gi and liver - continuing medical education - ucsf medical … rockey … · ·...
TRANSCRIPT
October 26th, 2012
GI and Liver
Don C. Rockey
Rockey 2012
A 48‐year‐old man with chronic alcoholism is evaluated because of progressive abdominal distention.
He complains of anorexia, weakness, and a 9‐kg (20‐lb) weight loss over the past six months.
Physical examination is unremarkable except for a temperature of 37.6 C (99.6 F), ascites, and signs of weight loss.
Rockey 2012
Laboratory studies:
Hemoglobin 13.9 g/dLHematocrit 41%Leukocyte count 7200/cu mm;
(normal differential)Serum aminotransferases:
AST 184 U/LALT 90 U/L
Serum alkaline phosphatase 116 U/LSerum bilirubin:
Total 1.1 mg/dLDirect 0.3 mg/dL
Serum albumin 3.1 g/dL
Rockey 2012
Radiograph of the chest is normal. Ultrasound examination of the abdomen demonstrates ascites. Paracentesis yields clear, nonbloody fluid. Ascitic fluid leukocyte count is 760/cu mm (70% mononuclear cells), protein is 4.4 g/dL, and albumin is 2.6 g/dL.
Rockey 2012
Which of the following is the most likely diagnosis?
(A) Cirrhosis with spontaneous bacterial peritonitis(B) Tuberculous peritonitis(C) Liver metastasis(D) Portal vein thrombosis
Rockey 2012
Serum albumin 3.1 – Ascitic fluid albumin 2.6 =
0.5
Serum‐Ascites Albumin Gradient (SAAG)
Rockey 2012
Easily the most useful test in the evaluation of ascites. A high gradient - difference of greater than 1.1 g/dl - identifies
portal hypertensive causes of ascites A low gradient - difference of less than 1.1 g/dl - identifies non
portal hypertensive causes of ascites In a study by Runyon et al (AIM ‘92), 1275 patients were
prospectively evaluated with paired serum and ascitic fluid samples.
The ascitic fluid total protein (AFTP) classified only 56% of cases correctly, compared to the SA gradient, which classified 97% correctly. Of interest, the AFTP did appear to separate most sterile cirrhotic ascites (AFTP < 2.5 g/dl) samples from cardiac ascites (AFTP > 2.5 g/dl)
Serum‐Ascites Albumin Gradient (SAAG)

Rockey 2012
Serum‐Ascites Albumin Gradient (SAAG)
Rockey 2012
Serum‐Ascites Albumin Gradient (SAAG)
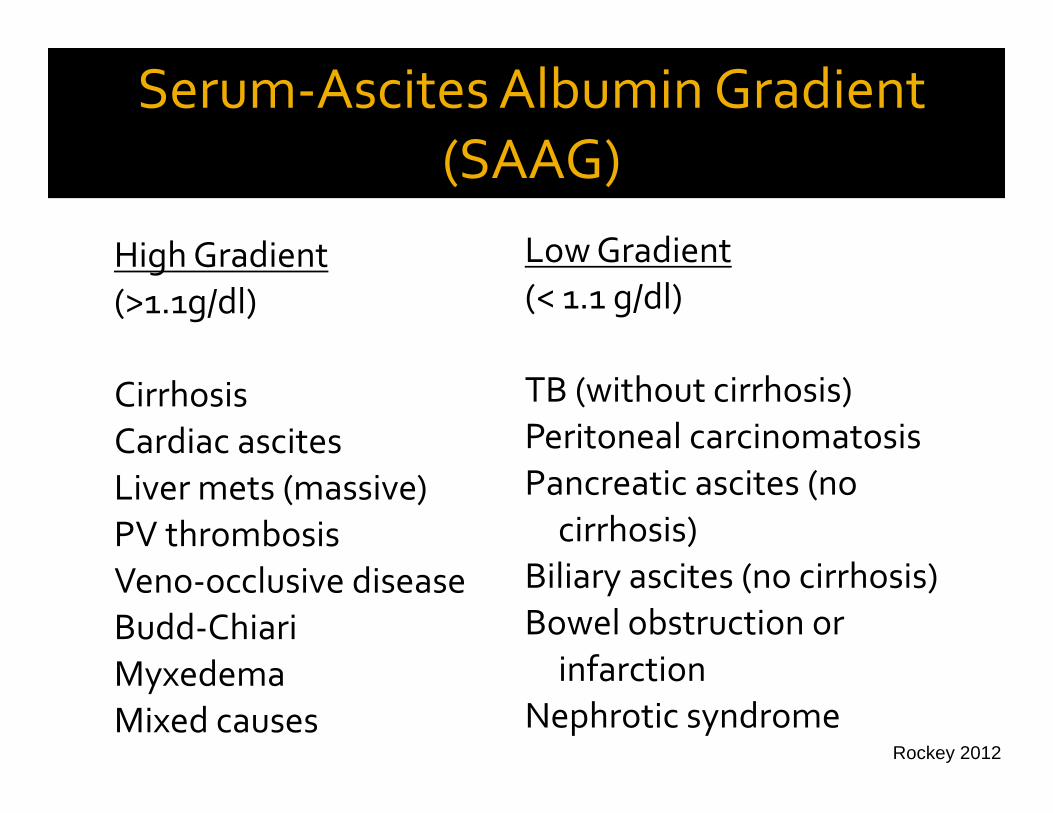
High Gradient(>1.1g/dl)
CirrhosisCardiac ascitesLiver mets (massive)PV thrombosisVeno‐occlusive diseaseBudd‐ChiariMyxedemaMixed causes
Low Gradient(< 1.1 g/dl)
TB (without cirrhosis)Peritoneal carcinomatosisPancreatic ascites (no cirrhosis)
Biliary ascites (no cirrhosis)Bowel obstruction or infarction
Nephrotic syndrome
Rockey 2012
Which of the following is the most likely diagnosis?
(A) Cirrhosis with spontaneous bacterial peritonitis(B) Tuberculous peritonitis(C) Liver metastasis(D) Portal vein thrombosis
Rockey 2012
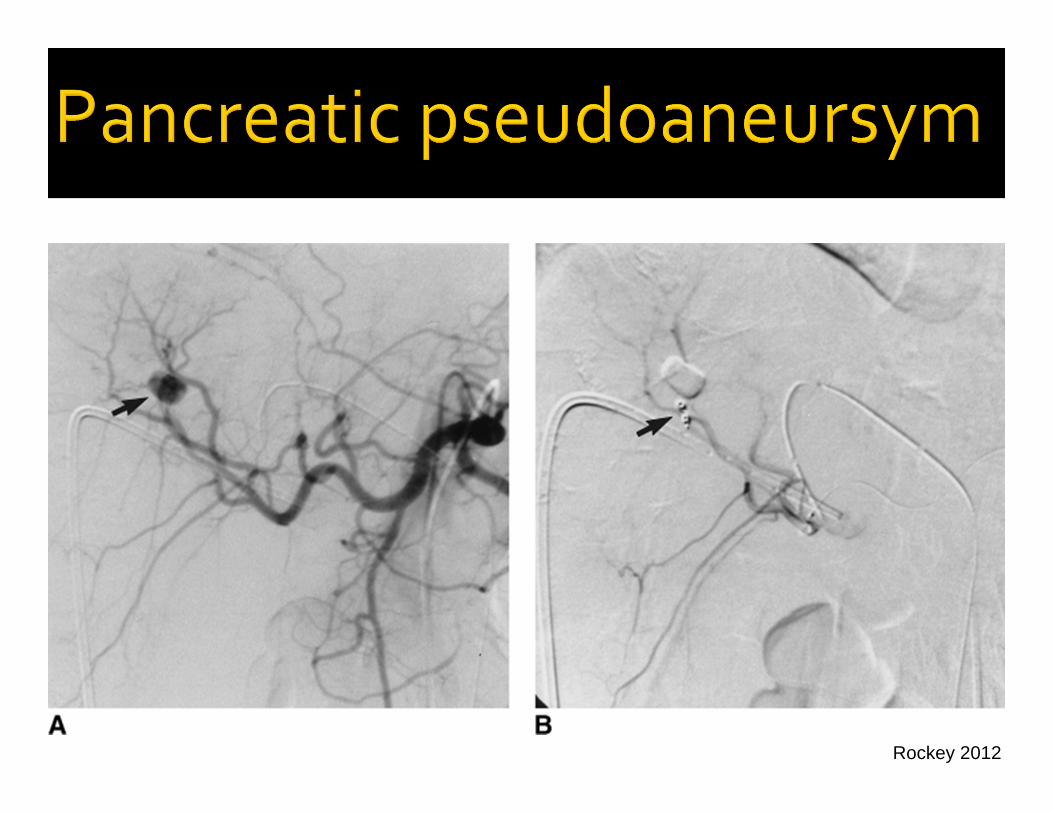
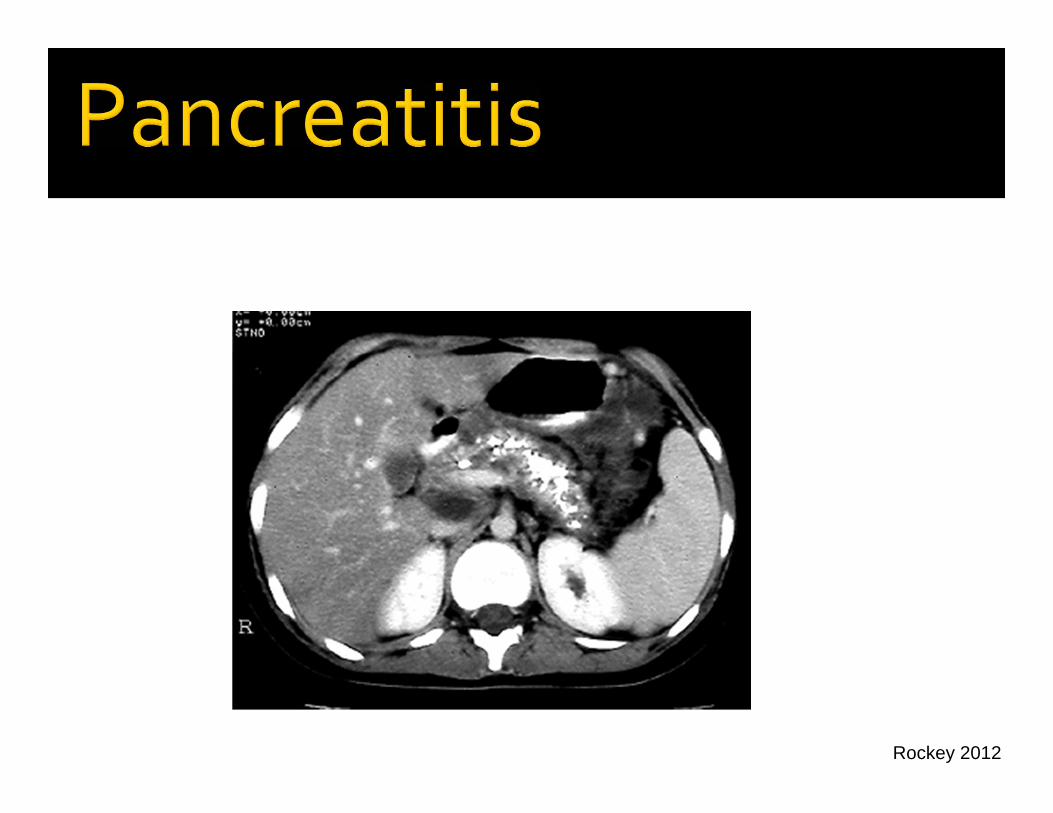
71y/o man admitted for GI bleeding Past history of heavy beer consumption, also a history of pancreatitis, presumed ETOH No past hx of liver diseaseNo medications On admission, NAD, BP 120/72, HR 98, melena

Rockey 2012
Laboratory data – Hgb 9.1, plts 135, AST 48, ALT 33, T bili 1.1, Alk phos 155, PT‐INR 1.0, BUN 33, Cr 1.2
EGD – negative, no ulcer disease, no portal hypertension
RUQ doppler ultrasound revealed normal appearing liver, normal ducts
Rockey 2012
Received 2 units of PRBCsWas about to be discharged, developed another episode of melena, HR 110 Repeat endoscopyNo EVs, normal stomach, normal duodenum, blood in the second portion of the duodenum
Rockey 2012
Which of the following is most likely to yield the correct diagnosis?
(A) Endoscopic ultrasound(B) Doppler ultrasound(C) MRI of the abdomen(D) Angiography(E) Enteroscopy
Rockey 2012
Rockey 2012
Rockey 2012
History of pancreatitis is key Ill defined bleeding sourceMust move rapidly and definitively to make a diagnosis
Take Home Points

Rockey 2012
Which of the following is most likely to yield the correct diagnosis?
(A) Endoscopic ultrasound(B) Doppler ultrasound(C) MRI of the abdomen(D) Angiography(E) Enteroscopy
Rockey 2012
A 67‐year‐old man with chronic atrial fibrillation comes to the emergency department because of severe periumbilical pain and nausea that started suddenly two hours ago. He describes the pain as “severe.”
On physical examination the patient appears acutely ill. He is unable to find a comfortable position. Temperature is 37.2 C (99.0 F). Pulse rate is 110 per minute; rhythm is irregular. Blood pressure is 150/90 mmHg. The abdomen is soft, flat, and nontender to palpation. Bowel sounds are active. No enlarged organs or masses are noted.
Rockey 2012
Laboratory studies:
Hemoglobin 14.0 g/dLLeukocyte count 12,000/cu mmSerum electrolytes NormalSerum amylase 120 U/LSerum bilirubin (total) 1.0 mg/dLSerum alkaline phosphatase 130 U/L
Upright and supine plain films of the abdomen show a nonspecific bowel gas pattern.
Rockey 2012
Which of the following diagnostic studies should you recommend now?
(A) Laparotomy(B) Upper endoscopy(C) Computed tomography of the abdomen(D) Doppler ultrasound examination of the abdomen(E) Mesenteric angiography
Rockey 2012
Acute Mesenteric Ischemia• A high index of suspicion in the setting of a compatible history and physical examination serves as the cornerstone to Dx
• Immediate diagnostic evaluation• Patients older than 60 history of atrial fibrillation recent myocardial infarction congestive heart failure arterial emboli postprandial abdominal pain and weight loss *Abdominal pain that is out of proportion to physical examination
Rockey 2012
• Laboratory data: Hemoconcentration, leukocytosis, and metabolic acidosis, with
high anion gap and lactate concentrations. High levels of serum amylase, aspartate aminotransferase,
lactate dehydrogenase• High levels of serum amylase, aspartate aminotransferase, lactate
dehydrogenase• Diagnosis:
• MR or CR angio evolving; test of choice angiography• Therapy:
• difficult, related to revascularization• Prognosis:
• Guarded
Acute Mesenteric Ischemia
Rockey 2012
Which of the following diagnostic studies should you recommend now?
(A) Laparotomy(B) Upper endoscopy(C) Computed tomography of the abdomen(D) Doppler ultrasound examination of the abdomen(E) Mesenteric angiography
Rockey 2012
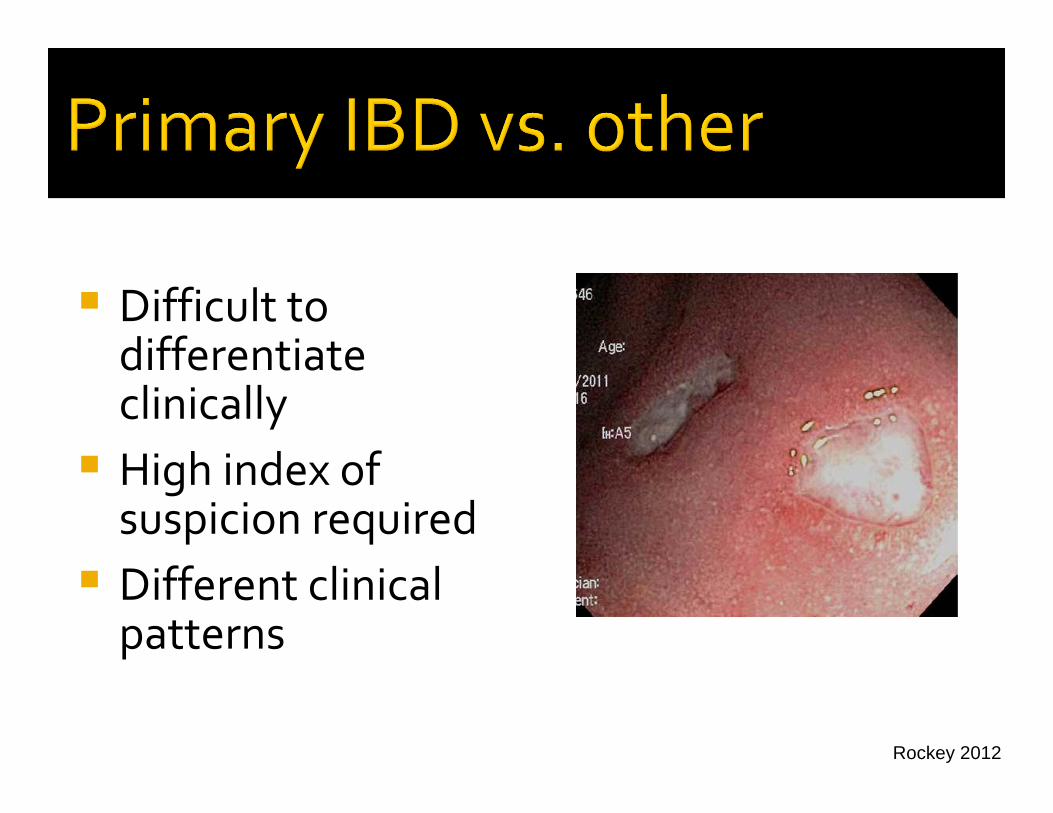
41 yo female with a past history of UC Treated intermittently with mesalamine and prednisone 1 week of progressively more frequent diarrhea, occasional blood stools, up to 8 per day + some abd pain, tenesmus, no FWas begun on a course of prednisone by her primary GI (now on 20 mg/day), perhaps a little better
Rockey 2012
On exam, slightly uncomfortable, AF. Abd soft, but diffusely tender
Laboratory data – Hgb 10.4, MCV 81, WBC 9.8
C diff toxin negative
Rockey 2012
Which of the following diagnostic studies should you recommend now?
(A) Repeat C dificile toxin assay(B) Upper endoscopy(C) Computed tomography of the abdomen(D) Colonoscopy(E) MRI of the abdomen
Rockey 2012
Difficult to differentiate clinically High index of suspicion required Different clinical patterns
Rockey 2012
Which of the following diagnostic studies should you recommend now?
(A) Repeat C dificile toxin assay(B) Upper endoscopy(C) Computed tomography of the abdomen(D) Colonoscopy(E) MRI of the abdomen
Rockey 2012
38 yo housewife with a history of HTN, presents with nausea, dark urine, and slight eye discoloration 2 weeks PTA.
Drinking wine with dinner (no more than one or two per evening). Sexually active.
Taking ES Excedrin, ibuprofen, spironolactone, and nitrofurantoin. Also, taking herbal supplements for weight loss about 1 month previously for about 3 weeks, stopped after began to get tired.
On examination, slightly obese (BMI 31), jaundiced, and tired appearing. Liver span was 14 cm, and slightly tender, without mass. No ascites.
Rockey 2012
Laboratory studies:Serum bilirubin (total) 13.5 mg/dLSerum alkaline phosphatase 350U/LSerum aminotransferases:AST 2,556U/LALT 1,592U/LSerum albumin 3.2 g/dLINR 1.9
RUQ doppler ultrasound – normal ducts, normal flow
Rockey 2012
Which of the following is the most likely cause of the abnormalities in liver function?
(A) Autoimmune hepatitis(B) Acute viral hepatitis A(C) Acute viral hepatitis B(D) Drug induced liver injury(E) Acute fatty liver disease of pregnancy
Rockey 2012
Laboratory studies:
Acetaminophen 9HAV IgM NegativeHCV Ab Negative HBV sAg NegativeANA 1:20AMA 1:20
Rockey 2012
Which of the following is the most likely cause of the abnormalities in liver function?
(A) Autoimmune hepatitis(B) Acute viral hepatitis A(C) Acute viral hepatitis B(D) Drug induced liver injury(E) Acute fatty liver disease of pregnancy
Rockey 2012
Which of the following medications is the most likely cause of the abnormalities in liver function?
(A) Spironolactone(B) Acetaminophen(C) Herbal medication(s)(D) Ibuprofen(E) Nitrofurantoin

Rockey 2012
Liver biopsy

Rockey 2012
• Any drug can cause DILI• Assessment of causality is extremely difficult; usually a diagnosis of exclusion
• The most critical component is typically timing: most episodes of DILI happen within 5‐90 days of exposure.
• DILI caused by certain drugs is often associated with a classic signature (hepatocellular, cholestatic, immunoallergic patterns)
• The most classic drugs associated with DILI are augmentin, dilantin, valproic acid, and isoniazid
(This case is tricky because nitrofurantoin causes DILI)
Rockey 2012
Liver tests rapidly declined
Herbalife® Hepatotoxicity
Rockey 2012
Which of the following medications is the most likely cause of the abnormalities in liver function?
(A) Spironolactone(B) Acetaminophen(C) Herbal medication(s)(D) Ibuprofen(E) Nitrofurantoin
Rockey 2012
AcetaminophenDILIViral hepatitisShock liver (ischemic hepatitis)Passed gallstone (choledocholithiasis)

Rockey 2012
48 y/o male with history of ETOH pancreatitis Progressive abdominal pain last 2 weeks Active drinking vodka until 2 d PTAOn exam, T 99.6, HR 92, Bp 110/67, + shifting dullness, with diffuse tenderness
Rockey 2012
Laboratory data – amylase 459, AST 85, ALT 22, T bili 2.1, Alk phos 121, PT‐INR 1.4, Alb 3.1, Cr 1.4
Rockey 2012
Which of the following is most likely to yield the correct diagnosis?
(A) Esophagogastroduodenoscopy(B) Doppler ultrasound of the abdomen(C) MRI of the abdomen(D) Paracentesis(E) Angiography
Rockey 2012
Paracentesis –WBC 1,345, 22% PMNs, Alb 2.1, SAAG (1.0); gram stain – no organisms
CT – pancreatic calcification, ascites, no liver lesions, splenomegaly
Differential diagnosis, next test?
Rockey 2012
Paracentesis –WBC 1,345, 22% PMNs, Alb 2.1, SAAG (1.0); gram stain – no organisms
CT – pancreatic calcification, ascites, no liver lesions, splenomegaly
Differential diagnosis, next test?
Ascitic fluid amylase 12,053
Rockey 2012
Which of the following is most likely to yield the correct diagnosis?
(A) Esophagogastroduodenoscopy(B) Doppler ultrasound of the abdomen(C) MRI of the abdomen(D) Paracentesis(E) Angiography
Rockey 2012
Setting of chronic pancreatitis Pancreatic ductal disruptionAscites fluid – inflammatory (amylase) Very difficult to differentiate from SBPTreatment is ERCP with PD stenting, or drainage of pseudocyst if present, or surgical correction of the defect
Rockey 2012
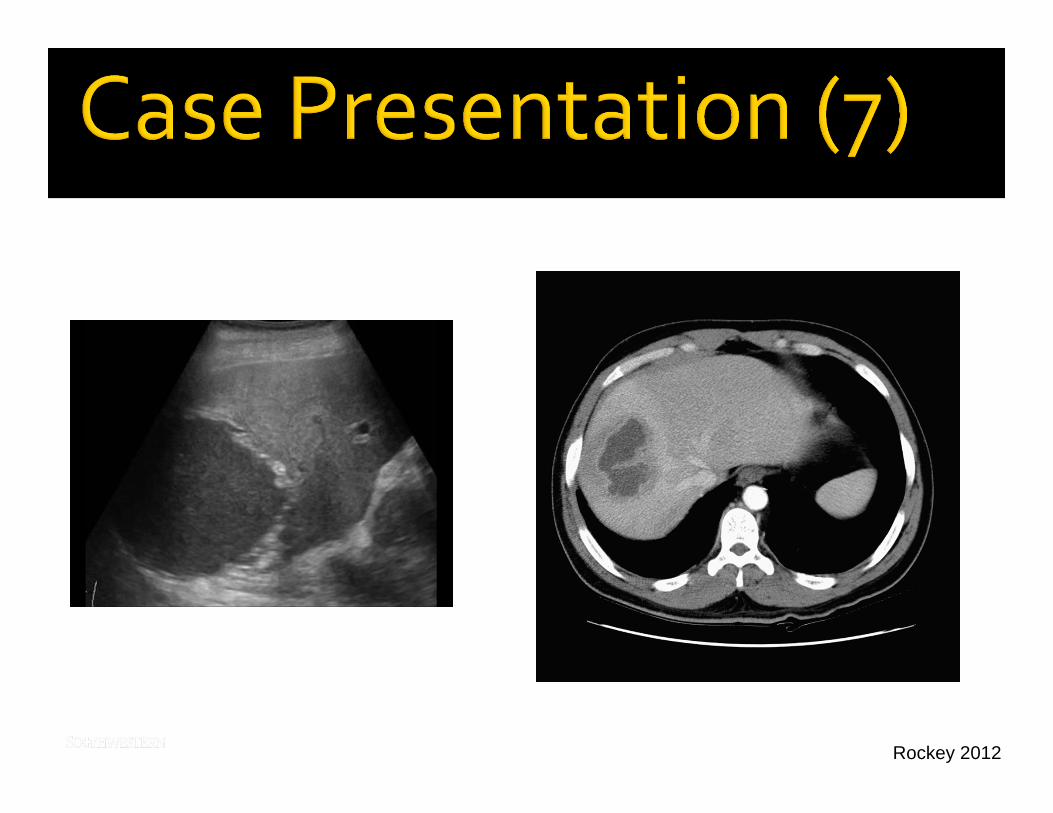
35 y/o male history of mid‐epigastric and right upper quadrant pain for the last month 10 pound weight loss and some SOB No past hx of liver disease and no medications On exam, confortable, VS normal, Temp 99.4. Abd soft, slight mid‐epi tenderness; stool G +
Rockey 2012
Laboratory studies:
Hemoglobin 11.9 g/dLLeukocyte count 14,200/cu mm;
(differential: 34% segs, 8% band forms, 40% lymphs,
4% eos, 16% monos)Serum aminotransferases:
AST 18 U/LALT 14 U/L
Serum alkaline phosphatase 216 U/LSerum bilirubin:
Total 1.3 mg/dLDirect 0.4 mg/dL
Serum albumin 3.2 g/dLINR 1.2
Rockey 2012
Rockey 2012
Blood culture specimens obtained during a febrile period show no growth.
Which of the following should you do now?
(A) Order serologic test for Echinococcus granulosus; begin mebendazole(B) Order serologic test for Entamoeba histolytica; begin metronidazole(C) Begin intravenous piperacillin/sulbactam and
gentamicin(D) Arrange for laparotomy
Rockey 2012
• Two varieties
• Different epidemiology
• Pyogenic ‐‐ elderly male, risk factors
• Amebic ‐‐ young male, risk factors
• Etiology of PLA has shifted dramatically; historically pylephlebitis, has shifted now to either biliary in etiology or cryptogenic
Liver Abscess
Rockey 2012
• Often is a subacute illness.
• The most common symptoms are RUQ pain and fever,but these are present together in only ≈ 40% of cases.
• Right sided lung findings are common.
• Laboratory tests are abnormal, but often nonspecific,except in the case of associated biliary tract disease inwhich case the bili and alk phos are elevated.Abnormalities in these tests should direct one to thebiliary tract and an early ERCP, particularly if cholangitisis in the differential diagnosis.
Liver Abscess

Rockey 2012
• Distinguishing pyogenic liver abscesses from amebicliver abscesses may be very difficult on clinical groundsas the presentation is very similar.
• The best clinical clue to differentiate between PLA andALA is the epidemiologic setting. A history of diarrheais usually not helpful, but recent travel to endemic areasof amebiasis is often present in patients withALA.
• Amebic antibodies are very sensitive in the setting ofALA.
• Lesion aspiration may also be very helpful.
Liver Abscess
Rockey 2012
•The patient had traveled to MexicoCity to visit his relatives 3 months PTA.
Liver Abscess

Rockey 2012
Blood culture specimens obtained during a febrile period show no growth.
Which of the following should you do now?
(A) Order serologic test for Echinococcus granulosus; begin mebendazole(B) Order serologic test for Entamoeba histolytica; begin metronidazole(C) Begin intravenous piperacillin/sulbactam and
gentamicin(D) Arrange for laparotomy
Rockey 2012
67 y/o man admitted for jaundice; first noted yellow eyes 8 weeks previouslyDrank beer daily (2 six packs), but stopped when noticed jaundice Family noted that he was confused and jaundicedNo past hx of liver diseaseNo medications
Rockey 2012
PE ‐ Jaundice, NAD, 122/72 HR 76, RR 10, AF, shifting dullness, liver 16 cm in span, no splenomegaly Laboratory data ‐AST 98, ALT 43, T bili 8.1, Alk phos 1,790, PT‐INR 1.0, Cr 1.7, UA + proteinAscites tapped – straw colored, SAAG 1.4 RUQ doppler ultrasound revealed normal ducts, hepatomegaly
Rockey 2012
Developed progressive renal failure, thought to be secondary to hepatorenal syndrome due to alcoholic liver disease. Died 12 days after admission.Differential diagnosis?
Rockey 2012
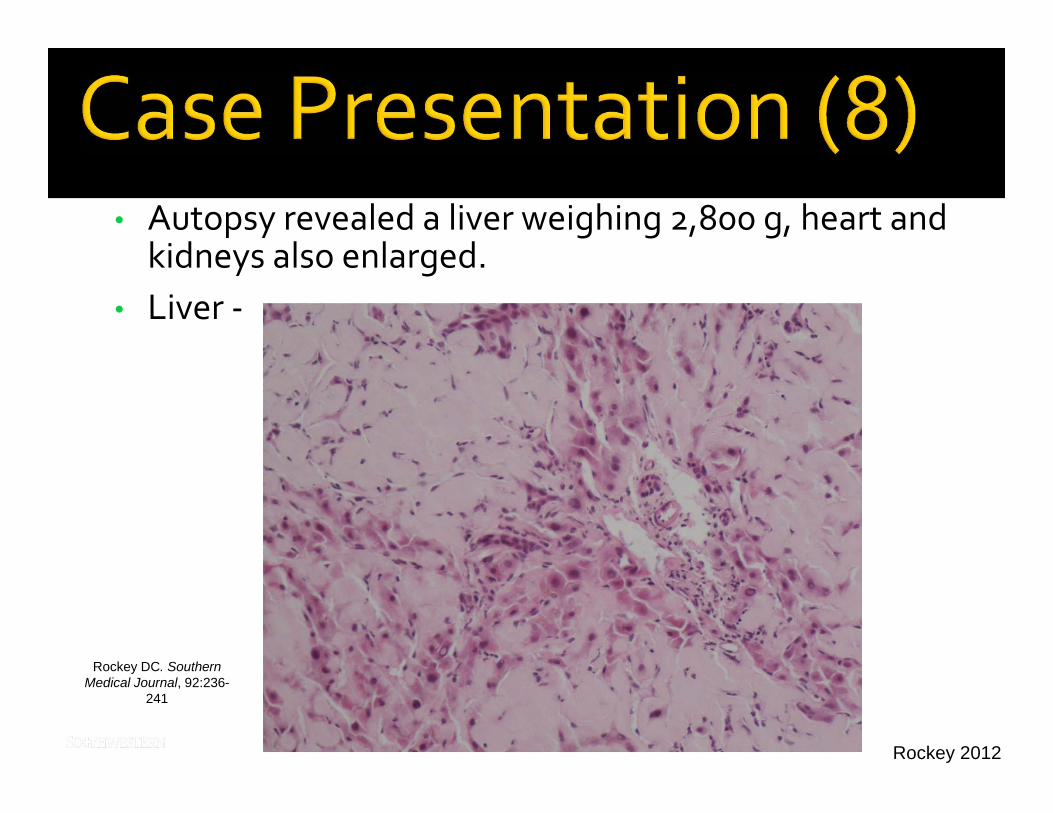
• Autopsy revealed a liver weighing 2,800 g, heart and kidneys also enlarged.
• Liver ‐
Rockey DC. SouthernMedical Journal, 92:236-
241

Rockey 2012
Urine protein – 2,800 mg/24 hours + light chains
Not all ascites is due to primary liver disease, even with a portal hypertensive SAAG Clue here was unusual liver tests and renal disease, atypical (protein)
Take Home Points
Rockey 2012
MalignancyTuberculosisGranulomasAmyloidMicroabscesses
Rockey 2012
A 74‐year‐old man is admitted to the hospital because of painless massive hematochezia. Eighteen months ago, a similar episode required hospitalization and transfusion of three units of packed red blood cells. At that time, colonoscopy documented pancolonic diverticulosis.
Medical history is otherwise unremarkable. On physical examination the patient is in no distress. Blood pressure and pulse rate show orthostatic changes. The abdomen is nontender. Rectal examination discloses maroon‐colored stool. Hemoglobin is 8.2 g/dL, and hematocrit is 24%.

Rockey 2012
The patient is given two units of packed red blood cells. There is no blood on nasogastric lavage. Colonoscopy documents diverticula; fine details are not well visualized because of old blood and blood clots. No other colonoscopic abnormalities are seen.
Seven more units of packed red blood cells are transfused because of persistent bleeding. Nasogastric aspirate is negative for blood. Radiolabeled red blood cell scan is negative, and abdominal angiography reveals no obvious site of active bleeding. Upper endoscopy is normal.
Three additional transfusions are required because of subsequent intermittent bleeding.
Rockey 2012
Which of the following is the most appropriate next step?
(A) Observation and continued blood transfusions(B) Repeat abdominal angiography(C) Right hemicolectomy(D) Subtotal colectomy and ileoproctostomy

Rockey 2012
Diverticula common in elderly patients
Disease of western society
Bleeding
occurs only in a small # of those with ticsmay be the first manifestation of disease is NOT associated with diverticulitis
Rockey 2012
Bleeding is brisk and painless
20% continue, 20% stop & rebleed, 60% never bleed again
Colonoscopy cannot localize
Radionuclide scanning/angio may localize
Therapy may be difficult
Rockey 2012
A 25‐year‐old white woman is admitted to you because she has weight loss, diarrhea and iron deficiency anemia. Her INR is 1.4.
Her referring physician considered a diagnosis of celiac sprue; however, an assay for anti‐endomysial antibodies was negative.
Upper endoscopy shows notched duodenal folds. Biopsy specimens reveal total villous atrophy – suggestive of celiac sprue.
Rockey 2012
The negative antibody assay results are most consistent with which of the following diagnoses?
(A) IgA deficiency(B) IgG deficiency(C) Concomitant vasculitis(D) Dermatitis herpetiformis(E) T‐cell lymphoma
Rockey 2012
Very commonProtean manifestationsDiarrhea, bloating, painMalabsorptionComplications – malignancy Therapy typically effective
Rockey 2012
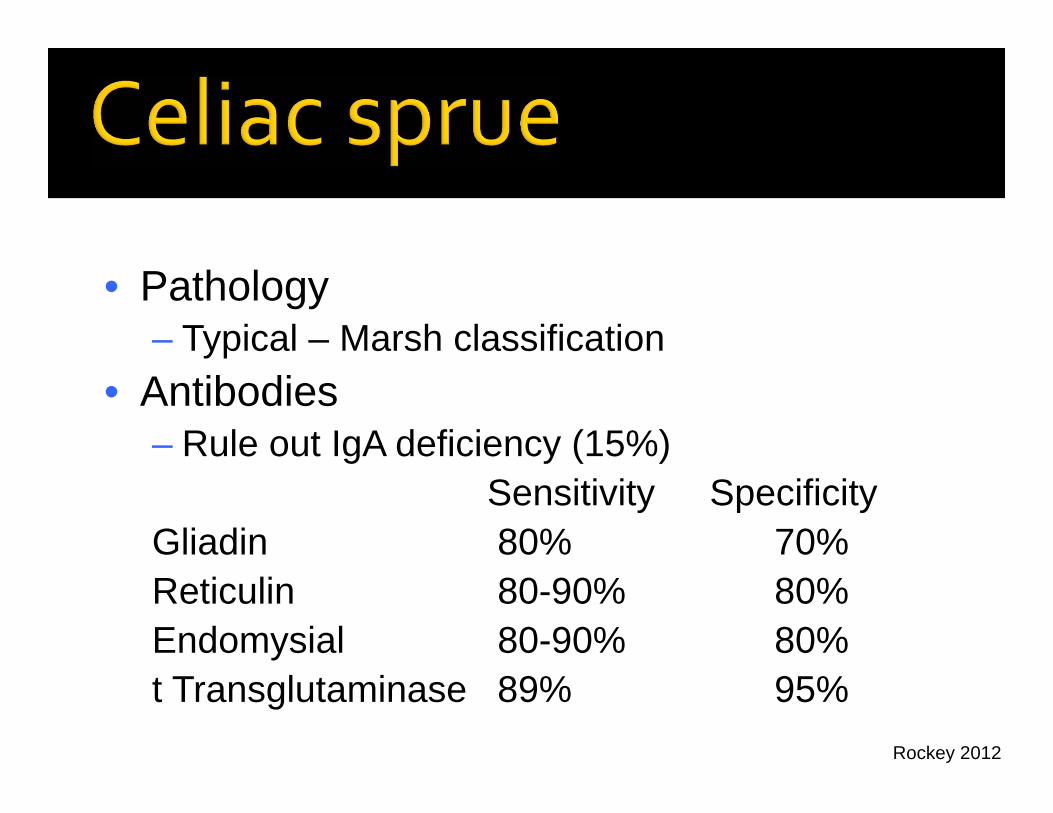
• Pathology– Typical – Marsh classification
• Antibodies– Rule out IgA deficiency (15%)
Sensitivity SpecificityGliadin 80% 70%Reticulin 80-90% 80%Endomysial 80-90% 80%t Transglutaminase 89% 95%
Rockey 2012
The negative antibody assay results are most consistent with which of the following diagnoses?
(A) IgA deficiency(B) IgG deficiency(C) Concomitant vasculitis(D) Dermatitis herpetiformis(E) T‐cell lymphoma
Rockey 2012
You are asked to evaluate a 45‐year‐old man, who has just been hospitalized because of new‐onset ascites, hematemesis, and melena. He has a history of chronic alcoholism but has not consumed alcoholic beverages for one year.
Physical examination reveals scleral icterus, proximal muscle wasting, multiple spider angiomas, and marked abdominal distention due to ascites. The patient is lucid with no evidence of asterixis.
Rockey 2012
Laboratory studies:
Hematocrit 23%Leukocyte count 4500/cu mmPlatelet count 72,000/cu mmSerum aminotransferases:AST 187 U/LALT 90 U/L
Serum alkaline phosphatase 154 U/L
Rockey 2012
Laboratory studies: (continued)
Serum bilirubin (total) 4.5 mg/dLSerum albumin 2.7 g/dLSerum ceruloplasmin NormalSerum ferritin NormalSerum iron NormalSerum total iron‐binding capacity NormalHBsAg NegativeAnti‐HCV (ELISA) Positive
Rockey 2012
The patient is given six units of packed red blood cells. Emergency upper endoscopy documents grade 3 esophageal varices, which are treated with band ligation. His condition stabilizes, and you recommend sodium restriction, diuretic therapy, and octreotide infusion.
Two days later, another episode of massive hematemesis occurs. Balloon tamponade is required after repeat band ligation fails to stop the bleeding.
Rockey 2012
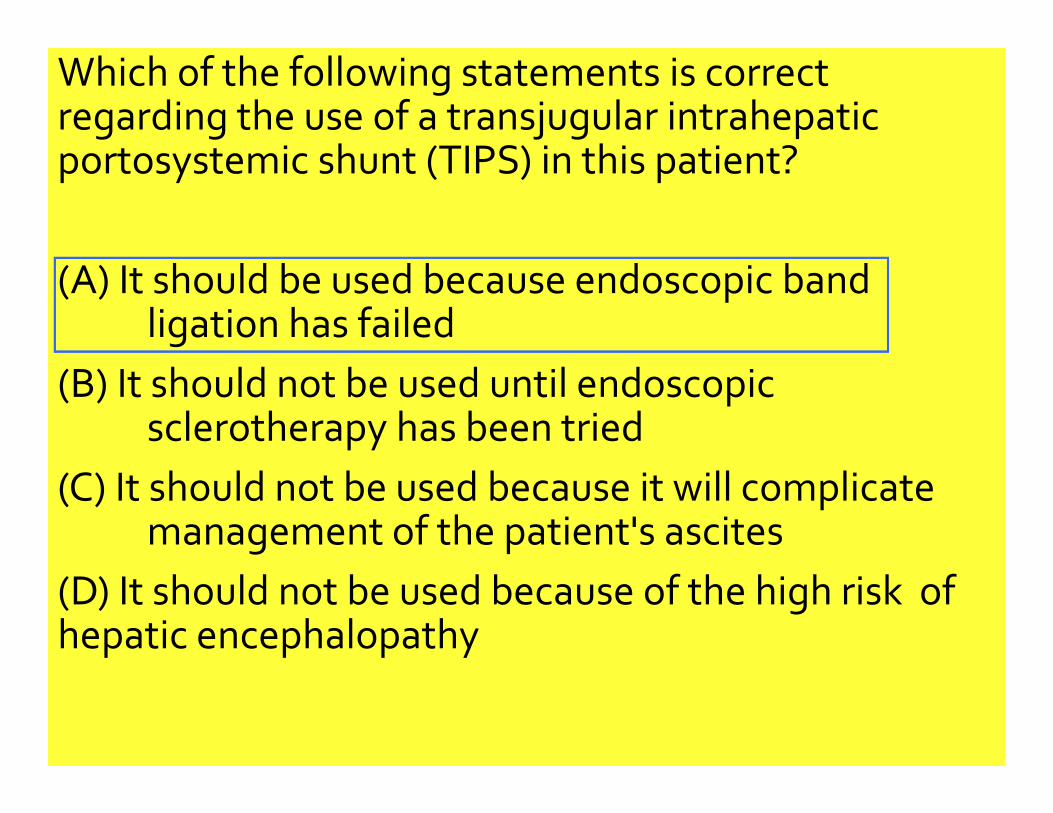
Which of the following statements is correct regarding the use of a transjugular intrahepatic portosystemic shunt (TIPS) in this patient?
(A) It should be used because endoscopic band ligation has failed
(B) It should not be used until endoscopic sclerotherapy has been tried
(C) It should not be used because it will complicate management of the patient's ascites
(D) It should not be used because of the high risk of hepatic encephalopathy
Rockey 2012
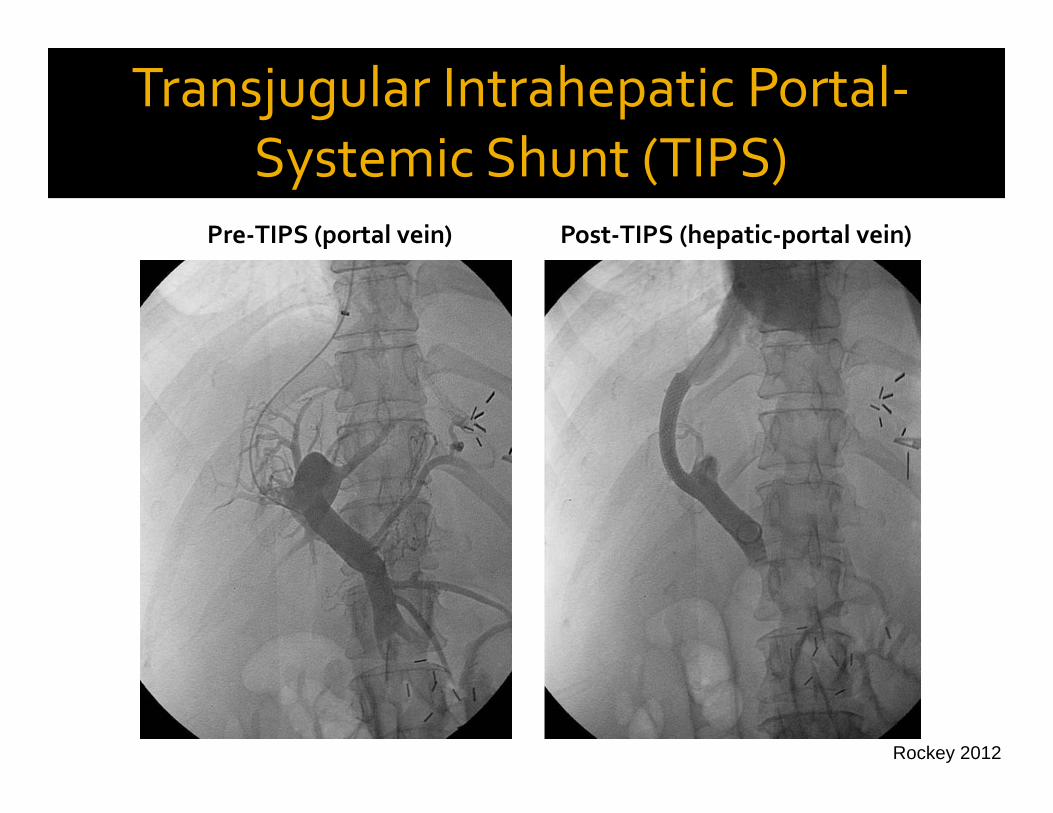
Pre‐TIPS (portal vein) Post‐TIPS (hepatic‐portal vein)
Transjugular Intrahepatic Portal‐Systemic Shunt (TIPS)
Rockey 2012
• Portal vein occlusion• Polycystic liver disease• Liver abscess• Cholangitis• Anomalous vena caval anatomy• Severe hepatic encephalopathy• Severe hepatic dysfunction• ? Renal insufficiency• Cardiac insufficiency
Contraindications
Transjugular Intrahepatic Portal‐Systemic Shunt (TIPS)
Rockey 2012
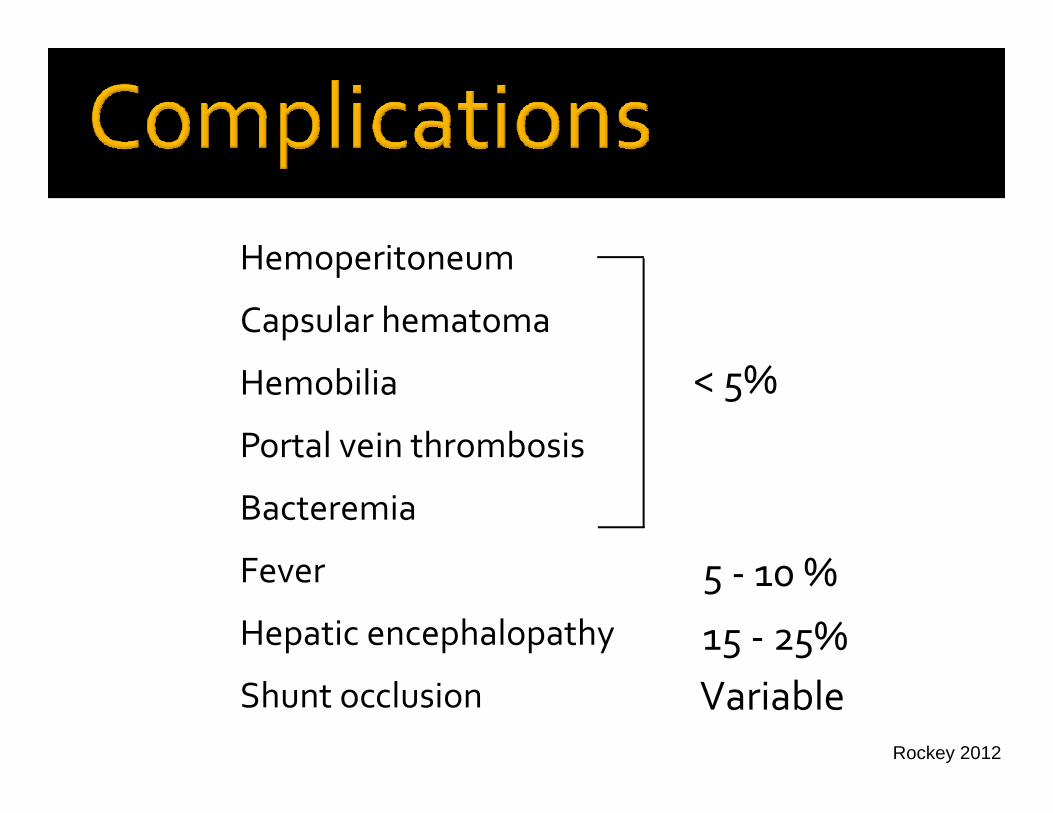
Hemoperitoneum
Capsular hematoma
Hemobilia
Portal vein thrombosis
Bacteremia
Fever
Hepatic encephalopathy
Shunt occlusion
< 5%
5 ‐ 10 %
15 ‐ 25%Variable
Rockey 2012
Which of the following statements is correct regarding the use of a transjugular intrahepatic portosystemic shunt (TIPS) in this patient?
(A) It should be used because endoscopic band ligation has failed
(B) It should not be used until endoscopic sclerotherapy has been tried
(C) It should not be used because it will complicate management of the patient's ascites
(D) It should not be used because of the high risk of hepatic encephalopathy
Rockey 2012
Rockey 2012
Rockey 2012
A 52 y.o. man with HCV is referred for evaluation after he is found to have HCV by his PCP
Abnormal liver tests for several years
Genotype 1a, viral load 1.1 x 106 (IU/mL)
He claims he is tired, but has no other symptoms
PMH – unremarkable, no other disease, denies risk factors for transmission
Rockey 2012
PE: VS normal, normal liver size
Lab data: AST 51, ALT 59, Alb 4.1, PT INR 1.0
Hgb 14.1, plts 139,000
What do you recommend?

Rockey 2012
Can’t APRI Fibrotest Fibrosure Ultrasound MR‐Elastography Other
How do you stage his disease non‐invasively?
Rockey 2012
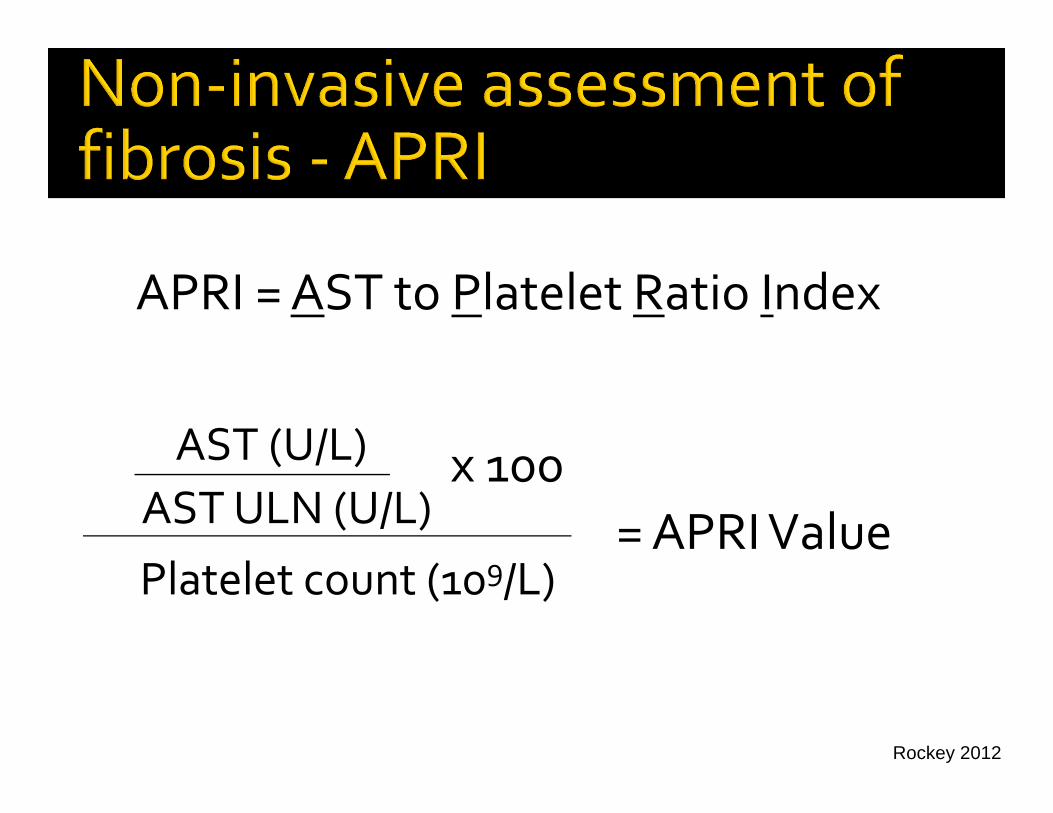
AST (U/L)AST ULN (U/L)Platelet count (109/L)
= APRI Valuex 100
APRI = AST to Platelet Ratio Index
Rockey 2012
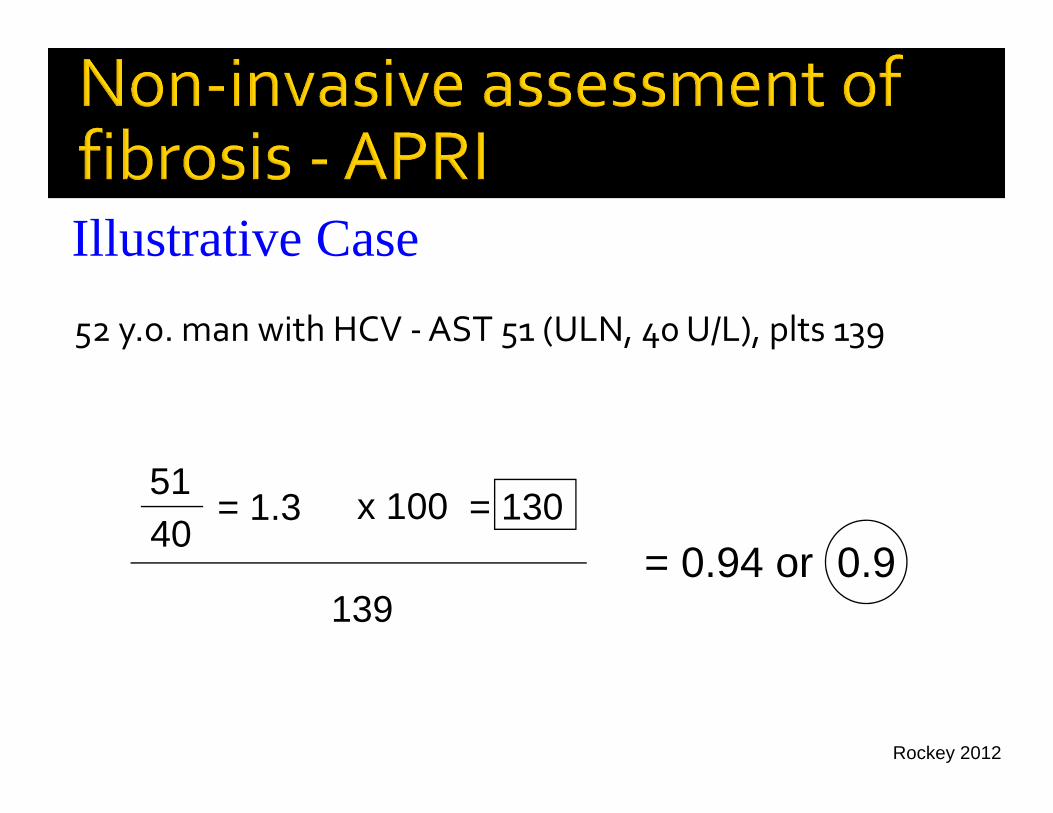
Illustrative Case
5140
= 130
139= 0.94 or 0.9
x 100= 1.3
52 y.o. man with HCV ‐AST 51 (ULN, 40 U/L), plts 139
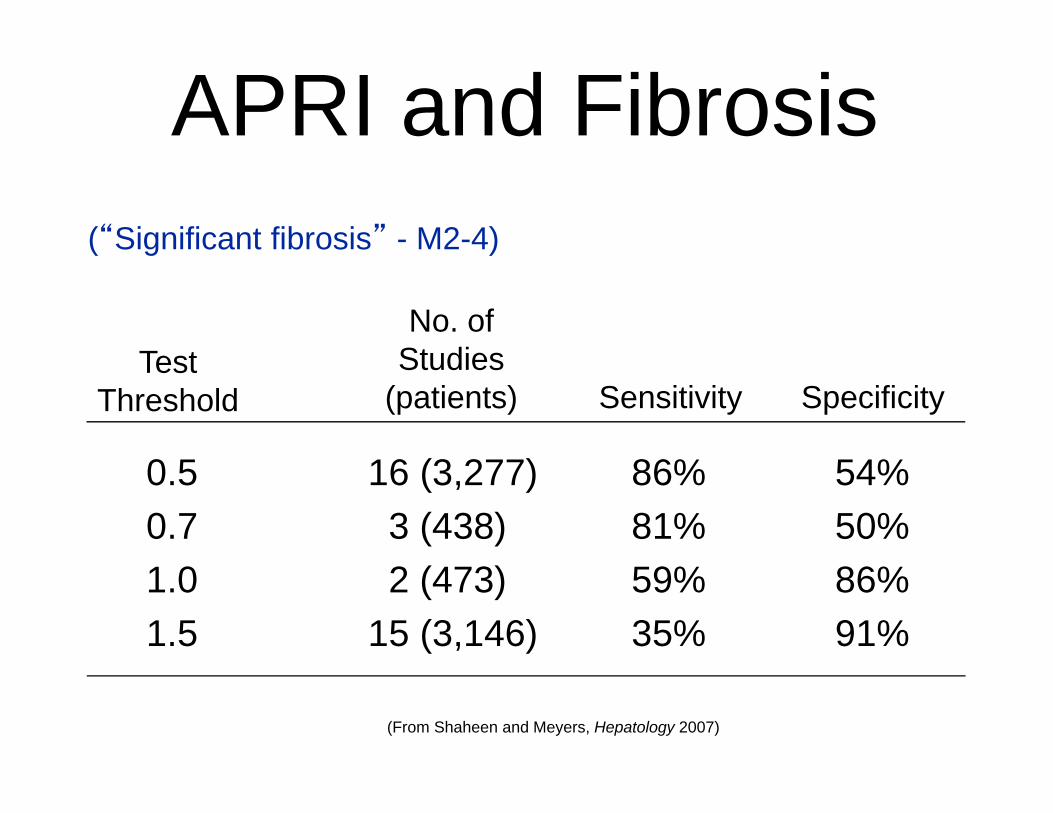
0.5 16 (3,277) 86% 54%0.7 3 (438) 81% 50%1.0 2 (473) 59% 86%1.5 15 (3,146) 35% 91%
APRI and Fibrosis
Test Threshold
(“Significant fibrosis” - M2-4)
Sensitivity Specificity
No. of Studies
(patients)
(From Shaheen and Meyers, Hepatology 2007)
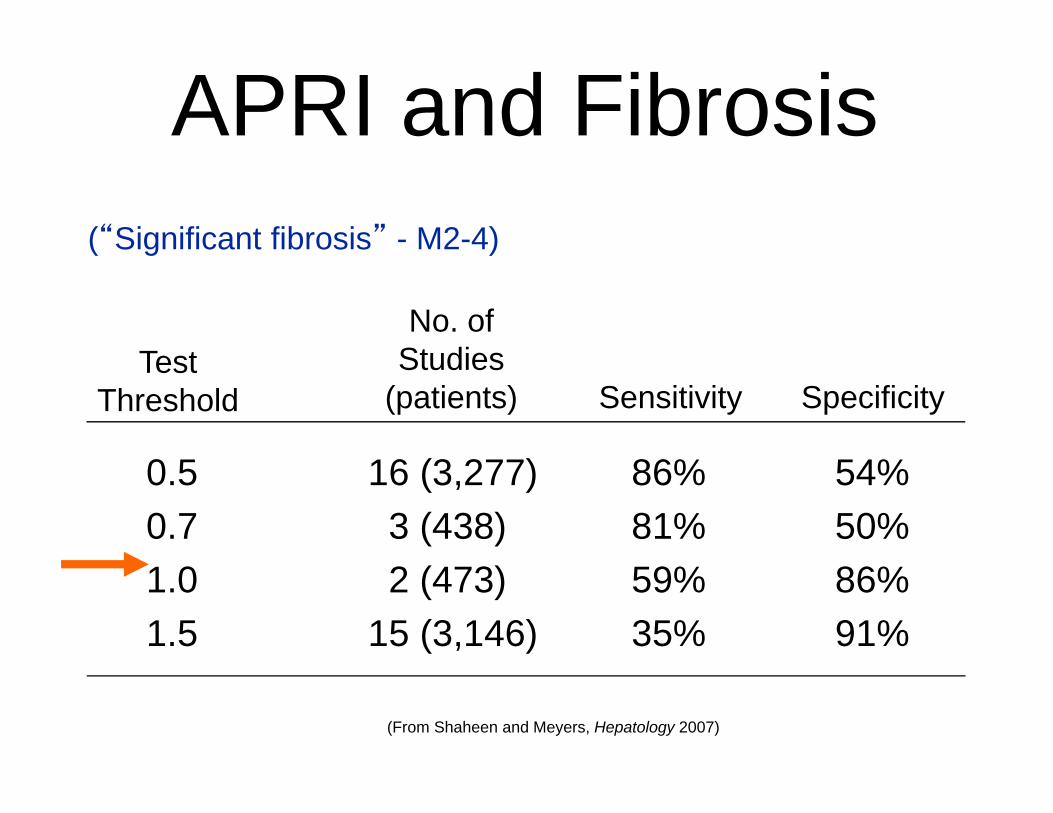
0.5 16 (3,277) 86% 54%0.7 3 (438) 81% 50%1.0 2 (473) 59% 86%1.5 15 (3,146) 35% 91%
APRI and Fibrosis
Test Threshold
(“Significant fibrosis” - M2-4)
Sensitivity Specificity
No. of Studies
(patients)
(From Shaheen and Meyers, Hepatology 2007)
Rockey 2012
Liver biopsy ‐Grade 2 inflammation, Stage 1‐2 fibrosis
Rockey 2012

Rockey 2012
Rockey 2012
Rockey 2012
New case
Rockey 2012
New case