gastroenterology flash cards. ibs = includes crohns and ulcerative colitis adjunctive- loperamide...
TRANSCRIPT

GastroenterologyFlash Cards

Ibs = Includes Crohns and Ulcerative Colitis• Adjunctive- Loperamide 2mg after each loose stool (max
16mg/day)• Antispasmotics- Dicyclomine, Propantheline, Hyoscyamine• Cholestyramine- For Bile Salt-induced diarrhea after Ileal
Resection• Aminosalicylates- next slide• Corticosteroids- next slide• Antibiotics – Cipro and Flagy• l• NEXT SLIDE= IMMUNOSUPRESSANTS

UlCERATIVE COLITIS• Immuno-modulator- MTX (Crohns only) Azathioprine,
6MP(Mercaptopurine)
• Infliximab (remicade) – UC & Crohns-for refractory pt. 40-80% response.. Up to 50% of patients develop antibodies against it.
• Adalimumab (Humira)-(Fully humanized- no antibodies form) UC & CD. For remicade failures. SUB-Q
• Certolizumab (Cimzia) – UC 62% response for C-React >10, 37% if C-React < 10
• Golimumab (Simponi) – UC Sub-q• Natalizab (Tysabri) – UC.. Assoc with
leukoencophalopathy.. Check for mental status change

IBS –treatment- Side-effects.• TNF-alpha antagonist-- Risk infection (screen TB & Hepatitis),
heart failure, hepatosplenic t-cell lymphoma when used w azathrioprine or 6mp in young males, antibody formation
• Antimotility agents- Risk of toxic megacolon
• Azathioprine (6MP)- Bone marrow supression, pancreatitis, hypersensitivity, need to check TPMT enzyme prior to giving. This enzyme is responsible for inactivating it. Must have TPMT
• Methotrexate- Bone marrow supression, pulmonary, hepatic toxicity
• Corticosteroids- adrenal supression, metabolic effects, infection.
Irritable Bowel (tx diarrhea or constipation)• Hyoscyamine/Dicyclomine- Target pain to spam and also tx diarrhea. Initial
or adjunctive therapy for IBS-D or IBS-M• Tricyclic-Antidepresants- Garget pain and diarrhea. Generally reserved for
IBS-D, low doses
• SSRI- Target pain and often have promotility action in IBS-D. Can also tx comorbid depression for anxiety
• Lubriprostone- Indicated for IBS-C in women> 18yo. Main adverse effect- nausea, very expensive
• Probiotics- Some potential improvement in global symptoms and pain• Alosetron- Indicated for IBS-D in women>18 yo, failing other therapies. Mus
be enrolled in program. Risk of ischemic colitis• Tegaserod- Indicated for IBS-C… available on emergy use only due to CV risk• Rifaximin– Some data to support improvement in bloating.

IBS- 5-aMINOSALICYLATES• General 5HT side-effects: rash, fever, pneumonitis, hepatotoxicity,
bone marrow depression, hemolytc anemia, pancreatitis.
• Sulfasalazine- (sulfa)- 20-25% discontinue due to intolerance to sulfa (hypersensitivty) (azulfidine and azulfidine EN).. Cleaved by colonic bacteria to 5ASA
• Meslamine (Pentasa, Asacol) – no sulfa- Delivers to large intestine (poor choice for crohns) Use for UC of large intestine. Suppository= procilir Mesalamine enema is more effective than hydrocortisone enema for left sided disease.
• Olsalazine (Dipentum) – delivers mesalamine past small intestine to large intestine and colon. Se= diarrhea in up to 25%
• Balsalazine (Colazal) = delivers mesalamine to large intestine. (ulcerative colitis is confined to large intestine)

IBS- Corticosteroids• 1. Works quickly to supress inflammation during Flareups• 2. No role in maintenance.. Although > 50% are dependent on
steroids• 3. Budesonide is about 15x more potent than prednisone. Allow 2
weeks overlap when changing from prednisone to budesonide. Only 10-20% is systemically absorbed.
• Prednisone- 20-60 mg/day• Budesonide Capsule (Entocort) 9mg/day, then 6mg q day for up to
3 months. Minimal absorption , for crohns, involving colon• Budesonide tablet (Uceris) 9mg/day x 8 weeks- for mild to mod UC• Hydrocortisone- 100mg q 8 hrs• Methylprednisolone 15-48 mg/day – 7010 days, chg to po when
gut if functional.

IBS –case 1• JT is admitted via the Emergency room with exacerbation of
Crohns. What is the initial treatment option?
1. Methotrexate 15mg q week2. Natalizumab now3. Methylprednisone 40 mg q day4. Mesalamine now
5. Answer: Steroids have the fastest action.

IBS-Case 2• KT is at home after a two week stay in the hospital for
exacerbation of Crohn’s. Her Crohns is slowly improving with the prednisone 20mg q day she is taking, however, her blood glucose has been in the 400s, what alternative therapy might be prudent?
1. Switch prednisone to Balsalazine2. Switch prednisone to Budesonide 9mg/day w 2 week
overlap3. Stop taking prednisone.4. Decrease prednisone and add sulfasalazine
5. Answer: budesonide is only 10-20% absorbed

IBS– case 3• JJ is taking Azulfidine for her Crohns and appears to be
controlling it at the moment. She breaks out in a rash and has in increase in her eosinophil count, what should we recommend?
a. Stop azulifidine and give prednisone.b. Stop azulifidine and switch to Asacolc. Stop azulifidine and swich to mesalamine enemad. Stop auzlifidine and switch to Infliximab
e. Answer: enema covers only colon. Use a non-sulfa 5-aminosalicylate such as asacol.

IBS-case 4• JL is a 84 YO female with Irritable Bowel Disease, Atrial Fib, post
Stroke who is currently suffering from constipation that has not responded to typical laxatives
• What do you recommend?
A. Add RifaximinB. Add LubiprostoneC. Add TegaserodD. Put patient on fluid restriction.
E. Answer: Add lubriprotone. Rifaximin is for bloating, tegaserod can’t be used if CV risk.

IBS treatment
Ulcerative Colitis• Mild to moderate-
aminosalicylate or budesonide
• Moderate to severe- Infliximab or azathioprine
• +/- short term steroid
• Last line: Vedolizumab
Crohns• Mild to moderate-
Aminosalicylate or budesonide
• Moderate to Severe- TNK-alpha inhibitor
• +/- short term steroid
• Last line: Vedolizumab or Natalizumab

Hepatitis b- Diagnosis and monitoring• HBsAg--- appears 1-10 weeks after exposure, for most pts it will
disappear in about • 6 months. For chronic pt it will stay POSITIVE.
• HBeAg---- This serologic marker indicates HBV replication and infectivity. It’s
• presence is usually associated with high HBV DNA levels.
• SEE NEXT SLIDE FOR MORE ANTIGEN/AB

Hepatitis b- Diagnosis and monitoring• HBV DNA- Assess replication, under 2,000 means HBV
is dormant. >20K• means treatment is needed. Biopsy and AST
and clinical signs• need to be considered.• HBcAg (core) The antibody to HBcAg is Anti-HBcIgM.
When this rises and HBcAG • decreases, we say they are cured.- Anti-HBCIgM POS and HBsAg negative.. Means you either
had Hep B or have been vaccinated- - ALT levels are also monitored - Vaccine prophylaxis– Anti-Hbs >- 10 mIU/ml

Hepatitis B –Case study• SS went to the physician’s office due to feeling fatigue and
complained of a ‘yellowish tint to her skin.’ Lab work was done with an elevated ALT/ AST and high HBsAG levels… She returned in 4 months with Decreased HBsAg, elevated AntiHBsAg, and positive. What does this mean?
a. SS has chronic Hepatitis Bb. SS is building resistance to Hep Bc. SS is cured of Hep Bd. There is not enough information to make a choice.
e. ANSWER: c… when HbsAG drops, it means hep B is gone, like wise the antiHBsAG means she will have immunity to hep b.

COMPLICATIONS OF PROTON PUMP INHIBITORS• Risk of fractures
• Hypomagnesium
• C-Diff
• CAP
• Inhibit CYP450- omeprazol inhibit clopidogrel• CYP2C19- inhibit diazepam

Treatment of Hepatitis B• TREATMENT FOR: -- chronic HBV pts ( HBeAg positive or HBeAg negative
chronic hepatitis. Pts with HBV DNA >2000 int units/ml – peristent biopsy, ALT >=2….
• TREAT WITH: IFN-a 16 weeks• PEGIFN-a: 48 weeks• LAM/ADV/ETV/ldT/TDF- minimum 1 year. Tx at least 6 months • after conversion
• END-POINT of TREATMENT- Seroconversion from HBeAg to anti_HBe

Cirrhosis• ENCEPHALPATHY-- give lactulose- titrate to 2-4 loose stools / day
(30ml qid may add Rifaximin 400mg tid
• SBP-CRITERIA------ Ascitic Protein < 1.5 gm/dl + Scr >= 1.2 = should receive treatment for prevention = bactrim ds q day
• Treatment= w cefotaxime if serum albumin/ascitis albumin < 1.1 otherwise ascitis is due to protal hypertension. Neutrophil count done, 10 ml ascitic fluid cultured.
• Eg: serum alb = 2.2 and ascitic alb = 1.4 SAAG= 2.2/1.4 = 1.5 portal htn

Spontaneous bacterial peritonitis & variceal bleed
• PROPHYLAXIS WITH TMP/SMX OR CIPRO- Pts who have had prior SBP, ascitic fluid protein is < 1.5gm/dl with impaired renal or liver failure (scr>=1.2mg/dl or BUN>=25, or serum sod <130)
• TREATMENT WITH 3RD GEN CEPH OR QUINOLONE- PMN >=250 cells/mm3 or Temp > 100 or abdom pain and/or tenderness, change in mental status
• VARICEAL BLEED---- 30-50% mortality with bleed, 70% recurrence rate in 1st month.
• 1. stabilize with iv fluids• 2. band ligation• 3. Proton-pump inhibitor drip , octreotide x 3-5
days, • 4. Vasopressin and nitroglycerin• 5. Non-specific beta blockers.

H Pylori• DIAGNOSIS--- Rapid Urease Urate Breath test• Fecal antigen test• IGG- test serologic• Confirmed success- 1st two are negative, IGG will remain POS
forever.
• TREATMENT: 4 drug regimen better than 3 drug.• 4 drugs x 14 days= 90% effective 2% reinfection • rate• IF PCN allergic.. Use flagyl in place of amoxil• 4 drug= PPI + Bismuth + flagyl + TCN … 10-14 days• Triple = PPI + amoxil or flagyl + Clarithromycin

Hepatitis C-traditional treatment• RIBAVIRIN (COPAGUS)- Purine Nucleoside analog x 12-24 weeks PLUS
Peginterferon alpha2a (pegasys) (USE BOTH OF THESE w one of the following:
• -Boceprevir (protease Inhibitor)– anemia, decrease neutrophil, dysgeusia
• -Telaprevir (protease Inhibitor)- Rash, Anorecal discomfort, steven-johnson
- Simeprevir (protease Inhibitor) 2nd generation..rash, life threating photosensitivity,
- Pruritis.
- ** beware of P450 drug interactions **
Hepatitis C - Treatment• DX: Serologic Assay for antibodies to Hep C. Detect or quantify
HCV RNN• if alt > 2x ULN and HBV DNA > 20k• SCREEN: people w fibrosis panel, consider lung biopsy• 20-30% of positive pts will get chronic respiratory
disease.
• Telaprevir 750mg tid x 12 wks boceprevir 800mg tid start after 4 wks
• Plus peg-inferon followed by after 4 weeks• Peg inft rivarvirin x 12 weeks
• Entecavir and tenofovir are Preferred.

Hepatitis c- harvoni
• HARONI – fixed dose of ledipasiir sofosbvir
• Treatment naive pts w or w/out cirrhosis– 12 weeks• Treatment duration Not- naïve pt w cirrhosis----- 24
weeks.
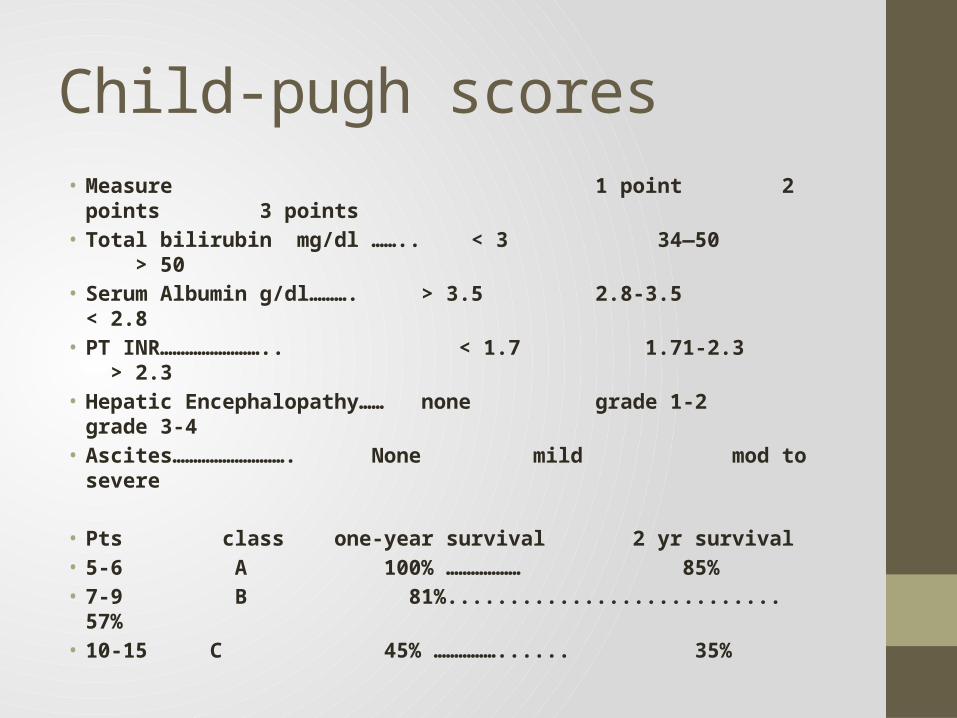
Child-pugh scores• Measure 1 point 2 points 3 points• Total bilirubin mg/dl …….. < 3 34—50 > 50• Serum Albumin g/dl………. > 3.5 2.8-3.5 < 2.8• PT INR…………………….. < 1.7 1.71-2.3 > 2.3• Hepatic Encephalopathy…… none grade 1-2 grade 3-4• Ascites………………………. None mild mod to severe
• Pts class one-year survival 2 yr survival• 5-6 A 100% ……………… 85%• 7-9 B 81%........................... 57%• 10-15 C 45% ……………...... 35%
Pepcid ulcer disease• PEPTIC ULCER - either duodenal or gastric• - etiology: H. pylori, NSAIDS• -risk: age > 60, hx pud, corticosteroids, anticoag, • asa.smoking, cvd, ra, ssri• - treatment: PPI for 8-12 weeks (2013 gerd • guidelines= 8 wks)
• GERD--- Don’t worry about dx.. Just tx with PPI• -treatment- 1st PPI second= h2 blockers • third= promotility agents, 4th- surgery
• Note: if take off asa for bleed.. Put back on asa within 1 week.

GERD
• ENDOSCOPY WARRENTED IF: -dysphagic, bleeding, wt loss, choking, cp..
• otherwise it is prudent to give PPI/H2 without endoscopy.
• PRESUMPTIVE GERD: No diagnosis needed. Ambulatory pH reflux monitoring recommended.
• LIFE-STYLE– wt loss, avoid eating 2-3 hrs prior to hs, avoid EtOH, caffeine chocolate, spicy food, nicotine, tight clothes, fats, anticholinergic benzo, tca, estrogen, calcium channel blockers. – if asymptomatic may stop
• TX::.. PPI x 8 weeks given before meals. If partial response then bid.
• Drug interactions (neutral stomach) – ketoconazole, iron, protease inhib.
GERD- CASE STUDY• LJ arrives at the pharmacy requesting for something to take for a
burning stomach.• When questioned how often, she says usually about once a day .
She has no bleeding and has been eating with no problems.. Usually after supper. What is your recommendation for her?
a. See a physician to get an endoscopeb. Sell her a bottle of proton-pump inhibitorc. Sell her a bottle of H2 blockersd. Tell her to eat some crackers.
e. Answer: Presumptive GERD does not need a dx, Proton pump inhibitors are more effective than H2-blocker.