forward looking statements 2013 accomplishments november1 2014 forward looking statements2013...
TRANSCRIPT
20 NOVEMBER 2014
2013 Accomplishments Forward Looking Statements
This presentation contains forward-looking statements that involve substantial risks and uncertainties. All statements, other than statements of historical facts, contained in this presentation, including statements regarding our strategy, future operations, prospects, plans and objectives of management, are forward-looking statements. The words ‘‘anticipate,’’ ‘‘believe,’’ ‘‘estimate,’’ ‘‘expect,’’ ‘‘intend,’’ ‘‘may,’’ ‘‘plan,’’ ‘‘predict,’’ ‘‘project,’’ ‘‘target,’’ ‘‘potential,’’ ‘‘will,’’ ‘‘would,’’ ‘‘could,’’ ‘‘should,’’ ‘‘continue,’’ and similar expressions are intended to identify forward-looking statements, although not all forward-looking statements contain these identifying words. We may not actually achieve the plans, intentions or expectations disclosed in our forward-looking statements, and you should not place undue reliance on our forward-looking statements. Actual results may differ materially from those indicated by such forward-looking statements as a result of various important factors, including: uncertainties inherent in the initiation of future clinical studies, expectations of expanding ongoing clinical studies, availability and timing of data from ongoing clinical studies, whether interim results from a clinical trial will be predictive of the final results of the trial or results of early clinical studies will be indicative of the results of future studies, expectations for regulatory approvals, development progress of the Company’s companion diagnostics, availability of funding sufficient for the Company’s foreseeable and unforeseeable operating expenses and capital expenditure requirements, other matters that could affect the financial performance of the Company, other matters that could affect the availability or commercial potential of the Company’s therapeutic candidates or companion diagnostics and other factors discussed in the "Risk Factors" section of the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 6, 2014.
1
Phase 1 first-in-human study of the enhancer of zeste-homolog 2 (EZH2)
histone methyl transferase inhibitor E7438 as a single agent in patients with advanced
solid tumors or B cell lymphoma V Ribrag,1 JC Soria,1 L Reyderman,2 R Chen,2
P Salazar,3 N Kumar,4 G Kuznetsov,4 H Keilhack,5 LH Ottesen,3 A Italiano6
1Institut Gustave Roussy, Villejuif, France; 2Eisai Inc., NJ, USA; 3Eisai Ltd., Hatfield, UK;
4Eisai Inc., Andover, MA, USA; 5Epizyme Inc., MA, USA; 6Institut Bergonié, Centre de Lutte Contre le Cancer de Bordeaux, Bordeaux, France;
2
Disclosures
• VR: Advisory board, Eisai Inc. • JCS: Nothing to disclose. • AI: Honoraria–GlaxoSmithKline, Pfizer,
PHarmaMar; Threshold Research Funding–Novartis, Pfizer, PharmaMar, Roche.
• LR, RC, PS, NK, GK, and LHO are employees of Eisai Inc.
• HK is an employee of Epizyme Inc.
3
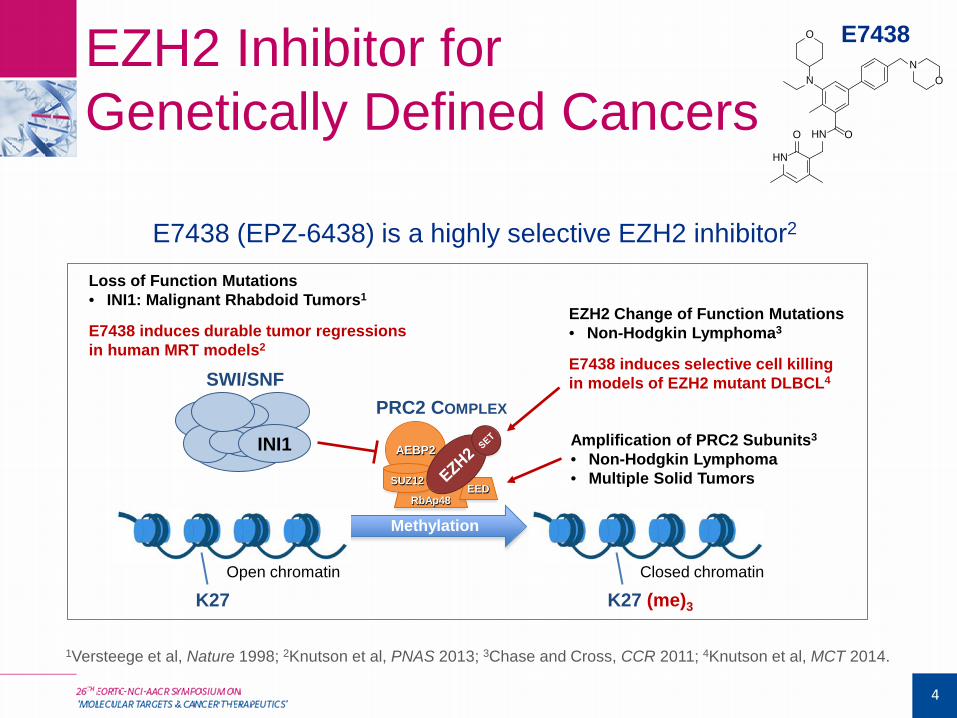
EZH2 Inhibitor for Genetically Defined Cancers
4
HN O
HN
O
NON
O E7438
E7438 (EPZ-6438) is a highly selective EZH2 inhibitor2
INI1
Loss of Function Mutations • INI1: Malignant Rhabdoid Tumors1
E7438 induces durable tumor regressions in human MRT models2
SWI/SNF
PRC2 COMPLEX
EZH2 Change of Function Mutations • Non-Hodgkin Lymphoma3
E7438 induces selective cell killing in models of EZH2 mutant DLBCL4
Amplification of PRC2 Subunits3
• Non-Hodgkin Lymphoma
• Multiple Solid Tumors
Methylation
K27 K27 (me)3
Closed chromatin Open chromatin
RbAp48 EED
AEBP2
SUZ12
1Versteege et al, Nature 1998; 2Knutson et al, PNAS 2013; 3Chase and Cross, CCR 2011; 4Knutson et al, MCT 2014.
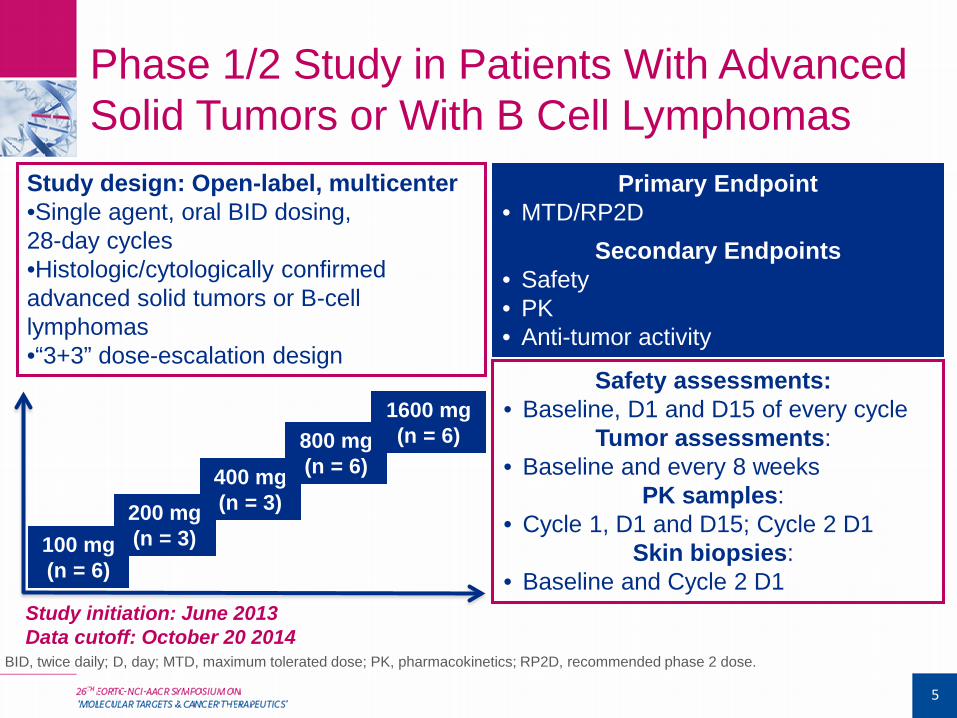
Phase 1/2 Study in Patients With Advanced Solid Tumors or With B Cell Lymphomas
Study design: Open-label, multicenter •Single agent, oral BID dosing, 28-day cycles •Histologic/cytologically confirmed advanced solid tumors or B-cell lymphomas •“3+3” dose-escalation design
Study initiation: June 2013 Data cutoff: October 20 2014
100 mg (n = 6)
200 mg (n = 3)
400 mg (n = 3)
800 mg (n = 6)
1600 mg (n = 6)
Primary Endpoint • MTD/RP2D
Secondary Endpoints • Safety • PK • Anti-tumor activity
Safety assessments: • Baseline, D1 and D15 of every cycle
Tumor assessments: • Baseline and every 8 weeks
PK samples: • Cycle 1, D1 and D15; Cycle 2 D1
Skin biopsies: • Baseline and Cycle 2 D1
5
BID, twice daily; D, day; MTD, maximum tolerated dose; PK, pharmacokinetics; RP2D, recommended phase 2 dose.
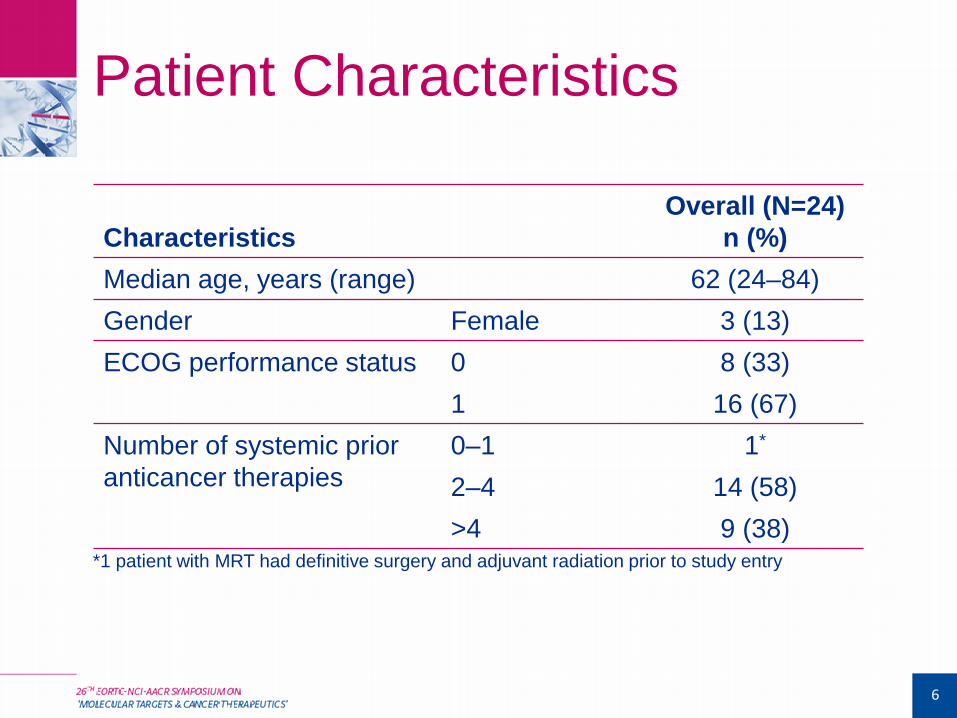
Patient Characteristics
Characteristics Overall (N=24)
n (%) Median age, years (range) 62 (24–84) Gender Female 3 (13) ECOG performance status 0 8 (33)
1 16 (67) Number of systemic prior anticancer therapies
0–1 1*
2–4 14 (58) >4 9 (38)
*1 patient with MRT had definitive surgery and adjuvant radiation prior to study entry
6
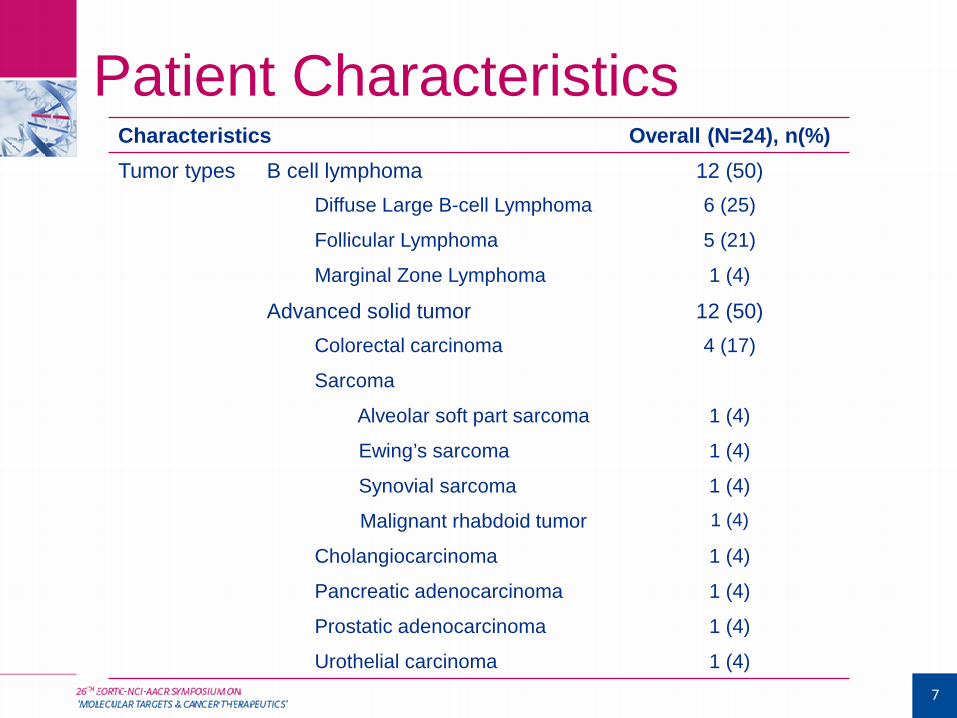
Patient Characteristics Characteristics Overall (N=24), n(%) Tumor types B cell lymphoma 12 (50)
Diffuse Large B-cell Lymphoma 6 (25)
Follicular Lymphoma 5 (21)
Marginal Zone Lymphoma 1 (4)
Advanced solid tumor 12 (50) Colorectal carcinoma 4 (17)
Sarcoma
Alveolar soft part sarcoma 1 (4)
Ewing’s sarcoma 1 (4)
Synovial sarcoma 1 (4)
Malignant rhabdoid tumor 1 (4)
Cholangiocarcinoma 1 (4)
Pancreatic adenocarcinoma 1 (4)
Prostatic adenocarcinoma 1 (4)
Urothelial carcinoma 1 (4) 7
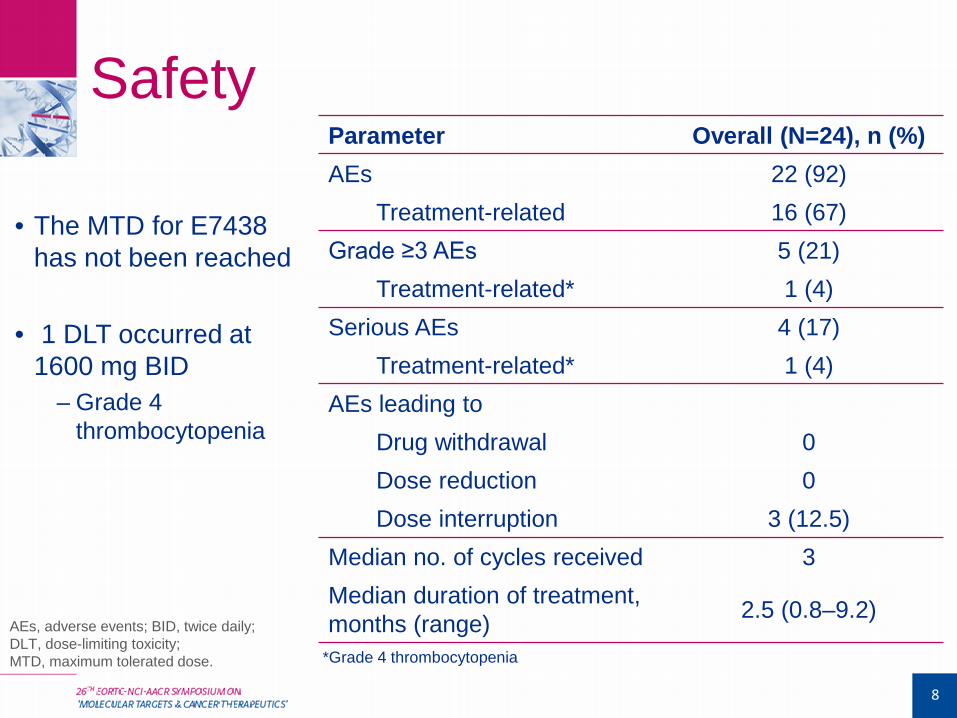
Safety Parameter Overall (N=24), n (%) AEs 22 (92)
Treatment-related 16 (67) Grade ≥3 AEs 5 (21)
Treatment-related* 1 (4) Serious AEs 4 (17)
Treatment-related* 1 (4) AEs leading to
Drug withdrawal 0 Dose reduction 0 Dose interruption 3 (12.5)
Median no. of cycles received 3 Median duration of treatment, months (range) 2.5 (0.8–9.2)
8
• The MTD for E7438 has not been reached
• 1 DLT occurred at
1600 mg BID – Grade 4
thrombocytopenia
AEs, adverse events; BID, twice daily; DLT, dose-limiting toxicity; MTD, maximum tolerated dose. *Grade 4 thrombocytopenia
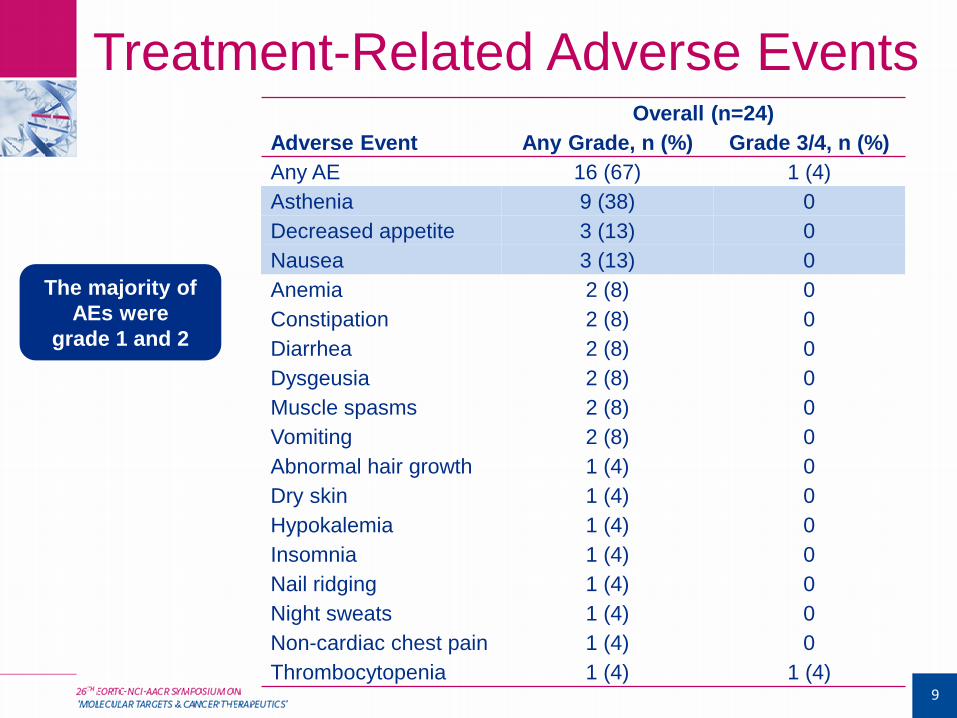
Treatment-Related Adverse Events Overall (n=24)
Adverse Event Any Grade, n (%) Grade 3/4, n (%) Any AE 16 (67) 1 (4) Asthenia 9 (38) 0 Decreased appetite 3 (13) 0 Nausea 3 (13) 0 Anemia 2 (8) 0 Constipation 2 (8) 0 Diarrhea 2 (8) 0 Dysgeusia 2 (8) 0 Muscle spasms 2 (8) 0 Vomiting 2 (8) 0 Abnormal hair growth 1 (4) 0 Dry skin 1 (4) 0 Hypokalemia 1 (4) 0 Insomnia 1 (4) 0 Nail ridging 1 (4) 0 Night sweats 1 (4) 0 Non-cardiac chest pain 1 (4) 0 Thrombocytopenia 1 (4) 1 (4)
9
The majority of AEs were
grade 1 and 2
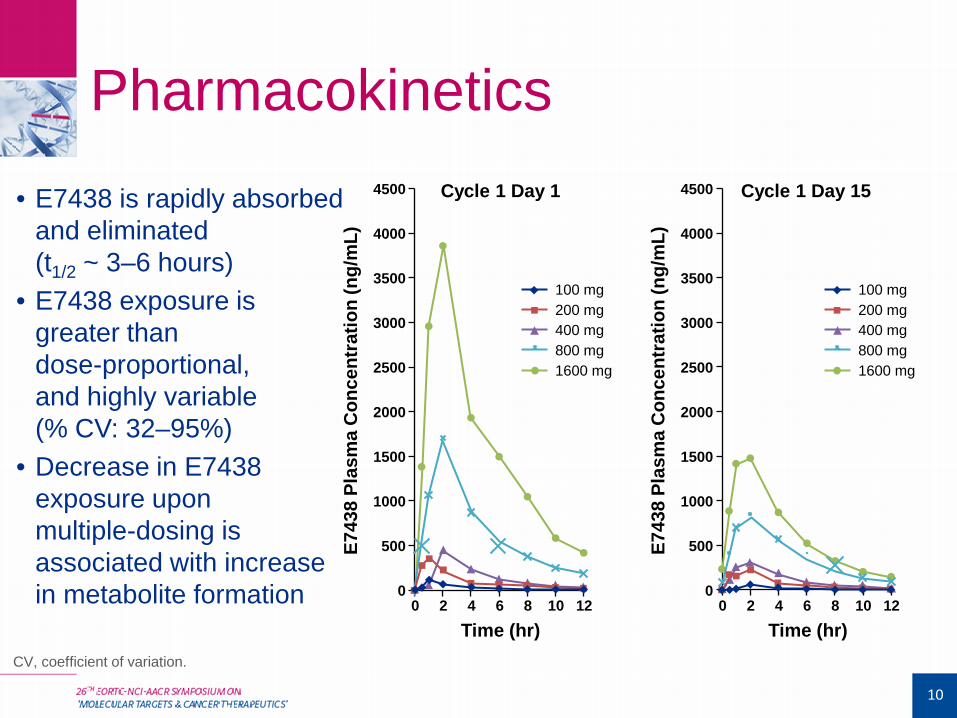
Pharmacokinetics • E7438 is rapidly absorbed
and eliminated (t1/2 ~ 3–6 hours)
• E7438 exposure is greater than dose-proportional, and highly variable (% CV: 32–95%)
• Decrease in E7438 exposure upon multiple-dosing is associated with increase in metabolite formation
Cycle 1 Day 1
Time (hr)
E743
8 Pl
asm
a C
once
ntra
tion
(ng/
mL)
0 0 2 4 6 8 10 12
500
1000
1500
2000
2500
3500
4500
4000
3000
100 mg 200 mg 400 mg 800 mg 1600 mg
Cycle 1 Day 15
Time (hr) E7
438
Plas
ma
Con
cent
ratio
n (n
g/m
L)
0 0 2 4 6 8 10 12
500
1000
1500
2000
2500
3500
4500
4000
3000
100 mg 200 mg 400 mg 800 mg 1600 mg
10
CV, coefficient of variation.
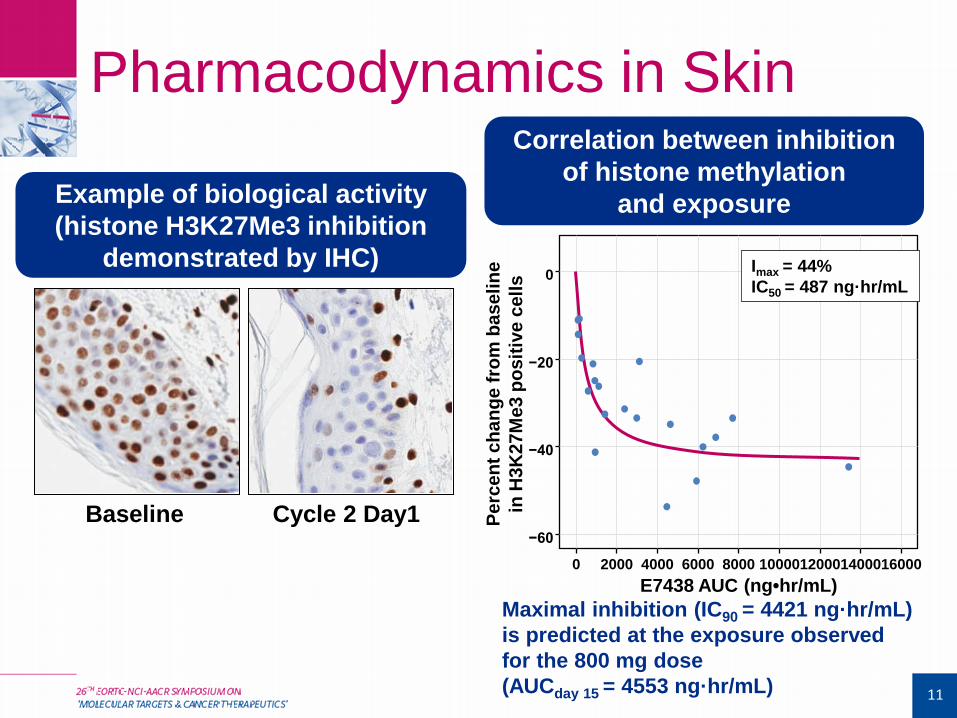
Pharmacodynamics in Skin
Maximal inhibition (IC90 = 4421 ng·hr/mL) is predicted at the exposure observed for the 800 mg dose (AUCday 15 = 4553 ng·hr/mL)
Perc
ent c
hang
e fr
om b
asel
ine
in
H3K
27M
e3 p
ositi
ve c
ells
0
−20
−40
−60
E7438 AUC (ng•hr/mL) 16000 14000 12000 10000 8000 6000 4000 2000 0
Imax = 44% IC50 = 487 ng·hr/mL
Example of biological activity (histone H3K27Me3 inhibition
demonstrated by IHC)
11
Correlation between inhibition of histone methylation
and exposure
Baseline Cycle 2 Day1
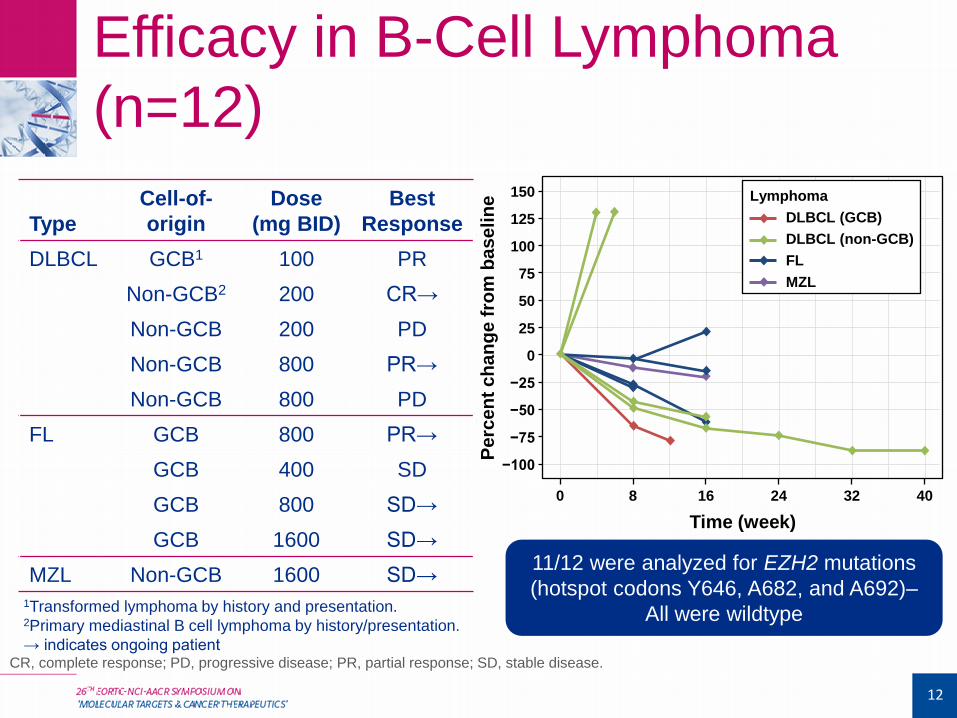
Efficacy in B-Cell Lymphoma (n=12)
12
1Transformed lymphoma by history and presentation. 2Primary mediastinal B cell lymphoma by history/presentation. → indicates ongoing patient
Type Cell-of-origin
Dose (mg BID)
Best Response
DLBCL GCB1 100 PR Non-GCB2 200 CR→ Non-GCB 200 PD Non-GCB 800 PR→ Non-GCB 800 PD
FL GCB 800 PR→ GCB 400 SD GCB 800 SD→ GCB 1600 SD→
MZL Non-GCB 1600 SD→
Perc
ent c
hang
e fr
om b
asel
ine
75
50
25
0
125
100
150
−50
−75
−100
−25
0
Time (week) 8 16 24 32 40
Lymphoma DLBCL (GCB) DLBCL (non-GCB) FL MZL
11/12 were analyzed for EZH2 mutations (hotspot codons Y646, A682, and A692)–
All were wildtype
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease.
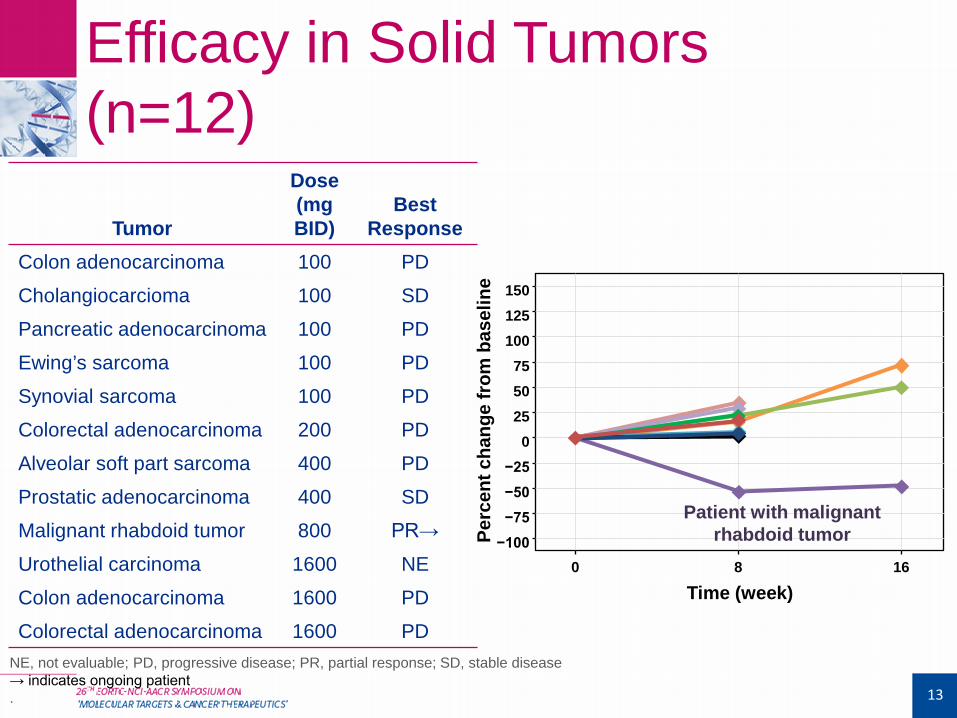
Efficacy in Solid Tumors (n=12)
13
Time (week)
Perc
ent c
hang
e fr
om b
asel
ine
75 50 25 0
125 100
150
−50 −75 −100
−25
8 0 16
Patient with malignant rhabdoid tumor
Tumor
Dose (mg BID)
Best Response
Colon adenocarcinoma 100 PD
Cholangiocarcioma 100 SD
Pancreatic adenocarcinoma 100 PD
Ewing’s sarcoma 100 PD
Synovial sarcoma 100 PD
Colorectal adenocarcinoma 200 PD
Alveolar soft part sarcoma 400 PD
Prostatic adenocarcinoma 400 SD
Malignant rhabdoid tumor 800 PR→
Urothelial carcinoma 1600 NE
Colon adenocarcinoma 1600 PD
Colorectal adenocarcinoma 1600 PD NE, not evaluable; PD, progressive disease; PR, partial response; SD, stable disease → indicates ongoing patient .
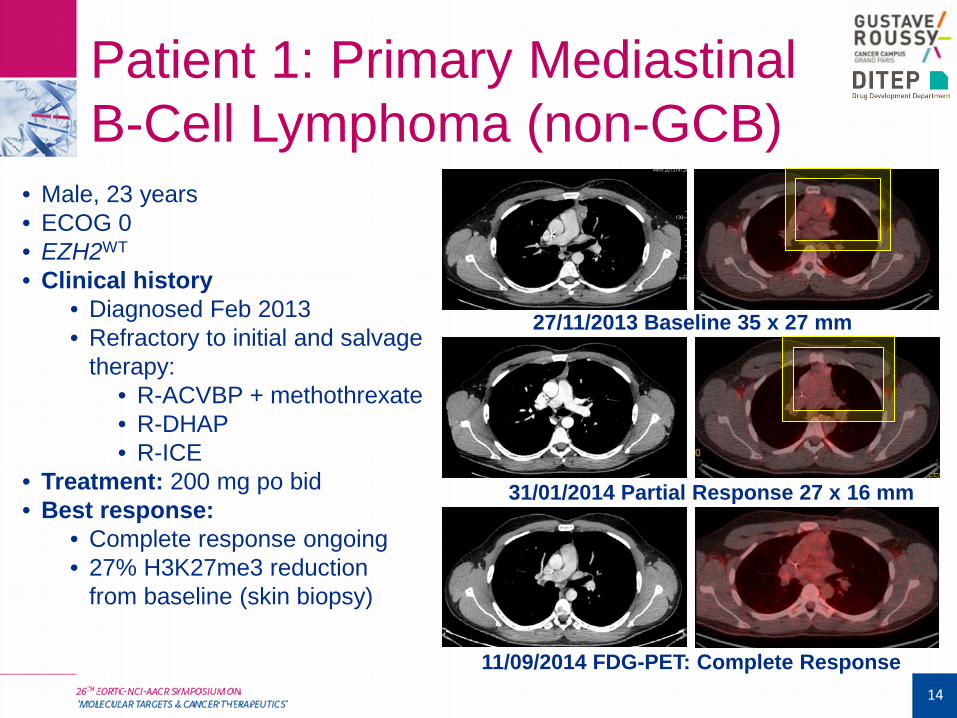
11/09/2014 FDG-PET: Complete Response
27/11/2013 Baseline 35 x 27 mm
31/01/2014 Partial Response 27 x 16 mm
Patient 1: Primary Mediastinal B-Cell Lymphoma (non-GCB)
14
• Male, 23 years • ECOG 0 • EZH2WT
• Clinical history • Diagnosed Feb 2013 • Refractory to initial and salvage
therapy: • R-ACVBP + methothrexate • R-DHAP • R-ICE
• Treatment: 200 mg po bid • Best response:
• Complete response ongoing • 27% H3K27me3 reduction
from baseline (skin biopsy)
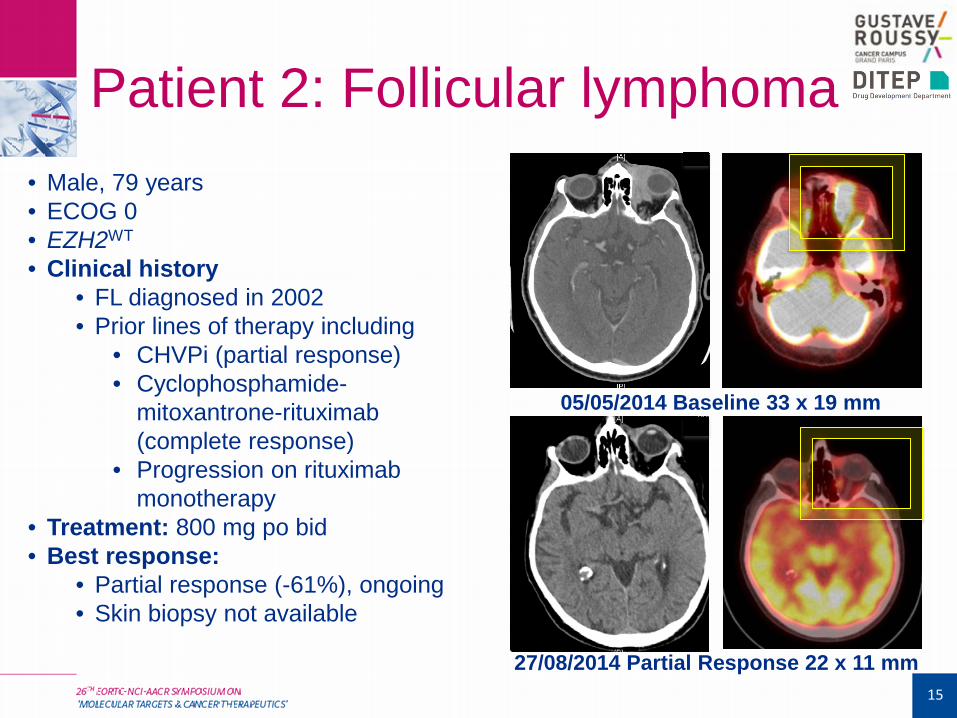
05/05/2014 Baseline 33 x 19 mm
27/08/2014 Partial Response 22 x 11 mm
Patient 2: Follicular lymphoma
15
• Male, 79 years • ECOG 0 • EZH2WT
• Clinical history • FL diagnosed in 2002 • Prior lines of therapy including
• CHVPi (partial response) • Cyclophosphamide-
mitoxantrone-rituximab (complete response)
• Progression on rituximab monotherapy
• Treatment: 800 mg po bid • Best response:
• Partial response (-61%), ongoing • Skin biopsy not available
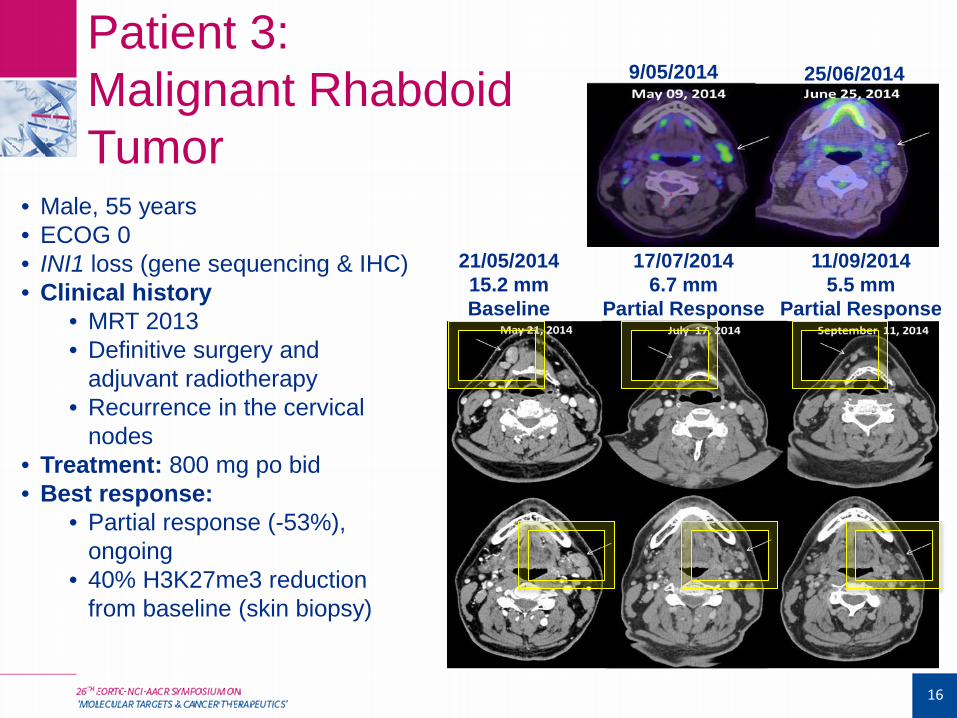
Patient 3: Malignant Rhabdoid Tumor
16
21/05/2014 15.2 mm Baseline
17/07/2014 6.7 mm
Partial Response
11/09/2014 5.5 mm
Partial Response
• Male, 55 years • ECOG 0 • INI1 loss (gene sequencing & IHC)
• Clinical history • MRT 2013 • Definitive surgery and
adjuvant radiotherapy • Recurrence in the cervical
nodes • Treatment: 800 mg po bid • Best response:
• Partial response (-53%), ongoing
• 40% H3K27me3 reduction from baseline (skin biopsy)
9/05/2014 25/06/2014
Conclusions
17
• The emerging Phase I safety profile is acceptable • MTD not reached, no treatment discontinuation for toxicity,
limited grade 3/4 toxicity
• Acceptable PK profile and confirmed dose-related target engagement in skin
• This trial is the first demonstration of clinical activity associated with EZH2 inhibition • Encouraging activity of E7438 was shown in B-cell NHL and
INI1-deficient MRT across a wide dose-range
• Further investigation in B-cell NHL and INI-1 deficient tumours is under discussion
Acknowledgements
The authors thank the patients and their families, as well as the investigators and their teams who took part in this study, and
Dr. Scott Barrett for his contributions.
This study was funded by Eisai Inc.
Editorial support was provided by Oxford PharmaGenesis Inc., and funded by Eisai Inc.
18