event analysis lessons learnt from medication reconciliation activities using event analysis to...
TRANSCRIPT
Event Analysis
Lessons learnt from Medication Reconciliation activities using Event Analysis to improve medication safety
Evonne Fong, Dale Mitchell, Stephen Lim
Pharmacy Department
Background
Medication Reconciliation (MR) since 2007 at AHS
?? How and what to measure??
SQuIRe • Compliance with MR processes on admission, transfer and discharge• Varying results
• Admission: approximately 50% of patients with MR done within 24 hours
• Discharge: approximately 70% of patients with discharge reconciliation done
KPIsWhat we found:
• 17.2 medication errors per 100 medications a patient takes
• 58.4 drug errors per 100 high risk patients
Where to next?? … High 5s
AHS joined WHO’s High 5’s Project in 2009• Global patient safety collaboration • Australia’s project: Assuring Medication
Accuracy at Transition Points of Care
Benefits….• New measures
• High 5s MR 1-4• **Event Analysis**

New High 5’s measures
1. Percent of patients with meds reconciled within 24 hours of admission
2. Mean number of outstanding undocumented intentional medication discrepancies per patient
3. Mean number of outstanding UNINTENTIONAL medication discrepancies per patient
4. Percent of patients with at least ONE outstanding unintentional discrepancy
Event Analysis (EA)
Unprecedented opportunity to obtain and analyse findings from around the world regarding safety and effectiveness of SOP • Contributing factors
• Any specific system changes needed
Unique? Similar? Why?
Event Analysis (EA)
Includes:• Description of event• Analysis of cause and effect• Identification of contributing factors• Recommended improvements in
processes/systems• Documentation of findings and
recommendations

Example – Ian’s Story
Day 1: Admitted to ED on 22/5/2013 (Wednesday)
Admission reason: mechanical fall for investigation and
rehabilitation + ?UTI
PMH: HTN, Parkinson’s Disease, neuropathic pain, depression
Pt unable to give accurate medication history
Pt transferred to acute medical unit
MO writes up medications on chart
Patient’s mobility assessed on the day of admission by physio
Example – Ian’s Story
Day 2: Patient transferred to General Medical ward
• Physio notes state decreased mobility and increased tremor
Day 3: reviewed by Consultant and Medical Officer.
• Noted decreasing mobility and worsening of tremor
• MO calls pharmacy and requests review of medications
• Notes state:
• “review of medications, discuss with GP about meds, ?Neurologist
involved in patient care; ?Increase dose and add medications”
Ian’s Story
Day 3:
After phone call from MO, a pharmacist reviews patient.
Patient poor historian; pharmacist phones wife and uses Webster pack to
obtain BPMH
When comparing BPMH to med chart, multiple discrepancies identified:
• Omitted levodopa/carbidopa CR 200/50mg nocte
• Omitted mirtazapine 30mg nocte
• Omitted pregabalin 25mg nocte
• Omitted quetiapine 50mg nocte
• Omitted amlodipine 10mg nocte
• Incorrect timing for patients other Parkinson’s medication
MO informed correct meds and times charted 56 hours post admission
Mobility and condition improved; patient discharged
Event Analysis
Incident reported by pharmacist doing BPMH
Decision made to complete EA
Concise EA completed by team:
• Chief Pharmacist
• Clinical Pharmacist
• Medical Officer
• Safety and Quality Unit Project Officer
Event Analysis
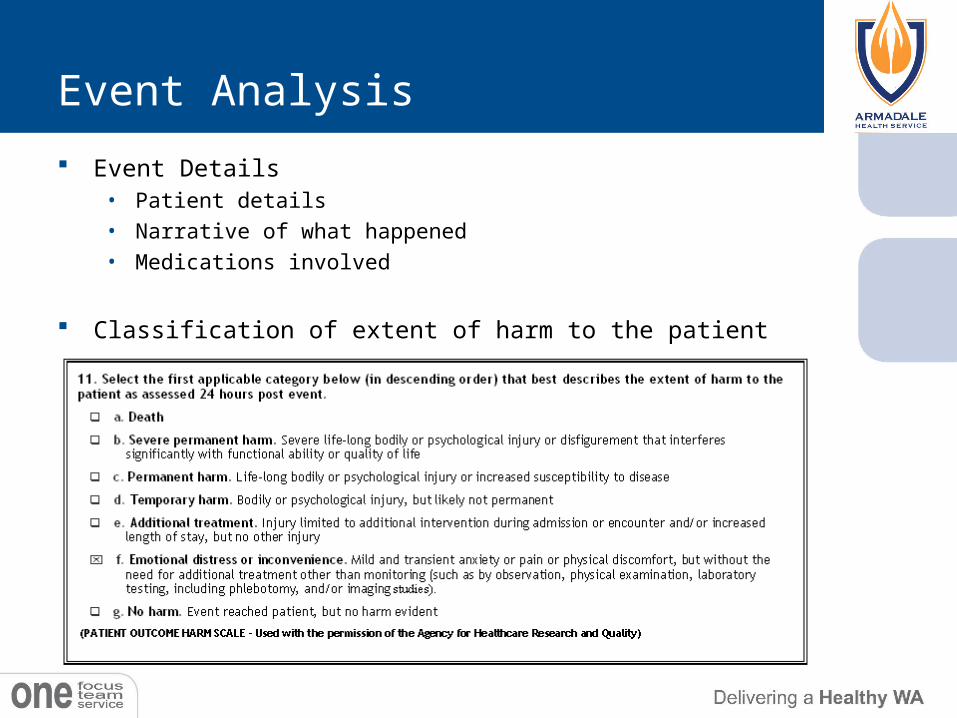
Event Details• Patient details• Narrative of what happened• Medications involved
Classification of extent of harm to the patient
Event Analysis
Contributing Factors Education and Training
• MO unable to collect BPMH accurately despite having Webster Pack. Did not know how
to decipher medication details from Webster Pack
• Missed the 10pm “slot”
Staffing
• Patient initially admitted to AMU for 24 hrs before transfer to medical ward. AMU does
not have allocated clinical pharmacist Med Rec not completed within 24 hrs.
• Gen Med pharmacist on leave; another pharmacist went to see pt when requested by Dr
Patient
• Patient poor historian
Primary Contributing Factors Education and Training
Event Analysis
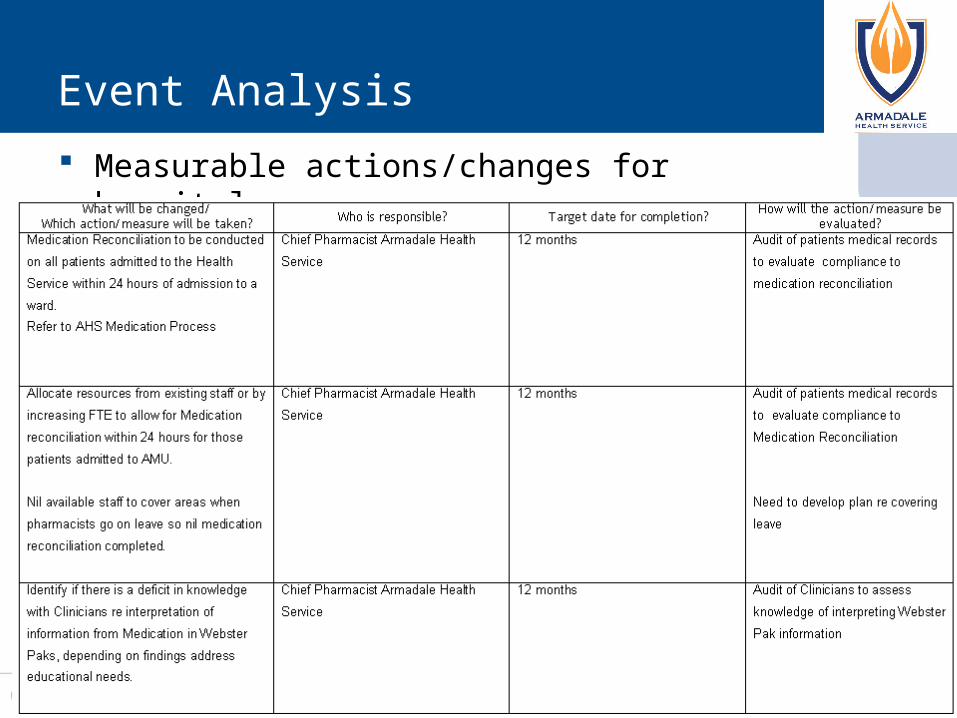
Measurable actions/changes for hospital
Conclusion
Event analysis beneficial as a “fact finding” tool • Used to seek and investigate patient safety
problems to identify if there are problems with the SOP and to identify cause and effect
• Multidisciplinary approach
• Less labour/resource intensive than RCA
• Measurable actions and changes to implement to improve patient safety