evento cerebro vascular dr. jorge o. contreras mónchez 05 de septiembre 2008 u.e.e.s
TRANSCRIPT

Evento cerebro vascular
Dr. Jorge O. Contreras Mónchez05 de Septiembre 2008
U.E.E.S.

Importancia
• Estadística
• Económica
• Humana
• Legal

Costos
• 31% muere en 6 meses despues de ACV
• De los sobrevivientes– 31% requiere asistencia
completa– 20% necesita ayuda para
caminar– 16% Pasa a asilos– 71% está imposibilitado
para trabajar
Sources: National Stroke Association, American Stroke Association

Discapacidad a las 2 semanas del ACV
• Hemiplejía 70-85%
• Dificultad para caminar 70-80%
• Dificultad para hablar 20-35%
• Pérdida visual 20%
• Depresión 40%
• Dependencia 50-85%
Modified from Dobkin, Neurologic Rehabilitation, 1996
Costos
Anualmente
$40,000,000,000.oo Dólares americanos
Sources: National Stroke Association, American Stroke Association
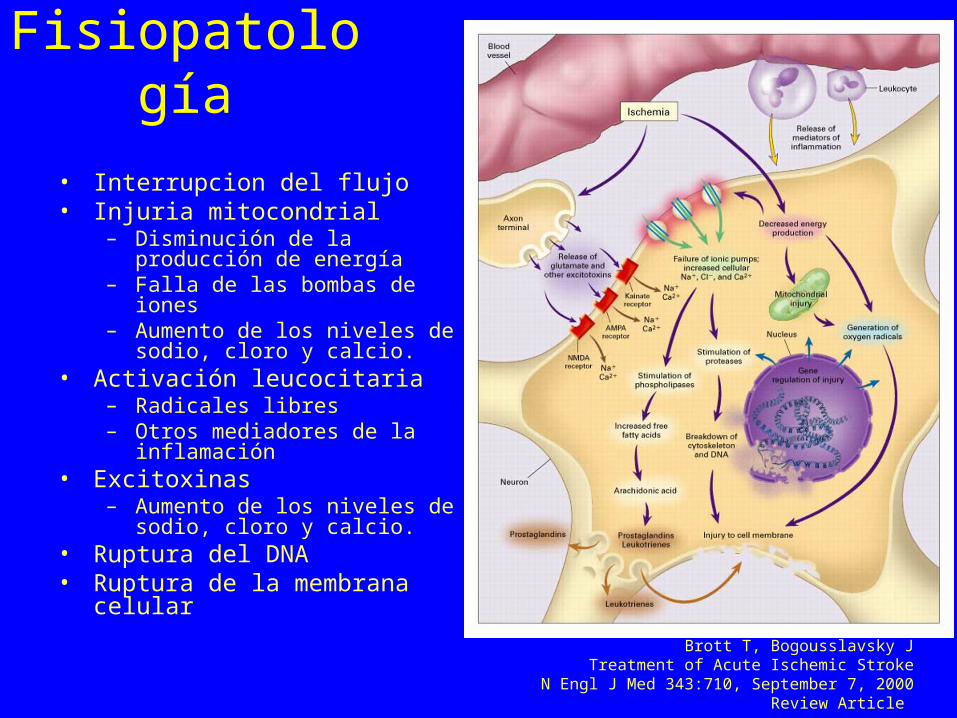
Fisiopatología
• Interrupcion del flujo• Injuria mitocondrial
– Disminución de la producción de energía
– Falla de las bombas de iones – Aumento de los niveles de sodio,
cloro y calcio.• Activación leucocitaria
– Radicales libres– Otros mediadores de la
inflamación• Excitoxinas
– Aumento de los niveles de sodio, cloro y calcio.
• Ruptura del DNA• Ruptura de la membrana celular
Brott T, Bogousslavsky JTreatment of Acute Ischemic Stroke
N Engl J Med 343:710, September 7, 2000 Review Article

• Abreviaturas: PARP, polimerasa de poli-A ribosa (poly-A ribose polymerase); iNOS,
sintasa inducible de óxido nítrico (inducible nitric oxide synthase).

Prevención
• Factores de riesgo NO modificables– Edad– Historia familiar– Edad

Prevención
• Estrategia básica
• Primaria
• Secundaria
• Terciaria

Prevención
• Factores de riesgo modificables– HTA– Tabaco– Obstruccion
carotidea– Dislipidemia– Obesidad– ACFA– Sedentarismo

Prevención
• Adjusted relative odds (95% CI) for ischemic cerebrovascular disease by categories of fasting glucose levels. Relative odds of 90 to 99 mg/dL, which constitutes the largest category, is defined as 1.
Sarah E. Vermeer et al. (behalf of the Dutch TIA Trial Study Group)
Impaired Glucose Tolerance Increases Stroke Risk in Nondiabetic Patients With Transient Ischemic Attack or Minor Ischemic Stroke
Stroke, Jun 2006; 37: 1413 - 1417.
Prevención
• Patients with documented coronary heart disease who were screened for inclusion in a secondary prevention clinical trial
• N=13 999• 6- to 8-year follow-up period • 1037 cases were identified with ischemic
cerebrovascular disease.• 576 cases were verified to have had ischemic stroke or
transient ischemic attacks.
Sarah E. Vermeer et al. (behalf of the Dutch TIA Trial Study Group)
Impaired Glucose Tolerance Increases Stroke Risk in Nondiabetic Patients With Transient Ischemic Attack or Minor Ischemic Stroke
Stroke, Jun 2006; 37: 1413 - 1417.

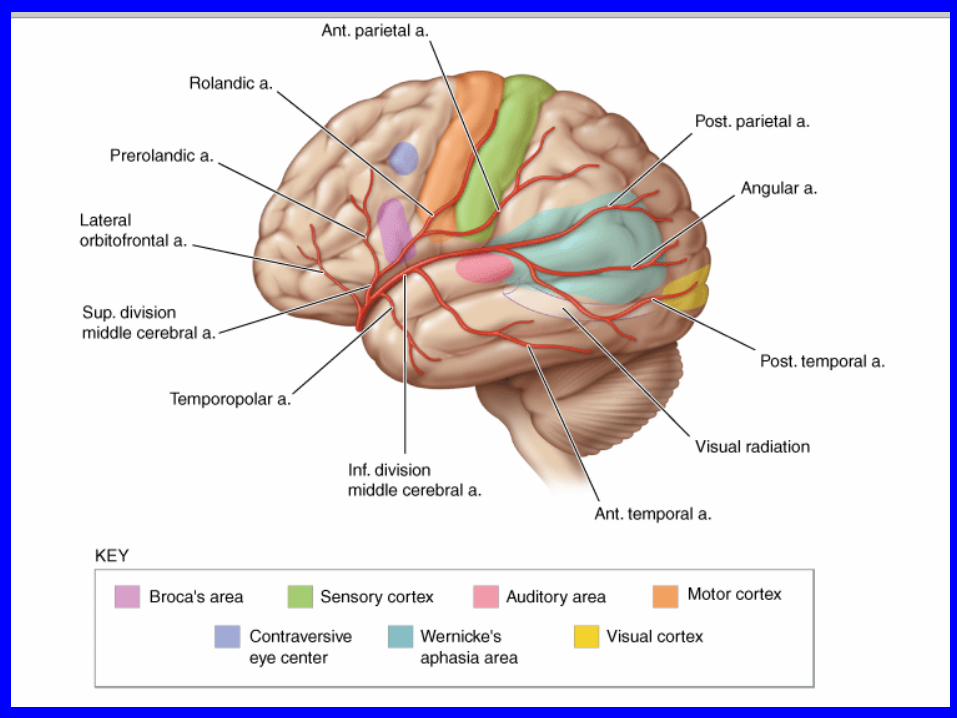
Cuadro clínico
• Hemiplejía súbita• Hemiparesia súbita• Hemiperestesia súbita• Disartria ó disfasia• Dificultad súbita para la bipedestaciuón ó
deambulación• Vision borrosa ó diplopia súbita• Cefalea severa• Confusión ó Amnesia



ACV isquémico
• CT Scans Obtained 1 Hour 40 Minutes after the Onset of Symptoms Suggestive of Cortical Stroke in the Territory of the Right Middle Cerebral Artery.
• An unenhanced CT scan (Panel A) shows a slight loss of differentiation of gray and white matter in the basal ganglia (arrows). A CT angiographic image shows occlusion of the first segment of the right middle cerebral artery (Panel B, arrow) and atherosclerotic lesions in the carotid bifurcation (Panel C, arrow). The external carotid artery is not shown.
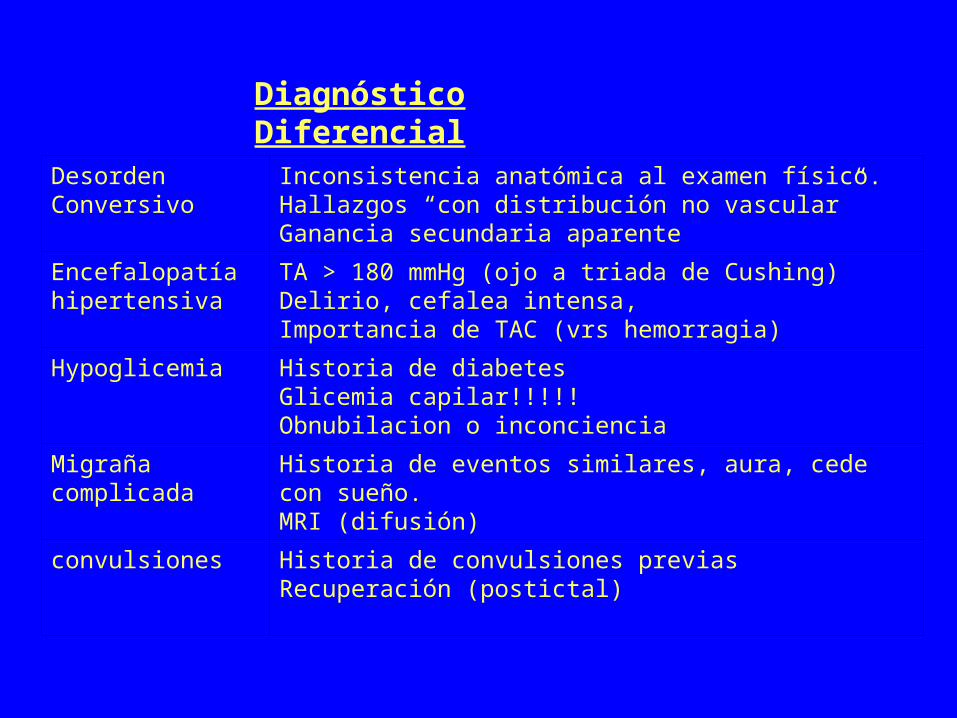
Diagnóstico Diferencial
Desorden Conversivo
Inconsistencia anatómica al examen físico. Hallazgos “con distribución no vascular”Ganancia secundaria aparente
Encefalopatía hipertensiva
TA > 180 mmHg (ojo a triada de Cushing) Delirio, cefalea intensa, Importancia de TAC (vrs hemorragia)
Hypoglicemia Historia de diabetesGlicemia capilar!!!!!Obnubilacion o inconciencia
Migraña complicada
Historia de eventos similares, aura, cede con sueño.MRI (difusión)
convulsiones Historia de convulsiones previasRecuperación (postictal)
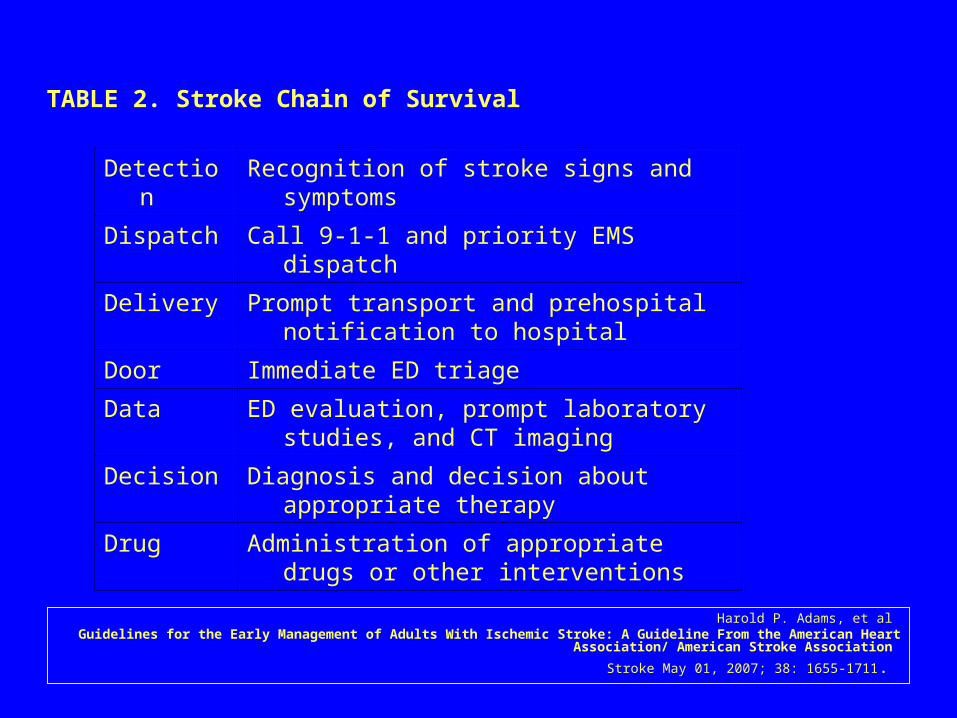
TABLE 2. Stroke Chain of Survival
Detection Recognition of stroke signs and symptoms
Dispatch Call 9-1-1 and priority EMS dispatch
Delivery Prompt transport and prehospital notification to hospital
Door Immediate ED triage
Data ED evaluation, prompt laboratory studies, and CT imaging
Decision Diagnosis and decision about appropriate therapy
Drug Administration of appropriate drugs or other interventions
Harold P. Adams, et al Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American
Stroke Association
Stroke May 01, 2007; 38: 1655-1711.
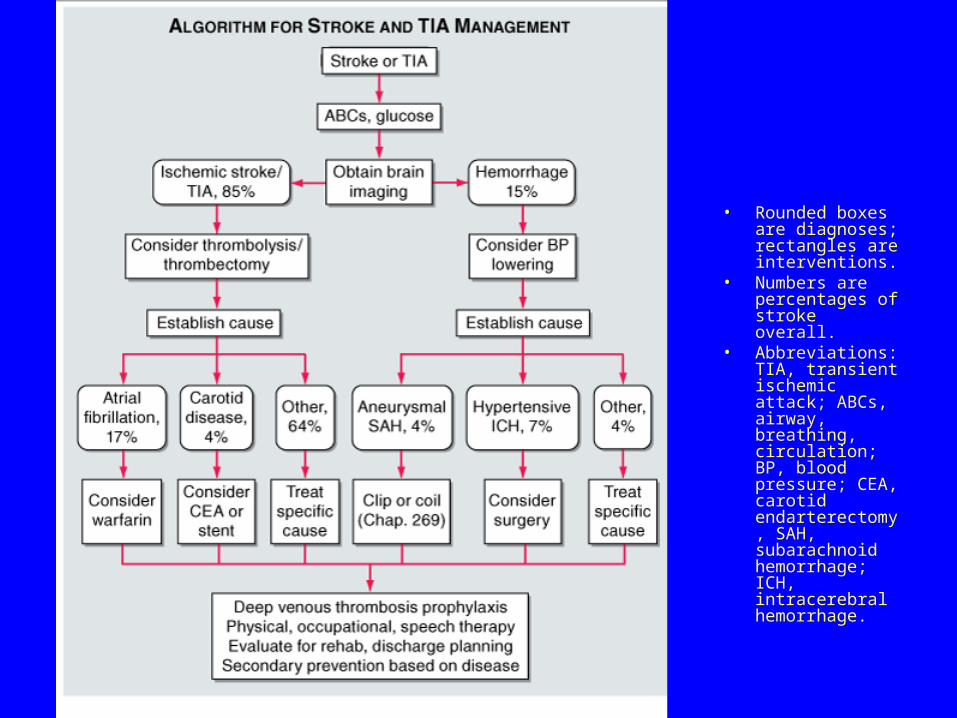
• Rounded boxes are diagnoses; rectangles are interventions.
• Numbers are percentages of stroke overall.
• Abbreviations: TIA, transient ischemic attack; ABCs, airway, breathing, circulation; BP, blood pressure; CEA, carotid endarterectomy, SAH, subarachnoid hemorrhage; ICH, intracerebral hemorrhage.

TABLE 3. Guidelines for EMS Management of Patients With Suspected Stroke
Recommended Not Recommended
Manage ABCs Dextrose-containing fluids in nonhypoglycemic patients
Cardiac monitoring Hypotension/excessive blood pressure reduction
Intravenous access Excessive intravenous fluids
Oxygen (as required O2 saturation <92%)
Assess for hypoglycemia
Nil per os (NPO)
Rapid transport to closest appropriate facility capable of treating acute stroke
Harold P. Adams, et al Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American
Stroke Association
Stroke May 01, 2007; 38: 1655-1711.

TABLE 9. Immediate Diagnostic Studies: Evaluation of a Patient With Suspected Acute Ischemic Stroke
All patients
Noncontrast brain CT or brain MRI
Blood glucose
Serum electrolytes/renal function tests
ECG
Markers of cardiac ischemia
Complete blood count, including platelet count*
Prothrombin time/international normalized ratio (INR)*
Activated partial thromboplastin time*
Oxygen saturation
Harold P. Adams, et al Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American
Stroke Association
Stroke May 01, 2007; 38: 1655-1711.

TABLE 9. Immediate Diagnostic Studies: Evaluation of a Patient With Suspected Acute Ischemic Stroke
Selected patients
Hepatic function tests
Toxicology screen
Blood alcohol level
Pregnancy test
Arterial blood gas tests (if hypoxia is suspected)
Chest radiography (if lung disease is suspected)
Lumbar puncture (if subarachnoid hemorrhage is suspected and CT scan is negative for blood)
Electroencephalogram (if seizures are suspected)
Harold P. Adams, et al Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American
Stroke Association
Stroke May 01, 2007; 38: 1655-1711.

¿Qué medidas son efectivas durante el episodio agudo?
• Trombolíticos • Antiagregantes plaquetarios y antitrombóticos
– Aspirina– Plavix– heparinas– Otros
• Uso de diuréticos• Uso de esteroides• Fisioterapia
– ¿Cómo? – ¿Cuándo?
• Neuroprotectores

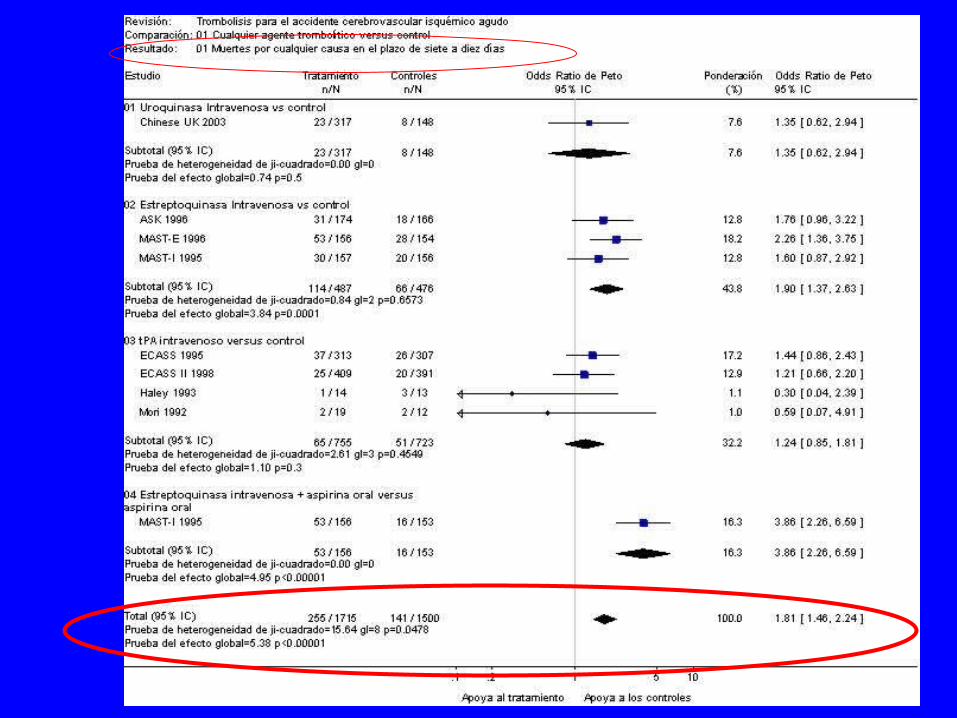
Trombolisis
t-PA vrs placebo(mortalidad)
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group.
Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-1587.
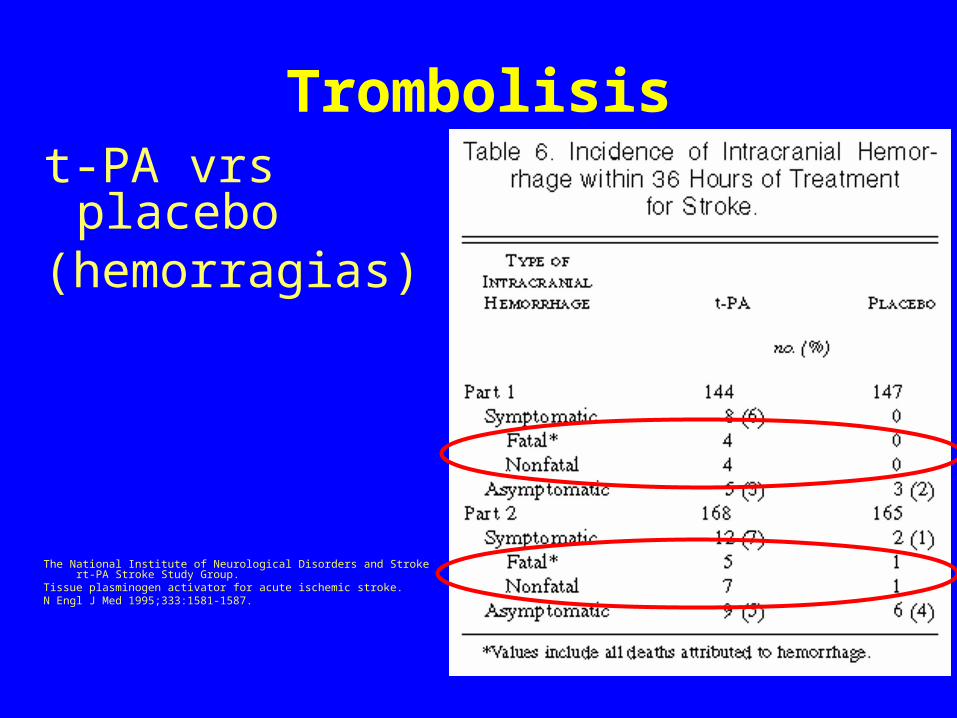
Trombolisist-PA vrs placebo(hemorragias)
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group.
Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-1587.
Trombolisis
• El tiempo es cerebro!
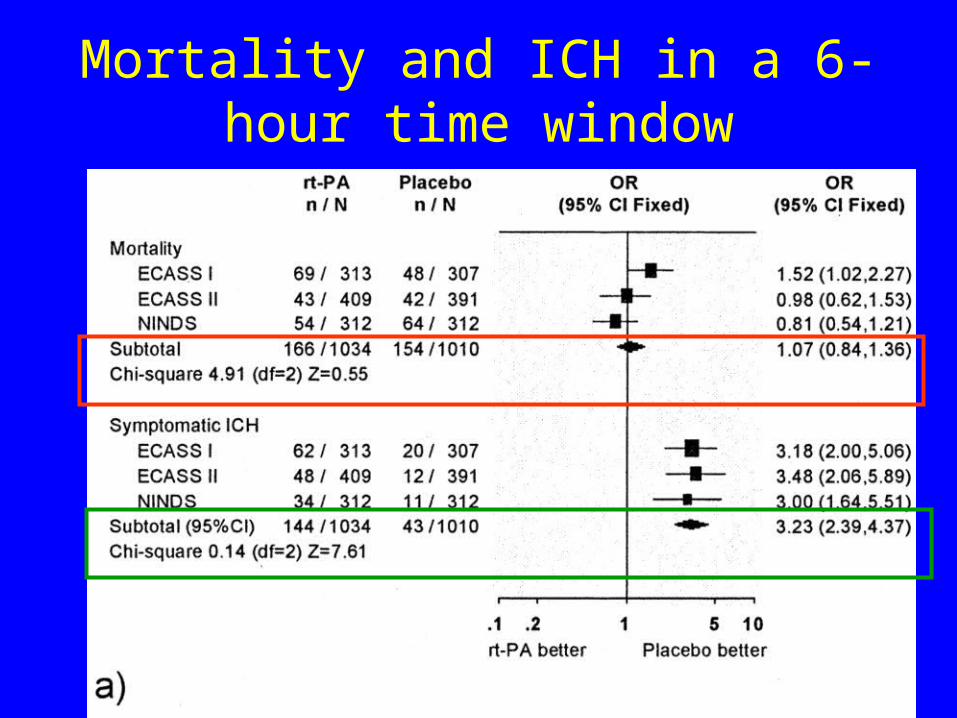
Mortality and ICH in a 6-hour time window

mortality and ICH in a 3-hour time window

independent vs dependent outcome or death in a 6-hour time window

independent vs dependent outcome or death in a 3-hour time window

Trombolisis en ACV
isquémico agudo


Preguntas interesantes• ¿Qué medidas son efectivas durante el episodio
agudo?– Trombolíticos – Antiagregantes plaquetarios y antitrombóticos
• Aspirina• Plavix• heparinas• Otros
– Uso de diuréticos– Uso de esteroides– Fisioterapia
• ¿Cómo? • ¿Cuándo?
– Neuroprotectores

Antiagregantes plaquetarios y antitrombóticos
• Aspirina– 160 mg a 300 mg de aspirina diarios– administrada por vía oral (o rectal en
pacientes con dificultad para deglutir) – iniciada dentro de las 48 horas posteriores al
supuesto accidente cerebrovascular isquémico

Antiagregantes plaquetarios y antitrombóticos
• Aspirina
– reduce el riesgo de un accidente cerebrovascular isquémico temprano recurrente sin un mayor riesgo de complicaciones por hemorragia temprana y mejora los resultados a largo plazo.




Anantes…!!!
Guías cínicas para uso de ASA
• SE recomienda el uso temprano (160-325 mg/day) Grado 1A
• Retarde el inicio al menos por 24 horas despues de usar tPA
• Aspirina es segura en combiacion con bajas dosis de heparina subcutánea.
Acute Ischemic Stroke
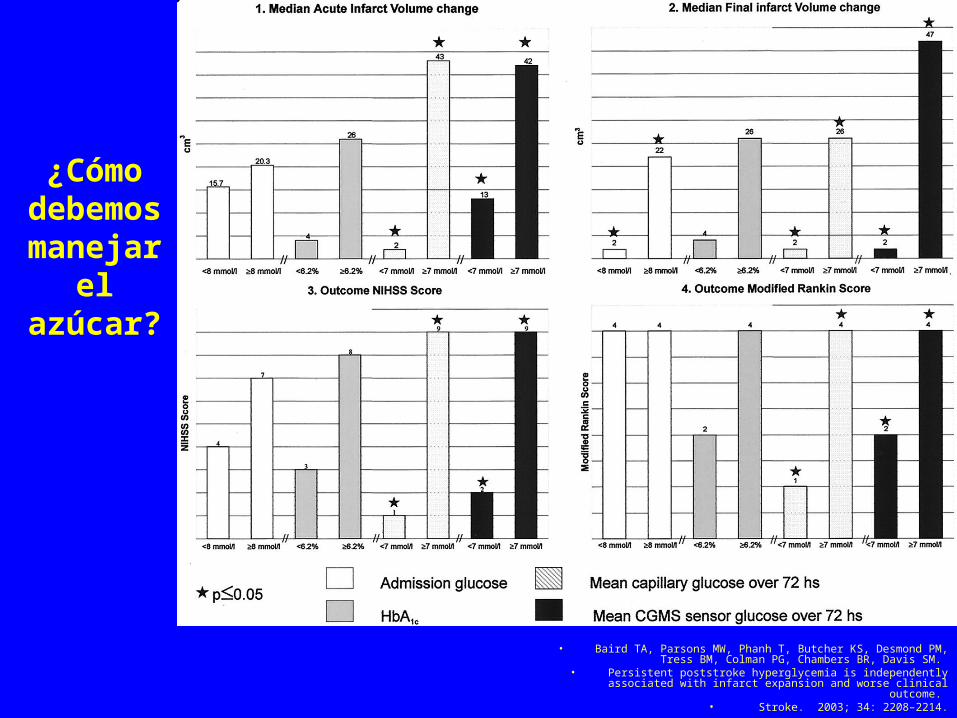
¿Cómo debemos
manejar el azúcar?
• Baird TA, Parsons MW, Phanh T, Butcher KS, Desmond PM, Tress BM, Colman PG, Chambers BR, Davis SM.
• Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome.
• Stroke. 2003; 34: 2208–2214.

Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001; 32: 2426–2432
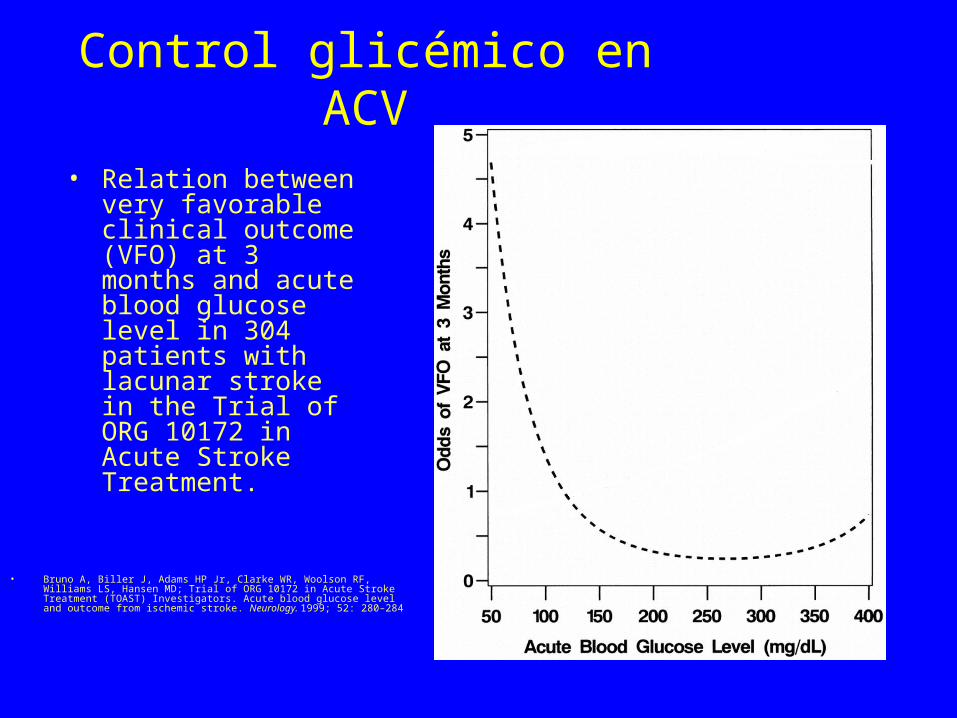
Control glicémico en ACV
• Bruno A, Biller J, Adams HP Jr, Clarke WR, Woolson RF, Williams LS, Hansen MD; Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators. Acute blood glucose level and outcome from ischemic stroke. Neurology. 1999; 52: 280–284
• Relation between very favorable clinical outcome (VFO) at 3 months and acute blood glucose level in 304 patients with lacunar stroke in the Trial of ORG 10172 in Acute Stroke Treatment.

Baird TA, Parsons MW, Phanh T, Butcher KS, Desmond PM, Tress BM, Colman PG, Chambers BR, Davis SM.
Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome.
Stroke. 2003; 34: 2208–2214

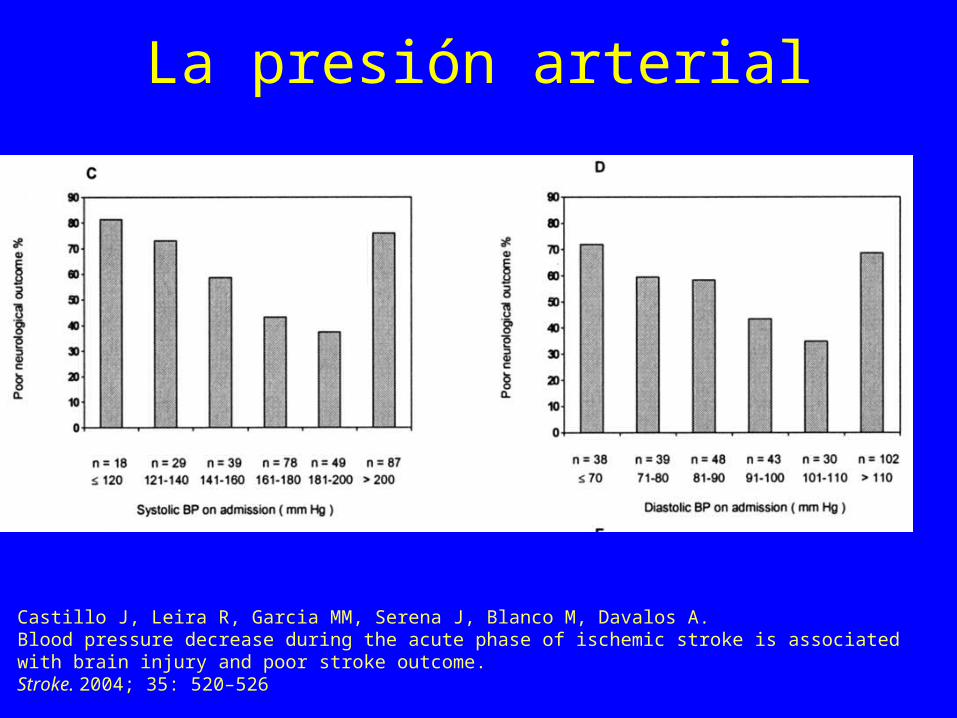
La presión arterial
Castillo J, Leira R, Garcia MM, Serena J, Blanco M, Davalos A. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke. 2004; 35: 520–526
La presión arterial
Castillo J, Leira R, Garcia MM, Serena J, Blanco M, Davalos A. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke. 2004; 35: 520–526
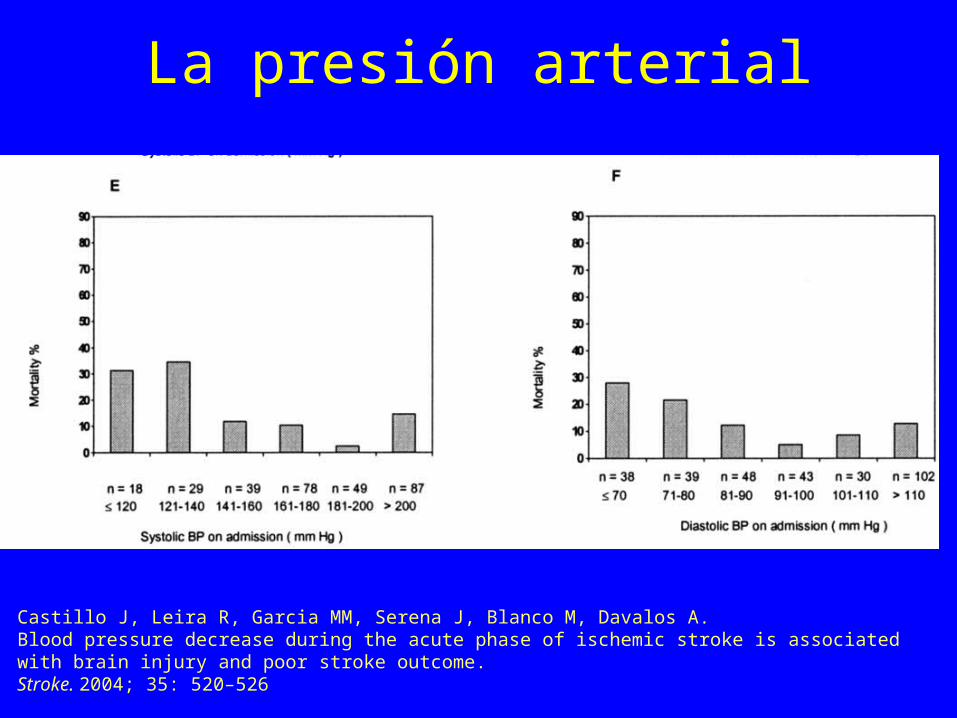
La presión arterial
Castillo J, Leira R, Garcia MM, Serena J, Blanco M, Davalos A. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke. 2004; 35: 520–526

La presión arterial
Castillo J, Leira R, Garcia MM, Serena J, Blanco M, Davalos A. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke. 2004; 35: 520–526
• The management of arterial hypertension remains controversial. Data to guide recommendations for treatment are inconclusive or conflicting.
Guidelines for the Early Management of Adults With Ischemic Stroke, 2007
• It is generally agreed that patients with markedly elevated blood pressure may have their blood pressure lowered. A reasonable goal would be to lower blood pressure by 15% during the first 24 hours after onset of stroke.
Guidelines for the Early Management of Adults With Ischemic Stroke, 2007

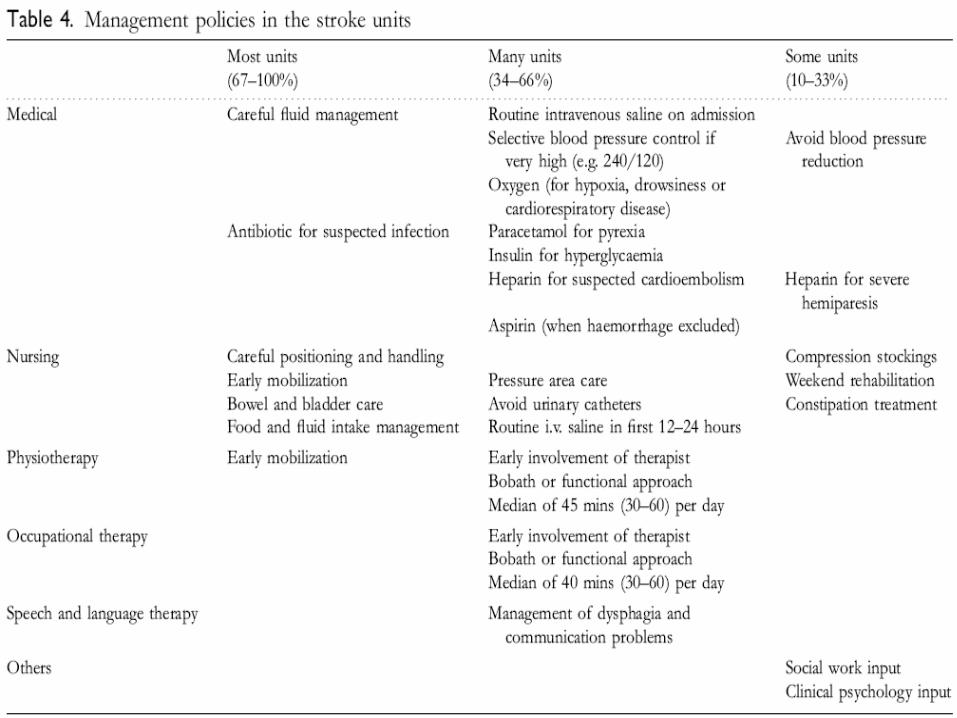
Langhorne P, Pollock A in conjunction with the Stroke Unit Trialists' Collaboration. What are the components of effective stroke unit care? Age Ageing 2002;31:365?371

Fisioterapia
Indredavik B, Bakke RPT, Slordahl SA, et al. Treatment in a combined acute and rehabilitation stroke unit. Which aspects are most important?
Stroke 1999;30:917?923

Manno EM, Adams RE, Derdeyn CP, Powers WJ, Diringer MN. The effects of mannitol on cerebral edema after large hemispheric cerebral infarct. Neurology. 1999; 52: 583–587.

Because of lack of evidence of efficacy and the potentialto increase the risk of infectious complications, corticosteroids(in conventional or large doses) are not recommendedfor treatment of cerebral edema and increasedintracranial pressure complicating ischemic stroke(Class III, Level of Evidence A).
Guidelines for the Early Management of Adults With Ischemic Stroke, 2007

Standardized Measures for Stroke: JCAHO Primary Stroke Centers
• tPA considered• Screen for dysphagia• Deep vein thrombosis prophylaxis• Lipid profile during hospitalization• Smoking cessation• Education about stroke• Plan for rehabilitation considered• Antithrombotic medications started within 48 hours• Antithrombotic medications prescribed at discharge• Anticoagulants prescribed to patients with atrial
fibrillation
• “El mejor médico es el que conoce la inutilidad de la mayor parte de las medicinas.”
Benjamin Franklin

• “Que la comida sea tu alimento y el alimento tu medicina.”
Hipócrates