the reason for the change (i.e., poor seizure
control, kidney stone formation) (Table 3-20).
The diet prescription is one of the most crucial aspects of ketogenic therapy. There
is a lack of standardization of the ratio, energy, fluid, protein, and the number of snacks
and meals prescribed at initiation of ketogenic therapy and during fine-tuning. Even after
this thorough literature review, many questions are left unanswered. Clinicians would
benefit from knowing which factors require an adjustment to the diet prescription and by
how much. The diet prescription is frequently adjusted when the patient experiences
weight loss or gain, delayed growth, delayed development, lack of maintaining ketosis,

61
Table 3-20. Basis of KetoGator Guidelines. Diet Prescription: Fluids Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Do fluids need to be restricted?
No B C2 E
(1) (1) (3)
N/A N/A
What are the results of prescribing 100% of the DRI for fluids or allowing unrestricted fluids?
No evidence -- What are the results of prescribing 100% of the DRI for fluids or allowing unrestricted fluids?
No data available
Does the amount of fluid given affect ketosis and/or seizure control?
Uncertain relationship between dehydration and ketogenic therapy
C1 (1) Does the amount of fluid given affect ketosis and/or seizure control?
No data available
What are the dangers of restricting fluids?
Risk for hypercalcuria and kidney stones
B (1) What are the dangers of restricting fluids?
No data available
Conduct a study comparing patients receiving 100% of the DRI for fluids or unrestricted fluids versus patients receiving <100% of the DRI for fluids. Document the efficacy, tolerance (including all adverse effects), and compliance.
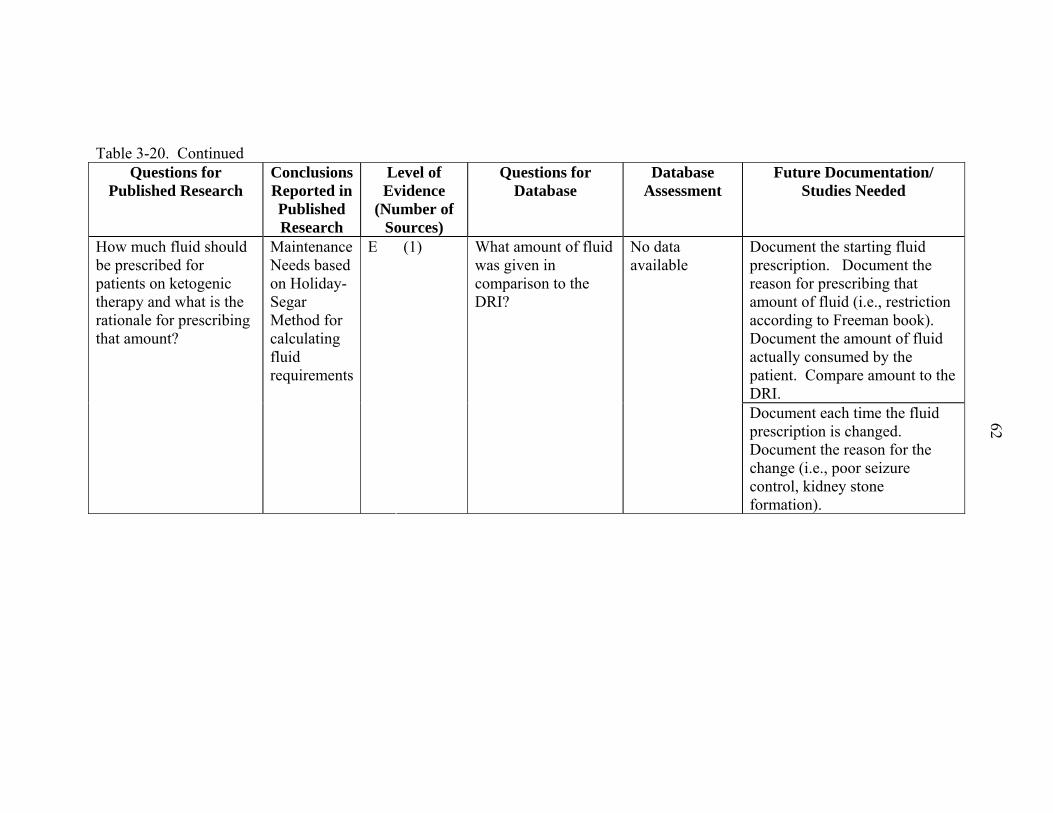
62
Table 3-20. Continued Questions for
Published Research Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Document the starting fluid prescription. Document the reason for prescribing that amount of fluid (i.e., restriction according to Freeman book). Document the amount of fluid actually consumed by the patient. Compare amount to the DRI.
How much fluid should be prescribed for patients on ketogenic therapy and what is the rationale for prescribing that amount?
Maintenance Needs based on Holiday-Segar Method for calculating fluid requirements
E (1) What amount of fluid was given in comparison to the DRI?
No data available
Document each time the fluid prescription is changed. Document the reason for the change (i.e., poor seizure control, kidney stone formation).

63
unpalatability of the ketogenic therapy, and/or changes in seizure frequency and/or
severity (56). It needs to be determined whether or not those factors require an
adjustment to ketogenic therapy for individual patients and what adjustments need to be
made (Table 3-21).
The RD often adjusts the diet prescription based on his/her expertise without the
use of a set protocol. Fine-tuning ketogenic therapy should be a joint effort among the
ketogenic team (14). Recommendations have been made to make only one change at a
time in the diet prescription or medications, and that any change should be tried for at
least 6 weeks before making another change (14). No studies were identified that tested
fine-tuning methods or reported evidence of successful ways of adjusting the therapy
according to the patient’s needs (Table 3-21). The limited amount of documentation on
fine-tuning the diet prescription demonstrates the need for the establishment of guidelines
for the dietary component of ketogenic therapy.
Monitoring Potential Adverse Effects
Growth and Development
It has been reported that growth of children for whom ketogenic therapy is
prescribed is different from normal growth (57). In a 2-year study of 237 children aged 2
months to 9 years 10 months, patients on ketogenic therapy grew well for the first six
months compared with the national average, with only a small drop in z-scores.
However, there was a continuous decline in height z-scores among all groups by the 2-
year mark. Some children lost up to 2 z-scores for height and weight by the end of the
study. The children received a range of 25 to 116 kcal/kg/d with an average of 64
kcal/kg/d, and the authors raise the question of whether or not an energy restriction is
necessary (54). Mady et al. reported 2 out of 45 adolescent patients experienced stunted

64
Table 3-21. Basis of KetoGator Guidelines. Diet Prescription Questions
for Published Research
Conclusions Reported in Published Research
Level of Evidence (Number
of Sources)
Questions for
Database
Database Assessment
Future Documentation/ Studies Needed
Do the following factors require an adjustment to ketogenic therapy for individual patients, and what adjustments should be made according-ly? Weight gain, weight loss, delayed growth, delayed develop-ment, lack of maintaining ketosis, unpalata-bility of the diet.
No evidence - See Tables 3-15, 3-18, and 3-20.
See Tables 3-15, 3-18, and 3-20.
Document each time the diet prescription is changed. Document the reason for the change (i.e., weight gain, weight loss, reduction in seizure control).
growth while on a diet prescription to maintain ideal body weight (7). In a retrospective
chart review of 21 patients aged 1 to 16 years, 18 (86%) patients were reported to have a
decline in height percentiles while receiving ketogenic therapy for 2 years. The calorie
prescription was not reported; however, protein prescription ranged from 0.52 to 1.2
grams per kilogram of actual body weight (g/kg), with a median of 0.95 g/kg. It may be
safe to assume that the patients with restricted protein prescriptions may also have

65
received restricted calorie prescriptions. The authors raise the question of how energy
and protein intake may affect growth of children on ketogenic therapy (57).
There have been several reports of normal growth in children while on the
ketogenic therapy. Couch et al. reported adequate linear growth of children on ketogenic
therapy for 6 months while providing energy as 75 kcal/kg/day. They found that “mean
percentile height, weight, and standard weight for height [standards for linear growth
derived from National Center for Health Statistics percentiles] were similar before the
diet and at 6 months” (52:p.1574). Kossoff et al. reported that there was an appropriate
average increase in height for 23 children on ketogenic therapy for an average duration of
1.6 years. Calorie prescriptions were calculated as basal metabolic needs plus activity
(22). Wheless recommended that if a child is experiencing poor growth while on the
ketogenic therapy, the albumin and total protein should be checked and height should be
monitored (12). Research is needed to determine how the diet prescription influences
seizure control as well as growth of infants, children, and adolescents on ketogenic
therapy.
Studies imply that there may be a correlation between growth and diet prescription
of patients on ketogenic therapy. Two studies reporting normal growth were 6 months
long. One study restricted energy (52) and the other provided maintenance energy (22).
It is concluded that 6 months may not be long enough to determine the rate at which
children grow on ketogenic therapy and if/how energy prescription affects growth. Two
studies reporting delayed growth were 2 years long. Energy and/or protein were
restricted for some patients in each study (54,57). These longer studies suggest that a
dietary restriction may cause delayed growth. It has not been established whether or not

66
dietary restriction or a lower body weight increases seizure control. If no relationship is
found, energy does not need to be restricted in patients on ketogenic therapy. If a
relationship is found, the benefits of seizure control may outweigh the risks of abnormal
growth. Clinicians are given the responsibility of providing the best care possible to the
patients, and in doing so, clinicians should strive to achieve normal growth in children on
ketogenic therapy. However, if future studies find normal growth to be unrealistic for
patients on ketogenic therapy, the cause for abnormal growth needs to be determined.
Our working hypothesis (Appendix C) is that fine-tuning ketogenic therapy
positively or negatively affects growth of children. Our database can be used to
determine if there is a correlation between changes in the patients’ energy prescription
and height and weight z-scores (Table 3-22).
It needs to be determined whether or not it is realistic for children to experience
normal growth while on ketogenic therapy. The height and weight of the patient need to
be plotted on the growth chart and documented in the medical record. In order to
determine the appropriate amount of energy required to promote growth, the height and
weight z-scores and energy prescription at initiation and at each clinic visit need to
documented in the medical record and entered into the database. The energy prescription
needs to be identified at each change in height and weight (Table 3-22).
While a recommended growth rate for children on ketogenic therapy is still
controversial, mental development is often expected to improve while on ketogenic
therapy (52,58). Development and behavior of 65 children on the ketogenic therapy was
evaluated at baseline and at 1 year. Thirty-four children continued ketogenic therapy,

67
Table 3-22. Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: Growth and Development Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Delayed C2 (2)
Normal C2 (2)
Is growth promoted/normal or delayed?
Usually normal, sometimes delayed
C2 (1)
What were the height z-scores at different durations of ketogenic therapy?
Data available for future analysis (Appendix B)
Plot the height of the patient on the growth chart at initiation and at each clinic visit. Document the height z-scores at initiation and at each clinic visit.
How do weight and heightt z-scores change in children while on ketogenic therapy?
Some patients lost up to 2 z-scores for height and weight by the end of a 2-yr study.
C2 (1) What were the weight z-scores at different durations of ketogenic therapy?
Data available for future analysis (Appendix B)
Plot the weight of the patient on the growth chart at initiation and at each clinic visit. Document the weight z-scores at initiation and at each clinic visit.
Is development promoted or delayed?
Promoted/ Beneficial
C2 D
(2) (1)
Is development promoted or delayed?
No data available
Document the level of development at each clinic visit. Perhaps, document reports given by physical therapists, school teachers, etc.

68
Table 3-22. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
These children should grow. A calorie restriction may not be necessary.
C2 (1) Do changes in calorie prescription correlate to patient’s height and weight on growth charts? For children that are not overweight, is a normal growth velocity correlated with an increase, decrease, or no change in calories? (Are they expected to grow or not?)
The majority of children seem to grow along the same height percentile curve from pre-study to 4 months on the diet. Adequate calories and protein need to be given to assist growth.
C2 (1)
What was the calorie prescription for each height z-score and weight z-score?
Data available for future analysis (Appendix B)
Document the height and weight z-scores and calorie prescription at initiation and at each clinic visit. Identify the calorie prescription at each change in height and weight z-scores and at each change in plots on the growth chart.

69
and they showed a statistically significant improvement in overall developmental
functioning, including attention and social skills (59). To continue research on
development of patients on ketogenic therapy, the level of development, perhaps, from
reports given by physical therapists, school teachers, etc. need to be documented in the
medical record and entered into the database (Table 3-22).
High Lipid Profiles
Fat is calculated to provide 70 to 90% of the calories for individuals on ketogenic
therapy. There has been concern about potential negative effects on the blood lipid
profiles of patients following this dietary regimen. Vining reports that children on
ketogenic therapy occasionally have markedly elevated triglycerides, which requires an
adjustment to ketogenic therapy (26).
A 6-month prospective cohort study of 141 children on ketogenic therapy was
conducted; 59 subjects also were studied after 12 months; 27 subjects were studied after
24 months. After 6 months of ketogenic therapy, mean plasma concentrations of total
cholesterol, low density lipoprotein (LDL) cholesterol, very low density lipoprotein
(VLDL) cholesterol, non-high density lipoprotein (non-HDL) cholesterol, and
triglycerides significantly increased, while mean high density lipoprotein (HDL)
cholesterol significantly decreased. Total cholesterol and LDL cholesterol remained
significantly high at 12 and 24 months; however, plasma concentrations were lower after
12 and 24 months than after 6 months. Triglyceride concentrations, although higher,
were not significantly different from baseline. HDL remained significantly low at 12 and
24 months (60).
Medical charts of 42 children on ketogenic therapy for an average of 10 months
were reviewed. Lab values were checked at initiation and at follow-up clinic visits.

70
There was a significant increase in the mean total cholesterol (p=0.017) and triglyceride
(p=0.027) concentrations. The authors suggested that the complications they reported
might be out-weighed by the seizure control. They recommend monitoring serum lipid
concentrations as long as children are on ketogenic therapy (47).
A subset of our database was analyzed as an example of how patient data can be
utilized. Analysis of variance was performed using Statistical Analysis Software (SAS).
Due to time constraints, patient data from individuals who were 3 years old or younger at
the time of ketogenic therapy initiation (n = 23) were analyzed. After initiation, patients
are scheduled for follow-up clinic visits every three months for the first year on ketogenic
therapy and then every six months for subsequent years on ketogenic therapy. Some
patients may have scheduled follow-up clinic visits before or after the allotted follow-up
time. For example, a patient may have a clinic visit at 8 months instead of 9 months. In
order to account for each clinic visit, date ranges were developed. Date ranges include
clinic visits at initiation, 1 to 3 months, 4 to 6 months, 7 to 9 months, 10 to 12 months, 13
to 18 months, 19 to 24 months, etc.
Ketogenic therapy was originally developed as a 2-year treatment for epilepsy.
However, many patients remain on ketogenic therapy for longer periods of time. This
raises concern for the negative effects of a high fat diet on blood lipid profiles. Our
database has been evaluated to determine if the duration of ketogenic therapy has an
effect on triglycerides, total cholesterol, LDL cholesterol, HDL cholesterol, and non-
HDL cholesterol (total cholesterol minus HDL cholesterol). Significant differences were
detected in triglyceride (p=0.0005), total cholesterol (p=0.0074), LDL cholesterol
(p=0.0008), and non-HDL cholesterol (p=0.0037) concentrations over the duration of

71
ketogenic therapy (i.e., among all date ranges). Significant differences in HDL
cholesterol concentrations were not detected (p=0.1309) among any date ranges. Figures
3-3, 3-5, 3-7, 3-9, and 3-11 depict changes in blood lipid profiles of each patient on
ketogenic therapy over time (i.e., months). Figures 3-4, 3-6, 3-8, 3-10, and 3-12 depict
changes in blood lipids from initiation (first date range) and throughout the first 3 months
(second date range) of ketogenic therapy.
Our database also was used to determine if the patients respond differently to
ketogenic therapy by evaluating their individual blood lipid profiles. Compared to each
other, the patients were detected to have statistically significant differences of triglyceride
(p=0.0014), total cholesterol (p<0.0001), LDL cholesterol (p<0.0001), HDL cholesterol
(p<0.0001), and non-HDL cholesterol (p<0.0001) concentrations. Figures 3-13, 3-14, 3-
15, 3-16, and 3-17 show the lipid concentrations of the individual patients.
Elevated blood lipid concentrations are a possible complication of ketogenic
therapy, but they may be avoidable. Experiments have been done to address the issue of
high lipid profiles; for example, medium chain triglycerides (MCT) in the form of oil are
sometimes used as opposed to the classic diet made with cream and butter. In
comparisons made between the classic diet and the MCT diet, both diets were found to
have similar anticonvulsant effects, but the classic diet increased cholesterol
concentrations while the MCT diet did not (61). Liu et al. reported that the MCT diet had
positive effects on lipid profiles (62). Prasad et al. observed that the serum cholesterol
concentrations were less elevated in patients on the MCT diet (16).
It is important to note that MCT oil is often prescribed to relieve constipation,
which is a common side effect of ketogenic therapy. As a result, lipid profiles may be

72
1 to
34
to 6
7 to
910
to 1
213
to 1
8
19 to
24
25 to
30
31 to
36
37 to
42
43 to
48
49 to
54
55 to
60
61 to
66
67 to
72
73 to
78
0
100
200
300
400
500
600
700
800
900
1000 KG0001KG0014KG0053
KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0154KG0156KG0158
KG0060KG0064
KG: KetoGator patient identification number
Months on Ketogenic Therapy
Trig
lyce
ride
(mg/
dl)
Figure 3-3. Triglyceride concentrations of individual patients on ketogenic therapy over
time
0In
itiat
e
1 to
3M
onth
s
0
100
200
300
400
500
600
700
800
900
1000 KG0014KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Duration of Ketogenic Therapy
Trig
lyce
ride
(mg/
dl)
Figure 3-4. Triglyceride concentrations of individual patients at baseline and 1 to 3
months post-initiation of ketogenic therapy

73
1 to
34
to 6
7 to
910
to 1
213
to 1
8
19 to
24
25 to
30
31 to
36
37 to
42
43 to
48
49 to
54
55 to
60
61 to
66
67 to
72
73 to
78
75
100
125
150
175
200
225
250
275 KG0001KG0014KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Months on Ketogenic Therapy
Tota
l Cho
lest
erol
(mg/
dl)
Figure 3-5. Total cholesterol concentrations of individual patients on ketogenic therapy
over time
0In
itiat
e
1 to
3M
onth
s
75
100
125
150
175
200
225
250
275 KG0014KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Duration on Ketogenic Therapy
Tota
l Cho
lest
erol
(mg/
dl)
Figure 3-6. Total cholesterol concentrations of individual patients at baseline and 1 to 3
months post-initiation of ketogenic therapy

74
1 to
34
to 6
7 to
910
to 1
213
to 1
8
19 to
24
25 to
30
31 to
36
37 to
42
43 to
48
49 to
54
55 to
60
61 to
66
67 to
72
73 to
78
20
30
40
50
60
70
80
90
100
110
120
130
140
150
160
170 KG0001KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Months on Ketogenic Therapy
LDL
(mg/
dl)
Figure 3-7. LDL cholesterol concentrations of individual patients on ketogenic therapy
over time
0In
itiat
e
1 to
3M
onth
s
20
30
40
50
60
70
80
90
100
110
120
130
140
150
160
170KG0053KG0060KG0064KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Duration on Ketogenic Therapy
LDL
(mg/
dl)
Figure 3-8. LDL cholesterol concentrations of individual patients at baseline and 1 to 3
months post-initiation of ketogenic therapy
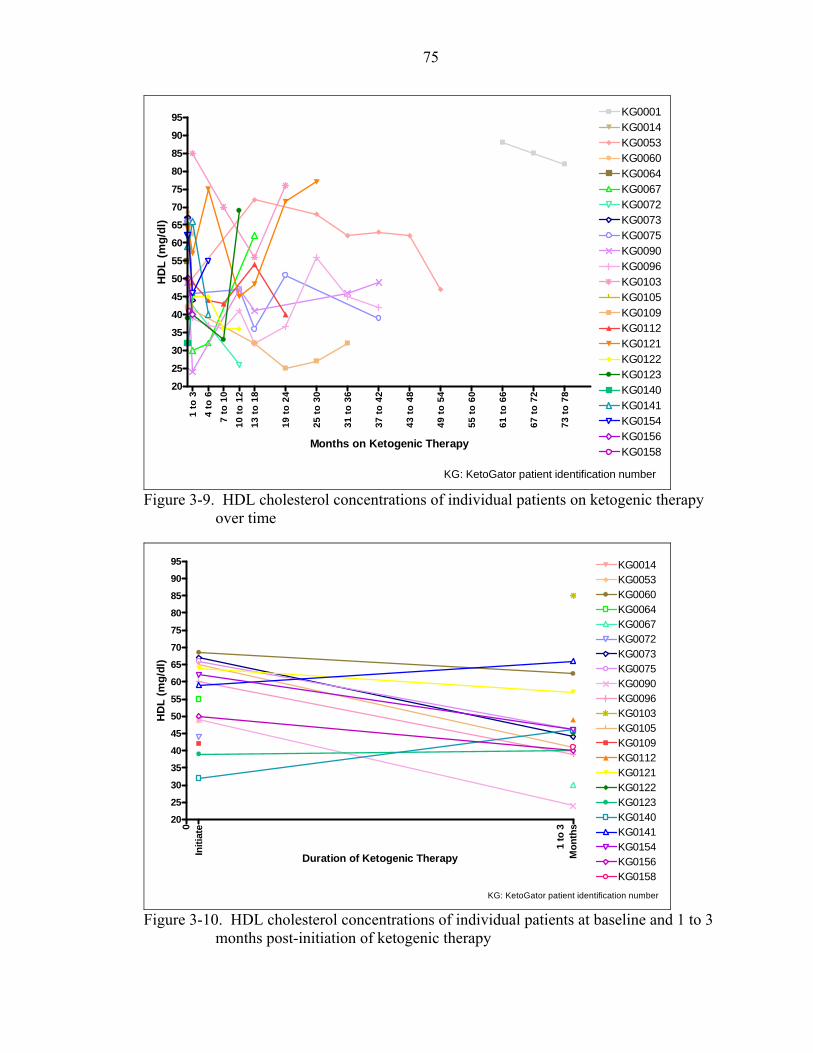
75
1 to
34
to 6
7 to
10
10 to
12
13 to
18
19 to
24
25 to
30
31 to
36
37 to
42
43 to
48
49 to
54
55 to
60
61 to
66
67 to
72
73 to
78
20
25
30
35
40
45
50
55
60
65
70
75
80
85
90
95 KG0001KG0014KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Months on Ketogenic Therapy
HD
L (m
g/dl
)
Figure 3-9. HDL cholesterol concentrations of individual patients on ketogenic therapy
over time
0In
itiat
e
1 to
3M
onth
s
20
25
30
35
40
45
50
55
60
65
70
75
80
85
90
95 KG0014KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Duration of Ketogenic Therapy
HD
L (m
g/dl
)
Figure 3-10. HDL cholesterol concentrations of individual patients at baseline and 1 to 3
months post-initiation of ketogenic therapy

76
1 to
3
4 to
6
7 to
9
10 to
12
13 to
18
19 to
24
25 to
30
31 to
36
37 to
42
43 to
48
49 to
54
55 to
60
61 to
66
67 to
72
73 to
78
0
1
2
3
4
5
6
7
8 KG0001KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Months on Ketogenic Therapy
Tota
l Non
-HD
L (m
g/dl
)
Figure 3-11. Non-HDL cholesterol concentrations of individual patients on ketogenic
therapy over time
0In
itiat
e
1 to
3M
onth
s
0
1
2
3
4
5
6
7
8 KG0053KG0060KG0064KG0067KG0072KG0073KG0075KG0090KG0096KG0103KG0105KG0109KG0112KG0121KG0122KG0123KG0140KG0141KG0154KG0156KG0158
KG: KetoGator patient identification number
Duration on Ketogenic Therapy
Tota
l Non
-HD
L (m
g/dl
)
Figure 3-12. Non-HDL cholesterol concentrations of individual patients at baseline and 1
to 3 months post-initiation of ketogenic therapy

77
KG
0001
KG
0014
KG
0053
KG
0067
KG
0072
KG
0073
KG
0075
KG
0090
KG
0096
KG
0103
KG
0105
KG
0109
KG
0112
KG
0121
KG
0122
KG
0123
KG
0140
KG
0141
KG
0154
KG
0156
KG
0158
KG
0060
KG
0064
KG
0008
KG
015
9
0
100
200
300
400
500
600
700
800
900
1000
Patients (KetoGator Identification Number)
Trig
lyce
ride
(mg/
dl)
Figure 3-13. Triglyceride concentrations of individual patients
KG
0001
KG
0008
KG
0014
KG
0053
KG
0060
KG
0064
KG
0067
KG
0072
KG
0073
KG
0075
KG
0090
KG
0096
KG
0103
KG
0105
KG
0109
KG
0112
KG
0121
KG
0122
KG
0123
KG
0140
KG
0141
KG
0154
KG
0156
KG
0158
KG
0159
75
100
125
150
175
200
225
250
275
Patients (KetoGator Identification Number)
Tota
l Cho
lest
erol
(mg/
dl)
Figure 3-14. Total cholesterol concentrations of individual patients

78
KG
0001
KG
0014
KG
0053
KG
0060
KG
0064
KG
0067
KG
0072
KG
0073
KG
0075
KG
0090
KG
0096
KG
0103
KG
0105
KG
0109
KG
0112
KG
0121
KG
0122
KG
0123
KG
0140
KG
0141
KG
0154
KG
0156
KG
0158
KG
0008
KG
0159
0102030405060708090
100110120130140150160170
Patients (KetoGator Identification Number)
LDL
(mg/
dl)
Figure 3-15. LDL cholesterol concentrations of individual patients
KG
0001
KG
0014
KG
0053
KG
0060
KG
0064
KG
0067
KG
0072
KG
0073
KG
0075
KG
0090
KG
0096
KG
0103
KG
0105
KG
0109
KG
0112
KG
0121
KG
0122
KG
0123
KG
0140
KG
0141
KG
0154
KG
0156
KG
0158
KG
0008
KG
0159
20
30
40
50
60
70
80
90
Patients (KetoGator Identification Number)
HD
L (m
g/dl
)
Figure 3-16. HDL cholesterol concentrations of individual patients

79
KG
0001
KG
0014
KG
0053
KG
0060
KG
0064
KG
0067
KG
0072
KG
0073
KG
0075
KG
0090
KG
0096
KG
0103
KG
0105
KG
0109
KG
0112
KG
0121
KG
0122
KG
0123
KG
0140
KG
0141
KG
0154
KG
0156
KG
0158
KG
0008
KG
015
9
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
5.5
6.0
6.5
7.0
7.5
Patients (KetoGator Identification Number)
Tota
l Non
-HD
L (m
g/dl
)
Figure 3-17. Non-HDL cholesterol concentrations of individual patients
impacted. In addition to investigating the changes in lipid profiles, the database should
also be evaluated to see how many patients received MCT oil and how the amount of
MCT oil given increased or decreased from initiation throughout ketogenic therapy
(Table 3-23).
Studies are warranted to determine the long-term effects of ketogenic therapy on
lipid profiles and to determine the most effective way to reduce complications. The
patients’ blood lipid profiles at initiation and at each clinic visit need to be documented in
the medical record and entered into the database. Abnormal blood lipid values need to be
identified. In order to determine the variables that may affect blood lipid profiles of
patients on ketogenic therapy, certain data need to be documented in the medical record
and entered into the database. The data include the AEDs the patient was taking and the

80
Table 3-23. Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: High Lipid Profiles Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Document blood lipid profiles at initiation and at each clinic visit.
How does ketogenic therapy affect triglyceride, total cholesterol, LDL, HDL, and non-HDL cholesterol concentrations?
It has the potential to significantly increase total cholesterol and triglyceride concentrations. (Complications may be out-weighed by seizure control.)
C1 C2
(1) (1)
How did the lipid concentrations change over the course of ketogenic therapy?
Over the duration of ketogenic therapy, significant differences were detected in triglyceride (p=0.0005), total cholesterol (p=0.0074), LDL cholesterol (p=0.0008), HDL cholesterol, and non-HDL cholesterol (p=0.0037) concentrations. No significant differences were detected in HDL cholesterol concentrations (p=0.1309).
Identify which blood lipid profiles are abnormal.

81
Table 3-23. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
At 6 months, ketogenic therapy significantly increased the mean plasma concentrations of total cholesterol, LDL, VLDL, non-HDL cholesterol, and triglycerides. Mean HDL decreased significantly though apoA-I increased. Significant but less marked changes persisted in children observed after 12 and 24 months on ketogenic therapy.
B (1) How did lipid concentrations differ among patients?
Compared to each other, the patients were detected to have statistically significant differences of triglyceride (p=0.0014), total cholesterol (p<0.0001), LDL cholesterol (p<0.0001), HDL cholesterol (p<0.0001), and non-HDL cholesterol (p<0.0001) concentrations.

82
Table 3-23. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
How did lipid concentrations differ among patients on particular AEDs? Are the blood lipids normal or abnormal?
Data available for future analysis (Appendix B)
Identify which AEDs the patient was on and the medication score when blood lipid concentrations were abnormal.
What were the lipid concentrations among different calories/kg/day prescribed?
Data available for future analysis (Appendix B)
Identify the calorie prescription (kcal/kg/d) when blood lipid concentrations were abnormal and normal.
Is there a relationship between lipid concentrations and AEDs or diet prescription?
No evidence --
How did lipid concentrations differ among different ratios prescribed?
Data available for future analysis (Appendix B)
Identify the ratio prescription when blood lipid concentrations were abnormal and normal.
How can high lipid concentrations be avoided or the risk reduced?
Medium chain triglyceride (MCT) oil as a fat source
C1 C2
(1) (2)
What quantity of MCT oil was administered?
Data available for future analysis (Appendix B)
Document the amount of MCT oil the patient receives. Identify the blood lipid concentrations at each change in MCT oil prescription.

83
medication score, the energy prescription (kcal/kg/d), the ratio prescription, and the MCT
oil prescription when blood lipid profiles were abnormal and normal (Table 3-23).
Other Adverse Effects
Several adverse effects have been reported in association with ketogenic therapy
(Table 3-24) including gastrointestinal disturbances (i.e., nausea, vomiting, reflux,
constipation, diarrhea, hunger, and abdominal pain) (5,8,18,22,25,63,64), kidney stones
(3,18,22,64), gall stones (3), hypoglycemic episodes (18,25,40,63), hypoproteinemia
(3),dehydration (18), anorexia (63), irritability (25), lethargy (18,63), severe acidosis
(25,63), hyperuricemia (63), vitamin/mineral deficiency (18), osteoporosis (18),
neuropathy (18), cardiac complications (65), bruising or bleeding (7,66), acute
pancreatitis (67), thinning hair and/or hair loss (7), amenorrhea (7), and delayed puberty
(7). Many studies report that adverse effects are uncommon and may have occurred in
only one patient.
There have been some suggestions for preventing kidney stones, hypoglycemia,
and constipation. A few studies have reported that kidney stones can be avoided by
allowing adequate hydration (12,26,55,68), using urine alkalinization (i.e., potassium
citrate) (12), and avoiding certain medications (i.e., carbonic anhydrase inhibitors)
(26,35,68). For patients with hypoglycemia (i.e., serum glucose <30 mg/dl) the protocol
followed at Johns Hopkins Hospital is the administration of 30 milliliters (mL) of orange
juice followed by a repeat serum glucose check in 1 hour (40). There are a variety of
treatments recommended for constipation. These include adequate fluid intake and the
inclusion of vegetables into daily meals, 25 grams of iceberg lettuce as a “free food”, 10
to 20 grams of avocado daily, calculation if MCT oil into meals, a carbohydrate-free stool
softener, carbohydrate-free laxative, a glycerin suppository, or an enema (14).

84
Table 3-24. Basis of KetoGator Guidelines. Monitoring Potential Adverse Effects: Other Adverse Effects Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Which of the following adverse effects were seen in the patients?:
Document the following adverse effects at initiation and at each clinic visit:
GI disturbances (nausea, vomiting, reflux, constipation, diarrhea, hunger, and abdominal pain)
B C1 C2
(1) (2) (4)
GI disturbances (nausea, vomiting, reflux, constipation, diarrhea, hunger, and abdominal pain)
See Table 3-2. Data available for future analysis (See appendix B).
GI disturbances (nausea, vomiting, reflux, constipation, diarrhea, hunger, and abdominal pain)
Kidney stones B C1 C2
(1) (2) (1)
Kidney stones No data available
Kidney stones
Gall stones B (1) Gall stones No data available
Gall stones
Hypoglycemic episodes
C1 C2 E
(1) (2) (1)
Hypoglycemic episodes
No data available
Hypoglycemic episodes
Dehydration C1 (1) Dehydration No data available
Dehydration
Anorexia C2 (1) Anorexia No data available
Anorexia
Irritability C2 (1) Irritability No data available
Irritability
What other adverse effects have been reported?
Lethargy C1 C2
(1) (2)
Lethargy No data available
Lethargy

85
Table 3-24. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Severe acidosis C2 (2) Severe acidosis No data available
Severe acidosis
Hyperuricemia C2 (1) Hyperuricemia No data available
Hyperuricemia
Hypoproteinemia B (1) Hypoproteinemia No data available
Hypoproteinemia
Vitamin/mineral deficiency
C1 (1) Vitamin/mineral deficiency
No data available
Vitamin/mineral deficiency
Osteoporosis C1 (1) Osteoporosis No data available
Osteoporosis
Neuropathy C1 (1) Neuropathy No data available
Neuropathy
Cardiac complications
C2 (1) Cardiac complications
No data available
Cardiac complications
Bruising C2 (2) Bruising No data available
Bruising
Thinning hair and/or hair loss
C2 (1) Thinning hair and/or hair loss
No data available
Thinning hair and/or hair loss
Amenorrhea in adolescents
C2 (1) Amenorrhea in adolescents
No data available
Amenorrhea in adolescents
Acute pancreatitis No data available
Acute pancreatitis
Acute pancreatitis D (1)
Others No data available
Others

86
Table 3-24. Continued Questions for
Published Research
Conclusions Reported in Published Research
Level of Evidence
(Number of Sources)
Questions for Database
Database Assessment
Future Documentation/ Studies Needed
Adequate Hydration
B C1 C2 E
(1) (1) (1) (1)
Urine alkalinization
E (1)
How can kidney stone formation be avoided?
Avoiding certain meds (CAI)
C1 C2
(1) (1)
How can kidney stone formation be avoided?
No data available
For patients that have experienced kidney stones, document precautions taken to avoid kidney stone formation (i.e., unrestricted fluid consumption).

87
There is no documentation of the above adverse effects in the database other than
the presence of GI disturbances and blood lipid profiles (Table 3-24). More studies are
warranted to investigate ways to decrease the frequency of all adverse effects. In order to
determine which complications may arise from ketogenic therapy, the following adverse
effects need to be documented in the medical record and entered into the database at
initiation and at each clinic visit: kidney stones, gall stones, hypoglycemic episodes,
dehydration, anorexia, irritability, lethargy, severe acidosis, hyperuricemia,
hypoproteinuria, vitamin/mineral deficiency, osteoporosis, neuropathy, cardiac
complications, bruising, thinning hair and/or hair loss, amenorrhea in adolescents, acute
pancreatitis, etc. For patients that have experienced adverse effects, strategies taken to
relieve the adverse effect need to be documented in the medical record and entered into
the database. It is crucial to document all adverse effects experienced by each patient so
clinicians can begin taking steps to prevent the occurrence (Table 3-24).
Based on the information available, it is apparent more data are required before a
comprehensive set of guidelines can be established. The next chapter comprises the KG
Guidelines, which were based on the topics recently discussed. The KG Guidelines are
an organized compilation of the available published data on clinical care of ketogenic
therapy. Additionally, it offers clinicians choices of treatment in several areas of
ketogenic therapy.
88
CHAPTER 4 DISCUSSION OF KETOGATOR GUIDELINES
The KetoGator (KG) Guidelines are a set of evidence-based guidelines for
initiating and monitoring patients on ketogenic therapy. They were developed based on
evidence from published research, and an evidence grading system was used to rank the
level of evidence of each guideline. Many questions pertaining to clinical care of patients
on ketogenic therapy remain unanswered. Lack of evidence from the literature places
gaps in the KG Guidelines, suggesting the need for future studies. The development of a
database that includes data obtained from medical records of patients on ketogenic
therapy could provide a way in which the safety and efficacy of different aspects of
ketogenic therapy could be evaluated. In order to develop a useful database that can be
used to address a variety of questions related to ketogenic therapy, more complete
documentation of key information must be included in patient medical records. The KG
Guidelines, developed as a result of the work completed for this study, are listed in Table
4-1.
Pre-Initiation
Patient Selection
Prior to initiation, it should be considered whether or not each patient is an
appropriate candidate for ketogenic therapy. Age does not appear to be a factor for
discouraging this treatment (7,17,19-22,24,26,27). There is no evidence to suggest
ketogenic therapy should not be tried in infants, children, adolescents, or adults.

89
All potential candidates must be screened for inborn errors of metabolism by
possibly measuring urinary organic acids and amino acids, serum amino acids, lactate,
pyruvate, and carnitine (12-14). This will help to ensure that patients with fatty acid
oxidation deficiency will not be treated with the high-fat content of ketogenic therapy.
Use of Ketogenic Therapy Combined with Other Treatments
Due to the reports of multiple adverse effects associated with Valproic Acid
(18,33), kidney stones or a decrease in bicarbonate levels associated with carbonic
anhydrase inhibitors (34,35), and encephalopathy associated with Phenobarbital (18),
clinicians may opt to keep these medications separate from ketogenic therapy. For
clinicians who opt to allow patients taking any one of these medications to be put on
ketogenic therapy, the patients should be carefully monitored. Physical symptoms and
caregiver reports should be checked frequently. Kidney stones may be avoidable while
taking carbonic anhydrase inhibitors with ketogenic therapy by ensuring adequate fluid
consumption and the possible use of urine alkalinizing agents (i.e., potassium citrate,
sodium citrate, sodium bicarbonate) (36). Taking precautions into consideration prior to
initiating ketogenic therapy may prevent the occurrence of potential adverse effects
during ketogenic therapy.
Patient/Parent Education
Educating the patient/parent prior to initiation may make a smoother transition
from a regular diet to the new diet prescription and, perhaps, aid in compliance.
Teaching sessions prior to initiation may focus on the nutrition assessment, overview of
ketogenic therapy including calculation methods for menus and development of food
lists, and discussion of goals and expectations (43). Things to consider discussing in a
pre-ketogenic therapy session include the process of food preparation and food weighing,

90
information for purchasing a scale that weighs in tenths of a gram, a description of meals
and beverages that will be eaten, requirements for the omission of carbohydrate-rich
foods, appropriate foods and nutritional supplements, the required follow-up
appointments, the possible adverse effects, the expected length of ketogenic therapy, and
alternative foods to enjoy at holidays and major events (14). It is important for clinicians
to keep in mind that patients/caregivers tend to view their educational needs differently
than do health care providers and they need to tailor the lessons to the individual patient
(49).
Initiation
Schedule Protocol
At initiation, ketogenic meals are generally increased by 1/3 caloric prescription
until the full caloric prescription is met (39,40). Oral feeders typically do not receive any
foods other than their ketogenic meals. Tube feeders typically have their non-ketogenic
meals decreased at the same rate that their ketogenic meals are increased (14). Another
option is to start ketogenic meals at full caloric prescription and gradually increase the
macronutrient ratio from 1:1 to full ratio prescription over 3 to 4 days (42).
Fasting
Two options are available for beginning the diet: inclusion of a fast (14,27,40,44)
or exclusion of a fast (42). Both methods have reportedly helped in the success of
ketogenic therapy. Including a fast supposedly increases hunger in the patient and
encourages them to eat all of their meals (14). Excluding the fast is successful in
achieving ketosis and may increase tolerance to the meals (42). Until further testing on
fasting occurs, it is the decision of the clinicians to fast or not fast their patients.

91
Laboratory Values
It is suggested that the following lab values be monitored at initiation: blood lipid
concentrations, complete blood count, metabolic panel, serum beta-hydroxybutyrate,
urinary ketone bodies, and urinary specific gravity (41). A complete list of lab tests is
found in Table 3-11.
Patient/Parent Education
During initiation, the principles of ketogenic therapy that have already been
introduced in the pre-initiation session should be reinforced (43). Strategies for problem
solving and facilitation of accuracy and creativity in menu development are important to
be addressed before the patient leaves the hospital (43).
Diet Prescription
Ratio. Since there is no available research on the efficacy of different ratios of
macronutrients, clinicians are referred to suggestions from other clinicians. The
recommendation made by Zupec-Kania, Werner, and Zupanc (Table 3-14) can be used
until further evidence identifies appropriate macronutrient ratios for each patient (14).
Calories. Two options are available for prescribing the calories: prescribe normal
calories (21,54) or restrict calories (7,14,44,53). A restriction is often 75 to 90% of the
DRI (14,44); ideal body weight can be used for calculating energy needs of overweight
children and actual weight can be used for underweight children (14). Until further
research comparing the efficacy, safety, and long-term outcomes of these two approaches
for estimating energy intake is available, it is the decision of the clinicians to prescribe
normal calories or to restrict calories.

92
Fluid. It seems apparent from the reviewed research that fluids should be
prescribed as maintenance needs (14,18,21,27,43,55). The Holiday-Segar method is an
option for calculating fluid prescription (Table 3-19) (14).
Post-Initiation
Laboratory Values
It is suggested that the following lab values be monitored at follow-up clinic visits:
blood lipid concentrations, complete blood count, metabolic panel, serum beta-
hydroxybutyrate, urinary ketone bodies, and urinary specific gravity (41). A complete
list of lab tests is found in Table 3-11. It is also suggested that the caregivers monitor
urinary ketone bodies and urinary specific gravity between follow-up clinic visits and
report them to the clinicians (41).
Growth and Development
Two options are available when planning for growth of the patients: normal growth
(22,52) or delayed growth (7,54,57). Until further research defines whether or not the
growth rates for children on ketogenic therapy are normal, it is the decision of the
clinicians to plan the treatment, specifically the diet prescription, for normal or delayed
growth. It is apparent cognitive and social development should improve while on
ketogenic therapy, and clinicians should look for signs that it is occurring (52,58,59).
Potential Adverse Effects
Since several adverse effects have previously been reported for patients on
ketogenic therapy, it is important to monitor physical symptoms and caregiver reports of
the following potential adverse effects: gastrointestinal (GI) disturbances
(5,8,18,22,25,63,64), high lipid profiles (26,47,60), kidney stones (3,18,22,64), gall
stones (3), hypoglycemic episodes (18,25,40,63), dehydration (18), anorexia (63),

93
irritability (25), lethargy (18,63), severe acidosis (25,63), hyperuricemia (63),
hypoproteinemia (3), vitamin/mineral deficiency (18), osteoporosis (18), neuropathy (18),
cardiac complications (65), bruising or bleeding (7,66), thinning hair and/or hair loss (7),
amenorrhea in adolescents (7), acute pancreatitis (67). High blood lipid concentrations, a
potential adverse effect of ketogenic therapy, may be prevented by using medium chain
triglyceride (MCT) oil as a fat source (16,61,62). For the prevention of kidney stone
formation, clinicians should consider ensuring adequate hydration (12,26,55,68),
providing urine alkalinization (12), and possibly avoiding certain medications,
specifically carbonic anhydrase inhibitors (26,68).
Surgery
If surgery is planned for a patient, clinicians familiar with ketogenic therapy need
to educate surgeons on the treatment and refer them to consult “Aneasthetic Guidelines
for Paediatric Patients on the Ketogenic Diet” (38:p.105).
Chapter Summary
The KG Guidelines outlined in this chapter form the beginning of the development
of evidence-based procedures for carrying out ketogenic therapy for patients with
epilepsy. The KG Guidelines can become more complete with improved documentation
and data analysis. This may lead to the standardization of care for ketogenic therapy.

94
Table 4-1. KetoGator (KG) Guidelines
Guidelines Level of Evidence
(Number of Sources)
PRE-INITIATION
Patient Selection
All ages, including:
Infants C2, D, E (3), (4), (2)
Adolescents C2 (1)
Adults C1, C2, E (1), (2), (1)
Screen and document inborn errors, by measuring:
- Urinary organic acids and amino acids - Serum amino acids, lactate, pyruvate, and carnitine
E (2)
Use of Ketogenic Therapy Combined with other Treatments
Carefully monitor patients taking valproic acid for adverse effects.
C1, C2 (1), (1)
Carefully monitor patients taking carbonic anhydrase inhibitors (topiramate, zonisamide, and acetazolamide) for kidney stones and/or a decrease in bicarbonate.
C2, D (2), (1)
Ensure patients consume adequate fluids and consider urine alkalinization for patients taking carbonic anhydrase inhibitors when planning for ketogenic therapy.
C2 (1)
Carefully monitor patients taking phenobarbital for encephalopathy.
C1
(1)
Patient/Parent Education
Teach patients/caregivers how to calculate menus and develop food lists. Focus on nutrition assessment, overview of ketogenic therapy including calculation methods, and discussion of goals and expectations. Meet with orally fed patients twice and tube feeders once.
C2 (1)
Things to consider discussing in a pre-ketogenic diet session include the process of food preparation and food weighing, information for purchasing a scale that weighs in tenths of a gram, a description of meals and beverages that will be eaten, requirements for the omission of carbohydrate-rich foods, appropriate foods and nutritional supplements, the required follow-up appointments, the possible adverse effects, the expected length of ketogenic therapy, and alternative foods to enjoy at holidays and major events
E (1)
Keep in mind that patients/caregivers tend to view their educational needs differently than health care providers.
C2 (1)
Tailor the lessons to the individual patient. C2 (1)
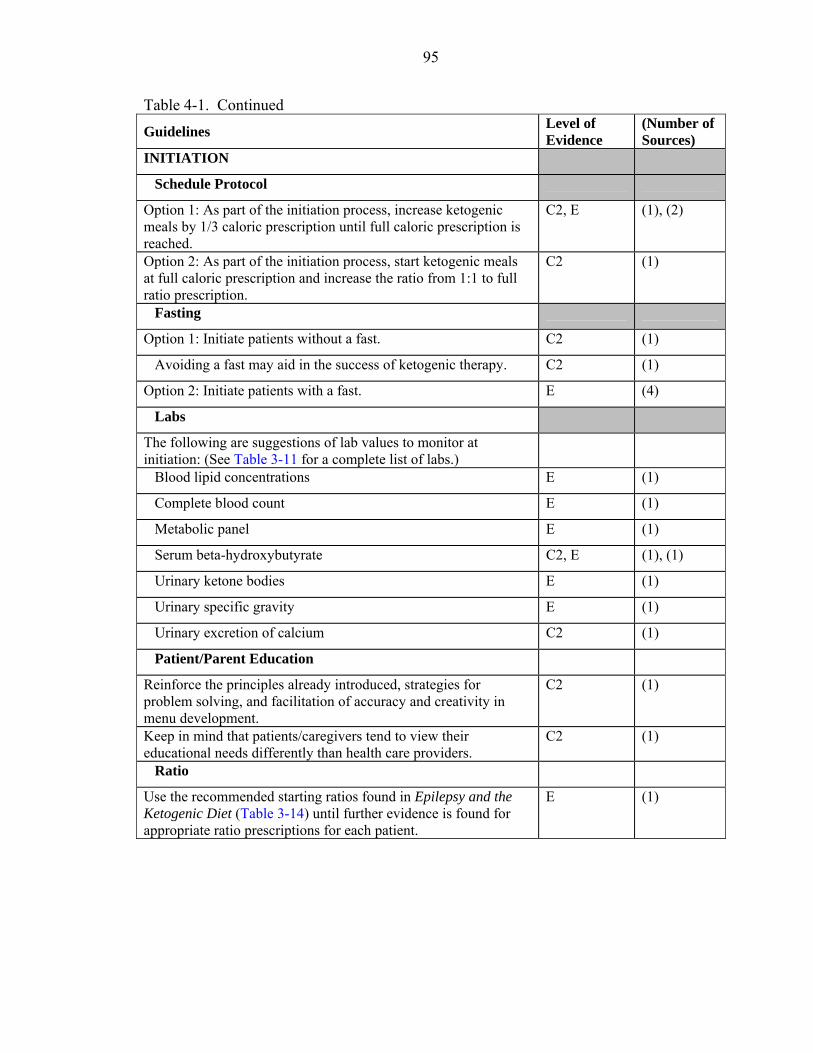
95
Table 4-1. Continued
Guidelines Level of Evidence
(Number of Sources)
INITIATION
Schedule Protocol
Option 1: As part of the initiation process, increase ketogenic meals by 1/3 caloric prescription until full caloric prescription is reached.
C2, E (1), (2)
Option 2: As part of the initiation process, start ketogenic meals at full caloric prescription and increase the ratio from 1:1 to full ratio prescription.
C2 (1)
Fasting
Option 1: Initiate patients without a fast. C2 (1)
Avoiding a fast may aid in the success of ketogenic therapy. C2 (1)
Option 2: Initiate patients with a fast. E (4)
Labs
The following are suggestions of lab values to monitor at initiation: (See Table 3-11 for a complete list of labs.)
Blood lipid concentrations E (1)
Complete blood count E (1)
Metabolic panel E (1)
Serum beta-hydroxybutyrate C2, E (1), (1)
Urinary ketone bodies E (1)
Urinary specific gravity E (1)
Urinary excretion of calcium C2 (1)
Patient/Parent Education
Reinforce the principles already introduced, strategies for problem solving, and facilitation of accuracy and creativity in menu development.
C2 (1)
Keep in mind that patients/caregivers tend to view their educational needs differently than health care providers.
C2 (1)
Ratio
Use the recommended starting ratios found in Epilepsy and the Ketogenic Diet (Table 3-14) until further evidence is found for appropriate ratio prescriptions for each patient.
E (1)

96
Table 4-1. Continued
Guidelines Level of Evidence
(Number of Sources)
Calories
Option 1: Prescribe normal maintenance calories based on DRI. C2, E (2), (1)
Option 2: Restrict calories to 75 to 90% of the DRI as recommended in the ADA Pediatric Manual for Clinical Dietetics (Table 3-17)
C2, E (1), (3)
When estimating calories, use ideal weight for overweight patients and actual weight for underweight patients.
E (1)
Fluids
Prescribe maintenance fluid needs based on the DRI. (Consider using the Holiday-Segar Method listed in Table 3-19.)
B, C2, E (1), (1), (3)
POST-INITIATION
Lab Values
The following are suggestions of lab values to monitor at follow-up clinic visits: (See Table 3-11 for a complete list of labs.)
Blood lipid concentrations E (1)
Complete blood count E (1)
Metabolic panel E (1)
Serum beta-hydroxybutyrate C2, E (1), (1)
Urinary ketone bodies E (1)
Urinary specific gravity E (1)
Urinary excretion of calcium C2 (1)
The following are suggestions of lab values to monitor between follow-up clinic visits by the caregivers:
Urinary ketone bodies E (1)
Urinary specific gravity E (1)
Growth and Development
Option 1: Plan for normal growth. C2 (2)
Option 2: Plan for delayed growth C2 (2)
Plan for improvement in development. C2, D (2), (1)
Adverse Effects
Monitor physical symptoms and caregiver reports for the following potential adverse effects:
GI disturbances (nausea, vomiting, reflux, constipation, diarrhea, hunger, and abdominal pain)
B, C1, C2 (1), (2), (4)

97
Table 4-1. Continued
Guidelines Level of Evidence
(Number of Sources)
High lipid profiles B, C1, C2 (1), (1), (1)
Kidney stones B, C1, C2 (1), (2), (1)
Gall stones B (1)
Hypoglycemic episodes C1, C2, E (1), (2), (1)
Dehydration C1, C2 (1), (1)
Anorexia C2 (1)
Irritability C2 (1)
Lethargy C1, C2 (1), (2)
Severe acidosis C2 (2)
Hyperuricemia C2 (1)
Hypoproteinemia B (1)
Vitamin/mineral deficiency C1 (1)
Osteoporosis C1 (1)
Neuropathy C1 (1)
Cardiac complications D (1)
Bruising C2 (2)
Thinning hair and/or hair loss C2 (1)
Amenorrhea in adolescents C2 (1)
Acute pancreatitis D (1)
For possible prevention of high lipid levels, consider the using medium chain triglyceride (MCT) oil as a fat source.
C1, C2 (1), (1)
For prevention of kidney stone formation, consider the following:
Ensure adequate fluid intake B, C1, C2, E (1), (1), (1), (1)
Provide urine alkalinization C2 (1)
Avoid certain medications (specifically carbonic anhydrase inhibitors)
C2, D (1), (1)
Surgery
Educate surgeons and instruct them to refer to “Aneasthetic Guidelines for Paediatric Patients on the Ketogenic Diet” when planning to perform any surgery that requires anesthesia on a patient on ketogenic therapy.
D/E (1)
98
CHAPTER 5 SUMMARY
The current study is the first to design an approach for establishing evidence-based
practice with ketogenic therapy. Emphasis was placed on thorough documentation of the
method of treatment given to each patient on ketogenic therapy as well as the consequent
results. The success of ketogenic therapy is based on the following: 1) efficacy of the
treatment, including improvement in seizures, reduction of medications, and
improvement in alertness, 2) tolerance to the treatment, and 3) compliance of the patient.
The current study reflects that these qualities are difficult to document, and they are often
times subjective measures. In addition, the majority of the studies regarding the clinical
practices and care of patients on ketogenic therapy that were reviewed for this study were
ranked C1 or below for the level of evidence (Table 2-1). The number of level B studies
is limited, and there are no level A studies in regards to clinical care of ketogenic therapy.
How, then, are clinicians to know what brings the greatest success to their patients, and
how is it possible for them to practice in an evidence-based manner? The current study
offers suggestions for ways of documenting efficacy, tolerance, and compliance, which is
an important step in moving towards treatment standardization.
Once the proper documentation has been established, data can easily be
incorporated into a database, similar to the one created and designed in the current study.
Running analyses of the data may provide answers to queries about the best way to treat
patients with ketogenic therapy. UF plans to analyze data in the database to answer
queries using the suggestions reported in the current study. The goal is that the answers

99
to the queries will increase the number and quality of recommendations for developing
standards of care for ketogenic therapy.
The ultimate goal of this study was to move towards the standardization of care for
ketogenic therapy, which to our knowledge has never been done. In the current study, a
program was designed for doing this and recommendations were made for carrying out
the process. The basic design is to review published research on clinical care; document
available data and compile the data into a usable database; analyze the data to determine
trends and outcomes; and formulate recommendations that will greatly improve the
overall consistency of initiating and monitoring ketogenic therapy.

100
APPENDIX A DATABASE PARAMETERS
Table A-1. Population Database Parameters* Parameter Category Parameter Demographics KetoGator Identification Number Gender Birth Date Date Initiated Date Stopped Race City State Zip code County Route of Feeding Ambulatory Blood Lipids Access Identification Number KetoGator Identification Number Clinic Date Triglycerides (TG) High Density Lipoprotein (HDL) Low Density Lipoprotein (LDL) Total/HDL Cholesterol Total Cholesterol Complete Blood Count Access Identification Number KetoGator Identification Number Clinic Date Red Blood Cell (RBC) Count Hemoglobin (Hgb) Hematocrit (Hct) Platelet Count Mean Cell Volume (MCV) Mean Cell Hemoglobin (MCH) Mean Cell Hemoglobin Concentration (MCHC) Mean Platelet Volume (MPV) Red Blood Cell Distribution (RBC Dist) White Blood Count (WBC) Gastrointestinal (GI) Issues Access Identification Number KetoGator Identification Number Clinic Date Constipation

101
Table A-1. Continued Parameter Category Parameter Diarrhea Vomiting Nausea Comments Height and Weight Access Identification Number KetoGator Identification Number Clinic Date Height Weight Height % Weight % Height z-score Weight z-score Body Mass Index (BMI) BMI % Beta-Hydroxybutyrate Access Identification Number KetoGator Identification Number Clinic Date Beta-Hydroxybutyrate Alertness-Development Access Identification Number KetoGator Identification Number Clinic Date Alertness Activity Development Metabolic Panel Access Identification Number KetoGator Identification Number Clinic Date Sodium (Na) Potassium (K+) Chloride (Cl-) Carbon Dioxide (CO2) Blood Urea Nitrogen (BUN) Creatinine Glucose (Glu) Calcium (Ca+2) Magnesium (Mg+2) Inorganic Phosphate (PO4) Uric Acid Total Protein Albumin Bilirubin Total Bilirubin Direct Alkaline Phosphatase

102
Table A-1. Continued Parameter Category Parameter Aspartate Aminotransferase (AST) Alanine Transaminase (ALT) Lactate Dehydrogenase (LDH) Total Seizures Access Identification Number KetoGator Identification Number Clinic Date Seizure Number Since Last Clinic Seizures per Week Simple Partial (SP) Seizures Number SP Length of Seizures SP Severity of Seizures Complex Partial (CP) Seizures Number CP Length of Seizures CP Severity of Seizures Secondary Generalized (SG) Seizures Number SG Length of Seizures SG Severity of Seizures Absence Seizures Number Absence Length of Seizures Absence Severity of Seizures Myoclonic (MC) Seizures Number MC Length of Seizures MC Severity of Seizures Clonic (CL) Seizures Number CL Length of Seizures CL Severity of Seizures Tonic (TN) Seizures Number TN Length of Seizures TN Severity of Seizures Tonic-Clonic (TC) Seizures Number TC Length of Seizures TC Severity of Seizures Diet Prescription Access Identification Number KetoGator Identification Number Clinic Date Calories per day Protein per day Ratio Number of Meals/Bolus Number of Snacks Calories per Snack Reason for change (in diet prescription) Weight Calories per weight in kilograms per day (Kcals/kg/day) Protein per weight in kilograms per day (Pro/kg/day)

103
Table A-1. Continued Parameter Category Parameter Urinary Ketones and Specific Gravity
Access Identification Number
KetoGator Identification Number Clinic Date Ketone Body Level (Ketones) Specific Gravity AEDs [17 types] Access Identification Number KetoGator Identification Number Clinic Date Total Dosage per Day Units per Day Number of Doses per Day Comments Size Form Name Brand Name Medications (not AEDs) [68 types] Access Identification Number KetoGator Identification Number Clinic Date Total Dosage per Day Units per Day Number of Doses per Day Comments Size Form Name Brand Name Supplements [32 types] Access Identification Number KetoGator Identification Number Clinic Date Total Dosage per Day Units per Day Number of Doses per Day Comments Size Form Name Brand Name Medication Scores Access Identification Number KetoGator Identification Number Medication Low dose (mg/kg/day)

104
Table A-1. Continued Parameter Category Parameter Arm Anthropometrics Access Identification Number KetoGator Identification Number Clinic Date Upper Arm Circumference (UAC) Upper Arm Circumference % (UAC%) Triceps Skin Fold (TSF) Triceps Skin Fold % (TSF%)
*Parameters recorded in the database containing data of patients treated with ketogenic therapy at the University of Florida from 1995-2004.

105
APPENDIX B DATABASE QUERIES
Potential Database Queries with Parameters and Procedures: Based on Current Available Data
KEY
I. = Broad general question
A. = Question specific enough to be addressed by data in the database 1. = Parameters in the database that are needed to address question
a) = TABLE/CATEGORY IN THE DATABASE (1) = Column heading in the database table
2. = Procedures to follow in addressing question a) = Category OR description of how to carry out procedures
(1) = Description of how to carry out procedures
I. The following parameters and procedures should be used with database queries when addressing a particular age group (age at initiation).
A. Use only those KG numbers whose initiation date is a particular time (i.e., 0 to 3 years, 4 to 12 years, and 13 to 18 years) after the birth date.
1. Parameters a) DEMOGRAPHICS
(1) Birth date (2) Date Initiated
2. Procedures a) Use Birth Date (in DEMOGRAPHICS) and Date Initiated (in DEMOGRAPHICS) to determine the age at initiation.
(1) Find and only use those KG numbers whose initiation date is a particular time (i.e., 0 to 3 years) after the birth date.
II. The following are date ranges of the duration of ketogenic therapy (not to be confused with the patients’ ages). Use these date ranges when a database query refers to them.
A. Initiation (Day 1) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Parameters

106
a) Find the Date Initiated (in DEMOGRAPHICS) for the only acceptable date for the 1st date range.
B. Initiation Week (1 – 7 days) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Find the Date Initiated (in DEMOGRAPHICS) for the earliest acceptable date for the 2nd date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 7 days to it to determine the latest acceptable date for the 2nd date range.
C. 1– 4 weeks 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 1 week to it to determine the earliest acceptable date for the 3rd date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 4 weeks to it to determine the latest acceptable date for the 3rd date range.
D. 1– 3.9 months 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 1 month to it to determine the earliest acceptable date for the 4th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 3.9 months to it to determine the latest acceptable date for the 4th date range.
E. 4– 6.9 months 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 4 months to it to determine the earliest acceptable date for the 5th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 6.9 months to it to determine the latest acceptable date for the 5th date range.
F. 7 to 9.9 months 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 7 months to it to determine the earliest acceptable date for the 6th date range.

107
b) Use Date Initiated (in DEMOGRAPHICS) and add 9.9 months to it to determine the latest acceptable date for the 6th date range.
G. 10 to 12.9 months (7mo to 1yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 10 months to it to determine the earliest acceptable date for the 7th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 12.9 months to it to determine the latest acceptable date for the 7th date range.
H. 13 to 18.9 months (1yr 1mo to 1yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 13 months to it to determine the earliest acceptable date for the 8th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 18.9 months to it to determine the latest acceptable date for the 8th date range.
I. 19 to 24.9 months (1yr 7mo to 2yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 19 months to it to determine the earliest acceptable date for the 9th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 24.9 months to it to determine the latest acceptable date for the 9th date range.
J. 25 to 30.9 months (2yr 1mo to 2yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 25 months to it to determine the earliest acceptable date for the 10th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 30.9 months to it to determine the latest acceptable date for the 10th date range.
K. 31 to 36.9 months (2yr 7mo to 3yr) 1. Parameters
a) DEMOGRAPHICS

108
(1) Date Initiated 2. Procedures
a) Use Date Initiated (in DEMOGRAPHICS) and add 31 months to it to determine the earliest acceptable date for the 11th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 36.9 months to it to determine the latest acceptable date for the 11th date range.
L. 37 to 42.9 months (3yr 1mo to 3yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 37 months to it to determine the earliest acceptable date for the 12th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 42.9 months to it to determine the latest acceptable date for the 12th date range.
M. 43 to 48.9 months (3yr 7mo to 4yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 43 months to it to determine the earliest acceptable date for the 13th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 48.9 months to it to determine the latest acceptable date for the 13th date range.
N. 49 to 54.9 months (4yr 1mo to 4yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 49 months to it to determine the earliest acceptable date for the 14th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 54.9 months to it to determine the latest acceptable date for the 14th date range.
O. 55 to 60.9 months (4yr 7mo to 5yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated

109
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 55 months to it to determine the earliest acceptable date for the 15th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 60.9 months to it to determine the latest acceptable date for the 15th date range.
P. 61 to 66.9 months (5yr 1mo to 5yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 61 months to it to determine the earliest acceptable date for the 16th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 66.9 months to it to determine the latest acceptable date for the 16th date range.
Q. 67 to 72.9 months (5yr 7mo to 6yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 67 months to it to determine the earliest acceptable date for the 17th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 72.9 months to it to determine the latest acceptable date for the 17th date range.
R. 73 to 78.9 months (6yr 1mo to 6yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 73 months to it to determine the earliest acceptable date for the 18th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 78.9 months to it to determine the latest acceptable date for the 18th date range.
S. 79 to 84.9 months (6yr 7mo to 7yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures
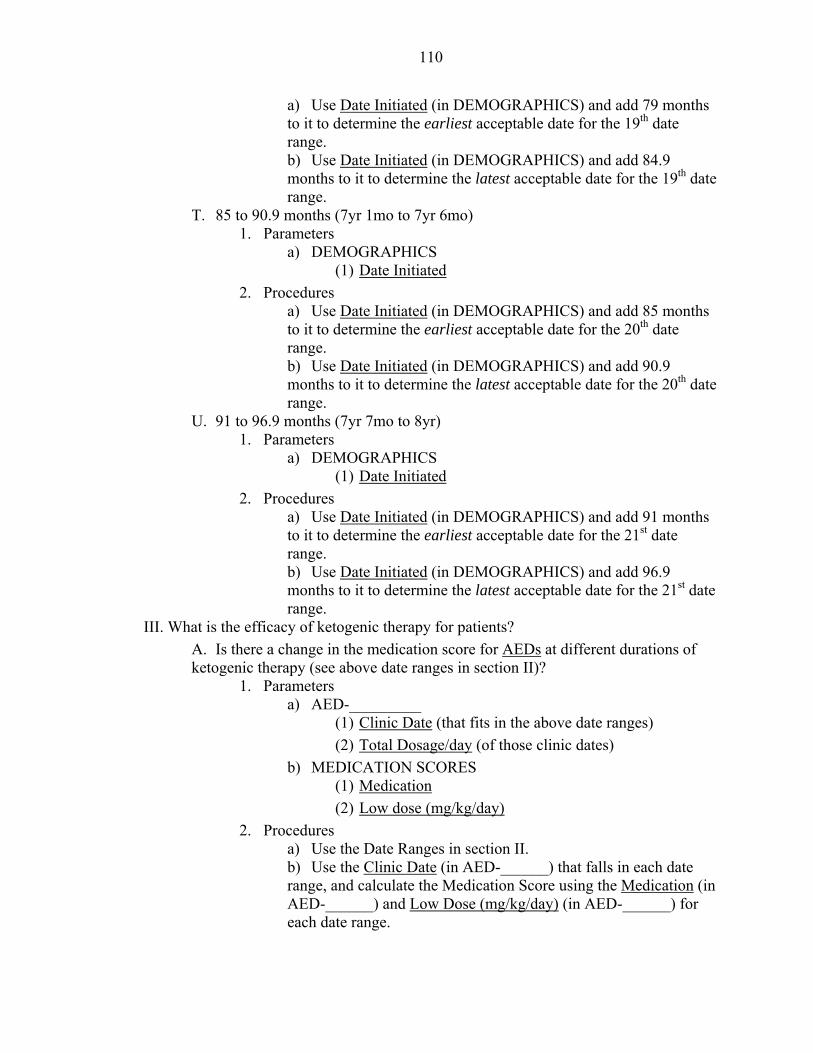
110
a) Use Date Initiated (in DEMOGRAPHICS) and add 79 months to it to determine the earliest acceptable date for the 19th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 84.9 months to it to determine the latest acceptable date for the 19th date range.
T. 85 to 90.9 months (7yr 1mo to 7yr 6mo) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 85 months to it to determine the earliest acceptable date for the 20th date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 90.9 months to it to determine the latest acceptable date for the 20th date range.
U. 91 to 96.9 months (7yr 7mo to 8yr) 1. Parameters
a) DEMOGRAPHICS (1) Date Initiated
2. Procedures a) Use Date Initiated (in DEMOGRAPHICS) and add 91 months to it to determine the earliest acceptable date for the 21st date range. b) Use Date Initiated (in DEMOGRAPHICS) and add 96.9 months to it to determine the latest acceptable date for the 21st date range.
III. What is the efficacy of ketogenic therapy for patients? A. Is there a change in the medication score for AEDs at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) AED-_________
(1) Clinic Date (that fits in the above date ranges) (2) Total Dosage/day (of those clinic dates)
b) MEDICATION SCORES (1) Medication (2) Low dose (mg/kg/day)
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Date (in AED-______) that falls in each date range, and calculate the Medication Score using the Medication (in AED-______) and Low Dose (mg/kg/day) (in AED-______) for each date range.

111
B. Is there a change in the average seizure number per week at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) SEIZURES
(1) Clinic Dates (that fits in the above date ranges) (2) Avg Seizures/Week (of those clinic dates)
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Dates (in SEIZURES) that fall in each date range, and find the Avg Seizures/Week (in SEIZURES) for each date range to determine the change in seizures/week.
IV. How did patients tolerate ketogenic therapy? (How frequently did GI disturbances occur?)
A. What is the frequency of episodes of vomiting, nausea, diarrhea, and constipation in at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) GI ISSUES
(1) Clinic Date (that fits in the above date ranges) and: (2) Vomiting (for those clinic dates) (3) Nausea (for those clinic dates) (4) Diarrhea (for those clinic dates) (5) Constipation (for those clinic dates)
2. Procedures a) Constipation:
(1) Use the Date Ranges in section II. (2) Use the Clinic Dates (in GI ISSUES) that fall in each date range, and find whether or not (yes/no) there was Constipation (in GI ISSUES) for each date range.
b) Diarrhea: (1) Use the Date Ranges in section II. (2) Use the Clinic Dates (in GI ISSUES) that fall in each date range, and find whether or not (yes/no) there was Diarrhea (in GI ISSUES) for each date range.
c) Vomiting: (1) Use the Date Ranges in section II. (2) Use the Clinic Dates (in GI ISSUES) that fall in each date range, and find whether or not (yes/no) there was Vomiting (in GI ISSUES) for each date range.
d) Nausea: (1) Use the Date Ranges in section II.

112
(2) Use the Clinic Dates (in GI ISSUES) that fall in each date range, and find whether or not (yes/no) there was Nausea (in GI ISSUES) for each date range.
V. Which laboratory values appear to be abnormal? A. Are lab values that are recorded abnormal at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) NORMAL RANGES OF LABS
(1) [Found outside of database] b) BLOOD LIPIDS
(1) Clinic Date (2) TG (3) HDL (4) LDL (5) Total Non-HDL Cholesterol (6) Total Cholesterol
c) COMPLETE BLOOD COUNT (1) Clinic Date (2) RBC (3) Hgb (4) Hct (5) Platelet Count (6) MCV (7) MCH (8) MCHC (9) MPV (10) RBC Dist (11) WBC
d) MAGNESIUM, PHOS INORG, URIC ACID (1) Clinic Date (2) Mg (3) Phosph Inorg (4) Uric Acid
e) BETA-HYDROXYBUTYRATE (1) Clinic Date (2) Beta-Hydroxybutyrate
f) METABOLIC PANEL (1) Clinic Date (2) Na (3) K

113
(4) Cl (5) CO2 (6) BUN (7) Creatinine (8) Glu (9) Ca (10) Mg (11) PO4 (12) Uric Acid (13) Protein Total (14) Albumin (15) Bilirubin Total (16) Bilirubin Direct (17) Alkaline (18) AST (19) ALT (20) LDH Total
g) KETONES AND SPECIFIC GRAVITY (1) Clinic Date (2) Ketones (3) Specific Gravity
2. Procedures a) Blood Lipids
(1) Use the Date Ranges in section II. (2) Use the Clinic Date (in BLOOD LIPIDS) that falls in each date range, and compare each value in BLOOD LIPIDS for each date range to the appropriate value in NORMAL RANGES OF LABS.
b) Complete Blood Count (1) Use the Date Ranges in section II. (2) Use the Clinic Date (in COMPLETE BLOOD COUNT) that falls in each date range, and compare each value in COMPLETE BLOOD COUNT for each date range to the appropriate value in NORMAL RANGES OF LABS.
c) Magnesium, Phos Inorg, Uric Acid (1) Use the Date Ranges in section II. (2) Use the Clinic Date (in MAGNESIUM, PHOS INORG, URIC ACID) that falls in each date range, and compare each value in MAGNESIUM, PHOS INORG, URIC ACID for each date range to the appropriate value in NORMAL RANGES OF LABS.

114
d) Beta-Hydroxybutyrate (1) Use the Date Ranges in section II. (2) Use the Clinic Date (in BETA-HYDROXYBUTYRATE) that falls in each date range, and compare each value in BETA-HYDROXYBUTYRATE for each date range to the appropriate value in NORMAL RANGES OF LABS.
e) Metabolic Panel (1) Use the Date Ranges in section II. (2) Use the Clinic Date (in METABOLIC PANEL) that falls in each date range, and compare each value in METABOLIC PANEL for each date range to the appropriate value in NORMAL RANGES OF LABS.
f) Ketones and Specific Gravity (1) Use the Date Ranges in section II. (2) Use the Clinic Date (in KETONES AND SPECIFIC GRAVITY) that falls in each date range, and compare each value in KETONES AND SPECIFIC GRAVITY for each date range to the appropriate value in NORMAL RANGES OF LABS.
VI. How did the ratio prescription change throughout ketogenic therapy? A. What was the ratio prescription at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) DIET PRESCRIPTION
(1) Clinic Date (2) Ratio
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Date (in DIET PRESCRIPTION) that falls in each date range, and find the Ratio (in DIET PRESCRIPTION) for each date range.
VII. What happened to energy intake in relation to the DRI during fine-tuning of the diet for individual patients at initiation and throughout the ketogenic therapy?
A. What was the calorie prescription at different durations of ketogenic therapy (see above date ranges in section II)? Compare the calorie prescriptions to the DRI for calories.
1. Parameters a) DIET PRESCRIPTION
(1) Clinic Date (2) Kcal/kg/day
b) DRI FOR CALORIES (1) [Found outside of database]
2. Procedures

115
a) Use the Date Ranges in section II. b) Use the Clinic Date (in DIET PRESCRIPTION) that falls in each date range, and find the Kcal/kg/day (in DIET PRESCRIPTION) for each date range. c) Compare the Kcal/kg/day (in DIET PRESCRIPTION) to the DRI for Calories.
VIII. How does the calorie prescription compare among the different weights? A. How many calories were prescribed for each weight (or BMI)?
1. Parameters a) DIET PRESCRIPTION
(1) Clinic Date (2) Kcal/kg/day
b) HEIGHT AND WEIGHT (1) Clinic Date (2) Wt (3) Wt % (4) Wt Z-score (5) BMI
2. Procedures a) Use the Clinic Date (in DIET PRESCRIPTION) and find the Kcal/kg/day (in DIET PRESCRIPTION). b) Use the same Clinic Date (in HEIGHT AND WEIGHT) and find the wt, wt %, wt z-score, and BMI (in HEIGHT AND WEIGHT). c) Compare the Kcal/kg/day to the wt, wt %, wt z-score, and BMI.
IX. How has the height and weight of patients changed throughout ketogenic therapy? A. What were the height z-scores at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) HEIGHT AND WEIGHT
(1) Clinic Date (that fits in the above date ranges) (2) Height z-score (of those clinic dates)
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Date (in HEIGHT AND WEIGHT) that falls in each date range, and find the Height z-score (in HEIGHT AND WEIGHT) for each date range.
B. What were the weight z-scores at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) HEIGHT AND WEIGHT
(1) Clinic Date (that fits in the above date ranges) (2) Weight z-score (of those clinic dates)

116
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Date (in HEIGHT AND WEIGHT) that falls in each date range, and find the Weight z-score (in HEIGHT AND WEIGHT) for each date range.
X. How did the amount of MCT given increase or decrease from initiation throughout the ketogenic therapy?
A. What amount of MCT was given at different durations of ketogenic therapy (see above date ranges in section II)?
1. Parameters a) SUP-MINERAL OIL
(1) Clinic Date (2) Total Dosage/day
2. Procedures a) Use the Date Ranges in section II. b) Use the Clinic Date (in SUP-MINERAL OIL) that falls in each date range, and find the Total Dosage/day (in SUP-MINERAL OIL) for each date range.
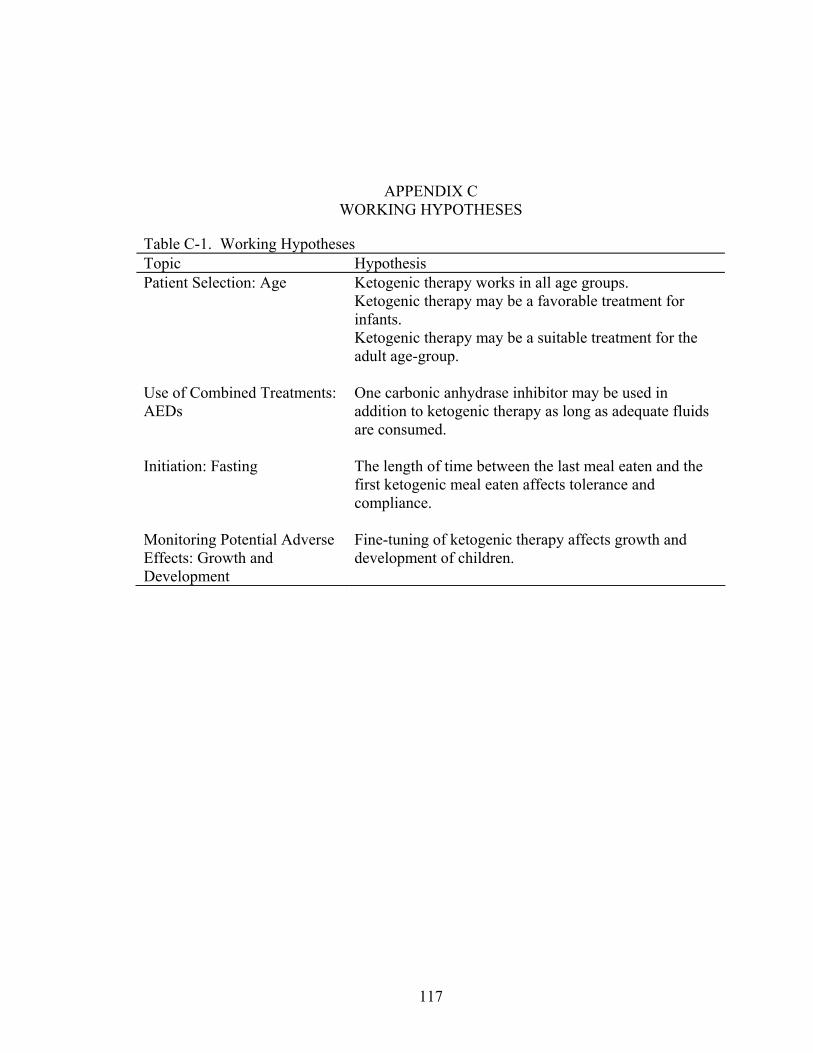
117
APPENDIX C WORKING HYPOTHESES
Table C-1. Working Hypotheses Topic Hypothesis Patient Selection: Age Ketogenic therapy works in all age groups. Ketogenic therapy may be a favorable treatment for
infants. Ketogenic therapy may be a suitable treatment for the
adult age-group. Use of Combined Treatments: AEDs
One carbonic anhydrase inhibitor may be used in addition to ketogenic therapy as long as adequate fluids are consumed.
Initiation: Fasting The length of time between the last meal eaten and the
first ketogenic meal eaten affects tolerance and compliance.
Monitoring Potential Adverse Effects: Growth and Development
Fine-tuning of ketogenic therapy affects growth and development of children.

APPENDIX D TOLERANCE AND COMPLIANCE FORMS

Patient’s Name:______________________________ Date of first meal:________________ Instructions: Circle the appropriate letter, number, or sets of numbers for each meal according to the code box below.
119
Tolerance of Ketogenic Therapy VOMITING
Day Meal # of times per hr Time after meal (hr) Estimated % of meal Nausea
1 1 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
1 2 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
2 1 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
2 2 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
2 3 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
3 1 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
3 2 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
3 3 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
4 1 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
4 2 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
4 3 NA 1 2 3 4 ≥5 NA 0-½ ½-1 1-2 2-4 ≥4 NA 0-24 25-74 75-100 NA C G R
Code Box: NA = Not Applicable NA = Not Applicable
0-½ = During feeding or within first 30 minutes after eating meal
NA = Not Applicable NA = Not Applicable C = Communicated by the pt G = w/ Gagging (upper body) R = w/ Retching/ dry heaving (lower body)

120
Day Meal Who answered the questions? Recorder’s Name
1 1 P M F O:____________
1 2 P M F O:____________
2 1 P M F O:____________
2 2 P M F O:____________
2 3 P M F O:____________
3 1 P M F O:____________
3 2 P M F O:____________
3 3 P M F O:____________
4 1 P M F O:____________
4 2 P M F O:____________
4 3 P M F O:____________
Code Box:
P = Patient M = Mother F = Father O = Other (specify who)
Print name legibly

Patient’s Name:______________________________ Date of first meal:________________
Instructions: Circle the appropriate letter, number, or sets of numbers for each meal according to the code box below.
121
Tolerance of Ketogenic Therapy CONSTIPATION
Date of last stool prior to initiation:________________ Day Meal # of stools during
initiation Consistency Color Gas
1 1 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
1 2 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
2 1 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
2 2 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
2 3 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
3 1 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
3 2 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
3 3 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
4 1 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
4 2 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
4 3 NA 0 1 2 ≥3 NA N LH LS LW Br C G Bl R NA NP WP
Code Box:
NA = Not Applicable NA = Not Applicable N = Normal LH = Large (Hard) LS = Large (Soft) LW = Large (+Watery)
Br = Brown C = Clay G = Green Bl = Black R = Red
NA =Not Applicable NP = No Pain WP = With Pain

122
Day Meal Who answered the questions? Recorder’s Name
1 1 P M F O:____________
1 2 P M F O:____________
2 1 P M F O:____________
2 2 P M F O:____________
2 3 P M F O:____________
3 1 P M F O:____________
3 2 P M F O:____________
3 3 P M F O:____________
4 1 P M F O:____________
4 2 P M F O:____________
4 3 P M F O:____________
Code Box:
P = Patient M = Mother F = Father O = Other (specify who)
Print name legibly
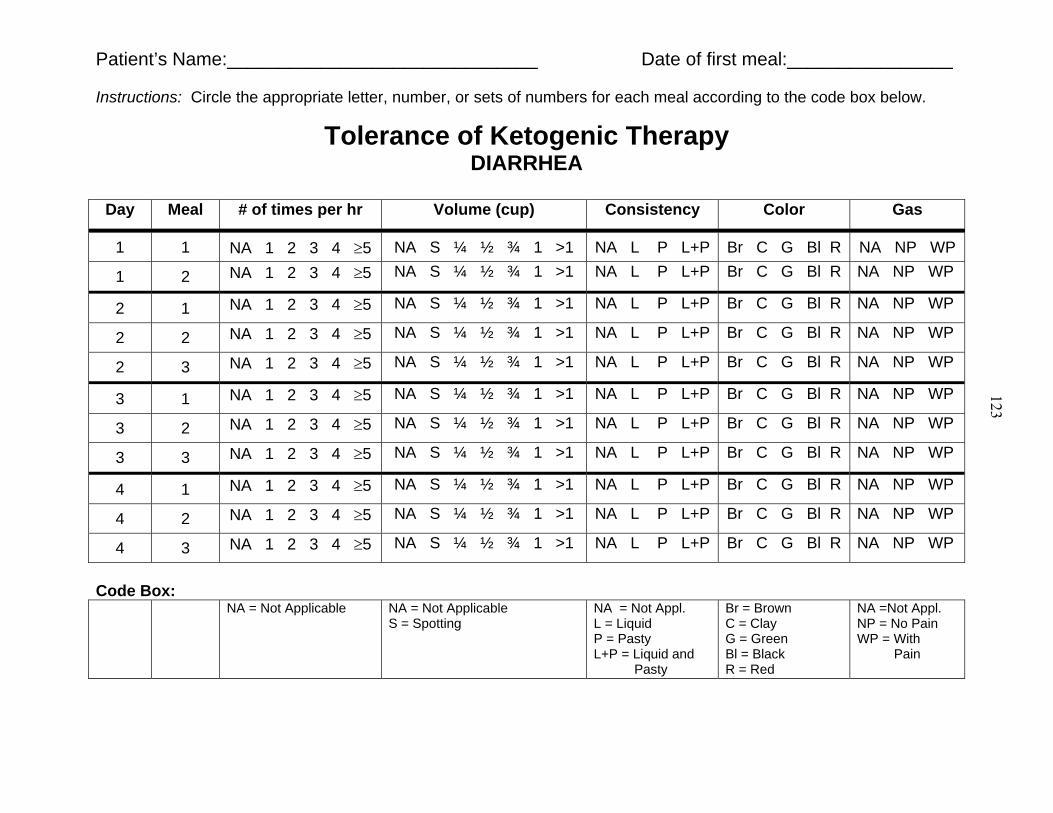
Patient’s Name:______________________________ Date of first meal:________________
Instructions: Circle the appropriate letter, number, or sets of numbers for each meal according to the code box below.
123
Tolerance of Ketogenic Therapy DIARRHEA
Day Meal # of times per hr Volume (cup) Consistency Color Gas
1 1 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
1 2 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
2 1 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
2 2 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
2 3 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
3 1 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
3 2 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
3 3 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
4 1 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
4 2 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
4 3 NA 1 2 3 4 ≥5 NA S ¼ ½ ¾ 1 >1 NA L P L+P Br C G Bl R NA NP WP
Code Box:
NA = Not Applicable NA = Not Applicable S = Spotting
NA = Not Appl. L = Liquid P = Pasty L+P = Liquid and Pasty
Br = Brown C = Clay G = Green Bl = Black R = Red
NA =Not Appl. NP = No Pain WP = With Pain

124
Day Meal Who answered the questions? Recorder’s Name
1 1 P M F O:____________
1 2 P M F O:____________
2 1 P M F O:____________
2 2 P M F O:____________
2 3 P M F O:____________
3 1 P M F O:____________
3 2 P M F O:____________
3 3 P M F O:____________
4 1 P M F O:____________
4 2 P M F O:____________
4 3 P M F O:____________
Code Box:
P = Patient M = Mother F = Father O = Other (specify who)
Print name legibly

Patient’s Name:______________________________ Date of first meal:________________ Instructions: Circle the appropriate letter, number, or sets of numbers for each meal according to the code box below.
125
Compliance of Ketogenic Therapy Normal Eating Habits: 1) Refusal to eat food (throughout the meal): 0 1 2 3 4 2) Length of time to complete a meal (minutes): 0-14 15-29 30-44 45-59 60-90
Code Box:
Day Meal Amount of Meal Consumed (%)
Refusal to Eat Food (throughout the meal)
Length of Time to Complete Meal (minutes)
1 1 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
1 2 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
2 1 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
2 2 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
2 3 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
3 1 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
3 2 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
3 3 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
4 1 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
4 2 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
4 3 0 1-24 25-49 50-74 75-100 0 1 2 3 4 0-14 15-29 30-44 45-59 60-90
0 = No refusal 1 = Eats at first but then refuses 2 = Refuses at first, but then willingly takes bites 3 = Refuses, but takes bites with persistent feeding 4 = Total refusal

126
Day Meal Who answered the questions? Recorder’s Name
1 1 P M F O:____________
1 2 P M F O:____________
2 1 P M F O:____________
2 2 P M F O:____________
2 3 P M F O:____________
3 1 P M F O:____________
3 2 P M F O:____________
3 3 P M F O:____________
4 1 P M F O:____________
4 2 P M F O:____________
4 3 P M F O:____________
Code Box: P = Patient
M = Mother F = Father O = Other (specify who)
Print name legibly

APPENDIX E DIET PRESCRIPTION FORM

Diet Prescription During Initiation of Ketogenic Therapy Patient’s name: ______________________________Date of Initiation:__________________________
Age: ____ Wt: ____(lbs) ____(kg) Ht: ____(in) ____(cm) Date and Time of last meal (prior to initiation):_______________
Instructions: For each meal record the calories, ratio, fluid amounts given, and the time the meal was actually received.
129
DAY 1: _______________ Meal 1 (day 1) Calories Ratio Fluids Time meal given Meal 2 (day 1) Calories Ratio Fluids Time meal given Meal 3 (day 1) Calories Ratio Fluids Time meal given
DAY 2: ________________ Meal 1 (day 2) Calories Ratio Fluids Time meal given Meal 2 (day 2) Calories Ratio Fluids Time meal given Meal 3 (day 2) Calories Ratio Fluids Time meal given
DAY 3: ______________ Meal 1 (day 3) Calories Ratio Fluids Time meal given Meal 2 (day 3) Calories Ratio Fluids Time meal given Meal 3 (day 3) Calories Ratio Fluids Time meal given

129
DAY 4: ______________ Meal 1 (day 4) Calories Ratio Fluids Time meal given Meal 2 (day 4) Calories Ratio Fluids Time meal given Meal 3 (day 4) Calories Ratio Fluids Time meal given
DAY 5: ______________ Meal 1 (day 5) Calories Ratio Fluids Time meal given Meal 2 (day 5) Calories Ratio Fluids Time meal given Meal 3 (day 5) Calories Ratio Fluids Time meal given

APPENDIX F PATIENT/PARENT EDUCATION FORM
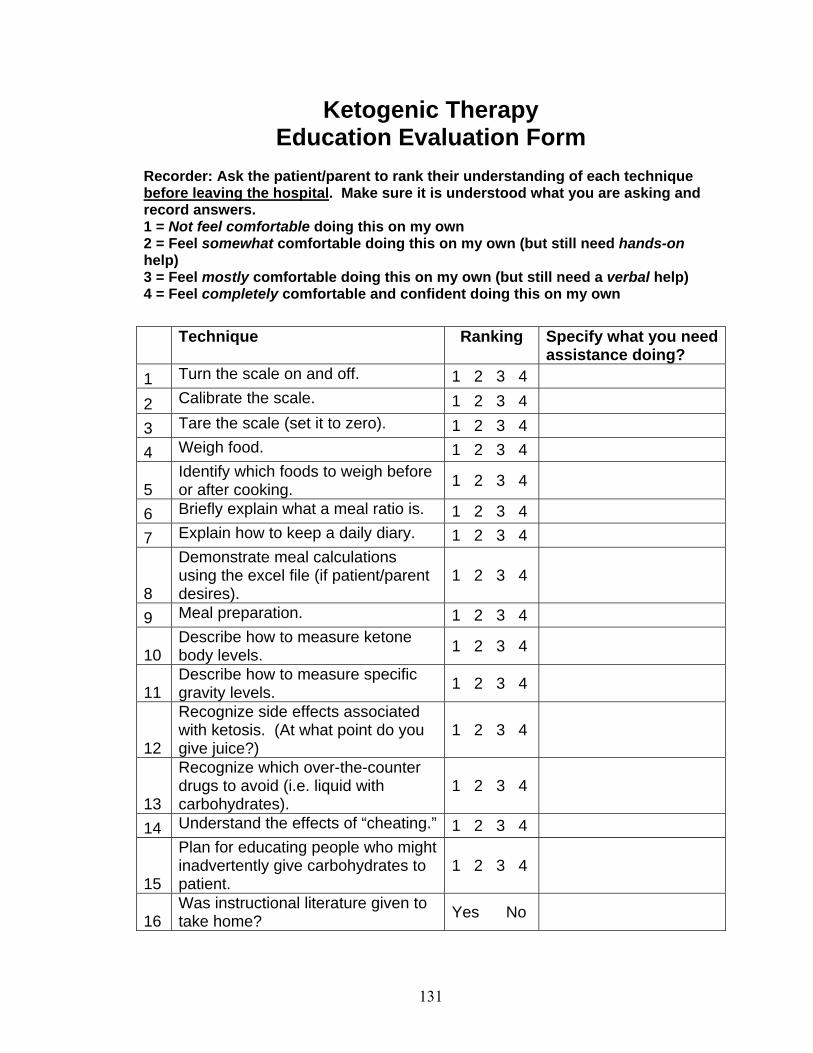
131
Ketogenic Therapy Education Evaluation Form
Recorder: Ask the patient/parent to rank their understanding of each technique before leaving the hospital. Make sure it is understood what you are asking and record answers. 1 = Not feel comfortable doing this on my own 2 = Feel somewhat comfortable doing this on my own (but still need hands-on help) 3 = Feel mostly comfortable doing this on my own (but still need a verbal help) 4 = Feel completely comfortable and confident doing this on my own
Technique Ranking Specify what you need
assistance doing? 1 Turn the scale on and off. 1 2 3 4
2 Calibrate the scale. 1 2 3 4
3 Tare the scale (set it to zero). 1 2 3 4
4 Weigh food. 1 2 3 4
5 Identify which foods to weigh before or after cooking. 1 2 3 4
6 Briefly explain what a meal ratio is. 1 2 3 4
7 Explain how to keep a daily diary. 1 2 3 4
8
Demonstrate meal calculations using the excel file (if patient/parent desires).
1 2 3 4
9 Meal preparation. 1 2 3 4
10 Describe how to measure ketone body levels. 1 2 3 4
11 Describe how to measure specific gravity levels. 1 2 3 4
12
Recognize side effects associated with ketosis. (At what point do you give juice?)
1 2 3 4
13
Recognize which over-the-counter drugs to avoid (i.e. liquid with carbohydrates).
1 2 3 4
14 Understand the effects of “cheating.” 1 2 3 4
15
Plan for educating people who might inadvertently give carbohydrates to patient.
1 2 3 4
16 Was instructional literature given to take home? Yes No

132
LIST OF REFERENCES
1. Edelstein, S. F. & Chisholm, M. (1996) Management of intractable childhood seizures using the non-MCT oil ketogenic diet in 20 patients. J. Am. Diet. Assoc. 96: 1181-1182. 2. Freeman, J. M., Vining, E. P., Pillas, D. J., Pyzik, P. L., Casey, J. C. & Kelly, L. M. (1998) The efficacy of the ketogenic diet-1998: a prospective evaluation of intervention in 150 children. Pediatrics 102: 1358-1363. 3. Hassan, A. M., Keene, D. L., Whiting, S. E., Jacob, P. J., Champagne, J. R. & Humphreys, P. (1999) Ketogenic diet in the treatment of refractory epilepsy in childhood. Pediatr. Neurol. 21: 548-552. 4. Hemingway, C., Freeman, J. M., Pillas, D. J. & Pyzik, P. L. (2001) The ketogenic diet: a 3- to 6-year follow-up of 150 children enrolled prospectively. Pediatrics 108: 898-905. 5. Katyal, N. G., Koehler, A. N., McGhee, B., Foley, C. M. & Crumrine, P. K. (2000) The ketogenic diet in refractory epilepsy: the experience of Children's Hospital of Pittsburgh. Clin. Pediatr. (Phila) 39: 153-159. 6. Lefevre, F. & Aronson, N. (2000) Ketogenic diet for the treatment of refractory epilepsy in children: a systematic review of efficacy. Pediatrics 105: E46. 7. Mady, M. A., Kossoff, E. H., McGregor, A. L., Wheless, J. W., Pyzik, P. L. & Freeman, J. M. (2003) The ketogenic diet: adolescents can do it, too. Epilepsia 44: 847-851. 8. Maydell, B. V., Wyllie, E., Akhtar, N., Kotagal, P., Powaski, K., Cook, K., Weinstock, A. & Rothner, A. D. (2001) Efficacy of the ketogenic diet in focal versus generalized seizures. Pediatr. Neurol. 25: 208-212. 9. Sheth, R. D. & Stafstrom, C. E. (2002) Intractable pediatric epilepsy: vagal nerve stimulation and the ketogenic diet. Neurol. Clin. 20: 1183-1194. 10. Crumrine, P. K. (2002) Lennox-Gastaut Syndrome. J. Child Neurol. 17: S70-S75.

133
11. Schwartz, R. H., Eaton, J., Bower, B. D. & Aynsley-Green, A. (1989) Ketogenic diets in the treatment of epilepsy: short-term clinical effects. Dev. Med. Child Neurol. 31: 145-151. 12. Wheless, J. W. (2001) The ketogenic diet: an effective medical therapy with side effects. J. Child Neurol. 16: 633-635. 13. Sankar, R. & de Menezes, M. (1999) Metabolic and endocrine aspects of the ketogenic diet. Epilepsy Res. 37: 191-201. 14. Zupec-Kania, B., Werner, R. R. & Zupanc, M. L. (2004) Clinical use of the ketogenic diet: the dietitian's role. In: Epilepsy and the ketogenic diet (Stafstrom, C. E. & Rho, J. M., eds.), pp. 63-81. Humana Press, Totowa, New Jersey. 15. Kinsman, S. L., Vining, E. P., Quaskey, S. A., Mellits, D. & Freeman, J. M. (1992) Efficacy of the ketogenic diet for intractable seizure disorders: review of 58 cases. Epilepsia 33: 1132-1136. 16. Prasad, A. N., Stafstrom, C. F. & Holmes, G. L. (1996) Alternative epilepsy therapies: the ketogenic diet, immunoglobulins, and steroids. Epilepsia 37 Suppl 1: S81-95. 17. Klepper, J., Leiendecker, R., Bredahl, S., Athanassopoulos, S., Heinen, F., Gertsen, E., Florcken, A., Metz, A. & Voit, T. (2002) Introduction of a ketogenic diet in young infants. J. Inherit. Metab. Dis. 25: 449-460. 18. Tallian, K. B., Nahata, M. C. & Tsao, C. Y. (1998) Role of the ketogenic diet in children with intractable seizures. Ann. Pharmacother. 32: 349-361. 19. Nordli, D. R., Jr., Kuroda, M. M., Carroll, J., Koenigsberger, D. Y., Hirsch, L. J., Bruner, H. J., Seidel, W. T. & De Vivo, D. C. (2001) Experience with the ketogenic diet in infants. Pediatrics 108: 129-133. 20. Klepper, J., De Vivo, D. C., Webb, D. W., Klinge, L. & Voit, T. (2003) Reversible infantile hypoglycorrhachia: possible transient disturbance in glucose transport? Pediatr. Neurol. 29: 321-325. 21. Nordli Jr, D. R. & De Vivo, D. C. (1997) The ketogenic diet revisited: back to the future. Epilepsia 38: 743-749. 22. Kossoff, E. H., Pyzik, P. L., McGrogan, J. R., Vining, E. P. & Freeman, J. M. (2002) Efficacy of the ketogenic diet for infantile spasms. Pediatrics 109: 780-783. 23. Schwartz, R. M., Boyes, S. & Aynsley-Green, A. (1989) Metabolic effects of three ketogenic diets in the treatment of severe epilepsy. Dev. Med. Child Neurol. 31: 152-160.

134
24. Sirven, J., Whedon, B., Caplan, D., Liporace, J., Glosser, D., O'Dwyer, J. & Sperling, M. R. (1999) The ketogenic diet for intractable epilepsy in adults: preliminary results. Epilepsia 40: 1721-1726. 25. Coppola, G., Veggiotti, P., Cusmai, R., Bertoli, S., Cardinali, S., Dionisi-Vici, C., Elia, M., Lispi, M. L., Sarnelli, C., Tagliabue, A., Toraldo, C. & Pascotto, A. (2002) The ketogenic diet in children, adolescents and young adults with refractory epilepsy: an Italian multicentric experience. Epilepsy Res. 48: 221-227. 26. Vining, E. P. (1999) Clinical efficacy of the ketogenic diet. Epilepsy Res. 37: 181-190. 27. Freeman, J. M., Freeman, J. B. & Kelly, M. T. (2000) The ketogenic diet: a treatment for epilepsy, 3 ed. Demos Medical Publishing, Inc., New York, NY. 28. (1997-2003) On-line Medical Dictionary. Dept. of Medical Oncology, University of Newcastle upon Tyne. <http://cancerweb.ncl.ac.uk/omd/>, Nov. 20, 2003. 29. (2003) Dictionary.com. Lexico Publishing Group, LLC. <http://dictionary.reference.com/>, Nov. 20, 2003. 30. Miller, V., Palermo, T. & Grewe, S. (2003) Quality of life in pediatric epilepsy: demographic and disease-related predictors and comparison with healthy controls. Epilepsy & Behavior 4: 36-42. 31. Mandel, A., Ballew, M., Pina-Garza, J. E., Stalmasek, V. & Clemens, L. H. (2002) Medical costs are reduced when children with intractable epilepsy are successfully treated with the ketogenic diet. J. Am. Diet. Assoc. 102: 396-398. 32. Gilbert, D. L., Pyzik, P. L., Vining, E. P. & Freeman, J. M. (1999) Medication cost reduction in children on the ketogenic diet: data from a prospective study. J. Child Neurol. 14: 469-471. 33. Ballaban-Gil, K., Callahan, C., O'Dell, C., Pappo, M., Moshe, S. & Shinnar, S. (1998) Complications of the ketogenic diet. Epilepsia 39: 744-748. 34. Takeoka, M., Riviello, J. J., Jr., Pfeifer, H. & Thiele, E. A. (2002) Concomitant treatment with topiramate and ketogenic diet in pediatric epilepsy. Epilepsia 43: 1072-1075. 35. Wilner, A., Raymond, K. & Pollard, R. (1999) Topiramate and metabolic acidosis. Epilepsia 40: 792-795. 36. Kossoff, E. H., Pyzik, P. L., Furth, S. L., Hladky, H. D., Freeman, J. M. & Vining, E. P. (2002) Kidney stones, carbonic anhydrase inhibitors, and the ketogenic diet. Epilepsia 43: 1168-1171.

135
37. Taking comfort in knowing the vagus nerve stimulator: options in seizure management. In: An introduction to seizure disorders and existing therapies (Jurasek, G., ed. EP Foundation for Education, Inc. 38. McNeely, J. K. (2000) Perioperative management of a paediatric patient on the ketogenic diet. Paediatr. Anaesth. 10: 103-106. 39. Vining, E. P., Freeman, J. M., Ballaban-Gil, K., Camfield, C. S., Camfield, P. R., Holmes, G. L., Shinnar, S., Shuman, R., Trevathan, E. & Wheless, J. W. (1998) A multicenter study of the efficacy of the ketogenic diet. Arch. Neurol. 55: 1433-1437. 40. Kossoff, E. H. (2004) More fat and fewer seizures: dietary therapies for epilepsy. The Lancet Neurology 3: 415-420. 41. (1999) Clinical pathway: ketogenic treatment program/intractable epilepsy. Shands Hospital at the University of Florida. 42. Wirrell, E. C., Darwish, H. Z., Williams-Dyjur, C., Blackman, M. & Lange, V. (2002) Is a fast necessary when initiating the ketogenic diet? J. Child Neurol. 17: 179-182. 43. MacCracken, K. A. & Scalisi, J. C. (1999) Development and evaluation of a ketogenic diet program. J. Am. Diet. Assoc. 99: 1554-1558. 44. Nevin-Folino, N., ed. (1998) The American Dietetic Association pediatric manual of clinical dietetics, 1st ed. The American Dietetic Association, Chicago. 45. Kleinman, R. E., ed. (2004) Pediatric nutrition handbook, 5 ed. American Academy of Pediatrics, Elk Grove Village, IL. 46. McClernon, C. S. & Acree, B. (2000) Ketogenic diet. In: The Florida Dietetic Association diet manual, 2000 ed. (Christie, C. & Mitchell, S., eds.). The Florida Dietetic Association, n.p. 47. Chesney, D., Brouhard, B. H., Wyllie, E. & Powaski, K. (1999) Biochemical abnormalities of the ketogenic diet in children. Clin. Pediatr. (Phila) 38: 107-109. 48. Gilbert, D. L., Pyzik, P. L. & Freeman, J. M. (2000) The ketogenic diet: seizure control correlates better with serum beta-hydroxybutyrate than with urine ketones. J. Child Neurol. 15: 787-790. 49. Choi-Kwon, S., Yoon, S. M., Choi, M. R., Kang, D. W. & Lee, S. K. (2001) The difference in perceptions of educational needs between epilepsy patients and medical personnel. Epilepsia 42: 785-789.

136
50. Kossoff, E. H., Krauss, G. L., McGrogan, J. R. & Freeman, J. M. (2003) Efficacy of the Atkins diet as therapy for intractable epilepsy. Neurology 61: 1789-1791. 51. (2002) Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Institute of Medicine, National Academy of Sciences, Washington, DC. 52. Couch, S., Schwarzman, F., Carroll, J., Koenigsberger, D., Nordli Jr, D. R., Deckelbaum, R. & DeFelice, A. (1999) Growth and nutritional outcomes of children treated with the ketogenic diet. J. Am. Diet. Assoc. 99: 1573-1575. 53. Freeman, J. M. & Vining, E. P. (1998) Ketogenic diet: a time-tested, effective, and safe method for treatment of intractable childhood epilepsy. Epilepsia 39: 450-451. 54. Vining, E. P., Pyzik, P., McGrogan, J., Hladky, H., Anand, A., Kriegler, S. & Freeman, J. M. (2002) Growth of children on the ketogenic diet. Dev. Med. Child Neurol. 44: 796-802. 55. Furth, S. L., Casey, J. C., Pyzik, P. L., Neu, A. M., Docimo, S. G., Vining, E. P., Freeman, J. M. & Fivush, B. A. (2000) Risk factors for urolithiasis in children on the ketogenic diet. Pediatr. Nephrol. 15: 125-128. 56. Hemingway, C., McGrogan, J. & Freeman, J. M. (2001) Energy requirements of spasticity. Dev. Med. Child Neurol. 43: 277-278. 57. Williams, S., Basualdo-Hammond, C., Curtis, R. & Schuller, R. (2002) Growth retardation in children with epilepsy on the ketogenic diet: a retrospective chart review. J. Am. Diet. Assoc. 102: 405-407. 58. Bergqvist, A. G. C., Chee, C. M., Lutchka, L. M. & R., B.-K. A. (1999) Treatment of acquired epileptic aphasia with the ketogenic diet. J. Child Neurol. 14: 696-701. 59. Pulsifer, M. B., Gordon, J. M., Brandt, J., Vining, E. P. & Freeman, J. M. (2001) Effects of ketogenic diet on development and behavior: preliminary report of a prospective study. Dev. Med. Child Neurol. 43: 301-306. 60. Kwiterovich Jr, P., Vining, E. P., Pyzik, P., Skolasky Jr, R. & Freeman, J. M. (2003) Effect of a high-fat ketogenic diet on plasma levels of lipids, lipoproteins, and apolipoproteins in children. J. Am. Med. Assoc. 290: 912-920. 61. Huttenlocher, P. R. (1976) Ketonemia and seizures: metabolic and anticonvulsant effects of two ketogenic diets in childhood epilepsy. Pediatr. Res. 10: 536-540.

137
62. Liu, Y. M., Williams, S., Basualdo-Hammond, C., Stephens, D. & Curtis, R. (2003) A prospective study: growth and nutritional status of children treated with the ketogenic diet. J. Am. Diet. Assoc. 103: 707-712. 63. DiMario, F. J., Jr. & Holland, J. (2002) The ketogenic diet: a review of the experience at Connecticut Children's Medical Center. Pediatr. Neurol. 26: 288-292. 64. Wheless, J. W., Baumgartner, J. & Ghanbari, C. (2001) Vagus nerve stimulation and the ketogenic diet. Neurol. Clin. 19: 371-407. 65. Best, T. H., Franz, D. N., Gilbert, D. L., Nelson, D. P. & Epstein, M. R. (2000) Cardiac complications in pediatric patients on the ketogenic diet. Neurology 54: 2328-2330. 66. Berry-Kravis, E., Booth, G., Taylor, A. & Valentino, L. A. (2001) Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann. Neurol. 49: 98-103. 67. Stewart, W. A., Gordon, K. & Camfield, P. (2001) Acute pancreatitis causing death in a child on the ketogenic diet. J. Child Neurol. 16: 682. 68. Kielb, S., Koo, H. P., Bloom, D. A. & Faerber, G. J. (2000) Nephrolithiasis associated with the ketogenic diet. J. Urol. 164: 464-466.

138
BIOGRAPHICAL SKETCH
Mandy Hammond Layman was born in Birmingham, Alabama, on July 24, 1980.
She and her two older brothers, Chad and Kyle, were born to Randy and Carolyn
Hammond. She started her college education at Samford University and received a
Bachelor of Science degree in nutrition/dietetics in May 2002. She moved to Gainesville,
Florida 3 months later and began the Master of Science – Dietetic Internship (MS-DI)
program at the University of Florida (UF). She quickly became interested in the
ketogenic therapy program at Shands Hospital and decided to work on a thesis with Dr.
Peggy Borum, a long-time advocate of the ketogenic therapy as a treatment for epilepsy.
She married Zack Layman from Montevallo, Alabama, during her time at UF in May
2003. In her spare time, she enjoys spending time with friends and family, traveling,
staying active mostly by running, and drawing. Mandy and her husband will soon move
to Orlando, Florida, where she plans to become a pediatric clinical dietitian.