guidelines for implementation of enhanced recovery...
TRANSCRIPT
GUIDELINES FORIMPLEMENTATION OF
ENHANCED RECOVERYPROTOCOLS
December 2009

www.asgbi.org.uk

1
Association of Surgeons of Great Britain and Ireland
ISSUES IN PROFESSIONAL PRACTICE
GUIDELINES FORIMPLEMENTATION OF
ENHANCED RECOVERYPROTOCOLS
AUTHORS
Mr Shakeeb Khan, MBBS, MRCS
Mr Marcel Gatt, MD, FRCS
Mr Alan Horgan, MD, FRCSConsultant Colorectal Surgeon and National Lead for
Enhanced Recovery Programmes, National Cancer Action Team.
Mr Iain Anderson, MD, FRCSConsultant Colorectal Surgeon and Director of Education,
Association of Surgeons of Great Britain and Ireland.
Professor John MacFie, MD, FRCSConsultant Colorectal Surgeon and Vice President,
Association of Surgeons of Great Britain and Ireland.
PUBLICATION DATEDecember 2009
PUBLISHED BYAssociation of Surgeons of Great Britain and Ireland
35-43 Lincoln’s Inn Fields, London, WC2A 3PE

2
FOREWORD
Issues in Professional Practice is an occasional series of bookletspublished by the Association of Surgeons of Great Britain andIreland to offer guidance on a wide range of areas which impact onthe daily professional lives of surgeons. Some topics will focus onclinical issues, some will cover management and service delivery,whist others will feature broader aspects of surgical working lifesuch as education, leadership and the law.
Peri-operative surgical care is undergoing a paradigm shift.Traditional practices such as prolonged pre-operative fasting (“nilby mouth from midnight”), bowel cleansing and the use ofnasogastric decompression are being shunned. These, and othersimilar changes, have been formulated into protocols calledEnhanced Recovery after Surgery (ERAS) pathways, and thisbooklet offers Guidelines for Implementation of EnhancedRecovery Protocols.
The Association hopes that this publication, and the others in theseries to follow, will provide concise advice and guidance on majorcurrent issues, and grow into a helpful and accessible resource tosupport your professional practice.
Suggestions for any potential topics for future booklets in theIssues in Professional Practice series would be gratefully received.
Professor Michael HorrocksPresident

3
CONTENTS
Page No.
Summary of Recommendations 4
Introduction 5
Components of Enhanced Recoveryand current recommendations 6
Special circumstances 16
Elderly and high risk patients
Emergency surgery
Setting up an ERAS protocol and improving compliance 17
Future research 19
Quality of life
Laparoscopic surgery
Gut specific nutrients
Index 20
References 21
ABBREVIATIONS
ERAS Enhanced recovery after surgery
FTc Velocity of blood flow in the descending aorta
QoL Quality of life
SV Stroke volume
TEDs Thrombo-embolic Deterrent stockings
PCA Patient controlled analgesia
PONV Postoperative nausea and vomiting

4
SUMMARY OF RECOMMENDATIONS
Peri-operative surgical care is undergoing a paradigm shift.Traditional practices such as prolonged pre-operative fasting (“nilby mouth from midnight”), bowel cleansing and the use ofnasogastric decompression are being shunned. These, and othersimilar changes, have been formulated into protocols calledEnhanced Recovery after Surgery (ERAS) pathways. TheAssociation of Surgeons of Great Britain and Ireland’s currentrecommendations on ERAS are summarised below and will bepresented in more detail in this document:
Pre-operative recommendations
1) Pre-operative counselling and training.
2) A curtailed fast (6 hours to solids and 2 hours to clear liquids)and pre-operative carbohydrate loading.
3) Avoidance of mechanical bowel preparation.
4) Deep vein thrombosis prophylaxis using low molecular weightheparin.
5) A single dose of prophylactic antibiotics covering both aerobicand anaerobic pathogens.
Peri-operative recommendations
1) High (80%) inspired oxygen concentration in the peri-operativeperiod.
2) Prevention of hypothermia.
3) Goal directed intra-operative fluid therapy.
4) Preferable use of short and transverse incisions for opensurgery.
5) Avoidance of post-operative drains and nasogastric tubes.
6) Short duration of epidural analgesia and local blocks.
Post-operative recommendations
1) Avoidance of opiates and the use of Paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDS).
2) Early commencement of post-operative diet.
3) Early and structured post-operative mobilisation.
4) Administration of restricted amounts of intravenous fluid.
5) Regular audit.

5
INTRODUCTION
Enhanced recovery after surgery (ERAS) protocols, also known as‘fast-track surgery’ or ‘multimodal optimisation’, are a combinationof evidence based peri-operative strategies which worksynergistically to expedite recovery after surgery [1, 2]. Thesestrategies include, for example, a curtailed pre-operative fast, pre-operative carbohydrate loading, pre-emptive analgesia and earlypost-operative mobilisation together with expedited re-introductionof diet and fluids. Although each of these individual strategies isbeneficial, to some extent, on its own, to achieve maximum benefitthey have to be used together in the form of a package. UsingERAS protocols, post-operative stays following colorectal resectioncan be safely reduced to around two to four days. This expediteddischarge is not achieved by lowering the prerequisites for releasefrom hospital, but rather by fulfilling standard discharge criteriaearlier due to an accelerated post-operative phase. The advantagesof ERAS have been repeatedly borne out in a number ofrandomised clinical trials and meta-analyses. The underlyingmechanism of ERAS protocols is thought to be an attenuation ofthe peri-operative stress response [3-5], although there is increasingevidence to suggest that benefits of ERAS are actually mediated byreturn of organ, particularly gut function [6].
The purpose of this document is threefold: To present the variouscomponents of enhanced recovery along with the rationale behindtheir inclusion; to suggest strategies to facilitate theirimplementation and compliance in day-to-day clinical practice,and; to propose directions for future research. Specific emphasisshall be given to ERAS in colorectal surgery as a reflection of themajority of research having been performed in this field. Many ofthe strategies are, however, transferrable to other branches ofsurgery. It is also noteworthy that different ERAS protocols havebeen trialled and validated in the literature. They have all beenshown to produce similar results, suggesting that protocols can betailored to take into account local requirements and availableresources. Nonetheless, it must be emphasised that the principles ofERAS presented in this document are guidelines only and may notbe applicable, particularly in the care of patients undergoingcomplex procedures.

6
COMPONENTS OF ERAS PROTOCOLS AND CURRENTRECOMMENDATIONS
Components of ERAS protocols can be broadly categorised intopre-operative, peri-operative and post-operative interventions.These shall be considered in turn, together with a brief review ofthe evidence and current recommendations.
Pre-operative components
1) Pre-operative counselling and training:
Recommendation: All patients undergoing elective surgery shouldbe counselled. Patients should be provided with both verbal as wellas written information.
All patients undergoing elective surgery should be counselledadequately. This process involves not only members of the surgicalteam who will be directly involved with the proposed procedure,but should also include other health professionals, such asphysiotherapists, dieticians, stoma and nutrition nurses, who willalso be involved in the peri-operative care of the patient. Someunits have a dedicated ERAS nurse. Counselling necessitates closecollaboration between all members of the surgical team and theprovision of both written and verbal information. Provision of thisinformation to patients may occur in the out-patient clinic, the pre-assessment clinic or the patient’s home. Patient information leafletson ERAS should be produced to facilitate patient education.Information discussed should include:
i.) What enhanced recovery involves, its core components andenvisaged benefits.
ii.) What the patient should expect during the course of thehospital stay. This should include specifics of how ERASis implemented locally and which modalities are employed.
iii.) Specific issues which may delay discharge (such as lack ofsocial support).
iv.) Clear and specific instructions should be given aboutmobilisation, early introduction of diet and breathingexercises. Active participation of the patients themselves intheir recovery should be sought, and daily targets for thepatient to achieve should be set up.
v.) Patients who may require a stoma should be identified andappropriately trained such that they are proficient at stomacare, ideally prior to surgery [7].
Pre-operative information and education has been shown toimprove patient satisfaction [8, 9], allay anxiety [10] and improve pain[11] and other outcomes [12].

7
2) Curtailed fasting and preoperative carbohydrate loading
Recommendation: Patients should be fasted for 6 hours to solidsbut they should be allowed small amounts of clear free fluids for upto 2 hours before induction of general anaesthesia. In addition, aclear carbohydrate rich drink (e.g. Polycal Liquid® (NutriciaClinical Ltd, Trowbridge, Wiltshire, UK), Preload® (VitafloInternational Ltd. Liverpool, UK), Maxijul® (SHS- Nutrition,Liverpool, UK)) should be administered orally the night beforesurgery and 3 hours prior to induction of anaesthesia.
Fasting for a minimum of 8 hours before a general anaesthetic hasbeen normal surgical practice for many years. It aims to reduce thevolume and acidity of stomach contents, thereby reducing the riskof regurgitation or aspiration. Recent studies, however, havedemonstrated that a short (3 hour) period of fasting after ingestionof clear fluids is safe and more acceptable to patients. Thisminimises patient thirst and improves post-operative well being. Ashort fast in combination with pre-operative carbohydrate loadinghas been shown to maintain nitrogen balance and reduce post-operative insulin resistance [13-15]. Carbohydrate loading involves theadministration of apposite carbohydrate drinks, such as PolycalLiquid® (200 ml), the night before surgery and 3 hours prior tosurgery. Each carton of Polycal Liquid® liquid provides 494 Kcal,equivalent to approximately 120 grams of carbohydrates. Anycommercially available preparation may be used. However, careshould be taken that the formulation used is clear and residue free.
Special circumstances:Non-insulin dependent diabetics: Pre-operative carbohydrate loadinghas been shown to be safe in non-insulin dependent diabeticpatients, and their use is also recommended in this subgroup ofpatients. In diabetic patients, a pre-operative carbohydrate load hasnot been shown to result in adverse effects such as hyper-glycaemiaor delayed gastric emptying. However, monitoring of blood glucoselevels should be carried out at regular intervals [16].
3) Avoidance of mechanical bowel preparation:
Recommendation: Oral mechanical bowel preparation should notbe used routinely in patients undergoing colonic resection. Ifclearance of the rectum is required for a left sided anastomosis, asingle phosphate enema on the morning of the surgery may be usedto evacuate the rectum.
Oral mechanical bowel clearing has traditionally been thought toreduce the severity of sepsis in the event of an anastomotic leak.However, a number of meta-analyses have suggested that, inpatients undergoing colorectal procedures, the avoidance ofmechanical bowel preparation is safe and does not result inincreased sepsis in the event of an anastomotic leak [17-20].

8
Additionally, the use of mechanical bowel preparation can result inserious adverse events, such as fluid imbalance, in certain patientsubgroups, including the elderly. We recognise that the evidence foromitting bowel preparation in patients undergoing rectal surgeryalone is equivocal.
4) Deep vein thrombosis prophylaxis
Recommendation: All patients undergoing surgery should bestarted on a once daily low molecular weight heparin (Enoxaparin20 mg) the night before surgery and continued for the entire lengthof the patient’s hospital stay. In addition, graduated compressionthromboembolic deterrent stockings (TEDs) should be used. Duringthe procedure, pneumatic mechanical compression stockings shouldbe used. Prophylaxis should be considered for up to one monthafter discharge, especially in those at a higher risk ofthromboembolic complications, such as those with residualmalignancy or previous episodes of thrombosis.
A single daily dose of low molecular weight heparin isrecommended for deep vein thrombosis prophylaxis because of itsease of administration and lower risk of bleeding complications [21].The use of low molecular weight heparin in conjunction withgraduated compression stockings was found to be the mosteffective anti-thromboprohylactic prophylaxis in a recent Cochranereview [22, 23]. There is an increased risk of thrombotic complicationsup to one month after surgery, due to a hypercoaguble state, andprolonged (up to 1 month after discharge) antithromboticprophylaxis with low molecular weight heparin confers significantbenefit in terms of reduction of thrombotic complications [24, 25].
5) Antibiotic prophylaxis
Recommendation: A single dose of antibiotics, covering bothaerobic and anaerobic organisms, should be administered justprior to incising the skin. In prolonged procedures (more than 4hours) or if there is major blood loss (greater than 1500 mls.) asecond dose may be administered.
Antibiotic prophylaxis is used to reduce the rates of woundinfection after surgery. Multiple doses have not been found toconfer any additional advantages and result in increased costs andrisk of infections such as Clostridium difficile. For this reason, asingle dose of antibiotics covering both aerobic and anaerobicorganisms should be administered just prior to incising the skin inall clean procedures which do not involve the insertion ofprosthetic materials. When deciding the type of antibiotic used,local resistance patterns should be considered. Increased risk ofacquiring a Clostridium difficile infection after using a third

9
generation cephalosporin should also be considered. In those whoare known to be carriers of MRSA (Methicillin resistantStaphylococcus aureus), prophylaxis with a glycopeptide antibiotic(Vancomycin, Teicoplanin) should be considered.
Peri-operative components
1) High inspired oxygen concentrations
Recommendation: Eighty percent (80%) oxygen should beadministered during anaesthesia and then continued for at least 6hours postoperatively. A face mask may be required to deliver thishigh concentration of oxygen.
Molecular oxygen is required by polymorphonuclear cells toproduce free radicals which form an important line of defenceagainst pathogens [26-28]. In addition, it plays an important role inthe synthesis of collagen for wound healing and angiogenensis.Higher tissue oxygenation levels in the immediate post-operativeperiod as a result of 80% inspired oxygen have been shown toimprove perfusion at the anastomotic site and reduce the risk ofsurgical site infections [29]. In addition, there is some evidence thatit may also reduce postoperative nausea and vomiting (PONV)although this is contentious [30, 31].
2) Prevention of hypothermia
Recommendation: Hypothermia (core temperature less than36°C) should be actively prevented using warm-air blankets.Warming should be continued for as long as the patient is inrecovery. If the procedure is expected to last for more than anhour, then warmed intravenous fluids should be used. Anoesophageal probe should be used during the procedure formeasurement of core body temperature.
General anaesthesia can disrupt the normal thermoregulatoryprocesses and result in hypothermia. In addition, exposure of thepatient to the cold theatre environment also contributes.Hypothermia (core temperature less than 36°C) can, in turn, leadto an increase in the incidence of surgical site infections, thoughtto be due to peripheral vasoconstriction induced hypoxia [32, 33] andan altered immune response. Other undesirable effects ofhypothermia include coagulopathy [34], increased cardiacmorbidity [35] and increased levels of circulating catecholamineswith a resultant exaggerated catabolic response [36]. Activeprevention of hypothermia during the peri-operative period hasbeen shown to reduce blood loss and prevent infective [33, 37] andcardiac complications [38].

10
For these reasons, hypothermia should be actively prevented usingwarm-air blankets. Warming should be continued for as long as thepatient is in recovery. If the procedure is expected to last for morethan an hour, then warmed intravenous fluids should be used [39, 40].An oesophageal probe should be used during the procedure formeasurement of core body temperature.
3) Goal directed intra-operative fluid therapy
Recommendation: An oesophageal Doppler probe (or otherminimally invasive methods of stroke volume measurement suchas LiDCO plus™ and LiDCO rapid™) should be used tocontinuously measure the cardiac output, and fluidadministration should be titrated according to variations in thecardiac output.
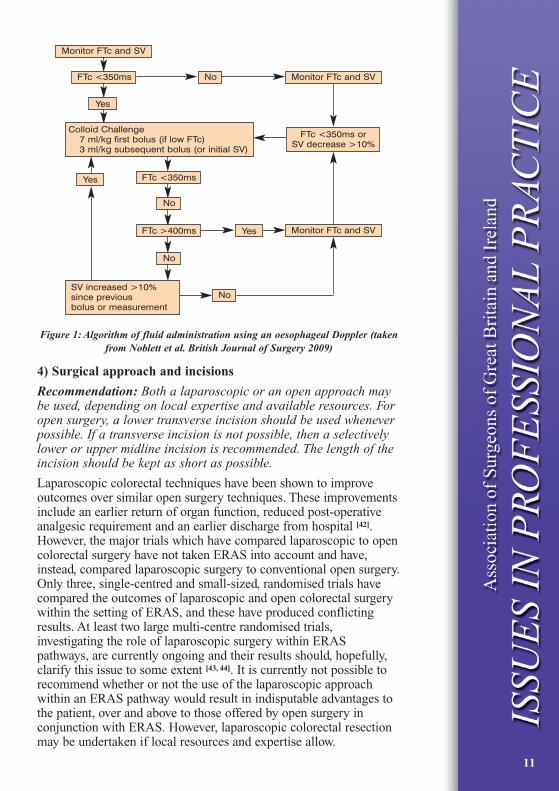
A degree of intra-operative splanchnic hypoperfusion may goundetected with conventional monitoring, and this plays animportant role in post-operative delay of return of gut function.In addition, occult hypoperfusion can lead to bacterialtranslocation across the gut wall which can result in sepsissyndrome. On the other hand, the administration of excessiveamounts of fluid during surgery can also result in delayed returnof gut function and cardiac morbidity. An oesophageal Dopplerprobe is a minimally invasive method of determining thehemodynamic status in the peri-operative period and allowsguided fluid management targeted against indicators of cardiacoutput. The intra-operative use of an oesophageal Doppler probehas been shown to accelerate the return of gut function andexpedite discharge after surgery [41]. The haemodynamic status ofthe patient should first be optimised using an oesophagealDoppler probe such that the cardiac output is maximum. Furtherboluses of colloids (on a background of maintenance fluids)should then be administered against variations in stroke volume(SV) and velocity of blood flow in the descending aorta (FTc). Ifresources do not permit the universal use of oesophagealDoppler, then its use may be restricted to high risk (ASA 3 andabove) and elderly patients. A schema for administering Dopplerguided fluid is shown in Figure 1.
Other minimally invasive methods of optimising the fluidbalance include LiDCO plus™ and LiDCO rapid™ and may beused instead of the oesophageal Doppler. These systems dependon a Lithium dilution technique to measure changes inhaemodynamic parameters, such as cardiac output and strokevolume, and provide continuous real-time measurements.
11
Figure 1: Algorithm of fluid administration using an oesophageal Doppler (takenfrom Noblett et al. British Journal of Surgery 2009)
4) Surgical approach and incisions
Recommendation: Both a laparoscopic or an open approach maybe used, depending on local expertise and available resources. Foropen surgery, a lower transverse incision should be used wheneverpossible. If a transverse incision is not possible, then a selectivelylower or upper midline incision is recommended. The length of theincision should be kept as short as possible.
Laparoscopic colorectal techniques have been shown to improveoutcomes over similar open surgery techniques. These improvementsinclude an earlier return of organ function, reduced post-operativeanalgesic requirement and an earlier discharge from hospital [42].However, the major trials which have compared laparoscopic to opencolorectal surgery have not taken ERAS into account and have,instead, compared laparoscopic surgery to conventional open surgery.Only three, single-centred and small-sized, randomised trials havecompared the outcomes of laparoscopic and open colorectal surgerywithin the setting of ERAS, and these have produced conflictingresults. At least two large multi-centre randomised trials,investigating the role of laparoscopic surgery within ERASpathways, are currently ongoing and their results should, hopefully,clarify this issue to some extent [43, 44]. It is currently not possible torecommend whether or not the use of the laparoscopic approachwithin an ERAS pathway would result in indisputable advantages tothe patient, over and above to those offered by open surgery inconjunction with ERAS. However, laparoscopic colorectal resectionmay be undertaken if local resources and expertise allow.
Yes
Yes
Yes FTc <350ms
FTc >400ms
FTc <350ms No Monitor FTc and SV
Monitor FTc and SV
Monitor FTc and SV
No
No
No
Colloid Challenge7 ml/kg first bolus (if low FTc)3 ml/kg subsequent bolus (or initial SV)
SV increased >10%since previousbolus or measurement
FTc <350ms orSV decrease >10%

12
When undertaking open procedures, a number of considerationsneed to be borne in mind. Short transverse incisions are thought tobe less painful, impair lung function to a lesser extent, and reducesubsequent post-operative analgesic requirement when comparedto vertical wounds. In addition, there is some evidence that theincidence of wound dehiscence may be reduced in transverseincisions. These were the conclusions of a Cochrane review in2005 [45]. However, the results of a recent large randomized trialdid not find that transverse incisions were less painful thanlongitudinal ones [46].
5) Avoidance of post-operative drains and nasogastric tubes
Recommendation: Routine abdominal drains and nasogastric tubesshould be avoided. If gastric decompression is required duringsurgery, a nasogastric tube may be inserted temporarily andremoved at the end of the procedure.
Nasogastric tubes may be painful and cause considerablediscomfort. This can render post-operative mobilisation difficult.There is good evidence that routine use of nasogastricdecompression delays the return of gut function, leads to anincrease in pulmonary complication and fever and prolongshospital stay. These findings are supported by at least two meta-analyses [47-49].
Abdominal drains have been traditionally placed to evacuate post-operative collections at the site of surgery and drain any possibleanastomotic leak. However, similar to nasogastric tubes, theycause considerable discomfort and can hinder mobilisation.Moreover, at least three meta-analyses have revealed that routineprophylactic drainage of the abdominal cavity does not confer anyadvantages [50-52].
6) Short duration of epidural analgesia and local blocks
Recommendation: All patients undergoing open colorectal surgeryshould receive epidural analgesia. It should be initiated at thebeginning of the procedure and continued for a maximum of 48hours. Weaning from epidural analgesia should start 12 hours post-operatively. Care should be taken that the equipment does notinterfere with mobilisation. Patients undergoing laparoscopicresection may or may not be administered epidural analgesiadepending upon the preference of the operating surgeon andanaesthetist.
A fine bore catheter placed into the epidural space at the level ofT9 and T10 can be used to deliver a mixture of a short actingopiate (Fentanyl 2mcg/ml) and a local anaesthetic solution(Bupivacaine 0.15%). This results in a blockade of the spinal

13
nerves. Epidurals analgesia directly attenuates the post-operativestress response and promotes the return of gut function by blockingthe sympathetic activity [53, 54]. However, this sympathetic blockadecan result in hypotension due to vasodilatation which can provedifficult to manage as it may not respond to intravenous fluids. Inthese situations, an early decision to transfer the patient to a highdependency unit must be taken and inotropic or vasopressorsupport initiated. Another disadvantage is that the equipment caninterfere with postoperative mobilisation. Whenever epidurals areutilised, these should be initiated at the beginning of the procedureand continued for a maximum of 48 hours. Weaning from epiduralanalgesia should start 12 hours post-operatively. Alternatives toepidural analgesia include transversus abdominis plane (TAP)blocks and other infiltrations with local anaesthetic aimed atreducing post-operative opiate usage.
The role of epidural analgesia in relation to laparoscopic colorectalsurgery is not clear. A small number of studies have questioned theuse of epidural analgesia in the setting of laparoscopic surgery.They argue that analgesic requirements after laparoscopic surgeryare lower and, as such, epidurals may not have an added advantageand, on the other hand, only increase the risk of epidural relatedcomplications [55-57]. However, a small number of trials haveproduced contradictory results and have shown that additionaladvantages may be obtained when epidurals and laparoscopicsurgery are used together [58, 59]. The current evidence level is weakand insufficient to advocate the universal use of epidural analgesiain laparoscopic colorectal resection. However, this should notpreclude the surgeon or the anaesthetist to use epidural analgesiafor laparoscopic surgery if they deem it to be safe and useful intheir local setting.
Post-operative Components
1) Avoidance of opiates and the use of Paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDS)
Recommendation: Post-operatively, patients should be prescribedregular Paracetamol and NSAIDS such as Ibuprofen or Diclofenacif there are no contraindications to their use. Opiates, includingCodeine preparations and Tramadol, should only be reserved forbreakthrough pain. Whenever opiates are used, attention should bepaid to prevent nausea and vomiting and regular antiemeticsprescribed.
Early return of gut function and prevention of its various adversesequels is thought to be one of the underlying mechanisms bywhich ERAS protocols work. Opiates are known to delay the returnof gut function and should be avoided whenever possible. Inaddition, they can cause considerable post-operative nausea and

14
vomiting (PONV). Opiate minimisation should include theavoidance of Codeine and Tramadol preparations as well as opiatecontaining patient controlled analgesia (PCA) infusions. In theirstead, patients should be prescribed paracetamol and NSAIDS, ifthere are no contraindications to their use. Opiates should be usedonly for purposes of rescue analgesia. Liberal use of antiemeticsshould be employed, but the limitation of these medications inexpediting the recovery of post-operative gut function should berecognised [60].
2) Early postoperative diet
Recommendation: Patients should be allowed oral fluids astolerated on the day of the surgery and built up to an oral diet overthe next 24 hours. Patients who are not meeting their nutritionalrequirements by 72 hours after surgery should be assessed by adietician.
Traditionally, oral diet and fluid has been reintroduced cautiouslyand gradually after bowel surgery, often rendering the patients nilby mouth or on oral sips only for many days in the post-operativeperiod. This, it was thought, was necessary for adequate healing ofbowel anastomoses. However, recently, early introduction of dietand fluids (within 24 hours post-operatively) has been shown to besafe [61, 62]. In addition, there is some evidence that early feedingmay be beneficial in reducing the risks of anastomotic dehiscence,infections and reducing the length of stay [63]. In our view, toleranceto early feeding provides a more objective evaluation of gutfunction than assessment on the basis of bowel sounds of passageof flatus.
3) Early postoperative mobilisation
Recommendation: A structured mobilisation plan should be inplace. Patients should be helped to sit out in a chair on the eveningof surgery and definitely by the first post-operative day. This shouldbe followed by gentle assisted mobilisation either the same day orthe next day. Patients should be seen by a named physiotherapistpre-operatively with the aim of explaining the mobilisation plan.This physiotherapist should then help enforce this plan throughoutthe post-operative period.
Even short periods of immobilisation can lead to deleteriousconsequences such as thromboembolism, loss of muscle strength,pulmonary atelectasis and worsening of pulmonary function.Continuous patient education regarding the benefits of mobilisationis recommended. It was shown in a randomised trial that avoidanceof bed-side entertainment systems is one pragmatic approach toencourage mobilisation [64].

15
4) Restricted amounts of intravenous fluid
Recommendation: It is not possible to recommend a single point intime by which all intravenous fluid administration should bestopped. However, in the majority of patients, this should bepossible by the second post-operative day, by which time adequateoral fluids should be tolerated and indwelling epidural cathetersremoved.
During the post-operative phase, intravenous fluids may be requiredas long as adequate oral fluid intake has not been achieved and/orepidural catheters are still in situ. However, excessive amounts ofintravenous fluid should be avoided. A daily regime of 1.5 to 2.5 Lshould suffice for most patents. The ability of individuals to get ridof accumulated sodium is greatly curtailed in the post-operativeperiod. For this and other reasons, balanced intravenous solutionssuch as Hartmann’s™ should be prescribed in preference to NormalSaline (0.9% NaCl) in an attempt to avoid sodium overload,hyperchloremic acidosis and a delayed return of gut function [65].
5) Audit
Recommendation: Clinical outcomes, including readmission ratesand compliance to the various ERAS strategies, should be regularlyaudited. Readmission rates after ERAS implementation should notexceed 10%. Audit findings should be discussed in regular auditmeetings attended by medical, nursing and other ancillary staff.Results should also be disseminated using the local IT systems suchas the intranet and e-mail.
A perceived disadvantage of many ERAS protocols is that, bydischarging patients home sooner, one is simply transferring theirresponsibility on to primary care providers whilst also predisposingpatients to higher readmission rates, despite the risks associatedwith such practices. This has not been borne out in trials, where theemphasis was to enhance patients’ recovery in preference to “fasttracking” patients through their hospital stay [66].
Continued audit should permit such problems to be detected early,and necessary modifications made to discharge criteria, so as toensure that patients receive the best possible care. Readmissionrates after ERAS implementation should not exceed 10%.Additionally, a continuous audit cycle should ensure detection ofany institutional problems associated with ERAS implementationas well ascertaining a continuously up-to-date and evidenced basedERAS practice.

16
SPECIAL CIRCUMSTANCES
1) Elderly patients and those with high co-morbidity
Such patients have been shown to benefit from enhanced recoveryand should be included in these programmes. There is no evidencefor concern in including ASA 3 and 4 patients into ERASprogrammes, although the literature in this area is limited [67].Elderly patients may not be able to cope at home after discharge ifthere is no one to assist them. This may delay patient discharge,cognisant of the fact that the overarching aim of ERAS is toenhance post-operative recovery, not to discharge patients homeearlier. The elderly may require a degree of input after dischargeand this may be in the form of regular telephone calls, a home-visitby a healthcare professional or even by a relative. Therefore,discharge planning should be initiated at a very early stage forthese patients.
Certain components of ERAS protocols may be even more relevantin this cohort of patients. For example, Doppler guided fluidtherapy may be particularly useful in the elderly and high riskpatients in whom accurate fluid administration is possibly moreimportant due to the increased risk of fluid overload.
2) Emergency surgery
Although ERAS pathways have been primarily studied in theelective setting, they should still be applied to the emergencysituation. Although in emergencies implementation of the pre-operative components may not be possible, every effort should bemade to implement as many components as possible [68].

17
SETTING UP AN ERAS PATHWAY AND IMPROVINGCOMPLIANCE
Enhanced recovery programmes require a multi-disciplinaryapproach and co-ordination. This can render their initiation andimplementation difficult. Compliance to these packages has oftenbeen reported to be low, especially in the post-operative period andoutwith the remits of clinical trials.Factors which can facilitateintroduction and implementation of enhanced recovery pathwaysand improve protocol compliance include:
1) Selected anaesthetic input
Patients should be managed by a selected group of anaesthetistswho are committed to the concept of enhanced recovery.
2) Patients should be managed on specific wards
The management of patients by a select group of medical andnursing staff trained in the principles of enhanced recovery mayimprove compliance. If resources permit, specialised unitsdedicated to implementing ERAS called ‘Enhanced RecoveryUnits’ should be set up. This may facilitate the organisationalaspects of running ERAS protocols. Such units can also play a rolein patient education, where patients are continuously reminded ofthe importance of their active participation in the success ofenhanced recovery. This may be facilitated by direct staff contact aswell as by using apposite posters and pamphlets.
3) Continuous staff education
The majority of strategies of ERAS pathways are simple measureswhich can be implemented by junior medical and nursing staff.Therefore, whenever junior medical staff rotate into a unit thatpractices enhanced recovery, targeted teaching sessions should beheld to ensure that all staff are familiar with the practices of the unit.
4) A multidisciplinary team approach
An ERAS team should be in place and should comprise one ormore surgeons, anaesthetists, nurses, dieticians andphysiotherapists. These individuals should be ‘signed up’ to theconcept of enhanced recovery. In the majority of hospitals, itshould not be necessary to expand the work force to formulate suchteams and a reconfiguration and collaboration of existing servicesshould be sufficient. The ERAS team may replace and take over therole of other previously existing teams such as the PainManagement Team whose members can, in turn, be trained to be apart of the new ERAS team. This would ensure that aspects such aspain control are dealt with in accordance with the principles ofERAS. In addition to the clinical care, the ERAS team should take

up additional roles such as ensuring compliance, auditing outcomesand continuous staff and patient education to facilitateimplementation of ERAS.
5) A local champion
Successful implementation of enhanced recovery packagesnecessitates a local ‘champion’. Such a person is essential tocoordinate the various aspects of enhanced recovery packages frompre-assessment until discharge. This may be any senior member ofthe ERAS multi-disciplinary team outlined above.
6) Audit and research
Regular auditing and dissemination of results should beundertaken. Wherever possible, an active research programme onERAS related issues is recommended. Regular audit and researchcan facilitate the development of local ERAS protocols tailored tothe specific requirements of the institution.
18

19
FUTURE RESEARCH
The safety and applicability of ERAS, in terms of reducing thepost-operative length of stay and morbidity, is well established fromwell designed randomised clinical trials and meta-analyses.However, certain issues related to ERAS require further research:
1) Influence on quality of life (QoL) and patient satisfaction
Although ERAS pathways have not been shown to adverselyinfluence patient satisfaction or quality of life, the full impact ofthe various strategies employed, as well as earlier discharge fromhospital after major surgery, requires further research for a betterunderstanding [69].
2) Role of laparoscopic surgery within an ERAS programme
Both laparoscopic surgery and ERAS significantly shorten post-operative lengths of stay. However, whether or not the inclusion oflaparoscopic surgery within a successful ERAS protocol offers anyfurther advantage to that of ERAS alone is not clear. There iscurrently no adequately powered study in the literature to answerthis question, but the results of on-going appropriately designedstudies are awaited [43, 44]. Current evidence seems to suggest that, inthe presence of a well implemented ERAS pathway, similar resultscan be obtained with or without the laparoscope. Future researchshould also compare the costs and quality of life after inclusion ofthe laparoscopic approach within an ERAS pathway.
3) Inclusion of gut specific nutrients in ERAS pathways
ERAS pathways are thought to work by preserving organ functionand particularly gut function. Glutamine is a conditionallyessentially amino acid which is used as a preferential nutrientsource by the gut enterocytes and cells of the immune system.Glutamine levels are known to be sub-normal in catabolic statessuch as after surgery, trauma or burns. Preliminary research hasshown that pre-operative oral Glutamine supplementation reducesseptic complications and length of stay after surgery. However,further research in the form of well designed and appropriatelypowered randomised trials is required [70-73].
4) Cost-benefit analysis
Whilst it is self-evident to some that ERAS should be cost effective,targeted studies investigating the cost-benefit interplay of ERASprotocols are conspicuous by their scarcity [74-77]. A sound economicbasis for implementing ERAS protocols in various surgicalspecialties would greatly enhance the argument in favour of ERAS.In many branches of surgery, such studies are eagerly awaited.

20
INDEX
Antibiotic prophylaxis 8
Audit 15, 18
Deep vein thrombosis prophylaxis 8
Diabetics 7
Education 6
Elderly patients 16
Emergency surgery 16
Enhanced recovery units 17
Epidural analgesia 12
Glutamine 19
Goal directed intra-operative fluid therapy 10
Gut specific nutrients 19
High (80%) inspired oxygen concentration 9
Hypothermia 9
Incisions 11
Intravenous fluids 11
Laparoscopic surgery 11, 19
Local blocks 12
Mechanical bowel preparation 7
Nasogastric tubes 12
Non steroidal anti-inflammatory drugs (NSAIDS) 13
Oesophageal Doppler 10
Opiates 13
Postoperative diet 14
Postoperative mobilisation 14
Preoperative counselling and training 6
Preoperative fasting 7
Preoperative carbohydrate loading 7
Quality of life 19
Research 19
Staff education 19
Surgical drains 12
Thromboembolic deterrent stockings (TEDs) 8

21
REFERENCES[1] Kehlet H, Wilmore D W. Fast-track surgery. British Journal of Surgery 2005; 92: 3–4
[2] Kehlet H, Wilmore D W. Evidence-based surgical care and the evolution of fast-tracksurgery. Ann Surg. 2008 Aug;248(2):1 89-98.
[3] Kehlet H, Wilmore D W. Multimodal strategies to improve surgical outcome. Am JSurg. 2002 Jun; 183(6):630-41.
[4] Fearon K C H, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong C H, Lassen Ket al. Enhanced recovery after surgery: A consensus review of clinical care for patientsundergoing colonic resection. Clinical Nutrition 2005; 24: 466-477
[5] Basse L, Raskov H H, Hjort Jakobsen D, Sonne E, Billesbølle P, Hendel H W,Rosenberg J, Kehlet H. Accelerated postoperative recovery programme after colonicresection improves physical performance, pulmonary function and body composition.Br J Surg. 2002 Apr;89(4):446-53
[6] Gatt M, Anderson A D, Reddy B S, Hayward-Sampson P, Tring I C, MacFie J.Randomized clinical trial of multimodal optimization of surgical care in patientsundergoing major colonic resection. Br J Surg 2005; 92: 1354–1362.
[7] Gatt M, Reddy B S, Mainprize K S. Day-case stoma surgery: is it feasible? Surgeon.2007 Jun;5(3):143-7
[8] Disbrow E A, Bennett H L, Owings J T. Effect of preoperative suggestion onpostoperative gastrointestinal motility. West J Med 1993; 158: 488–492.
[9] Lee A, Gin T. Educating patients about anaesthesia: effect of various modes on patients’knowledge, anxiety and satisfaction. Curr Opin Anaesthesiol. 2005 Apr;18(2):205-8
[10] Kiyohara L Y, Kayano L K, Oliveira L M,Yamamoto M U, Inagaki M M, Ogawa N Y etal. Surgery information reduces anxiety in the pre-operative period. Rev Hosp Clin Fac MedSao Paulo. 2004 Apr;59(2):51-6.
[11] Egbert L D, Battit G E, Welch C E, Bartlett M K. Reduction of postoperative pain byencouragement and instruction of patients. A study of doctor–patient rapport. N EnglJ Med 1964;270:825–7.
[12] Kruzik N. Benefits of preoperative education for adult elective surgery patients. AORNJ. 2009 Sep;90(3):381-7.
[13] Soop M, Nygren J, Thorell A, Weidenhielm L, Lundberg M, Hammarqvist F,Ljungqvist O. Preoperative oral carbohydrate treatment attenuates endogenousglucose release 3 days after surgery. Clin Nutr. 2004 Aug;23(4):733-41
[14] Svanfeldt M, Thorell A, Hausel J, Soop M, Rooyackers O, Nygren J, Ljungqvist O.Randomized clinical trial of the effect of preoperative oral carbohydrate treatment onpostoperative whole-body protein and glucose kinetics.. Br J Surg. 2007Nov;94(11):1342-50
[15] Nygren J, Soop M, Thorell A, Efendic S, Nair K S, Ljungqvist O. Preoperative oralcarbohydrate administration reduces postoperative insulin resistance. Clin Nutr. 1998Apr;17(2):65-71.
[16] Gustafsson U O, Nygren J, Thorell A, Soop M, Hellström P M, Ljungqvist O,Hagström-Toft E. Pre-operative carbohydrate loading may be used in type 2 diabetespatients. Acta Anaesthesiol Scand. 2008 Aug;52(7):946-51
[17] Guenaga K K, Matos D, Wille-Jørgensen P. Mechanical bowel preparation for electivecolorectal surgery. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001544. Review
[18] Pineda C E, Shelton A A, Hernandez-Boussard T, Morton J M, Welton M L.Mechanical bowel preparation in intestinal surgery: a meta-analysis and review of theliterature. J Gastrointest Surg. 2008 Nov;12(11):2037-44. Epub 2008 Jul 12.
[19] Bucher P, Mermillod B, Gervaz P, Morel P. Mechanical bowel preparation for electivecolorectal surgery: a meta-analysis. Arch Surg. 2004 Dec;139(12):1359-64; discussion 1365
[20] Slim K, Vicaut E, Launay-Savary M V, Contant C, Chipponi J. Updated systematicreview and meta-analysis of randomized clinical trials on the role of mechanical bowelpreparation before colorectal surgery. Ann Surg. 2009 Feb;249(2):203-9. Review
[21] Levine M N, Raskob G, Landefeld S, Kearon C. Hemorrhagic complications ofanticoagulant treatment. Chest. 2001 Jan;119(1 Suppl):108S-121S.

22
[22] Gould M K, Dembitzer A D, Doyle R L, Hastie T J, Garber A M. Low-molecular-weight heparins compared with unfractionated heparin for treatment of acute deepvenous thrombosis. A meta-analysis of randomized, controlled trials. Ann Intern Med.1999 May 18;130(10):800-9.
[23] Wille-Jørgensen P, Rasmussen M S, Andersen B R, Borly L. Heparins and mechanicalmethods for thromboprophylaxis in colorectal surgery. Cochrane Database ofSystematic Reviews 2004, Issue 1. Art. No.: CD001217.DOI:10.1002/14651858.CD001217.
[24] Rasmussen M S, Jørgensen L N, Wille-Jørgensen P. Prolonged thromboprophylaxiswith Low Molecular Weight heparin for abdominal or pelvic surgery. CochraneDatabase of Systematic Reviews 2009, Issue 1. Art. No.: CD004318. DOI:10.1002/14651858.CD004318.pub2.
[25] Huo M H, Muntz J. Extended thromboprophylaxis with low-molecular-weightheparins after hospital discharge in high-risk surgical and medical patients: a review.Clin Ther. 2009 Jun;31(6):1129-41. Review.
[26] Babior B M. Oxygen-dependent microbial killing by phagocytes. N Engl J Med1978;298:659-68.
[27] Allen D B, Maguire J J, Mahdavian M, et al. Wound hypoxia and acidosis limitneutrophil bacterial killing mechanisms. Arch Surg 1997;132: 991-6.
[28] Hopf H W, Hunt T K, West J M, et al. Wound tissue oxygen tension predicts the risk ofwound infection in surgical patients. Arch Surg. 1997;132(9):997-1004.
[29] Qadan M, Akça O, Mahid S S, Hornung C A, Polk HC Jr. Perioperative supplementaloxygen therapy and surgical site infection: a meta-analysis of randomized controlledtrials. Arch Surg. 2009 Apr;144(4):359-66; discussion 366-7.
[30] Greif R, Laciny S, Rapf B, Hickle R S, Sessler D I. S upplemental oxygen reduces theincidence of postoperative nausea and vomiting. Anesthesiology 1999; 91: 1246–1252.
[31] Orhan-Sungur M, Kranke P, Sessler D, Apfel C C Does supplemental oxygen reducepostoperative nausea and vomiting? A meta-analysis of randomized controlled trials.Anesth Analg. 2008 Jun;106(6):1733-8.
[32] Ozaki M, Sessler D I, Suzuki H, Ozaki K, Tsunoda C, Atarashi K. Nitrous oxidedecreases the threshold for vasoconstriction less than sevoflurane or isoflurane.Anesth Analg. 1995 Jun;80(6):1212-6.
[33] Melling A C, Ali B, Scott E M, Leaper D J. Effects of preoperative warming on theincidence of wound infection after clean surgery: a randomised controlled trial.Lancet. 2001 Sep 15;358(9285):876-80
[34] Schmied H, Kurz A, Sessler D I, Kozek S, Reiter A. Mild hypothermia increases bloodloss and transfusion requirements during total hip arthroplasty. Lancet. 1996 Feb3;347(8997):289-92.
[35] Frank S M, Fleisher L A, Breslow M J, Higgins M S, Olson K F, Kelly S, Beattie C.Perioperative maintenance of normothermia reduces the incidence of morbid cardiacevents. A randomized clinical trial. JAMA. 1997 Apr 9;277(14):1127-34.
[36] Frank S M, Higgins M S, Breslow M J, Fleisher L A, Gorman R B, Sitzmann J V, RaffH, Beattie C. The catecholamine, cortisol, and hemodynamic responses to mildperioperative hypothermia. A randomized clinical trial. Anesthesiology. 1995Jan;82(1):83-93.
[37] Wong P F, Kumar S, Bohra A, Whetter D, Leaper D J. Randomized clinical trial ofperioperative systemic warming in major elective abdominal surgery. Br J Surg. 2007Apr;94(4):421-6.
[38] Elmore J R, Franklin D P, Youkey J R, Oren J W, Frey C M. Normothermia isprotective during infrarenal aortic surgery. J Vasc Surg. 1998 Dec;28(6):984-94.
[39] Smith C E, Gerdes E, Sweda S, Myles C, Punjabi A, Pinchak A C, Hagen J F.Warming intravenous fluids reduces perioperative hypothermia in women undergoingambulatory gynecological surgery. Anesth Analg. 1998 Jul;87(1):37-41
[40] Lindwall R, Svensson H, Söderström S, Blomqvist H. Forced air warming andintraoperative hypothermia. Eur J Surg. 1998 Jan;164(1):13-6.
[41] Noblett S E, Snowden C P, Shenton B K, Horgan A F. Randomized clinical trialassessing the effect of Doppler-optimized fluid management on outcome after electivecolorectal resection. Br J Surg. 2006 Sep;93(9):1069-7.

23
[42] Reza M M, Blasco J A, Andradas E, Cantero R, Mayol J. Systematic review oflaparoscopic versus open surgery for colorectal cancer. Br J Surg. 2006Aug;93(8):921-8.
[43] Wind J, Hofland J, Preckel B, Hollmann M W, Bossuyt P M, Gouma D J, et al.Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodalmanagement versus standard care (LAFA trial). BMC Surg. 2006 Nov 29;6:16
[44] Conventional versus laparoscopic surgery for colorectal cancer within an enhancedprogramme. www.octo-oxford.org.uk/alltrials/trials/EnROL.html
[45] Brown S R, Goodfellow P B. Transverse verses midline incisions for abdominalsurgery. Cochrane Database Syst Rev. 2005 Oct 19;(4):CD005199.
[46] Seiler C M, Deckert A, Diener M K, Knaebel H P, Weigand M A, Victor N, Büchler MW. Midline versus transverse incision in major abdominal surgery: a randomized,double-blind equivalence trial (POVATI: ISRCTN60734227). Ann Surg. 2009Jun;249(6):913-20
[47] Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominalsurgery. Cochrane Database Syst Rev. 2007 Jul 18;(3):CD004929.
[48] Cheatham M L, Chapman W C, Key S P, Sawyers J L. A meta-analysis of selectiveversus routine nasogastric decompression after elective laparotomy. Ann Surg. 1995May;221(5):469-76
[49] Nelson R, Tse B, Edwards S. Systematic review of prophylactic nasogastricdecompression after abdominal operations. Br J Surg. 2005 Jun;92(6):673-80.
[50] Karliczek A, Jesus E C, Matos D, Castro A A, Atallah A N, Wiggers T. Drainage ornondrainage in elective colorectal anastomosis: a systematic review and meta-analysis.Colorectal Dis. 2006 May;8(4):259-65.
[51] Jesus E C, Karliczek A, Matos D, Castro A A, Atallah A N. Prophylactic anastomoticdrainage for colorectal surgery. Cochrane Database Syst Rev. 2004 Oct18;(4):CD002100
[52] Urbach D R, Kennedy E D, Cohen M M. Colon and rectal anastomoses do not requireroutine drainage: a systematic review and meta-analysis. Ann Surg. 1999Feb;229(2):174-80
[53] Holte K, Kehlet H. Epidural anaesthesia and analgesia - effects on surgical stressresponses and implications for postoperative nutrition. Clin Nutr. 2002Jun;21(3):199-206
[54] Marret E, Remy C, Bonnet F. Postoperative Pain Forum Group. Meta-analysis ofepidural analgesia versus parenteral opioid analgesia after colorectal surgery. Br JSurg. 2007 Jun;94(6):665-73
[55] Neudecker J, Schwenk W, Junghans T, Pietsch S, Böhm B, Müller J M. Randomizedcontrolled trial to examine the influence of thoracic epidural analgesia onpostoperative ileus after laparoscopic sigmoid resection. Br J Surg. 1999Oct;86(10):1292-5
[56] Zafar N, Davies R, Greenslade G L, Dixon A R. The evolution of analgesia in an“Accelerated” recovery programme for resectional laparoscopic colorectal surgerywith anastomosis. Colorectal Dis. 2009 Jan 16. “Accepted Article”; doi: 10.1111/j.1463-1318.2009.01768.x
[57] Levy B F, Tilney H S, Dowson H M, Rockall T A. A systematic review of post-operativeanalgesia following laparoscopic colorectal surgery. Colorectal Dis. 2009 Feb 7.Accepted Article; doi: 10.1111/j.1463-1318.2009.01799.x
[58] Zingg U, Miskovic D, Hamel C T, Erni L, Oertli D, Metzger U. Influence of thoracicepidural analgesia on postoperative pain relief and ileus after laparoscopic colorectalresection: Benefit with epidural analgesia. Surg Endosc. 2009 Feb;23(2):276-82.
[59] Senagore A J, Whalley D, Delaney C P, Mekhail N, Duepree H J, Fazio V W. Epiduralanesthesia-analgesia shortens length of stay after laparoscopic segmental colectomyfor benign pathology. Surgery. 2001 Jun;129(6):672-6.
[60] Traut U, Brügger L, Kunz R, Pauli-Magnus C, Haug K, Bucher H C, Koller M T.Systemic prokinetic pharmacologic treatment for postoperative adynamic ileusfollowing abdominal surgery in adults. Cochrane Database Syst Rev. 2008 Jan23;(1):CD004930.

24
[61] Andersen H K, Lewis S J, Thomas S. Early enteral nutrition within 24h of colorectalsurgery versus later commencement of feeding for postoperative complications.Cochrane Database Syst Rev. 2006 Oct 18;(4):CD004080
[62] Lewis S J, Andersen H K, Thomas S. Early enteral nutrition within 24 h of intestinalsurgery versus later commencement of feeding: a systematic review and meta-analysis. J Gastrointest Surg. 2009 Mar;13(3):569-75.
[63] Lewis S J, Egger M, Sylvester P A, Thomas S. Early enteral feeding versus “nil bymouth” after gastrointestinal surgery: systematic review and meta-analysis ofcontrolled trials. BMJ. 2001 Oct 6;323(7316):773-6.
[64] Papaspyros S, Uppal S, Khan S A, Paul S, O’Regan D J. Analysis of bedsideentertainment services’ effect on post cardiac surgery physical activity: a prospective,randomised clinical trial. Eur J Cardiothorac Surg. 2008 Nov;34(5):1022-6
[65] Powell-Tuck J, Gosling P, Lobo D N, Allison S P, Carlson G L, Gore M et al. BritishConsensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients(GIFTASUP). London: NHS National Library of Health.http://www.ics.ac.uk/downloads/ 2008112340_GIFTASUP%20 FINAL_31-10-08.pdf
[66] Jakobsen D H, Sonne E, Andreasen J, Kehlet H. Convalescence after colonic surgerywith fast-track vs conventional care. Colorectal Dis. 2006 Oct;8(8):683-7
[67] Delaney C P, Fazio V W, Senagore A J, Robinson B, Halverson A L, Remzi F H. ‘Fasttrack’ postoperative management protocol for patients with high co-morbidityundergoing complex abdominal and pelvic colorectal surgery. Br J Surg. 2001Nov;88(11):1533-8
[68] Finan P J, Campbell S, Verma R, MacFie J, Gatt M, Parker M C, Bhardwaj R, Hall NR. The management of malignant large bowel obstruction: ACPGBI positionstatement. Colorectal Dis. 2007 Oct;9 Suppl 4:1-17.
[69] Khan S, Wilson T, Ahmed J, Owais A, MacFie J. Quality of Life and PatientSatisfaction with Enhanced Recovery Protocols. Colorectal Dis. 2009 Jul 6. AcceptedArticle; doi:10.1111/j.1463-1318.2009.01997.x
[70] Grimble R F. Nutritional modulation of immune function. Proceedings of the nutritionsociety 2001; 60: 389-397.
[71] Buchman A L. Glutamine: is it a conditionally required nutrient for the humangastrointestinal system. Jour of Am College of Nutr 1996; 15: 199-205
[72] Jian Z M, Cao J D, Zhu X G, Zhao W X, Yu J C, Ma E L, Wang X R, Zhu M W, ShuH, Liu Y W. The impact of alanyl-glutamine on clinical safety, nitrogen balance,intestinal permeability, and clinical outcome in postoperative patients: a randomized,double-blind, controlled study of 120 patients. J. Parenter. Enteral Nutr (1999). 23:S62–66
[73] Morlion B J, Stehle P, Wachtler P, Siedhoff H P, Köller M, König W, Fürst P,Puchstein C. Total parenteral nutrition with glutamine dipeptide after majorabdominal surgery: a randomized, double-blind, controlled study. Ann Surg. 1998Feb;227(2):302-8.
[74] King P M, Blazeby J M, Ewings P, Longman R J., Kipling R M., Franks PJ et al. Theinfluence of an enhanced recovery programme on clinical outcomes, costs and qualityof life after surgery for colorectal cancer. Colorectal Disease 2006; 8: 506–513
[75] Kariv Y, Delaney C P, Senagore A J, Manilich E A, Hammel J P, Church J M, Ravas J,Fazio V W. Clinical outcomes and cost analysis of a “fast track” postoperative carepathway for ileal pouch-anal anastomosis: a case control study. Dis Colon Rectum.2007 Feb;50(2):137-46
[76] Bosio R M, Smith B M, Aybar P S, Senagore A J. Implementation of laparoscopiccolectomy with fast-track care in an academic medical center: benefits of a fullyascended learning curve and specialty expertise. Am J Surg. 2007 Mar;193(3):413-5;discussion 415-6.
[77] King P M, Blazeby J B, Ewings P, Franks P J, Longman R J, Kendrick A H et al.Randomized clinical trial comparing laparoscopic and open surgery for colorectalcancer within an enhanced recovery programme. Br J Surg 2006; 93: 300–308.


Association of Surgeons of Great Britain and Ireland
35-43 Lincoln’s Inn Fields, London, WC2A 3PE
Tel: 020 7973 0300 Fax: 020 7430 9235www.asgbi.org.uk
A Company limited by guarantee, registered in England 06783090Printed on
recycled paper