evidence-based guidance for physiotherapists : the use … · evidence based child health...
TRANSCRIPT
EVIDENCE-BASED GUIDANCEFOR PHYSIOTHERAPISTS
CHA
RTER
ED
OF PH
YSIOTH
ERA
PY
SOC
IETY
DIG
NA SEQ
UI
CHA
RTER
ED
OF
PHYSIO
THER
AP
Y
SOC
IETY
DIG
NA SEQ
UI
ASSOCIATION OF PAEDIATRIC CHARTERED PHYSIOTHERAPISTS
The use of Botulinum Toxin in Children with Neurological Conditions
ASETH
Toxogic
UIDANAP
ond
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 1
2
This guidance is targeted at paediatric physiotherapists involved in the management of children with neurologicalconditions where botulinum toxin (BTX-A) may be an appropriate adjunctive treatment.
To date there are no standardised pathways or consensus of practice for providing BTX-A injection services forchildren. Current provision and practice varies from one locality to another throughout the UK.
Nationally, paediatric physiotherapists have expressed a need for evidence/consensus-based guidance as there is littlespecific advice regarding physiotherapy intervention following BTX-A treatment.
EVIDENCE-BASED GUIDANCEFOR PHYSIOTHERAPISTS The use of Botulinum Toxin in Children with Neurological Conditions
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 2

3
BOTULINUM TOXIN WORKING PARTY
Lesley Katchburian, Clinical Specialist Physiotherapist (Neurodisability), Great Ormond Street Hospital,London (chair)
Stephanie Cawker, Clinical Specialist Physiotherapist (Neurodisability), Great Ormond Street Hospital, London
Susan Coombe, Paediatric Physiotherapist, Norfolk and Norwich Hospital, Norwich, Norfolk
Eileen Kinley, Specialist Paediatric Physiotherapist, Royal Liverpool Children’s NHS Trust,Alder Hey, Liverpool
Robert Shaw, Paediatric Community Physiotherapist, Barnstaple Health Centre, Barnstaple, North Devon
Laura Wiggins,APCP Secretary, Lead Paediatric Physiotherapist, North Glasgow CHCP
Elspeth Will, Clinical Specialist Physiotherapist, Guy’s & St Thomas’ NHS Foundation Trust, London
ACKNOWLEDGEMENTS
The following organisations were consulted:
Association of Paediatric Chartered Physiotherapists (APCP)Chartered Society of Physiotherapy (CSP)Evidence Based Child Health Unit, Institute of Child Health, Royal Liverpool Children's NHS Trust,Alder HeyMembers of The Scoping Groups:Angela Black, Dawn Walton, Pam Chimiak, Pat Clements, Sue Kelly, Susan Cleverley,Jill Davis, Jeanne Hartley,Valerie Kennedy, Sheila McNeill UK Spasticity Forum
The Working Group would also like to thank all those paediatric physiotherapists who responded to the APCPNational Botulinum Toxin Survey, via the national study day and through the iCSP website.
The working party meetings were also sponsored by educational grants from:Association of Paediatric Chartered PhysiotherapistsAllergan LtdIpsen LtdThe writing and printing of the document were also sponsored by an unrestricted educational grant from Ipsen Ltd.
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 3

4
EXECUTIVE SUMMARY
• Botulinum toxin (BTX-A) is an established clinical tool in the management of children with neurological disorders.Current clinical practice has seen an expansion of the clinical indications for BTX-A, with its increasing use in thetreatment of pain and dystonia as well as dynamic spasticity
• The selection of the appropriate child for injection, the target muscle(s), treatment goals, and the post-injectionprogramme are a team decision.This should involve the child and their family, as well as the multidisciplinary team(MDT).The child’s physiotherapist plays a key role in this process
• Physiotherapists who are experienced in the assessment and treatment of growing children with neurologicalconditions have the knowledge and skills required to assess the suitability for BTX-A treatment, and to select theappropriate post-injection management
• Accurate patient assessment identifying the primary problem, and the resultant muscle groups responsible, willresult in more successful treatment with BTX-A.This needs to be used in conjunction with an ongoing therapyprogramme with specific post-injection management. Pre- and post-injection assessments are required forappropriate patient selection, to set realistic goals and to review outcomes
• In most cases BTX-A is unlikely to be successful when used in isolation. In order to maximise its effect, it shouldbe used in conjunction with other appropriate management strategies such as targeted motor training,strengthening, stretching, orthoses etc.A post-injection management programme is likely to optimise the effects ofBTX-A. However, to date there is no consensus regarding content, timing and frequency
• Before considering whether or not a child may benefit from BTX-A treatment, it is important that the relevantsupport services are in place for the child and their parents or carer so that an appropriate post-injectionmanagement programme can be planned and carried out. If follow-up services are inadequate, the use of BTX-Amay not be appropriate.The MDT also needs to consider the ability of child and family to participate and cooperatewith a post-injection management programme
• In all cases, there should be active communication between the BTX-A injection services and the local team.Thisshould involve close liaison between the treating physiotherapist and the injecting team.The responsibility for thechild’s ongoing physical management programme should remain with the referring team
• Physiotherapists should continue to be aware of, and contribute to, research into current clinical practice with BTX-A.This will assist in extending the existing knowledge base and further refine its use. Further research isrequired specifically to look at the adjunctive treatments which are used in conjunction with BTX-A. It is thiscombination of BTX-A with adjunctive interventions that is most likely to result in a successful outcome forchildren with neurological impairments
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 4

5
INTRODUCTION
The adverse effects of spasticity on the growing child are well documented (Graham et al 2003). Botulinum toxin(BTX-A) has been used over the last 15 years in the management of dynamic spasticity in the child with aneurological condition.There is increasing clinical evidence to support its use, but there remains a paucity of practicalguidance available for paediatric physiotherapists.
Paediatric physiotherapists are key members of the multidisciplinary team (MDT) involved in the management ofchildren with neurological conditions.They have the skill set required to assess the need for BTX-A in thispopulation, and are therefore ideally placed to be directly involved with decision making, evaluation and ongoingmanagement of children undergoing BTX-A (Boyd et al 1999).
This guidance is targeted at paediatric physiotherapists involved in the management of children with neurologicalconditions where BTX-A may be an appropriate adjunctive treatment. It is based on the available clinical evidencetogether with expert opinion. Current practice as outlined in the document is based on expert consensus from 16 established paediatric BTX-A services within the UK.This has been further supplemented with informationprovided in the APCP National Survey examining ‘The role of paediatric physiotherapists in the use of botulinumtoxin A – a reflection of current practice (2006)’.
The scientific evidence has been systematically reviewed using the Scottish Intercollegiate Guidelines Network (SIGN)www.sign.ac.uk. Throughout the document the recommendations have been graded where appropriate (seeAppendix 1) to provide the reader with an indication of the effectiveness of the intervention in relation to the levelof scientific evidence.
This is a consensus document of good practice. It is not intended to be a rigid set of rules, but a tool to assistand inform the clinician in the areas of:
• Patient selection • Assessment, goal setting and outcome measures • Post-injection management• Communication • Audit
It is important to note that this guidance is based on current practice, which includes off-license usageof BTX-A.
Details of the practical application of BTX-A (such as injection technique and dosage) is beyond the scope of thisguidance. For those physiotherapists interested in learning more about injection technique or how to become a non-medical injector, we would direct the reader to the practical techniques of BTX- A injections as covered in ‘The roleof physiotherapists in the management of spasticity with botulinum toxin: a consensus guideline’, a supplementproduced in association with Guidelines.
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 5
BACKGROUND
CURRENT PRACTICE
Within the UK there appears to be no agreed or standardised pathway for paediatric BTX-A injection services, andcurrent provision varies depending on locality.
Children receive BTX-A injections usually via one of the following routes:
• Children may be injected by individual practitioners (such as a paediatrician, orthopaedic surgeon,neurologist or occasionally therapy injectors). Ideally this is carried out in co-ordination with follow-upservices, but may sometimes be performed as an isolated procedure
• Children may be referred to a local injection therapy team, who ideally would co-ordinate assessment andfollow-up with the child’s individual therapist and orthotics department
• Where there is no BTX-A service available locally, children may be referred to one of a limited number oftertiary centres which provide BTX-A/spasticity management services
BTX-A ADMINISTRATION
In children, pain management in conjunction with the injection procedure is an important issue.
Children are usually injected under one the following methods of sedation:
• General anaesthesia• Oral sedation (such as Midazolam)• Nitrous oxide (Entonox) sedation
This may be carried out in conjunction with topical analgesia such as EMLA/AMITOP/ethyl chloride spray.
Sedation varies between centres and depends usually on the number of injections, age of the child, respiratory stateand resources available.
The children receive their injections using some form of accurate localisation technique, such as:
• Palpation/ needle movement• EMG guidance • Nerve stimulator• Ultrasound (this is increasingly becoming the technique of choice to identify muscles in paediatrics as it is
precise and non-invasive (Heinan et al 2006))
Although physiotherapists are not always directly involved with the injection process, they have an important role toplay in liaison with the injecting centre prior to injection. In many cases they provide advice regarding muscleselection, timing of repeat injection and in some cases are part of the decision-making process regarding the mostappropriate method of sedation for the child.
6
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 6

7
BOTULINUM TOXIN
IndicationsBTX-A is indicated for the treatment of focal spasticity.The evidence for its use is well documented and will not beaddressed here. Please refer to the Summary of Product Characteristics (www.emc.medicines.org.uk) for thespecific indications for each branded product.
Mode of actionBTX-A is a local muscle relaxant which is highly selective for peripheral nerve terminals containing acetylcholine.When injected into muscle the toxin is taken up into the nerve terminal by endocytosis. Once inside the nerve cell,BTX-A prevents the release of acetylcholine into the synaptic cleft resulting in a reduced muscle contraction. BTX-Ais taken up by the neuromuscular junction within 12 hours.The onset of the response varies, but usually occursgradually over the first week.There can be a huge variation in clinical response with effects observed immediately, orin some cases after 2-3 weeks.The effect of BTX-A is temporary; recovery of the nerve terminal takes place via‘sprouting’ (re-establishing the original neuromuscular connection), this takes place gradually over 12-16 weeks.Although the clinical response may vary, generally the injected muscles show some detectable weakness for 3-4months. In some cases the functional benefits of BTX-A may continue long after the chemical effects of the BTX-Ahave gone.
Due to the temporary effect of BTX-A, repeat injections may be required.The recommended minimum time intervalfor re-injection is 3 months; (more frequent re-injection is associated with a higher incidence of side effects andantibody formation).
The ideal frequency of re-injection in the paediatric population has yet to be established and depends on timely clinicalassessment and evaluation. However, in view of the paucity of evidence of the effect of BTX-A on growing muscle, andthe aim to prolong the effect with adjunctive measures, most paediatric centres limit their frequency of re-injection toa maximum of two injection sessions a year. Usually there is a re-injection interval of 6-12 months, unless specificallyindicated for pain or acute dystonia interfering with function, which may require more frequent re-injection.
ReferencesAPCP National Botulinum Toxin Survey:The role of the physiotherapist in the use of botulinum toxin A - a reflection of current practice. 2006. (In press)
Boyd R, Kerr Graham H. Objective measurement of clinical findings in the use of botulinum toxin A for the management of children with cerebral
palsy. Eur J Neurol 1999;6:23-35
Graham H, Selber P. Musculoskeletal aspects of cerebral palsy. J Bone Joint Surg Br 2003;85B:152-166
Heinan F, Molenaers G, Fairhurst C et al. European consensus table on botulinum toxin for children with cerebral palsy. Eur J Neurol 2006;10:215-225
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 7
SECTION A: PATIENT SELECTION
Although licensed only for use in cerebral palsy, BTX-A may also be appropriate for children with:
• Post-traumatic brain injury• Genetic conditions (i.e hereditary spastic paraplegia)• Metabolic conditions (i.e mitochondrial disorders)• Neurodegenerative disorders
A child should be considered for BTX-A treatment where there is focal, dynamic spasticity and/or dystonia whichmay now, or in the future, interfere with function, care-giving, result in torsional abnormalities or cause pain [D].
KEY CONSIDERATIONS
AgeThere is no evidence to suggest that age is an absolute criteria for patient selection. Research supports positiveresults for BTX-A treatment at all ages, but generally younger children (< 8 years) are considered most appropriate(randomised controlled trials reviewed ages from 2-16 years).
Recommendations• Younger children are considered more appropriate for BTX-A treatment as they are less likely to have
established fixed soft tissue, bony torsional abnormalities, or to have learned compensatory movementpatterns in the presence of long-established spasticity/dystonia [B]
• BTX-A may be appropriate for the older child who still has a dynamic component to their functionalproblem when used in conjunction with other treatment modalities [B]
Muscle selectionBTX-A works by reducing the dynamic component of overactive spastic or dystonic muscles.Appropriate muscleselection is a key factor. It is important to identify the specific muscles involved in causing the child’s primaryfunctional problem.
The highest quality studies have concentrated on investigating the effects of injections into gastrocnemius and/orsoleus muscles in the ambulant child with dynamic equinus (the licensed use of BTX-A), and have shown improvedclinical and functional outcomes at all ages.
More extensive use of BTX-A in the treatment of other muscle groups remains ‘off-license’.Where doses and musclegroups represent appropriate but unlicensed use of BTX-A, this is however in line with agreed clinical practice.
There have been fewer studies, mainly of lower evidence levels, investigating outcomes for other lower limb musclegroups in ambulant children. Successful outcomes have been reported to correct a variety of gait problems, includingcrouch, scissoring, and equinovarus/valgus foot deformity.The muscles injected have included tibialis posterior,peroneii, hamstrings, hip adductors, and hip flexors.
There are relatively few studies involving non-ambulant children, but evidence suggests that injections into adductorsmay reduce the rate of hip subluxation.
8
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 8
9
Other outcomes for non-ambulant children include reduced spasm/pain, (including the perioperative period),improved caregiving, and improved sitting.The muscles injected have included hip flexors, adductors, hamstrings andquadriceps. More recently positive outcome has been reported following injections to the trunk muscles (includingparaspinals and shoulder girdle) to improve posture.
Studies investigating BTX-A in the upper limb suggest improvements following injections into a number of muscles inthe arm and hand. Initial work with BTX-A injections to the upper limb, demonstrated an improvement in cosmesisand little change in function. More recent work has highlighted a positive correlation with BTX-A and functionalimprovement.
Number of muscle groups injectedBTX-A, although recognised as a focal treatment for dynamic spasticity, is increasingly used for multi-level injections.These may offer both the ambulant and non-ambulant child a more comprehensive management strategy in one episode.
Muscle selectivityIn predicting which children may benefit from BTX-A, there is evidence within the literature to suggest a correlationwith a child’s ability to perform isolated movements pre-injection, and a positive outcome post-injection in recruitingboth agonist and antagonist muscle activity.
The following factors do not preclude treatment with BTX-A, but proceed with caution if thepatient has:
• Fixed contractures –most studies do not exclude the presence of fixed contractures, but BTX-A alonewill not lengthen shortened muscles, and it may need to be considered in conjunction with other treatmentmodalities [B]
• Established bony deformities: BTX-A cannot alter torsional abnormalities [B] • Marked muscle weakness: reducing spasticity may unmask marked muscle weakness which may have a
detrimental effect on function [D]• Generalised spasticity: where alternative methods of spasticity management may be more appropriate [D]• Problems with implementation of an effective post-injection management programme [D]
RecommendationBTX-A works by reducing overactivity in spastic or dystonic muscle. Successful outcome therefore depends onaccurate selection of the muscle(s) primarily responsible for the identified problem [B]
ReferencesAde-Hall RA, Moore AP. Botulinum toxin type A in the treatment of lower limb spasticity in cerebral palsy.The Cochrane Database of Systematic
Reviews 2000 Issue 1 Art No: CD001408. DOI: 10.1002/14651858. CD00148
Baker R, Jasinski M, Maciag-Tymecka I et al. Botulinum toxin treatment of spasticity in diplegic cerebral palsy: a randomised double-blind, placebo-
controlled, dose-ranging study. Dev Med Child Neurol 2002;44:666-675
Boyd RN, Pliatsios V, Graham HK. Use of objective measures in predicting response to botulinum toxin A in children with cerebral palsy. Dev Med
Child Neurol 1998; 40(Suppl 78):48
Calderon-Gonzalez R, Calderon-Sepulveda R, Rincon-Reyes M et al . Botulinum toxin A in the management of cerebral palsy. Pediatr Neurol
1994;10(4):284-288
Corry JS, Cosgrove AP,Walsh EG et al. Botulinum toxin A in the hemiplegic upper limb: a double blind trial. Dev Med Child Neurol 1997;39(3):185-93
El-Etribi MA, Salem ME, El- Shakankiry HM et al.The effect of botulinum toxin type A injection on spasticity in children with spastic diplegic cerebral
palsy:an Egyptian study. Int J Rehabil Res 2004;27(4):275-281
Fattal-Valevski A, Giladi N, Domanievitz D et al. Parameters for predicting favorable responses to botulinum toxin in children with cerebral palsy.J
Child Neurol 2002;17(4):272-277
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 9
Fehlings D, Rang M, Glazier J, et al.An evaluation of botulinum toxin A injections to improve upper extremity function in children with hemiplegic
cerebral palsy. J Paediatr 2000;137:331-337
Friedman A, Diamond M, Johnston MV et al. Effects of botulinum toxin A on upper limb spasticity in children with cerebral palsy. Am J Phys Med
Rehabil 2000;79:53-59
Heinan F,.Linder M, Mall V et al.Adductor spasticity in children with cerebral palsy and treatment with botulinum toxin A:The parents view of
functional outcome. Eur J Neurol 1999;6(4):S47-S50
Kanovsky P, Bares M, Severa S et al. Functional benefit of botulinum toxin (Dysport®) in the treatment of dynamic equines cerebral palsy spasticity: a
prospective, multicentre, double-blind, placebo-controlled study. Cesk Slov Neurol Neurochir 2004:67(1)16-23
Koman LA, Mooney I, Smith B et al. Management of cerebral palsy with botulinum A toxin: preliminary investigation. J Pediatr Orthop 1993;13(4):489-95
Mall V, Heinen F, Siebel A et al.Treatment of adductor spasticity with BTX-A in children with CP: a randomized, double-blind, placebo-controlled study.
Dev Med Child Neurol 2006;48: 10-13
Molenaers G, Desloovere K, Eyessen M et al. Botulinum toxin type A treatment of cerebral palsy: an integrated approach. Eur J Neurol;1999:6 (suppl 4)
Mulligan H, Borkin H, Chaplin K et al.The efficacy of botulinum toxin A in the treatment of spasticity in ambulant children with cerebral palsy: a
structured review. New Zealand. J Physio 2001;29(3):18-28
Paolicelli PB, Ferrari A, Lodesani M et al. Use of botulinum toxin type A in walking disorders of children with cerebral palsy. Eur Medicophys
2001;37(2):83-92
Papadonikolakis AS,Vekris MD, Korompilias AV et al. Botulinum A toxin for treatment of lower limb spasticity in cerebral palsy - gait analysis in 49
patients. Acta Orthop Scand 2003; 74(6):749-755
Pidcock FS, Fish DE, Johnson-Greene D et al. Hip migration percentage in children with cerebral palsy treated with botulinum toxin type A. Arch Phys
Med Rehabil 2005; 86(3):431-435
Placzek G, Deuretzbacher G, Meiss AL.Treatment of lateralisation and subluxation of the hip in cerebral palsy with botulinum toxin A: Preliminary
results based on the analysis of migration percentage data. Neuropediatr 2004;35(1):6-9
Steenbeek D, Meester-Delver A, Becher JG et al.The effect of botulinum toxin type A treatment of the lower extremity on the level of functional
abilities in children with cerebral palsy: evaluation with goal attainment scaling. Clin Rehabil 2005;19(3):274-282
Ubhi T, Bhakta BB, Ives H L et al. Randomised double blind placebo controlled trial of the effect of botulinum toxin on walking in cerebral palsy. Arch
Dis Child 2000;83:481-487
Wall S A, Chait LA,Temlett JA et al. Botulinum toxin chemo denervation: a new modality in cerebral palsied hands. B J Plast Surg 1993;46:703-706
Wong V. Use of botulinum toxin injection in 17 children with spastic cerebral palsy. Paediatr Neurol 1998;18(2):124-131
Wong V, Ng A, Sit P. Open label study of botulinum toxin for upper limb spasticity in cerebral palsy. Eur J Child Neurol 2002;2:138-142
Zelnik N, Giladi N, Keren G et al.The role of botulinum toxin in the treatment of lower limb spasticity in children with cerebral palsy- a pilot study.
Isr J Med Sci 1997;33(2):129-133
10
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 10

11
SECTION B: ASSESSMENT, GOAL SETTING AND OUTCOME MEASURES
ASSESSMENT
Pre-injection• Following an initial screening for suitability for BTX-A injections the child should be assessed, ideally within
the four weeks prior to injection.At this stage goals should be agreed.
Two further assessments are recommended post-injection:
• Early post-injection phase (at peak chemical effect), around 3-6 weeks.This will inform how best to targetongoing post-injection management. In the early post-injection phase, a positive change in the range ofmovement, dynamic spasticity, or pain would normally be expected
• Late post-injection phase (when the chemical effect of the toxin has disappeared) between 3 and 6 months.Thiswill inform the decision as to whether further BTX-A injections are indicated, and the required time scale, aswell as reviewing long-term management such as referral on to surgical services or back to the local team [D]
Clinical note In the initial post-injection phase there may be some deterioration in function due to changes in tone and range ofmotion (ROM), this usually resolves within 4-6 weeks post-injection.
There may be a difference in timing of response dependent on the level of neurological involvement.The child withdiplegia or total body involvement may show earlier changes (between 2 and 4 weeks) post-injection. However, achild with hemiplegia may show later changes i.e between 4 and 6 weeks (Baker et al 1999).This may have implicationsfor the timing of the post-injection reviews.
GOAL SETTING
The literature identifies success with the following functional goals (in many cases there may be overlap in goals withthe ambulant and non-ambulant child):
Ambulant• Functional walking may improve [C] • Appearance of walking may improve [B]• Gross motor skills may improve e.g. standing, transfers, sitting ability [D]• The risk of deformity may be reduced in the short-term and may delay surgical intervention [B]• Improved tolerance of orthoses or casting [D]• Reduction in painful spasms [D]• Improved sleep pattern[D]
Non-ambulant • Personal care and hygiene may improve [D]• Nursing care may be easier [D]• Reduction in pain (including peri-operative use) [D]• Improved sleep pattern [D]• Improved tolerance of postural management equipment [D]• Improved quality of life [D]
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 11
Upper limb• Personal care and hygiene may improve [D]• Cosmesis may improve [D]• Function may improve [C]
Goal setting, measurement and assessment should be a collaborative process, involving the child and theirparents or carer, as part of a MDT [D].
Good practice states that specific goals should be set with the relevant outcome measure.All parties shouldunderstand and agree to the goals which should adhere to the SMART directive (see Table 1).
Table 1: SMART directive Goals must be SMART
S = SpecificM = Measurable A = AchievableR = RealisticT = Timed
Above all the goals should express realistic, achievable benefits that are meaningful to the child and their parents or carer.
OUTCOME MEASURES
Measurement selection Measurement selection should follow the guidance outlined in The Chartered Society of Physiotherapy (CSP) CoreStandard (see Table 2).
Table 2:The Chartered Society of Physiotherapy Core Standard 6
Taking account of the patient’s problems, a published, standardised, valid, reliable and responsive measure isused to evaluate the change in the patient’s health status:
• The physiotherapist selects an outcome measure that is relevant to the patient’s problems • The physiotherapist ensures that the outcome measure is acceptable to the patient• The physiotherapist selects an outcome measure that he/she has the necessary skill and experience to use,
administer and interpret • The physiotherapist takes account of the patient’s welfare during the administration of the measure• Written instructions in the manufacturers manual, test designer’s manual or service guidelines are followed
during the administration and scoring of the measure• The result of the measurement is recorded promptly• The same measure is used at the end of the episode of care
12
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 12
13
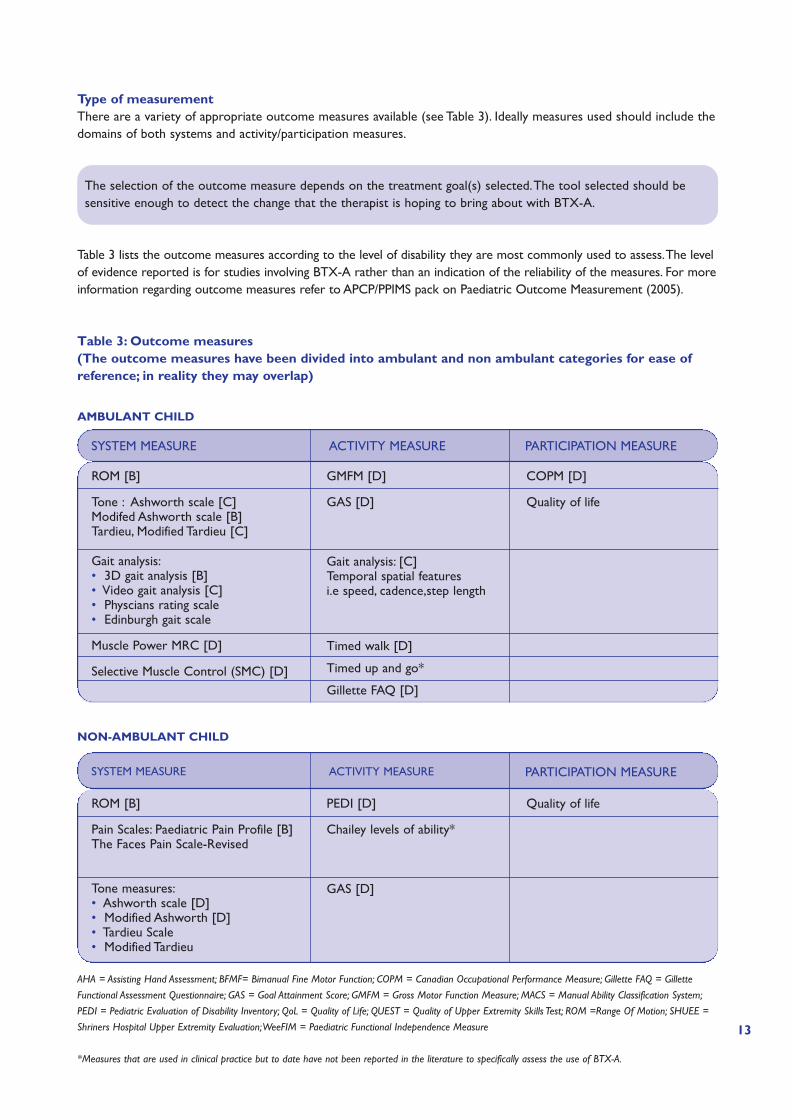
Type of measurementThere are a variety of appropriate outcome measures available (see Table 3). Ideally measures used should include thedomains of both systems and activity/participation measures.
The selection of the outcome measure depends on the treatment goal(s) selected.The tool selected should besensitive enough to detect the change that the therapist is hoping to bring about with BTX-A.
Table 3 lists the outcome measures according to the level of disability they are most commonly used to assess.The levelof evidence reported is for studies involving BTX-A rather than an indication of the reliability of the measures. For moreinformation regarding outcome measures refer to APCP/PPIMS pack on Paediatric Outcome Measurement (2005).
Table 3: Outcome measures(The outcome measures have been divided into ambulant and non ambulant categories for ease ofreference; in reality they may overlap)
SYSTEM MEASURE ACTIVITY MEASURE PARTICIPATION MEASURE
ROM [B]
Tone : Ashworth scale [C]Modifed Ashworth scale [B]Tardieu, Modified Tardieu [C]
Gait analysis:• 3D gait analysis [B]• Video gait analysis [C]• Physcians rating scale • Edinburgh gait scale
Muscle Power MRC [D]
Selective Muscle Control (SMC) [D]
GMFM [D]
GAS [D]
Gait analysis: [C]Temporal spatial featuresi.e speed, cadence,step length
Timed walk [D]
Timed up and go*
Gillette FAQ [D]
COPM [D]
Quality of life
NON-AMBULANT CHILD
AMBULANT CHILD
SYSTEM MEASURE ACTIVITY MEASURE PARTICIPATION MEASURE
ROM [B]
Pain Scales: Paediatric Pain Profile [B]The Faces Pain Scale-Revised
Tone measures:• Ashworth scale [D]• Modified Ashworth [D]• Tardieu Scale• Modified Tardieu
PEDI [D]
Chailey levels of ability*
GAS [D]
Quality of life
AHA = Assisting Hand Assessment; BFMF= Bimanual Fine Motor Function; COPM = Canadian Occupational Performance Measure; Gillette FAQ = Gillette
Functional Assessment Questionnaire; GAS = Goal Attainment Score; GMFM = Gross Motor Function Measure; MACS = Manual Ability Classification System;
PEDI = Pediatric Evaluation of Disability Inventory; QoL = Quality of Life; QUEST = Quality of Upper Extremity Skills Test; ROM =Range Of Motion; SHUEE =
Shriners Hospital Upper Extremity Evaluation;WeeFIM = Paediatric Functional Independence Measure
*Measures that are used in clinical practice but to date have not been reported in the literature to specifically assess the use of BTX-A.
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 13
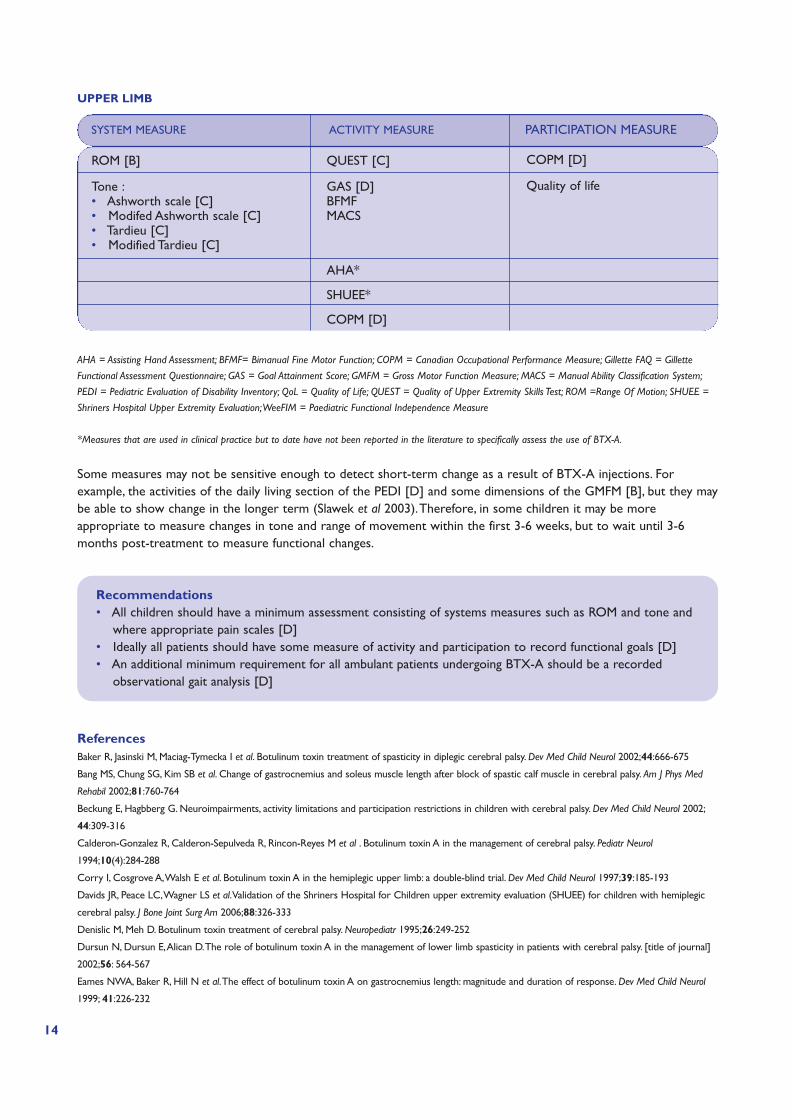
Some measures may not be sensitive enough to detect short-term change as a result of BTX-A injections. Forexample, the activities of the daily living section of the PEDI [D] and some dimensions of the GMFM [B], but they maybe able to show change in the longer term (Slawek et al 2003).Therefore, in some children it may be moreappropriate to measure changes in tone and range of movement within the first 3-6 weeks, but to wait until 3-6months post-treatment to measure functional changes.
Recommendations• All children should have a minimum assessment consisting of systems measures such as ROM and tone and
where appropriate pain scales [D] • Ideally all patients should have some measure of activity and participation to record functional goals [D]• An additional minimum requirement for all ambulant patients undergoing BTX-A should be a recorded
observational gait analysis [D]
References Baker R, Jasinski M, Maciag-Tymecka I et al. Botulinum toxin treatment of spasticity in diplegic cerebral palsy. Dev Med Child Neurol 2002;44:666-675
Bang MS, Chung SG, Kim SB et al. Change of gastrocnemius and soleus muscle length after block of spastic calf muscle in cerebral palsy. Am J Phys Med
Rehabil 2002;81:760-764
Beckung E, Hagbberg G. Neuroimpairments, activity limitations and participation restrictions in children with cerebral palsy. Dev Med Child Neurol 2002;
44:309-316
Calderon-Gonzalez R, Calderon-Sepulveda R, Rincon-Reyes M et al . Botulinum toxin A in the management of cerebral palsy. Pediatr Neurol
1994;10(4):284-288
Corry I, Cosgrove A,Walsh E et al. Botulinum toxin A in the hemiplegic upper limb: a double-blind trial. Dev Med Child Neurol 1997;39:185-193
Davids JR, Peace LC,Wagner LS et al.Validation of the Shriners Hospital for Children upper extremity evaluation (SHUEE) for children with hemiplegic
cerebral palsy. J Bone Joint Surg Am 2006;88:326-333
Denislic M, Meh D. Botulinum toxin treatment of cerebral palsy. Neuropediatr 1995;26:249-252
Dursun N, Dursun E,Alican D.The role of botulinum toxin A in the management of lower limb spasticity in patients with cerebral palsy. [title of journal]
2002;56: 564-567
Eames NWA, Baker R, Hill N et al.The effect of botulinum toxin A on gastrocnemius length: magnitude and duration of response. Dev Med Child Neurol
1999; 41:226-232
14
AHA = Assisting Hand Assessment; BFMF= Bimanual Fine Motor Function; COPM = Canadian Occupational Performance Measure; Gillette FAQ = Gillette
Functional Assessment Questionnaire; GAS = Goal Attainment Score; GMFM = Gross Motor Function Measure; MACS = Manual Ability Classification System;
PEDI = Pediatric Evaluation of Disability Inventory; QoL = Quality of Life; QUEST = Quality of Upper Extremity Skills Test; ROM =Range Of Motion; SHUEE =
Shriners Hospital Upper Extremity Evaluation;WeeFIM = Paediatric Functional Independence Measure
*Measures that are used in clinical practice but to date have not been reported in the literature to specifically assess the use of BTX-A.
UPPER LIMB
SYSTEM MEASURE ACTIVITY MEASURE PARTICIPATION MEASURE
ROM [B]
Tone :• Ashworth scale [C]• Modifed Ashworth scale [C]• Tardieu [C]• Modified Tardieu [C]
QUEST [C]
GAS [D]BFMFMACS
AHA*
SHUEE*
COPM [D]
COPM [D]
Quality of life
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 14
15
El-Etribi MA, Salem ME, El- Shakankiry HM et al.The effect of botulinum toxin type A injection on spasticity in children with spastic diplegic cerebral
palsy:an Egyptian study. Intl J Rehabil Res 2004;27:275-281
Eliasson AC, Rosblad B, Beckung E et al. Development and reliability of a system to classify hand function in children with cerebral palsy: MACS AACPDM
: 2005 Florida
Falso M, Fiaschi A, Manganotti P. Pedobarometric evaluation of equinus foot disorder after botulinum toxin A in children with cerebral palsy: a pilot study.
Dev Med Child Neurol 2005;47: 396-402
Fattal-Valevski A, Giladi N, Domanievitz D et al. Parameters for predicting favorable responses to botulinum toxin in children with cerebral palsy.J Child
Neurol 2002;17(4):272-277
Hicks CL, von Baeyer CL, Spafford P et al.The Faces Pain Scale-Revised.Toward a common metric in paediatric pain measurement. Pain 2001;93;173-183
Hunt A, Goldman A, Seers K et al. Clinical validation of the paediatric pain profile. Dev Med Child Neurol 2004;46:9-18
Hurvitz EA, Conti GE, Brown SH. Changes in movement characteristics of the spastic upper extremity after botulinum toxin injection. Arch Phys Med
Rehabil 2003;84:444-454
Kanovsky P, Bares M, Severa S et al. Functional benefit of botulinum toxin (Dysport®) in the treatment of dynamic equinus cerebral palsy spasticity: a
prospective, multicentre, double-blind, placebo-controlled study. Cesk Slov Neurol Neurochir 2004;67:16-23
Krumlinde-Sunholm L, Eliasson AC. Development of the assisting hand assessment: a rasch built measure intended for children with unilateral upper limb
involvement. Scand J Occupat Ther 2003;10:16-26
Paolocelli PB, Ferrai A, Lodesan M et al. Use of botulinum toxin type A in walking disorders of children with cerebral palsy. Europa Medicophysica
2001;37:83-92
Papadonikolakis AS,Vekris MD, Korompilias AV et al. Botulinum A toxin treatment of lower limb spasticity in cerebral palsy. Acta Orthop Scand
2003;74:749-755
Polack F, Morton R,Ward C et al. Double blind comparison study of two doses of botulinum toxin A injected into calf muscles in children with
hemiplegic cerebral palsy. Dev Med Child Neurol 2002;44:551-555
Sarioglu B, Seradaroglu G,Tutuncuoglu S et al.The use of botulinum toxin type A treatment in children with spasticity. Pediatr Neurol 2003;29:299-301
Slawek J, Kilmont L. Functional improvement in cerebral palsy patients treated with botulinum toxin A injections – preliminary results. Eur J Neurol
2003;10:313-317
Steenbeek D, Meester-Delver A, Becher JG et al.The effect of botulinum toxin type A treatment of the lower extremity on the level of functional abilities
in children with cerebral palsy: evaluation with goal attainment scaling. Clin Rehabil 2005;19(3):274-282
Sutherland DH, Kaufman KR,Wyatt MP et al. Injection of botulinum A toxin into gastrocnemius muscle of patients with cerebral palsy :a 3-dimensional
motion analysis study. Gait and Posture 1995;4:269-279
Wallen MA, O’Flaherty SJ,Waugh M-C. Functional outcomes of intramuscular botulinum toxin A in the upper limbs of children with cerebral palsy: a
phase II trial. Arch Phys Med Rehabil 2004;85:192-200
Williams EN, Carroll SG, Reddihough DS et al. Investigation of the timed ‘ Up & Go’ test in children. Dev Med Child Neurol 2005;47:518-524
Wong V, Ng A, Sit P. Open label study of botulinum toxin for upper limb spasticity in cerebral palsy. Eur J Child Neurol 2002;2:138-142
Zelnik N, Giladi N, Keren G et al.The role of botulinum toxin in the treatment of lower limb spasticity in children with cerebral palsy- a pilot study. Isr J
Med Sci 1997;33(2):129-133
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 15
SECTION C: POST-INJECTION MANAGEMENT PROGRAMME
BTX-A AS AN ADJUNCTIVE TREATMENT
BTX-A should be used in conjunction with, and as part of, a long-term management programme. Specific goals for itsuse should be agreed with the child, their parents or carer and the MDT.
Depending on the agreed goals, treatment with BTX-A, when used with other interventions, can provide a ‘window ofopportunity’ to achieve longer-term benefits for the child with a neurological condition. It is therefore imperative thata timely and appropriate physiotherapy management programme is in place during the post-injection period.
Without therapy support, the benefits of the intervention are unlikely to be maximised.The child’s physiotherapist isbest placed to take responsibility for developing and co-ordinating an appropriate post-injection managementprogramme, with advice and support from tertiary/injecting teams when required or appropriate.
The selection and timing of any follow-up intervention will depend on:
• The agreed goals for the BTX-A injections• The ability of the child and their parents or carer to participate• The availability and structure of local resources
INTERVENTIONS
RecommendationBTX-A is less likely to be successful when used in isolation from other management strategies.The guidancerecommends that appropriate, timely interventions, used in conjunction with BTX-A, can improve the outcomefor many children with neurological conditions [D].
The following specific interventions have been reported both in the literature and in the APCP National Survey topotentiate the effect of BTX-A, but to date there is no consensus regarding timing and frequency.
PhysiotherapyAlthough physiotherapy is recommended in conjunction with BTX-A, as in the case of much therapeutic interventionwith neurological conditions, there is little evidence in the literature to support its specific effectiveness.To meet thetherapeutic goals post-injection, a combination of impairment level interventions and functional activity basedinterventions have been reported in the literature.
Strategies described post-intervention include:
• Neurodevelopmental therapy • Targeted motor training • Gait/locomotion training • Activities of daily life / functional training • Therapeutic horse riding • Constraint induced movement therapy • Motor re-learning programme • Home activity programmes • Muscle strengthening
These were consistent with the therapeutic interventions highlighted in the APCP National Survey.
16
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 16

17
Timing and frequency The clinical response to BTX-A varies between children. It is therefore impossible to be prescriptive about thetiming of intervention post-injection. It is the responsibility of the child’s physiotherapist to assess outcomepost-injection and identify the treatment required to potentiate the effect of BTX-A, including the timing andfrequency of this intervention.
In the APCP National Survey, 69% of respondents would increase therapy provision in the acute post-injection periodwhen clinically indicated.The favoured approach being increased blocks of intensive therapy usually for 6 weeks withinthe acute phase.
RecommendationThe child’s therapy programme should be reviewed in the initial post-injection period in order to implementany changes required due to an alteration in tone, range of motion or function [D].
ReferencesLannin N, Clark K, Scheinberg A. New South Wales therapy practices for children with cerebral palsy who have received botulinum toxin-A. Aus
Occupational Ther J 2004;51:208-212
Leach J. Children undergoing treatment with botulinum toxin: the role of the physical therapist. Muscle & Nerve 1997:20(suppl 6):2194-2207
O’Neil ME, Fragala MA, Dumas HM. Physical therapy intervention for children with cerebral palsy who receive botulinum toxin A injections. Paediatr
Phys Ther 2003;15(4):204-215
Muscle stretchingSustained stretch is widely used to prevent contracture development.There are few studies which examine thesuccess of stretching programmes, and no specific studies relating to BTX-A. However, improvement in a stretchingprogramme is a frequently quoted goal in relation to BTX-A. In the APCP National Survey, 73% of respondentsworked specifically on muscle stretching post-injection.
BTX-A by reducing a child’s dynamic tone, may make stretching of the injected muscles easier to performand improve the tolerance of stretching programmes.
ReferencesLannin N, Clark K, Scheinberg A. New South Wales therapy practices for children with cerebral palsy who have received botulinum toxin-A. Aus
Occupational Ther J 2004;51:208-212
O’Neil ME, Fragala MA, Dumas HM. Physical therapy intervention for children with cerebral palsy who receive botulinum toxin A injections. Paediatr
Phys Ther 2003;15(4):204-215
Pin T, Dyke P, Chan M.The effectiveness of passive stretching in children with cerebral palsy. Dev Med Child Neurol 2006; 48:855-862
Tardieu C, Lespargot A,Tarbary C et al. For how long must the soleus muscle be stretched each day to prevent contracture. Dev Med Child Neurol
1988;30:3-10
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 17
Muscle strengtheningWeakness is a recognised characteristic in the child with a neurological condition. In children with spastic cerebralpalsy, short-term strength training programmes demonstrate functional improvements, particularly evident in gaitfunction, without increases in spasticity or abnormal movement patterns [B].
Following BTX-A, the period of chemical denervation of the injected muscles provides an opportunity forstrengthening antagonist, and where indicated, agonist muscles in motor training programmes [D].
In the APCP National Survey, 82% of respondents worked specifically on muscle strengthening post-injection.
ReferencesBoyd RN, Pliatsios V, Starr R et al. Biomechanical transformation of the gastroc–soleus muscle with botulinum toxin A in children with cerebral palsy.
Dev Med Child Neurol 2000;42:32-41
Damiano DL,Abel MF. Functional outcomes of strength training in spastic cerebral palsy. Arch Phys Med Rehabil 1998;79:119-125
Dodd KJ,Taylor NF, Kerr Graham H.A randomized clinical trial of strength training in young people with cerebral palsy. Dev Med Child Neurol
2003;45:652-657
OrthosesOrthoses are commonly used for children with neurological conditions to prevent deformity, support normal jointalignment and to facilitate function.Although the use of orthotics is advocated in conjunction with BTX-A, there arefew studies in the literature that examine the specific role of BTX-A and orthoses.
In the APCP National Survey, 65% of respondents stated that improved splint tolerance was a goal of BTX-Atreatment and 75% would modify orthoses post-injection.
Recommendations• Where there are problems with splint tolerance due to dynamic overactivity of the muscle, it may be
appropriate to reduce spasticity with BTX-A to improve the tolerance of the orthosis [D]
• Following treatment with BTX-A, a review of the child’s orthotic prescription may be necessary, togetherwith a review of sitting and standing equipment [D]
There are claims in the literature that night splinting and day orthoses offer sustained stretch of spastic muscle,preserve muscle length, and influence the long-term effects of BTX-A treatment.A combined approach of multi-levelinjections and orthoses in an integrated approach has been shown to have a longer lasting effect in comparison toBTX-A in isolation (Heinan et al 2006; Molenaars et al 1999).
However, there have been smaller conflicting studies looking specifically at the long-term carry over following nighttime splinting and BTX-A which have not shown any clinical significance (Rosenbloom et al 2003; Givon et al 2003).
In the non-ambulant child there has been increasing use of use of BTX-A injections to adductors and hamstrings,together with a variable hip abduction orthosis in an attempt to control hip subluxation.To date the short-termevidence has been encouraging, but the long-term radiological outcome for this combined approach remains unknown(Boyd et al 2001).
18
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 18

19
ReferencesBoyd RN, Dobson F, ParrottJ et al.The effect of botulinum toxin type A and a variable hip abduction orthosis on gross motor function: a
randomized controlled trial. Eur J Neurol 2001;8(5):109-119
Givon U, Bendel E, Schindler A et al.Are night splints a useful adjuvant for botulinum toxin therapy? AACPDM C5;11
Heinan F, Molenaers G, Fairhurst C et al. European consensus table on botulinum toxin for children with cerebral palsy. Eur J Neurol 2006; 10: 215-225
Molenaers G, Desloovere K, Eyessen M et al. Botulinum toxin type A treatment of cerebral palsy: an integrated approach. Eur J Neurol;1999:6 (suppl 4)
Morris C. Orthotic management of children with cerebral palsy. J Pediatr Orthop 2002;14(4):150-158
Rosenbloom L,Ade-Hall R, Moore P et al. Does BTXA treatment for spasticity improve function in children with cerebral palsy? Results of a two
year randomised placebo controlled trial.AACPDM C6;12
CastingImmobilisation of a muscle in the lengthened position as in casting, increases the overall musculotendinous unit length,resulting in an increase range of movement (Mcnee et al 2007).
Individually, casting and BTX-A have both been shown to be effective in increasing range of movement. Combinedtreatment (BTX-A + casting) is most commonly used where there is dynamic spasticity with early myostaticcontracture. Comparative studies have shown a prolonged effect of improved ROM in comparison to both castingand BTX-A alone.
The time required to achieve an improved ROM has been shown to be reduced when using the combination of BTX-A and casting, versus casting alone.
There have been smaller conflicting studies which have suggested BTX-A combined with casting has resulted in anincreased speed of contracture recurrence in comparison to BTX-A alone [D]. However a recent systematic reviewof the literature has found that the evidence both for and against casting remains weak [B].
There is great variety in casting techniques and a paucity of detail reported in the literature specifically relating toBTX-A.
Timing of casting with BTX-AAlthough there is agreement in the literature regarding the indications for casting, there is no consensus regarding thetiming of casting post BTX-A injection.The procedure mainly relies on local practice and service resources.
The alternatives reported in the literature are • Immediately post-injection or• Delayed into the acute post-injection phase (this may in some centres coincide with the first post-injection review)
From the APCP National Survey it would appear that when casting is indicated, 73% of respondents would delaycasting post-injection.
The advantages for delaying casting• Ability to assess the true dynamic component of the spasticity/dystonia• Evidence from the animal models suggests that increased activity results in increased uptake of BTX-A and
therefore would argue against early immobilisation• There have been concerns expressed regarding prolonged immobilisation in the acute post-injection phase,
resulting in a lack of opportunity for rehabilitation and strengthening programmes • Comparative studies have suggested that delaying the cast application post-injection results in a more prolonged
effect of increased ROM, together with less discomfort reported during the casting process
The advantages of casting immediately post-injection• Ease of application, particularly if the child is sedated• In the case of repeat injections, when a child is known to have a degree of fixed contracture and has previously
responded well to a combination of BTX-A and casting
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 19
Recommendations• A combination of BTX-A with casting may be indicated in the presence of dynamic spasticity and mild
contracture [D]• Frequent cast changes should result in an improvement in ROM without excessive weakness post
BTX-A [D] • A combination of casting + BTX-A should result in a reduced time to achieve improvement in ROM in
comparison to casting alone [D]
ReferencesAckman JD, Russman BS,Thomas SS et al. Comparing botulinium toxin A with casting for treatment of dynamic equinius in children with cerebral
palsy. Dev Med Child Neurol 2005; 47: 620-627
Bottos M, Benedetti M G, Salucci P et al. Botulinum toxin with and without casting in ambulant children with spastic diplegia; a clinical and functional
assessment. Dev Med Child Neurol 2003;45:758 -763
Booth MY,Yates CC, Edgar TS et al. Serial casting combined intervention with botulinum toxin A and serial casting In the treatment of spastic equinus
in children. Paed Phys Ther 2003;15(4):216-220
Corry I S, Cosgrove A.P, Duffy CM et al. Botulinum toxin compared with stretching casts in the treatment of spastic equinus; a randomised
prospective trial. J Pediatr Orthop; 1998;18(3):304-331
Desloovre K, Molanaers G, Jonkers I et al.A randomised study of combined botulinum toxin type A and casting in the ambulant child with cerebral
palsy using objective outcome measures. Eur J Neurol 2001;8(suppl 5):75-87
Eleopra R,Tugnoli V, De Grandis D.The variability in the clinical effect induced by botulinum toxin type A: the role of muscle activity in humans. Mov
Disord 1997;12:89-94
Kay R, Rethlefen S, Fern-Buneo A et al. Botulinum Toxin as an adjunct to serial casting in children with cerebral palsy. J Bone Joint Surg Am
2004;86A(11)
Mcnee A,Will E, Lin J-P et al.The effect of serial casting on gait in 107 children with cerebral palsy:preliminary results from a crossover trial. Gait and
Posture 2007;25:463-468
Newman C, Kennedy A,Wlah M et al. Delayed versus immediate casting after botulinum toxin injection for partially reducible spastic equinus. Dev
Med Child Neur 2006;107:38-39
O’Neil ME, Fragala MA, Dumas HM. Physical therapy intervention for children with cerebral palsy who receive botulinum toxin A injections. Paediatr
Phys Ther 2003;15(4):204-215
Functional Electrical StimulationFunctional electrical stimulation (FES) has been used as an adjunct to physiotherapy to promote motor control andperformance. In combination with BTX-A, it has been proposed that FES optimises the effect of reduced activity inthe injected muscle. However, there is little evidence to date to support that adjuvant electrical therapy has asignificant effect on outcomes measured or any increased long-term benefit. In the APCP National Survey only 5% ofrespondents reported using FES post-injection.
ReferencesDetrembleur C, Lejeune TM, Renders A et al. Botulinum Toxin and short-term electrical stimulation in the treatment of equinus in cerebral palsy. Mov
Disord 2002;17(1):162-169
Gregoric M, Damjan H, Gros N et al. Effects of functional electrical stimulation and botulinum toxin therapy on gait in cerebral palsy. Gait & Posture
2003; 18:Abstract
Kerr C, McDowell B, Cosgrove A et al. Electrical stimulation in cerebral palsy: a randomized controlled trial. Dev Med Child Neurol 2006; 48:870-876
Positioning Twenty four-hour postural care is widely used as a management strategy in the care of children with neurologicalconditions.There are to date no specific studies looking at postural management and BTX-A. However, improvingpostural management is a frequently quoted goal in conjunction with BTX-A. In the APCP National Survey 59% ofrespondents would review postural management post-injection.
20
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 20
21
COMMUNICATION
Evidence from the APCP National Survey cites lack of communication as the largest area of frustration for therapists.Without effective communication between injecting centres and local teams, a successful outcome with BTX-A isunlikely, due to lack of timely co-ordination of therapy, orthoses and equipment.
RecommendationOngoing and effective communication between all team members is crucial to a successful outcome [D].
The physiotherapist, as a key member of the team will therefore need to:
• Liaise and communicate with the other team members throughout the assessment and review process• Discuss and agree on the goals of BTX-A injection • Agree on the most appropriate post-injection management programme to achieve those goals • Advise and support the child, family and all those involved in the child’s care to deliver the management
programme [D]
AUDIT
It is best practice to record all stages of the BTX-A management programme.
Audit of the use of BTX-A should include:
• Criteria for its use • Treatment goals • Baseline assessment measures• Outcome measures• Adverse events• Interpretation of results; follow-up treatment plan• User satisfaction questionnaire• Plans for future management
It is only through audit, and its relationship to best practice in the field of BTX-A, that future management canimprove for children with neurological conditions.
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 21
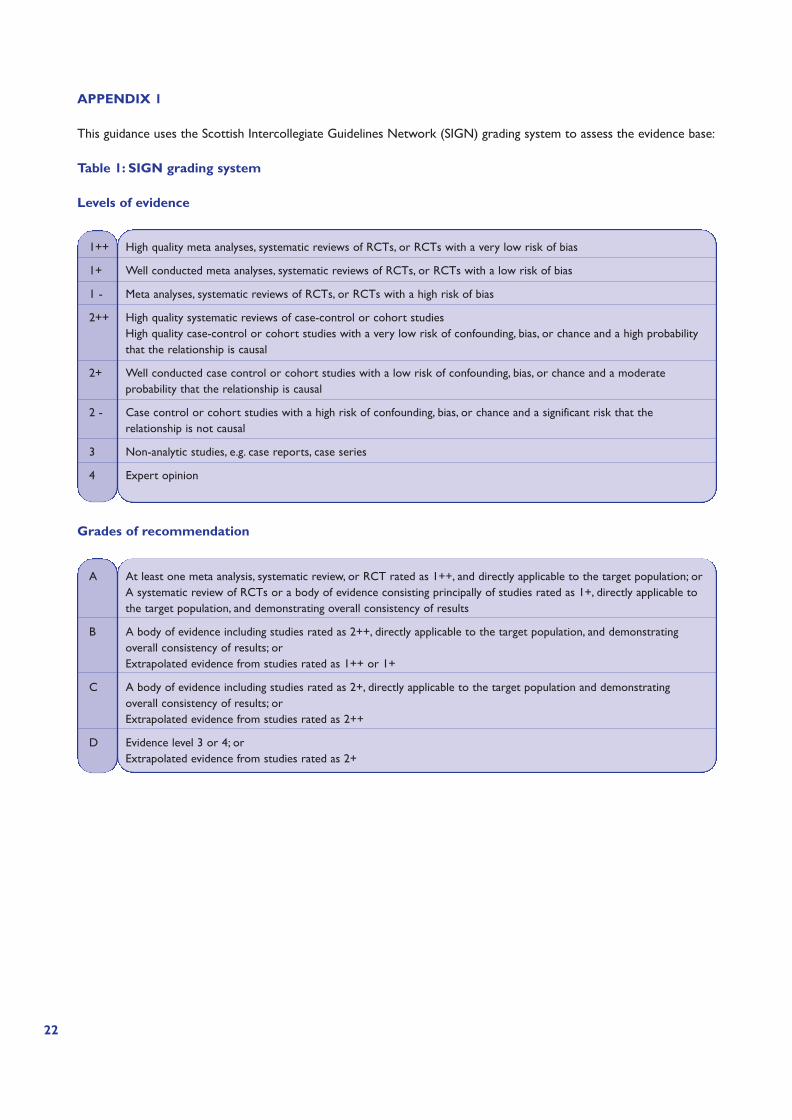
APPENDIX 1
This guidance uses the Scottish Intercollegiate Guidelines Network (SIGN) grading system to assess the evidence base:
Table 1: SIGN grading system
Levels of evidence
Grades of recommendation
22
1++ High quality meta analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias
1+ Well conducted meta analyses, systematic reviews of RCTs, or RCTs with a low risk of bias
1 - Meta analyses, systematic reviews of RCTs, or RCTs with a high risk of bias
2++ High quality systematic reviews of case-control or cohort studiesHigh quality case-control or cohort studies with a very low risk of confounding, bias, or chance and a high probabilitythat the relationship is causal
2+ Well conducted case control or cohort studies with a low risk of confounding, bias, or chance and a moderateprobability that the relationship is causal
2 - Case control or cohort studies with a high risk of confounding, bias, or chance and a significant risk that therelationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
A At least one meta analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; orA systematic review of RCTs or a body of evidence consisting principally of studies rated as 1+, directly applicable tothe target population, and demonstrating overall consistency of results
B A body of evidence including studies rated as 2++, directly applicable to the target population, and demonstratingoverall consistency of results; orExtrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the target population and demonstratingoverall consistency of results; orExtrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; orExtrapolated evidence from studies rated as 2+
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 22

23
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 23

CHA
RTER
ED
OF PH
YSIO
THER
AP
Y
SOC
IETY
DIG
NA SEQ
UI
CHA
RTER
ED
OF
PHYSIO
THER
AP
Y
SOC
IETY
DIG
NA SEQ
UI
ASSOCIATION OF PAEDIATRIC CHARTERED PHYSIOTHERAPISTS
April 2008
A16411 Physio Guidelines.qxd 4/4/08 09:44 Page 24