foot 23 ankle practice the failed cavovarus foot: what
TRANSCRIPT

© 2016 AAOS Instructional Course Lectures, Volume 65 331
23
Management of the adult cavovarus foot is complex and requires an un-derstanding of not only the etiology of the deformity but also any muscle im-balances occurring about the foot and ankle. The goal of surgical intervention is to attain a plantigrade and balanced foot, which requires a systematic and stepwise treatment algorithm. To ac-complish this, it is important for the surgeon to evaluate if the deformity is flexible or rigid, determine the apex (or, in some feet, apices) of the defor-mity, evaluate any muscle imbalances
occurring about the foot and ankle, and determine if ancillary procedures are necessary. A failure to consider these principles and apply appropriate treat-ment may result in inadequate treatment and recurrence and progression of the deformity.
Treatment of the cavovarus foot be-gins with a thorough evaluation that includes a clinical examination and appropriate radiographic studies. To determine the true extent of the defor-mity, it is important for the surgeon to evaluate patients in both the standing
and seated positions. There is often variation in the extent of the deformity; therefore, it is important for the sur-geon to have a good understanding of its complex three-dimensional nature, including the supinated and varus align-ment of the hindfoot, the plantarflexed medial column, and associated forefoot pronation. A patient’s gait should be ob-served to evaluate for associated muscle weakness, particularly a slight footdrop, and any attempted compensation for this weakness with the toe extensors.
Flexibility of the DeformityWhenever possible, the surgeon should perform osteotomies rather than ar-throdesis. After an osteotomy, the foot will be more flexible, and recuperation will generally be easier and quicker compared with more complex hind-foot arthrodesis procedures. The most common error that surgeons have made over the past decades was pushing the envelope with respect to flexibility and performing an osteotomy in cases in which arthrodesis would have been more appropriate. Unfortunately, be-cause of its historically poor outcomes, arthrodesis has been considered a
The Failed Cavovarus Foot: What Went Wrong and Why?
Jonathan R.M. Kaplan, MDMark S. Myerson, MD
Dr. Myerson or an immediate family member has received royalties from Biomet, DePuy, and Tornier; serves as a paid consultant to or is an employee of Biomet, BioMedical Enterprises, and Tornier; and serves as an unpaid consultant to Tornier. Neither Dr. Kaplan nor any immediate family member has received anything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject of this chapter.
AbstractThe adult cavovarus foot exists on a spectrum and, therefore, requires a thorough evalua-tion to determine the extent of the deformity and then choose from a multitude of surgical procedures to achieve correction. Regardless of the severity of the deformity, treatment should include an algorithmic approach to adequately achieve a stable, balanced, and plantigrade foot. To prevent failure, the surgeon should evaluate whether the deformity is flexible or rigid, determine the location of the apex or apices of the deformity, evaluate any muscle imbalances occurring about the foot and ankle, and determine the need for additional procedures. A failure to consider these principles and, subsequently, the extent of the deformity often results in recurrence and progression of the deformity.
Instr Course Lect 2016;65:331–342.
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

332 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
salvage procedure; however, the poor outcomes may be related to a failure to consider some of the principles of deformity correction, including muscle balance and a plantigrade foot.1-4
Various examination techniques have been used to evaluate the flexibil-ity of the cavovarus foot, including the Coleman block test, a prone examina-tion, and a supine or seated examina-tion.5-7 Coleman and Chestnut5 were the first to describe the Coleman block test, in which a block is placed under the lat-eral column to accommodate the plan-tarflexed first ray. In forefoot-driven cavus, the initial deformity occurs as the peroneus longus overpowers the tibialis anterior, resulting in a plan-tarflexed first ray with subsequent ca-vovarus of the hindfoot. If the varus alignment of the hindfoot corrects with the Coleman block test, then it is considered passively correctable and, in theory, can be treated with an elevation osteotomy of the first metatarsal only. The authors of this chapter, however, have found that this is rarely the case
because the cavovarus foot exists on a spectrum of deformity. Furthermore, the Coleman block test does not reveal the full extent of deformity correction. The authors of this chapter recommend supplementing the Coleman block test with an examination in which the sur-geon manually manipulates the hind-foot of a patient in a seated or prone position. If the varus alignment of the hindfoot is correctable, the heel will easily move into valgus alignment with the foot in equinus7 (Figure 1). The extent of deformity correction can be determined with this examination technique and typically consists of os-teotomies involving both the hindfoot and the forefoot rather than an isolated first metatarsal osteotomy, which may be mistakenly recommended with the use of only the Coleman block test.
Radiographic studies should include AP, oblique, and lateral views of the foot and an AP view of the ankle. Ra-diographic abnormalities include an increased calcaneal pitch, an increased Meary angle, and a decreased Hibbs
angle.8 A hindfoot alignment radio-graph also is beneficial for evaluating the extent of malalignment in the coro-nal plane.9 In addition to these standard radiographic views, weight-bearing radiographs with the Coleman block may be beneficial for radiographically determining the flexibility of the defor-mity (Figure 2).
The flexible cavovarus foot is amenable to motion-sparing surgical corrections that consist of a combina-tion of hindfoot, midfoot, and fore-foot osteotomies in addition to the required tendon transfers. The truly flexible cavovarus foot may not require tendon transfers, but this is not typi-cally the case. In general, the authors of this chapter use a combination of a first metatarsal osteotomy, a calcaneal osteotomy, and a peroneus longus to brevis transfer for milder deformities. With respect to the hindfoot, the cal-caneal osteotomy has traditionally been described as either a lateral slide oste-otomy or a lateral closing wedge osteot-omy.10 Instead, it should be thought of as a three-dimensional osteotomy that consists of a lateral closing wedge oste-otomy combined with a shift both prox-imally and superiorly (Figure 3).11 The closing wedge osteotomy with lateral shift improves the weight-bearing axis of the hindfoot, and the superior shift accommodates the increased calcaneal pitch. The principle of correction is to start proximally and progress distally, beginning with the calcaneal osteotomy and followed by the midfoot and fore-foot osteotomies.
It is essential for the surgeon to recognize the many subtleties of a calcaneal osteotomy, both preoperatively and intraoperatively. As the incision is being made, the surgeon must consider the need for additional procedures, such
Clinical photographs of the hindfoot of a patient in the prone posi-tion. A, The hindfoot is in varus alignment without manipulation or correction of the deformity. B, Manipulation of the hindfoot into valgus alignment demon-strates a flexible deformity.
Figure 1
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

© 2016 AAOS Instructional Course Lectures, Volume 65 333
The Failed Cavovarus Foot: What Went Wrong and Why? Chapter 23
as peroneal tendon repair or transfer and the possibility of lateral ligament reconstruction. As dissection is carried down to bone, the surgeon must take special care to prevent injury to the ad-jacent peroneal tendons and the sural nerve. After dissection down to bone, the surgeon must elevate an adequate amount of periosteum to allow for a wedge of bone to be removed. The authors of this chapter prefer to use a saw to perform the wedge resection, with the first cut made perpendicular to the axis of the calcaneus and at a 45° angle to the tuberosity. In general, the second cut is made at a 20° angle to the first cut; however, the angle can be increased or decreased, depending on the amount of correction required. The varus alignment of the hindfoot should be evaluated intraoperatively, with both direct visualization and flu-oroscopy, to ensure that no overcorrec-tion (with subsequent valgus alignment of the hindfoot) or undercorrection (with persistent varus alignment) oc-curs. Bruce et al12 reported that tarsal tunnel volume is reduced after a lateral calcaneal osteotomy; therefore, pro-phylactic tarsal tunnel release should be considered for patients who require an extensive lateral shift. Finally, it is important for the surgeon to tamp down any laterally overhanging bone that may cause irritation to the peroneal tendons and persistent postoperative symptomatology.
As the calcaneus is moved into val-gus alignment, the eversion produces further plantar flexion of the first metatarsal; therefore, a first metatar-sal dorsiflexion osteotomy should be performed to correct the plantarflexed first ray. While the medial column is plantarflexed, the lateral column is both rotated and adducted, and rotational
malalignment must be addressed to prevent persistent lateral column over-load. It is important for the surgeon to evaluate the forefoot and determine if the deformity is isolated to the first ray or if it affects the entire forefoot. Cavo-varus isolated to the first ray is amenable to correction with a dorsiflexion oste-otomy of the first metatarsal; global cavovarus may require a tarsometa-tarsal truncated-wedge arthrodesis13 or osteotomies at the bases of all the metatarsals.
Apex of the DeformityAlthough motion preservation is de-sirable, an arthrodesis that produces a stable, plantigrade foot is better than a joint-sparing surgery that fails to com-pletely correct the deformity. Therefore, it is necessary for the surgeon to de-termine the apex of the deformity in both the sagittal and coronal planes. In addition to arthrodesis, it is impor-tant that tendon transfers and ancillary procedures are performed, otherwise the procedure is likely to fail.
A, Lateral weight-bearing radiograph of the foot taken without the Coleman block demonstrates an increased calcaneal pitch, a decreased Meary angle, and a decreased talar declination angle. There also is a rotation-al deformity about the midfoot and forefoot, with an elevated medial column and metatarsal stacking. B, Lateral weight-bearing radiograph of the foot taken with the Coleman block placed under the lateral column demonstrates correction of the plantarflexed first ray and some improvement in the cal-caneal pitch, the talar declination angle, and rotational deformity. C, Hind-foot alignment weight-bearing radiograph taken without the Coleman block demonstrates bilateral varus alignment of the hindfoot. D, Hindfoot alignment weight-bearing radiograph taken with the Coleman block placed under the left lateral column demonstrates improvement in hindfoot alignment compared with the contralateral side.
Figure 2
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

334 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
Because it is difficult to appreciate the apex of the deformity with only a clinical examination, radiographs should be taken in both the coronal and sagittal planes. In the sagittal plane, the apex is classified as anterior if it is locat-ed in the midfoot at the intertarsal or tarsometatarsal joints or posterior if it is located in the hindfoot.14 In the coro-nal plane, the apex can occur anywhere along the lateral column.
A midfoot arthrodesis is the best technique to correct an anterior-apex deformity because the deformity is located distal to the transverse tarsal joint and because a triple arthrodesis would fail to address the deformity in
the sagittal plane. Although a midfoot arthrodesis may be more technically challenging, correction is more accu-rate if it is performed at the apex of the deformity. Although multiple tech-niques have been described to correct an anterior-apex deformity, the specific location of the deformity should deter-mine which technique is selected.13,15-17
The Cole midtarsal osteotomy and the Japas osteotomy are options to correct a deformity in which the apex occurs at the midtarsal joint. The Cole midtarsal osteotomy is a dorsal closing wedge osteotomy, in which a wedge of bone is removed from one cut through the cuboid joints and navicular and a
second cut through the cuboid joints and cuneiforms.16 Because the Cole midtarsal osteotomy may result in shortening of the foot,16 the authors of this chapter prefer to use the Japas osteotomy, which is a dorsal wedge osteotomy performed at the navicu-locuneiform and cuboid joints. This technique maintains length, allows for multiplanar correction, and, most im-portantly, is performed at the apex of the deformity.17 It is important for sur-geons who are performing a Japas oste-otomy to resect more bone dorsally and medially; this creates a tapered wedge with minimal to no bone removed from the cuboid and allows for dorsiflexion
Illustrations demonstrate the steps of a calcaneal osteotomy for surgical correction of a flexible cavovarus foot. A, The incision (dashed line) is typically made at a level beneath the peroneal tendons and the sural nerve; how-ever, it should be adjusted based on additional necessary procedures. B, The periosteum is elevated, and retractors are used to protect the adjacent soft tissue. C, A wedge of bone is removed (arrow) from the lateral calcaneus. Inset shows an axial view of the wedge of bone being removed (arrow) from the lateral calcaneus. D, The calcaneal osteotomy is closed, and the tuberosity is simultaneously shifted laterally, proximally, and superiorly (shaded area). The dashed line represents the positioning of the tuberosity before the osteotomy is closed. E, After the osteotomy is secured with an appropriately sized screw, the final position of the tuberosity should be more posterior with an improvement in calcaneal pitch.
Figure 3
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons
© 2016 AAOS Instructional Course Lectures, Volume 65 335
The Failed Cavovarus Foot: What Went Wrong and Why? Chapter 23
medially, dorsal translation, and lateral rotation.14 Although less common, if the apex of the deformity in the sag-ittal plane occurs more distally at the tarsometatarsal joint, it may be more amenable to a Jahss dorsal wedge oste-otomy at the tarsometatarsal joints. The Jahss dorsal wedge osteotomy is similar to a midfoot osteotomy, in that more bone is resected dorsally and medially, which allows for correction of both the cavus and the rotational deformity.13
Triple arthrodesis supplemented by appropriate soft-tissue balancing with tendon transfers is the best technique to correct a deformity in the hindfoot because the deforming forces typically occur distal to the site of the triple arthrodesis. In addition to the stan-dard triple arthrodesis technique that Ryerson described in 1923, other tech-niques, including beak triple arthro-desis, have been used specifically to correct posterior-apex cavovarus de-formities.18-20 To perform a beak triple arthrodesis, the surgeon makes an oste-otomy through the anterior calcaneus and the talar head-neck region to cre-ate a talar beak, which is then used to lock the forefoot under the talus at the level of the navicular. This technique not only improves the cavovarus foot with its apex at the talonavicular joint but also provides additional length to the foot.
Understanding the three- dimensional nature of the cavovarus foot is key be-cause the varus alignment of the hind-foot is corrected with a truncated- wedge resection at the level of the subtalar joint, whereas midfoot rotation is corrected through the transverse tarsal joint. A truncated-wedge resection provides better decompression compared with a triangular-wedge resection because it allows for easier correction of the
deformity, albeit with slight shortening of the foot.
The authors of this chapter prefer to use two incisions to allow for joint preparation and deformity correction as well as for exposure for associated tendon transfers. The authors first per-form a posterior tibial tendon release, which is tagged for later transfer, fol-lowed by a plantar fascia release. For a typical cavovarus deformity, the authors first correct the subtalar joint into 5° of valgus alignment; provisionally fix it with a guide pin; and then correct the transverse tarsal joint with rotation, ab-duction, and dorsiflexion. To correct a more severe deformity in which the apex of the deformity is located directly at the talonavicular joint, the authors use the beak triple arthrodesis tech-nique, in which the navicular is recessed under the head of the talus. The articu-lar surface and the dorsal cortex of the navicular are débrided; a notch is cut in the plantar half of the talar head, and the dorsal half of the talar head is kept intact; and the navicular is slid under the head of the talus. This technique corrects the deformity and preserves the length of the foot without resection of a
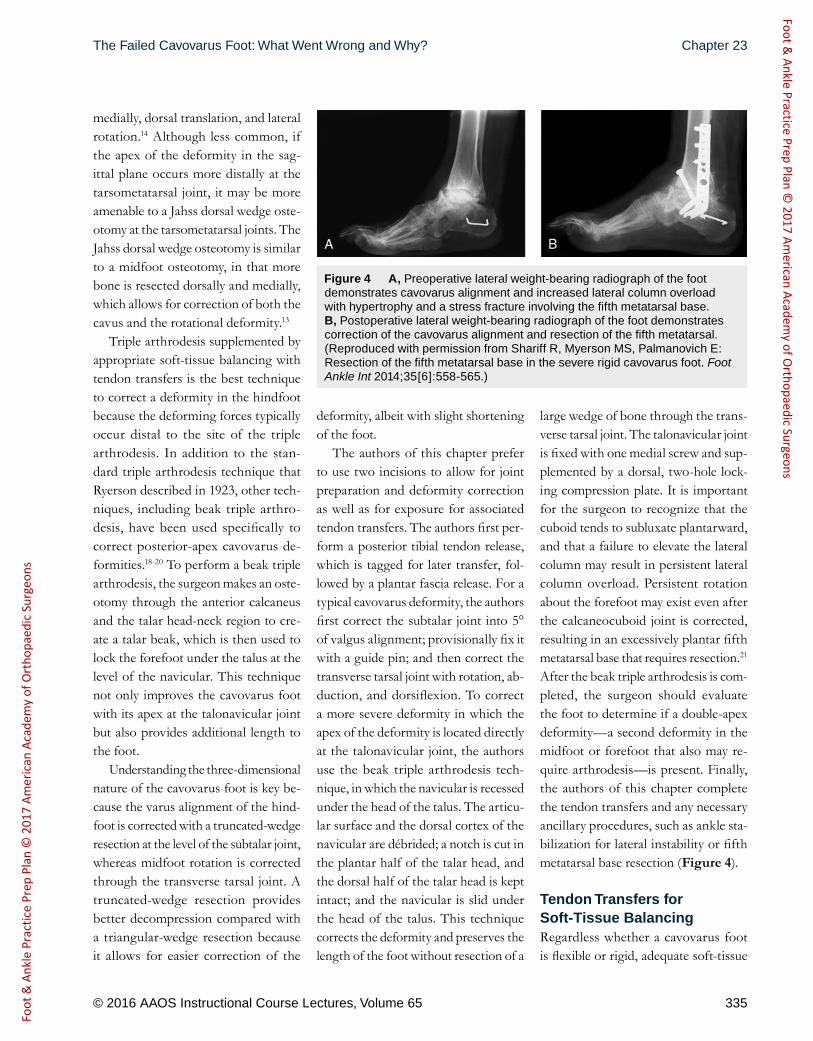
large wedge of bone through the trans-verse tarsal joint. The talonavicular joint is fixed with one medial screw and sup-plemented by a dorsal, two-hole lock-ing compression plate. It is impor tant for the surgeon to recognize that the cuboid tends to subluxate plantarward, and that a failure to elevate the lateral column may result in persistent lateral column overload. Persistent rotation about the forefoot may exist even after the calcaneocuboid joint is corrected, resulting in an excessively plantar fifth metatarsal base that requires resection.21 After the beak triple arthrodesis is com-pleted, the surgeon should evaluate the foot to determine if a double-apex deformity—a second deformity in the midfoot or forefoot that also may re-quire arthrodesis—is present. Finally, the authors of this chapter complete the tendon transfers and any necessary ancillary procedures, such as ankle sta-bilization for lateral instability or fifth metatarsal base resection (Figure 4).
Tendon Transfers for Soft-Tissue BalancingRegardless whether a cavovarus foot is flexible or rigid, adequate soft-tissue
A, Preoperative lateral weight-bearing radiograph of the foot demonstrates cavovarus alignment and increased lateral column overload with hypertrophy and a stress fracture involving the fifth metatarsal base. B, Postoperative lateral weight-bearing radiograph of the foot demonstrates correction of the cavovarus alignment and resection of the fifth metatarsal. (Reproduced with permission from Shariff R, Myerson MS, Palmanovich E: Resection of the fifth metatarsal base in the severe rigid cavovarus foot. Foot Ankle Int 2014;35[6]:558-565.)
Figure 4
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

336 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
balancing with tendon transfers must be performed to achieve a stable, planti-grade foot. As previously discussed, os-seous correction alone does not rectify the underlying cause of the deformity, which is a dynamic muscle imbalance that occurs across the hindfoot, mid-foot, and forefoot.22,23 Traditionally, in Charcot-Marie-Tooth disease, the peroneus longus overpowers the weak tibialis anterior, resulting in a plantar-flexed first ray, and the posterior tibial tendon overpowers the weak peroneus brevis, accentuating the elevated arch
and contributing to the varus alignment of the hindfoot.24,25
To be adequate for transfer, a ten-don should usually have at least grade 4 strength; transfer of a tendon that is not phasic will result in a slight loss of power.26 Tendon transfer not only aug-ments lost function but also removes the force that contributes to the defor-mity. This is best illustrated in a transfer of the posterior tibial tendon, which is frequently the major deforming force in the cavovarus foot. Because the poste-rior tibial tendon has a broad insertion,
inserting on not only the navicular but also more distal secondary attachments, it is important that the tendon is trans-ferred regardless of its exact strength; failure to do so will lead to a recurrence and progression of the deformity be-cause of its insertion distal to the site of arthrodesis. Recurrence and progres-sion of the deformity is common in the treatment of the cavovarus foot because surgeons often mistakenly perceive that a weak posterior tibial tendon will not function as an effective transfer. Although the weak tendon may have only minimal strength, it will still cause recurrent deformity and gradually result in adductovarus of the midfoot.
Transfer of the posterior tibial ten-don not only removes the deforming force but also strengthens the already weak eversion. The exact location of the site for insertion of the posterior tibial tendon depends on the extent of the deformity and the strength of the remaining muscles. For example, in a foot with weak dorsiflexion strength, the posterior tibial tendon can be transferred to the lateral cuneiform to maximize dorsiflexion and to minimize inversion or eversion deformity.27 The cavovarus foot, however, commonly has weak eversion strength as a result of the weak peroneus brevis; therefore, the authors of this chapter recommend a more lateral transfer of the posterior tibial tendon to the cuboid to improve not only dorsiflexion strength but also eversion strength.
The technique used to transfer the posterior tibial tendon is equally impor-tant as the location of the insertion site. Transfer of the posterior tibial tendon through the interosseous membrane is more phasic and may maintain a greater amount of strength than a nonphasic transfer. First described by Watkins
Preoperative AP (A) and lateral (B) radiographs of the foot demonstrate a double-apex deformity. The posterior apex occurs at the transverse tarsal joint, with an increased calcaneal pitch and a decreased talar declination angle. The second apex occurs distally in the midfoot, with increased medial column height compared with lateral column height and an elevated navicular and medial cuneiform, which suggest over-pull of the tibialis anterior. Postoperative AP (C) and lateral (D) radiographs of the foot demonstrate improved alignment. The foot is plantigrade with improved correction of both apex deformities. Note the improved talar declination angle, calcaneal pitch, and plantigrade measurement ratio, with an increase in height from the medial cuneiform to the floor and a decrease in height from the fourth metatarsal base to the floor.
Figure 5
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

© 2016 AAOS Instructional Course Lectures, Volume 65 337
The Failed Cavovarus Foot: What Went Wrong and Why? Chapter 23
et al,28 this technique was modified by Hsu and Hoffer29 to a four-incision technique that allows for effective transfer through less invasive inci-sions. Biomechanically, the interosseous transfer has been shown to provide a greater degree of dorsiflexion compared with subcutaneous transfer; however, this has not been substantiated clinical-ly.27 The Bridle procedure modifies the transfer of the posterior tibial tendon through the interosseous membrane to the dorsum of the foot by adding a dual anastomosis of the tibialis anterior mus-cle and the peroneus longus muscle.30,31 The authors of this chapter often find that an anastomosis is not necessary to
achieve muscle balance and, therefore, prefer interosseous transfer without anastomosis.
The peroneus longus should be transferred to the peroneus brevis via a direct tenodesis between the pero-neus longus and brevis. This not only decreases the plantar flexion on the first ray but also further augments the weak eversion. The peroneus longus typically is sutured to the peroneus brevis in a side-to-side manner; however, if the peroneus brevis is torn substantially, the peroneus longus can be transferred directly to the fifth metatarsal base. If both the peroneus brevis and longus are torn and the surgeon is not able
to transfer the posterior tibial tendon into the cuboid to compensate for lat-eral weakness, then either a transfer of the flexor digitorum longus or a transfer of the flexor hallucis longus to the fifth metatarsal base should be performed.
A failure to recognize subtle changes in the forefoot is another reason that treatment of the cavovarus foot may not succeed. These subtle changes of the forefoot typically consist of clawing of the hallux as well as the lesser toes and occur if the intrinsic muscles are weak and overpowered by the extrinsic mus-cles.32 To correct clawing of the hallux, a modified Jones procedure, in which the extensor hallucis brevis is trans-ferred to the neck of the first metatarsal and the hallux interphalangeal joint is fused, is recommended.33-36 Although less commonly performed, transfer of the flexor hallucis longus to the dorsal aspect of the base of the proximal pha-lanx is an effective technique to cor-rect clawing of the hallux.37,38 Similar
Preoperative AP (A) and lateral (B) radiographs of the foot demonstrate varus alignment of the ankle, a recurrent cavovarus foot after tri-ple arthrodesis without transfer of the posterior tibial tendon, and the develop-ment of ankle arthritis as well as a hypertrophic reaction at the fifth metatarsal base as a result of persistent lateral column overload. Postoperative AP (C) and lateral (D) radiographs of the foot demonstrate improvement in the varus alignment of the ankle, the cavovarus foot, and the plantigrade measurement ratio.
Figure 6
Lateral weight-bearing radiograph of the foot taken after intramedullary screw fixation of a fifth metatarsal base fracture and calcaneal osteotomy to correct varus alignment of the hindfoot. Although screw fixation may be somewhat inadequate, failure likely occurred as a result of persistent lateral column overload, which is evident in the increased plantigrade measurement ratio between the medial cuneiform to floor length and the fourth metatarsal base to floor length.
Figure 7
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

338 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
to the modified Jones procedure, the Hibbs procedure involves transferring the overpowering extensor digitorum longus more proximally to the dorsal aspect of the associated metatarsals.39 For both the modified Jones procedure and the Hibbs procedure, the tendons can be transferred more proximally into the midfoot to the level of the cunei-forms if additional dorsiflexion strength is desired. Similar to hindfoot tendon transfers, the modified Jones procedure
and the Hibbs procedure not only re-move the deforming force but also im-prove dorsiflexion strength.
Ancillary ProceduresThe final step in the algorithmic ap-proach for the treatment of the cavo-varus foot involves recognizing the need for ancillary procedures. In most cavovarus feet, the plantar fascia is con-tracted and requires release; however, in some cavovarus feet, the plantar fascial
contracture may also require release of the abductor hallucis tendon and ab-ductor fascia. The cavovarus foot is commonly associated with contracture of the gastrocnemius-soleus complex, which causes an equinus deformity. To completely appreciate the extent of an equinus contracture deformity, it is important for the surgeon to ex-amine the patient in both the seated and standing positions as well as ex-amine the patient’s gait. The surgeon should also perform the Silfverskiöld test because it can differentiate between an isolated gastrocnemius contracture that requires gastrocnemius recession and a more global contracture of the gastrocnemius- soleus complex that re-quires Achilles tendon lengthening.
Regardless whether a cavovarus foot is flexible or rigid, it is important for the surgeon to evaluate the stability of the lateral ligamentous complex; a failure to address instability may compromise correction of the deformity. Generally, correction of the deformity as previous-ly discussed will alleviate stress on the ankle; however, if the instability of the lateral ligamentous complex is substan-tial, the authors of this chapter perform ligament reconstruction using a modi-fied Chrisman-Snook procedure.40
A cavovarus foot always has an in-creased load along the lateral column. It is important for the surgeon to evaluate the extent of loading because additional procedures may be required to resolve excessive loading, particularly to the fifth metatarsal base. Because the fifth metatarsal rotates under the cuboid in severe deformities, the prominence of the base of the fifth metatarsal will remain despite good correction of the cavovarus foot through the transverse tarsal joint. To avoid excessive pressure and pain, the authors of this chapter
Preoperative AP (A) and lateral (B) weight-bearing radiographs taken after a failed triple arthrodesis demonstrate a persistent cavovarus foot. Undercorrection is evident with an increase in the calcaneal pitch, a decrease in the Meary angle as well as the talar declination angle, and metatarsal stacking with a fifth metatarsal base fracture as a result of persistent lateral column overload. Postoperative AP (C) and lateral (D) weight-bearing radio-graphs of the foot taken after revised triple arthrodesis demonstrate correction of the deformity with improvement in the calcaneal pitch, the talar declination angle, the Meary angle, forefoot rotation, and the plantigrade measurement ratio.
Figure 8
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

© 2016 AAOS Instructional Course Lectures, Volume 65 339
The Failed Cavovarus Foot: What Went Wrong and Why? Chapter 23
recommend resection of the fifth meta-tarsal base.21 Because the peroneus brevis does not function in severe de-formities, removal of the base of the fifth metatarsal will not compromise the outcome of the procedure. If nec-essary and as previously discussed, it is still possible to transfer the peroneus longus to the remaining fascia around the base of the fifth metatarsal.
Case StudiesCase 1: Double-Apex DeformityAn example of a double-apex defor-mity in the sagittal plane is shown in Figure 5, A and B. The patient had both a posterior and an anterior apex, both of which needed to be addressed to achieve a plantigrade foot. Recon-struction involved a triple arthrodesis to address the posterior apex and a first tarsometatarsal arthrodesis to address the anterior apex (Figure 5, C and D). Additional procedures included a tibi-alis anterior tendon transfer to correct the elevated medial column at the mid-foot, Achilles tendon lengthening, and a modified Jones procedure.
Case 2: Failure of Triple Arthrodesis Performed Without Tendon TransferThe patient had progression of a ca-vovarus foot after undergoing a triple arthrodesis performed by an outside physician. Because the original proce-dure was performed without appropri-ate tendon transfers, recurrence of the cavovarus foot and varus alignment of the ankle developed in the patient because of the persistent deforming force from the posterior tibial tendon (Figure 6, A and B). Treatment for this recurrent, progressive deformity required tibiotalocalcaneal arthrodesis
with a concomitant posterior tibial ten-don transfer and a fifth metatarsal base resection (Figure 6, C and D).
Case 3: Persistent Lateral Column OverloadAn outside physician treated a patient with intramedullary screw fixation for a fifth metatarsal base fracture and with a lateral calcaneal sliding osteotomy for varus alignment of the hindfoot. Al-though the patient initially came to the senior author (M.S.M) of this chapter for evaluation of a persistent fifth meta-tarsal base fracture, she was noted to have hardware failure and persistent lateral column overload as a result of undercorrection of the varus alignment (Figure 7).
Case 4: Failed Triple Arthrodesis as a Result of UndercorrectionThe patient whose radiographs are shown in Figure 8, A and B had a persistent cavovarus foot after undergoing a triple arthrodesis per-formed by an outside physician. In this patient, the cavovarus foot persisted be-cause of undercorrection of the defor-mity, causing persistent lateral column overload and a subsequent fifth meta-tarsal base fracture. The treatment re-quired a revised triple arthrodesis with derotation to correct the malalignment, appropriate tendon transfers, and intra-medullary screw fixation of the fifth metatarsal base fracture (Figure 8, C and D).
Preoperative lateral weight-bearing radiographs of the left (A) and right (B) feet demonstrate cavovarus deformities with increased calcaneal pitch, decreased talar declination angles, decreased Meary angles, and varus alignment of the hindfeet, which is evident in the increased visualization of the sinus tarsi and poor visualization of the tibiotalar joint. Postoperative lat-eral weight-bearing radiographs of the left (C) and right (D) feet demonstrate improvement in the cavovarus deformities; however, there is a slight under-correction in the left foot compared with the right foot plus a slight residual increase in the calcaneal pitch and visualization of the sinus tarsi, which sug-gest varus alignment. There also is an increased plantigrade measurement ratio in the left foot compared with the right foot.
Figure 9
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

340 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
Case 5: Derotational Midfoot Osteotomy After Correction of Varus Alignment of the HindfootThe patient underwent a left cavovarus foot reconstruction that consisted of a calcaneal osteotomy, a first metatarsal
osteotomy, plantar fascia release, and a peroneus longus to brevis transfer. At a later date, the patient underwent a right cavovarus foot reconstruction that consisted of a calcaneal osteotomy, a midfoot derotational osteotomy, and plantar fascia release. Although the
preoperative radiographs (Figure 9, A and B) demonstrated a similar sever-ity of varus alignment in both feet, the postoperative radiographs (Figure 9, C and D) demonstrate better correction in the right foot, which is likely a result of the midfoot derotational osteotomy.
Case 6: Inadequate Reconstruction Requiring Triple ArthrodesisThe senior author (M.S.M) of this chapter examined a patient who had undergone a calcaneal osteotomy, a first tarsometatarsal arthrodesis, and osteot-omies of the second through fifth meta-tarsal shafts to correct a cavovarus foot. It was unclear if there was malreduction or malunion of the first tarsometatarsal arthrodesis; however, the procedure re-sulted in flexion of the hallux and sub-sequent elevation of the medial column in the midfoot and contracture of the tibialis anterior tendon (Figure 10, A through C). The treatment required a triple arthrodesis, a lateral transfer of the tibialis anterior, revision of the first tarsometatarsal malunion, and a hallux metatarsophalangeal joint arthrodesis (Figure 10, D and E).
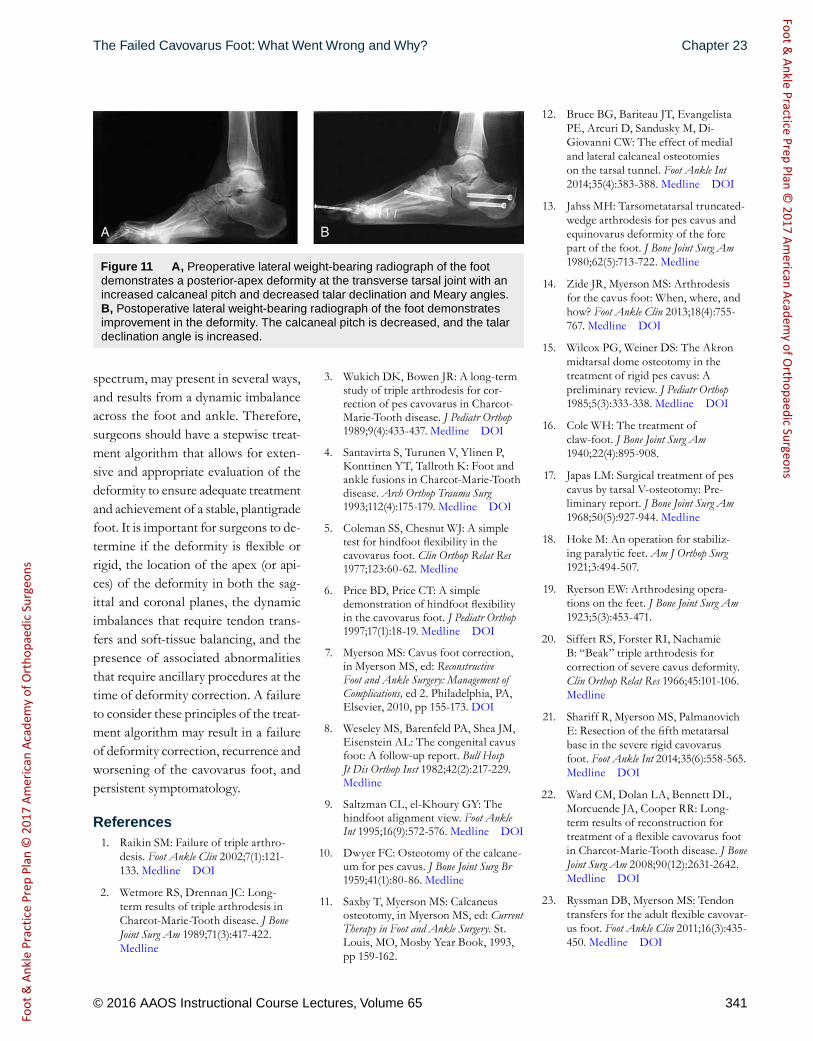
Case 7: Single-Apex Deformity Requiring Calcaneal and Midfoot OsteotomiesThe patient had a flexible, single-apex deformity at the transverse tarsal joint. The treatment required appropriate tendon transfers, plantar fascia release, and both a calcaneal osteotomy and a midfoot osteotomy to achieve a planti-grade foot (Figure 11).
SummaryIt is important for surgeons to recog-nize that the cavovarus foot is a com-plex deformity that exists on a broad
A, Clinical photograph shows a cavovarus foot with plantar flexion of the first ray and subsequent elevation of the medial column at the midfoot. Preoperative AP (B) and lateral (C) radiographs of the foot demonstrate an anterior-apex deformity with flexion at the hallux metatarsophalangeal joint and subsequent elevation of the medial column at the midfoot. Postoperative AP weight-bearing (D) and lateral (E) radiographs demonstrate a plantigrade foot. There is improvement in the midfoot deformity as well as the flexion deformity of the hallux metatarsophalangeal joint. (Panels B through E reproduced with permission from Zide JR, Myerson MS: Arthrodesis for the cavus foot: When, where, and how? Foot Ankle Clin 2013;18[4]:755-767.)
Figure 10
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons
© 2016 AAOS Instructional Course Lectures, Volume 65 341
The Failed Cavovarus Foot: What Went Wrong and Why? Chapter 23
spectrum, may present in several ways, and results from a dynamic imbalance across the foot and ankle. Therefore, surgeons should have a stepwise treat-ment algorithm that allows for exten-sive and appropriate evaluation of the deformity to ensure adequate treatment and achievement of a stable, plantigrade foot. It is important for surgeons to de-termine if the deformity is flexible or rigid, the location of the apex (or api-ces) of the deformity in both the sag-ittal and coronal planes, the dynamic imbalances that require tendon trans-fers and soft-tissue balancing, and the presence of associated abnormalities that require ancillary procedures at the time of deformity correction. A failure to consider these principles of the treat-ment algorithm may result in a failure of deformity correction, recurrence and worsening of the cavovarus foot, and persistent symptomatology.
References1. Raikin SM: Failure of triple arthro-
desis. Foot Ankle Clin 2002;7(1):121-133. Medline DOI
2. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis inCharcot- Marie-Tooth disease. J BoneJoint Surg Am 1989;71(3):417-422.Medline
3. Wukich DK, Bowen JR: A long-termstudy of triple arthrodesis for cor-rection of pes cavovarus in Charcot- Marie-Tooth disease. J Pediatr Orthop1989;9(4):433-437. Medline DOI
4. Santavirta S, Turunen V, Ylinen P,Konttinen YT, Tallroth K: Foot andankle fusions in Charcot-Marie-Toothdisease. Arch Orthop Trauma Surg1993;112(4):175-179. Medline DOI
5. Coleman SS, Chesnut WJ: A simpletest for hindfoot flexibility in thecavovarus foot. Clin Orthop Relat Res1977;123:60-62. Medline
6. Price BD, Price CT: A simpledemonstration of hindfoot flexibilityin the cavovarus foot. J Pediatr Orthop1997;17(1):18-19. Medline DOI
7. Myerson MS: Cavus foot correction,in Myerson MS, ed: ReconstructiveFoot and Ankle Surgery: Management ofComplications, ed 2. Philadelphia, PA,Elsevier, 2010, pp 155-173. DOI
8. Weseley MS, Barenfeld PA, Shea JM,Eisenstein AL: The congenital cavusfoot: A follow-up report. Bull HospJt Dis Orthop Inst 1982;42(2):217-229.Medline
9. Saltzman CL, el-Khoury GY: Thehindfoot alignment view. Foot AnkleInt 1995;16(9):572-576. Medline DOI
10. Dwyer FC: Osteotomy of the calcane-um for pes cavus. J Bone Joint Surg Br1959;41(1):80-86. Medline
11. Saxby T, Myerson MS: Calcaneusosteotomy, in Myerson MS, ed: CurrentTherapy in Foot and Ankle Surgery. St.Louis, MO, Mosby Year Book, 1993,pp 159-162.
12. Bruce BG, Bariteau JT, EvangelistaPE, Arcuri D, Sandusky M, Di-Giovanni CW: The effect of medialand lateral calcaneal osteotomieson the tarsal tunnel. Foot Ankle Int2014;35(4):383-388. Medline DOI
13. Jahss MH: Tarsometatarsal truncated- wedge arthrodesis for pes cavus andequinovarus deformity of the forepart of the foot. J Bone Joint Surg Am1980;62(5):713-722. Medline
14. Zide JR, Myerson MS: Arthrodesisfor the cavus foot: When, where, andhow? Foot Ankle Clin 2013;18(4):755-767. Medline DOI
15. Wilcox PG, Weiner DS: The Akronmidtarsal dome osteotomy in thetreatment of rigid pes cavus: Apreliminary review. J Pediatr Orthop1985;5(3):333-338. Medline DOI
16. Cole WH: The treatment ofclaw-foot. J Bone Joint Surg Am1940;22(4):895-908.
17. Japas LM: Surgical treatment of pescavus by tarsal V-osteotomy: Pre-liminary report. J Bone Joint Surg Am1968;50(5):927-944. Medline
18. Hoke M: An operation for stabiliz-ing paralytic feet. Am J Orthop Surg1921;3:494-507.
19. Ryerson EW: Arthrodesing opera-tions on the feet. J Bone Joint Surg Am1923;5(3):453-471.
20. Siffert RS, Forster RI, NachamieB: “Beak” triple arthrodesis forcorrection of severe cavus deformity.Clin Orthop Relat Res 1966;45:101-106.Medline
21. Shariff R, Myerson MS, PalmanovichE: Resection of the fifth metatarsalbase in the severe rigid cavovarusfoot. Foot Ankle Int 2014;35(6):558-565.Medline DOI
22. Ward CM, Dolan LA, Bennett DL,Morcuende JA, Cooper RR: Long-term results of reconstruction fortreatment of a flexible cavovarus footin Charcot-Marie-Tooth disease. J BoneJoint Surg Am 2008;90(12):2631-2642.Medline DOI
23. Ryssman DB, Myerson MS: Tendontransfers for the adult flexible cavovar-us foot. Foot Ankle Clin 2011;16(3):435-450. Medline DOI
A, Preoperative lateral weight-bearing radiograph of the foot demonstrates a posterior-apex deformity at the transverse tarsal joint with an increased calcaneal pitch and decreased talar declination and Meary angles. B, Postoperative lateral weight-bearing radiograph of the foot demonstrates improvement in the deformity. The calcaneal pitch is decreased, and the talar declination angle is increased.
Figure 11
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons

342 © 2016 AAOS Instructional Course Lectures, Volume 65
Foot and Ankle
24. Mann RA, Missirian J: Pathophysiol-ogy of Charcot-Marie-Tooth disease.Clin Orthop Relat Res 1988;234:221-228. Medline
25. Alexander IJ, Johnson KA: Assess-ment and management of pes cavusin Charcot-Marie-tooth disease. ClinOrthop Relat Res 1989;246:273-281.Medline
26. Jeng C, Myerson M: The uses oftendon transfers to correct paralyt-ic deformity of the foot and ankle.Foot Ankle Clin 2004;9(2):319-337.Medline DOI
27. Goh JC, Lee PY, Lee EH, Bose K:Biomechanical study on tibialis poste-rior tendon transfers. Clin Orthop RelatRes 1995;319:297-302. Medline
28. Watkins MB, Jones JB, Ryder CT Jr,Brown TH Jr: Transplantation of theposterior tibial tendon. J Bone Joint SurgAm 1954;36(6):1181-1189. Medline
29. Hsu JD, Hoffer MM: Posterior tibialtendon transfer anteriorly through theinterosseous membrane: A modifica-tion of the technique. Clin Orthop RelatRes 1978;131:202-204. Medline
30. Rodriguez RP: The Bridle procedurein the treatment of paralysis of thefoot. Foot Ankle 1992;13(2):63-69.Medline DOI
31. Richardson DR, Gause LN: Thebridle procedure. Foot Ankle Clin2011;16(3):419-433. Medline DOI
32. Olson SL, Ledoux WR, Ching RP,Sangeorzan BJ: Muscular imbalancesresulting in a clawed hallux. Foot AnkleInt 2003;24(6):477-485. Medline
33. Giannini S, Girolami M, Ceccarelli F,Maffei G: Modified Jones operationin the treatment of pes cavovarus. ItalJ Orthop Traumatol 1985;11(2):165-170.Medline
34. de Palma L, Colonna E, TravasiM: The modified Jones procedurefor pes cavovarus with claw hallux.J Foot Ankle Surg 1997;36(4):279-283.Medline DOI
35. Jones R III: The Soldier’s foot and thetreatment of common deformities ofthe foot. Br Med J 1916;1(2891):749-753. Medline DOI
36. Breusch SJ, Wenz W, Döderlein L:Function after correction of a clawedgreat toe by a modified RobertJones transfer. J Bone Joint Surg Br2000;82(2):250-254. Medline DOI
37. Kadel NJ, Donaldson-Fletcher EA,Hansen ST, Sangeorzan BJ: Alterna-tive to the modified jones procedure:Outcomes of the flexor hallucis longus(FHL) tendon transfer procedure forcorrection of clawed hallux. Foot AnkleInt 2005;26(12):1021-1026. Medline
38. Steensma MR, Jabara M, AndersonJG, Bohay DR: Flexor hallucis longustendon transfer for hallux claw toedeformity and vertical instability ofthe metatarsophalangeal joint. FootAnkle Int 2006;27(9):689-692. Medline
39. Hibbs RA: An operation for “clawfoot.” JAMA 1919;73(21):1583-1585.DOI
40. Acevedo JI, Myerson MS: Mod-ification of the Chrisman-Snooktechnique. Foot Ankle Int2000;21(2):154-155. Medline
Foot
& A
nkle
Pra
ctic
e Pr
ep P
lan
© 2
017
Amer
ican
Aca
dem
y of
Ort
hopa
edic
Sur
geon
sFoot &
Ankle Practice Prep Plan © 2017 Am
erican Academy of O
rthopaedic Surgeons