gallium-67 in of sarcoidosis: serum angiotensin-converting
TRANSCRIPT

Thorax 1982;37:11-18
Gallium-67 in the evaluation of sarcoidosis:correlations with serum angiotensin-convertingenzyme and bronchoalveolar lavageD BEAUMONT, JY HERRY, M SAPENE, P BOURGUET, JJ LARZUL,B DE LABARTHE
From the Hopital de Pontchaillou, Rennes, France
ABSTRACT Gallium-67 (67Ga) scanning was assessed for its usefulness in the evaluation and follow-upof 54 patients with sarcoidosis, both treated and untreated. Scans were repeated in 23 subjects.Serum levels of angiotensin-converting enzyme (ACE) were determined concurrently in all 54 patientsand bronchoalveolar lavage was performed in 29 patients. Gallium-67 scan was effective in thedetection and assessment of lesions not revealed by traditional methods of investigation, particularlythose affecting the mediastinum, spleen, and salivary glands. The scan also enabled fibrotic lesions,which do not show uptake, to be distinguished from granulomatous lesions, which do-an advantageof prognostic interest particularly in patients with pulmonary lesions. Another merit of 67Gascanning was that it offered a means of following disease progression in each site. In patientsshowing spontaneous clearing of disease or receiving treatment the scintigraphic method was moresensitive than serum ACE determination. Scan findings showed a rough correlation with serum ACEbut not with bronchoalveolar lavage findings. This suggests that the three markers probably reflectdifferent stages of the granulomatous process. On the strength of this study the indications for galliumscanning in sarcoid patients can be defined more clearly than has previously been possible.
Sarcoidosis, a systemic granulomatous disease ofunknown cause may involve such a variety of sitesas to require multiple methods of investigation.The course of the disease is unpredictable. Custom-ary investigative approaches give a relatively pooridea of the spread and activity of the granulomatousprocess. Recently, serum angiotensin-converting
Address for reprint requests: Dr Jean-Yves Herry,Laboratoire des Radio-Isotopes, Centre Eugene Marquis,Centre Hospitalier de Pontchaillou, 35011 Rennes, France.
enzyme (ACE)1 and the lymphocyte count inbronchoalveolar lavage fluid2 have been proposed asmarkers of disease activity. The object of the presentstudy was to assess the usefulness of 67Ga uptake as
another possible marker. Gallium-67 concentrates ininflammatory tissue34 through an imperfectly under-stood mechanism. It is commonly used to identifyoccult postoperative abscesses. Several investi-gators5-15 have reported particularly intense con-centration of gallium in sarcoid granulomas and, in
Table 1 Gallium-67 scanning in sarcoid patients: summarised data from the literature
Authors Reference Year Number of Scintigraphicfollow-up (two or more scans) Other marker of diseasepatients Treated patients Untreated patients activity used
McKusick 5 1973 1 1 0 0Fogh 6 1974 7 0 0 0Heshiki 7 1974 29 0 0 0Kinoshita 8 1974 3 3 0 0Galassi 9 1975 2 0 0 0Schermuly 10 1975 25 1 0 0Israel 1 1 1976 27 3 0 0Niden - 12 1976 6 2 0 0Mishkin 13 1978 40 1 0 0Siemsen 22 1978 111 64 0 0Nosal 15 1979 27 0 0 ACE*Present study 1981 54 8 16 ACE* BALt
*Angiotensin-converting enzyme. tBronchoalveolar lavage.
11
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from
2Beaumont, Herry, Sapene, Bourguet, Larzul, de Labarthe
some instances, clearing of uptake in patients oncorticosteroid therapy (table 1). In the present studygallium scan results were compared with those ofserum ACE determination and bronchoalveolarlavage lymphocyte count and were evaluated in thefollow-up of patients either treated or not.
Methods
Fifty-four patients with mediastinal and pulmonarysarcoidosis were studied. Diagnosis was based onsuggestive radiographic findings supported byhistological examination of one or more tissuebiopsy specimens. The Kveim test was not performed.Thirty-five of the patients were males and 19 females,with ages ranging from 13 to 65 years (mean35 years). In 24 of the patients two or three repeatscans were performed at 6-12 month intervals. Datafrom 70 such examinations were retained forevaluation. They formed three groups: 52 examin-ations performed in untreated patients with acute orchronic sarcoidosis comprised group A; eightexaminations in untreated patients displaying clearsigns of disease regression comprised group B; and10 examinations in patients on corticosteroids at thetime of examination comprised group C. We did notattempt to classify the group A patients moreprecisely, since disease activity is notoriously difficultto define by classical methods. The group A patientsformed three subgroups: nine patients with radio-graphic evidence of mediastinal adenopathy alone(group Al); 31 with pulmonary involvement(group A2); 12 with radiographic evidence ofpulmonary fibrosis (group A3). Data from morethan one examination in the same patient wereretained only if the patient showed a change ofdisease status as defined by the above grouping.Thirty patients with suspected abdominal abscessesand submitted to the same investigative protocolserved as controls.
Anterior and posterior total views were obtainedwith a whole body imager 72 hours after theintravenous injection of 60 ,uCi/kg of 67Ga citrate.Additional local camera views were obtained of theface and chest regions.16
Uptake in mediastinum, lungs, parotid glands,eyes, nose, and spleen was graded "blind" by twoobservers according to the classification proposed byseveral investigators.712141517 Grading was relative toliver activity, grade 0 signifying uptake comparableto background; grade 1 uptake less than, grade 2uptake equal to, and grade 3 uptake greater thannormal hepatic activity.Serum ACE was assayed in all cases concurrently
with 67Ga scanning by the method of Cushman andCheung18 modified to facilitate analysis of elevated
values.19 In a previous study a control populationhad shown the upper limit of normal to be 33 U/ml.'9
In 29 patients bronchoalveola'r lavage was per-formed simultaneously with the above studies. Salinewas pumped into the lungs through a fibreopticbronchoscope and gently recovered in 30 ml pulsesto a total of 300 ml. The lavage fluid was analysedby the method of Reynolds,20 the alveolar lymphocytecount being expressed as number of cells/l00 mlfluid. In 18 patients the T-lymphocyte populationwas quantified by anti-T-cell cytotoxicity.
Results
CONTROLSScanning data obtained from control subjects havebeen detailed in a previous report.16 They were
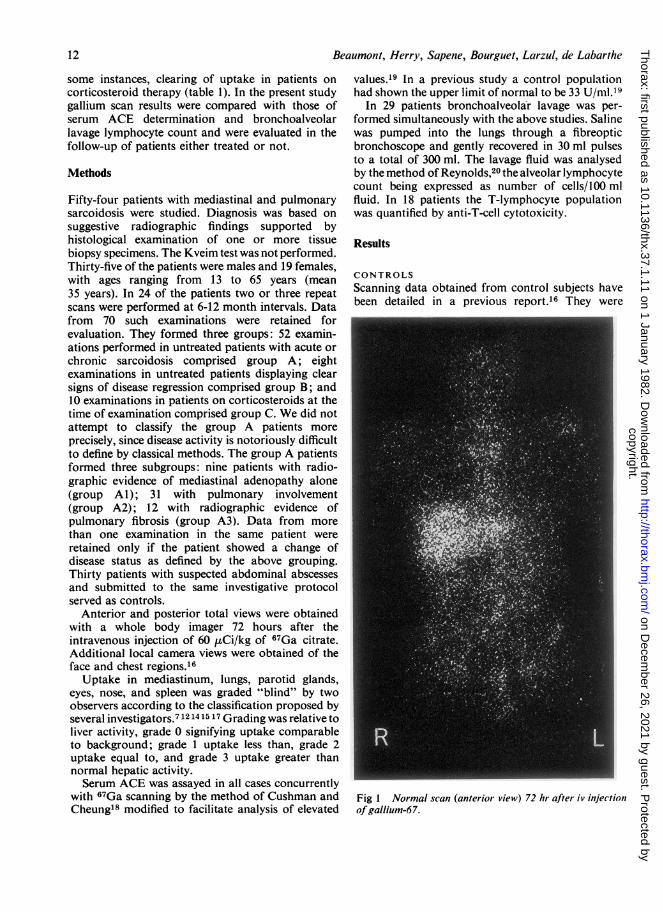
Fig I Normal scan (anterior view) 72 hr after iv injectionofgallium-67.
12
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from
13Gallium-67 in the evaluation of sarcoidosis
consistent with observations described by otherinvestigators:21 22 72 hr after injection, activity over
the liver was pronounced in all cases, with diffuseuptake in the skeleton as a whole but no uptake inmediastinum, lungs or salivary glands (fig 1).Grade 1 uptake was noted in the eyes and nose, andbreast uptake in 45 % of the women examined.
PATIENTS
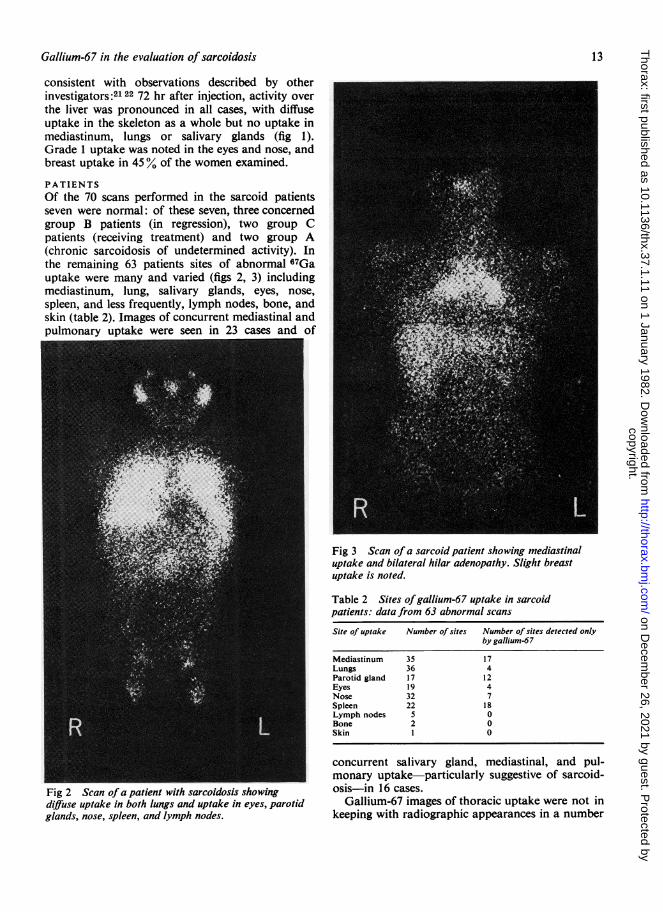
Of the 70 scans performed in the sarcoid patientsseven were normal: of these seven, three concernedgroup B patients (in regression), two group Cpatients (receiving treatment) and two group A(chronic sarcoidosis of undetermined activity). Inthe remaining 63 patients sites of abnormal 67Gauptake were many and varied (figs 2, 3) includingmediastinum, lung, salivary glands, eyes, nose,
spleen, and less frequently, lymph nodes, bone, andskin (table 2). Images of concurrent mediastinal andpulmonary uptake were seen in 23 cases and of
Fig 3 Scan of a sarcoid patient showing mediastinaluptake and bilateral hilar adenopathy. Slight breastuptake is noted.
Fig 2 Scan ofa patient with sarcoidosis showingdiffuse uptake in both lungs and uptake in eyes, parotidglands, nose, spleen, and lymph nodes.
Table 2 Sites ofgallium-67 uptake in sarcoidpatients: data from 63 abnormal scans
Site of uptake Number of sites Number of sites detected onlyby gallium-67
Mediastinum 35 17Lungs 36 4Parotid gland 17 12Eyes 19 4Nose 32 7Spleen 22 18Lymph nodes 5 0Bone 2 0Skin I 0
concurrent salivary gland, mediastinal, and pul-monary uptake-particularly suggestive of sarcoid-osis-in 16 cases.
Gallium-67 images of thoracic uptake were not inkeeping with radiographic appearances in a number
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from

4Beaumont, Herry, Sapenie, Bourguet, Larzul, de Labarthe
of cases23 (table 2). In 17 of these cases gallium scanslocalised mediastinal lesions undetectable on plainchest films and four patients displayed pulmonaryparenchymal uptake but had normal chest films; inthree of these four patients pulmonary involvementwas confirmed by open lung biopsy. Abnormalradiographic appearance in the absence of 67Gauptake suggest fibrotic sequelae of sarcoidosis: thiswas the case in seven group A2 patients (withoutspecific evidence of fibrosis on chest films) and fourgroup A3 patients (with evidence of fibrosis). In theeight other group A3 patients persistence of 67Gauptake pointed to the presence of a still activegranulomatous process.
Extrathoracic 67Ga images pointed to sites ofinvolvement undetected clinically or radiographically(table 2). Salivary gland 67Ga uptake was seen in12 patients with no corresponding clinical signs; inthree of these patients, uptake was intense (grades 2and 3) but gland size was normal; in nine of the12 patients, poor lacrimal secretion on the Schirmertest pointed to associated lacrimal gland involvementconsistent with a diagnosis of Sj6gren's syndrome.Gallium-67 uptake by the spleen in the absence of
ACEu/mI100
60 @
:* . -** ..*0%
0~~~~~~
0 1 2 3 4 5
clinical or radiographic signs of splenomegaly wasobserved in 18 patients, attaining grade 2 or 3 in 12.Uptake in nose and eyes was common and, withrespect to uptake patterns seen in control subjects,could be regarded as abnormal at grade 2 or 3intensity: by this definition seven patients showedclinically asymptomatic abnormal uptake in thenose, confirmed by nasal mucosa biopsy in twopatients, and four patients showed ocular involve-ment. In a small number of cases some uncommonsites of disease involvement were not localised bygallium scans: kidney, muscle, prostate, heart, andbrain. Hepatic lesions, of course, cannot be imagedby 67Ga scanning because of normally intensehepatic uptake.The group A patients showed a correlation between
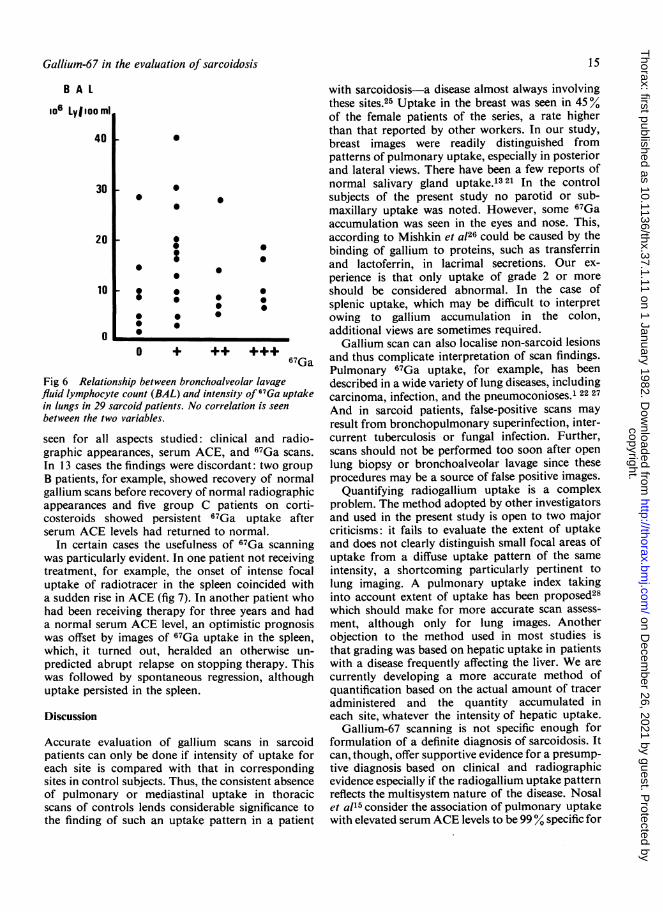
serum ACE and number of sites of 67Ga uptake24(fig 4). Of the 18 patients with disease clearing eitherspontaneously or in response to therapy, 10 exhibitedclinical signs of cure with normal ACE levels butseveral sites of 67Ga uptake (fig 5). Alveolar lym-phocyte counts in bronchoalveolar lavage fluid-both absolute and relative T-cell counts-showedno correlation with intensity of lung radiotraceruptake (fig 6).
In 11 of the 24 patients submitted to repeatexaminations, parallel patterns of development were
ACEu/ml
50
33
67Ga
Fig 4 Relationship between number of 67Ga uptakesites (mediastinum, lungs, salivary glands, spleen, andlymph nodes) and serum levels of angiotensin-convertingenzyme (ACE) in group A untreated sarcoid patients. Apositive correlation is seen between the two variables(r = 0(43;p < 001).
o
* Untreated
+On steroids
+
0*I.
* +0
0
+
+
* + 0
0 1 2 3 4 67Ga
Fig 5 Relationship between number of 67Ga uptakesites and serum ACE levels in sarcoid patients undergoingregression or on treatment (groups B and C). Frequentpersistence of 67Ga uptake is seen despite normalangiotensin-converting enzyme levels (ACE).
14
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from
Gallium-67 in the evaluation of sarcoidosis
B AL
1o6 LylioomI1
40
30
20
10
0
0
0
0
0
0
0i
O + ++ +++67Ga
Fig 6 Relationship between bronchoalveolar lavagefluid lymphocyte count (BAL) and intensity of 67Ga uptakein lungs in 29 sarcoid patients. No correlation is seen
between the two variables.
seen for all aspects studied: clinical and radio-graphic appearances, serum ACE, and f67Ga scans.
In 13 cases the findings were discordant: two group
B patients, for example, showed recovery of normalgallium scans before recovery of normal radiographicappearances and five group C patients on corti-costeroids showed persistent 67Ga uptake afterserum ACE levels had returned to normal.
In certain cases the usefulness of 67Ga scanningwas particularly evident. In one patient not receivingtreatment, for example, the onset of intense focaluptake of radiotracer in the spleen coincided witha sudden rise in ACE (fig 7). In another patient whohad been receiving therapy for three years and hada normal serum ACE level, an optimistic prognosiswas offset by images of 67Ga uptake in the spleen,which, it turned out, heralded an otherwise un-
predicted abrupt relapse on stopping therapy. Thiswas followed by spontaneous regression, althoughuptake persisted in the spleen.
Discussion
Accurate evaluation of gallium scans in sarcoidpatients can only be done if intensity of uptake foreach site is compared with that in correspondingsites in control subjects. Thus, the consistent absenceof pulmonary or mediastinal uptake in thoracicscans of controls lends considerable significance tothe finding of such an uptake pattern in a patient
with sarcoidosis-a disease almost always involvingthese sites.25 Uptake in the breast was seen in 45%of the female patients of the series, a rate higherthan that reported by other workers. In our study,breast images were readily distinguished frompatterns of pulmonary uptake, especially in posteriorand lateral views. There have been a few reports ofnormal salivary gland uptake.13 21 In the controlsubjects of the present study no parotid or sub-maxillary uptake was noted. However, some 67Gaaccumulation was seen in the eyes and nose. This,according to Mishkin et a!26 could be caused by thebinding of gallium to proteins, such as transferrinand lactoferrin, in lacrimal secretions. Our ex-perience is that only uptake of grade 2 or moreshould be considered abnormal. In the case ofsplenic uptake, which may be difficult to interpretowing to gallium accumulation in the colon,additional views are sometimes required.
Gallium scan can also localise non-sarcoid lesionsand thus complicate interpretation of scan findings.Pulmonary 67Ga uptake, for example, has beendescribed in a wide variety of lung diseases, includingcarcinoma, infection, and the pneumoconioses.1 22 27And in sarcoid patients, false-positive scans mayresult from bronchopulmonary superinfection, inter-current tuberculosis or fungal infection. Further,scans should not be performed too soon after openlung biopsy or bronchoalveolar lavage since theseprocedures may be a source of false positive images.
Quantifying radiogallium uptake is a complexproblem. The method adopted by other investigatorsand used in the present study is open to two majorcriticisms: it fails to evaluate the extent of uptakeand does not clearly distinguish small focal areas ofuptake from a diffuse uptake pattern of the sameintensity, a shortcoming particularly pertinent tolung imaging. A pulmonary uptake index takinginto account extent of uptake has been proposed28which should make for more accurate scan assess-ment, although only for lung images. Anotherobjection to the method used in most studies isthat grading was based on hepatic uptake in patientswith a disease frequently affecting the liver. We arecurrently developing a more accurate method ofquantification based on the actual amount of traceradministered and the quantity accumulated ineach site, whatever the intensity of hepatic uptake.
Gallium-67 scanning is not specific enough forformulation of a definite diagnosis of sarcoidosis. Itcan, though, offer supportive evidence for a presump-tive diagnosis based on clinical and radiographicevidence especially if the radiogallium uptake patternreflects the multisystem nature of the disease. Nosalet al15 consider the association of pulmonary uptakewith elevated serum ACE levels to be 99% specific for
15
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from

Beaumont, Herry, Sapene, Bourguet, Larzul, de Labarthe
Fig 7 Gallium-67(A andB) scans of a 25-year-old patientwith untreated sarcoidosis, who showed a clear rise inserum ACE levels with no clinical or radiographicchanges.67Ga scan (B) showed the onset of intense focal uptake inthe spleen.
sarcoidosis. Pulmonary uptake ofgallium,29 however,and sometimes elevated ACE levels30 have both beenreported in silicosis patients. We share the view ofDe Remee et al3 that the results of these techniquesmust be confirmed by histopathological examin-ation before definitive diagnosis can be established.
Gallium-67 scans sometimes merely confirmknown sites of disease involvement. The advantage,though, is that with a single non-invasive investi-gation one has an overall view of the disease pattern,sometimes obviating the need for additionalexplorations, such as mediastinal tomography andscans of the salivary glands or spleen. In addition,hitherto unsuspected lesions are often detected bygallium scans. Instances of mediastinal adenopathyfor example, invisible on radiographs but disclosedby gallium scintigraphy, were seen in the presentstudy and have been described by others.7 10 In our
experience, scanning evidence of subclinical salivarygland or splenic involvement is also common.
Finally, in three patients in the present study 67Gascanning was more sensitive than radiography indetecting pulmonary lesions. Some lesions, however,notably of the skin or heart, were too small to showup on gallium scan. Others, as in the liver, werehidden by normal intense uptake.With thoracic sites of involvement 67Ga scans
enable granulomatous lesions, which accumulatetracer, to be distinguished from fibrotic lesions,which do not. In the present series 67Ga scansrevealed fibrotic residua in 11 patients, includingseven in whom radiography was not suggestive offibrosis. Then again, 67Ga uptake may be the onlysign of granulomatous tissue within apparentlypurely fibrotic tissue, with clear implications fortreatment planning.'0
Gallium-67 scan, serum ACE level, and broncho-alveolar lavage lymphocyte count each correlateswith clinical disease activity.31-33 Concordance ofthe results of these three investigations, however,was not as close in our study as might be expected.Our findings are in line with the observations ofGupta et al34 who found a significant correlation
16
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from

Gallium-67 in the evaluation of sarcoidosis
between ACE levels and 67Ga scans but not betweenbronchoalveolar lymphocyte count and 67Ga scans.35They are, however, at odds with those of Crystalet al,33 who report a statistically significant cor-relation between the lavage fluid lymphocyte countand pulmonary 67Ga uptake. Such variabilityreflects the difficulty of comparing data subject towidely differing modes of evaluation. Results of thethree tests probably correspond to different stagesof the granulomatous reaction in sarcoid patientsand are thus complementary rather than concord-ant.24 Gallium scanning in our view, possesses twoadvantages: first, it provides an overall picture of thedisease, whereby the progression of the granu-lomatous process can be followed at each site ofinvolvement; and second, it is a more sensitiveindicator of disease activity than serum ACE levelsin patients in whom the disease is only mildlyactive or actually regressing.15 31 In our experiencean additional merit of scintigraphy over ACEmeasurement and one that is particularly useful inthe follow-up of patients receiving treatment, is thatit appears less affected by corticosteroid admin-istration.Although 67Ga scintigraphy is an innocuous,
simple method of investigation and is thus suitablefor outpatient use, two limiting factors must beconsidered: cost and radiation dose delivered to thepatient. Estimated whole-body dose is 260 mrad/mCi,equivalent to an average of 600 mrad per exam-ination; the dose to the gonads is of the same order.Although low,36 37 this dose is not a negligibleconsideration in young patients.
In conclusion, the findings of the present studyhighlight certain problem areas where 67Ga scanningis useful in the investigation of sarcoidosis. Theseare, firstly, diffuse chronic pulmonary involvement,where granulomatous lesions can be distinguishedfrom fibrosis; secondly, cases where several organ-systems are involved and where certain sites may bemissed; and thirdly, sarcoid patients on treatment,in whom 67Ga scans may offer evidence of persistentdisease activity and thus a solid basis for planningthe dosage and duration of continued treatment.Whether or not routine use of 67Ga scintigraphyshould be envisaged for the diagnosis, staging andfollow-up of all sarcoid patients is a question thatrequires further study. One factor to be consideredis the abandonment of classical investigativemethods, notably repeat tomography, that wouldresult from such a decision.
References
Lieberman J. Elevation of serum angiotensin convertingenzyme (ACE) level in sarcoidosis. Anm J Med 1975;59:365-72.
17
2 Dauber JH, Rossman MD, Daniele RP. Broncho-alveolarcell populations in acute sarcoidosis. Observations insmoking and nonsmoking patients. J Lab Clin Med1979;94:862.
Tsan MF, Chen WY, Scheffel V, Wagner HN. Studies onGa accumulation in inflammatory lesions. I) Ga uptakeby PMN leucocytes. J Nucl Med 1978;19:36-44.
Weiner R, Hoffer PB, Thakur ML. Lactoferrin: its role asa Ga-67 binding protein in polymorphonuclear leuco-cytes. J Nucl Med 1981 ;22:32-7.
McKusick KA, Singh Soin J, Ghiladi A, Wagner HN.67 Gallium accumulation in pulmonary sarcoidosis.JAMA 1973;223:688.
6 Fogh J, Bertelsen SV, Schmidt A. Diagnostic value of 67Gascintigraphy in chest surgery. Thorax 1974;29:26-31.
7Heshiki A, Schatz SL, McKusick KA, Bowersox DW,Singh Soin J, Wagner HN. Gallium-67 citrate scanningin patients with pulmonary sarcoidosis. Am J Roentgenol1974;122:744-9.
8 Kinoshita F, Ushio T, Maekawa A, Ariwa R, Kubo A.Scintiscanning of pulmonary diseases with 67Ga-citrate.J Nucl Med 1974;15:227-33.
9 Galassi A. Experiences de scintigraphies pulmonairesavec le gallium 67. Bronches 1975;25:240-55.
10 Schermuly VW, Behrend J, Pohls PH. Die 67Ga Szinti-graphie bei der Sarkoidose. Fortschr Roentgenstr 1975;122:54-62.
Israel HL, Park CH, Mansfield CM. Gallium scanning insarcoidosis. Ann NY Acad Sci 1976;278:514-6.
12 Niden AH, Mishkin FS. 67Gallium citrate lung scans ininterstitial lung disease. Chest 1976;69:266-8.
13 Mishkin FS, Tanaka TT, Niden AH. Abnormal galliumscan patterns of the salivary gland in pulmonarysarcoidosis. Ann Intern Med 1978;89:933-5.
14 Siemsen JK, Grebe SF, Sargent EN, Wentz D. Gallium-67scintigraphy of pulmonary diseases as a complement toradiography. Radiology 1976;118:371-5.
11 Nosal, A. Schleissner LA, Mishkin FS, Lieberman J.Angiotensin-l-converting enzyme and gallium scan innoninvasive evaluation of sarcoidosis. Ann Intern Med1979 ;90:328-3 1.
16 Herry JY, Beaumont D, Moisan A, Larzul JJ, Le Jeune JJ,de Labarthe B. Interpretation de la scintigraphie auGallium 67 dans la sarcoidose. J Biophys Med Nucl1980;4:293-7.
17 Gupta SM, Sziklas JJ, Spencer RP, Rosenberg R. Signifi-cance of diffuse pulmonary uptake in radiogalliumscans. J Nucl Med 1980;21:328-32.
18 Cushman DW, Cheung HS. Spectrophotometric assay a,ndproperties of the angiotensin-converting enzyme ofrabbit lung. Biochem Pharmacol 1971 ;20:1637-48.
19 Le Treut A, Couliou H, Delbary M, Larzul JJ, de LabartheB, Le Gall JY. Le dosage de l'enzyme de conversion del'angiotensine I par methode spectrophotom6trique.Clin Chim Acta 1979;98:1-4.
20 Reynolds HY, Fulmer JD, Kazmierowski JA, RobertsWC, Frank MM, Crystal RG. Analysis of cellular andprotein content of BAL from patients with idiopathicpulmonary fibrosis and chronic hypersensitivity pneumo-nitis. J Clin Invest 1977;59:165-75.
21 Larson SM, Hoffer PB. Normal patterns of localization.In: Hoffer PB, Bekerman C, Henkin RE, eds.Gallium-67 Imaging. New York: John Wiley and Sons,1978.
22 Siemsen JK, Grebe SF, Waxman AD. The use of Gallium-67 in pulmonary disorders. Semin Nucl Med 1978;8:235-49.
23 Herry JY, Beaumont D, Bourguet P et al. Comparison ofdata from gallium-67 scintigraphy and thoracic radi-ography in the assessment of mediastinal and pulmonary
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from

Beaumont, Herry, Sapene, Bourguet, Larzul, de Labarthe
sarcoidosis. In: Medical Radionuclide Imaging (Proc IntSymposium Heidelberg 1980) IAEA-SM-247/145: 507-13.
24 de Labarthe B, Beaumont D, Larzul JJ et al. Angiotensin-converting enzyme, gallium-67 scintigraphy andbroncho-alveolar lavage in the evaluation of mediastinaland pulmonary sarcoidosis. Proc 3rd European Con-ference on Sarcoidosis and Other GranulomatousDisorders, Novi Sad, 22-24 May 1980.
25 Mitchell DN, Scadding JG. Sarcoidosis. Am Rev RespirDis 1974;110:774-802.
26 Mishkin FS, Maynard WP. Lacrimal gland accumulationof 67Ga. J Nucl Med 1974;15:630-1.
27 Bekerman C, Hoffer PB, Bitran JD, Gupta RG. Gallium-67citrate imaging studies of the lung. Semiin Nucl Med 1980;10:286-301.
28 Line BR, Fulmer JD, Reyniolds HY et al. Gallium-67citrate scanning in the staging of idiopathic pulmonaryfibrosis: correlation with physiologic and morphologicfeatures and bronchoalveolar lavage. Am Rev Respir Dis1978 ;118-2:355-65.
29 Siemsen JK, Sargent EN, Grebe SF, Winsor DW, WentzD, Jacobson G. Pulmonary concentration of Ga-67 inpneumoconiosis. Am J Roentgenol 1974;120:815-20.
30 Groonhagen-Riska C, Kurppa K, Fyhrquist F, Selroos 0.
Angiotensin converting enzyme and lysozyme in silicosisand asbestosis. Scand J Respir Dis 1978;59:228-31.
31 De Remee RA, Rohrbach MS. Serum angiotensin con-verting-enzyme in evaluating the clinical course ofsarcoidosis. Ann Intern Med 1980;92:361-5.
32 Larzul JJ, Letreut A, Couliou H, Beaumont D, DelavalPH, Sapene M, de Labarthe B. Taux serique de l'enzymede conversion de l'angiotensine dans la sarcoidose.Nouv Presse Med 1981;9:675-8.
33 Crystal RG, Roberts WC, Hunninghake GW, Gadek JE,Fulmer JD, Line BR. Pulmonary sarcoidosis: a diseasecharacterized and perpetuated by activated lungT-lymphocytes. Ann Intern Med 1981;94:73-94.
34 Gupta RG, Bekerman C, Sicilian L, Oparil S, Szidon JP.Gallium-67 citrate scanning and serum angiotensinconverting-enzyme levels as indicators of diseaseactivity in sarcoidosis. Clin Res 1979;27:705A (abstr).
35 Gupta RG, Bekerman C, Catchatourian R, Sicilian L,Szidon JP. Relationship between broncho-alveolarcellular analysis and 67Gallium citrate uptake insarcoidosis. Clin Res 1979;27:662A (abstr).
36 MIRD-Dose estimate report 2, summary of currentradiation dose estimates to humans from 66Ga, 67Ga and72Ga-citrate. J Nucl Med 1973 ;14:755.
3 Nelson B, Hayes RL, Edwards CL, Kniseley RM,Andrews GA. Distribution of gallium in human tissuesafter intravenous administration. J Nucl Med 1972;13:92-100.
18
copyright. on D
ecember 26, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.37.1.11 on 1 January 1982. D
ownloaded from