executive summary meeting report - who · executive summary meeting report ... use of standard rrl...
TRANSCRIPT
REPORT FOR WHO-COORDINATED IBVPD SURVEILLANCE NETWORK,
LABORATORY TECHNICAL WORKING GROUP MEETING
EXECUTIVE SUMMARY MEETING REPORT
WHO-Coordinated IBVPD Surveillance Network
Laboratory Technical Working Group Meeting
29th-30th October 2014
Geneva, Switzerland
2
CONTENTS
Background ................................................................................................................................................... 3
Objectives ..................................................................................................................................................... 3
Background documents in participant file .................................................................................................. 4
Meeting summary ........................................................................................................................................ 4
Network overview and regional updates ......................................................................................... 4 Improving data quality of the IBVPD laboratory network ............................................................... 5
Quality Assurance and Quality Control ............................................................................................ 6
Optimization of laboratory procedures in the network .................................................................. 7
Annex 1: Meeting agenda ............................................................................................................................ 9
Annex 2: List of participants ...................................................................................................................... 12
3
BACKGROUND
In 2011 the WHO established a laboratory Technical Working Group (TWG) to provide technical
guidance throughout the WHO-Coordinated Global Invasive Bacterial Vaccine Preventable Disease (IB-
VPD) Network, for strengthening the laboratory capacities related to the identification and
serotyping/serogrouping of Streptococcus pneumoniae (Spn), Haemophilus influenzae (HI) and Neisseria
meningitidis (Nm) and the improvement of the quality of laboratory data collected through the
surveillance network.
In 2013, a Strategic Review of the IB-VPD network was carried out and the findings were presented at a
meeting in Geneva and the resulting recommendations from the review to strengthen the IB-VPD
surveillance network and the strategic plan from this review was endorsed by the Strategic Advisory
Group of Experts on Immunization Epidemiology (SAGE EPI) technical oversight body.
The laboratory TWG was convened in October 2014 to assess the status of the implementation of the
Strategic Review recommendations, to gain a better understanding of regional and specific lab related
issues, to provide guidance on how to improve the data quality of the IB-VPD laboratory network by
development of a strategy for more standard reporting from regional and national reference
laboratories performing PCR testing and the data linkage between clinical and laboratory data. The
group also discussed how to better optimize the laboratory procedures in the network and strengthen
the Quality Assurance (QA) and Quality Control (QC) systems.
Some of the key achievements from 2013 – 2014 include the implementation of Performance Measures
at all levels. In the area of monitoring laboratory performance, achievements include a continued
external quality assessment (EQA) global programme and implementation of global external quality
control QC system between the Global and regional reference labs (RRLs). Regions have started the
transition to case-based reporting of RRLs data and linkages between these data and the sentinel site (SS)
data have improved.
MEETING OBJECTIVES
To review the regional updates for the status of the recommendations from the strategic review,
the flow of samples and information, the monitoring of lab performances and the site
assessments.
To review any 2013 data quality issues and ways to improve laboratory data. These include the
use of standard RRL reporting forms, introduction to the web-based tool and addressing data
quality issues at the sentinel site level for missing information and availability of reagents.
To review the External Quality Assessment (EQA) and Quality Control (QC) programmes and to
define the way forward.

4
Optimisation of lab procedures, addressing the challenges of bacteriology capacities at the site
level and the molecular testing capacities of the regional laboratories.
BACKGROUND DOCUMENTS IN PARTICIPANT FILE
October 2014 update on status of action points of the 2014 WHO Management Framework
Reference laboratory process and performance metrics
Draft IBD Lab Variables ST/SG for the Regional Reference Labs
List of participants
Meeting agenda
MEETING SUMMARY
I. Network overview and regional updates
The meeting began with a global overview of the network and the global status of the implementation
of the strategic review recommendations.
Overall there has been a lot of progress with completion of 26 out of 30 iTAG recommendations that
were to be implemented by the first year.
The objective of the network has changed from documenting and measuring diseases to monitoring
vaccine impact, providing a good baseline before vaccine introduction in countries. An important
component of this process is sharing case base data and the linking of laboratory and clinical data. The
main achievements that were highlighted in the global and regional updates included:
Progress and transition to case based reporting; case-based 2013 data was received from 6 out
of 9 RRLs and one sentinel site laboratory
Continued monitoring of laboratory performance at all levels of the laboratory network and
distribution of External Quality Assessment (EQA) proficiency testing panels globally
Implementation of a global quality control programme for confirmatory testing between the
global and regional reference labs
Improved referral systems between sentinel sites laboratories (SSLs) and the RRLs for either
confirmatory testing or PCR for diagnosis and serotyping/serogrouping (ST/SG)
Development of a new web based tool to improve data collection and bridge linkages between
data collected at all levels of the surveillance network.
Some of the current challenges that need additional resources and capacity building activities are in the
areas of sample referral and testing, such as specimen storage, testing capacities at RRL, shipping
5
logistics, regulations (Material Transfer Agreement (MTA), Import permit), site visits and trainings, the
data management system and low rates of bacterial isolation at country level.
There is still a need to improve linkage between data for all laboratory testing done at SSL and RRL levels
and the clinical database. The use of a unique patient ID number when samples are referred for lab
testing is still a challenge.
II. Improving data quality of the IBVPD laboratory network
An overview of the RRL 2013 data consolidation and analysis processes showed that huge efforts have
been made to improve the quality of laboratory data collected through the surveillance network. 3144
samples from Meningitis Surveillance were received and tested at the RRLs in 2013. Of these 1003 (32%)
were positives for one of the three pathogens (Spn, HI or Nm). ST/SG data could be assigned to 833
(83%) of positive cases. PCR data from RRL shows an important increase in diagnostic yield of bacterial
meningitis. This highlighted the importance of developing a strategy to prioritize retrospective linkages
between RRL and SS data.
Linking of the RRL data with clinical database from sentinel sites could be done on samples that were
reported in the RRL databases with a unique ID number; these represented around 30% of 2013 data
reported from RRLs.
One of the challenges that were addressed is the quality and categorization of the samples that are
referred to the RRL. Information to categorize the samples into the Probable Bacterial Meningitis1 (PBM)
cases (WBC, glucose and protein) and results of initial laboratory testing (culture, Gram stain and Rapid
diagnostic tests (RDT)) are often missing. WHO reinforces its recommendation that SSL send ALL
suspected meningitis cases to the RRL till more data can be linked and more analysis can be done to
assess the use of prioritization algorithm for samples referral.
The group emphasized the importance of linkage between data quality and availability /use of the
necessary quality controlled laboratory reagents, supplies and equipment at the sentinel site level (use
of sheep blood for culture, TI media for cerebrospinal fluid (CSF) transport, RDT kits to provide quick
feedbacks to clinicians, availability of incubators and freezers etc.).
There have been improved linkages between RRL and clinical databases for the 2013 data with 6 out of 9
having reported case-based data. However there are still challenges in the data management system
such as the inconsistent use of the unique ID number or missing information on lab testing performed at
the sentinel site level. These limit the data analysis and comparison between sentinel site lab testing
results and RRL results.
1 Definition of PBM: A suspected meningitis case (as defined above) with CSF examination showing at least one of the following:
Turbid appearance;
Leukocytosis (> 100 cells/mm3);
Leukocytosis (10-100 cells/ mm3) AND either an elevated protein (>100 mg/dl) or decreased glucose (< 40
mg/dl) Note: if protein and glucose results are not available, diagnose using the first two conditions (i.e. turbid appearance or leukocytosis > 100 cells/mm
3)
6
WHO has started the development of a web based system to bridge the gap between laboratory and
epidemiological data and improve surveillance data. The system is being pilot tested in PAHO and SEARO
and more regions showed interest in pilot testing it. This would improve the data check, cleaning,
analysis and feedback mechanisms throughout the year.
The standard form for reporting PCR data from reference laboratories and sentinel sites performing PCR
was reviewed and the group recommended WHO to revise and distribute the form to all labs reporting
PCR by end of 2014.
Recommendations to improve laboratory data quality are:
Caution in reporting the non-typeable (NT) and non-groupable; distinction between real NT and
NT because of methods limitations
Standard use of the drop down options that are listed in the reporting form; Include comments
whenever it is necessary to explain the final result
RRLs to receive lab testing results from referring sentinel sites for a better tackling of
discrepancies and improved feedbacks mechanisms
Active data analysis and feedback mechanisms throughout the year
The web based tool to be pilot tested at RRL in coordination with ROs that are interested in
implementing the system
Data consolidation at regional level before submission to WHO HQ
III. Quality assurance and quality control
1. EQA
In 2014, WHO coordinated the global External Quality Assessment (EQA) programme in coordination
with the National EQA Unit at the Public Health England (PHE). The EQA for IBVPD provides proficiency
testing panels to assess diagnostic capabilities at sentinel site level to identify Spn, HI and Nm (Culture,
Microscopy and RDT). AMST was included in the testing but did not count into the overall scoring as
WHO does not provide technical support for these tests. Serotyping/serogrouping capacities are
assessed for labs that have the capacities to do it. Preliminary 2014 results from sentinel sites and RRLs
showed a high level of performance in the labs that submitted results. Data summary is as follows:
o 109 labs were included in participant list received from ROs o 90 labs did submit results o 83 had passing score of >75% o 7 labs failed the EQA exercise o 19 labs did not submit results
The RRLs received more challenging proficiency testing (PT) panels and were assessed on the methods
for genotypic characterization. All except one RRL had >90% passing score. One RRL had 82% score.
7
Challenges of 2014 EQA survey included holding back by customs of the infectious diseases PT panels
and delays in panels deliveries to the labs which resulted in postponing the closing date of the survey
and delays in data analysis and feedbacks.
Recommendations to improve the EQA in 2015:
WHO to continue the EQA to monitor lab performance globally
WHO to avoid contracting with different suppliers every year to decrease challenges and build
capacities consistently
Timelines to be set up and agreed upon in January-February 2015 and quicker turnover of the
process so corrective actions can be implemented quickly
Next EQA survey to be ready by May 2015; WHO to provide updated and correct information on
participant labs 2 months in advance to the survey
2. QC for confirmatory testing between RRL and GRL
Preliminary results of the first year of implementing global external QC programme for confirmatory
between the RRLs and CDC Global Reference Lab (GRL) showed a high level of concordance
identification and ST/SG of Spn, HI and Nm by PCR. Data of 6/9 RRLs were summarized and discussion on
general concordance and typical discrepant results were addressed. The average of concordance
between the RRL and CDC GRL results was 91% for pathogen detection and 93% for ST/SG, which
indicated a very high performance of the RRLs. Some of the common reasons for the discrepancies seen
could be transcriptional errors, differing sample conditions, differences in interpretation of PCR results (
as in the lack of standardized Cycle Threshold (CT) cut-off values for the target genes or use of the
human RNaseP gene in the interpretive scheme), and unequivocal starting volume of extraction.
Recommendations on QC for confirmatory testing:
The QC is an useful exercise for RRLs and GRL so WHO to continue its monitoring in 2015
RRLs to continue sending 50 specimens to GRL and additional difficult samples can be sent but
will not be included in the scoring
Discrepant results will be discussed, followed by troubleshooting and a third lab will test this if
no consensus is reached (Refer to WHO guidelines developed in 2013)
The timing of the QC worked well but development of timeline table from CDC GRL for 2015 is
needed and that will be distributed to RRLs through WHO and ROs.
IV. Optimizing the use of laboratory procedures in the network
The TWG addressed the availability and use of WHO recommended laboratory procedures at all levels
and reinforced the need of building bacteriology capacity based on the findings from the site
assessments and efforts to improve bacterial isolation rates at the sentinel site level. Regions provided
8
inputs on their procurement system and challenges are mainly noticed in AFR and EUR for procuring lab
supplies and ensuring their availability at the country level in a timely manner.
CDC GRL presented a new direct PCR procedure without DNA extractions on CSF for the detection of
bacterial meningitis pathogens plus RNaseP and ST/SG of Hib, NmA, B, C, W, X and Y. The group
emphasized the added value of the implementation of this new technique for surveillance purposes,
especially in labs that receive large volume of samples as the traditional PCR and DNA extraction are
time consuming and requires extensive manipulation that can introduce cross-contamination..
The optimization of reporting PCR data was also discussed and the CT cut-off values to report the PCR
results for target genes as well as RNaseP human genes were determined by the group.
Recommendations for optimal use of lab procedures in the network:
The Direct PCR to be validated in RRLs that are interested in using it for surveillance
The cut off point for the CT values used for target genes should be adopted as below 35 being
positive and above 35 being negative (equivocal between 36-40 to be diluted when possible).
For RNaseP standardization, first test for pathogens target genes as a priority. If this is negative
(>35) then test for RNaseP and if RNaseP>35 then report it as inconclusive; the cut off is 35.
A list of lab equipment/ supplies for sentinel sites and RL, including estimated quantities needed
by year, to be compiled in consultation with ROs for submission into the WHO catalogue.
9
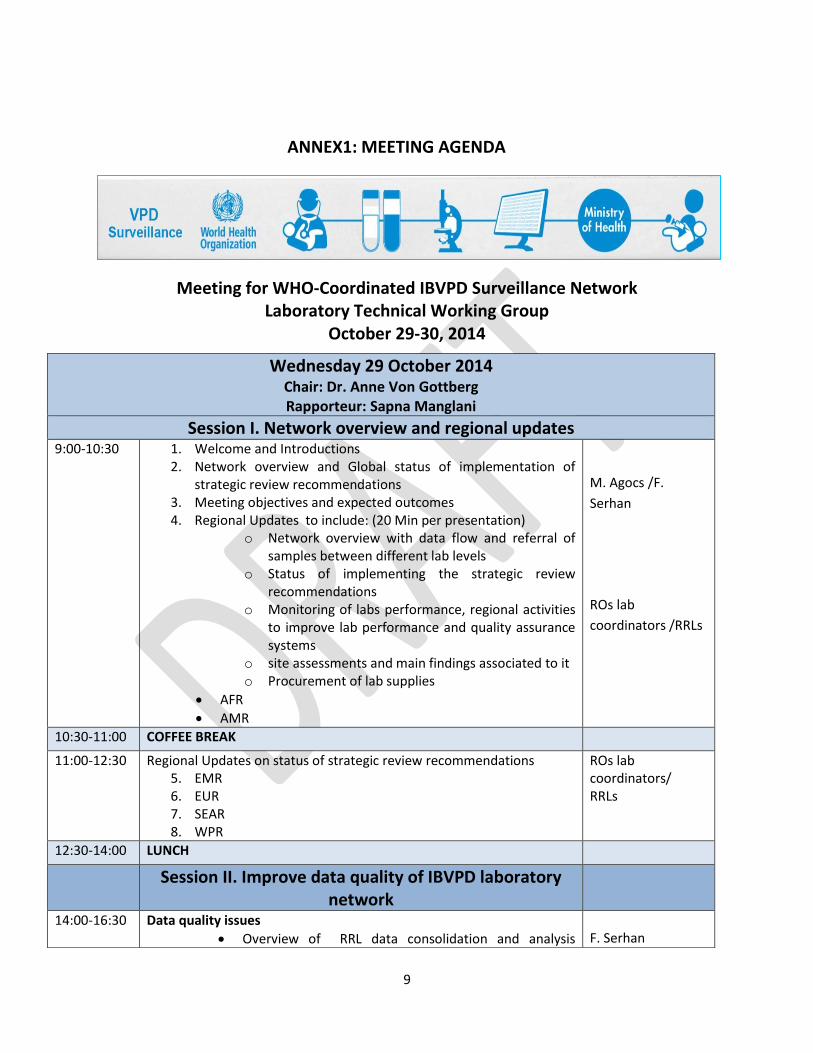
ANNEX1: MEETING AGENDA
Meeting for WHO-Coordinated IBVPD Surveillance Network Laboratory Technical Working Group
October 29-30, 2014
Wednesday 29 October 2014 Chair: Dr. Anne Von Gottberg Rapporteur: Sapna Manglani
Session I. Network overview and regional updates 9:00-10:30
1. Welcome and Introductions 2. Network overview and Global status of implementation of
strategic review recommendations 3. Meeting objectives and expected outcomes 4. Regional Updates to include: (20 Min per presentation)
o Network overview with data flow and referral of samples between different lab levels
o Status of implementing the strategic review recommendations
o Monitoring of labs performance, regional activities to improve lab performance and quality assurance systems
o site assessments and main findings associated to it o Procurement of lab supplies
AFR
AMR
M. Agocs /F.
Serhan
ROs lab
coordinators /RRLs
10:30-11:00 COFFEE BREAK
11:00-12:30 Regional Updates on status of strategic review recommendations 5. EMR 6. EUR 7. SEAR 8. WPR
ROs lab coordinators/ RRLs
12:30-14:00 LUNCH
Session II. Improve data quality of IBVPD laboratory network
14:00-16:30
Data quality issues
Overview of RRL data consolidation and analysis
F. Serhan
10
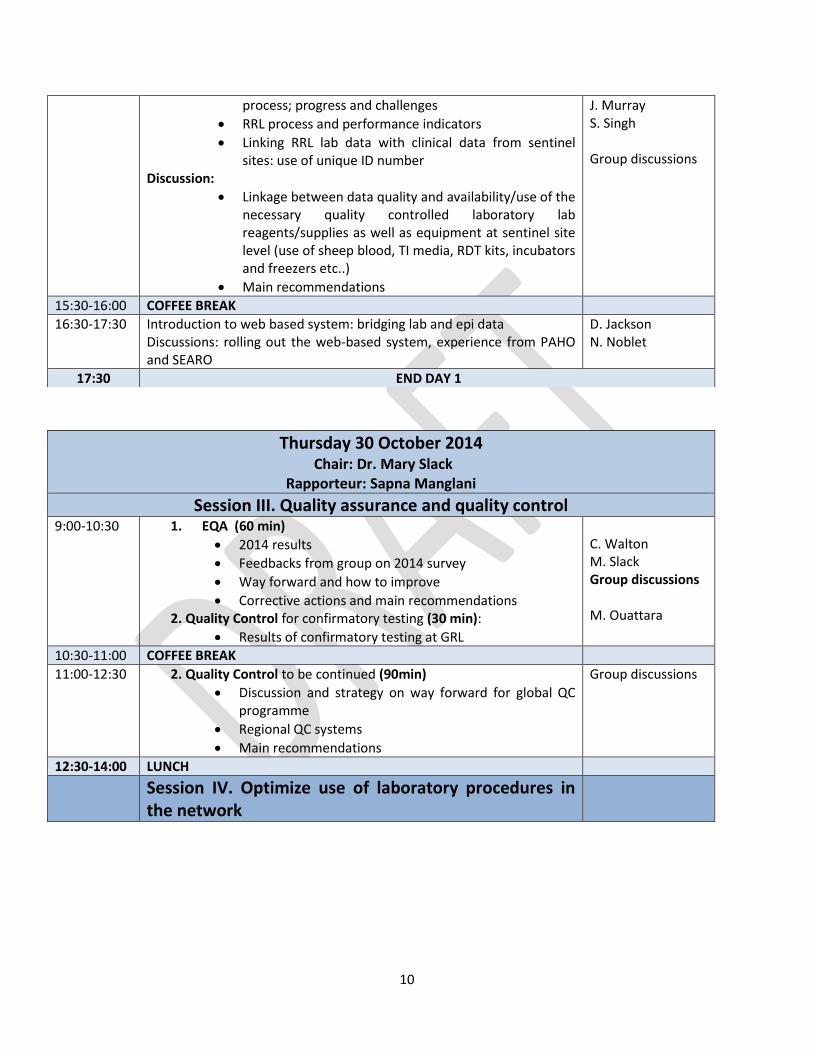
process; progress and challenges
RRL process and performance indicators
Linking RRL lab data with clinical data from sentinel sites: use of unique ID number
Discussion:
Linkage between data quality and availability/use of the necessary quality controlled laboratory lab reagents/supplies as well as equipment at sentinel site level (use of sheep blood, TI media, RDT kits, incubators and freezers etc..)
Main recommendations
J. Murray S. Singh Group discussions
15:30-16:00 COFFEE BREAK
16:30-17:30
Introduction to web based system: bridging lab and epi data Discussions: rolling out the web-based system, experience from PAHO and SEARO
D. Jackson N. Noblet
17:30 END DAY 1
Thursday 30 October 2014 Chair: Dr. Mary Slack
Rapporteur: Sapna Manglani Session III. Quality assurance and quality control
9:00-10:30
1. EQA (60 min)
2014 results
Feedbacks from group on 2014 survey
Way forward and how to improve
Corrective actions and main recommendations 2. Quality Control for confirmatory testing (30 min):
Results of confirmatory testing at GRL
C. Walton M. Slack Group discussions M. Ouattara
10:30-11:00 COFFEE BREAK
11:00-12:30 2. Quality Control to be continued (90min)
Discussion and strategy on way forward for global QC programme
Regional QC systems
Main recommendations
Group discussions
12:30-14:00 LUNCH
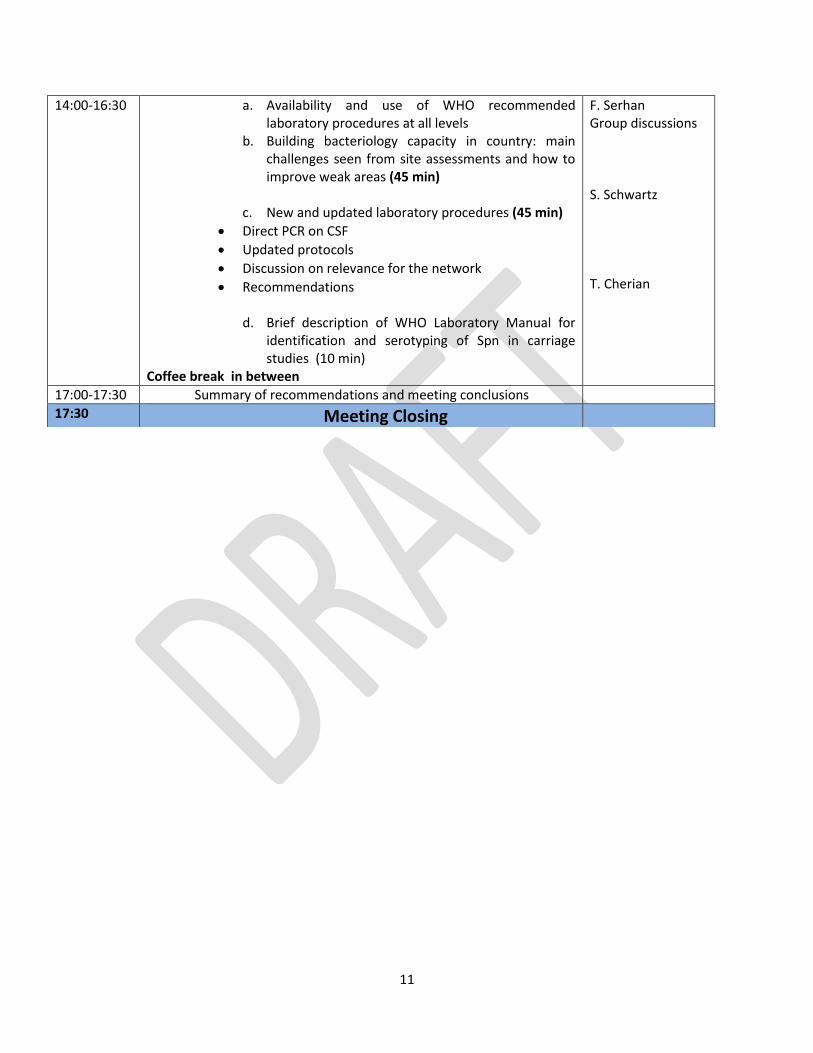
Session IV. Optimize use of laboratory procedures in the network
11
14:00-16:30 a. Availability and use of WHO recommended laboratory procedures at all levels
b. Building bacteriology capacity in country: main challenges seen from site assessments and how to improve weak areas (45 min)
c. New and updated laboratory procedures (45 min)
Direct PCR on CSF
Updated protocols
Discussion on relevance for the network
Recommendations
d. Brief description of WHO Laboratory Manual for identification and serotyping of Spn in carriage studies (10 min)
Coffee break in between
F. Serhan Group discussions S. Schwartz T. Cherian
17:00-17:30 Summary of recommendations and meeting conclusions
17:30 Meeting Closing
12
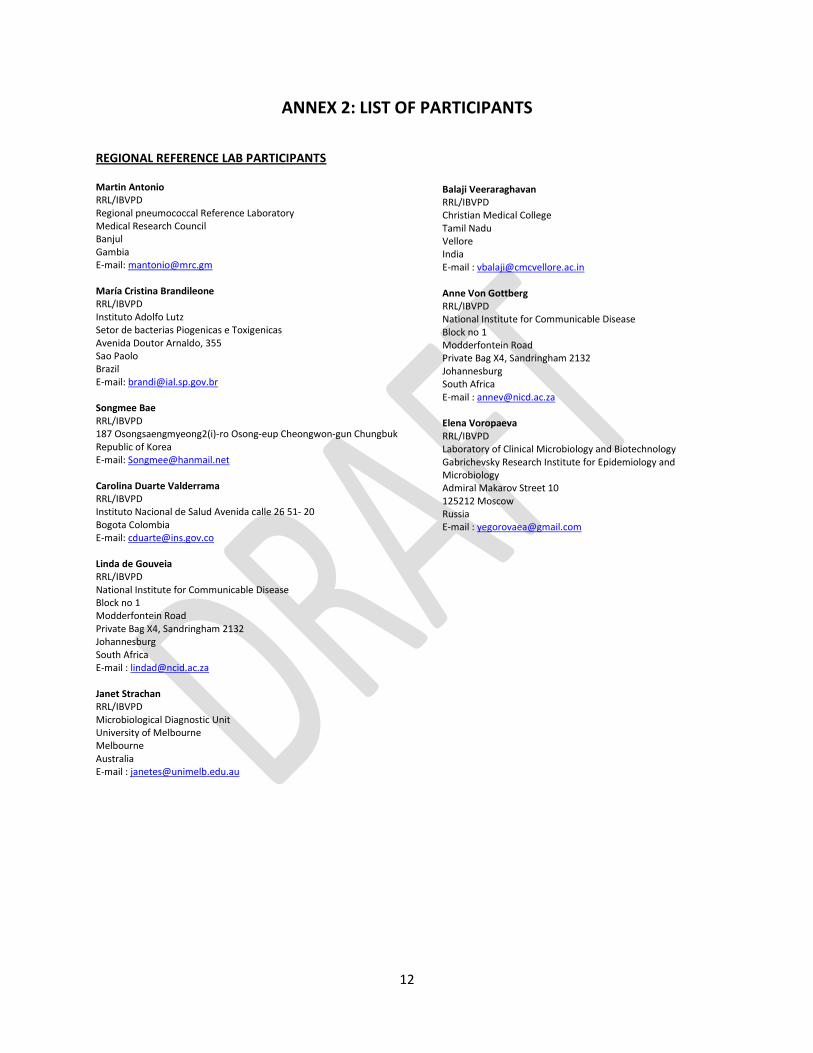
ANNEX 2: LIST OF PARTICIPANTS
REGIONAL REFERENCE LAB PARTICIPANTS Martin Antonio RRL/IBVPD Regional pneumococcal Reference Laboratory Medical Research Council Banjul Gambia E-mail: [email protected] María Cristina Brandileone RRL/IBVPD Instituto Adolfo Lutz Setor de bacterias Piogenicas e Toxigenicas Avenida Doutor Arnaldo, 355 Sao Paolo Brazil E-mail: [email protected] Songmee Bae RRL/IBVPD 187 Osongsaengmyeong2(i)-ro Osong-eup Cheongwon-gun Chungbuk Republic of Korea E-mail: [email protected] Carolina Duarte Valderrama RRL/IBVPD Instituto Nacional de Salud Avenida calle 26 51- 20 Bogota Colombia E-mail: [email protected] Linda de Gouveia RRL/IBVPD National Institute for Communicable Disease Block no 1 Modderfontein Road Private Bag X4, Sandringham 2132 Johannesburg South Africa E-mail : [email protected] Janet Strachan RRL/IBVPD Microbiological Diagnostic Unit University of Melbourne Melbourne Australia E-mail : [email protected]
Balaji Veeraraghavan RRL/IBVPD Christian Medical College Tamil Nadu Vellore India E-mail : [email protected] Anne Von Gottberg RRL/IBVPD National Institute for Communicable Disease Block no 1 Modderfontein Road Private Bag X4, Sandringham 2132 Johannesburg South Africa E-mail : [email protected] Elena Voropaeva RRL/IBVPD Laboratory of Clinical Microbiology and Biotechnology Gabrichevsky Research Institute for Epidemiology and Microbiology Admiral Makarov Street 10 125212 Moscow Russia E-mail : [email protected]
13
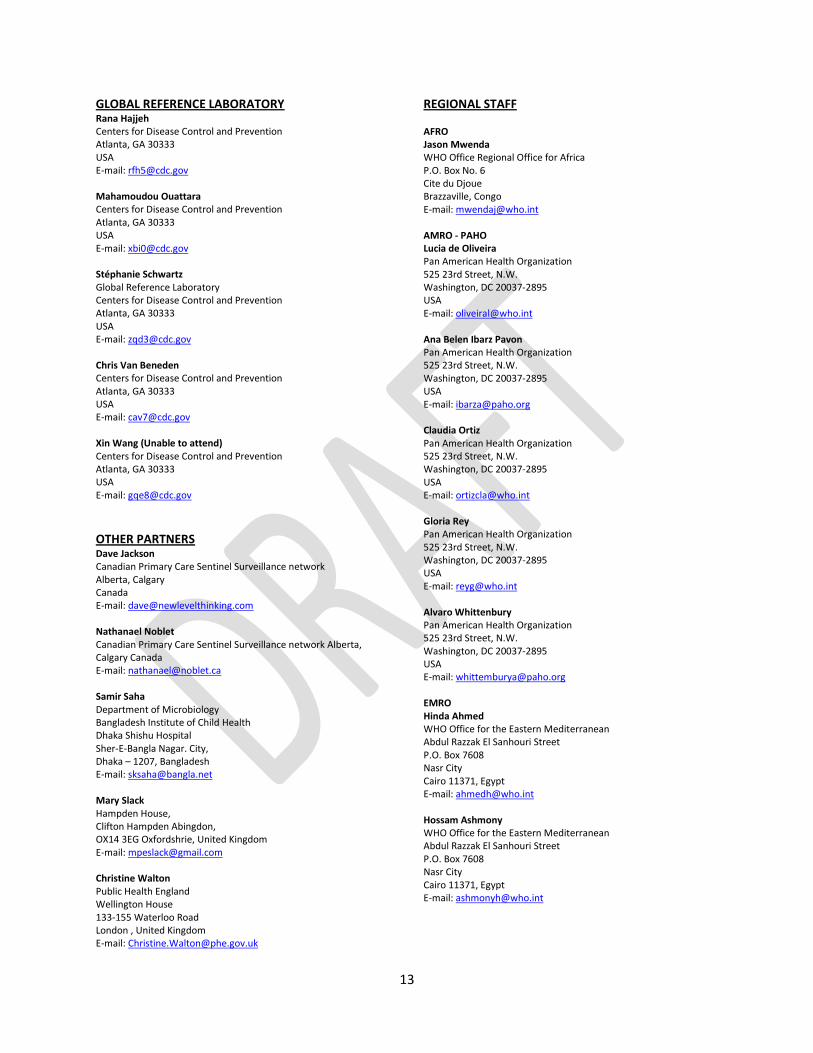
GLOBAL REFERENCE LABORATORY Rana Hajjeh Centers for Disease Control and Prevention Atlanta, GA 30333 USA E-mail: [email protected] Mahamoudou Ouattara Centers for Disease Control and Prevention Atlanta, GA 30333 USA E-mail: [email protected] Stéphanie Schwartz Global Reference Laboratory Centers for Disease Control and Prevention Atlanta, GA 30333 USA E-mail: [email protected] Chris Van Beneden Centers for Disease Control and Prevention Atlanta, GA 30333 USA E-mail: [email protected] Xin Wang (Unable to attend) Centers for Disease Control and Prevention Atlanta, GA 30333 USA E-mail: [email protected]
OTHER PARTNERS Dave Jackson Canadian Primary Care Sentinel Surveillance network Alberta, Calgary Canada E-mail: [email protected] Nathanael Noblet Canadian Primary Care Sentinel Surveillance network Alberta, Calgary Canada E-mail: [email protected] Samir Saha Department of Microbiology Bangladesh Institute of Child Health Dhaka Shishu Hospital Sher-E-Bangla Nagar. City, Dhaka – 1207, Bangladesh E-mail: [email protected] Mary Slack Hampden House, Clifton Hampden Abingdon, OX14 3EG Oxfordshrie, United Kingdom E-mail: [email protected] Christine Walton Public Health England Wellington House 133-155 Waterloo Road London , United Kingdom E-mail: [email protected]
REGIONAL STAFF AFRO Jason Mwenda WHO Office Regional Office for Africa P.O. Box No. 6 Cite du Djoue Brazzaville, Congo E-mail: [email protected] AMRO - PAHO Lucia de Oliveira Pan American Health Organization 525 23rd Street, N.W. Washington, DC 20037-2895 USA E-mail: [email protected] Ana Belen Ibarz Pavon Pan American Health Organization 525 23rd Street, N.W. Washington, DC 20037-2895 USA E-mail: [email protected] Claudia Ortiz Pan American Health Organization 525 23rd Street, N.W. Washington, DC 20037-2895 USA E-mail: [email protected] Gloria Rey Pan American Health Organization 525 23rd Street, N.W. Washington, DC 20037-2895 USA E-mail: [email protected] Alvaro Whittenbury Pan American Health Organization 525 23rd Street, N.W. Washington, DC 20037-2895 USA E-mail: [email protected] EMRO Hinda Ahmed WHO Office for the Eastern Mediterranean Abdul Razzak El Sanhouri Street P.O. Box 7608 Nasr City Cairo 11371, Egypt E-mail: [email protected] Hossam Ashmony WHO Office for the Eastern Mediterranean Abdul Razzak El Sanhouri Street P.O. Box 7608 Nasr City Cairo 11371, Egypt E-mail: [email protected]
14
EURO Dovile Videbaek WHO Office for Europe 8, Scherfigsvej Copenhagen Denmark E-mail: [email protected] Annemarie Wasley WHO Office for Europe 8, Scherfigsvej Copenhagen Denmark E-mail: [email protected]
SEARO Samir Saha Child Health Research Foundation Department of Microbiology Dhaka Shishu Hospital Sher-e-Bangla Nagar Dhaka -1215 Bangladesh E-mail: [email protected] Pushpa Ranjan Wijesinghe World Health Organization Regional Office for South-East Asia I.P Estate, Ring Road New Delhi India E-mail: [email protected]
WPRO Kimberley Fox WHO Office for the Western Pacific United Nations Avenue P.O. Box 2932 1000 Manila Philippines E-mail: [email protected] Varja Grabovac WHO Office for the Western Pacific United Nations Avenue P.O. Box 2932 1000 Manila Philippines E-mail: [email protected]
WHO HEADQUARTERS STAFF Mary Agocs Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Thomas Cherian Department of Immunization, Vaccines and Biologicals Avenue Appia, 20 1211 Geneva 27 Switzerland, E-mail: [email protected]
Carine Cruz Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Marta Gacic Dobo Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Ana Maria Henao Restrepo Department of Immunization, Vaccines and Biologicals Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Sapna Manglani Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland, E-mail: [email protected] Jillian Muray Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Tomoka Nakamura Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Fatima Serhan Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected] Simar Singh Department of Immunization, Vaccines and Biologicals Expanded Programme on Immunization Avenue Appia, 20 1211 Geneva 27 Switzerland E-mail: [email protected]