finals ms2
TRANSCRIPT

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 1/323
TOPICS SUBTOPICS

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 2/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 3/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 4/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 5/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 6/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 7/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 8/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 9/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 10/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 11/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 12/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 13/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 14/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 15/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 16/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 17/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 18/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 19/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 20/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 21/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 22/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 23/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 24/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 25/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 26/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 27/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 28/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 29/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 30/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 31/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 32/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 33/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 34/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 35/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 36/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 37/323
CONTENT
ASSESSMENTCARDIOVACULAR
CARDIAC SIGNS AND SYMPTOMS
I. HEALTH HISTORY AND CLINICAL MANIFESTATIONS
1. Chest pain or discomfort (angina pectoris, Myocardial infarction, Valvular heart disease)
2. Shortness of breath or dyspnea (Myocardial infarction, Left ventricular Failure, Heart failure)
3. Palpitations (dysrythmias resulting from myocardial ischemia, valvular heart disease, ventricular aneurysm, stress,
4. Fatigue (earliest symptoms associated with several cardiovascular disorders)
5. Dizziness and syncope or loss of consciousness (postural hypotension, dysrythmias, vasovagal effect, cerebrovasc
6. Intermittent claudication characterized by extremity pain with exercise (this indicate peripheral vascular disease)
II. ASSESS FOR CHEST PAIN
a. Angina Pectoris
• Substernal or retrosternal pain spreading across chest; may radiate to inside of arm, neck or jaw.
• 5-15 minutes in duration
• Usually related to exertion, emotion, eating, cold and smoking
• Rest, nitroglycerine, oxygen are the relieving measures
b. Myocardial Infarction
• Substernal pain or pain over precordium; may spread widely throughout chest. Pain in shoulders and hands may b
• 15 minutes in duration
• Occurs spontaneously but may be squeal to unstable angina.
• Morphine sulfate is the relieving measure
c. Pleuritic pain• Pain arises from inferior portion of pleura; may be referred to costal margins or upper abdomen. Patient may be ab
• 30 + minutes in duration
• Often occurs spontaneously. Pain occurs or increases with inspiration
• Rest, time is the relieving measures
d. Pericarditis
• Sharp, severe substernal pain or pain to the left sternum; may be felt in epigastrium and may be referred to neck,
• The duration is intermittent
• Sudden onset. Pain increases with inspiration, swallowing, coughing, and rotation of trunk.
• Sitting upright, analgesia, anti-inflammatory medications are the relieving measures
e. Esophageal pain
• Substernal pain; may be projected around chest to shoulders
• 5-60 minutes in duration
• Recumbency, cold liquids and exercise. May occur spontaneously
• Food, antacid, nitroglycerine are the relieving measures

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 38/323
HEAD TO TOE EXAMINATION
CORONARY ARTERY DISEASE
Non Modifiable Risk Factor
f. Anxiety
• Patient may complain of numbness and tingling of hands and mouth
• 2 –3 minutes in duration
• Stress, emotional tachypnea
• Removal of stimulus and relaxation are the relieving measures
III. PHYSICAL ASSESSMENT
A Physical Examination is performed to confirm the data obtained in the health history. In addition to observing the pshould include the evaluation of the following:
1. Effectiveness of the heart as a pump
2. Filling volumes and pressures
3. Cadiac output
4. Compensatory mechanisms
1. General Appearance
2. Cognition
3. Skin
4. Blood pressure
5. Arterial pulses
6. Jugular Venous Pulsation and Pressures
7. Heart
8. Extremities
9. Lungs
10. Abdomen
• A narrowing or obstruction of one or more coronary arteries as a result of atherosclerosis
• An accumulation of lipid-containing plaque in the arteries
• Causes decreased perfusion of myocardial tissue and inadequate myocardial oxygen supply.
• Can cause angina, dysrythmias, myocardial infarction, heart failure and death.
• Collateral circulation, more than one artery supplying a muscle with blood, is normally present in coronary arteries
• Symptoms occur when the coronary artery is occluded to the point that inadequate blood supply to the muscle occ
• Coronary artery narrowing is significant if the lumen diameter of the left main artery is reduced at least 50%, or if a
• The goal of treatment is to alter the atherosclerotic progression.
ü Family History of Coronary Heart Disease (CHD)
ü Increasing age
ü Gender (3x in men)
ü Race (Africans Americans)

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 39/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 40/323
ANGINA PECTORIS
A. Provides the most definitive source of diagnosis
B. Shows the presence of atheroslerotic lesions
• Assess O2 level, pulmonary blood flow, Cardiac Output, heart structures
• Coronary artery visualization; use to diagnose CAD; assess coronary patency a
• R sided heart catheterization – medial cubital or brachial vein
• L sided heart catheterization – brachial or femoral artery
4. Blood Lipids Levels
• May be elevated
• Cholesterol-lowering medications may be prescribed to reduce the developmen
C. Implementation
1. Instruct client regarding the purpose of diagnostic medical surgical procedures expectations2. Assist the client to identify risk factors that can be modified
3. Assist the client to set goal to promote lifestyle changes that will reduce the impact of risk factors
4. Assist the client to identify barriers to compliance with the therapeutic plan and to identify methods to overcome ba
5. Instruct the client regarding a low-calorie, low-sodium, low-cholesterol, and low-fat diet, with an increase in dietary
6. Stress to the client that dietary changes are not temporary and must be maintained for life; instruct the client regard
7. Provide community resources to the client regarding exercise, smoking reduction, and stress reduction.
D. Surgical Procedure
1. Percutaneous Transluminal Coronary Angioplasty (PTCA) to compress the plaque against the walls of the arte
2. Laser angioplasty to vaporize the plaque
3. Atherectomy to remove the plaque from artery4. Vascular stent to prevent the artery from closing to prevent restenosis
5. Coronary Artery Bypass graft improve flow to the myocardial tissue that is at risk for ischemia or infarction becau
E. Medications
A. Nitrates to dilate coronary arteries to decrease preload and afterload.
B. Calcium channel blockers to dilate coronary arteries and reduced vasospasms.
C. Cholesterol-lowering medications to reduce the development of atherosclerotic plaques
D. Beta-blockers to reduce blood pressures in individuals who are hypertensive
A. Description
a. Chest pain resulting from Myocardial Ischemia caused by inadequate myocardial blood and oxygen supply
b. Caused by imbalance between oxygen supply and demand
c. Causes include obstruction of coronary blood flow because of atherosclerosis, coronary artery spasm and condition
d. The goal of treatment is to provide relief of an acute attack, correct imbalance between the myocardial oxygen sand further attack to reduce the risk of MI

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 41/323
Associated with the acute coronary insufficiency
Last longer than 15 minutes
Symptoms of worsening cardiac ischemia
B. Patterns of Angina
a. Stable Angina
• Also called exertional angina
• Occurs with activities that involved exertion or emotional stress, and is relieved
• It is usually has a stable pattern of onset, duration, severity, and relieving factor
b. Unstable Angina• Also called preinfarction angina
• Occurs with unpredictable degree of exertion or emotion and increase the occur
• Pain may not be relieved with Nitroglycerine
c. Variant Angina
• Also called Prinzmetal’s or Vasospastic Angina
• Result from coronary artery spasm, similar to classic angina but last longer
• May occur at rest
• Attack may be associated with ST segment division noted on the ECG
d. Intractable Angina
• A chronic incapacitating angina that is unresponsive to intervention
e. Preinfarction Angina
f. Post infarction
• Occurs after MI, when residual ischemia may cause episode of angina
C. Assessment
1. Pain
2. Dyspnea
3. Pallor
4. Sweating
5. Palpitations and tachycardia
6. Dizziness and faintness
7. Hypertension
8. Digestive disturbance
D. Diagnostic Study
1. ECG: normal during rest, with ST depression or elevation and/or T wave inversio
2. Stress Test: Pain or changes in the ECG or vital signs during testing may indicat
3. Cardiac Enzymes: Normal findings in Angina
4. Cardiac Catheterization: Provides a definitive diagnosis by providing information
E. Implementations
1. Immediate management
• Assess pain
8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 42/323
MYOCARDIAL INFARCTION
• Provide bed rest
• Administer oxygen at 3 L nasal cannula as prescribe by the doctor
• Administer Nitroglycerine as prescribe to dilate coronary arteries, reduced the oxygen requirements of the myocar
• Obtain a 12-lead ECG
2. Following Acute Episodes
• Instruct the client regarding the purpose of diagnostic medical and surgical procedure and the pre procedure and p• Assist the client to identify angina-precipitating event
• Instruct the client to stop activity and rest if the chest pain occurs and to take nitroglycerine as prescribe
• Instruct the client regarding the prescribe medication
• Instruct client to seek medical attention if pain persist
• Provide diet instruction to the client, stressing the dietary changes are not temporary and must be maintain for life
• Assist the client to identify risk factor that can be modified
• Assist the client to set goals that will promote changes in lifestyle to reduce impact of risk factor
• Assist the client identify barriers to compliance with therapeutic plan to identify methods to become barriers
• Provide community resources to the client regarding exercise and stress reduction
F. Medications
1. Refer medication to treat Coronary Artery Disease
2. Antiplatelet therapy to inhibit platelets aggregation and reduce the risk of developing an Acute MI
A. Description
• Occurs when Myocardial Tissues is abruptly and severely deprived of oxygen.
• Ischemia can lead to necrosis of myocardial tissue if blood flow is not restored.
• Infarction does not occur instant but evolves over several hours
• Obvious physical changes do not occur in the heart until 6 hours after the infarction, when the infarction area appe
• After 48 hours, the infarction turns to gray with yellow steaks as neutrophils invade the tissue
• By 6 – 10 days after infarction, granulation to tissue forms
• Over 2 –3 months, the necrotic area develops into scar, scar tissue permanently changes the size and shape of th
B. Location Of Myocardial Infarction
• Obstruction of the left anterior descending (LAD) artery results in the anterior se
• Obstruction of the circumflex results in the posterior wall MI or lateral wall MI
• Obstruction of the right coronary artery results in the inferior wall MI
C. Risk Factors
• Atherosclerosis
• Coronary Artery Disease
• Elevated Cholesterol Levels
• Smoking

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 43/323
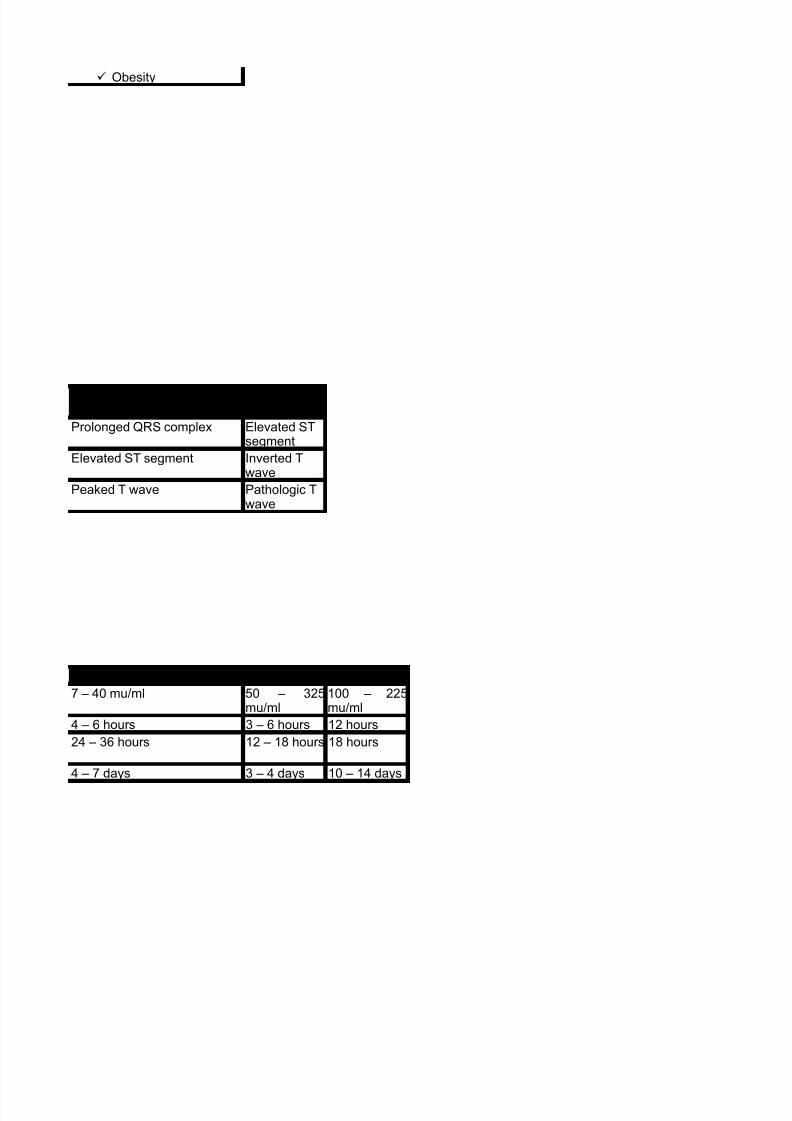
• Hypertension
• Obesity
• Physical Inactivity
• Impaired Glucose Tolerance
• Stress
D. Diagnostics Study A. Total Creatinine Kinase
a. Rise within 3 hours after the onset of chest pain
b. Peak within 24 hours after the damage and death of the tissue
B. Creatinine Phosphokinase-MB isoenzymes
a. Peak elevation occur 12 –24 hours after the onset of the chest pain
b. Levels returns to normal 48 – 72 hours later
C. Troponin Level
a. Rise within 3 hours
b. Remain elevated for up to 7 days
D. Myoglobin
a. Rises within 1 hour after cell death, peaks in 4 – 6 hours and returns to normal within 24- 36 hours or less
E. Lactate Dehydrogenase (LDH) Levels
a. Rises within 12 –24 hours after MI
b. Peak between 40 – 72 hours and fall to normal in 7 days
c. Serum levels of LDH isoenzymes rise higher than serum level of LDH2
F. White Blood Cells (WBC) counts
a. An elevated white blood cell counts of 10,000-20,000 cells/mm3 appears on the second day following after the MI a
G. Electrocardiogram (ECG)
a. ST segment elevation, T wave inversion, abnormal Q wave
b. Hours to days after MI; ST and T wave changes will return to normal but the Q wave usually remain permanently
H. Diagnostic Test for The Acute Stage
a. Exercise tolerance test or stress test may be prescribed to assess for ECG changes and ischemia to evaluate fotherapy
b. Thallium Scan may be prescribed to assess for ischemia or necrotic muscle tissue
c. Cardiac catheterization: performed to determine the extent and location of the obstruction of the coronary artery
E. Assessment
1. Pain
2. Nausea and vomiting
3. Diaphoresis
4. Dyspnea
5. Dysrhytmia
6. Feeling of fear and anxiety
7. Pallor, cyanosis, coolness of the extremities

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 44/323
CANCER
Definition of Terms:
Carcinogenesis: the origin of cancer
AGENTS THAT CAN PREDISPOSE TO CANCER:
1. Chemical carcinogens-( tobacco, ether, benzene, coal tar and asbestos)
8. Feeling of doom, restlessness
F. Complications of Myocardial infarctions
1. Dysrythmias
2. Heart failure
3. Pulmonary Edema
4. Cardiogenic Shock
5. Thrombophlebitis
6. Pericarditis
7. Mitral valve insufficiency
8. Post Infarction Angina
9. Ventricular Rupture
10. Dressler’s Syndrome (a combination of pericarditis, pericardial effusion, which can occur several weeks to months
G. Implementations of Myocardial Infarctions
1. Obtain description of chest discomfort
2. Assess vital signs
3. Assess cardiovascular status and maintain cardiac monitoring
4. Obtain 12 lead ECG5. Administer nitroglycerine as prescribed
6. Administer morphine sulfate as prescribe to release chest discomfort that is unre
7. Administer oxygen at 2 – 4 L by nasal cannula as prescribe
8. Place the client in semi-fowlers position to enhance comfort and tissue oxygenat
Cancer- a group of diseases in which cells multiply w/o restraint, destroys healthy tissue, & endangers
Neoplasia – new, altered and abnormal development of cells that may be benign or malignant
Tumor – mass or swelling in or on the body
Anaplasia – means lack of differentiation
Biopsy – the removal & examination of tissue from the living body
Carcinogenesis – development of cancerous cells from normal ones
Carcinoma – any malignant tumor derived from epithelial tissue
Chemotherapy – treatment of disease, especially cancer, by means of chemical agents/drugs
Dysplasia – means deranged development, disordered maturation
Hyperplasia – constitutes an increase in the number of cells in organ or tissue, which may then have i
Proliferation- refers to the process of cell renewal or replacement. In cancer, proliferation process con
Differentiation- refers to the process by which cells diversify, acquire specific structural and functiona
Cellular Transformation & Derangement Theory= normal cells may be transformed into cancer cel
Failure of the Immune Response Theory= all individuals possess cancer cells, however, cancer cells
Ø These act by causing cell mutation or alteration in cell enzymes & proteins causing altered c

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 45/323
2. Physical Agents
4. Viruses- these viruses are called oncogenic viruses. They infect the host DNA or RNA resulting in ce
5. Immune system alterations- as seen in patients with immunodeficiency disease, the elderly and tho
6. Hormonal factors- hormones make the cell more sensitive to the process of carcinogenesis or may
7. Dietary factors- some studies link dietary factors to cancer development. High fat diet and low fiber
PREDISPOSING FACTORS
1. Age – older people are more prone. This is a very important factor for cancer development.
2. Sex – women for breast, men for prostate
3. Urban versus Rural residence
4. Geographic distribution
5. Occupation
6. Heredity
7. Stress
8. Precancerous lesions- these can lead to transformation into Cancer
9. Obesity [breast and colorectal]
WARNING SIGNALS OF CANCER [CAUTION] by the American Cancer Society (ACS)
SITE OF CANCER and DANGER SIGNAL
CHARACTERISTICS OF BENIGN & MALIGNANT NEOP
Characteristics
Speed of Growth
o Radiation Physical irritation/trauma, ultraviolet rays form diagnostic or therapeuti
o These will usually cause cancer after long time of exposure and interaction
3. Genetics. The human DNA has specific genes for cancer called= Oncogene. When this gene is exp
C – Change in bowel or bladder habits
A – A sore that does not heal
U – Unusual bleeding/discharge; unexplained anemia and sudden weight loss
T – Thickening or lumps in breast or elsewhere
I – indigestion or difficulty of swallowing
O – Obvious change in wart or mole
N – Nagging cough or hoarseness of voice
1. Breast – lump or thickening in breast
2. Colon & rectum – change in bowel habits/bleeding
3. Kidney & bladder – urinary difficulty/bleeding
4. Lung – persistent cough/lingering respiratory ailment
5. Prostate – urinary difficulty
6. Mouth, larynx & pharynx – sore that does not heal, difficulty in swallowing & hoarseness
7. Skin – sore that does not heal, change in wart or mole
8. Stomach – indigestion
9. Uterus – unusual bleeding or discharge
Mode of Growth Remains localized

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 46/323
Capsule
Metastasis
Effect of neoplasm
Prognosis
Distinguishing Characteristics of Neoplastic cells
PATHOPHYSIOLOGIC BASIS OF MALIGNANT NEOPLASM
HOW CANCER SPREADS: Metastasis
Pathways of Spread:
-Liver & lungs – most frequently involved in hematogenous dissemination
PRIMARY PREVENTION OF CANCERS
Avoid exposure to sunlight, use protective sunscreen, limit sun exposure bet 10am-3pm
Avoid artificial sources of UV light
Avoid environmental l & occupational carcinogens [arsenicals, pesticides, coal tar products]
Avoid frequent exposure to ionizing radiation,
X-rays & radioisotopes
Avoid high-fat foods
Reduce weight; avoid obesity
Do not smoke, avoid secondhand smoke
Avoid environmental & occupational carcinogens [asbestos, hydrocarbons, radon]
Wear protective clothing & mask when exposed to carcinogens
Annual CXR
Cell characteristics Well differentiated Poorly differentiated
Recurrences Extremely unusual Common following su
• 1. Direct seeding of body cavities or surfaces
• 2. Lymphatic spread
• 3. Hematogenous spread
• 4. Direct transplantation of tumor cells: (ex: on surgical instrument) – theoretically, it can occur bu
1. Skin
2. Oral. Annual oral examination.
3. Breast. Monthly BSE from age 20-21
4. Lung
Predisposing Factors/Etiologic Factors
Cellular Aberrations
Cancer Cell ProliferationDisrupt Normal cell growth &Interfere w/ tissue function
Malignant cells produceenzymes, hormones &other substances
ü Pressureü Obstructionü Painü Effusionü Thrombosis,üEmbolusüthrombophlebitis
(Paraneoplastic Syndrome)ü Anemiaü Hypercalcemiaü Edemaü DIC

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 47/323
Avoid high-fat foods
Limit intake of alcohol
Avoid occupational carcinogens
Digital rectal examination [> 40y/o]; rectal biopsy, proctoscopic examination,
Reduce fat intake to no > 30% of caloriesAvoid salt-cured & nitrite-cured foods
Reduce weight, avoid obesity
Annual Pap’s smear from age 40.
DIETARY RECOMMENDATIONS AGAINST CANCER
Avoid obesity
Cut down on total fat intake
Increase intake of high fiber foodsInclude foods rich in Vitamin A & C in daily diet
Include cruciferous vegetables [broccoli, cauliflower, cabbage, Brussels sprouts]
Moderate consumption of alcoholic beverages
Moderate consumption of salt-cured, smoked-cured and nitrate-cured foods
CANCER EARLY DETECTION
THERAPEUTIC MODALITIES FOR CANCER and the GOALS OF CA
Surgery
Radiotherapy
Chemotherapy
5. Prostate
6. Colorectal.
7. Uterus
8. Basic. Annual PE and blood examination.
§ Breast self-examination [BSE]
• Done 1x a month, 1 wk after the 1st day of menstruati
§ Testicular self-examination [TSE]
• Done by males 15-35 y/o, monthly preferably after a w§ Mammography
• Baseline at 35-39y/o, then every 1-2 yrs
§ Papanicolau smear
• Every 3yrs after 3 negative test for three consecutive
§ Rectal digital examination
• Yearly starting at age 40 / yearly at >50yo
1. Cure- the aim of this modality is to make sure that the client will be disease-free & live norm
2. Control- this modality deals with cancer not cured but controlled by therapy over long period
3. Palliative- cure & control not possible but maintain as high as quality for the client
Ø May be done for curative, palliative, reconstructive, preventive and prophylactic purposes.
Ø Used for radiosensitive cancers like skin cancer, seminoma and early stage Hodgkin’s. the r
Ø This involves administering cytotoxic drug to intervene and interrupt the cell cycle.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 48/323
Immunotherapy or biotherapy
Surgical Interventions
Preventive. Removal of precancerous lesions/benign tumors
Diagnostic. Biopsy
Curative. Removal of an entire tumor [en bloc resection]Reconstructive. Improvement of structure/function of an organ
Palliative. Relief of distressing signs & symptoms [oophorectomy w/ breast Ca to reduce estrogen sec
Chemotherapy
Nursing Interventions for Chemotherapeutic Side-Effects
Radiation Therapy
Ø Involves treatment with agents derived from biologic sources or with agents that affect biol
Ø use of drugs to retard the growth of or destroy cancerous cells
Ø use to cure, for palliation, combined w/ surgery, combined with radiation
• Classification/Effect
ü Anti-neoplastic agents
§ Cell-cycle specific: attack cells at a specific point in the process of cell div
§ Cell-cycle non-specific: act at one time during cell division
ü Hormones.§ Alter hormone balance
§ Modify growth of hormone-dependent tumor
• Administration
ü IV – most common route
ü Arterial infusion - direct
ü Regional perfusion
ü Intraperitoneal
ü Oral, IM [less common]
q GI system
N & V= Antiemetic are given
Diarrhea. Replace fluid-electrolyte losses, low-fiber diet
Constipation. increased fluid intake & fibers
q Integumentary system
Pruritus, urticaria. Provide good skin care
Stomatitis. Provide good oral care; avoid hot & spicy food
Alopecia/skin pigmentation/nail changes. Reassure that it is temporary
q Hematopoeitic
Anemia. Provide frequent rest periods
Neutropenia. Protect from infection. Avoid people with infection, crowds Thrombocytopenia. Protect from trauma. Avoid ASA
q Genito-Urinary system
Hemorrhagic cystitis. Provide 2-3L fluids/day
Urine color changes. Reassure that it is harmless
q Reproductive system
Premature menopause/amenorrhea. Reassure menstruation resumes a

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 49/323
Principles of Radiation Protection [DTS]
Nursing Interventions for Radiotherapy Side-Effects
Nursing Interventions for Radiotherapy Side-Effects
Nursing Interventions for Radiotherapy Side-Effects
Ø use of ionizing radiation to cause damage and destruction to cancerous growths
q Effect: Radiation → damage at the cellular level
§ indirectly: water molecules w/in the cell are ionized
§ directly: causes strand breakage in the double helix of DNA
§ Not every cell is damaged beyond repair
q use to cure, for palliation, combined w/ surgery
ü PreOP: to reduce size of tumor
ü PostOP: to retard or control metastasis
q Administration
ü External
§ Orthovoltage machines –superficial lesions
§ Megavoltage (Co-60) – deeper structures
§ Linear accelerators – deep lesions; less harmful
ü Internal [Brachytherapy]
§ Sealed [implants
§ Unsealed [radioactive iodine]
q Distance
ü Maintain a distance of at least 3 ft. when not performing nursing proced
q Time
ü Limit contact for 5 min each time, a total of 30min/shift.
q Shielding
ü Use lead shield during contact with client.
q Skin reactions [erythema, desquamation, atrophy, necrotic/ulcerative lesions, dep
ü Keep area dry
ü Wash area w/ water, no soap, pat dry, do not rub
ü Do not apply ointments, powders or lotion, heat
ü Use soft cotton fabrics for clothing
q Bone marrow suppression
ü Monitor blood counts weekly
ü Good personal hygiene, nutrition, adequate rest
ü Teach signs of infection to report to physician
q Hemorrhage [Platelets are vulnerable to radiation]
ü Monitor platelet count
ü Avoid physical trauma or use of aspirin
ü Teach signs of hemorrhageü Monitor stool & skin for signs
ü Use direct pressure over injection sites until bleeding stops
q Fatigue [Results from high metabolic demands for tissue repair & toxic waste rem
ü Plenty of rest and good nutrition
q Stomatitis
ü Administer analgesics before meals

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 50/323
Immunotherapy
Bone Marrow Transplantation
DIAGNOSTIC TESTS
Only with understanding of the most common laboratory examination can the nurse provide the patient with clear e
2. CYTOLOGIC tests
3. ENDOSCOPY
ü Bland diet, no smoking/alcohol
ü Good oral hygiene/ saline rinse q 2 hrs
ü Sugarless lemon drops or mint to ↑ salivation
q Weight loss [anorexia, pain & effect of Ca]
q Diarrhea
q Nausea & vomiting
q Headache
q Hair loss/ alopecia
q Cystitis
q Social isolation
Ø Use of biologic response modifiers that have ability to alter immunologic relations
q Types:
ü Interferons
ü Monoclonal antibodies
ü Lymphokines & cytokines [interleukin –2]
ü Colony stimulating factors
q Side effects
ü Influenza-like ss, fatigue, leukopenia, N&V
q used to treat
ü Acute lympphoblastic leukemia
ü Acute myelogenous leukemia
ü Aplastic anemia
ü Chronic myelogenous leukemia
q Types:
ü Allogeneic BMT: bone marrow comes from a healthy donor [usually imm
ü Autologous BMT: client is given own bone marrow
1. BLOOD TESTS
• Blood chemistries, complete blood count and other specialized assay can provide important info
• Tumor markers can be used to measure hormones, oncofetal proteins secreted by malignant tu
• These tests help detect suspected primary or metastatic disease and monitor therapy• They cannot determine the location and size of a malignancy
• ASPIRATION TESTS- fine needle aspiration of body fluids permits evaluation of a palpable mass, a l
• BONE MARROW ANALYSIS allows examination of bone marrow aspirate to identify leukemic cells.
• PAPANICOLAOU TESTS- is widely used to detect cervical cancer, endometrial and extrauterine malig
• These can be performed on the entire GIT, respiratory tract, urinary tract and peritoneal cavity.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 51/323
4. HISTOLOGIC TESTS
5. NUCLEAR imaging and Scanning
6. RADIOGRAPHIC test
7. Ultrasonography
8. STOOL OCCULT EXAMINATION
GENERAL Promotive and Preventive Nursing Management
1. Lifestyle Modification
2. Nutritional management
3. Screening
4. Early detection
Nursing Interventions for CancerMAINTAIN TISSUE INTEGRITY
MANAGEMENT OF STOMATITIS
MANAGEMENT OF ALOPECIA
Alopecia begins within 2 weeks of therapy
MANAGEMENT TO PROMOTE NUTRITION
• Biopsy is a common procedure that provides a detailed description that helps classify malignancy
• Include CT, MRI and Radionuclide imaging
• Are used to visualize internal body structures to detect, identify, and localize malignancy and guide
• These include CXR, mammography
• This non-invasive procedure is used to evaluate organs and localize masses except the lungs and bo
• Permits early detection of colorectal cancer, providing positive results in 80% of patients with this d
¯ Handle skin gently
¯ Do NOT rub affected area
¯ Lotion may be applied
¯ Wash skin only with SOAP and Water
Use soft-bristled toothbrush
Oral rinses with saline gargles/ tap water
Avoid ALCOHOL-based rinses
Ø Regrowth within 8 weeks of termination
Ø Encourage to acquire wig before hair loss occurs
Ø Encourage use of attractive scarves and hats
Ø Provide information that hair loss is temporary BUT anticipate change in texture and color
Ø Serve food in ways to make it appealing
Ø Consider patient’s preferences
Ø Provide small frequent meals
Ø Avoids giving fluids while eating
Ø Oral hygiene PRIOR to mealtime
Ø Vitamin supplements

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 52/323
MANAGEMENT TO RELIEVE PAIN
Moderate pain- Weak opiods (meperidine)
MANAGEMENT TO DECREASE FATIGUE
MANAGEMENT TO IMPROVE BODY IMAGE
MANAGEMENT TO ASSIST IN THE GRIEVING PROCESS
MANAGE COMPLICATION: INFECTION
MANAGE COMPLICATION: Bleeding
CHEMOTHERAPEUTIC AGENTS
Ø Mild pain- NSAIDS
Ø Severe pain- Morphine
Ø Administer analgesics round the clock with additional dose for breakthrough pain
Ø Plan daily activities to allow alternating rest periods
Ø Light exercise is encouraged
Ø Small frequent meals
Ø Therapeutic communication is essential
Ø Encourage independence in self-care and decision making
Ø Offer cosmetic material like make-up and wigs
Ø Some cancers are curable
Ø Grieving can be due to loss of health, income, sexuality, and body image
Ø Answer and clarify information about cancer and treatment options
Ø Identify resource people
Ø Refer to support groups
Ø Fever is the most important sign (38.3 Celsius)
Ø Administer prescribed antibiotics X 2weeks
Ø Maintain aseptic technique
Ø Avoid exposure to crowds
Ø Avoid giving fresh fruits and veggie
Ø Hand-washing
Ø Avoid frequent invasive procedures
Ø Thrombocytopenia (<100,000) is the most common cause
Ø <20, 000à spontaneous bleeding
Ø Use soft toothbrush
Ø Use electric razor
Ø Avoid frequent IM, IV, rectal and catheterization
Ø Soft foods and stool softeners
• These are drugs that are utilized to destroy cancer cells by interfering with neoplastic cell growth an

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 53/323
NURSING CARE OF TERMINALLY ILL PATIENT
1. Nutrition
2. Activity
3. Prevent tissue breakdown & vascular complications
4. Observe for toxic reactions to tx [diarrhea]
5. Supportive measures & drugs for pain relief
6. Maintain open communication with patient & family
7. Control of odor
VEHICULAR ACCIDENT
• The following are included: Alkylating agents, nitroureas, antimetabolites, Plant alkaloids, anti-tumo
1. ALKYLATING AGENTS
• These agents produce breaks in the DNA and are most effective in the S (synthesis) pha
• examples are busulfan, carboplatin, chlorambucil, cisplatin and cyclophosphamide
2. NITROSOUREAS
• Act in the same manner as alkylating agents but they can pass the brain barrier because they
• Examples are carmustine, lomustine and steptozocin
3. ANTIMETABOLITES
• They interfere with DNA synthesis and inhibit purine synthesis
• Examples are: Mercaptopurine, 5-FU, Cytarabine and Thioguanine
4. PLANT ALKALOIDS
• They kill cancer cells by inhibiting mitosis and the vital enzymes that protect the DNA strands
• Examples are paclitaxel, doxetaxel, vinblastine and vincristine
5. ANTIBIOTIC anti-neoplastics
• Achieve their effects by binding with DNA
• Examples are bleomycin, dactinomycin, doxorubicin and mitomycin
6. HORMONAL ANTINEOPLASTICS
• Useful in treating cancer because they inhibit neoplastic growth in specific tissues without dir
• Examples are tamoxifen, aminogluthetimide, androgens, mitotane, corticosteroids
Ø Directed towards making the pt. physically & psychologically as comfortable as po
q High calorie & protein diet
q Small frequent feedings
q ↑ fluids intake, 1000-1500ml above the N
q Frequent turning, skin massage, air mattresses
q Active and passive ROM
Ø Directed towards making the pt. physically & psychologically as comfortable as po
q Infectious organisms cause formation of offensive odors
q Frequent change of dressings

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 54/323
WOUNDS
Types of Wounds
Management
• An unforeseen and unplanned event or circumstance frequently causing loss or injury in an
• Wounds involving injury to soft tissues can vary from minor tears to severe crushing i
• The primary goal is to restore the physical integrity and function of the injured tissue, w
• Proper documentation of the wound, using precise descriptions and correct terminolo
• Such information may be needed in the future for forensic evidence. Photographs are
• Determining When and How the wound occurred is important, because a treatment de
• Using aseptic technique, the clinician inspects the wound to determine the extent of d
• Sensory, motor, and vascular function are evaluated for changes that might indicate c
• Laceration – skin tear with irregular edges and vein bridging
• Avulsion – tearing away from supporting structures
• Abrasion – denuded skin
• Hematoma – tumor-like mass of blood trapped under the skin
• Ecchymosis/Contusion – blood trapped under the surface of the skin
• Stab – incision of the skin with well-defined edges, usually caused by a sharp instruments
• Cut – incision of the skin with well-defined edges, usually longer than deep
• Patterned – wound representing the outline of the objects
• Hair around the wound maybe clipped or shaved (only as directed) if it is anticipated that th
• Typically, the area around the wound is cleaned with normal saline solution or a polymer ag

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 55/323
TRAUMA
CRUSH INJURIES
Assessment and Diagnostic Findings
Management
• Antibacterial agents, such as povidone-iodine (Betadine) or hydrogen peroxide, should not
• If indicated, the area is infiltrated with a local intradermal anesthetic through the wound mar
• The nurse then assists the physician, nurse practitioner, or physician assistant in cleaning a
• The wound is irrigated gently and copiously with sterile isotonic saline solution to remove su
• Devitalized tissue and foreign matter are removed because the impede healing and may en
• Any small bleeding vessels are clamped or tied. Alternatively, hemostasis maybe achieved
• After wound treatment, a nonadherent dressing is commonly applied to protect the wound.
• The dressing serve as a splint and also as a reminder to the patient that the area is injured.
• The unintentional or intentional wound or injury inflicted on the body for a mechanism again
• Occurs when a person is between caught between objects, run over by a moving vehicle or
• Hypovolemic shock resulting from extravasation of blood and plasma into injured tissues af
• Paralysis of a body part
• Erythema and blistering of the skin
• Damaged body parts (usually an extremity) appearing swollen, tense and hard.
• Renal dysfunction (prolonged hypotension causes kidney damage and acute renal insufficie
• In conjunction with maintaining the airway, breathing, and circulation, the patient is observe
• Injury to the back can cause severe kidney damage. Severe muscular damage causes a sig

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 56/323
MULTIPLE INJURIES
Assessment and Diagnostic Findings
• Major soft tissue injuries are splinted early to control bleeding and pain. Again, the serum la
• If an extremity is involved, it is elevated to relieve swelling and pressure.
• To restore neurovascular function, the physician may perform Fasciotomy (surgical incision
• Medications for pain and anxiety are then administered as prescribed, and the patient is qu
• Hyperbaric chamber can be used for hyperoxygenation of the crushed tissue, if indicated.
• Care of the patient with multiple injuries requires a team approach, with one person respon
• After injury, the body is hypermetabolic, hypercoagulable, and severely stressed.
• Mortality in patients with multiple injuries is related to the severity of the injuries and the num
• Potentially affects every body system.
• The nursing staff assumes responsibility for assessing and monitoring the patient, ensuring
• X-ray
• Physical Evidences (eg Hematoma, Lacerations, etc..)
• CT Scan
• MRI
• EEG or ECG

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 57/323
Management
PERSONAL INJURY
Is any physical or mental injury to a person that results from another person’s negligence or harmfu
Auto Accidents
Other Vehicle Accidents (Aviation, Bicycle, Boat, Motorcycle, Railroad, Truck)
Construction/On the Job Accidents
Dangerous or Defective Products
Medical Malpractice (Misdiagnosis, Surgical Negligence)
Nursing Home Abuse and Neglect
Construction Accidents
Product Liability
Scope and Practice of Emergency Nursing
Issues in Emergency Nursing Care
Documentation of Consent
Consent to examine and treat the patient is part of the ED record. The patient must consent to
Limiting Exposure to Health Risk
• The goals of treatment are to determine the extent of injuries and to establish priorities of tr
• Any injury interfering with a vital physiologic function (eg airway, breathing, circulation) is an
• Essential life-saving procedures are performed simultaneously by the emergency team.
• Clothes are usually cut off, and a rapid physical assessment is performed.
• Transfer from field management to the ED must be orderly and controlled, with attention giv
Ø The emergency nurse has had specialized education, training, and experience to gain e
Ø These issues include legal issues occupational health and safety risk for ED staff, and t
• Increasing numbers of people infected with hepatitis B and with Hu
o Providing Holistic Care

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 58/323
Principles of Emergency Care
Triage
Assess and Intervention
• Sudden illness or trauma is a stress to physiologic and psychologic
ü Patient –focused intervention
ü Family- focused intervention
v Anxiety and Denial
v Remorse and Guilt
v Anger v Grief
o Emergency Nursing and the Continuum of Care
• One principle underlying emergency care is that the patient will be
o Discharge Planning
§ Before discharge, instructions for continuing care are given to the pat
o Community Service
§ Before discharge, some patients require the services of a social work
§ Emergency in this age group may be more difficult to manage becaus
ü An atypical presentation
ü An altered response to treatment
ü A greater risk of developing complications
Ø Emergency care is care that must be rendered without delay.
• Word Triage comes from the French word trier, meaning “to sort”.
• A basic and widely used system uses three categories:
o Emergent- patients have the highest priority, their conditions are life
o Urgent- patients have serious health problems, but not immediately
o Non-urgent- patients have episodic illness that can be addressed w
• A fourth increasingly used class is “fast-track” these patients requir
• Patient with an emergency or urgent health problem stabilization, p
• The primary survey focuses on stabilizing life-threatening condition
• The ED staff work collaboratively and follow the ABCD (airway, bre
o Establish a patent airway

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 59/323
AIRWAY OBSTRUCTION
Acute upper airway obstruction is a life threatening medical emergency.The airway may be partially or completely occluded.
If the airway is completely obstructed, permanent brain damage or death will occur within 3 to 5 minutes se
Partial obstruction of the airway can lead to progressive hypoxia, hypercarbia, and respiratory and cardiac a
PATHOPHYSIOLOGY
Aspiration of foreign bodies.
Anaphylaxis.
Viral or Bacterial infection
Trauma
Inhalation of chemical burnAspiration of bolus meat is the most common cause of airway obstruction in adults.
In children, Peritonsillar abscesses, epiglottitis, and other acute infectious processes of the posterior pharyn
CLINICAL MANIFESTATION
Choking
Apprehensive appearance
Inspiratory and expiratory stridor
Labored breathing
Use of accessory muscle ( suprasternal and intecostal refraction)Flaring nostrils
Increasing anxiety
Restlessness
Confusion
ASSESSMENT AND DIAGNOSTIC FINDINGS
Assessment of the patient who has a foreign object occluding the airway may involve simply asking the per
o Provide adequate ventilation, employing resuscitation measures whe
o Evaluate and restore cardiac output by controlling hemorrhage preve
o Determine neurologic disability by assessing neurologic function usin
• After these priorities have been addressed the ED team proceeds
o A complete health history and head to toe assessment
o Diagnostic and Laboratory testing
o Insertion or application of monitoring devices such as electrocardiog
o Splinting of suspected features
o Cleaning and dressing of wounds
o Performance of other necessary intervention based on the individua

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 60/323
If the patient is unconscious inspection of the oropharynx and may reveal the offending object.
Xrays, laryngoscopy or bronchoscopy also may performed.
MANAGEMENT
Head tilt chin maneuver
Jaw-thrust maneuver
Oropharyngeal airway insertionEndotracheal intubation
Cricothyroidotomy (cricothyroid membrane puncture)
HYPOVOLEMIC SHOCK
Possible problem associated with hypovolemic shock:
MANAGEMENT
Heat Stroke
• Shock is a condition in which theres is loss of effective circulatory blood volume.
• Inadequate organ tissue perfusion following ultimate resulting in cellular metabolic arra
•
In any emergency situation the onset of shock should be anticipated by assessing all inju
• Altered tissue perfusion related to failing circulation.
• Impaired gas exchange related to a ventilation perfusion imbalance.
• Decreased cardiac output related to decreased circulating blood volume.
• The goal of treatment are to restore and maintain tissue perfusion and to correct physiolo
• Ensuring a patient airway and maintaining breathing are crucial.
• Ventilatory assistance is given as required.
• A rapid physical examination performed to determine the cause of cause.
• Restoration of the circulating bllod volume is accomplished with rapid fluid and blood r
• Large- gauge intravenous needles are inserted into peripheral vein. Two or more cathete
• A Central Venous Pressure (CVP) catheter also may be inserted to serve as a guide for f
• Intravenous fluid are infusedat rapid rate until systolic blood pressure or CVP rises to a
• Blood component thereapy may also be prescribed.
• An indwelling urinary catheter is inserted to record urinary output everyhour.
Ø Is an acute medical emergency caused by failure of the heat-regulating mechanis
Ø RISK FACTOR: those not acclimatized to heat, elderly and young people, those u

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 61/323
SIGN AND SYMPTOMS
MANAGEMENT
FROSTBITE
ASSESSMENT
INTERVENTION
• profound central nervous system (CNS) dysfunction (confusion, delirium, bizarre
• elevated body temperature
• hot dry, skin
•
anhidrosis (absence of sweating)• tachypnea
• hypotension
• tachycardia
• primary goal is to reduce the high temperature
• cool sheets and towels or continuous sponging w/ cool water
• Ice applied to the neck, groin, chest, and axillae while spraying w/ tepid water
• cooling blanket
• Iced saline lavage on the stomach or colon if the temperature does not decrease
• Immersion of the patient in a cold water bath if possible
• monitored VS, ECG,CVP
• Fluids are administered
• urine output is measured frequently
• Blood specimen is obtained
• additional supportive care: dialysis for renal failure, antiseizure agent, potassium
Ø Is a damage to tissues and blood vessels as a result of prolonged exposure to co
• Numbness
• paresthesia
• Pallor
• Severe pain, swelling, erythema, and blistering that occur once the client is in a
• Necrosis and gangrene may develop in cases

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 62/323
HYPOTHERMIA
ASSESSMENT AND DIAGNOSTIC FINDINGS
MANAGEMENT
• Handle the tissues gently
• Rearm the affected part rapidly and continuously with a warm water bath (90-10
• Avoid thawing, interrupted periods of warmth, or massage (may result in further
• Do not derided blisters.
• Leave area exposed initially for continued assessment, and then apply bulky dre
Ø is a condition in which the core(internal) temperature is 35’C (95’F) or less as a re
Ø occurs when a patient loses the ability to maintain body temperature.
• Progressive deterioration
• Apathy
• Poor judgment
• Ataxia
• Dysarthria
• Drowsiness
• pulmonary edema
• Acid-base abnormalities
• Coagulopathy
• eventual coma
• Shivering
• continuous monitoring:
• ABC’s of basic life support are the priority.
• V/S
• CVC
• urine output,
• ABG levels,• blood chemistry determinations
• chest x-ray
• monitored ECG
• rewarming:
• Core rewarming for severe hypothermia
• Passive external rewarming use of warm blankets or over-the-bed heaters.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 63/323
NEAR-DROWNING
FACTORS
MANAGEMENT
DECOMPRESSION SICKNESS
ASSESSMENT
• supportive care:
• external cardiac compression
• Defibrillation temperature < 31’C
• Mechanical ventilation w/ PEEP
• Administration of warmed intravenous fluid
• administration of Na bicarbonate• administration of anti arrythythmic medication
• Insertion of an dwelling urinary catheter
Ø Survival for at least 24 hrs after submission. The most common consequence is h
Ø one of the leading causes of unintentional death in children younger 14 years of a
• Alcohol ingestion
• inability to swim
• diving injuries
• hypothermia
• exhaustion
• maintaining cerebral perfusion and adequate oxygenation to prevent further dam
• Immediate cardiopulmonary resuscitation – the greatest influence on survival
• ABG analysis
• use of endotracheal intubations w/ positive pressure ventilation
Ø also called “the bend,” occurs in patient who has engaged in diving, high-altitude Ø result from nitrogen bubbles trapped in the body. They may occur in joint or musc
• History is obtained from the patient or diving buddy.
• evidence of rapid ascent
• loss of air in the tank

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 64/323
MANAGEMENT
Major disorders of the neuromusculoskeletal system
TRAUMATIC BRAIN INJURIES
A. Etiology and path physiology
Motor vehicle accidents are the most common cause; can result from assaults, falls, and
Cause by a sudden force to the head
Acceleration injury: immobile head struck by moving object
Deceleration injury: head is hit by stationary object
Deformation injury: force disrupts the integrity of the skull
Fractures
Lineal: simple break in the bone
Depressed: break that results in fragmentsOf bone penetrating brain tissue
Basilar: occurs over the base of frontal and temporal lobes; ecchymosis is common over are
Hemorrhages (secondary brain injury)
Epidural: hematoma forms between the dura and the skull; may result from a laceration of th
Subdural: hematoma forms between the dura and arachnoid layers; generally follows venou
• buddy breathing
• recent alcohol intake or lack of sleep
• a flight within 24 after diving
• Sign and symptoms: joint or extremity pain, numbness, hypesthesia, and loss
• Neurologic symptoms mimicking those of a stroke or spinal cord injury could ind
• Cardiopulmonnary arrest can also occur in severe cases of DCS
• Patent airway and adequate ventilation
• 100% oxygen is administered
• Chest x-ray is obtained
• At least one intravenous is stared with lactated Ringer’s or normal saline solutio
• If an air embolus is suspected, the head of the bed should be lowered.
• The patient’s wet clothing is removed, and the patient is kept warm.• Transfer to the closest hyperbaric chamber capable of treating DCS is initiated.
• If air transport is necessary, low altitude flight (below 1000 ft) is required
• If aspiration is suspected, antibiotics and other treatment may be prescribed.
8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 65/323
Intracerebral hematoma
Cerebral contusions manifest depending on areas involved
Brainstem contusions result in unresponsiveness
Complications include cerebral edema, brain abscess, meningitis, diabetes insipidus
B. Clinical findings
Signs of increased intracranial pressure (ICP)Lack of oriental to time and place
Positive Babinski reflex
Seepage of cerebral spinal of basilar skull fracture
C. Therapeutic interventions
Nursing care of clients with head injuries
A. ASSESMENT
B. ANALYSIS/NURSING DIAGNOSIS
Concussion: temporary distruption of synaptic activity; brief loss of consciousness (<5 minutes
Contusions: bruising of brain tissue, with slight bleeding of small cerebral vessels into surroun
• Subjective: lethargy; indifference to surroundings; altered sensory function (e.g
• Objective
• Control seizures with anticonvulsants
• Mechanical ventilation; hyperventilation constricts cerebral vessels lowering ICP
• Monitor ICP with external catheter such as ventricular catheter or subarachnoid
• Reduce cerebral edema with glucocorticoides and loop diuretics; there is disagr
• Maintain adequate fluid and electrolyte balance
• Surgical intervention in cases of depressed skull fractures or hematomas
• Airway and breathing pattern
• Neurological status (see Neurological Assessment and Glasgow Coma Scale)• Signs of increased intracranial pressure (see Brain Tumor)
• Circumstances of injury
• Presence of glucose in clear drainage from nose or ears, which indicates cerebr
• Risk for aspiration related to loss of gag reflex or inability to expectorate

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 66/323
C. PLANNING/IMPLEMENTATION
D. EVALUATION/OUTCOMES
POSTRAUMATIC STRESS DISORDERS
A. Etiologic factors
B. Behavioral/clinical findings
• Decreased intracranial adaptive capacity related to increased ICP
• Risk for disuse syndrome related to long-term immobility
• Ineffective role performance related to impaired neuromuscular function
• Institute neurologic assessments every 15 minutes for several hours, progressin
• Maintain airway by suctioning as necessary (coughing increase intracranial pres
• Keep the client’s head elevated 30 degree to reduce venous pressre within the c
• Administer glucocorticoids and/or diuretics if ordered
• Institute seizure precautions; administer anticonvulsants if ordered
• Monitor for fluid or electrolyte imbalances; diabetes inspidus or syndrome of ina
• I f the client’s eyes remain open, protect the corneas with moistened pads, artifi
• Support client’s nutritional needs; administer tube feedings or assist with small f
• Position the client to prevent pressure ulcers• Provide range-of-motion exercises and splints to prevent contractures
• Provide auditory and tactile stimulation
• Assist client to avoid activities that increase ICP such as the Valsalva maneuver
• Recognize that confusion upon return of consciousness may be a defense again
• Utilize hypothermia as ordered to reduce temperature and metabolic demands
• Encourage client and family to participate in planning and care
• Maintains a patient
• Improves level of consciousness
• Remains free from complications of immobility
• Participates in decisions about administration of care
• Follows a divesting event that is outside the range of usual human experience (e
• Individual’s response must involve intense fear, helplessness, or horror; in child
• The traumatic event of reliving the experience, or exposure to situations that fos
• Exposure to a traumatic event resulting in actual death, threatened death, or se

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 67/323
C. Therapeutic interventions
Nursing care of clients with posttraumatic stress disorders
ASSESMENT
A. ANALYSIS/NURSING DAIGNOSIS
• Feeling of isolation and detachment
• Difficulty sleeping
• Violet outburst of anger
• Depression
• Interrupted concentration
• Hyper vigilance• Avoidance of associated stimuli
• Duration of disturbance more that 1 month
• Neurobiology of PTSD does not follow stress response, study indicates a hyper
• Same as Panic Disorders
• Behavior modifications to provide controlled exposure to recall of the event
• Supportive therapy• Use of Eye Movement, Desensitization, Reprocessing techniques (EMDR)
• Imagery, relaxation, and meditation may also be useful
• Behavior associated with anxiety disorders
• History of traumatic experience
• Sleep-pattern disturbance
• Screening for symptoms of major depression, phobias, and substance abuse
• Presence of depression, outburst of anger, and/of decreased concentration
• Anxiety related to threat to security and self-concept and recall of traumatic expe• Ineffective coping related to an inability to meet role expectations, and pervasiv
• Fear related to feelings of panic, altered judgment, and pervasive anxiety
• Risk for injury related to flight from the stress producing object or situation, feelin
• Powerlessness related to overwhelming, pervasive anxiety
• Compromised family coping related to disturbed relationships, pervasive anxiety
• Impaired social interaction related to pervasive anxiety

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 68/323
B. PLANNING/IMPLEMENTATION
C. EVALUATION/OUTCOMES
ANAPHYLACTIC REACTION
SIGN AND SYMPTOMS
Respiratory Signs
Nasal congestion
Itching
Sneezing and coughing
Possible repiraory distress
Chest tightness
Other repiratory difficulties suc as wheezing, dyspnea and cyanosis
Skin Manifestation
Flushing with a sense of warmth and diffuse erytheme
Generalized itching over the entire body
Uticaria (hives)Massive facial angioedema possible with accompanying upper repiratory edema
Cadiovascular Manifestation
Tachycardia or Bradycardia
Peripheral vascular collapse as in dicated by
• Post-trauma response related to unusual life experience causing avoidance or t
• Risk for violence: self-directed or directed toward
• See Fundamental Principles When Caring for clients with anxiety disorders
• Stay with client memory of the event returns to the conscious level
• Protect client from acting out violently with disregard for safety of self or other
• Uses coping mechanism to more realistically deal with the traumatic event
• Verbalizes decrease in dreams or flashbacks regarding the traumatic event
• Follows prescribes treatment regimen
• Demonstrates new adaptive ways of coping with anxiety
Ø Anaphylactic reaction is an acute hypersensitivity reaction that occurs within second or
Ø Pallor
8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 69/323
Gastro Intestinal Problem
NauseaVomiting
Colicky abdominal pains
Diarhea
NURSING INTERVENTION
Early endotracheal intubation is essential to preserve airway patency
Oropharyngeal suction may be necessary to remove excessive secretion
Resuscitiva measure are used especially for patient with stridor and progdressive pulmon
Pharmacologic management
Additional treatments may include the following;
INSECT STING
CLINICAL MANIFESTAION
Generalized uticaria,
Itching,malaise, and anxiety due to laryngeal edema to severe broncho spasm,
shock and death
MANAGEMENT
Ø Imperceptible pulse
Ø Decreasing blood preasure
Ø Circulatory failure, leading to coma and death
Ø Establishing a Patent aiway and ventilation is essential
Antihisatmines (eg, diphenhldramine [bendril] ) to block further histamines binding at target
Aminophyline titrated by IV drip for severe broncho spasman wheezing refractory to other treatm
Albuterol ( proventile, Ventoli ) inhalers or humidified, treatments too decreased bronchoconstric
Isoproterenol (Isuprel ) or (Inopromine ) for reduced cardiac output; oxygen to enhance tissue p
IV benzodiazepines (eg, diazepam [valium ] ) for control of seizures
Ø A person may have an extreme sensitivity to the venoms of the insect in the other hym

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 70/323
Stinger removal if the sting is from a bee because the venom is associated with sacs around the b
Stringer is remove with one quick scrape of finger nail over the site.
Wound care with soup and water is sufficient for stings.
Scratching is avoided because it result in Histamine responses.
Ice application is reduced the swelling and also reduced venom absorption.
Oral antihistamine and analgesic can be given to decrease the itching and pain.
Epinephrine (aqeous ) injected ubcutaneously-in the case of anaphylactic or sever allergic respo
To Minimize you chances Of being a Stung;
Avoid places where you stinging insects congregate such as a camp and picnic sitesand insect fe
Wear covering the feet and avoid going barefoot
Spray garbage scans with quick acting insecticide.
Avoid perfumes, scented soap and bright colors, which attract bees.
If you are stung; do the ff;
Inject self immediately with epinephrine if allergy is known or allergic response occurs
Remove the stinger with one quick scrape of the finger nail; do not squeeze the venom sac.
Clean the area with soapy water and apply ice
Report to the nearest health care facility for further examination if allergic response is suspected.
SNAKES BITE
The greatest number of bites occurs through the daylight hours into the early evening duri
CLINICSL MSNIFESTATION
Classic clinical signs of envenomation are;
Edema
Ecchymosis and hemorrhage bullae
Lymp node tenderness
Nausea and vomiting
Numbness and metallic taste in the mouth
FasciculationHypotension,
Paresthesias, seizures, and coma
MANAGEMENT
Ø Children between the ages of 1 to 9 yr/ old are most the likely victims.
§ Initial first aid of the site of the snake bite includes having the person lie down,
§ Removing constrictive items such as rings, providing warmth, cleansing and immobilizing the

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 71/323
HEMORRHAGE
A. Types
B. Assessment
C. Intervention: external
§ Airway breathing and circulation are the priorities of care,
§ Initial valuation in the ED is performed
§ And includes information the ff;
Ø Whether the snakes was venomous or non venomous; if the snake is dead; it should
Ø Sequence of events sign and symptoms (fang punctures, pain edema and erythema o
Ø Severity of poisonous effects
Ø Vital signsØ Laboratory data (complete blood count, urinalysis, and coagulation studies)
Ø Administration of Antivenin (Antitoxin)
Ø ACP (horse serum- derived antivenin )
1. Venous: dark color; steady flow
2. Arterial: bright color; spurts3. Capillary; red; oozes
• Restlessness
• Anxiety
• Rapid, weak pulse
• Cool, moist, pale skin
• Rapid respirations
• Thirst
• Nausea/ vomiting
• Alteration/ vomiting
• Hypotension
• Apply direct pressure with a clean cloth for a least 6 minutes (use gloves if availa
• Elevate injured part above heart level
• If arterial bleeding does not respond to direct pressure, attempt to control by app
• Tourniquets are not recommended unless an extremity is amputed or severely m
o Leave tourniquet exposed
o Tag or lebel victim with location of tourniquet
o Apply proximal to wound
o Tourniquet should not be removed except by a physician

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 72/323
• Treat for shock

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 73/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 74/323
8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 75/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 76/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 77/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 78/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 79/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 80/323
Cancer is one of the leading causes of death worldwide. The term describes all forms of ne
There are numerous theories espoused as to the cause of cancer. Cancer begins when a n
differentiated.
they undergo destruction. The failure of the immune response system will lead to inability
ompounds, Spoilt Foods, and preservatives like nitrites.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 81/323
is B virus, HSV, HPV, Epstein Barr virus. The RNA viruses are the HIV and the HTCLV.
mor. The hormone-responsive tissues are considered targets for four types of cancers- pr
coffee intake, nitrosamines and vitamin deficiencies.
Benign Malignant
Grows slowly Grows rapidlly
Infiltrates surrounding tissues
cture, and growth behavior, leading to become malignant cells.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 82/323
Encapsulated Not encapsulated
Never occur Very common
Not harmful to host Always harmful
Very good progno Poor prognosis
Benign cells are typically encapsulated non-invasive and highly differentiated. Mitosis is ra
Malignant cells are non-encapsulated, invasive and poorly differentiated. They have uncon
-whenever malignant neoplasm penetrates into a natural “open fie
-involves: peritoneal cavity, (most often), pleural, p space and
-pattern of lymph node involvement follows the natural route of dr
-This is the most common mode of spread!
- Malignant cells are disseminated through the blood stream

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 83/323
Guaiac stool exam for occult blood[50 y/o and above].
hase of cell cycle

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 84/323
oclonal antibodies.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 85/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 86/323
ications.
odify the host’s biologic response to tumor cells
ess of therapy.
ticular tumor and can be used to screen, diagnose, assess prognosis, evaluate response to treatmen

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 87/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 88/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 89/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 90/323
motorcycles, boats, bicycles, etc.
escription of the wound.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 91/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 92/323
o less than 2.5 mmol/L is an indication of successful resuscitation.
ebridement and fracture repair.
ollecting laboratory specimens, and documenting activities and the patient’s response
8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 93/323
posed to criminal law cases, which involve a defendant and the State of Utah. Persona
ious or in critical condition and unable to make decision. If the patient is unconscious a
y for immediate treatment.
rvices.
lth care problems in crisis situations. The emergency nurse establishes priorities, monit
t of as fast-paced, technology-driven environment in which serious illness and death a
oviders are at an increased risk for exposure to communicable disease through blood

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 94/323
hological healing. Some are experience real and terrifying fear of death and other assa
priate setting for ongoing care.
ions should be given not only verbally but also in writing, so that the patient can refer to
. For patients and families who cannot provide at home, community agencies may be c
severity of their health problems and the immediacy with which these problems must b
our.
to the appropriate setting (intensive care unit, operating room, general care unit) are th

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 95/323
storing effective circulation.
eters

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 96/323
to therapy.
il there is improvement in the patient clinical coordination.
heat waves, especially when they are accompanied by high humidity.
nd debilitating diseases, and those taking certain medication.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 97/323
ine may prescribed

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 98/323
rs.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 99/323
s after diving.ess, or hypesthesia.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 100/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 101/323
te (countercoup) as a result of rebound reaction

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 102/323
ions)
ted behaviors
e event with intense fear/, helplessness, or horror; onset at any age

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 103/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 104/323
al responsiveness
e, such as medication (eg, penicillin, iodinated contrast material) and other agents, suc

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 105/323
nd wasps,)venom allergy is thought to be an IgE-medication, and it reaction it constitu

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 106/323
snake bite occurs from pit vipers( crotalidae). The most common site is the upper extre

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 107/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 108/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 109/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 110/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 111/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 112/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 113/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 114/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 115/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 116/323
oplastic diseases that are malignant and can cause death.
rmal cell is transformed into a neoplastic cell by a transforming agent by exposure or int
of the WBC to destroy cancer cells

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 117/323
state, breast, brain and endometrium.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 118/323
e and the growth is very slow. Metastasis does not happen.
rolled proliferation that can be erratic. The cells contain few identified cellular characteris
ld”
joints
ainage

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 119/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 120/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 121/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 122/323
t and check for tumor recurrence.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 123/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 124/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 125/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 126/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 127/323
dult younger than 44 years of age. The incidence is increasing in adults older than 44

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 128/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 129/323
l injury can occur in a wide variety of ways. The following are some of the most com
nd brought to the ED wi thout family or friends, this fact should be documented.
or and continuously assess acut ely ill and injured patients, supports and attends to f
re confronted on a daily basis.
r other body fluids. The reemergence of tuberculosis, a major health problem.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 130/323
ults on their personal identify and body integrity.
them later.
ontacted before discharge to arrange services.
e treated.
e priorities of emergency care.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 131/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 132/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 133/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 134/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 135/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 136/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 137/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 138/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 139/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 140/323
h as latex insect stings and wash yellow jacket, hornet or foods (eg, eggs, peanuts).

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 141/323
es an acute emergency.Although stings in any area of the body can trigger anaphyla

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 142/323
memity.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 143/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 144/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 145/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 146/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 147/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 148/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 149/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 150/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 151/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 152/323
raction. These agents are called carcinogens that can permanently change the DNA stru

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 153/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 154/323
tics, they have altered biochemical properties such as hormone-like secretions and they h

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 155/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 156/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 157/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 158/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 159/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 160/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 161/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 162/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 163/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 164/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 165/323
on accidents resulting in personal injury:
milies, supervises allied health personnel, and teaches patients and families within a

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 166/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 167/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 168/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 169/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 170/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 171/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 172/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 173/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 174/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 175/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 176/323
Repeated administration of parenteral or oral therapeutic agents (eg, repeated expos

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 177/323
xis, stings of the head and neck or multiple stings are especially serious

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 178/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 179/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 180/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 181/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 182/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 183/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 184/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 185/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 186/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 187/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 188/323
ture of the cell. Some other agents are called co-carcinogens because they can alter gen

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 189/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 190/323
ave chromosomal instability. They can potentially cause new mutation in the cancer cells

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 191/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 192/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 193/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 194/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 195/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 196/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 197/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 198/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 199/323
d penetrating trauma.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 200/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 201/323
time-limited, high pressured care environment. The strength of nursing and medicin

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 202/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 203/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 204/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 205/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 206/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 207/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 208/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 209/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 210/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 211/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 212/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 213/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 214/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 215/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 216/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 217/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 218/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 219/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 220/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 221/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 222/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 223/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 224/323
tic information in the cell enhancing cellular transformation.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 225/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 226/323
rendering them resistant to therapy. They metastasize to distant sites!

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 227/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 228/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 229/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 230/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 231/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 232/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 233/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 234/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 235/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 236/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 237/323
are complementary in an emerg ency situation. The emergency health care staff me

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 238/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 239/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 240/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 241/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 242/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 243/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 244/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 245/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 246/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 247/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 248/323
ld allergic response occurred.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 249/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 250/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 251/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 252/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 253/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 254/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 255/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 256/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 257/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 258/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 259/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 260/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 261/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 262/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 263/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 264/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 265/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 266/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 267/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 268/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 269/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 270/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 271/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 272/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 273/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 274/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 275/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 276/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 277/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 278/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 279/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 280/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 281/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 282/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 283/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 284/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 285/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 286/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 287/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 288/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 289/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 290/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 291/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 292/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 293/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 294/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 295/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 296/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 297/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 298/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 299/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 300/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 301/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 302/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 303/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 304/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 305/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 306/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 307/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 308/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 309/323
are for patient’s in an emergency situation.

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 310/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 311/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 312/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 313/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 314/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 315/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 316/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 317/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 318/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 319/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 320/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 321/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 322/323

8/14/2019 Finals Ms2
http://slidepdf.com/reader/full/finals-ms2 323/323