good health is fundamental to living a productive life
TRANSCRIPT

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 1/43
1
AN OVERVIEW OF HEALTH AND NUTRITIONAL SERVICES IN INDIA
BRIEF CONTENTS
PreambleImportance of health and nutrition
Definition of health and nutritionWho standards of health and nutritionHealth and nutritional problemsMalnutritionHealth and nutritional schemes in IndiaHealth and nutritional policies and legislationsInstitutional mechanism for health and nutritionFinancial budgets for health and nutritional programmes
³It is health that is real wealth and not pieces of gold and silver´.
Mahatma Gandhi, Father of Nation (India).
³The doctor of the future will no longer treat the human frame with drugs, but rather will
cure and prevent disease with nutrition.´
Thomas Edison.
1. Preamble
R esearch in Health and Nutritional services provided to human being is so important to
underpin both policy making and project designing. Though there has been progress in
improving health and nutrition of people in India; some challenges remain and new ones have
emerged India. The social, economic, and cultural factors influence human¶s health and
nutritional status. The major health problems of the 21st century include nutritional deficiencies
and dietary changes in both rural and urban settings. The research in Health and Nutritional
services can help to identify the biological and socio-cultural components of solutions to
nutrition and health problems. Favorable health policies and effective and equitable health
services are critical to the broader development goal of breaking the cycle of poverty, high
fertility, poor health, low productivity and slow economic growth.
1.1 The Concept of Health
Health is primarily a personal responsibility and demands personal care to enjoy it. It is
an essential requirement of all irrespective age, caste, creed, race, religion and economic
standard. Health of an individual can be affected by general health condition of the society and
vice-versa. Therefore, health of the community needs higher attention while considering the

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 2/43
2
development of a region or a country. It is a precious asset for everyone. It is the crown of all
possessions and untheft treasure. It is certain that health is a basic need of all human beings from
womb to tomb. Good nutrition is a firm foundation for human happiness, and sound health and
skilled performance. It constitutes the most important readily improved environmental influence
of health.
The advances in medical sciences have the treatment of many diseases possible and
simple. And yet the benefits of modern medicines have not reached the vast majority of people
in poverty groups and rural areas, especially women. But it is the women who are the prime
producers of the necessities of the life, women on whom the society depends so heavily for
economic support and family health care.
According to the census 2011 of India about 68.84 percent of Indian population is living
in rural areas as against 31.16 percent in urban areas. There are nearly 6, 40, 867 villages in India
which are scattered over larger areas as compared to urban areas (Census of India, 2011)
1. Urban
areas are not only concentrated but are also attracting centres for economic activities and for
services like health, transport. As a result, large population of hospitals, dispensaries clinics and
medical centers are found in urban areas than in rural areas. On the contrary, villages being
smaller size, most of the health services like hospitals, dispensaries and clinics became
uneconomical as their capacities remain under utilized. Moreover, health problems are rampant
in rural areas, not merely because of lack of medical facilities but because of general poverty,
lack of balanced and nutritious diet to large proportion of rural population, and more over lack of
knowledge with regard to health and hygiene.
1.2 Importance of Health and Nutrition
Health and nutrition are the most important contributory factors for human resource
development in the country. Food consumption, which largely depends on production and
distribution, determines health and nutrition of the population. Accessing by the poor to
services that improve health, nutrition and fertility outcomes is one of the three pillars of the
World Bank's Health, Nutrition, and Population Sector Strategy (Anne Tinker, 2000, p.7)2.
Health and nutrition are vital for livelihood of the human being on the earth. Especially, it
requires during the childhood to sustain thereafter. A good health and nutrition can reduce the
risk of chronic diseases in later life. Nourishing well balanced diets are essential for proper
growth of immunity, physical, and mental development. A women¶s health and nutrition status

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 3/43
3
have important implications for her wellbeing. A Poor nutritional status of women affects not
their health but also the health of their offspring. Maternal nutrition is so important determinant
of pregnancy outcomes, nutrition outcomes and indicators of women¶s health.
Nutrition is critical for health and well-being and is important at every stage of life. Good
nutritional status is widely accepted as an important indicator of national development. Foods
provide energy, nutrients and other substances needed for health. Optimal nutritional status helps
ensure a healthy child hood, pregnancy and a robust newborn. Food consumption, both in terms
of quantity and quality, plays a major role in determining nutritional status. Healthful nutrition
reduces stress, enhances immunity, affects longevity and improves outlook and the quality of
life. The prevalence of malnutrition and infectious disease among the young has important
implications for the health and well-being of the population, because ill health in childhood can
affect an individual¶s physical and mental development, susceptibility to disease, and capacity
for work.
Good health and nutrition is fundamental to live a productive life, meeting basic needs
and contributing to community life. It is an enabling condition for the development of human
potential. The components of health are multiple and their interactions are complex. The health
of an individual is strongly influenced by genetic make-up, nutritional status, access to health
care, socioeconomic status, relationships with family members, participation in community life,
personal habits and lifestyle choices. A healthy population can lead the nation better in all the
frontiers.
Adolescence is the future generation of any country. Their nutritional needs are critical
for the well being of a society. If the adolescence are well-nourished, they can make optimal use
of their skills, talents and energies and would be healthy and responsible citizens. Adolescence,
a second period of rapid growth cycle may serve as an opportunity for compensating faltered
early childhood growth though a good health and nutritional components. Poor nutrition starts
before birth and goes up to death and can spam into generation.
1.3 Definition of Health
The most acceptable definition of health is given by the WHO (1978): Health is the state
of complete physical, mental, social and spiritual well-being, and not merely an absence of
disease or infirmity. It is a significant departure from the medical model. It is a definition of
positive health and goes beyond the mere absence of a disease: the focus being on maintaining

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 4/43
4
good health, rather than on the treatment of different diseases. This comprehensive definition
has made it necessary to define the health of a community in a broad perspective, and not merely
in terms of the individual demographic indicators such as Infant Mortality R ate (lMR ), Life
Expectancy at Birth (LEB), Mortality R ate by Causes, and so on. A community could be healthy
if almost every individual in it were healthy. The primary requirements for anyone to be healthy
are availability of adequate food, shelter and clothing.
This definition tells us that health is a positive state of human life. In other words, it is a
state of complete well-being not just the absence of disease. A person may not be suffering from
any disease and yet may not enjoy complete well-being. There are many times when one feel
tired or exhausted and incapable of concentrating on their work. At such times they are not
enjoying complete well-being, even though at other times they do. There are also times when
one suffers from an infection or periods of ill health. This means no person enjoys full health all
the time. However, a person can be called healthy if he or she enjoys good health most of the
time. Another dimension which is also gaining prominence is spiritual health. Health relates to
physical well-being, who people are as individuals, how people relate to their environment, what
they know value and believe how they make decisions and behave. The dimensions of health as
described in figure 1.
F ig. The dimensions of Health
1.3.1 Physical Health is easy to detect and describe. A person is physically healthy if he or she
looks alert, is responsive, energetic, and vigorous. Physical health is discussed in terms of
wellness of the body and absence of bodily disorders. It includes the characteristics such as one¶s
weight, susceptibility to disease, nutritional status, fitness and powers of recovery from illness.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 5/43
5
1.3.2 Social health is one¶s ability to get along with other people in one¶s life and have a
productive role in one¶s family or community. It relates to social abilities, skills and insights.
Positive social interaction can be seen both as a means of achieving health and as a part of health
itself.
1.3.3 Mental or emotional health is expressed in terms of understanding one¶s emotions,
coping with everyday problems and handling stress in a non-destructive way. The mental
components of health are related to one¶s self-esteem, self-confidence and the way you cope with
problems.
1.3.4 Spiritual health may involve a religious belief, or it may simply relate to that sense of
being part of a larger environment or world.
1.4 The social construct of health
It recognizes that a person¶s cultural background, religion, family structure, support
networks, level of education and income all interrelate to affect their view of health status as
shown in figure 2. Cultural factors may influence dietary patterns. This, in turn, may bring into
question the relevance of the standard dietary pyramid. R eligious factors may determine whether
immunisation occurs or a potentially lifesaving blood transfusion is allowed. Family and culture
may determine the type and amount of physical activity which people, especially females,
engage in. Health status is affected by gender; education; income and social status; successful
social relationships; and culture. Understanding this social view of health enables to realize that
health does not mean the same to all people and as society changes.
Access to
Services Peers
Gender
Culture
Education
Media
Income
HEALTH
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 6/43
6
Environment Religion Family
Fig 2: Social construct of health
1.5 Definition of Nutrition
Nutrition refers to the availability of energy and nutrients to the body¶s cells in relation to
body requirements. It is a basic human need and a prerequisite to a healthy life. Nutrition can be
defined as ³The science of foods, the nutrients and other substances therein; their action,
interaction and balance in relationship to health and disease; the processes by which the
organism ingests, digests, absorbs, transports and utilizes nutrients and disposes of their end
products. In addition, nutrition must be concerned with the social, economic, cultural and
psychological implications of food and eating´. Household nutrition involves physical and
economic access to balanced diets and safe drinking water for the children, women and men of every family. Nutritional status is the condition of health of an individual as influenced by the
utilization of nutrients. Nutrition is essential from the very early stages of life for proper growth,
development and to remain active along with the human growth cycle as shown in figure.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 7/43
7
Nutrition throughout the life cycle
Source: Prepared by Nina Seres f or the ACC/SCN-appointed Commission on the Nutr ition Challenges of the 21st
Centur y.
BABY
LBW
CHILD
STUNTED
ADOLESCENT
STUNTED
WOMEN
MALNOURISHED
PREGNANCY LOW
WEIGHT GAIN
MALNUTRITION
ELDERLY
INADEQUATE FOOD
HEALTH & CARE
INADEQUATE FOOD
HEALTH & CARE
INADEQUATE FOOD
HEALTH & CARE
INADEQUATE
CATCHUP GROWTH
MENTALLY RETARD RISK OF
CHRONIC DISEASES IN
ADULT HOOD
INADEQUATE FEEDING, FREQUENT
INFECTIONS INADEQUATE FOOD HEALTH
& CARE
GROWTH FAILURE
REDUCED MENTAL CAPA
HIGH MMR

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 8/43
8
A proper diet and good nutrition targeted to many solutions to the health and nutritional
problems of mankind as shown in the figure.
S ource: Anonymous author
1.6 Current Nutritional Status
The National Family Health Survey 05-06 (NFHS-3) gives statistics of the nutritional status of
women and children of India. According to the NFHS-3, 43 percent of children under age five
years are underweight for their age (WAZ<-2SD) and 48 percent of children under age five years
are stunted (HAZ<-2SD). NFHS-3 shows that 36% of all women age 15-49 in India are
underweight (BMI <18.5). And that girls and boys 0-35 months were about equally likely to be
underweight. The girls having slightly better health status2.
Table1: Child Mortality Statistics
Countries
Per
Capita
GDP
Under-fivemortality rate
MDG
target
Average annual rate of Reduction (%)
Progresstowardsthe MDG
target1990 2006Observed Required
1990 2006 2007 - 2015
Er itrea 271 147 74 49 4.3 4.6on track
Bangladesh 428 149 69 50 4.8 3.6 on track
India 976 115 76 38 2.6 7.6 insufficient
Pakistan 996 130 97 43 1.8 9.0 insufficient
Niger ia 1,169 230 191 77 1.2 10.1 insufficient
Philippines 1,639 62 32 21 4.1 4.8 on track

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 9/43
9
Sr i Lanka 1,676 32 13 11 5.6 2.2 on track
Egypt 1,770 91 35 30 6.0 1.6 on track
Indonesia 1,869 91 34 30 6.2 1.3 on track
S ource: Unicef
Table1 demonstrates how countries with comparable per capita GDP like the Philippines,
Sri Lanka and Egypt have made better progress towards at reducing child mortality. In fact,
Bangladesh and Eritrea, which have approximately half and quarter of India¶s per capita GDP,
respectively, and had higher infant mortality rates to start with, have made commendable
progress between 1990 and 20063.
1.7 Malnutrition
Malnutrition refers to any imbalance in satisfying nutrition requirements. It is the
condition that results from taking an unbalanced diet in which certain nutrients are lacking, in
excess (too high an intake), or in the wrong proportions (Dorland's Medical Dictionary and
Sullivan, Arthur; Steven M. Sheffrin, 2003). A number of different nutrition disorders may arise,
depending on which nutrients are under or overabundant in the diet. Malnutrition infection
complex are shown in the figure.
Malnutrition
Weak education
and Health S stemImpaired Child
Develo ment
Weak education
and Health S stemCompromised
Immunit
Infection Poverty
Disease R educed
Productivit
Energy Loss

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 10/43
10
Fig: Malnutrition-Infection Complex
S ource: S chaible, U., Kaufmann, S ., Malnutrition and Infection: complex mechanisms and Global Impact. PLoS
Medicine. May 2007.
India has one of the highest rates of malnutrition in the world. Nearly one in every two of
India¶s 120 million children is underweight, almost double the prevalence in Sub-Saharan Africa.
An undernourished child will fail to reach her human potential in her adult years ± in terms of
educational attainment, health and productivity ± perpetuating a vicious cycle of poverty and
malnutrition.
India has a serious problem of child undernutrition. R eduction of child undernutrition is
imperative, since it has enormous consequences for child and adult morbidity mortality, as well
as productivity. Undernutrition directly affects many aspects of children¶s development,
retarding physical and cognitive growth and increasing susceptibility to disease. Improved policyand programs are needed if India is to reach the nutrition MDG (Millennium Development Goal)
target of halving the figures for malnutrition by the year 2015 (from in 1990 to in 2015).
The nutritional status of young children is an important indicator of health and
development²it is not only a reflection of past health insults but an important indicator of future
health trajectories4. Malnutrition plays a key role in maternal mortality, just as in infant and
child deaths. In 1965, a World Health Organization Expert Committee on Nutrition in
Pregnancy and Lactation wrote, ³Next to young children, pregnant and lactating women are
nutritionally the most vulnerable group, especially in the developing regions of the world, and
yet comparatively little is known of their special nutritional needs´. R egrettably, little has
changed since then and maternal malnutrition remains a major problem in India and Pakistan. In
this two countries the majority of women are in a constant state of nutritional stress, beginning in
childhood, then adolescence, and continuing through the childbearing period which often
commences before growth has ceased, and consists of a continuous cycle of pregnancy and
lactation, all too often resulting in premature death. Chronic protein-energy malnutrition, iron-
deficiency anaemia, and deficiencies of iodine and vitamin A are among the common nutritional
deficiencies that affect women in the two countries5.
Almost 50% of pre-school children in rural India are malnourished6. An adequate intake
of calories does not ensure that the need for micronutrients has been met. Being underweight
due to wasting (i.e., low weight-for-height, indicating acute weight loss) or stunting (i.e., low

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 11/43
11
height-for-age, indicating chronic restriction of a child¶s nutrition), micronutrient deficiencies, as
well as being overweight, are forms of malnutrition. Approximately 852 million people around
the world are unable to obtain enough food to lead healthy and productive lives. Undernutrition
in children is responsible for an increased risk of illness and death from many infectious
diseases, causing nearly 3.6 million deaths, including some attributed to diarrhea, pneumonia,
measles and malaria. Poor nutrition can result from either inadequate or excessive levels of
nutrient intake and influences the development of chronic disease.
Malnutrition is a condition where there is insufficient or inadequate consumption of basic
nutrients required by the body which leads to the manifestation of various diseases and disorders.
According to the World Health Organization, malnutrition is the biggest contributor to child
mortality, as it directly or indirectly leads to various deficiency disorders. Thus, these
malnutrition facts speak for themselves. So, to deal with this worldwide menace, it is important
to know all about the various kinds of malnutrition diseases that exist and what are the symptoms
that they show.
1.8 Consequences of Poor nutrition
A women with poor nutritional status, as indicated by a low body mass index, short
stature, anemia, other micro-nutrient deficiencies, has a greater risk on abstracted labour, having
a baby with a low birth weight, having adverse pregnancy outcomes, producing lower quality
breast milk, death due to post partum haemortag and illness for herself and her baby.
1.9 Reasons for Malnutrition
In communities or areas that lack access to safe drinking water, these additional health risks
present a critical problem. Lower energy and impaired function of the brain also represent the
downward spiral of malnutrition as victims are less able to perform the tasks they need to in
order to acquire food, earn an income, or gain an education.
Since the common assumption is that food insecurity is the major cause of malnutrition,
almost completely ignoring the contribution of infection and inappropriate feeding practices,
policy inputs have been skewed towards food-based interventions.
Malnutrition among children is often caused by the synergistic effects of inadequate or
improper food intake, repeated episodes of parasitic or other childhood diseases such as
diarrhoea, and improper care during illness (Pelletier 1994; R uzicka and Kane 1985)[7] [8].
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 12/43

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 13/43
13
factors such as lower levels of household wealth and maternal education are important causes of
childhood undernutrition (UNICEF 1998)19.
1.10 List of Malnutrition Diseases
Malnutrition increases the risk of infection and infectious disease; for example, it is a major risk
factor in the onset of active tuberculosis (Schaible UE, Kaufmann SH, 2007)20.
1.10.1 Marasmus is a disease that results from severe deficiency of both proteins and calories
and is one of the most common malnutrition diseases in children. Thus, this condition results in
overall energy deficiency. In this condition, a person looks emaciated and the body weight of the
person maybe lower than 80% of the normal required weight of the person. The occurrence of
this disease is higher in infants below the age of one. This disease is rampant in African countries
and certain other third world countries. In this disease, there is extensive muscle wasting. There
might also be edema, dry and scaly skin, loose skin, etc. Furthermore, the adipose tissue reserves
of the person get severely depleted, especially from the buttocks and thighs. The person is also
seen to be very irritable, fretful and voraciously hungry. The person also becomes very
susceptible to contracting infectious diseases, which further increases the mortality rate of this
disease. The treatment of this disease will not only consist of providing the person with all the
required nutritional supplements that he is deficient of but will also entail treating dehydration
and any other infections that he may be suffering from.
1.10.2 Kwashiorker is one of the most acute protein malnutrition diseases in the world. It is also
said to be protein-calorie malnutrition similar to marasmus, but what sets it apart from marasmus
is the presence of edema, that is typically seen in the feet. Other signs of this disease include a
distended abdomen, an enlarged liver, thinning hair which is normally coarse in texture, loss of
teeth, skin depigmentation, and dermatitis. Children suffering from this condition normally end
up developing irritability and anorexia as well. Although it was believed for long that this disease
was caused by protein deficiency, it is now being said that other factors, like vitamin and mineral
deficiency also play a very important role in causing this disease. Once again, as is seen in
marasmus, due to the severe deficiency of various essential nutrients, the person has an increased
susceptibility to contracting diseases and even developing diseases after getting vaccinated for
that particular disease.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 14/43
14
1.10.3 Anemia is one of the most common malnutrition diseases seen the world over. Anemia
can be caused due to a variety of reasons, but one of the main reasons for anemia is a diet that is
deficient in iron and vitamin B12. A diet deficient in iron leads to a type of anemia known as
iron deficiency anemia. This kind of anemia is one of the most common malnutrition diseases in
the world and is especially rampant in developing countries. It is also particularly seen in
pregnant women in these regions. It leads to various problems like shortness of breath, tiredness
and fatigue, pallor and other symptoms that point towards a low hemoglobin count. Deficiency
of vitamin B12 leads to a type of anemia known as megaloblastic anemia.
1.10.4 Goiter is a disease that is mostly caused due to deficiency of iodine in the diet. This leads
to typical goiter symptoms like swelling of the thyroid gland which is visible as a large swelling
in the neck. Other symptoms present in goiter will be similar to those seen in hypothyroidism,
like lethargy, weakness, low metabolic rate, increased susceptibility to cold, ptosis, etc.
Sometimes, the swelling in the neck may be so large, that it may lead to compression of the
windpipe or the larynx, which may cause difficulty in breathing and speaking. This disorder is
typically seen in countries that have deficient iodine in their soil, or in countries where the food
supplements available are not iodized. Goiter treatment will depend on the size and cause of
goiter. If the swelling is small and is only due to slight iodine insufficiency, then providing
iodine supplements can help treat the disorder. However, if the swelling is large and is causing
pressure on the windpipe or larynx, then it is best to do an emergency partial or complete
thyroidectomy, depending on the case.
1.10.5 Hyponatremia is a condition that is caused due to deficiency of sodium in the blood and
diet. This is a serious type of electrolyte disturbance that is normally seen in people who have
high levels of antidiuretic hormone. In this disease, the concentration of sodium in the plasma is
less than 135mEq/L. This condition is often seen as a result of a complication of some other
serious medical illness, like diarrhea, excessive vomiting, polydipsia, etc. Typical symptoms
include nausea, vomiting, headache, etc. If the symptoms are not treated in time and worsen
further, there may even be mental clouding, confusion, convulsions, stupor and the person may
even eventually go into coma. The treatment for this disease depends on the underlying cause. In
cases of severe volume depletion, there may be need of intravenous administration of saline.
Serious symptoms like seizures normally require treatment using hypertonic saline.
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 15/43
15
1.10.6 Hypokalemia is caused due to deficiency of potassium in the diet. Normally, the
symptoms to start showing, there needs to be not only insufficient consumption of potassium but
also excessive loss of potassium from the body. Thus, it is often seen as a complication of
dehydration or diarrhea and malnutrition. The signs and symptoms of this include myalgia,
muscle cramps, tetany, slight change in blood pressure, constipation, etc. Serious effects of it
include respiratory depression and cardiac arrhythmias. The most important approach to treat this
disease is to include foods high in potassium in the diet. If the person is also suffering from
dehydration or diarrhea, then he will need fluid replenishment and treatment with antibiotics as
well.
1.10.7 Vitamin Deficiency is also commonly seen in many malnutrition diseases. Given below
is a list of the various vitamins and what their deficiency leads to:
1.10.7.1 Vitamin A Deficiency of it is relatively common in developing countries, though it is
rarely seen in developed countries. One of the most common symptoms causing due to the
deficiency of this vitamin is night blindness it can even lead to complete blindness if there is
severe depletion in the levels of this vitamin. Causing blindness due to vitamin A deficiency
among malnourished children can be seen all over the world. Other symptoms are increased
susceptibility to infections, lack of appetite, dry and rough skin and hair, and poor wound
healing. This Vitamin can be restored in the body with the help of including foods that are rich in
vitamin A in the diet.
1.10.7.2 Vitamin B1 or thiamine is a nutrient that is available in many sources, like yeast and
pork, which are obviously a rarity in malnourished environments. One of the most common
symptoms of this vitamin deficiency is the manifestation of beriberi. It is a nervous system
disorder, which leads to symptoms like severe lethargy and fatigue, inability to derive energy,
difficulty in walking, loss of muscle with muscle wasting and eventual complications of the
cardiovascular, nervous, muscular and gastrointestinal systems. It is also commonly seen in
alcoholics. The treatment of this will involve administration of thiamine in the form of thiamine
hydrochloride tablets or injections.
1.10.7.3 Vitamin B2 or R iboflavin deficiency is normally seen in conjunction with protein-
energy malnutrition diseases and is also seen in alcoholics. The signs and symptoms this vitamin
deficiency includes sore throat with swelling and redness of the mouth, cheilosis, angular
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 16/43
16
stomatitis, glossitis, seborrhic dermatitis, etc. The deficiency symptoms can be reversed with the
help of including foods rich in riboflavin, like meat, eggs, cheese, yogurt, etc.
1.10.7.4 Vitamin B3 or niacin deficiency leads to a disease called pellagra. It often results from
alterations of protein metabolism in the body. People who have a staple diet of maize also often
end up suffering from pellagra. The signs and symptoms of it includes photosensitivity,
dermatitis, dementia, diarrhea, alopecia, insomnia, weakness, ataxia, etc. Cases of pellagra that
are left untreated have a high mortality rate, as the person can die within four to five years of
being diagnosed. To prevent this from happening, it is important to include niacin rich foods in
the diet.
1.10.7.5 Vitamin B12 deficiency is one of the most common deficiencies seen in the spectrum of
vitamin B deficiencies. It is found only in animal products; hence, a deficiency of this vitamin is
often seen in vegetarians. Signs of the vitamin deficiency include tingling sensation of tongue,
white spots on skin, mouth sores, shortness of breath, memory loss, headaches resembling
migraine attacks, etc. However, one of the most important and prominent symptoms of the
vitamin is megaloblastic anemia. This is the type of anemia where the red blood cells are large
and immature in nature.
1.10.7.6 Vitamin C or ascorbic acid is a vitamin that is found in citrus fruits. Although an
overdose of the vitamin is rare and the deficiency can be seen in developing countries habitually.
Deficiency of this vitamin leads to a condition known as scurvy and the symptoms like bleeding
gums, delayed wound healing, spots on skin and increased susceptibility to infections. This
vitamin can be obtained by eating fruits like oranges, lemon, lime, grapefruit, etc.
1.10.7.7 Vitamin D deficiency normally occurs due to inadequate intake of calcium coupled
with inadequate sunlight exposure. The symptoms of the deficiency of it include impaired bone
formation, thus, causing bone softening diseases like osteomalacia. It is also a major
contributing factor towards the development of osteoporosis in women living in developing
countries. To help prevent this from occurring, one needs to have a diet that is high in calcium
and foods with vitamin D. The Deficiency and Excess of Nutrients narrated in the table 2.
Table 2: Deficiency and Excess of Nutrients
Nutrients Deficiency Excess
Food energy Starvation, Marasmus Obesity, diabetes mellitus, Cardiovascular

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 17/43
17
disease
Simple
carbohydratesnone diabetes mellitus, Obesity
Complex
carbohydratesnone Obesity
Saturated fat low sex hormone levels Cardiovascular disease
Trans fat none Cardiovascular Disease
Unsaturated fat none Obesity
Fat
Malabsorption of Fat-soluble
vitamins, R abbit Starvation (If
protein intake is high)
Cardiovascular Disease (claimed by some)
Omega 3 Fats Cardiovascular Disease Bleeding, Hemorrhages
Omega 6 Fats none Cardiovascular Disease, Cancer
Cholesterol none Cardiovascular disease
Protein kwashiorkor R abbit starvation
Sodium hyponatremia Hypernatremia, hypertension
Iron Anemia Cirrhosis, heart disease
Iodine Goiter, hypothyroidism Iodine Toxicity (goiter, hypothyroidism)
Vitamin A
Xerophthalmia and Night
Blindness, low testosterone
levels
Hypervitaminosis A (cirrhosis, hair loss)
Vitamin B1 Beri-Beri
Vitamin B2
Cracking of skin and Corneal
Ulceration
Vitamin B3
(Niacin)Pellagra dyspepsia, cardiac arrhythmias, birth defects
Vitamin B12 Pernicious anemia

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 18/43
18
Vitamin C Scurvy diarrhea causing dehydration
Vitamin D R icketsHypervitaminosis D (dehydration, vomiting,
constipation)
Vitamin E nervous disorders Hypervitaminosis E (anticoagulant: excessive
bleeding)
Vitamin K Haemorrhage
Calcium
Osteoporosis, tetany,
carpopedal spasm,
laryngospasm, cardiac
arrhythmias
Fatigue, depression, confusion, anorexia,
nausea, vomiting, constipation, pancreatitis,
increased urination
Magnesium HypertensionWeakness, nausea, vomiting, impaired
breathing, and hypotension
PotassiumHypokalemia, cardiac
arrhythmiasHyperkalemia, palpitations
1.11 Health and Nutritional Programmes in India
1. 11.1 Programmes on Health Sector
Department of Health and Family Welfare, Government of India is administering the
various programmes/schemes and enacted various legislations on health sector and some of the
important are:
1. 11.1.1 National Diarrhoeal Diseases Control Programme was launched in 1981 to reduce
the mortality in children below five years due to diarrhoeal diseases through introduction of Oral
R
ehyderation Therapy (OR
T). The high priority accorded to the Programme is part of the package of services rendered under the MCH programme which was initiated during 1980-85
has now been strengthened extensively. The Anganwadi Centres of the ICDS Scheme have
served as nucleus for the propagation of this programme which has been found to be an effective
measure to prevent dehydration.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 19/43
19
1.11.1.2 Cancer Control Programme bridges the geographical gaps in the availability of cancer
treatment facilities across the country, the programme launched in 1975-76 was revised in 1984-
85 and subsequently in December 2004. At any point of time, it is estimated that there are nearly
25 lakh cancer cases and about 4 lakh deaths occurs every year in this country. In view of the
magnitude of the problem and the requirement this was initiated.
1.11.1.3 Mental Health Programme was started in 1982 with the objectives to ensure the
availability and accessibility of minimum mental health care for all, to encourage mental health
knowledge and skills and also to promote community participation in mental health service
development and stimulate self-help in the community. There was a shift in approach of mental
health care services from hospital based care to community based mental health care.
1.11.1.4 Emergency Facilities of State Hospitals located on National Highways for up
gradation & strengthening of Emergency Trauma Care Facility in State Government Hospitals
located on National Highways under the scheme ³Assistance for Capacity Building´ with a view
to provide immediate treatment to the victims of road traffic injury. The network of trauma care
facilities along the corridors will bring down the morbidity and mortality on account of
accidental trauma by observing the golden hour concept.
1.11.1.5 Prevention and Control of Diabetes, Cardiovascular Disease and Strokes a pilot
scheme has been launched in January, 2008 with the aim of prevention and control of non-
communicable diseases (NCDs) using health promotion and health education advocacy. The
early detection of persons with high level of risk of developing disease through opportunistic
screening and capacity building of health system at all levels to tackle NCDs and improvement
of quality of care. A well developing trained manpower at various health care set-ups in
Districts/States. The pilot scheme encompasses 10 States with one District each namely,
Kamrup, Assam; Jalandhar, Punjab; Bhilwara, R ajasthan; Jabalpur, Madhya Pradesh; Shimoga,
Karnataka; Kancheepruam, Tamil Nadu; and Thiruvananthapuram, Kerala. Under the Pilot
project, Health promotion activities were undertaken in 300 schools (30 in each district) and at
15 workplaces (1-2 workplace per district) in all the 10 States.
1.11.1.6 Central Government Health Scheme (CGHS) is a scheme for providing health care to
serving Central Government employees and their dependant family members. Over the years, the
scheme has bee extended to cover central government pensioners, their dependant family
members and certain other categories like members of parliament and ex-members of parliament,

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 20/43
20
freedom fighters etc., The membership of this scheme stood at 9.35 lakhs with 32 lakh
beneficiaries as on 31.3.2009. The beneficiaries are being provided health service through a huge
network of: Dispensaries (247 Allopathic, 82 Ayush), Yoga Centres (4), Polyclinics (19),
Laboratories (66), Dental Units (21) and Gynae±maternity Hospital (1). In addition, beneficiaries
enjoy medical facilities in around 400 private empanelled hospitals and around 170 diagnostic
centres, all over the country.
1.11.1.7 Health Minister¶s Discretionary Grant is a Financial Assistance to the poor and
indigent patients is given from the Health Minister¶s Discretionary Grant to defray a part the
expenditure on hospitalization/treatment in Govt. Hospital as these patients cannot be considered
for financial assistance under R ashtriya Arogya Nidhi due to income of above poverty line, but
less than R s.50,000/- per annum.
1.11.1.8 National Vector Borne Disease Control Programme is a comprehensive programme
for prevention and control of vector borne diseases namely Malaria, Filaria, Kala-azar, Japanese
Encephalitis (JE), Dengue and Chikungunya which is covered under the overall umbrella of
NR HM. The States are responsible for implementation of programme whereas the Directorate of
NVBDCP, Delhi provides technical assistance, policies and assistance to the States in the form
of cash & commodity, as per approved pattern.
1.11.1.9 Pradhan Mantri Swasthya Suraksha Yojana (PMSSY) was approved by
Government of India in March, 2006 with the objective of correcting regional imbalance in the
availability of affordable and reliable tertiary healthcare services and also to augment facilities
for quality medical education in the country. It has two components in its first phase - (i) setting
up of six AIIMS-like institutions and (ii) upgradation of 13 existing Government medical college
institutions.
1.11.1.10 Other Health Programmes are Prevention and Control of Deafness; Prevention and
Control of Fluorosis; National Filaria Control Program, R ashtriya Arogya Nidhi, Leprosy
Eradication Programme (NLEP); TB Control Programme (R NTCP); Programme for Control of
Blindness (NPCB); Iodine Dificiency Disorders Control Programme, National AIDS Control
Program, National Program for Prevention and Control of Deafness, Tobacco Control Program
and School Health Programs.
1.11.2 Rural Health Services

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 21/43
21
The health and family welfare programme in the country is being implemented through
primary health care system. In rural areas, primary health care services are provided through a
network of 146036 Sub-Centres, 23458 Primary Health Centres and 4276 Community Health
Centres as on March 2008 based on the following norms of population case load/work load and
distance. The population norms for SC/PHC/CHC are as follows:
1.11.2.1 Sub-Centre is the first peripheral contact point between Primary Health Care system
and the community. It is manned by one Female (ANM) and one Male Health Worker and one
LHV for six such Sub-Centres. These are assigned task relating to maternal health child health,
family welfare, nutrition, immunization, diarrhea control and control of communicable diseases.
These centers facilitated with basic drugs for minor ailments needed for taking care for essential
health need for women and children.
1.11.2.2 Primary Health Centre (PHC) is the first contact point between village community
and the Medical Officer. It is manned by a Medical Officer and 14 other staff. It acts as a referral
Unit for 6 Sub-Centres and has 4-6 beds for patients. It performs curative, preventive, promotive
and Family Welfare services. There are 23, 458 PHCs functioning in the country. These are
being strengthened under NR HM to provide a package of essential public health programmes
and support for outreach services to ensure regular supplies of essential drugs and equipment,
round the clock services in all PHCs across the country, upgrading single doctor PHC to 2
doctors PHC by posting AYUSH practitioners at PHC level, provision of 3 Staff Nurses in a
phased manner.
1.11.2.3 Community Health Centre (CHC) is established and maintained by the State
Governments and as per standards it is supposed to be manned by four Medical specialists i.e.
Surgeon, Physician, Gynecologist and Pediatrician supported by 21 paramedical and other staff.
It has 30 in-door beds with one OT, X-ray, and Labour room and Laboratory facilities and serves
as a referral centre for 4 PHCs. It provides facilities for emergency obstaetrics care and specialist
consultations. At present 4276 CHCs are functioning in the country. Indian Public Health
Standards lays down that this CHC is to be manned by 6 Medical Specialists including
Anaesthetics and an eye surgeon (for 5 CHCs) supported by 24 paramedical and other staff with
inclusion of two nurse midwives in the present system of seven nurse midwives.
1.11.2.4 Mobile Medical Units/Health Camps initiated with the objective to take health care to
the door step of the public in the rural areas, especially in under-served areas, these, have been

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 22/43
22
provided, one per district under NR HM. Two kinds of MMUs are envisaged, one with diagnostic
facility for the States other than North-East States, Himachal Pradesh and J&K. In addition, for
the North- Eastern States, Himachal Pradesh and J&K, specialized facilities and services such as
X-ray, ECG and ultrasound are proposed to be provided in MMUs.
1.11.3 Maternal Health Programmes
The promotion of maternal and child health has been one of the most important
objectives of the Family Welfare Programme in India. Under the NR HM and the R CH
Programme, the Government of India is actively pursuing the goals of reduction in Maternal
Mortality by focusing on the 4 major strategies of essential obstetric and new born care for all,
skilled attendance at every birth, emergency obstetric care for those having complications and
referral services. The other major interventions are provision of Safe Abortion Services and
services for R TIs and STIs. The National Population Policy 2000 and National Health Policy
2002 have set the goal of reducing MMR to less than 100 per 100000 live births by the year
2010.
1.11.3.1 Schemes for Improving Obstetric Care Services initiatives are under implementation
to achieve the goal of reduction in Maternal Mortality. These interventions are Essential
Obstetric Care; Quality Ante Natal care; Prophylaxis and treatment of Nutritional Anemia; Post
natal care for mother and newborn; Skilled Attendance at Birth; Provision of Emergency
Obstetric and Neonatal Care at FR Us; and R eferral Services at both Community and Institutional
level.
1.11.3.2 Janani Suraksha Yojana (JSY) is a safe motherhood intervention under the National
R ural Health Mission (NR HM) being implemented with the objective of promoting institutional
delivery among the poor pregnant women. It launched on 12th April 2005, is being implemented
in all states and UTs. It is a 100 % centrally sponsored scheme and it integrates the benefits with
delivery and post delivery care. Besides the maternal care, the scheme provides cash assistance
to all eligible mothers for delivery care. This programme has identified, the Accredited Social
Health Activist (ASHA) as an effective link between the Government and the poor pregnant
women. Here the main role is to facilitate pregnant women to avail Services of maternal care and
arrange referral transport. The Yojana subsidizes the cost of Caesarean Section or for the
management of Obstetric complications, up to R s. 1500 per delivery to the Government

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 23/43
23
Institutions, where Government specialists are not in position. All BPL pregnant women aged 19
years and above, preferring to deliver at home is entitled to cash assistance of R s. 500 per
delivery, up to two live births.
1.11.3. 3 Village Health and Nutrition Day (VHNDs) Organizing at Anganwadi centre at least
once every month to provide ante natal and post partum care for pregnant women, promote
institutional delivery and health education apart from other various services.
1.11.3.4 1odine Prophylaxis Programme was initiated by realizing the serious health and social
implications of the problem of iodine deficiency disorders Government of India launched a
National Goitre Control Nutrient Deficiency Control Programmes Programme (NGCP) in 1962.
This programme is now called the Iodine Prophylaxis Programme. The basis of the programme
was a study conducted in the mid-fifties in the Kangra Valley, by the Scientists of All India
Institute of Medical Sciences. The study showed that the prevalence of goitre comes down
considerably when the common salt supply to the population is replaced by iodized salt. In
keeping with the results of this study the control programme was initiated. The main objectives
of the control programme are to identify goitre endemic regions, supply iodized salt in place of
ordinary common salt in goitre endemic areas and assess the impact of the programme over a
period of time.
1.11.4 Child Health Programmes
Since the inception of the family planning Programme in 1951, and subsequent inclusion
of maternal and child health, focus has been on reducing the commonest cause of mortality
among the under fives in the country. The Infant Mortality R ate has declined from 134 per
thousand live births in 1947-50 to 53 per thousand live births in 2008, which is still high. There
is hence a firm commitment for the reduction of the MMR , IMR and the TFR under the National
R ural Health Mission (NR HM).
Some important child health programme are Navjaat Shishu Suraksha Karyakram
(NSSK); Integrated Management of Neonatal and Childhood Illness; Facility Based Integrated
Management of Neonatal and Childhood Illness (F- IMNCI); Sick New Born Care (SNCU);
Infant and young child feeding; Nutrition R ehabilitation Centres (NR Cs); School Health
Programme; and Home Based New Born Care.
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 24/43
24
1.11.4.1 Scheme of Oral Rehydration Therapy¶s main objectives of the scheme of oral
rehydration therapy is to reduce the incidence of death due to dehydration from diarrhoea
diseases, particularly among young children by promoting the use of oral rehydration solution
(OR S) to prevent dehydration and by educating mothers in this regard. Diarrhoea is a serious
health problem in our country, afflicting millions of young children every year. Children
exposed to poor environmental sanitation and hygiene, without access to safe drinking water; in
particular suffer from repeated episodes of diarrhoea. If immediate remedial measures are not
taken, it may even lead to the child's death.
1.11.4.2 Universal Immunization Programme was introduced in 1978 as Expanded
Programme of Immunization. This gained momentum in 1985 as Universal Immunization
Programme (UIP) and implemented in phased manner to cover all districts in the country by
1989-90. UIP become a part of Child Survival and Safe Motherhood Programme in 1992. Since,
1997, immunization activities have been an important component of National R eproductive and
Child Health Programme. Immunization is one of the key areas under National R ural Health
Mission (NR HM) launched in 2005. Under the Universal Immunization Programme Government
of India is providing vaccination to prevent six vaccine preventable diseases i.e. Diphtheria,
Pertussis, Tetanus, Polio, Measles and severe form of Childhood Tuberculosis.
1.11.4.3 Pulse Polio Immunization was initiated in the pursuance of the World Heath Assembly
resolution of 1988; this Programme was started nation-wide from 1995 to eradicate polio in India
covering children in the age group 0-3 years. In order to accelerate the pace of polio eradication,
all children under the age of 5 years were targeted since 1996-97. From 1999-2000 house to
house vaccination of missed children was also introduced to vaccinate children missed during the
fixed booth based vaccination of children.
1.12 Nutritional Programmes
1.12.1 Special Nutrition Programme was launched in the country in 1970-71. It provides
supplementary feeding to the extent of about 300 calories and 10 gm. of proteins to pre-school
children and about 500 calories and 20 gm. of protein to expectant and nursing mothers for 300
days a year. At present SNP is operated, as a part of the Minimum Needs Programme in the
various states. The nutrition component of the ICDS programme is funded by States and Union

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 25/43
25
Territories from the SNP budget. At present about 21.5 million beneficiaries are covered under
this programme.
1.12.2 Balwadi Nutrition Programme is being implemented since 1970-71 through five
national level voluntary organisations. The Central grant is given for. supplemerltary feeding of
children. It consists of 300 calories and 10 gm. of p' Aein per child per day for 270 days a year.
During 1991-92, about 0.23 million children in the age group 3-5 years in 5640 balwadis were
covered by the scheme.
1.12.3 Goitre Control Programme was initiated by the GoI in 1962 to identify goiter endemic
regions and to assess the impact of goitre control measures. The availability and production of
iodized salt and strengthening of administrative machinery controlling the entry of noniodized
salt in the endemic regions have been recommended as measpres to improve the implementaion
of the programme.
1.12.4 National Nutritional Anaemia Control Programme results from deficiency of iron and
folic acid in the body. A person suffering from anaemia feels weak and has a low capacity to
work. Nutritional anaemia is a widely prevalent problem in our country. It is especially affects
women in the reproductive age and young children. It is estimated that more than 50 per cent of
pregnant women in our country are anaemic. This is directly or indirectly responsible for about
one fifth of maternal deaths and is a major cause of premature births and low birth weight babies.
This programme aims at significantly decreasing the prevalence and incidence of anaemia in
women in the reproductive age group, particularly pregnant and lactating women, and preschool
children by giving them iron and folic acid tablets.
1.12.5 National Prophylaxis Programme for Prevention of Nutritional Blindness aims at
protecting children, between 6 months and 5 years of age, from vitamin A deficiency by giving
them large doses of vitamin A on periodic basis. An estimated 5 to 7 per cent children in our
country suffer from eye problems resulting from vitamin A deficiency. Night blindness and other
mild deficiency symptoms in the eye, for instance lack of luster, haziness and other changes such
as dry, foamy, triangular spots on the white part of the eye, can be cured with vitamin A therapy.
However, if the condition is untreated, the cornea in the eye gets severely damaged and blindness
results which condition cannot be reversed.
1.12.6 Nutritional Programme for Adolescent Girls (NPGA) was launched by the Planning
Commission initially for a period of two years i.e. 2002-03 and 2003-04 in 51 identified
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 26/43
26
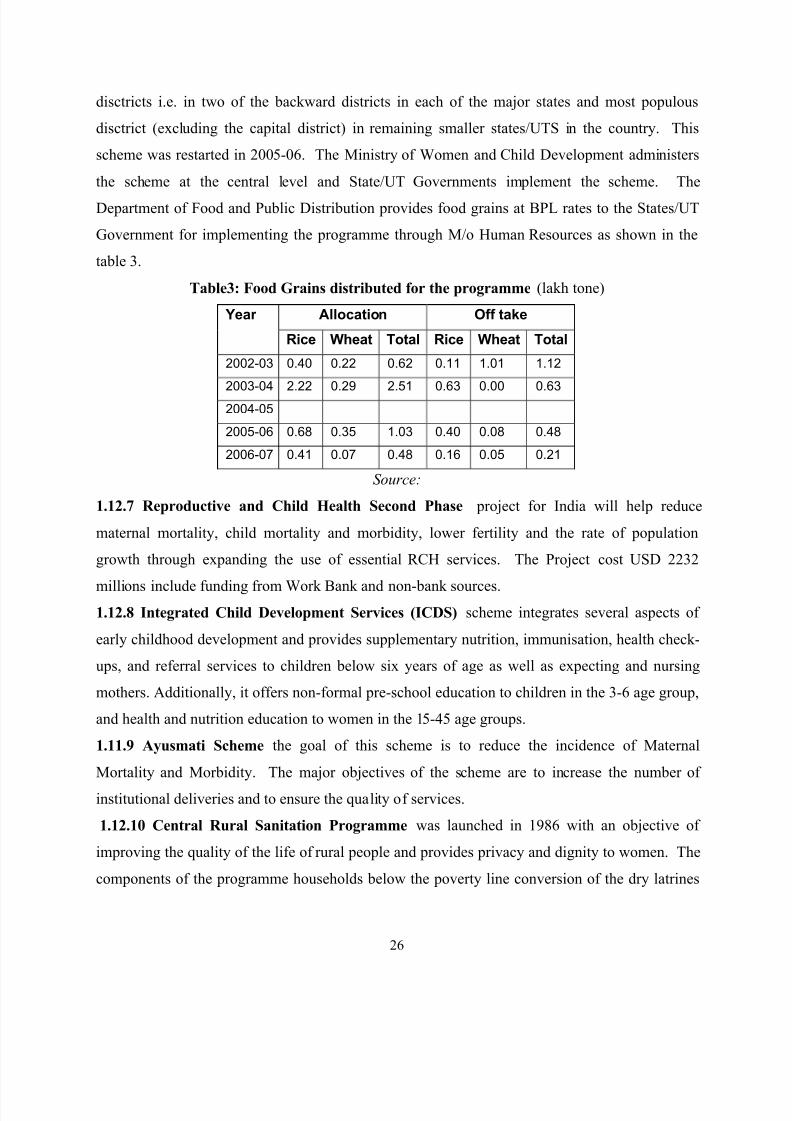
disctricts i.e. in two of the backward districts in each of the major states and most populous
disctrict (excluding the capital district) in remaining smaller states/UTS in the country. This
scheme was restarted in 2005-06. The Ministry of Women and Child Development administers
the scheme at the central level and State/UT Governments implement the scheme. The
Department of Food and Public Distribution provides food grains at BPL rates to the States/UT
Government for implementing the programme through M/o Human R esources as shown in the
table 3.
Table3: Food Grains distributed for the programme (lakh tone)
Year Allocation Off take
Rice Wheat Total Rice Wheat Total
2002-03 0.40 0.22 0.62 0.11 1.01 1.12
2003-04 2.22 0.29 2.51 0.63 0.00 0.632004-05
2005-06 0.68 0.35 1.03 0.40 0.08 0.48
2006-07 0.41 0.07 0.48 0.16 0.05 0.21
S ource:
1.12.7 Reproductive and Child Health Second Phase project for India will help reduce
maternal mortality, child mortality and morbidity, lower fertility and the rate of population
growth through expanding the use of essential R CH services. The Project cost USD 2232
millions include funding from Work Bank and non-bank sources. 1.12.8 Integrated Child Development Services (ICDS) scheme integrates several aspects of
early childhood development and provides supplementary nutrition, immunisation, health check-
ups, and referral services to children below six years of age as well as expecting and nursing
mothers. Additionally, it offers non-formal pre-school education to children in the 3-6 age group,
and health and nutrition education to women in the 15-45 age groups.
1.11.9 Ayusmati Scheme the goal of this scheme is to reduce the incidence of Maternal
Mortality and Morbidity. The major objectives of the scheme are to increase the number of
institutional deliveries and to ensure the quality of services.
1.12.10 Central Rural Sanitation Programme was launched in 1986 with an objective of
improving the quality of the life of rural people and provides privacy and dignity to women. The
components of the programme households below the poverty line conversion of the dry latrines

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 27/43
27
to water pour flush toilets, construction of village sanitary complexes for women, setting up of
sanitary marts, intensive campaign for awareness creation and health education etc.
1.12.11 Nutrition Friendly Schools Initiative (NFSI) the main aim is to provide a framework
for designing integrated school based intervention programmes. It addresses the double burden
of nutrition-related ill-health and building on add interconnecting on-going school-based
programmes being implemented by various partner agencies like UNESCO, WHO, WOR LD
BANK etc.
1.12.12 Infant and Young Child Feeding Project (IYCF) the major objectives of the
programme are to create knowledge on Breastfeeding, Timely and appropriate complementary
child feeding, safe infant feeding communities affected by HIV, better maternal nutrition, and the
lactation. This programme was funded by USAID.
1.13 World Health Organisation Child Growth Standards (2011)
1.13.1 Anthropometric Indices
y For children the anthropometric indices were: Body mass index for Age Z-scores (BAZ),
Height-for-Age Z-scores (HAZ), and Weight-for-Age Z-scores (WAZ). These indices
allow comparison between children of different ages.
y Low Height-for-Age Z score (HAZ) indicates µstunting.¶ It is a good indicator for chronic
undernutrition as it does not vary according to short term factors, such as illness. Itsignifies poor environmental conditions.
y Body Mass Index (BMI) is used to compare weight to height ratio of different
individuals. BMI is calculated by dividing the weight in kilograms by the height in
meters squared.
y BMI±for-Age Z score (BAZ), compares BMI of child with the BMI of children of the
same age. Children who have low BAZ are described as being µwasted¶. Wasting is also
sometimes called global undernutrition or global acute malnutrition (GAM).
y Low weight-for-age (WAZ) indicates the child is underweight. Low WAZ may reflect
wasting or stunting. This general property makes WAZ a good indicator for nutritional
status (Onis & Blössner, 2003)20.
Z scores are in reference to The WHO Child Growth Standards (2011) median values as follows
BAZ <-2 SD indicates wasting.
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 28/43
28
BAZ <-3 SD indicates severe wasting.
HAZ <-2 SD indicates stunting
HAZ <-3 SD indicates severe stunting
WAZ <-2 SD indicates undernutrition.
WAZ <-3 SD indicates severe undernutrition.
The WHO growth reference is based on an international group of children. This is appropriate as
a comparison group, as all children grow similarly when their health needs are met. Also any
difference in growth between ethnicities is minor compared to the effect of environment.
(Physical Status...,1995).
For women body mass index (BMI) was used. BMI indicates an adult¶s health status. BMI was
calculated by dividing the weight in kilograms by the height in meters squared. For adults BMI
values are age-independent and the same for both sexes. However different populations have
different body proportion which means the same BMI of people in different nations may have
different nutritional status (WHO Global Database).
BMI classifications for Asian adults are as follows:
Severe thinness, BMI<16.00 (kg/m2)
Moderate thinness, BMI = 16.00 - 16.99 (kg/m2)
Mild thinness, BMI = 17.00 - 18.49 (kg/m2)
Healthy weight, BMI = 18.5-22.9 (kg/m2)
Overweight, BMI>23 (kg/m2)
The WHO international cut-offs are the same with the exception of the cut-off for overweight
being >25 (kg/m2)
1.14 Indian Public Health Standards (IPHS): Indian Public Health Standards (IPHS), which
detail the specifications of standards so that the citizen is confident of getting public health
services in the hospital. These standards are lain down in sub-centers, PHCs, CHCs,
Subdivisional/ Sub-district Hospitals and District Hospitals not only for personal and physical
infrastructure, but also for delivery of services and management. Each Hospital would, as part
of IPHS, be required to set up a R ogi Kalyan Samittee (R KS)/Hospital Management Committee)
which will bring in community control into the management of public hospitals.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 29/43
29
1.15 Goals and Strategies for Eleventh Five Year Plan
1.15.1 Reducing Malnutrition
y Virtual elimination of acute severe malnutrition and reduction in malnutrition among
children under 3 years of age up to at least 25.3% by the end of XIth five year plan.
Malnutrition in children upto 5 years is to be brought down to atleast 30% by 2011.
y Exclusive breast-feeding to be increased to 75%. Complete feeding of infants aged 6-9
months to be increased to at least 80%.
y IYCF practices to be given priority for promotion of feeding best practices.
y Mission mode approach to combat malnutrition among children under 3 years in tribal
areas to be introduced.
y Expansion of Management of Child Malnutrition Scheme throughout the State including
establishment of Malnutrition Treatment Centres (MTCs) in district hospitals.
y Training component for management malnutrition to be strengthened.
1.15.2 Reducing Infant Morbidity & Mortality
y R eduction in Infant Mortality R ate atleast to 32/1000 by the end of XIth five year plan.
Complete immunization coverage to be increased to 90% of children.
y Strengthening Integrated Management Child hood Illness (IMCI) system.
y Empowering families for child care and development.
1.15.3 Reducing Maternal Mortality Ratio
y MMR to be brought down to atleast 148 per one lac of live births by the end of the XIth
five year plan.
y Promotion of institutional deliveries.
y Iron and Folic Acid supplementation to pregnant women.
y
Anemia in women to be reduced to 24.3% by the end of the XIth
five year plan.y Improvement in antenatal services to cover all pregnant women.
y Expansion in emergency delivery services.
y Efforts will be made to provide atleast one medical facility available for 24 hours within
15-20 km radius.
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 30/43
30
1.15.4 Goals and Strategies for Adolescent Girls in Eleventh Five Year Plan
y Issues concerning adolescent girls will be addressed keeping in mind the life cycle
approach.
y Kishori Shakti Yojana to be strengthened.
y School health check up programme to be initiated and expanded to all the schools
including educational institutions for girls.
y Programme on the lines of National Nutrition Mission for providing food grain to
adolescent girls upto 18 years weighing less then 35 k.g. needs to be promoted
throughout the state.
y Mid-Day-Meal programme for girls to be extended upto 10th class.
y Adolescent girls clubs to be formed and supported.
y Specific scheme for non-school going girls in 6 to 11 years of age to be formulated and
implemented.
1.15.5 Goals and Strategies for Nutrition in Eleventh Five Year Plan
y Separate department for food security and nutrition to focus on food security in an
integrated manner is recommended.
y Food and nutrition security and safety policy be developed and implemented.
y Special food and nutrition cell on the lines of Food & Nutrition Board to be setup.
y A system of demonstration in proper cooking methods including counseling on
nutritional requirements to be developed for creating awareness.
y The services of graduate/post-graduates of home science colleges to be utilized in
creating awareness regarding food security and nutrition.
y R egular inspections and quality checks to ensure clean and healthy foods for the
customers at each and every eating place.
y Food and Nutrition visitors proposed to be appointed. Participation of NGOs could be
promoted.y Supply chain under TPDS to be improved to ensure availability of food stock at FPSs.
y Department of Food & Civil Supplies to be strengthened in terms of manpower and
mobility.
y Civil Supplies Corporation recommended to be set up.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 31/43
31
y Strict enforcement of Food Adulteration Act is to be ensured.
y Sufficient stock of food grain and other essential commodities to be maintained at
strategic points particularly in areas frequently facing drought situation.
y Grain Banks could be set up through women SHGs.
y Assessment of poverty levels need to be assessed regularly for appropriate management
of supplies.
1.16 Health and Nutritional Policies and Legislations
1.16.1 Constitutional provisions
Various ministries of the government of India have developed policies related to Health
and Nutrition. Some of the policies deal explicitly with adolescent health and development
issues, whereas others have done so implicitly. Important relevant policies and plans that have
been developed in India include:
1.16.1.1 The Children¶s Code Bill, 2000 presented to the former Prime Minister of Inida, Shri
Atal Behari Vajpayee at a high level meeting attended by Union Ministers and Child R ights
experts on November 14 by Mr. Justice CR Krishna Iyer, Chairperson of the National Expert
Group on Child R ights. The day was observed as the millennium's first children's day.
1.16.1.2 National Health Policy, 1983 (the draft National Health Policy 2000 is in the process
of finalization) aimed at attaining health for all through primary health care. While the policydid not mention adolescence specifically, it emphasized safe motherhood and child survival as
well as the need for the provision of health care for school-going children through the school
health program.
1.16.1.3 National Plan of Action for Children (Planning Commission of India), 1992
commits itself to ensure all rights to all children upto the age of 18 years. The Government shall
ensure all measures and an enabling environment for survival, growth, development and
protection of all children, so that each child can realize his or her inherent potential and grow up
to be a healthy and productive citizen.
1.16.1.4 Decade of the Girl Child, 1991±2000 Department of Women and Child Development
has formulated a National Plan of Action for the SAAR C Decade of the Girl Child (1991-2000
A.D.). The plan of Action is to ensure survival, protection and development of the girl child with
the ultimate objective of building up a better future for the girl child.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 32/43
32
1.16.1.5 National Policy on Child Labor, 1987 scheme was started in 1988 to rehabilitate child
labour. The Scheme seeks to adopt a sequential approach with focus on rehabilitation of children
working in hazardous occupations & processes in the first instance. Under the Scheme, after a
survey of child labour engaged in hazardous occupations & processes has been conducted,
children are to be withdrawn from these occupations & processes and then put into special
schools in order to enable them to be mainstreamed into formal schooling system.
1.16.1.6 National Population Policy, 1997 & 2000 have developed by Indian states for
themselves. Where applicable, these have included concerns about adolescent health and
development. Adolescent health is the domain of the Ministry of Health and Family Welfare and
the Departments of Health and Family Welfare of the states. The Ministry is significantly
involved with the issues of nutrition and development of children, particularly girl children. The
major thrust to adolescent health, however, was given in the Policy. R ecognizing that the needs
of adolescents, including the need for protection from unwanted pregnancies and STIs, have not
been specifically addressed in the past, This Policy underscored adolescent health as a strategic
focus in achieving socio-demographic goals. It aims at ensuring that adolescents¶ need for
information, counseling, population education, and contraceptive services are accessible and
affordable; food supplements and nutrition services are available; and the legislation on restraint
of child marriage is enforced. It also emphasized that reproductive health services for adolescent
girls and boys are especially needed in rural areas, where adolescent marriage and pregnancy are
most prevalent.
1.16.1.7 National Education Policy, 1974 initiative was identified in this Policy, which
recognized the right to education for all segments of the population and made elementary
education for all children compulsory, including adolescent boys and girls. The programs have
been developed and implemented to universalize education and reduce school dropouts,
especially among adolescent girls. In many states, the education of girls is free until the graduate
and postgraduate levels.
1.16.1.8 National Youth Policy, 1986 and Draft New National Youth Policy, 2000 placed
adolescent health as a subsection under the health sector. Youth empowerment and gender justice
were recognized as the major thrust areas of the policy. Apart from various policies, several
legislative provisions have also been introduced that directly or indirectly protect the rights of
adolescents.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 33/43
33
1.16.1.9 National Health Policy-2002 (NHP-2002)
The National Health Policy-2002 (NHP-2002) gives prime importance to ensure a more
equitable access to health services across the social and geographical expanse of the country. The
policy outlines the need for improvement in the health status of the people as one of the major
thrust areas in the social sector. It focuses on the need for enhanced funding and organizational
restructuring of the public health initiatives at national level in order to facilitate more equitable
access to the health facilities. An acceptable standard of good health amongst the general
population of the country is sought to be achieved by increasing access to the decentralized
public health system by establishing new infrastructure in deficient areas, and by upgrading the
infrastructure in the existing institutions. Emphasis has been given to increase the aggregate
public health investment through a substantially increased contribution by the Central
Government. Priority would be given to preventive and curative initiatives at the primary health
level through increased sectoral share of allocation.
1.16.1.10 National Health Policy -1983
The NHP, 1983, was the first attempt to synthesise recommendations of three important
earlier committees, the Bhore Committee of 1946 (Government of India, 1946), the Mudaliar
Committee of 1962 (Government of India, 1962), and the Shrivastav Committee of 1975
(Government of India, 1975, 1976) and the Alma Ata declaration of global demand of Health for
All by 2000. It was largely dictated by global slogans and the field realities in India. All targets
were set to be achieved by 2000, as was in Alma Ata declaration, IMR of 60 by 2000, MMR of
200 by 2000 etc. It also reiterated the resolution of taking health services to the doorstep of the
people and ensuring fuller cooperation of the community, it failed to even declare health care as
a fundamental right of the people and quieted the WHO preamble of 1948 that states, µThe
enjoyment of the highest attainable standard of health is one of the fundamental R ights of every
human being without distinction of race, religion, political belief, economic or social condition¶
None of the health impact goals set in NHP 1983 were achieved by 2000.
1.16.1.11 National Health Policy 2002 and NRHM 2005
The second major policy endeavor is National Health Policy 2002 (NHP 2002) and it closely
followed on the heels of the National Population Policy 2000 ( NPP 2000). Both policies grew
in the context of liberalization and globalization. The concept of Health for All and Health is a
Fundamental Human R ight that was the corner stone of the Soviet Health Policy was given a go

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 34/43
34
bye. After the collapse of the Soviet Union the health programs were also gradually privatized.
However ambitious health goals were set in NHP 2002. NHP 2002 was followed by a massive
National R ural Health Mission launched by the Prime Minister in 2005.
The National Health Policy-2002 (NHP-2002) gives prime importance to ensure a more
equitable access to health services across the social and geographical expanse of the country. The
policy outlines the need for improvement in the health status of the people as one of the major
thrust areas in the social sector. An acceptable standard of good health amongst the general
population of the country is sought to be achieved by increasing access to the decentralized
public health system by establishing new infrastructure in deficient areas, and by upgrading the
infrastructure in the existing institutions. Emphasis has been given to increase the aggregate
public health investment through a substantially increased contribution by the Central
Government. Ministry of Health and Family Welfare is responsible for ensuring safe food to the
consumers. This is done through the Prevention of Food Adulteration (PFA) Act 1954 and the
PFA R ules 1955 made there under. The Food Safety & Standards Act, 2006, a new law
encompassing the domains of various food related laws in the country has been enacted to
revamp the food safety requirements in keeping with modern day needs as well as the
international trend towards modernization. The new law aims to ensure safe, hygienic and
wholesome food for the citizens of the country. It bestows responsibility on the Food
manufacturers, traders etc. to manufacture and supply safe, hygienic and wholesome food. The
Act also provides for compensation to the victim or the legal representative to be paid by vendor
/manufacturer, in case of injury or death of consumer by adulterated / injurious food article. The
Food Safety and Standards Authority of India has been established to implement the provisions /
mandate of this new law, for laying down science based standards for articles of foods and to
regulate their manufacture, storage, distribution, sale and import to ensure the availability of safe
and wholesome food for human consumption.
1.16.1.12 The National Nutrition Policy
The National Nutrition Policy adopted by the Government of India in 1993 under the aegis
of the Depart ment of Women a nd Child Deve lopment, advocated a multi-sectora l
st rategy for eradicating malnutrition and achieving optimum nutrition for all. The
implementation strategy involves setting up Inter Sectoral Coordination mechanism at Centre,
State and District levels, Advocacy and sensitisation of policy makers and programme

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 35/43
35
managers, intensifying micronutrient malnutrition control activities, reaching nutrition
information to people, establishing nutrition monitoring and mapping at State,
District and Community level, and developing district-wise disaggregated data on
nut rit ion. Develop ment of S ta te Pla ns o f Acton on Nutrition by respective States was also
an important mandate. The Objectives of the Policy are:
y To reduce the incidence of severe (8.7 per cent) and moderate (43.8 per cent)
malnutrition by half by the year 2000 A.D.
y All adolescent girls from poor families to be covered through the ICDS by 2000 A.D. in
all CD blocks of the country and 50% of urban slums.
y To increase per capita availability of 215Kg, for that, to achieve production targets of 230
MT by 2000.
y At least 100 days of employment created for each rural landless family, employment
opportunities in urban slum dwellers and urban poor.
y Distribution of iodized salt to cover all endemic areas.
y Nutritional blindness to be completely eradicated by 2000 A.D.
y To expand the Nutrition intervention net through ICDS so as to cover all vulnerable
children in the age group 0 to 6 years.
1.16.1.13 National Rural Health Mission (NRHM) launched in 2005, the difficult areas with
unsatisfactory health indicators were classified as special focus States to ensure greatest attention
where needed. The thrust of the Mission is on establishing a fully functional, community owned,
decentralized health delivery system with inter-sectoral convergence at all levels, to ensure
simultaneous action on a wide range of determinants of health like water, sanitation, education,
nutrition, social and gender equality. The mission is shifting the focus to a functional health
system at all levels, from the village to the district. The architectural correction envisaged under
NR HM is organized around five pillars, each of which is made up of a number of overlapping
core strategies. These five fillers are: (1) Increasing Participation and Ownership by the
Community, (2) Improved Management Capacity (3) Flexible Financing (4) Innovations in
human resources development for the health sector, and (5) Setting of standards and norms with
monitoring.
1.17 National Health Legislative Acts
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 36/43
36
Besides constitutional provisions, some other legislative acts have been promulgated to
safeguard the health and some of the National Health Legislative Acts are:
y Workmen¶s Compensation Act 1912
y The Child Marriage R estraint Act 1929
y The R ed Cross Society Act (Allocation of Property) 1936
y The Drugs and Cosmetic Acts 1940
y The Indian Nursing Council Act 1947
y The Dentist Act 1948
y The Pharmacy Act 1948
y The Drugs (Control) Act 1948
y The Minimum Wages Act 1948
y The Factors Act 1948
y The Employees State Insurance (ESI) Act 1948
y The Plantation Labor Act 1951
y The Mines Act 1952
y The Prevention of Food Adulteration Act 1954 (Amended 1956, 1964,
1971, 1976, 1986)
y The Indian Air Craft (Public Health) R ules 1954
y The Indian Medical Council Act 1956 (Amended 1964, 1993 and 2001)
y The Children Act 1960
y The Maternity Benefit Act 1961
y The Atomic Energy Act 1962
y The R egistration of Birth and Death Act 1969
y The Medical Termination of Pregnancy (MTP) Act 1971 (R ules 1975)
y The Water (Prevention and Control Pollution) Act 1974
y The Air (Prevention and Control Pollution ) Act 1981
y The Dangerous Machines (R egulation) Act 1983
y The Narcotic Drugs and Psychotropic Substance Act 1983
y Juvenile Justice Act 1986
y The Child Labor (Prohibition and R egulation) Act 1986

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 37/43
37
y The Environment (Protection) Act 1986
y The Consumer Protection Act (CPA) 1986
y The Epidemic Diseases Act 1987
y The Mental Heath Act 1987
y The R ehabilitation Council of India Act 1992
y The Transplantation of Human Organs Act 1994
y The Pre-natal Diagnostic Techniques (R egulation and prevention of misuse) Act 1994
y The Persons with Disabilities (Equal Opportunity, Protection of R ights and Full
Participation) Act 1995
y The National Environmental Tribunal Act 1995
y The Biomedical Waste (Management and Handling) R ules 1998
y Immoral Traffic (Prevention) Act, 1956
y The Prenatal Diagnostic Techniques (R egulation and Prevention of Misuse) Act of 1994.
1.18 Committees on Health and Nutrition
1.18.1 Sir John Bhorewas Committee ± 1943 for the first time a committee headed by Sir John
Bhorewas appointed to study the existing health conditions and make recommendations to
prevent communicable diseases, promote health and provide basic health care. It submitted its
report in 1946; the major recommendations therein still form the basis of the Indian public health
system. The committee concentrated on preventive medicine and tried to link health with social
justice. It gave some pragmatic directions recommending population based national net work of
maternity sub-centers (SC-one for 20,000 population), a primary health center ( PHC-one for one
lakh population) and a secondary center , also called the referral center ( SHC-one for each
taluka or teshil) and a specialized hospital with teaching facilities at the district level.
1.18.2 The Mudaliar Committee ± 1962 gave its report in 1962 concentrated on medical
education and development of training infrastructure for static medical units.1.18.3 The Shrivastav Committee ± 1975 gave its report in 1975 urged the training of a cadre
of health assistants to serve as links between qualified medical practitioners and multipurpose
workers (e.g. school teachers, post masters, gram-sevaks, etc.).
1.19 Institutional mechanism for Health and Nutrition
8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 38/43
38
1.19.1 National Nutrition Monitoring Bureau (NNMB) was established under the aegis of
Indian Council of Medical R esearch in the year 1972, with the Central R eference Laboratory at
the National Institute of Nutrition (NIN), Hyderabad. It carries out surveys under the guidance
of a Steering Committee and has been generating dynamic database on diet and nutritional status
of the communities regularly, since inception and it has the following objectives:
To collect, on a continuous basis, on representative segments of population in each of the
States, data on dietary pattern and nutritional status adopting standardized and uniform
procedures and techniques, and
To periodically evaluate the ongoing national nutrition programmes to identify their strengths
and weaknesses and to recommend appropriate corrective measures.
1.19.2 Food and Nutrition Board as reconstituted on 26 July 1990, advises Government,
coordinates and reviews the activities in regard to food and nutrition extension/education;
development, production & popularization of nutritious Foods and Beverages; measures required
to combat deficiency diseases; and 'Conservation and efficient utilization as well as
augmentation of food resources by way of food preservation .and processing.
1.19.3 National Family Health Survey (NFHS) has undertaken height and weight measurement
in a representative sample of children and women at state level. NFHS (I, II &III) provides valid
state level estimates of under nutrition and comparable state level estimates at two time points
i.e. 1992-93, 1998- 99 and 2005-06.
1.19.4 National Sample Survey Organization (NSSO) Conducts every five years the
information on expenditure on food at family level is collected on a statistically adequate and
representative sample all over the country. This information is used to calculate poverty levels
based on expenditure on calories. The disadvantages are that this does not provide information
on dietary consumption at the family and individual level and does not assess nutritional status;
the survey is done only once in 5 years. However, if coupled with the NNMB survey, the data
may provide excellent insights into changing dietary patterns in India.
1.19.5 The Nutrition Society of India (NSI), Hyderabad established in 1967 is an association of
nutrition professionals, programmers and policy makers from India and abroad. It is dedicated to
disseminate the results of the latest research in nutrition ± basic and applied aspects; analyse the
current status of nutrition programmes in the country and recommend appropriate strategies to
promote nutrition of the community at large. The NSI, through its annual meetings provides a

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 39/43
39
forum for young scientists to present their research findings. It is the recognized Indian
representative of
y International Union Nutritional Sciences (IUNS), through the adhering body, Indian
National Science Academy (INSA), and
y Federation of Asian Societies of Nutrition
1.19.6 National Rural Health Mission (NRHM) was launched on 12th April 2005, to provide
accessible, affordable and accountable quality health services to the poorest households in the
remotest rural regions.
i. Establishment of New Born Care facilities and Facility Based Integrated Management of
Neonatal and Childhood Illnesses (F-IMNCI)
ii. Navjaat Shishu Suraksha Karyakram
iii. Integrated Management of Neonatal and Childhood Illnesses (IMNCI) and Pre-Service
IMNCI
iv. Home Based Care of Newborns
v. Universal Immunization
vi. Early detection and appropriate management of Acute R espiratory Infections, Diarrhoea
and other infections
vii. Infant and young child feeding including promotion of breast feeding
viii. Management of children with malnutrition
ix. Vitamin A supplementation and Iron and Folic Acid supplementation School Health
Programme.
1.20 Trends in Policy Development
Although the National Health Policy (NHP) in India was not framed until 1983, India has
built up a vast health infrastructure and initiated several national health programmes over last five
decades in government, voluntary and private sectors under the guidance and direction of various
committees (Bore, Mudaliar, Kartar Singh, Srivastava), the Constitution, the Planning Commission,
the Central Council of Health and Family Welfare, and Consultative Committees attached to the
Ministry of Health and Family Welfare. The period after 1983 witnessed several major
developments in the polices impacting the health sector - adoption of National Health Policy in
1983, 73rdand 74th Constitutional Amendments in 1992, National Nutrition Policy in 1993,

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 40/43
40
National Health Policy in 2002,National Policy on Indian System of Medicine and Homeopathy in
2002, Drug Policy in 2002, introduction of Universal Health Insurance schemes for the poor in
2003, and inclusion of health in Common Minimum Programme of the UPA Government in 2004.
The first National Health Policy in 1983 aimed to achieve the goal of `Health for All' by
2000 AD, through the provision of comprehensive primary healthcare services. It stressed the
creation of an infrastructure for primary healthcare; close co-ordination with health-related services
and activities (like nutrition, drinking water supply and sanitation); the active involvement and
participation of voluntary organisations; the provision of essential drugs and vaccines; qualitative
improvement in health and family planning services; the provision of adequate training; and medical
research aimed at the common health problems of the people. The main objective of the revised
National Health Policy, 2002 is to achieve an acceptable standard of good health among the
general population of the country and has set goals to be achieved by the year 2015. The major
policy prescriptions are as follows:
y Increase public expenditure from 0.9 percent to 2 percent by 2010.
y Increase allocation of public health investment in the order of 55 percent for the primary
health sector; 35 percent and 10 percent to secondary and tertiary sectors respectively.
y Gradual convergence of all health programmes, except the ones (such as TB, Malaria,
HIV/AIDS, R CH), which need to be continued till moderate levels of prevalence are
reached.y Need to levy user charges for certain secondary and tertiary public health services, for
those who can afford to pay.
y Mandatory two year rural posting before awarding the graduate medical degree.
y Decentralising the implementation of health programmes to local self governing bodies
by 2005.
y Setting up of Medical Grants Commission for funding new Government Medical and
Dental colleges.
y Promoting public health discipline.
y Establishing two-tier urban healthcare system - Primary Health Centre for a population of
one lakh and Government General Hospital.
y Increase in Government funded health research to a level of 2 percent of the total health
spending by 2010.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 41/43
41
y Appreciation of the role of private sector in health, and enactment of legislation by 2003
for regulating private clinical establishments.
y Formulation of procedures for accreditation of public and private health facilities.
y Co-option of NGOs in national disease control programmes.
y Promotion of tele medicine in tertiary healthcare sector.
y Full operationalisation of National Disease Surveillance Network by 2005.
y Notification of contemporary code of medical ethics by Medical Council of India.
y Encouraging setting up of private insurance instruments to bring secondary and tertiary
sectors into its purview.
y Promotion of medical services for overseas users.
y Encouragement and promotion of Indian System of Medicine.
Through the 73rdand 74th Constitutional Amendment Acts (1992), the local bodies
(Municipalities and Panchayat) have been assigned 29 development activities, which have a direct
and indirect bearing on health. These include health and sanitation (covering hospitals, PHCs and
dispensaries), family welfare, drinking water, women and child development, the public distribution
system and poverty alleviation programmes.
The Common Minimum Programme announced by the UPA government in 2004 has
proposed to raise public spending on health to at least 2-3 percent of the Gross Domestic Product
(GDP) over the next five years, with focus on primary healthcare. The present Government has
proposed to take all steps to ensure availability of life saving drugs at reasonable prices through
revival of Public Sector Units in the manufacture of critical bulk drugs. The budget 2004-05 has
proposed three major initiatives in the health sector. They are: (i) redesigning the Universal
Health Insurance scheme introduced in 2003 to make it exclusive for below poverty level people
with a reduced premium (ii) introduction of Group Health Insurance scheme for members of Self
Help Groups and Credit Link Groups at a premium of R s 120 per person for an insurance cover
of R s 10000, and (iii) exemption of income tax for the hospitals working in rural areas.
1.21 Health Expenditure
The amount allocated during five year plans in India for health and family welfare and total
investment can be seen in the table 4.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 42/43
42
Table 4: Status of Expenditure in F YPs (Rs. in Crores)F YPs Total Plan Investment Health Family Welfare
I 1960.0 65.2 0.1
II 4672.0 140.8 2.2
III 8576.0 225.0 24.9
IV15778.8 335.5 284.4
V 39322.0 682.0 497.4
VI 97500.0 1821.0 1010.0
VII 180000.0 3392.0 3256.2
VIII 798000.0 7575.9 6500.0
IX 859200.0 10818.0 15120.2
X 1484131.3 31020.3 27125.0
XI 2156571.0 136147.0
(S ource: S tate Institute of Health and F amily Welfare, Jaipur)
References:
1. Census of India, 2011
2. Anne Tinker, Kathleen Finn, and Joanne Epp. (June 2000). Improving Women¶s HealthIssues and Interventions, Health, Nutrition and Population ( HNP) Discussion Paper , TheWorld Bank.
3. III National Family Health Survey, 2006.
4. Satyarupa Shekhar Jay Chaudhuri (2011), ³Integrated Child Development Services
(ICDS) scheme in brief´ Centre for Development Finance, IFMR , Chennai.
5. UNICEF (1998) State of the World¶s Children. New York. pp 7±87.
6. World Health Organization Expert Committee, 1965.
7. National Family Health Survey (NFHS), 1998±99.
8. Pelletier, D. L. 1994. The relationship between child anthropometry and mortality in
developing countries: Implications for policy, programs and future research. Journal of
Nutrition S upplement 124(10S): 2047S±2081S.
9. R uzicka, L. T. and P. Kane. 1985. Nutrition and child survival in south Asia. In K.
Srinivasan and S. Mukerji, eds. Dynamics of population and family welfare, pp. 333± 57.
Bombay: Himalaya Publishing House.
10. Sommer, A. and M. S. Loewenstein. 1975. Nutritional status and mortality: A prospective
validation of the QUAC stick. American Journal of ClinicalNutrition 28(3): 287±92.
11. Chen, L. C., A. K. M. A. Chowdhury, and S. L. Huffman. 1980. Anthropometric
assessment of energy-protein malnutrition and subsequent risk of mortality among preschool aged children. American Journal of Clinical Nutrition 33(8): 1836±45.
12. Vella, V., A. Tomkins, A. Borghesi, G. B. Migliori, B. C. Adriko, and E. Crevatin.
1992a. Determinants of child nutrition and mortality in north-west Uganda. Bulletin of
the World Health Organization 70(5): 637±43.
13. Vella, V., A. Tomkins, J. Nidku, and T. Marshall. 1992b. Determinants of child mortality
in south-west Uganda. Journal of Biosocial S cience 24(1): 103±12.

8/3/2019 Good Health is Fundamental to Living a Productive Life
http://slidepdf.com/reader/full/good-health-is-fundamental-to-living-a-productive-life 43/43
14. Santhanakrishnan, B. R . and R . R amalingam. 1987. R isk factors of mortality in children
with diarrhoeal disease in Madras, India. Journal of DiarrhoealDisease Research 5(1):
36±9.
15. Katz, J., K. P. West, Jr., I. Tarwotjo, and A. Sommer. 1989. The importance of age in
evaluating anthropometric indices for predicting mortality. American Journal of
Epidemiology 130(6): 1219±26.
16. Briend, A., B. Wojtyniak, and M. G. M. R owland. 1988. Breast feeding, nutritional
status, and child survival in rural Bangladesh. British Medical Journal 296(6626): 879±
82.
17. Balgir R S, Kerkatta AS, Murmu B, Dash BP (2002) ³Clinical assessment of health and
nutritional status of Gond children in Kalahandi district of Orissa´, Indian Journal of
Nutritionan Dietetics, 39(1): 31-37.
18. Brunner E (1997) ³Inequalities in diet and health´, In: PS Shetty, K McPherson (Eds.):
Diet, Nutrition and Chronic Disease: Lessons from Contrasting World, Chichester : John
Wiley & Sons, Inc., pp.77-94.19. Danzon M, Donohue J (2000) Foreword. In: Michaelsen KF, Weaver L, Branca F,
R obertson A, eds. Feeding and nutrition of infants and young children. Geneva: UNICEF.
pp ix±xx.
20. State of the World¶s Children. New York. pp 7±87, UNICEF 1998
21. Onis, M., Blössner, M. (2003). The World Health Organization Global Database on Child
Growth and Malnutrition: methodology and applications. International Journal of
Epidemiology, 32, 518-26.
Websites
www.wcd.nic.inwww.nipccd.nic.in
www.worldbank.org
www.cag.gov.in
www.wcd.nic.in/icds.htm