gillette children’s specialty healthcare · pmr (physical medical ......
TRANSCRIPT
Gillette Children’s Specialty Healthcare
16Sep~27Sep 2013
Katrine Chau, QEH
Sanne Fong, PMH
1

Multi-disciplinary visit 2 Occupational Therapists Katrine Chau, QEH Sanne Fong, PMH 4 Nurses
Overseas Corporate Scholarship Program for AH Professionals 13/14 –
Gillette Children’s Specialty Healthcare
on 16Sep~27Sep 2013
2

Why we choose Gillette Children’s Specialty Healthcare (GCSH) to visit?
3
GCSH provides the highly specialized care that children who have disabilities and complex conditions need. The expertise’s are known worldwide. Gillette Children's is always changing to meet the needs of children, adolescents and young adults, providing medical treatment and technology to care for children with disabilities and chronic conditions
Objectives
1. Compare and contrast the service organization and care delivery model between overseas and Hong Kong
2. Explore the feasibility of adopting new service model / protocols/ guidelines in Hong Kong
3. Acquire an understanding of the disease / condition management 4. Appreciate the collaboration of the multi-disciplinary team in
related care service 5. Gain an understanding on the inter-facility communication and
coordination to ensure continuity of care 6. Identify the areas where training needs to be improved and able to
set up associated training curriculum for service development 7. Evaluate the effectiveness of related services through Allied Health
quality framework
4
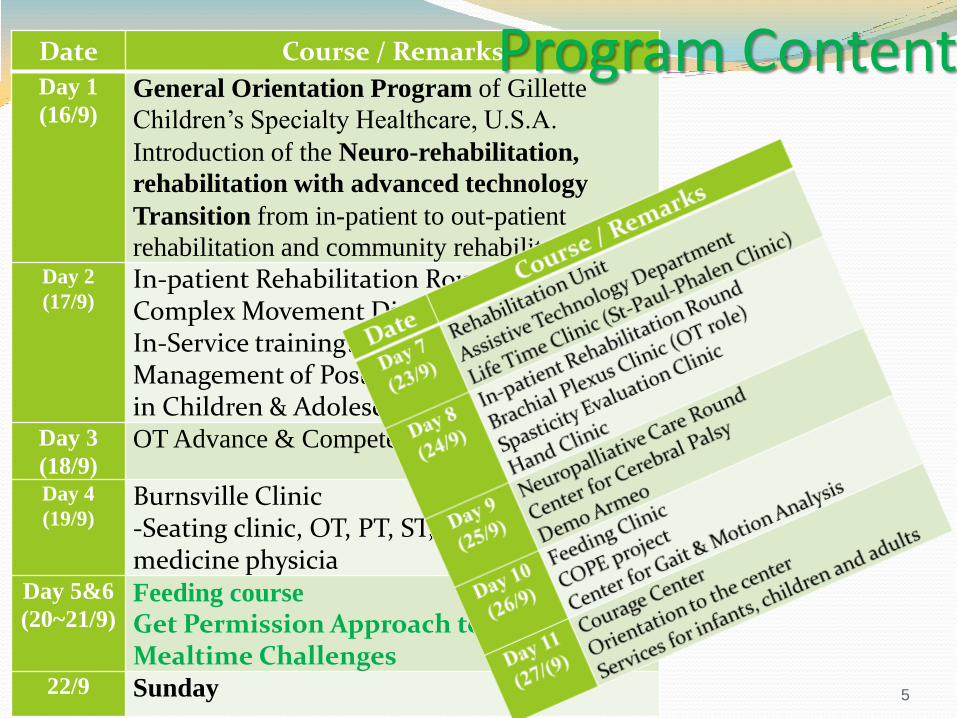
Date Course / Remarks
Day 1
(16/9) General Orientation Program of Gillette
Children’s Specialty Healthcare, U.S.A. Introduction of the Neuro-rehabilitation,
rehabilitation with advanced technology Transition from in-patient to out-patient
rehabilitation and community rehabilitation Day 2
(17/9) In-patient Rehabilitation Round Complex Movement Disorder Clinic In-Service training: Psychiatric & Behavioral Management of Post Concussive Syndrome in Children & Adolescents
Day 3
(18/9) OT Advance & Competencies
Day 4
(19/9) Burnsville Clinic -Seating clinic, OT, PT, ST, ATD, Rehab medicine physicia
Day 5&6
(20~21/9) Feeding course
Get Permission Approach to Sensory Mealtime Challenges
22/9 Sunday 5
Program Content

Services
6

Services of the center Rehabilitatioin Therapies
Upper-Extremity Therapy Services
Seating and Mobility Evaluations
Assistive Technology Services
Feeding clinic ~ Information for Familites and Health-care Providers
Neurotrauma Clinic
Center for pediatric Neurosciences
Gillette Lifetime Specialty healthcare: St. Paul – Phalen clinic
Center for Gait and Motion Analysis
7
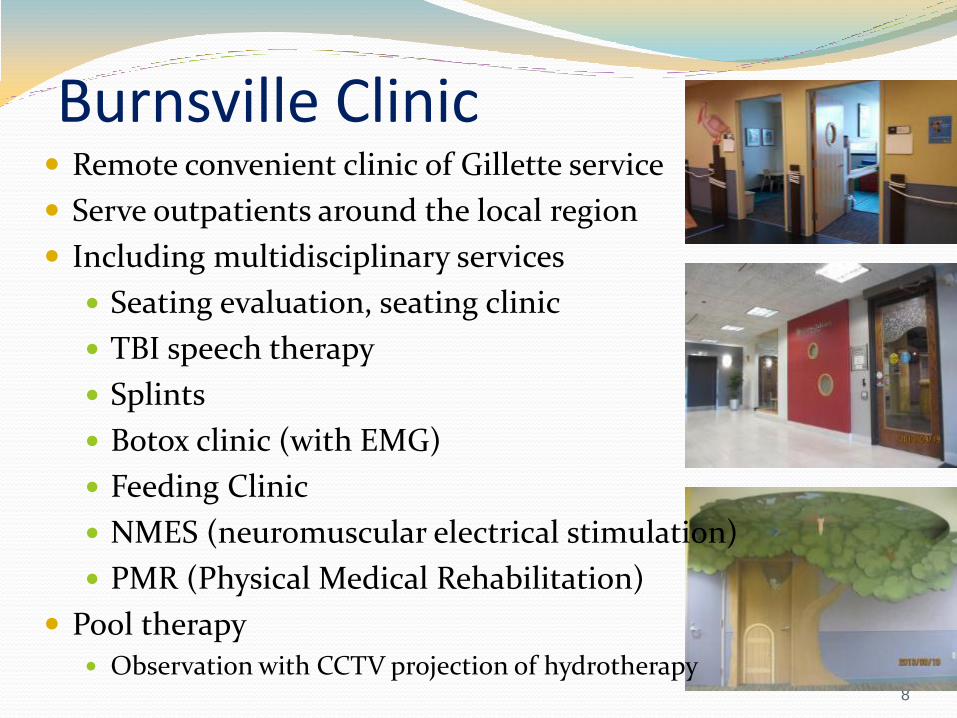
Burnsville Clinic
8
Remote convenient clinic of Gillette service
Serve outpatients around the local region
Including multidisciplinary services
Seating evaluation, seating clinic
TBI speech therapy
Splints
Botox clinic (with EMG)
Feeding Clinic
NMES (neuromuscular electrical stimulation)
PMR (Physical Medical Rehabilitation)
Pool therapy Observation with CCTV projection of hydrotherapy
Complex movement Clinic Jointly seen by Rehabilitation medicine physician,
neurologist and neurosurgeon
For decision of medical treatment for complicated cases
9
Feeding Clinic Jointly assessed by OT, ST & Dietitian
OT: oral-motor skills and sensory based issues,
feeding skills of care giver; meal preparation,
ST: swallowing skills and VFSS; vital stimulation
Dietitian: nutritional issue, concerning intake, supplement, ? Knowledge of gastrotomy
=> generate a new/ optimal schedule of meal time and use of supplement; best posture, mehtod and support during swallowing

Respiratory Therapist >30 RT shared between Regions hospital, and Gillette Childrens
Consultation by referral
For all pulmonary and respiratory problems for paediatric and adult cases
Care giver and nurses education, suction, change of trache, titration of oxygen; recommendation of ventilator and mode of use and other accessories for resp problems
Just for in-patients, ensure patient can return to home with optimum level of support
? IDSP program model for tele-medical consultation by nurses
Then cases will be follow up in OPD by physician
10
Advocacy of Family support
Family Voices of Minnesota ~ keeping families at the center of health care
Parent to parent
Do you know a child who could benefit from a medical grant?
Kids live better at home
Pacer Center~ champions for children with disabilities
Pediatric services : providing exceptional care for children at home
Helping more families find strength in numbers begins with 1
11

Family service Recreation therapy
12

AAC Jointly assessed by SLP and OT and provide treatment
To get the cognitive level/ response level of clients
Try out different kind of switches
13
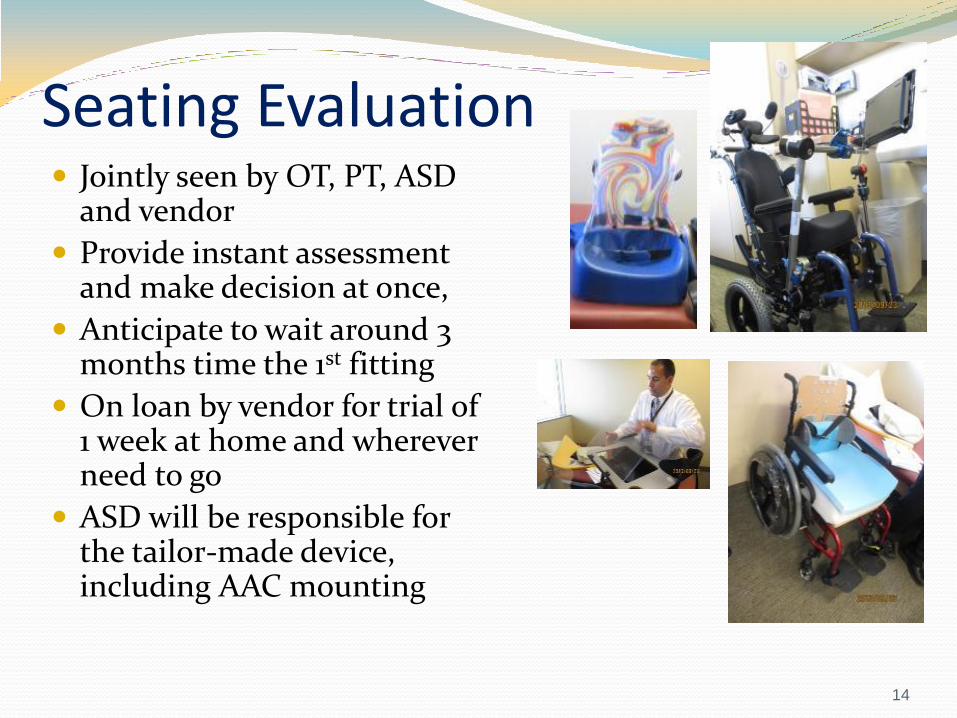
Seating Evaluation Jointly seen by OT, PT, ASD
and vendor
Provide instant assessment and make decision at once,
Anticipate to wait around 3 months time the 1st fitting
On loan by vendor for trial of 1 week at home and wherever need to go
ASD will be responsible for the tailor-made device, including AAC mounting
14
Lifetime Clinic Cater for cases transition from paediatric to adult
Out-patient base
? All Gillette case will be entertain in Lifetime Clinic?
CP
Epileptic
Spinal bifida
Neuromuscular
poliomyelitis
Provide continuum care
Tackle multiple problems in adult life including sex counselling
15

Lifetime Clinic
Efficient One-stop service as patients live far away
Self-finance => fund raising projects
Patient & family-centred service model
Brachial Plexus Service Clinic, seen by orthopaedic surgeon
Pre-clinic Hand function assessment (Active Movement Scale, Modified Mallet Assessment) with recommendation for home programme
Hand splint;
Scar management
17
Hand Clinic Evaluate by hand surgeon
Expect OT will fix the condition upon referral on the same day

Spasticity evaluation PT
OT
Rehabilitation Physical medicine
Neurosurgeon
Ortho physician
18
Advanced clinics Complex movement disorder clinic
(physician, neuro-surgeon, nurse, neurologist)
Spasticity Evaluation clinic (physician, ortho surgeon, neurologisst)
Therapist’s role: pre-clinic assessment and video taking

Armeo demo Provide environment for gravity assistive training
(not robotic)
Benefit those cases with acute phases
TBI
Young stroke
SCI
Brachial plexus injury
? Hemiplegia
3 sessions x6weeks or 2 sessions x9 weeks
19
Gait analysis
4 PT & 5 engineer/technician, 1 PTA
15 gait analysis, make recommendation
For diagnostic purpose, pre-surgery assessment, then follow up one year, one-stop-service
Energy consumption as outcome indicator of treatment
Dynamic EMG for both LE & UE with instant video
20
Courage Centre Out-patient rehabilitation, 40 in-patient beds waiting for foster-family
Pool & gym are program based, open to public PH as recreational facilities
ABLE program 3sessionsx5daysx12weeks
Activitiy-Based-Locomotor-Exercise, run by fitness specialists
For SCI & neuromuscular condition (11 to 60)
Wellness and fitness of clients
Vocational rehabilitation (4 weeks job-readiness training) Assessing and training of ability, skills, behaviour
AT introduced by staff who is severely handicapped
SPORTS & recreation
Clinic
Multiple purpose Rm: AAC & Tele-medical consultation
Paediatric & adolescent service
Thera-suit method
Healing garden
Dr. pet visit daily
21

Patient management / Service model**
22
Inpatient Rehabilitation Round Coordinated by Rehabilitation coordinator, lead by paediatrician Weekly round for setting goal of rehabilitation plan, Priority for
the week ahead (how to support goal for d/c) Case information Medical update Goal for discharge, with discharge date (will be changed according
to patient’s progress) Community re-entry Family education Equipment Positioning/mobility Cognition Medical Selfcare Transition (to out-patient)
family dynamic Strength Barriers
23
Inpatient Rehabilitation Round Protocols/ treatment guidelines of specific disease
such as SDR
Role delineation among OT, PT, CP & ST
Role of OTA
Who is responsible for training of PCA?
Licensing of home visit
24

Integrated Rehabilitation Plan
In addition to rehabilitation round, discharge goal
Treatment goals and progress will be recorded right after treatment;
Record in the EDM system
All disciplines can share the progress of the case
WeeFim will be filled by different disciplines
Rehabilitation plan will match with the discharge goal set in Rehab round
Discharge summary that indicate difference between initial in-take and pre-discharge status
25

Neuro-palliative care round Weekly round
Team members included:
Physician
Social worker
Chaplian
Nurse
Pharmicist
No fixed ward for palliative, but referral based,
Prepare parents for planning of “end-of-life” service
26
Discharge process Patient-family service
More community based, social worker will due with the community service; ? Need for financial support, home helper, home modification
CP will liaise with school for additional help to school, personal assistant in school
Biweekly family conference, whoever involved in the treatment of the case will sit
Checklist according to discharge plan
27
Nurse round

Facilities
28
Healing Garden Donated by a family that has benefited from Gillette, the
family involved in design => design from user’s perspective
Different texture of floor
Ramp and stairs
Multisensory
Musical instrument
Shaded area: mail box for ventilate joys or sorrows
Different plants
Playground facilities, for climbing and crawling,
Limited entry, for Rx purpose
Playhouse
30

Healing Garden in Gillette

Ronald McDonald House Build inside the hospital
Daily operated by volunteer
Home like atmosphere
Support 3 families
Free for food, laundry service
For transition
For parents’ overnight
Provides respite, comfort, convenience to a New Community of Familities
32
Laundry service by parents
Family resource centre
Double bed room and single bed room vs isolated bed
Bathing facilities
Fund donation
Printing material of individual needs
d/c from hospital => school with IEP,
Service government subsidy vs private insurance
33

34
Patient Resource Centre
Gait Lab
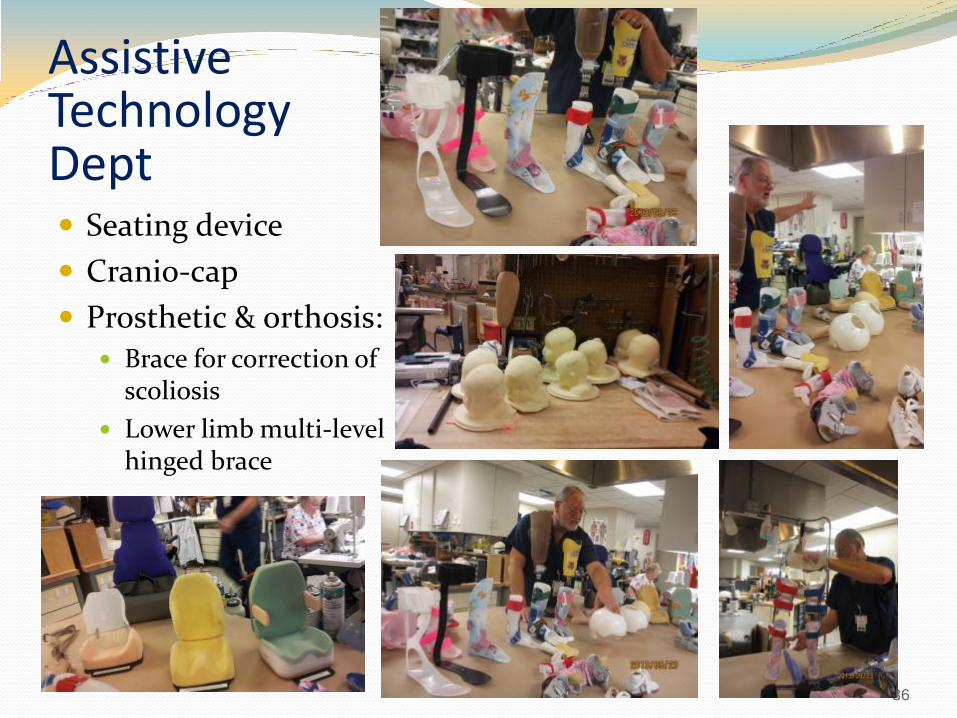
Assistive Technology Dept Seating device
Cranio-cap
Prosthetic & orthosis: Brace for correction of
scoliosis
Lower limb multi-level hinged brace
36
Assistive Technology Dept Efficient
Brace in 1-2 days
Participated in seating evaluation, tailor-made seating device, with commercially available frame from vender
Clear role delineation of technician and clinical staff
Attend Rehab Round
Colourful material with client’s preference
Material are more advanced => enhance efficiency
Use of CAD
37

Information from patients’ perspective Educational material for self management
38
Educational pamphlets
Epilepsy life stages ~ preteens and early teens
Brachial plexus injuries
Juvenile rheumatoid arthritis
Neuromuscular conditions
Center for Cerebral Palsy
Managing Spasticity~ our family-focused approach to treatment
Cerebral palsy Road map: what to expect as your child grows
39

Educational pamphlets for parent
40
• Mobility
• Musculoskeletal
• Communication and cognition
• Feeding and Nutrition
• Social/ Emotional Development
and Behaviour
• Self-Care and Daily Living Skills
• Sensory Functions
• Recreation & Fitness
Assessment and Intervention
Key providers in Care Team

Educational package
After your injury ~ information and resources about neurotrauma
Working together: your guide to Brain injury rehabilitation at Gillette
41
Package encourage self-management
All About me
At a glance: my health information, medical needs and relevant documents
Make your move! A transition guide for teens
42

Tube feeding for love educational workshop for parents and care givers Information from expert (Marsha Dunn Klein)
Sharing among parents
Introduction of the web-site “meal time notions”
Offer information for parents Tube feeding with potential to change into oral feeding
Keep interact with babies during the tube feeding process
Workshop runs after office hour to facilitate working parents to participate
43

Staff development
44
In-service training Psychiatric Management of child & adolescent with concussion Culturally related due to high volume of sports injury
among kids and adolescent, considered as Neuropsychiatric disorder, will last for 6/12
6-35% mild TBI result in post-concussion syndrome
Collaboration of medical, rehabilitation and psychiatric for follow up the case and family
ADHD symptoms, depression, anxiety, irritability
Functionally include poor sleep quality
Rx methodology: CBT, behavior intervention for sleep
Grief as kids may not be able to return to previous sports
45

OT Advance leadership workshop OT competency
Evidence based
outcome
Pros & cons of specialization,
? Wise therapy investment
What to do in the next 5 years
46

The Center for Pediatric Rehabilitation The inpatient rehabilitation programs and services include:
Acquired Brain Injury Program (BI)
Cerebral Palsy Program-Selective Dorsal Rhizotomy Service (SDR)
Other Comprehensive Inpatient Medical Rehabilitation (CMR)
Spinal Cord Injury Program (SCI)
Rehabilitation post Complex Orthopedic Surgery –Single event multilevel surgery (SEMLS) Service
There are 18 in-patient beds in Gillette’s rehabilitation units.
In general, the patient’s length of stay is 3 to 6 months. On average, the number of admission is 105 per year.
47

48
Manpower There are many part-time staff in Gillette and their working
hours are very various. This flexibility in working hours results
in low turn-over rate. In September 2013, the overall full-time
equivalents (FTE) manpower is 1111.
Case observation PT with Locomat
School for Mathematics
OT for electrical stimulation
ST
2xsessions PT, 2xsessions OT, 2xsessions School 2xsessions ST 1x music therapy 1x recreation therapy
49

People we met in
Gillette Children’s Specialty Healthcare
FEEDING COURSE Marsha Dunn Klein, M.Ed., O.T.R./L.
Tonya (OT)
Advance Technology Department
Lifetime Clinic
Hand Clinic w/
Dr. Ann Van Heest
Whole team dine with Janey (PT), Tonya (OT) & Candace Vegta (SLP, course coordinator)
Dr. M Gormley Paediatric Rehab
Medical Physician
Team life in Twin Cities
52
Objectives 1. Compare and contrast the service organization and
care delivery model between overseas and Hong Kong
• PCA service facilitate return to home (over-night, or 24 hr PCA can be parents, but hired by rehabilitation agent)
• Level 1 trauma centre, supported by rehabilitation service • Cases referred by other hospitals, follow through the rehabilitation,
• Screen by Rehabilitation Coordinator, endorsed by rehabilitation physician, then further assessed by nurse; and team evaluation
• No NICU, but situated in Region Hospital • Neurosurgeon will support other hospitals • Ronald McDonald Family Home => transition home to facilitate return to
home programme • No step down service • Emphasize on education of care taker, PCA, • Rehabilitation Garden
53
Objectives
2. Explore the feasibility of adopting new service model / protocols/ guidelines in Hong Kong
• Pre-surgery thorough assessment and planning for SDR cases (same in HK)
54

Objectives
3. Acquire an understanding of the disease / condition management
• Parent-to-parent volunteer service as peer support
• Complex movement clinic
• Spasticity evaluation clinic (same in HK)
• Hand clinic (same in HK)
55
Objectives
4. Appreciate the collaboration of the
multi-disciplinary team in related care service
• Early discharge plan
• Mini-round (everyday), each case with a mail box, include nurses, physician and therapists
• Multidisciplinary weekly round, coordinated by rehabilitation coordinator,
• Task specific, with a separate team for planning of rehabilitation schedule, with automatic system for pottering of patient that saved professional time; patient and relative can refer to the schedule and empower self-management
56

Objectives 4. Appreciate the collaboration of the
multi-disciplinary team in related care service
• Social work, CP & rehabilitation coordinator
• Chaplain
• OT, PT, ST
• Physician, case surgeon,
• Handover time include not only nurse but also assistants
57
Objectives 5. Gain an understanding on the inter-facility
communication and coordination to ensure continuity of care
• Partner with other hospitals and set up satellite clinics
for regional population
• Burnsville Clinic in Fairview Pediatric Rehabilitation
• Courage Center in Golden Valley
58
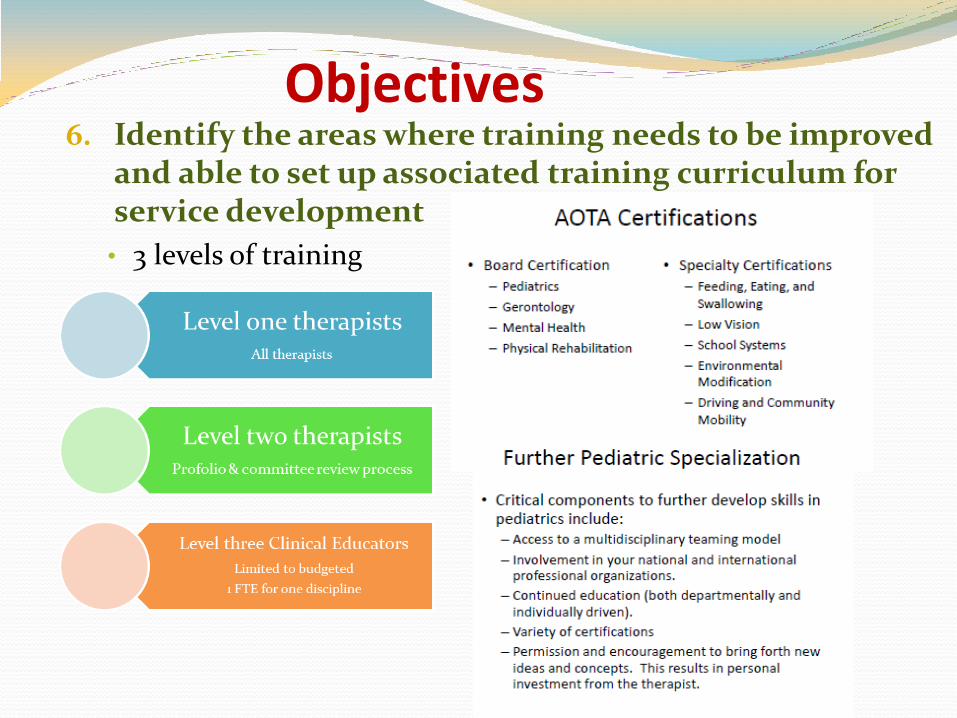
Objectives 6. Identify the areas where training needs to be improved
and able to set up associated training curriculum for service development
• 3 levels of training
59

Objectives 7. Evaluate the effectiveness of related services through
Allied Health quality framework Services being observed include inpatient acute rehabilitation,
out-patient services for both pediatric and transition to adult clinic, Feeding Clinic, Seating evaluation, Brain Injury Program, Brachial Plexus Clinic.
Centers of Excellence included Center for Cerebral Palsy, Center for Pediatric Neurosciences, and Center for Pediatric Rehabilitation.
GCSH has partner with other hospitals and set up satellite clinics for regional population, including Burnsville Clinic in Fairview Pediatric Rehabilitation, Courage Center in Golden Valley. Both facilitate clients with disability transition from adolescent to adulthood.
Training and supervision of professional staff are centralized so that service are aligned and much cost-effective.
60

Additional points to learn from GCSH:
Joint a 2 days multidisciplinary certificate course in feeding. Audiences included occupational therapists, speech pathologists, and dietitians. Hence all parties will share similar language for communication.
Appreciate the collaboration of the multi-disciplinary team in related care service
Gain an understanding on the inter-facility communication and coordination to ensure continuity of care
could identify some improved areas for setting up associated curriculum or service guideline
61

Care Team ~ Key providers are in bold
Adaptive Equipment Specialist/
Vendor of Medical Equipment
Audiologist
Child Life Specialist
Neurodevelopmental Pediatrician
Neuropsychologist / Psychologist
Nurse/ Nurse Practitioner
Orthotist
Ophthalmologist
Pediatric Neurologist
Pediatric Neurosurgeon
Pediatric Orthopedist
Pediatric Rehabilitation Medicine Physician
Respiratory Therapist
Sleep Health Specialist
Social Worker
Therapeutic Recreation Specialist * (done by OT in HK)
Occupational Therapist
Physical Therapist
Speech and Language Pathologist
62
Multi-disciplinary activities
63
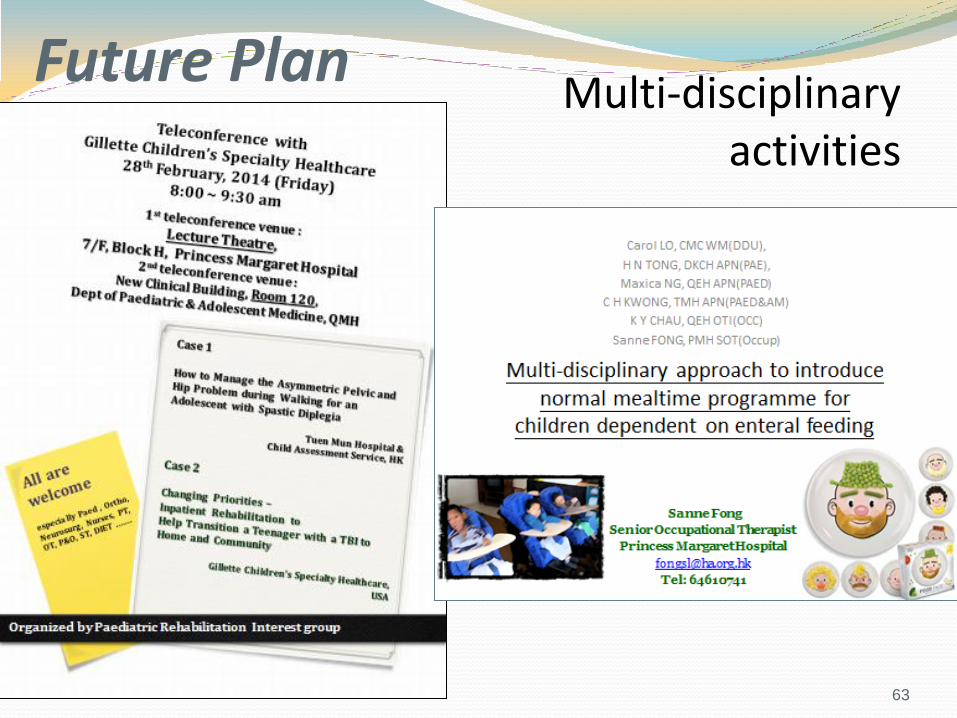
Future Plan
Multi-disciplinary approach to introduce normal mealtime programme for children dependent on enteral feeding
Plan:
To implement a pilot multidisciplinary normal mealtime programme for children in need of tube-feeding in CMC, DKCH, QEH, TMH and PMH.
Long term goal:
to develop a protocol for encouraging children in need of GT feeding to receive proper treatment without losing feeding ability
Short term goal:
to try a one-year pilot cross-district multidisciplinary project including nurse and OTs in education of family of GT care and oral-feeding training
Common challenges

Action plan in principle and brief schedule Plan/ Item Details Timeframe
Arrange presentation to ask for support from clinical department
Identify inclusive criteria 1. Those just decided to have GT 2. Those kids may consider wean off GT
1Q2014
To develop written education material for parents and introduce to related professions
1. Nurse: in stoma care, NGT care 2. OT: importance of normal meal time
1Q2014
Recruitment of cases
To identify outcome measures for the pilot study And recruitment of cases (3-4 cases x 5 hospitals = 15-20 cases)
2Q2014
To introduce treatment guideline/ protocol to other hospitals
Documentation Preliminary result analysis Final analysis
4Q2014 1Q2015

Detail action plan for pilot project Suggested actions Details
Responsible colleagues
Schedule
Get Clinical support to implement the project in the 5 hospitals
Dr. Bill Chan (UCH), Dr. CK Li (PWH) Dr. CY Lee (CMC), Dr. Kwong L(TMH) Dr. W Tse (QEH), Dr. N Tse (PMH) Dr. SL Lee (QMH/DKCH)
Carol & Sanne
4Q2013
Define Inclusive criteria
1. Children fed by NG/ gastrostomy/gastro-jejunostomy tube, 2. Medically stable and safe oral feeding 3. Caregiver would actively participate in the feeding
training/ treatment
Katrine & Maxica
4Q2013
Suggest and design documentation format of outcome measure
1. Amount of oral intake (frequency, tolerance), pre-post 2. Feeding behavior checklist (still searching Chinese
validated tool) 3. Enjoyment of mealtime satisfaction (subjectively rate by
caregiver)
Template ready by 1Q 2014
Educational pamphlet 1. Feeding material 2. Gastrostomy care 3. NGT care
OT team Nurse team Nurse team
1Q 2014
Implementation of the project
1. start oral feeding training by OT when they are in-patient; 2. Education on tube feeding and care will be provided by
nurse before discharge. 3. Follow up in OPD by OT
Joint disciplines effort
2Q 2014
Data analysis OT team 4Q 2014
Introduce treatment guideline/ protocol to other hospitals +/- NGOs
Joint disciplines effort
1Q 2015
Inspirations / reflections Training of therapists
Invite expert to deliver special topic
Encourage therapists to take up research projects by funding => LR, suggest project, implementation
Manpower
Allow different contract type => for retain staff
Support by volunteers
Fund raising for special projects
67
HKCH … a centre of excellence that provide client-centred service
68