femtosecond laser assisted cataract surgery for … laser assisted cataract surgery for cataract and...
TRANSCRIPT

Femtosecond laser assisted cataract surgery for cataract
and rle
Prof.Dr.Mahmut Kaşkaloğlu
Kaşkaloğlu Eye Hospital
Izmir, Turkey
june 2016

• No financial disclosure
Cataract surgery decreases mortality rate
• …..United States Medicare patients with cataract, those who underwent cataract surgery had 30% reduced mortality compared with those who did not undergo surgery………….
• Tseng VL,Yu F, PhD,1,3 Lum F, Coleman AL., Cataract Surgery and Mortality in the United States Medicare Population.Ophthalmology 2016;123:1019-1026

• Cataract surgery is the most common operation
• Europe average 10,000 per million
• 450,000 cataract operations in Turkey – About 6000 per million
• Today many RLE with multifocals
• All patients expect perfect results
• How do we make it better and safer?

Asclepion-Meditec Phacolase Er:YAG
Paradigm Photon Nd:YAG
WaveLight Adagio Er:YAG
erbium:YAG laser, Nd:YAG laser (2000)
ARC Laser's Dodick Laser Photolysis
Nd:YAG

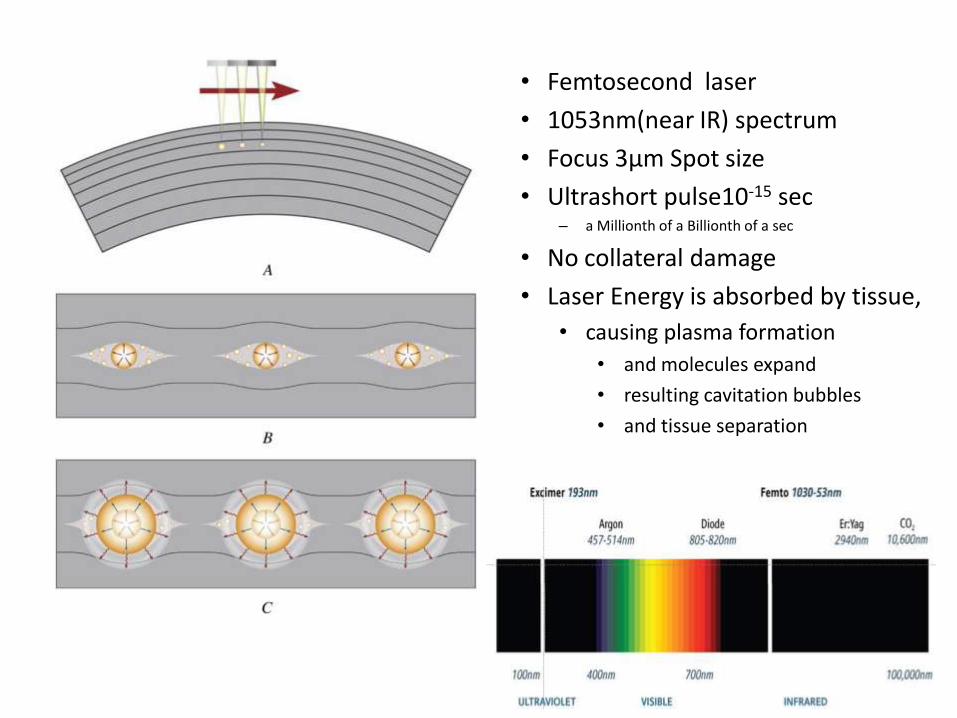
• Femtosecond laser
• 1053nm(near IR) spectrum
• Focus 3µm Spot size
• Ultrashort pulse10-15 sec – a Millionth of a Billionth of a sec
• No collateral damage
• Laser Energy is absorbed by tissue,
• causing plasma formation
• and molecules expand
• resulting cavitation bubbles
• and tissue separation

Femtolaser in ophthalmology:
• Flap creation: LASIK
• Lenticule extraction: SMILE
• Channel for ICR
• Corneal graft
• Intracor
• Arcuate incisions
• Glaucoma
• Cataract
Future use of Femtolaser in ophthalmology:
• Treatment of tractional vitreous attachments.
• Reversing presbyopia.
• Refractive index shaping.
• Corneal collagen crosslinking (CXL).
• Reversing cataract. • Lubatschowski H. Applications of the Femtosecond Laser A new era of ophthalmology. CRST Europe 2012 feb. 52-54
Problems with conventional phaco
Difficult learning curve
Dependent of the surgeon’s dexterity
For perfect results all steps must be within acceptable tolerances
Most complications caused by the surgeon, 10X LASIK
Many manual steps which cannot be executed with reproducible precision and predictability.
• Efficacy : – More predictable and accurate capsulotomy
– More consistent corneal incision construction
– Better refractive results
• Safety : – Less ultrasound energy
– Less risk of capsule tears
– Less incision leakage and astigmatism
Potential benefits of Femto cataract surgery

Current FS platforms
• LenSx (Alcon Lab., USA)
• Catalys (Optimedica Corp.,USA)
• LensAr (LensAr Inc., USA)
• Victus (Technolas, Germany; Bausch&Lomb, USA)
• Ziemer Femto LDV Z (Ziemer Ophthalmic System AG,USA)

1.Catalys: Liquid optics, nonapplanating
2.LensAR: Fluid interface, nonapplanating
3.LenSx: Curved lens, applanating
4.Victus: Dual modality
5.Ziemer: Liquid interface
Interface
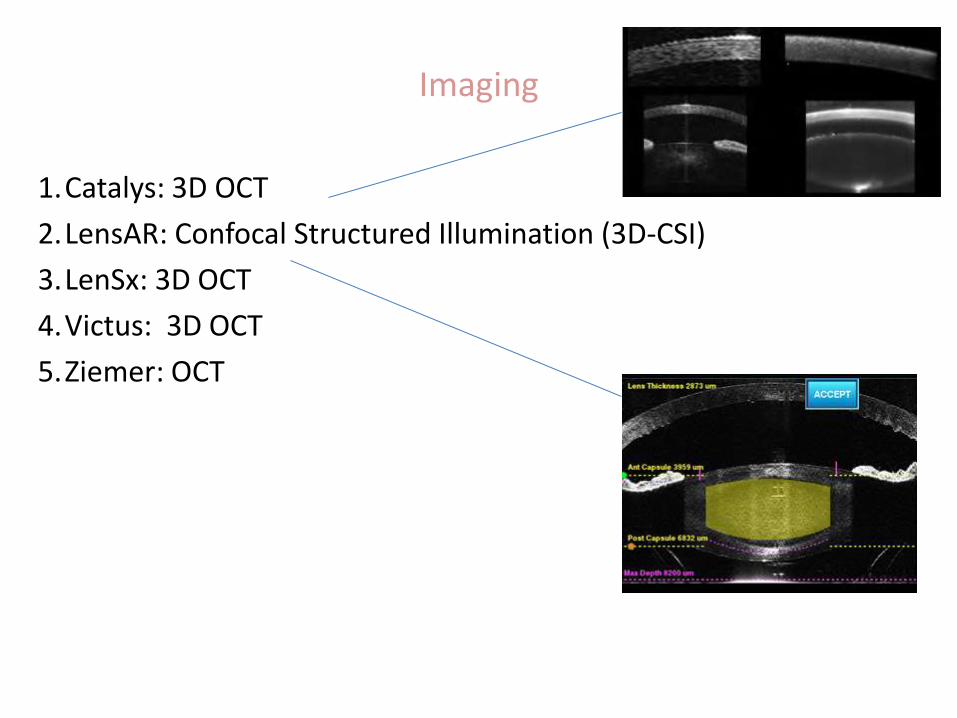
1.Catalys: 3D OCT
2.LensAR: Confocal Structured Illumination (3D-CSI)
3.LenSx: 3D OCT
4.Victus: 3D OCT
5.Ziemer: OCT
Imaging

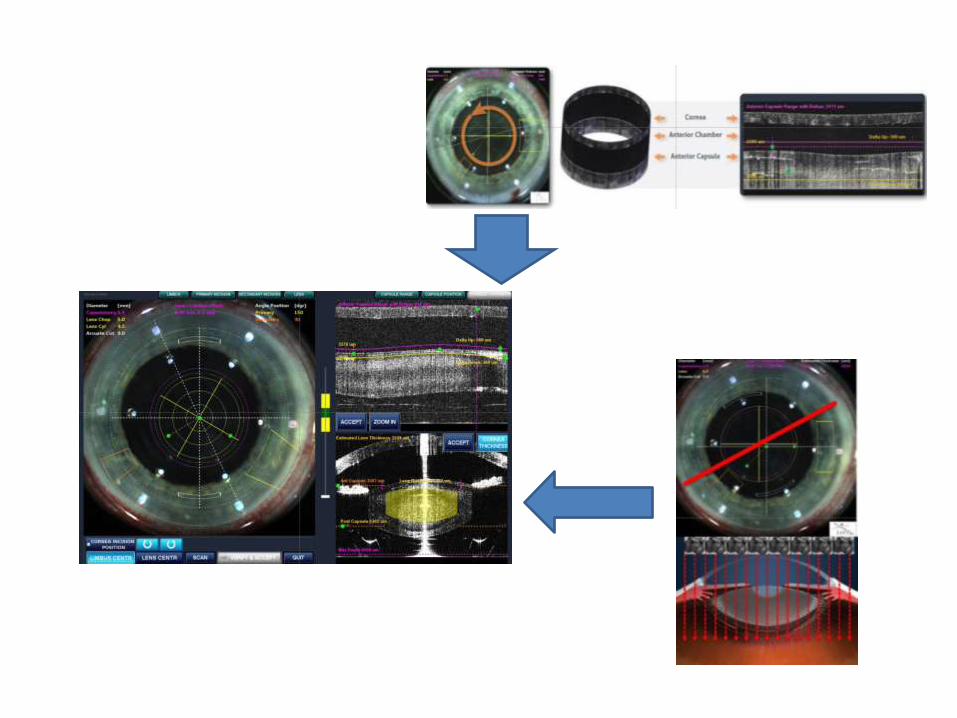
LenSx® Laser
Touch screen Graphic User Interface
Real-time video imaging for 3D visualization
True image-guided surgical planning
Sterile or unsterile.
Can be located in the same room or different rooms.

• Corneal incisions
• Capsulotomy
• Laser lens fragmentation
• Arcuate incisions
• Lasik flaps (not yet available)
Applications of LenSx

Patient selection • General
– Can lie flat and still
– Back problems
– Tremor
• Inform • Subconjunctival hemorrhage
• Check • Lids
• Pupil dilation
• Anterior capsule
• Cataract type
• Zonules
• Docking – Patient lies flat
to PI
– Bubbles in interface or suction loss:
• Undock and dock again
– Suction loss during femto:
• proceed with manual phaco

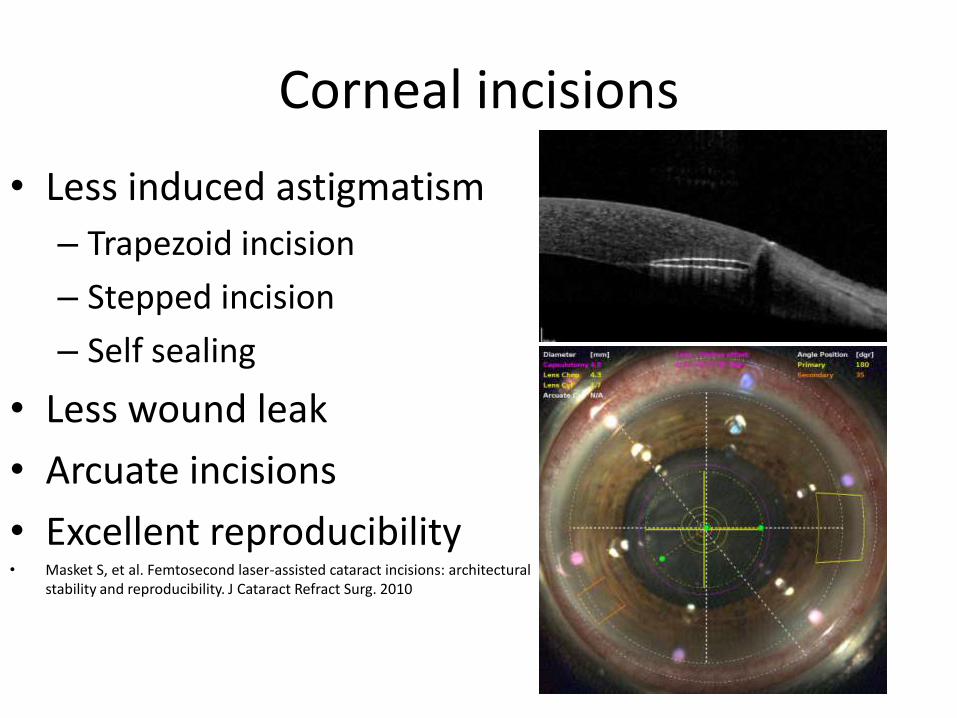
• Less induced astigmatism
– Trapezoid incision
– Stepped incision
– Self sealing
• Less wound leak
• Arcuate incisions
• Excellent reproducibility • Masket S, et al. Femtosecond laser-assisted cataract incisions: architectural
stability and reproducibility. J Cataract Refract Surg. 2010
Corneal incisions

• Exact sizing – Stability
• Better Effective lens position
– Less capsular opacity – Stable refraction
• Perfect shape • Perfect centralization
– Less aberration – Less phimoses
• More capsule strenght – Less capsule tear
1. Nagy Z, et al. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009 2. Kranitz K, et al. Femtosecond laser capsulotomy and manual continuous curvilinear capsulorhexis parameters and their effects on intraocular lens centration. J Refract Surg. 2011 3. Friedman NJ, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011 4.Dick HB, et al. Intraocular lens fixated in the anterior capsulotomy created in the line of sight by a femtosecond laser. J Refract Surg. 2014
Capsulotomy

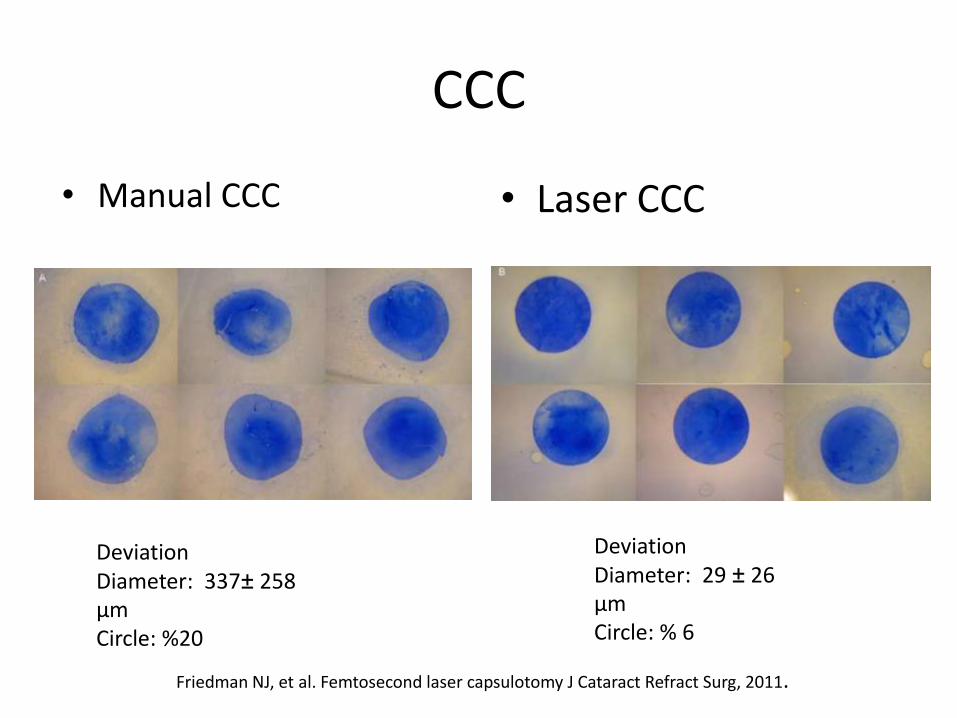
CCC
• Manual CCC • Laser CCC
Deviation Diameter: 337± 258 µm Circle: %20
Deviation Diameter: 29 ± 26 µm Circle: % 6
Friedman NJ, et al. Femtosecond laser capsulotomy J Cataract Refract Surg, 2011.

• Optimal CCC for IOL:
• 4.8mm to 5.2mm
• Prefemto Pupil diameter 1.5mm larger than CCC
• To Prevent Pupil constriction after femto:
– Preop NSAI, Cyclopentolate, Neosynephrine – Keep interval between femto and phaco short – Repeat Neonynephrine after Femto – Adrenaline in BSS – First cases 40% now less than 15%
Pupil size
Watch for Intumescence
Calcification
Always stain capsule
• Prefemto:
– Iris hooks or Malyugin ring • Benefit to patient
questionable
– If pupil too small for minimal CCC , manual phaco maybe safer
• Post femto: – Adrenaline – Viscodilation – Iris hooks – Malyugin ring
• What to do if you cannot do femto ?
Small Pupil
• Gently tap and tilt the nucleus
• Decompress air bubbles from behind the lens
• Gently inject BSS
• See bubbles come forward
• Aggressive, rapid, hydrodissection may cause posterior capsule rupture
Hydrodissection
o Divide&conquer, chop
o Don’t be discouraged during the learning curve
o Our total femto procedure duration is now 10m vs 19m during the early period
Phacoemulsification
Harder cataracts cylinder pattern facilitate central debulking

• Matrix pattern
Lens fragmentation
• Effective phaco time (EPT) and cumulative dispersive energy
(CDE) reduced1,5
• Central corneal thickness reduced, less endothelial cell loss6
• Some studies indicate less early macular thickness after
Femto.
5. Conrad-Hengerer I, et al. Effect of femtosecond laser fragmentation on effective phacoemulsification time in cataract surgery. J Refract Surg. 2012 6. Takacs AI, et al. Central corneal volume and endothelial cell count following femtosec-ond laser-assisted refractive cataract surgery compared to conventional phacoemulsification. J Refract Surg. 2012

– During Femto CCC laser cuts 300µm
circular cortex
– This is flush with the CCC edge
– Hydrodissection may not be possible between the capsule and the layer of cortex
– In theory this is a safety zone
– With some experience this is not an issue and all cortex can be removed easily
Cortex removal

Arcuate Relaxing incisions:
– 80% depth
– Opened during surgery
– Opened later
– Nomograms are being developed
– Long term efficacy to be determined
– For refractive cataract and RLE cases toric IOL is the better option
RK+ RLE (FEMTO-AK)
Preop. Data: - CDVA: 0.5/0.5 - Otoref.:
- OD: +1.25 +6.25x175 - OS: +3.75-5.75x110
- Corneal ast.: - OD 4.75 D - OS: 5.25 D
- OD: Femto RLE+ mono toric - OS: Femto RLE+ mono toric+ AK
Postop. Data: - UDVA: 0.7-0.8 / 0.7 - Otoref.: OD: +2.00-2.75x90 OS: +0.75-0.75x115

Asena BS, Kaskaloglu M. Laser-assisted cataract surgery: softlens assisted interface(SoftFit) versus direct contact interface. Eur J Ophthalmol 2016; 26(3): 242 - 247
• Kaskaloglu Eye Hospital Izmir
• February 2013-February 2016
• 670 eyes
• No laser complications – Incomplete CCC in 62 eyes
– 1 anterior capsule tear
– 1 posterior capsule break
• Average operation time 14 minutes

• We are still in the early phase of this advanced technology
• We already know that – It can do CCC better than us
• May lead to better refractive outcome
– It can lower the phaco time
• May reduce endothelial cell loss
– Planned incision architecture
• Less induced astigmatism
Conclusion:
Disadvantages:
• Narrow palpebral aperture, deep orbit, high brow
• Posture problems
• Corneal opacities
• Small pupil, synechia
• White, advanced cataract

• Femto laser is a tool
• We will learn how to maximize this tool for the benefit of our patients. – Change laser parameters such energy levels, spot separation
for the type of cataract
• Manipulation will improve – Remember how Nagahara chop and modifications
revolutionized phaco

– The Industry will improve the machine • Interface
• Automatic recognition of the density of the cataract
• Improve automatic warnings to prevent
– Excess energy
– Wrong positioning
• Hopefully lower the cost
• Many still are skeptical of the value of femto laser cataract surgery but it is here to stay for some time
– ICCE
– ICCE
– PHACO
– FEMTO
– ?????

Thank you for your attention