gastrointestinal stromal tumours (gist) et al. ann surg oncol. 2007;14:134 -142. gist diagnosis...
TRANSCRIPT

What’s new in gastrointestinal stromal tumours (GIST) in the past
12 months
Professor John R Zalcberg
Alfred Health,Faculty of Medicine
Monash University, MelbourneAUSTRALIA

Disclosures
• Novartis• Pfizer• Bayer• BMS• MSD
• No stock ownership relevant to this topic
Research support/Travel Support/Advisory Board compensation relevant to this topic
;

Overview
• Treatment of advanced disease
• Adjuvant therapy

What’s new in gastrointestinal stromal tumours (GIST) in the past
12 months
but
… to know where you’re going, you need to know where you’ve come
from…. James Baldwin

GIST
Mesenchymal neoplasms: now recognized as a biologically and clinically distinct entity
Shared ancestry with Interstitial Cells of Cajal (coordinate peristalsis)
Clinical presentation is variable
Diagnosis is still challenging in some cases/based on c-kit expression
Nilsson et al. Cancer. 2005;103:821-829.Gold et al. Ann Surg Oncol. 2007;14:134-142.

GIST Diagnosis -Immunohistochemistry
KIT protein (CD117): positive in 95% of cases
DOG1: positive in >95% of KIT-positive GIST and 35% of KIT-negative GIST
Courtesy of J. Fletcher. Presented at: Global Interdisciplinary Specialists Training Around the World (GISTour) 2009. 22 November 2009, Taipei, Taiwan.* Parkkila S et al. Mod Pathol. 2010 Jan 15. [Epub ahead of print]
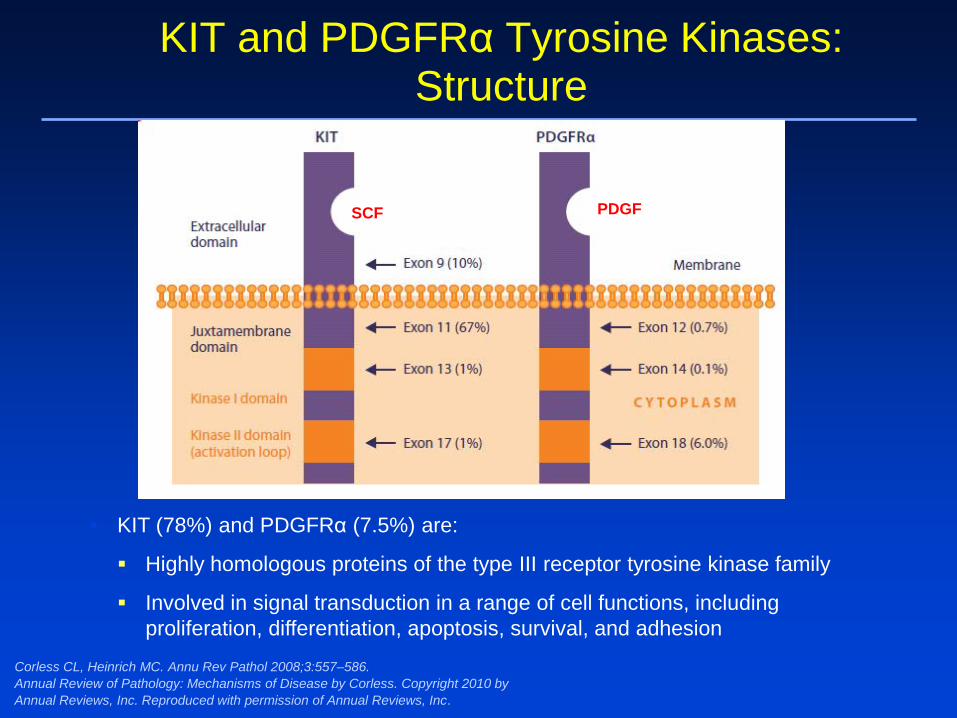
KIT and PDGFRα Tyrosine Kinases: Structure
KIT (78%) and PDGFRα (7.5%) are:
Highly homologous proteins of the type III receptor tyrosine kinase family
Involved in signal transduction in a range of cell functions, including proliferation, differentiation, apoptosis, survival, and adhesion
Corless CL, Heinrich MC. Annu Rev Pathol 2008;3:557–586.Annual Review of Pathology: Mechanisms of Disease by Corless. Copyright 2010 by Annual Reviews, Inc. Reproduced with permission of Annual Reviews, Inc.
SCF PDGF

Wild-Type (WT) GIST (15%)(No KIT or PDGFRA Mutation)
Alteration Estimated Frequency References
BRAF mutation < 7% Agaram et al. Genes Chromosomes Cancer. 2008;47(10):853-859
KRAS mutation <1% Heinrich and Corless, unpublished
Increased IGF1R expression 50% Tarn et al. PNAS. 2008;105(24):8387-8392
Germline SDHA, SDHB, SDHC or SDHD mutation* ~12% Janeway et al. PNAS. 2011;108(1):314-318
Pantaleo et al. J Natl Cancer Inst. 2011;103(12):983-7
Loss of SDHB expression High Janeway et al. PNAS. 2011;108(1):314-318
Germline NF1 mutation Rare Andersson et al. Am J Surg Pathol. 2005; 29:1170-1176
*Carney-Stratakis syndrome: association of GIST and paraganglioma

WT-GIST (qWT for KIT, PDGFRA, RAS, SDH
Presentation by J Sicklick; UCSD
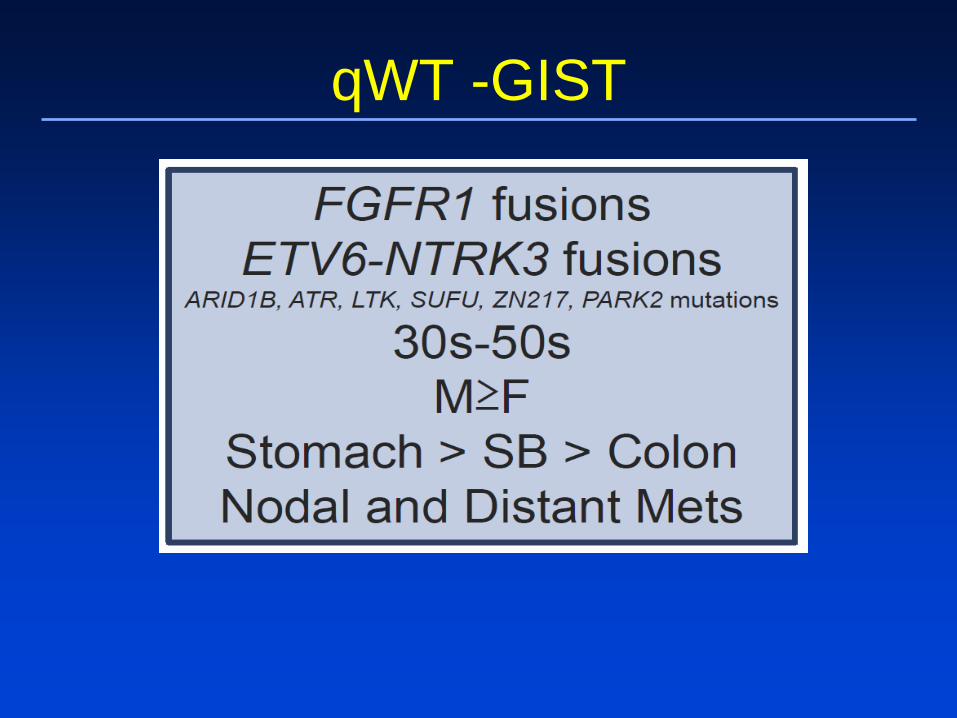
qWT -GIST

Location
GIST may occur anywhere along the GI tract or elsewhere in the abdomen or retroperitoneum:
– Oesophagus 2%
– Stomach 60%
– Small intestine 25%
– Colon / Rectum 5%
– Other (mesentery, retroperitoneum) 8%
Corless & Heinrich. Annu Rev Pathol Mech Dis. 2008;3:557-586.

Mutation Subtypes According to the Primary Location
Genotype Stomach (n=738)
Small bowel (n=261)
KIT mutationExon 9Exon 11Exon 13Exon 17
65.2%1.8%61.4%1.2%0.8%
79.7%23%54%2.3%0.4%
PDGFRA mutationExon 12Exon 14Exon 18
22.9%3.1%0.5%19.3%
1.2%0%0.4%0.8%
Wild type 11.9% 19.1%
Wardelmann et al. Pathologe 2010 epub ahead of print

Treatment of Advanced disease

MetaGIST; Analysis of High and Low Imatinib Doses: Design of Trials
Followfor PFS and OS
Imatinib(400
mg/day)
Imatinib(800
mg/day)
Progressivedisease
1. Verweij J, et al. Lancet 2004;364:1127–1134.2. Blanke CD, et al. J Clin Oncol 2008;26:626–632.
Metastatic or unresectable
GIST
EORTC/ISG/AGITG Study 620051
North American Intergroup Study S00332

Median OS (months) 49 / 49
3-year estimate (%) 60 / 61
Hazard ratio 1.00
P value (logrank test) 0.97
0 1 2 3 4 5 60
10
20
30
40
50
60
70
80
90
100
400 mg (818 patients)800 mg (822 patients)
Years
MetaGIST: Overall Survival
Van Glabbeke et al. ASCO 2007. Abstract 10004.

Median PFS (months) 6 / 19
3-year estimate (%) 5 / 17
P value (logrank test) 0.017
KIT exon 9 mutants: 400 mg / 800 mg
0 1 2 3 4 50
10
20
30
40
50
60
70
80
90
100
Years
KIT exon 9 mutants
MetaGIST: Progression Free Survival (KIT exon 9)
Van Glabbeke et al. ASCO 2007. Abstract 10004.

• 14% of GIST patients exhibit primary resistance:i.e. early tumor progression (within 6 months of beginning imatinib therapy)
• 50% of all GIST patients exhibit tumor progression within 2-5 years of starting imatinib therapy i.e.secondary resistance
Demetri et al. N Engl J Med. 2002;347:472-480.Verweij et al. Lancet. 2004;364:1127-1137.
Imatinib Resistance in GIST

• Primary imatinib resistance is more common in GISTs with the following genotypes
• KIT exon 9 mutations
• PDGFRA D842V mutations
• No detectable mutations (WT KIT/PDGFRAgenotype)
• Secondary imatinib resistance is commonly associated with the emergence of new kinase mutations
Antonescu et al. Clin Cancer Res. 2005;11:4182-4190.Heinrich et al. J Clin Oncol. 2003;21:4342-4349.Debiec-Rycher et al. Eur J Cancer. 2006;42:1093-1103.Heinrich et al. J Clin Oncol. 2006;29:4764-4774.
Mechanisms of Imatinib Resistance

Resistance to imatinib
Routine Practice
• Confirm progression (do not change a treatment that’s working)
• Check compliance• Test blood levels
(where appropriate)
• Surgery/ablation for localized or focal PD (continue TKI afterwards)
• Change TKI’s• Clinical trials of new agents
Change in TKI therapy
• Increase dose of imatinib• Replace imatinib with sunitinib• Replace sunitinib with
regorafenib• Other TKI’s
Management of Secondary Resistance

Change in TKI therapy
• Increase dose of imatinib• Replace imatinib with sunitinib• Replace sunitinib with
regorafenib• Other TKI’s
Management of Secondary Resistance

Dose Escalation of Imatinib in Case of Progression with 400 mg/day
133 patients crossover to 800 mg
response: 2% PR, 27% SDPFS: median 81 days
1Blanke et al. JCO, 20082Zalcberg et al. Eur J Cancer 41, 2005
EORTC 620052S00331
133 patients crossover to800 mg
response: 3% PR, 28% SDPFS: median 5 months
Progression free survival

Change in TKI therapy
• Increase dose of imatinib• Replace imatinib with sunitinib• Replace sunitinib with
regorafenib• Other TKI’s
Management of Secondary Resistance

(Sunitinib:placebo) Placebo (n=118)
Sunitinib (n=243)
50 mg/day, 4 weeks on, 2 weeks offImatinib-
refractory or -intolerant GISTpatients
Conducted at 56 sites in Europe, USA, Australia and Asia (Singapore).Final protocol dated August 2003
Randomization2:1
Placebo
4 weeks on, 2 weeks off
Cross over tosunitinib atprogression
Continue aslong as clinical benefit
Phase 3 trial of sunitinib in imatinib-resistant/-intolerant GIST
Sunitinib

Demetri et al. Lancet. 2006;3681329-1338.
Phase III Trial: Sunitinib in Advanced GIST After Imatinib Failure

17 / 214 16 / 187 22 / 142 19 / 86 7 / 47 5 / 23 2 / 522 / 96 9 / 84 10 / 66 7 / 37 2 / 25 3 / 6 0 / NA
Overall Survival with Crossover to Sunitinib
0 / 118Placebo0 / 243Sunitinib
No. events / no. at risk
Sunitinib (N=243)Placebo (N=118)Hazard ratio=0.7695% CI (0.54, 1.06)P=0.107
Current data
Time (weeks)
Ove
rall
surv
ival
pro
babi
lity
(%)
100
90
80
70
60
50
40
30
20
10
00 13 26 39 52 65 78 91 104
70% crossovers in placebo group
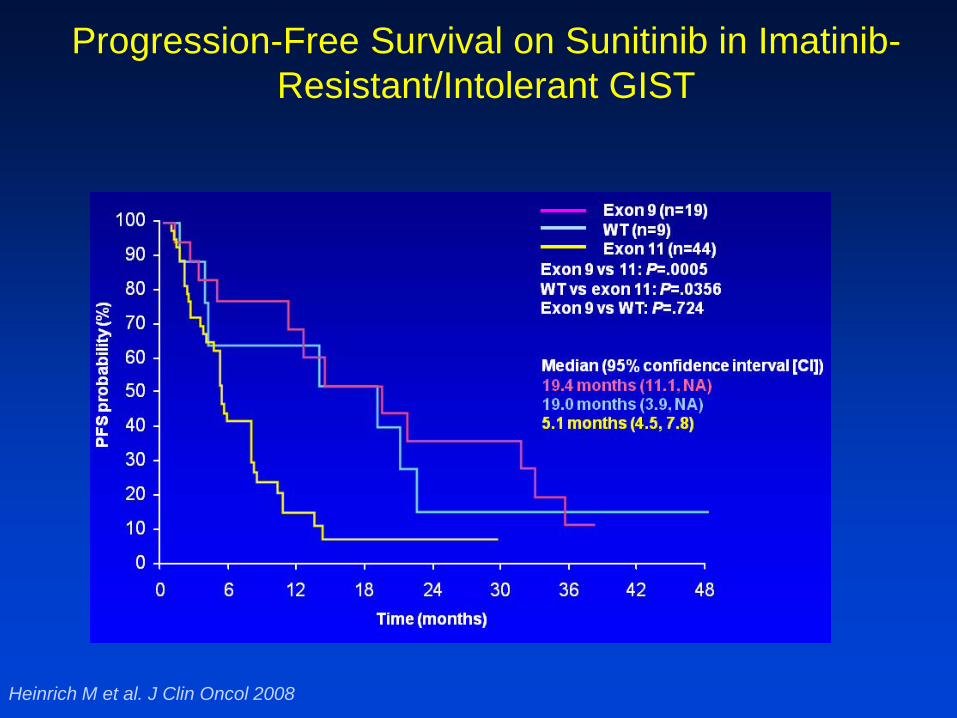
Heinrich M et al. J Clin Oncol 2008
Progression-Free Survival on Sunitinib in Imatinib-Resistant/Intolerant GIST

Change in TKI therapy
• Increase dose of imatinib• Replace imatinib with sunitinib• Replace sunitinib with
regorafenib• Other TKI’s
Management of Secondary Resistance

OF F
TREATMENT
Disease progression
blinded central review
GIST – Regorafenib In Progressive Disease (GRID): Study Design
– Global trial: – Stratification: treatment line (2 vs >2 prior lines),
geographical location (Asia vs “Rest of World”)– Primary endpoint = PFS
2 : 1
Regorafenib + best supportive
care (BSC)(n=133)
Placebo + BSC (n=66)
RANDOM I ZAT I ON
UnblindingCrossover offered for
placebo arm or continued regorafenib
for treatment arm
Regorafenib (unblinded)
until next progression
Metastatic/ unresectable
GIST pts progressing
despite at least prior imatinib and sunitinib
Demetri et al. ASCO 2012

GRID Study: PFS (primary endpoint per blinded central review)
Demetri et al. ASCO 2012

GRID Study: Overall Survival (following 85% cross-over of patients on placebo arm)
Demetri et al. ASCO 2012

ITT curves from Demetri GD et al. Lancet 2013; 381: 295–302
Days from randomization
1.00
0.75
0.50
0.25
00
PFS
pro
babi
lity
50 100 150 200 250 300
All patients (ITT population)Placebo (n=66) HR 0.27 (0.19–0.39)Regorafenib (n=133) p<0.0001
Secondary KIT mutation presentPlacebo (n=27) HR 0.22 (0.12–0.40)Regorafenib (n=50) p<0.001
Regorafenib shows benefit over placebo in patients with secondary KIT mutations

Change in TKI therapy
• Increase dose of imatinib• Replace imatinib with sunitinib• Replace sunitinib with
regorafenib• Other TKI’s
Management of Secondary Resistance
Other TKIs, when all 3 standard TKIs have failed for advanced GIST?
• Nilotinib• Masitinib • Vatalanib• Dasatinib• Dovitinib• Sorafenib• Pazopanib • Crenolanib • Ponatinib• BLU-285• DCC-2618
Clinical activity of BLU-285, a KIT/PDGFRα inhibitor in GIST
Management of Secondary Resistance
Abstract no: 2803523, CTOS 2017 Maui, Hawaii. Presented by Dr. Michael Heinrich

36
• High kinome selectivity*
• Binds active conformation
BLU-285
1. Evans EK et al. Sci Transl Med. 2017 Nov 1;9(414)*Kinome illustration reproduced courtesy of Cell Signaling Technology, Inc. (www.cellsignal.com)
BLU-285 IC50 Imatinib IC50
KIT Exon 11 deletion JM domain mutations
0.6 nM 12 nM
KIT Exon 11 V560G 1 nM 87 nM
KIT Exon 11/13 ATP binding site
mutations
11 nM 9160 nM
KIT Exon 11/14 28 nM 19650 nM
KIT Exon 17Activation
loop mutations
<2 nM 60–12750 nM
KIT Exon 17 D816V 0.27 nM 8150 nM
PDGFRα Exon 18 D842V 0.24 nM 759 nM
BLU-285: highly selective targeting and potent inhibition of mutant KIT and PDGFRα in GIST

37
Advanced GIST(n=46) MTD
Part 2 Dose expansion
PDGFRα D842V-mutant GIST (n=50)
Unresectable GIST after imatinib and ≥1 other TKI (n=50)
Part 1 Dose escalation
Key objectives
• Part 1: MTD, safety, pharmacokinetics, ctDNA analyses, anti-tumor activity
• Part 2: response rate, duration of response, safety
• 3+3 design with enrichment• MTD determined to be 400 mg PO QD• RP2D determined to be 300 mg PO QD
BLU-285 Phase 1 study

Tumor reduction across multiple KIT genotypes (central radiology review)
38
N=30 patients 300 mg (RP2D) – 400 mg (MTD)
-7020 of 30 (67%) patients with tumor shrinkage
50
-10
-20
-40
-50Max
imum
redu
ctio
n: s
um o
f dia
met
er
chan
ge fr
om b
asel
ine
(%)
-60
-30
0
10
20
30
40
PD
SD
PR
1317
1113
1113
1117
913
11 13 111317
10 111317
1113
1117
1117
9 1117
9 1317
917
111318
1117
1117
9 9 11 KIT mutation by exon ^
111417
11 91318
1117
917
1117
* * * **
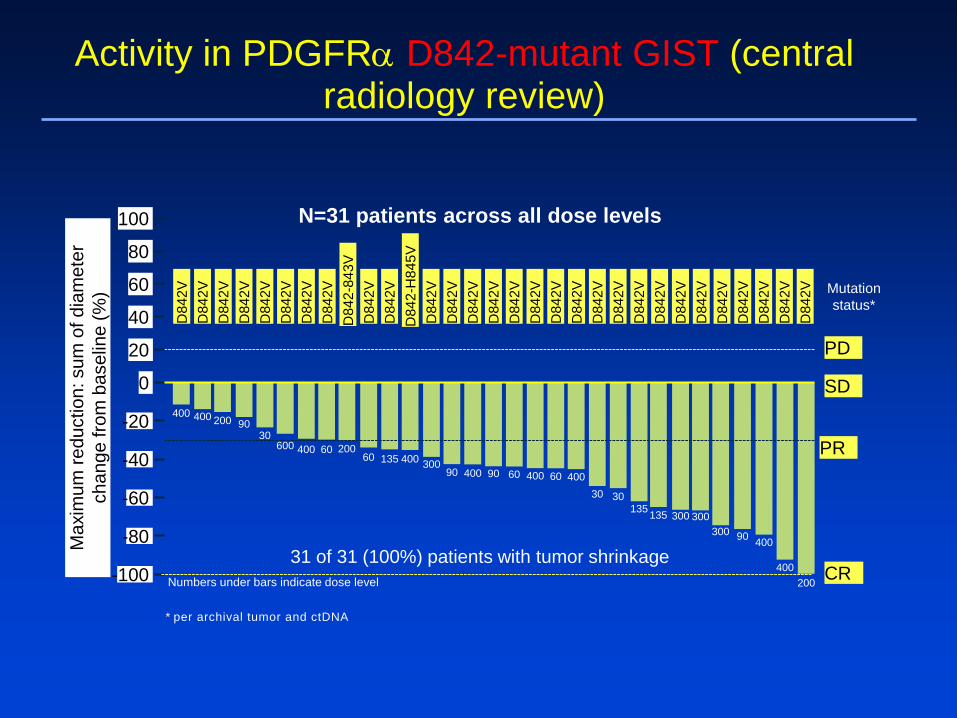
Activity in PDGFRα D842-mutant GIST (central radiology review)
31 of 31 (100%) patients with tumor shrinkage
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2-84
3VD
842V
D84
2VD
842-
H84
5VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
D84
2VD
842V
40
-40
-60
-100
Max
imum
redu
ctio
n: s
um o
f dia
met
erch
ange
from
bas
elin
e (%
)
-80
-20
0
20 PD
SD
PR
CR
80
60
100 N=31 patients across all dose levels
Mutation status*
* per archival tumor and ctDNA
400 400
400
30400
135 300
200
300 90 400
400200
300135
30
60400 90 609030040013560
2006040060030
90
Numbers under bars indicate dose level
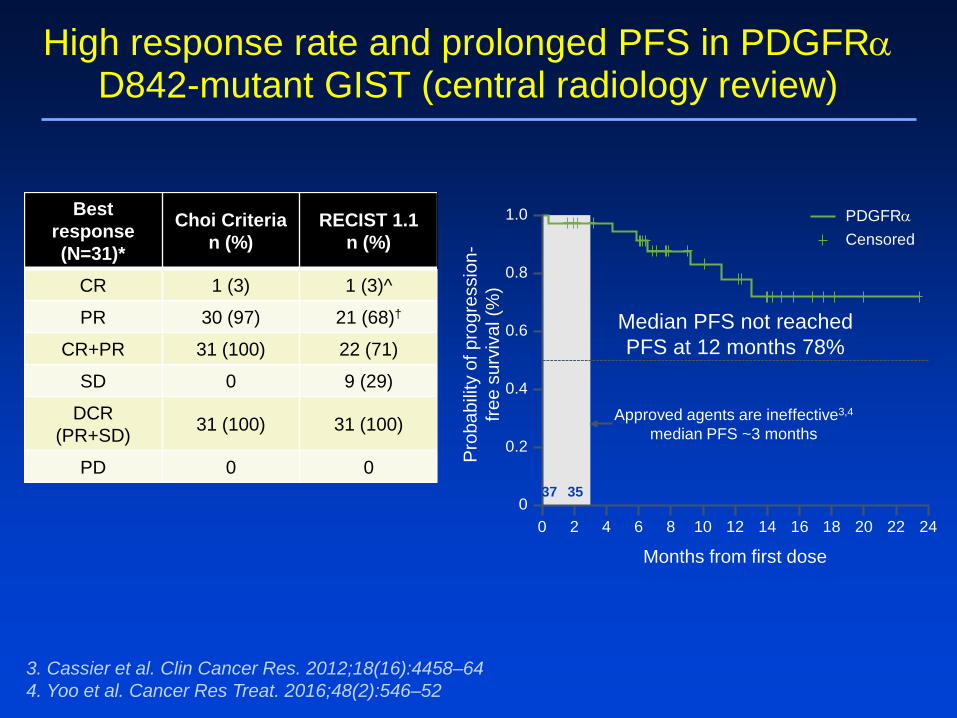
High response rate and prolonged PFS in PDGFRαD842-mutant GIST (central radiology review)
Best response(N=31)*
Choi Criterian (%)
RECIST 1.1n (%)
CR 1 (3) 1 (3)^
PR 30 (97) 21 (68)†
CR+PR 31 (100) 22 (71)
SD 0 9 (29)
DCR (PR+SD) 31 (100) 31 (100)
PD 0 0
Median PFS not reachedPFS at 12 months 78%
0 8 16 24
1.0
0.8
0.6
0.4
0.2
0
Months from first dose
Pro
babi
lity
of p
rogr
essi
on-
free
surv
ival
(%)
6 14 224 12 202 10 18
37 35 32 30 20 18 15 12 5 3 2 1 0PDGFR
PDGFRαCensored
Approved agents are ineffective3,4
median PFS ~3 months
3. Cassier et al. Clin Cancer Res. 2012;18(16):4458–64 4. Yoo et al. Cancer Res Treat. 2016;48(2):546–52

Investigators conclusion; BLU-285 has potent, clinically important activity in GIST
41
• BLU-285 is well-tolerated
• High response rates and prolonged PFS in PDGFRα-driven GIST
• Prolonged PFS in heavily pretreated KIT-driven GIST
• Based on these encouraging data:
– Phase 3 randomized study comparing BLU-285 to regorafenib in third-line GIST is planned to begin 2018

Switch pocket inhibitors – DCC2618
1Janku et al. JCO 2017; 55 (suppl. abstr. 2515)
• Bind to the ”switch pocket” of the kinase stabilizing it in an inactive confirmation
• Also inhibits the most aggressive exon 17 and 18 gain-of-function mutations in the activation switch.
On dose escalation Responses1
FDG-PET response 14/18 (78%)RECIST response 2/18 (11%)

Tumor Control in GIST Patients – DCC2618
Best Response per RECIST KIT & PDGFRα All Doses (n=37)
91% Disease Control (PR & SD) at Best Responseby RECIST at ≥100 mg Daily
##
*
# ##### #

Early Progression Free Survival Data
Notes: (a) Circles are patients (potentially >1 at any time point) who had not progressed as of end of treatment/study or last visit date if still on treatment; (b) Data is based on tumor response data investigator assessment.
Progression-Free Survival Rate KIT- and PDGFRα-driven GISTPatients; ≥ 100 mg daily (n=49) vs. < 100 mg daily (n=4)
Median PFS with placebo in 3rd/4th line (<1 month)
All patients treated at <100mg daily (n=4)
mPFS cannot be determined
mPFS is 15.2 weeks (CI 4.4 to 24)P
rogr
essi
on-fr
ee s
urvi
val
All patients treated at ≥100mg daily (n=49)

DCC-2618: Overview
• Phase 3 Registration Study for the treatment of patients with GIST who have received 3 prior therapies
• Phase 3 study for patients who have progressed on or are intolerant of imatinib
• 91% Disease Control by Best Response (PR & SD) by RECIST ≥100 mg daily
• Disease Control Rate ≥ 100 mg daily: • 76% (12 weeks)• 57% (24 weeks)
• Encouraging early PFS data• Clinical validation of broad
spectrum KIT profile
Current &Future Plans
Clinical Proof-of-Concept
in Heavily-Pretreated GIST Patients

Pivotal Phase 3 Study in 4th Line+ GIST Initiated Jan 2018(1)
Global Trial(n=120)
Placebo
150 mg QDDCC-2618
GIST Patients
3 prior lines of therapy(1)
80 Patients
40 Patients
Randomized2:1
Primary Endpoint for Approval = Median Progression Free Survival
Following progression: (a) placebo patients can crossover to DCC-2618 and (b) DCC-2618 patients can continue on treatment.
Abstract no: 2803523, CTOS 2017 Maui, Hawaii. Presented by Dr. Michael Heinrich

GIST the new generation*
*Robert Maki – ASCO CSS 2017
• Inhibition of ETV1 ( a survival factor for GIST); KIT and MEK inhibitors resulted in a DCR of 65% @8 weeks – no PR
• Immmune modification; Dasatanib + ipilimumab; Phase 1 reported. RR seen using Choi criteria
• RCT of Nivolumab vs Nivolumab + Ipilimumab underway Responses seen
• Dysregulation of hedgehog pathway (in 10% of mGIST) leads to increased expression of KIT

RImatinib, continuous
IMA IMAREGO REGO
weeks0 3 4 7 8 11 12 15
ALT-GIST study
1 week washout period – might these revive GIST progenitor cells?


Adjuvant Therapy: Imatinib

Recurrence-Free Survival
Presented By Chandrajit Raut at 2017 ASCO Annual Meeting
PERSIST-5: Five years of adjuvant imatinib
• 67 (74%) patients had high risk and 24 (26%) intermediate risk GIST
• 45 (49%) out of the 91 patients discontinued adjuvantimatinib

Ongoing randomised Phase III adjuvant trials
Trial Design Key eligibility criteria Primaryend point
SSG XXIINCT02413736
Imatinib 400mg/d 3 vs. 5 yrs
Very high risk of recurrence• gastric GIST, >10
mitoses/50 HPFs;• non-gastric GIST, >5
mitoses/50 HPFs, or• rupture
RFS
ImadGISTNCT02260505
Imatinib 3 yrs vs. imatinibmaintenance
Estimated risk of recurrence≥ 35%
DFS
Joensuu H et al. JAMA Oncol 2017;3:602-9

Acknowledgements
• The many patients and their families who contributed to these studies
• LifeRaft and other patient advocacy groups
• The many investigators that have designed and conducted these studies and were happy to share their data for this presentation
• The many companies involved in this international effort to improve outcomes for patients with GIST