fmri abnormalities in dorsolateral prefrontal cortex during a working memory task in manic, euthymic...
TRANSCRIPT

Psychiatry Research: Neuroimaging 182 (2010) 22–29
Contents lists available at ScienceDirect
Psychiatry Research: Neuroimaging
j ourna l homepage: www.e lsev ie r.com/ locate /psychresns
fMRI abnormalities in dorsolateral prefrontal cortex during a working memory taskin manic, euthymic and depressed bipolar subjects
Jennifer Townsenda, Susan Y. Bookheimera, Lara C. Foland–Rossb, Catherine A. Sugarc,d, Lori L. Altshulera,e,⁎aDepartment of Psychiatry and Biobehavioral Sciences, UCLA School of Medicine, Los Angeles, CA, United StatesbLaboratory of NeuroImaging, Department of Neurology, UCLA School of Medicine, Los Angeles, CA, United StatescDepartment of Biostatistics, School of Public Health, University of California, Los Angeles, CA, United StatesdJane and Terry Semel Institute of Neuroscience and Human Behavior, University of California, Los Angeles, United StateseDepartment of Psychiatry, VA Greater Los Angeles Healthcare System, West Los Angeles Healthcare Center, United States
⁎ Corresponding author. 300 UCLA Medical Plaza, SuiteCA 90095-7057, United States. Tel.: +1 310 794 9911; fax
E-mail address: [email protected] (L.L. Alt
0925-4927/$ – see front matter © 2010 Elsevier Irelanddoi:10.1016/j.pscychresns.2009.11.010
a b s t r a c t
a r t i c l e i n f oArticle history:Received 29 October 2008Received in revised form 5 October 2009Accepted 22 November 2009
Keywords:Bipolar disorderDorsolateral prefrontal cortexParietal cortexManiaDepressionEuthymiaWorking memory
Neuropsychological studies of subjects with bipolar disorder suggest impairment of working memory notonly in acute mood states, but also while subjects are euthymic. Using fMRI to probe working memoryregions in bipolar subjects in different mood states, we sought to determine the functional neural basis forthese impairments. Typical working memory areas in normal populations include dorsolateral prefrontalcortex (BA9/46) and the posterior parietal cortex (BA40). We evaluated the activation in these regions usingan n-back task in 42 bipolar subjects (13 manic, 15 euthymic and 14 depressed subjects) and 14 controlsubjects. While both control and bipolar subjects performed similarly on the task, bipolar subjects in all threemood states showed a significant reduction in activation in right BA9/46 and right BA40. Patients withbipolar disorder exhibit significantly attenuated neural activation in working memory circuits, independentof mood state. The reduction of neural activation may suggest a trait-related deficit. Subjects with bipolardisorder activated other additional frontal and temporal regions, perhaps as a compensatory mechanism, butthis remains to be further explored.
1544, Box 957057, Los Angeles,: +1 310 794 9915.shuler).
Ltd. All rights reserved.
© 2010 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Many studies have documented an alteration in neuropsycholog-ical function in patients with bipolar disorder during the manic anddepressed mood states (Clark et al., 2001; Malhi et al., 2007;Martinez-Aran et al., 2004; Murphy et al., 1999; Rubinsztein et al.,2006). Several have additionally reported a persistence of neuropsy-chological dysfunction even after the acute mood state resolves.Relevant to the current study, euthymic bipolar subjects have beenreported to perform significantly worse than normal control subjectson measures of executive functioning, including working memory(Altshuler et al., 2004; Depp et al., 2007; Ferrier et al., 1999; Goldberget al., 1993; Malhi et al., 2007; Martinez-Aran et al., 2004; Rossi et al.,2000; Thompson et al., 2007; Trivedi et al., 2008, 2007; van Gorp et al.,1998). Persistent neurocognitive abnormalities in euthymic bipolarpatients may provide clues to brain areas of underlying pathology inthe illness. To date, however, the neurophysiological correlates forthese cognitive impairments remain underexplored.
Two consistent functional neuroimaging findings of workingmemory in normal populations are activation of the dorsolateralprefrontal cortex (dlPFC) (BA9/46) and activation of the inferior,posterior parietal cortex (BA40) (Belger et al., 1998; Carlson et al.,1998; Cohen et al., 1997; Curtis 2006; Smith and Jonides, 1998). fMRIstudies probing these brain regions in the bipolar population haverarely been performed. It is possible that the workingmemory deficitsobserved during neurocognitive testing in euthymic bipolar subjectsimplicate dysfunction in the dlPFC and/or the posterior parietalcortices in these patients.
To our knowledge, only five fMRI studies have been reported usingworking memory tasks in subjects with bipolar disorder duringeuthymia. Lagopoulos et al. (2007) demonstrated that euthymic bipolarsubjects (n=10) failed to engage dlPFC during a Sternberg workingmemory task compared to normal controls. Monks et al. (2004) alsofound reduced activation in dlPFC in bipolar euthymic (n=12)compared to control subjects using an n-back task. Drapier et al.(2008) foundnodifferences in this regionbetweeneuthymic andcontrolsubjects, but observed a trend toward increased left ventrolateralactivation in euthymic compared with control subjects. However, Adleret al. (2004) found no significant differences in dlPFC activation ineuthymic bipolar subjects (n=15) compared to a normal control group.Frangou et al. (2008) found no significant between-group differences in
23J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
theworkingmemory task using the n-back taskwith a small sample size(n=7 bipolar subjects; n=7 normal control subjects). Thus, the extantfMRI literature of working memory in bipolar disorder remainsinconsistent.
While the above studies evaluated euthymic bipolar vs. normalcontrol subjects, no studies to date have directly compared neuralactivation during a working memory task in bipolar subjects in arange of mood states. This would allow for an exploration of moodstate-specific neurofunctional deficits. To our knowledge, only onefMRI study in the literature to date has reported on bipolar patients indifferent mood states while performing a neurocognitive task, andthat study involved a set shifting/response inhibition task (Blumberget al., 2003).
In the present study, we sought to evaluate the neurofunctionalbasis for the working memory deficits seen in bipolar patients usingthe n-back task. The n-back task is one of the most common fMRIparadigms used to observe working memory function in normal andpatient populations (Wager and Smith, 2003) and it has been usedsuccessfully in the euthymic bipolar population (Drapier et al., 2008;Frangou et al., 2008; Monks et al., 2004). We evaluated subjects acrossall three mood states to assess the extent to which the presence andseverity of these deficits are mood-state specific or enduring despiteremission of the acute state. Based on the persistent working memoryneurocognitive deficits reported in euthymic bipolar subjects anddiscussed above, we hypothesized there would be a reduced neuralactivation of the traditional working memory areas of BA 9/46 andBA40 in all bipolar patient groups irrespective of mood state.
2. Methods
2.1. Subjects
The Institutional Review Board at UCLA and the VA Greater LosAngeles Healthcare System approved the study protocol. Each subjectprovided written informed consent. Subjects with bipolar I disorderwere recruited through the UCLA Mood Disorders Clinic, the BipolarDisorders Clinic of the Veterans Affairs Greater Los Angeles HealthCare System, and the inpatient units of both hospitals. Subjectsenrolled in other research projects of the UCLA Mood DisordersResearch Program were also invited to participate. Control subjectswere recruited by advertisement in local newspapers and campusflyers. Both control and patient populations were evaluated using theStructured Clinical Interview for DSM-IV (SCID) to confirm anaccurate diagnosis or the absence thereof. Illness duration andmedication information for patients was obtained by patient self-report and by reference to medical records when available. Exclusion
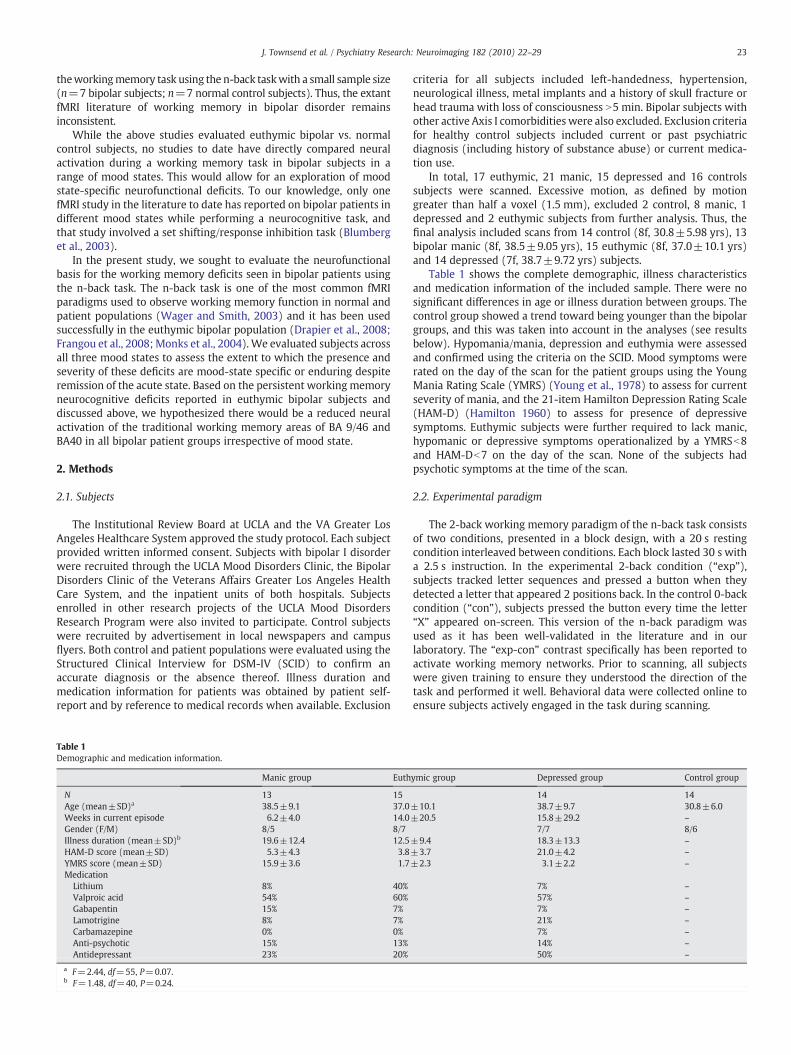
Table 1Demographic and medication information.
Manic group Euth
N 13 15Age (mean±SD)a 38.5±9.1 37.0Weeks in current episode 6.2±4.0 14.0Gender (F/M) 8/5 8/7Illness duration (mean±SD)b 19.6±12.4 12.5HAM-D score (mean±SD) 5.3±4.3 3.8YMRS score (mean±SD) 15.9±3.6 1.7Medication
Lithium 8% 40%Valproic acid 54% 60%Gabapentin 15% 7%Lamotrigine 8% 7%Carbamazepine 0% 0%Anti-psychotic 15% 13%Antidepressant 23% 20%
a F=2.44, df=55, P=0.07.b F=1.48, df=40, P=0.24.
criteria for all subjects included left-handedness, hypertension,neurological illness, metal implants and a history of skull fracture orhead trauma with loss of consciousness N5 min. Bipolar subjects withother active Axis I comorbidities were also excluded. Exclusion criteriafor healthy control subjects included current or past psychiatricdiagnosis (including history of substance abuse) or current medica-tion use.
In total, 17 euthymic, 21 manic, 15 depressed and 16 controlssubjects were scanned. Excessive motion, as defined by motiongreater than half a voxel (1.5 mm), excluded 2 control, 8 manic, 1depressed and 2 euthymic subjects from further analysis. Thus, thefinal analysis included scans from 14 control (8f, 30.8±5.98 yrs), 13bipolar manic (8f, 38.5±9.05 yrs), 15 euthymic (8f, 37.0±10.1 yrs)and 14 depressed (7f, 38.7±9.72 yrs) subjects.
Table 1 shows the complete demographic, illness characteristicsand medication information of the included sample. There were nosignificant differences in age or illness duration between groups. Thecontrol group showed a trend toward being younger than the bipolargroups, and this was taken into account in the analyses (see resultsbelow). Hypomania/mania, depression and euthymia were assessedand confirmed using the criteria on the SCID. Mood symptoms wererated on the day of the scan for the patient groups using the YoungMania Rating Scale (YMRS) (Young et al., 1978) to assess for currentseverity of mania, and the 21-item Hamilton Depression Rating Scale(HAM-D) (Hamilton 1960) to assess for presence of depressivesymptoms. Euthymic subjects were further required to lack manic,hypomanic or depressive symptoms operationalized by a YMRSb8and HAM-Db7 on the day of the scan. None of the subjects hadpsychotic symptoms at the time of the scan.
2.2. Experimental paradigm
The 2-back working memory paradigm of the n-back task consistsof two conditions, presented in a block design, with a 20 s restingcondition interleaved between conditions. Each block lasted 30 s witha 2.5 s instruction. In the experimental 2-back condition (“exp”),subjects tracked letter sequences and pressed a button when theydetected a letter that appeared 2 positions back. In the control 0-backcondition (“con”), subjects pressed the button every time the letter“X” appeared on-screen. This version of the n-back paradigm wasused as it has been well-validated in the literature and in ourlaboratory. The “exp-con” contrast specifically has been reported toactivate working memory networks. Prior to scanning, all subjectswere given training to ensure they understood the direction of thetask and performed it well. Behavioral data were collected online toensure subjects actively engaged in the task during scanning.
ymic group Depressed group Control group
14 14±10.1 38.7±9.7 30.8±6.0±20.5 15.8±29.2 –
7/7 8/6±9.4 18.3±13.3 –
±3.7 21.0±4.2 –
±2.3 3.1±2.2 –
7% –
57% –
7% –
21% –
7% –
14% –
50% –

Table 2Behavioral data analysis for experimental and control conditions.
Controlgroup
Manicgroup
Euthymicgroup
Depressedgroup
Total accuracy(% correct±SD)
87.4±4.1 88.4±2.6 84.3±4.2 94.9±2.4
Average reaction time(s±SD)
0.49±0.04 0.56±0.03 0.55±0.05 0.49±0.03
24 J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
2.3. Image acquisition
Functional neuroimaging data were collected using a 3.0 Tesla GEMRI scanner at the UCLA Brain Mapping Center. For all scans, subjectswere positioned comfortably in a supine orientation with their headlocated in a head RF coil and stabilized with foam pads to minimizehead motion. Blood oxygen level dependent (BOLD) functionalimages were acquired with a gradient echo-planar imaging (EPI)sequence, and covered 16 trans-axial slices (3 mm thick, 1 mm gap)encompassing the cerebrum (TR/TE=2500/35 ms, FOV=24 cm,matrix=64×64). All scanning parameters were selected to optimizethe quality of the BOLD signal, especially within the dlPFC and inferiorparietal lobule, while maintaining a sufficient number of slices toacquire as much of the brain as possible within the technical confinesof the scanner. Before the collection of fMRI data for each subject, weacquired a reference EPI scan to register each subject′s data intostandard space.
2.4. Behavioral data analysis
Behavioral data were collected during scanning, and accuracy ofperformance and reaction times were recorded for the experimentaland control tasks. Due to technical difficulties with the button box andtrigger system, not all subjects had usable behavioral data for lateranalysis. However, subjects with and without behavioral data werecompared on fMRI regions of interest (ROI) activation to evaluatepossible group differences and to ensure all subjects used in the finalanalyses performed the task (Carter et al., 2008). Differences betweengroups on each task for both accuracy and response time wereassessed with a mixed-effects analysis of variance model in Excel.
2.5. fMRI analysis
Functional images were examined closely for severe motion or spikeartifacts. All subjects with more than half a voxel of motion (N1.5 mm)were excluded. Data processingwas carriedout usingFEAT (FMRI ExpertAnalysis Tool) Version 5.91, part of FSL 4.0 (FMRIB′s Software Library,www.fmrib.ox.ac.uk/fsl). The following pre-statistics processing wasapplied: motion correction usingMCFLIRT (Jenkinson et al., 2002); non-brain removal using BET (Smith 2002); spatial smoothing using aGaussian kernel of FWHM5mm;grand-mean intensity normalization ofthe entire 4D dataset by a single multiplicative factor; and high-passtemporal filtering (Gaussian-weighted least-squares straight line fitting,with sigma=65.0 s).
Time-series statistical analysis was carried out using FILM withlocal autocorrelation correction (Woolrich et al., 2001). Registrationto high-resolution structural and standard space images was carriedout using FLIRT (Jenkinson et al., 2002, Jenkinson and Smith, 2001),using 7 degrees of freedom to register functional images to subject′shigh-resolution structural images and 12 degrees of freedom toregister those high-resolution images to standard space. All registra-tions were manually inspected to ensure proper registration.Statistical images were generated for the experimental vs. control(“exp-con”) contrasts for each subject, and these were used insubsequent analyses. Higher-level statistical analyses for within andbetween group analyses were carried out using FLAME 1+2 (FMRIB′sLocal Analysis of Mixed Effects) (Beckmann et al., 2003; Woolrichet al., 2004). Within-group results were reported using a cluster-based model (Friston 1997; Hochberg and Benjamini, 1990; Worsleyet al., 1997). Using this method, a threshold of ZN2.3 is consideredconservative and is standard with this software. The resulting clusterswere then tested for significance using random field theory with afinal significance test of PN .05, corrected for multiple comparisons(Genovese et al., 2002).
Due to our a priori hypothesis and the as yet undevelopedmethodsfor analyzing a between group whole-brain differences in four groups
with fMRI data, we used a region of interest analysis for the between-group results. This approach is more conservative than whole-brainapproaches in which any activated cluster is accepted as relevant, acommon error in the neuroimaging literature (Poldrack, 2006). As theliterature consistently shows bilateral dlPFC and bilateral parietalregions subserve working memory (Belger et al., 1998; Carlson et al.,1998; Cohen et al., 1997), regions of interest (ROI) were drawn inthese areas of the brain to interrogate differences in the workingmemory network between groups. Rather than use an anatomically-drawn ROI, we used an ROI analysis approach using the maximallyactivated voxel in the left and right dlPFC (BA46/9 centered at x=−42, y=28, z=22 and x=42, y=32, z=30) and in left and rightposterior parietal cortex (BA 40 centered at x=−56, y=−56, z=28and x=56, y=−52, z=28) and dilating a 5 mm sphere around thevoxel to define the ROI. These maximally activated voxels in oursubjects are quite similar to those reported in the literature (Belgeret al., 1998; Carlson et al., 1998; Cohen et al., 1997) and thus wereused to create a ROI. For large regions with poorly defined anatomicalboundaries and marked functional heterogeneity, the use of afunctionally-defined ROI is more appropriate and has been used inother studies (Anand et al., 2007, 2005; Siegle et al., 2007). The timecourse of the voxels in the entire 5 mm sphere was used to calculate amean percent signal change in that region for the exp-con contrast ofeach subject using FEATQuery. These mean percent signal changevalues for each subject were entered into a second-level analysis ofvariance (ANOVA) to determine brain activation differences as afunction of group. Follow-up pairwise group comparison t-tests wereperformed.
3. Results
3.1. Behavioral results
All groups performed the n-back task with high accuracy. Therewere no differences in accuracy (ANOVA: F=1.45, df=3,34,P=0.25) or reaction times (ANOVA: F=0.99, df=3,34, P=0.41) inbehavioral performance between groups (Table 2). While the groupsappear to have differences in spread for the accuracy measure, a testfor inequality of variance was not significant. Additionally, pairwisecomparisons of the groups using (i) regular t-tests (assuming equalvariances), (ii) Welch′s t-tests (not assuming equal variances) and(iii) nonparametric Wilcoxon rank-sum tests all showed no signifi-cant behavioral differences after adjusting for multiple comparisons.
3.2. Within-group results
Table 3 and Fig. 1 display the within-group regions of activation ineach group.
Control subjects activated typical working memory regions(Fig. 1a) including bilateral frontal lobe dlPFC (BA 9/46), bilateralparietal lobe supramarginal gyri (BA 39/40), as well as bilateralprecuneous (BA 19) and bilateral inferior frontal gyrus (right BA 47and left BA 44) (Table 3).
Manic subjects did not activate the working memory circuitsactivated in the control subjects. Instead they activated other frontallobe regions including activated bilateral inferior frontal gyrus (BA 44/

Table 3Within-group results showing the coordinates of maximally activated voxels.
Controls Depressed Euthymic Manic
x y z Z score x y z Z score x y z Z score x y z Z score
Frontal lobeR MFG (BA 46/9) 42 32 30 3.84a 42 28 20 3.45a 42 38 24 3.28
48 12 32 3.30a
L MFG (BA46/9) −42 28 22 3.28a −34 32 16 2.84−54 16 26 2.98
R MFG (BA 10) 38 46 22 3.30 30 58 −6 3.14 30 50 −10 2.96a
L MFG (BA 10) −28 50 2 2.80 −34 54 12 3.18a
R IFG (BA 47) 34 24 −4 3.71 36 14 −10 3.23 32 20 0 2.99a 36 42 −6 3.2244 18 −6 3.00
L IFG (BA 47) −38 18 −14 2.86R IFG (BA 44) 48 12 26 3.18 56 12 10 2.74L IFG (BA 44) −48 10 22 3.37a −56 12 28 2.87 −46 6 8 3.17
−34 8 28 2.96 −42 2 28 3.15a
R IFG (BA 45) 50 12 20 2.96L IFG (BA45/46) −50 22 18 3.54 −44 20 8 3.01SFG (BA 9) 0 44 18 3.29Insula −38 16 0 3.65Cingulate 12 32 10 3.05a
Parietal lobeR SMG (BA 40/39) 56 −52 28 3.65a 34 −54 30 3.13a
30 −58 40 2.9138 −46 38 2.80
L SMG (BA 40/39) −56 −56 28 3.33 −46 −58 30 2.58R IPL (BA 39/40) 44 −50 38 3.00 50 −54 42 2.94a
L IPL (BA 39/40) −58 −58 22 3.29 −58 −60 38 2.73 −42 −56 42 3.08−44 −50 38 2.69a
−24 −56 40 2.55R Precun. (BA19) 24 −74 38 2.85 28 −74 36 2.90L Precun. (BA19) −28 −74 24 3.90a −22 −68 34 2.86
Temporal lobeL MTG (BA 39) −46 −66 24 3.26
−48 −64 12 3.04R MTG (BA 39) 26 −58 18 3.07L MTG (BA 37) −46 −52 8 2.86
Occipital lobeL MOG (BA19) −34 −74 30 2.98 −52 −66 8 3.12
a Denotes additional regions within 10 mm in any direction.
25J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
45 and BA 47) as well as other frontal regions in left precentral gyrus(BA44) and bilateral middle frontal gyri (BA 10 and BA 11). They alsoactivated the left middle temporal gyrus (BA 21, 37 and 39), and leftinferior parietal lobule (BA 40) (Fig. 1b). The bilateral middle frontalgyri and temporal activations were not active in the control group, butwere seen in depressed and euthymic groups.
Euthymic subjects activated predominately right hemisphereregions. They showed similar activation to both controls and bipolardepressed subjects in right dlPFC (BA9/46), again activating a moreventral portion of this region than the control subjects, and rightinferior frontal gyrus (BA 47). Unlike the control subjects, theeuthymic subjects additionally activated right superior frontal gyrus(BA 10) and right anterior cingulate (BA 24) (Fig. 1c).
Bipolar depressed subjects activated bilateral dlPFC (BA9/46) butthe activation occurred more ventrally and medially than in controls(Table 3). Bipolar depressed subjects also activated bilateral parietalregions (BA 39/40). Additional regions not activated in controls,including bilateral middle frontal gyri (BA 10), bilateral inferiorfrontal gyri (BA 47), and temporal limbic regions (BA 39/40 and theleft insula) were also activated (Fig. 1d).
Due to a trend in age differences between control and patientgroups (ANOVA F=2.44, df=3,52, P=.0748), and because we wantto compare regional areas of activation across groups, additionalanalyses using age as a covariate were performed. The results of theseanalyses exhibited no substantive differences with those from theinitial unadjusted within-group analyses.
3.3. Between-group ROI results
ROIs were drawn in left and right dlPFC centered and left and rightsupramarginal gyri (posterior parietal cortex BA40). fMRI ROIactivation results did not differ significantly within bipolar or controlsubgroups between the subjects with and without behavioral data. Itwas therefore appropriate to assume that all subjects were activelyengaged in the task, thus the entire group of subjects was included inthe following analyses. A four group ANOVA revealed significantbetween-group differences in the right dlPFC (F=3.33, df=3,52,P=0.026); (Fig. 2). Control subjects activated right dlPFC significantlymore than bipolar subjects, irrespective of mood state (controls vs.manic subjects: T=2.49, df=1,23, P=0.01; control vs. euthymicsubjects: T=3.63, df=1,26, P=0.0006; control vs. depressedsubjects: T=1.75, df=1,23, P=0.04). There were no differencesbetween bipolar subjects across mood states (manic vs. euthymicsubjects: T=0.50, df=1,26, P=0.62; manic vs. depressed subjects:T=−0.48, df=1,25, P=0.64; euthymic vs. depressed: T=−1.01,df=1,27, P=0.32).
Similarly, a four group ANOVA showed that control subjectsactivated right BA 40 significantly more than any patient group(overall F=3.15, df=3,52, P=0.03; controls vs. manic subjects:T=2.40, df=1,25, P=0.01; control vs. euthymic subjects: T=2.81,df=1,25, P=0.005; control vs. depressed subjects: T=1.66,df=1,26, P=0.05) (Fig. 3). Again, there were no differences in rightBA40 across mood states among bipolar subjects (manic vs. euthymic

Fig. 1. Within-group results for NBACK task, EXP–CON condition (z> 1.7, P=.05 corrected).
26 J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
subjects: T=0.97, df=1,26, P=0.34; manic vs. depressed subjects:T=−0.43, df=1,25, P=0.67; euthymic vs. depressed subjects: T=−1.25, df=1,27, P=0.22).
There were no significant between-group differences betweencontrol, depressed, euthymic or manic subjects in either of the a prioriregions in the left hemisphere (dlPFC: ANOVA: F=0.61, df=3,52,P=0.61; BA40: ANOVA: F=0.38, df=3,52, P=0.77) (Figs. 2 and 3).
Due to a trend in age differences between control and patient groups(ANOVA F=2.44, df=3,52, P=.0748), we performed follow-up
Fig. 2. Activation in DLPFC: ROI results.
analyses of co-variance (ANCOVA) with age as a covariate. Adjust-ment for age did not affect the observed group differences in theright dlPFC or BA40 in either the overall models or the post hocpairwise comparisons. This is not surprising given the fact thatwe did not find a significant relationship between age and activationin these regions either overall (right dlPFC: F=1.38, df=1,54,P=0.25; right BA40: F=0.33, df=1,54, P=0.57) or in any of thesubgroups.
Fig. 3. Activation in parietal cortex: ROI results.

27J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
4. Discussion
Our study replicates prior studies demonstrating activation ofbilateral dlPFC and parietal regions in normal control subjects (Adleret al., 2004; Belger et al., 1998; Carlson et al., 1998; Cohen et al., 1997;Frangou et al., 2008; Lagopoulos et al., 2007; Monks et al., 2004; Smithand Jonides, 1998). Working memory task performance was associ-ated with activation in dlPFC (BA46, BA9), inferior frontal gyrus (IFG)(BA47), left IFG (BA44), and parietal lobe (BA39/ BA40) in controlsubjects. These areas are part of the cognitive control network,defined by functional connectivity and described by Cole andSchneider (2007) (Cole and Schneider, 2007). Supporting the goalof this study, all subjects demonstrated some activation of theworkingmemory network. However, bipolar subjects failed to engagethis cognitive control network to the same extent as the controlsubjects. While bipolar subjects activated dlPFC and parietal regions,they showed significantly less activation than the control subjects inboth the right frontal and right parietal regions involved in workingmemory. Bipolar subjects across all mood states additionally activatedtemporal lobe and other frontal lobe structures (see Table 3).
Working memory tasks activate bilateral frontal and parietalregions. However, there is a laterality effect with the right hemisphereas predominant regardless of stimulus type (Nystrom et al., 2000). Inthis regard, it is interesting that the major differences betweenpatients and controls were found in the right hemisphere. Theabnormal neurophysiologic pattern in this region, specifically the lessrobust right-sided dorsal frontal activation in bipolar disorder, mayrelate to the clinical phenomenon of impairment in working memorypreviously reported (Altshuler et al., 2008, 2004; Clark et al., 2001;Coffman et al., 1990; Depp et al., 2007; Ferrier et al., 1999; Goldberget al., 1993; Malhi et al., 2007; Martinez-Aran et al., 2004; Morice1990; Murphy et al., 1999; Rossi et al., 2000; Rubinsztein et al., 2006;Senturk et al., 2007; Tam et al., 1998; Thompson et al., 2007; Trivediet al., 2008, 2007; van Gorp et al., 1998).
Our study adds to the small literature using fMRI during workingmemory tasks in euthymic bipolar subjects and suggests networkimpairments even in the absence of an acute mood state. The lack ofbehavioral differences between groups is consistent with the majorityof the literature (Frangou et al., 2008; Lagopoulos et al., 2007; Monkset al., 2004), but not all (Adler et al., 2004; Drapier et al., 2008). Thisstudy′s fMRI results are consistent with two other working memorystudies involving smaller numbers of euthymic subjects. Using theSternberg task, Lagopoulos et al. (2007) studied 10 bipolar womenand 10 matched controls. Monks et al. (2004) studied 12 bipolar menand 12matched controls using the n-back task. Both studies, like ours,found a reduction in activation of right dlPFC and parietal regions ineuthymic bipolar subjects compared to controls.
In contrast, Frangou et al. (2008) found no between groupdifferences while subjects performed an n-back task. However, asthere were only 7 subjects in each group for that study, the negativeresults may have been due to reduced power to detect groupdifferences. Interesting, their data did suggest some dysfunction inthe network in bipolar subjects, as differential activation patterns inthese regions were observed when examining the effects of memoryload. Specifically, controls were found to show an increased activationin dlPFCwith increasedmemory load, as has been shown in a previousstudy of normal controls (Nystrom et al., 2000). Euthymic subjectsshowed no such pattern. Similar to Frangou, Adler et al. (2004) did notfind significant differences in activation in dlPFC or parietal cortexin 15 euthymic bipolar subjects and 15 matched controls using then-back task. It is unclear why our study differs from this latter studydespite a similar paradigm and sample size. As in our study, however,a heightened activation in temporal lobe structures was observed inthe bipolar subjects that was not observed in the normal controlgroup while performing this task. Lagopoulos et al. (2007) similarlyfound engagement of temporal lobe activation in the bipolar subjects
when performing the working memory task. Thus, three of the fivestudies (including the current one) that used fMRI to assess frontallobe neural activation during aworkingmemory task have found thatlimbic/temporal lobe structures are activated in bipolar subjectsduring a task that does not normally activate these brain regions.Some imaging studies in patients with bipolar disorder havesuggested limbic hyperactivity not only in mania (Altshuler et al.,2005), but even during euthymia (Hassel et al., 2008; Lawrence et al.,2004; Yurgelun-Todd et al., 2000). Whether this represents a com-pensatory mechanism or a chronically hyperactive brain region inbipolar illness remains to be further studied.
Increased activation in an orbitofrontal region (BA10) was alsoobserved in the subjects with bipolar disorder, but not in the controlsubjects. Subjects in all three states showed significant activation in BA10,whereas the control subjects showed no such activation in this region.Tasks involving conflict resolution and decision making typically recruitthis region (Cabeza and Nyberg, 2000; Zhang et al., 2003). Other studieshave found activation of this brain region during semantic retrieval andmaking familiarity judgments (Buckner et al., 2000; Eldridge et al., 2000;MacLeod et al., 1998;Wagner et al., 1998). The exact reason for activationof this brain region in our patient population is not clear. Activation of thisfrontopolar region is not commonly reported inworkingmemory studiesamong normal control subjects, suggesting that this region is not a part ofthe typically functioning working memory network. As the bipolarsubjects performedaswell as controls, it is possible that activationof BA10in thebipolar groupmay represent a compensatoryphysiologic activation.We had no a priori hypothesis regarding this region in patients whileperforming a working memory task. However, this brain region haspreviously been reported as active in bipolar subjects across a variety oftasks in ours (Altshuler et al., 2008) and others′ (Roth et al., 2006;Strakowski et al., 2004) studies. Interestingly, this frontal lobebrain regionshows the greatest expansion in size across the primate species(Semendeferi et al., 2001). The role of BA10 in mood regulation is notknown and requires further investigation.
There are several limitations of the present study. First, a numberof bipolar subjects were excluded from participation. For example, themost severely manic patients were excluded due to their inability toremain still in the scanner. Additionally, patients with currentcomorbidities were excluded. Some patients who were screened forthe study refused to participate (although the exact number was nottracked). Thus, how representative our bipolar sample is of the overallbipolar population is unclear. It is also possible that the use ofmedication could be a confound in our study. If medication were aprimary factor, however, we might have expected to see a globaldampening of activation across all brain regions rather than aselective decrease in activation in some specific regions (e.g. dlPFC,parietal) and increased activation in others (e.g. BA10, temporal lobe).In addition, the areas directly related to the network, there was alaterality difference between groups, that is, unlikely to be due to theeffects of medication. Thus, medication use per se does not appear tobe solely responsible for the findings. One published study hassuggested that treatment at least with lithium, a common medicationused by our bipolar subjects, does not alter brain activation whileperforming a memory task (Silverstone et al., 2005). Additionally, acurrent review of the bipolar disorder neuroimaging studies exam-ining medication effects on brain activation suggest either nosignificant effect or ameliorative effects of psychotropic medicationson abnormal functional measures (Phillips et al., 2008). Future studieswith unmedicated subjects would help further refine the rolemedication may play in fMRI findings.
In a recent review, impaired verbal memory and executive functionhave been proposed as potential cognitive endophenotypes for bipolardisorder (Glahn et al., 2004), particularly since these deficits presentearly in the illness course and do not exclusively result frommultiple orprolonged episodes or only subjective complaints (Gruber et al., 2008;Martinez-Aran et al., 2005; Nehra et al., 2006). These may not be an

28 J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
artifact of illness duration or episode frequency, but instead may relatemore inherently to the biology of the disorder. A recent study foundabnormal frontal activation in relatives of bipolar subjects, suggestingthat a genetic liability for bipolar disordermay be characterized bymoregeneral frontal lobe abnormalities (Drapier et al., 2008).
Our study points to an underlying neurofunctional deficit that maybe related to a cognitive deficit previously reported in subjects withbipolar disorder. While the relative ease of our task did not result ingroup differences in behavioral performance, it revealed differences inthe regional brain function while performing this task. In bipolarsubjects, deficits were revealed in activation of this network,regardless of mood state. While we had hypothesized that a decreasein neural activation would be present in euthymic subjects comparedto control subjects, it was also found that the subjects in a mood stateof mania or depression did not significantly differ in degree of neuralactivation from the euthymic subjects. A greater number of subjects ineach group might have allowed for subtle differences across moodstates to show significant differences. But our findings stronglysuggest a more illness-related than mood state-related alteration inneural activation. Thus, the results of our study suggest an enduringneurophysiological abnormality in a specific cognitive network inbipolar illness. The underlying etiology of the functional deficit mightbe structural in nature, but this remains to be further explored andsuch studies are ongoing in our laboratory. Some unpublished data byour group suggests decreases in cortical thickness in these sameregions where functional deficits have been observed in bipolarsubjects compared to controls. Thus, there may be a structuralabnormality that drives the functional deficits. If structural abnor-malities are confirmed to be associated with the functional abnor-malities, it would remain to be determined whether they occur earlyin the illness or occur as the result of mood episodes (Altshuler 1993).Future studies including patients in their first mood episode wouldhelp address this important issue.
In summary, consistent with previous reports, we found dlPFC andparietal activation in healthy subjects during a working memory task.This pattern in activation was significantly decreased in bipolarsubjects, regardless of mood state at the time of scanning. Our studysupports the presence of an enduring neurophysiological abnormalityin a specific cognitive network in bipolar illness. This neurophysio-logical deficit may underlie the working memory neurocognitivedeficit previously reported across mood states. How or if these deficitsare involved with mood dysregulation, the defining feature of bipolardisorder, remains to be determined. Future studies that examinewhether structural differences occur in overlapping regions as well aswhether structural deficits exist in brain regions that project to thisarea would be of interest.
Acknowledgments
The authors gratefully acknowledge The Stanley Medical Re-search Institute, NARSAD (National Association for Research onSchizophrenia and Affective Disorders), and the National Institute ofMental Health (K24 MH001848, R21 MH075944, 5F31MH078556)for their financial support of this study. For generous support theauthors also wish to thank the Brain Mapping Medical ResearchOrganization, Brain Mapping Support Foundation, Pierson-LovelaceFoundation, The Ahmanson Foundation, William M. and Linda R.Dietel Philanthropic Fund at the Northern Piedmont CommunityFoundation, Tamkin Foundation, Jennifer Jones-Simon Foundation,Capital Group Companies Charitable Foundation, Robson Family andNorthstar Fund. The project described was supported by GrantNumbers RR12169, RR13642 and RR00865 from the National Centerfor Research Resources (NCRR), a component of the NationalInstitutes of Health (NIH); its contents are solely the responsibilityof the authors and do not necessarily represent the official views ofNCR or NIH.
References
Adler, C.M., Holland, S.K., Schmithorst, V., Tuchfarber, M.J., Strakowski, S.M., 2004.Changes in neuronal activation in patients with bipolar disorder duringperformance of a working memory task. Bipolar Disorders 6, 540–549.
Altshuler, L.L., 1993. Bipolar disorder: are repeated episodes associated withneuroanatomic and cognitive changes? Biological Psychiatry 33, 563–565.
Altshuler, L.L., Ventura, J., van Gorp, W.G., Green, M.F., Theberge, D.C., Mintz, J., 2004.Neurocognitive function in clinically stable men with bipolar I disorder orschizophrenia and normal control subjects. Biological Psychiatry 56, 560–569.
Altshuler, L., Bookheimer, S., Proenza, M.A., Townsend, J., Sabb, F., Firestine, A.,Bartzokis, G., Mintz, J., Mazziotta, J., Cohen, M.S., 2005. Increased amygdalaactivation during mania: a functional magnetic resonance imaging study. AmericanJournal of Psychiatry 162, 1211–1213.
Altshuler, L., Bookheimer, S., Townsend, J., Proenza, M.A., Sabb, F., Mintz, J., Cohen, M.S.,2008. Regional brain changes in bipolar I depression: a functional magneticresonance imaging study. Bipolar Disorders 10, 708–717.
Anand, A., Li, Y., Wang, Y.,Wu, J., Gao, S., Bukhari, L., Mathews, V.P., Kalnin, A., Lowe,M.J.,2005. Antidepressant effect on connectivity of the mood-regulating circuit: anFMRI study. Neuropsychopharmacology 30, 1334–1344.
Anand, A., Li, Y.,Wang, Y., Gardner, K., Lowe,M.J., 2007. Reciprocal effects of antidepressanttreatment on activity and connectivity of the mood regulating circuit: an FMRI study.The Journal of Neuropsychiatry and Clinical Neurosciences 19, 274–282.
Beckmann, C.F., Jenkinson, M., Smith, S.M., 2003. General multilevel linear modeling forgroup analysis in FMRI. Neuroimage 20, 1052–1063.
Belger, A., Puce, A., Krystal, J.H., Gore, J.C., Goldman-Rakic, P., McCarthy, G., 1998.Dissociation of mnemonic and perceptual processes during spatial and nonspatialworking memory using fMRI. Human Brain Mapping 6, 14–32.
Blumberg, H.P., Leung, H.C., Skudlarski, P., Lacadie, C.M., Fredericks, C.A., Harris, B.C.,Charney, D.S., Gore, J.C., Krystal, J.H., Peterson, B.S., 2003. A functional magneticresonance imaging study of bipolar disorder: state- and trait-related dysfunction inventral prefrontal cortices. Archives of General Psychiatry 60, 601–609.
Buckner, R.L., Logan, J., Donaldson, D.I., Wheeler, M.E., 2000. Cognitive neuroscience ofepisodic memory encoding. ACTA Psychologica (Amsterdam) 105, 127–139.
Cabeza, R., Nyberg, L., 2000. Neural bases of learning and memory: functionalneuroimaging evidence. Current Opinion in Neurology 13, 415–421.
Carlson, S., Martinkauppi, S., Rama, P., Salli, E., Korvenoja, A., Aronen, H.J., 1998.Distribution of cortical activation during visuospatial n-back tasks as revealed byfunctional magnetic resonance imaging. Cerebral Cortex 8, 743–752.
Carter, C.S., Heckers, S., Nichols, T., Pine, D.S., Strother, S., 2008. Optimizing the designand analysis of clinical functional magnetic resonance imaging research studies.Biological Psychiatry 64, 842–849.
Clark, L., Iversen, S.D., Goodwin, G.M., 2001. A neuropsychological investigation ofprefrontal cortex involvement in acute mania. American Journal of Psychiatry 158,1605–1611.
Coffman, J.A., Bornstein, R.A., Olson, S.C., Schwarzkopf, S.B., Nasrallah, H.A., 1990.Cognitive impairment and cerebral structure by MRI in bipolar disorder. BiologicalPsychiatry 27, 1188–1196.
Cohen, J.D., Perlstein, W.M., Braver, T.S., Nystrom, L.E., Noll, D.C., Jonides, J., Smith, E.E.,1997. Temporal dynamics of brain activation during a working memory task.Nature 386, 604–608.
Cole, M.W., Schneider, W., 2007. The cognitive control network: integrated corticalregions with dissociable functions. Neuroimage 37, 343–360.
Curtis, C.E., 2006. Prefrontal and parietal contributions to spatial working memory.Neuroscience 139, 173–180.
Depp, C.A., Moore, D.J., Sitzer, D., Palmer, B.W., Eyler, L.T., Roesch, S., Lebowitz, B.D.,Jeste, D.V., 2007. Neurocognitive impairment in middle-aged and older adults withbipolar disorder: comparison to schizophrenia and normal comparison subjects.Journal of Affective Disorders 101, 201–209.
Drapier, D., Surguladze, S., Marshall, N., Schulze, K., Fern, A., Hall, M.H., Walshe, M.,Murray, R.M., McDonald, C., 2008. Genetic liability for bipolar disorder ischaracterized by excess frontal activation in response to a working memory task.Biological Psychiatry 64, 513–520.
Eldridge, L.L., Knowlton, B.J., Furmanski, C.S., Bookheimer, S.Y., Engel, S.A., 2000.Remembering episodes: a selective role for the hippocampus during retrieval.Nature Neuroscience 3, 1149–1152.
Ferrier, I.N., Stanton, B.R., Kelly, T.P., Scott, J., 1999. Neuropsychological function ineuthymic patients with bipolar disorder. British Journal of Psychiatry 175, 246–251.
Frangou, S., Kington, J., Raymont, V., Shergill, S.S., 2008. Examining ventral and dorsalprefrontal function in bipolar disorder: a functional magnetic resonance imagingstudy. European Psychiatry 23, 300–308.
Friston, K.J., 1997. Testing for anatomically specified regional effects. Human BrainMapping 5, 133–136.
Genovese, C.R., Lazar, N.A., Nichols, T., 2002. Thresholding of statistical maps infunctional neuroimaging using the false discovery rate. Neuroimage 15, 870–878.
Glahn, D.C., Bearden, C.E., Niendam, T.A., Escamilla, M.A., 2004. The feasibility ofneuropsychological endophenotypes in the search for genes associated withbipolar affective disorder. Bipolar Disorders 6, 171–182.
Goldberg, T.E., Gold, J.M., Greenberg, R., Griffin, S., Schulz, S.C., Pickar, D., Kleinman, J.E.,Weinberger, D.R., 1993. Contrasts between patients with affective disorders andpatients with schizophrenia on a neuropsychological test battery. American Journalof Psychiatry 150, 1355–1362.
Gruber, S.A.,Rosso, I.M., Yurgelun-Todd,D., 2008.Neuropsychologicalperformancepredictsclinical recovery in bipolar patients. Journal of Affective Disorders 105, 253–260.
Hamilton, M., 1960. A rating scale for depression. Journal of Neurology, Neurosurgeryand Psychiatry 12, 56–62.
29J. Townsend et al. / Psychiatry Research: Neuroimaging 182 (2010) 22–29
Hassel, S., Ladouceur, C., Kerr, N., Fissell, K., Almeida, J., Kupfer, D., Phillips, M.L., 2008.Increased ventral striatal activity but not amygdala to mild happy faces in euthymicbipolar disorder: comorbid anxiety, illness duration andmedication effects. BipolarDisorders 10, 916–927.
Hochberg, Y., Benjamini, Y., 1990. More powerful procedures for multiple significancetesting. Statistics in Medicine 9, 811–818.
Jenkinson, M., Smith, S., 2001. A global optimisation method for robust affineregistration of brain images. Medical Image Analysis 5, 143–156.
Jenkinson, M., Bannister, P., Brady, M., Smith, S., 2002. Improved optimization for therobust and accurate linear registration and motion correction of brain images.Neuroimage 17, 825–841.
Lagopoulos, J., Ivanovski, B., Malhi, G.S., 2007. An event-related functional MRI study ofworking memory in euthymic bipolar disorder. Journal of Psychiatry andNeuroscience 32, 174–184.
Lawrence, N.S., Williams, A.M., Surguladze, S., Giampietro, V., Brammer, M.J., Andrew, C.,Frangou, S., Ecker, C., Phillips, M.L., 2004. Subcortical and ventral prefrontal corticalneural responses to facial expressions distinguish patients with bipolar disorder andmajor depression. Biological Psychiatry 55, 578–587.
MacLeod, A.K., Buckner, R.L., Miezin, F.M., Petersen, S.E., Raichle, M.E., 1998. Rightanterior prefrontal cortex activation during semantic monitoring and workingmemory. Neuroimage 7, 41–48.
Malhi, G.S., Ivanovski, B., Hadzi-Pavlovic, D., Mitchell, P.B., Vieta, E., Sachdev, P., 2007.Neuropsychological deficits and functional impairment in bipolar depression,hypomania and euthymia. Bipolar Disorders 9, 114–125.
Martinez-Aran, A., Vieta, E., Reinares, M., Colom, F., Torrent, C., Sanchez-Moreno, J.,Benabarre, A., Goikolea, J.M., Comes, M., Salamero, M., 2004. Cognitive functionacross manic or hypomanic, depressed, and euthymic states in bipolar disorder.American Journal of Psychiatry 161, 262–270.
Martinez-Aran, A., Vieta, E., Colom, F., Torrent, C., Reinares, M., Goikolea, J.M., Benabarre, A.,Comes, M., Sanchez-Moreno, J., 2005. Do cognitive complaints in euthymic bipolarpatients reflect objective cognitive impairment? Psychotherapy and Psychosomatics 74,295–302.
Monks, P.J., Thompson, J.M., Bullmore, E.T., Suckling, J., Brammer, M.J., Williams, S.C.,Simmons, A., Giles, N., Lloyd, A.J., Harrison, C.L., Seal, M., Murray, R.M., Ferrier, I.N.,Young, A.H., Curtis, V.A., 2004. A functional MRI study of working memory task ineuthymic bipolar disorder: evidence for task-specific dysfunction. Bipolar Dis-orders 6, 550–564.
Morice, R., 1990. Cognitive inflexibility and pre-frontal dysfunction in schizophreniaand mania. British Journal of Psychiatry 157, 50–54.
Murphy, F.C., Sahakian, B.J., Rubinsztein, J.S., Michael, A., Rogers, R.D., Robbins, T.W.,Paykel, E.S., 1999. Emotional bias and inhibitory control processes in mania anddepression. Psychological Medicine 29, 1307–1321.
Nehra, R., Chakrabarti, S., Pradhan, B.K., Khehra, N., 2006. Comparison of cognitivefunctions between first- and multi-episode bipolar affective disorders. Journal ofAffective Disorders 93, 185–192.
Nystrom, L.E., Braver, T.S., Sabb, F.W., Delgado, M.R., Noll, D.C., Cohen, J.D., 2000. Workingmemory for letters, shapes, and locations: fMRI evidence against stimulus-basedregional organization in human prefrontal cortex. Neuroimage 11, 424–446.
Phillips, M.L., Travis, M.J., Fagiolini, A., Kupfer, D.J., 2008. Medication effects inneuroimaging studies of bipolar disorder. American Journal of Psychiatry 165,313–320.
Poldrack, R.A., 2006. Can cognitive processes be inferred from neuroimaging data?Trends in Cognitive Sciences 10, 59–63.
Rossi, A., Arduini, L., Daneluzzo, E., Bustini, M., Prosperini, P., Stratta, P., 2000. Cognitivefunction in euthymic bipolar patients, stabilized schizophrenic patients, andhealthy controls. Journal of Psychiatric Research 34, 333–339.
Roth, R.M., Koven, N.S., Randolph, J.J., Flashman, L.A., Pixley, H.S., Ricketts, S.M., Wishart, H.A.,Saykin, A.J., 2006. Functionalmagnetic resonance imaging of executive control in bipolardisorder. Neuroreport 17, 1085–1089.
Rubinsztein, J.S., Michael, A., Underwood, B.R., Tempest, M., Sahakian, B.J., 2006.Impaired cognition and decision-making in bipolar depression but no ‘affectivebias’ evident. Psychological Medicine 36, 629–639.
Semendeferi, K., Armstrong, E., Schleicher, A., Zilles, K., Van Hoesen, G.W., 2001.Prefrontal cortex in humans and apes: a comparative study of area 10. AmericanJournal of Physical Anthropology 114, 224–241.
Senturk, V., Goker, C., Bilgic, A., Olmez, S., Tugcu, H., Oncu, B., Atbasoglu, E.C., 2007.Impaired verbal memory and otherwise spared cognition in remitted bipolarpatients on monotherapy with lithium or valproate. Bipolar Disorders 9 (Suppl 1),136–144.
Siegle, G.J., Thompson, W., Carter, C.S., Steinhauer, S.R., Thase, M.E., 2007. Increasedamygdala and decreased dorsolateral prefrontal BOLD responses in unipolardepression: related and independent features. Biological Psychiatry 61, 198–209.
Silverstone, P.H., Bell, E.C., Willson, M.C., Dave, S., Wilman, A.H., 2005. Lithium altersbrain activation in bipolar disorder in a task- and state-dependent manner: an fMRIstudy. Annals of General Psychiatry 4, 14.
Smith, S.M., 2002. Fast robust automated brain extraction. Human Brain Mapping 17,143–155.
Smith, E.E., Jonides, J., 1998. Neuroimaging analyses of human working memory.Proceedings of the National Academy of Sciences, U S A 95, 12061–12068.
Strakowski, S.M., Adler, C.M., Holland, S.K., Mills, N., DelBello, M.P., 2004. A preliminaryFMRI study of sustained attention in euthymic, unmedicated bipolar disorder.Neuropsychopharmacology 29, 1734–1740.
Tam, W.C., Sewell, K.W., Deng, H.C., 1998. Information processing in schizophrenia andbipolar disorder: a discriminant analysis. Journal of Nervous and Mental Disease 186,597–603.
Thompson, J.M., Gray, J.M., Hughes, J.H., Watson, S., Young, A.H., Ferrier, I.N., 2007.Impaired working memory monitoring in euthymic bipolar patients. BipolarDisorders 9, 478–489.
Trivedi, J.K., Goel, D., Sharma, S., Singh, A.P., Sinha, P.K., Tandon, R., 2007. Cognitivefunctions in stable schizophrenia & euthymic state of bipolar disorder. IndianJournal of Medical Research 126, 433–439.
Trivedi, J.K., Dhyani, M., Sharma, S., Sinha, P.K., Singh, A.P., Tandon, R., 2008. Cognitivefunctions in euthymic state of bipolar disorder: an Indian study. CognitiveNeuropsychiatry 13, 135–147.
van Gorp, W.G., Altshuler, L., Theberge, D.C., Wilkins, J., Dixon, W., 1998. Cognitiveimpairment in euthymic bipolar patients with and without prior alcoholdependence. A preliminary study. Archives of General Psychiatry 55, 41–46.
Wager, T.D., Smith, E.E., 2003. Neuroimaging studies of working memory: a meta-analysis. Cognitive, Affective & Behavioral Neuroscience 3, 255–274.
Wagner, A.D., Desmond, J.E., Glover, G.H., Gabrieli, J.D., 1998. Prefrontal cortex andrecognition memory. Functional-MRI evidence for context-dependent retrievalprocesses. Brain 121 (Pt 10), 1985–2002.
Woolrich, M.W., Ripley, B.D., Brady, M., Smith, S.M., 2001. Temporal autocorrelation inunivariate linear modeling of FMRI data. Neuroimage 14, 1370–1386.
Woolrich, M.W., Behrens, T.E., Smith, S.M., 2004. Constrained linear basis sets for HRFmodelling using Variational Bayes. Neuroimage 21, 1748–1761.
Worsley, K.J., Poline, J.B., Friston, K.J., Evans, A.C., 1997. Characterizing the response ofPET and fMRI data using multivariate linear models. Neuroimage 6, 305–319.
Young, R.C., Biggs, J.T., Ziegler, V.E., Meyer, D.A., 1978. A rating scale for mania:reliability, validity and sensitivity. British Journal of Psychiatry 133, 429–435.
Yurgelun-Todd, D.A., Gruber, S.A., Kanayama, G., Killgore, W.D., Baird, A.A., Young, A.D.,2000. fMRI during affect discrimination in bipolar affective disorder. BipolarDisorders 2, 237–248.
Zhang, J.X., Leung, H.C., Johnson, M.K., 2003. Frontal activations associated withaccessing and evaluating information in working memory: an fMRI study.Neuroimage 20, 1531–1539.