medication errors an ounce of prevention is worth a pound ... · medication error:any preventable...
TRANSCRIPT

9/16/2016
1
Medication Errors an ounce of prevention is worth a pound of cure
Kelly Biastre, PharmD. CPh., Sr. Consultant Med SafetyBaptist Health Jacksonville, FlAnd Mandy Clark, PharmD., BCACPWalgreen’s Health Systems Registered Store Manager
Technician Education DaySeptember 24, 2016 – Jacksonville, FL
2
Disclosure
Kelly Biastre has no financial disclosures, vested interests or affiliations with any corporate organizations offering financial support or grant monies for this continuing education activity.
Mandy Clark has no financial disclosures, vested interests or affiliations with any corporate organizations offering financial support or grant monies for this continuing education activity.
3
Objectives
Define the classifications of adverse drug events and med errors (Kelly)
Review patient cases and describe 2 different pathways to medication errors in the hospital setting and in the community setting. (Mandy and Kelly)
Discuss at least 2 error reduction strategies and prevention methods (Mandy and Kelly)
List at least 2 components of a culture of safety (Kelly)
Define a Root Cause Analysis (RCA) and list the steps and people involved (Mandy)
4
Baptist Health
Baptist Health Jacksonville Campus is a 500+ bed tertiary hospital affiliated with Wolfson Children’s Hospital (199 beds); level 3 NICU~ 21,000 admissions per year~ Dispense ~250,000 doses per month
5
Impact of Medical Errors
Medical Errors are the third top leading cause of death in the US
Estimated annual deaths = 251,000
National Patient Safety Foundation 1/3 of Americans have been affected by a medication
mistake 28% of these are due to a med error
6
Key Definitions/Classifications
Medication Error: Any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient or consumer_source NCCMERP
An Adverse Event (AE): an unintended injury resulting from medical intervention related to a drug - Usually preventable source_Institute of Medicine
Adverse Drug Reaction (ADR): Any response to drug that is unintended, which occurs in doses normally used in man –usually not preventable) _source World Health Organization

9/16/2016
2
7
Definitions
• “Preventable ADE”: harm caused by the use of a drug as a result of an error• Patient given a normal dose of drug but the drug was
contraindicated in this patient• These events warrant examination by the provider to determine
why it happened
• “Non-Preventable ADE”: drug-induced harm occurring with appropriate use of medication• Anaphylaxis from penicillin in a patient with no previous history
of an allergic reaction• While these are currently non-preventable, future studies may
reveal ways in which they can be prevented
8
Objectives
Define the classifications of adverse drug events and med errors (Kelly)
Review patient cases and describe 2 different pathways to medication errors in the hospital setting and in the community setting. (Mandy and Kelly)
Discuss at least 2 error reduction strategies and prevention methods (Mandy and Kelly)
List at least 2 components of a culture of safety (Kelly)
Define a Root Cause Analysis (RCA) and list the steps and people involved (Mandy)
9
Walgreen’s and CVS
Top 2 drug store chains in the United States
Patient touch pointsRetail Pharmacies
Mail Order
Specialty Pharmacies
Over 2.8 BILLION prescriptions were filled in2015 between these two companies.
http://investors.cvshealth.com/financial-information/annual-report-archivehttp://files.shareholder.com/downloads/WAG/2754333417x0x866062/2D854509-EE85-422F-BD51-84FDB77041C1/Walgreens_Boots_Alliance_Inc._2015_Annual_Report.pdf
10
Error Rates in Community Practice
According to the IOM report Preventing Medication Errors there are 51.5 MILLION errors per 3 BILLION prescriptions per year. 6.5% of those errors are considered clinically significant.
Let’s break it down… There are 4 errors per every 250 prescriptions filled
PER pharmacy per day.
For every 2000 prescriptions filled per week by a pharmacy 2 of the prescriptions statistically have clinically significant errors.
11
Common Pathways to ErrorsIn Community Practice
Dispensing ErrorsEnvironmental Factors
12
Dispensing Errors
1. Choosing the wrong patient2. Choosing the wrong drug3. Dispensing with wrong directions4. Dispensing the wrong quantity5. Incorrectly labeling the bottle6. Dispensing expired medication

9/16/2016
3
13
How can we choose the wrong patient? Similar Names John Smith
John Smith Jr.
John Smith Sr.
Similar DOB 12/25/1950 is Kathy
Jones
12/25/1950 is Karen Jones
How can we prevent choosing the wrong patient? Verify the DOB
Verify address
Verify phone number
Look at patient history
Dispensing Errors: Patient14
What are some ways that we could choose the wrong drug? Handwriting
Similar Names LASA or SALA
Drug Location
How can we prevent these errors? Verify the Rx if you
cannot read it.
Verify eRx if there is conflicting information
Change drug locations
Verify NDC numbers
Dispensing Errors
15
Common Mix Ups (look alike sound alike)
16
Look alike sound alike medications in the hospital
17
Tall Man Letters – applies to both community and hospital
https://pharmacyexam-krishnapublicati.netdna-ssl.com/images/TallManLetters.png
18
Example of Tall Man Letters

9/16/2016
4
19
Dispensing Errors
How do prescriptions end up with incorrect directions? Bad handwriting
Double directions on eRx
Improper use of abbreviations
Drugs that are dosed in mg but come in mL’s.
Drug packaging U-100 vs U-500 insulin
When in doubt, ASK.
20
Example: mg vs mL
It is billed to the insurance in mL but is prescribed to administer in mg. https://www.globalpharmacyplus.com/media/product/05/victoza-18mg-3ml-1-carton-3-pens.jpg
21
Example: abbreviations
qd is mistaken as qid Write out daily
qod is mistaken for qid Write out every other day
µg can be mistaken for mg Write out microgram or mcg
U can be mistaken for a 0 or 4 Write out units
https://www.ismp.org/tools/errorproneabbreviations.pdf
22
What is the top drug? A. Minocin
B. Neurontin
C. Indocin
Answer? A. Minocin
How about this one?
https://s3.amazonaws.com/pharmacytimes/v1_media/_image/June15CYR2.PNG
23
Workflow What is the process in place
for the intake of prescriptions?
What is the process for filling prescriptions?
Patient pick up areas What processes are in place
to prevent the wrong patient getting the wrong drug?
Inventory What are the drug locations?
Rotation of stock?
CNO (clean / neat / orderly)
Other factors Noise
Distractions
Temperature
Volume of Business
Environmental Factors24
Workflow Maintain workflow and have
set rotation schedule to prevent burnout of the staff.
Always put medications back after filling
Use totes to separate patients to prevent errors.
Work on one Rx at a time.
Patient pick up areas Verify that you have the
correct patient prescriptions at pick up.
Address
Phone number
Date of birth
If multiple bags look at each one.
Some places have computer enhancements in place to prevent picking up the wrong Rx. Do not override these programs.
What can you do to help with Environmental Factors?

9/16/2016
5
25
Inventory Separate LASA drugs
Have dividers between the medications
Rotate Stock
Return to stock the medication immediately after use.
Other factors Do not disturb
pharmacist while transcribing prescriptions
Maintain equipment
Schedule according to patient demand
Take breaks as required
What can you do to help with Environmental Factors?
26
Case Study - 3
• You are a Senior Technician at a local community pharmacy. You are in charge of training, Mandy, the new technician on how to receive new patient prescriptions into the pharmacy and filling prescriptions.
• Patient John Smith walks up and hands you his son’s prescription for a azithromycin.
• Mandy takes the prescription and says that we will get it ready.
27
Approaches to reducing dispensing errorsin both community and hospital
Ensure safe dispensing procedures
Separate drugs with similar drug names
Keep interruptions to a minimum
Awareness of high risk drugs like heparin, chemo and potassium chloride
Introduce safe systematic procedures for dispensing
28
Approaches to reducingdispensing errors
Read labels at least 3 times
Prepare meds in a well lighted area
Check expiration dates of the drugs
Be alert to unusually high dosages
When in doubt, ASK
Double check all calculations
Do not make assumptions
When you have made an error, reflect on what went wrong and why. Ask how you could have prevented the error.
29
Common pathways to med errors in the hospital setting
Med errors can occur anywhere in the med use system
Occur most frequently in the Ordering (56%) and Administration (34%) phase JAMA.1995; 274:29-34
30
What happened?
Errors can occur at any point in the med use process
Selection
Ordering
Dispensing
Administering
Monitoring

9/16/2016
6
31
Confirmation Bias
Experiments conducted during the 1960s demonstrated that people have a tendency to seek information that confirms their existing beliefs.
Unfortunately, this type of bias prevents us from looking at situations objectively
can influence the decisions we make
can lead to poor or faulty choices
32
Is this confirmation bias?
33
Is this confirmation bias?34
How errors happen with confirmation bias
Errors happen when products look alike
35
We can read this!
Aoccodring to a rscheearch sduty at Cmbarigde Uinervtisy, it deosn’t mttear in waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and the lsat ltteer be in the rghit palce. The rset can be a toatl mses and you can sitll raed it wouthit porbelms. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wohle.
36
What we see and read is different

9/16/2016
7
37
Heparin – High Alert and LASA38
What we know about making errors
All of us make errors
Errors are not made on purpose
No one wants to admit to making an error if they know the punishment is the result
Error does not equate to bad behavior
Errors happen for a reason Lucian Leape, MD
Safety in our System: High Alert Medications Lynn Eschenbacher, Pharm.D. Medication Safety Officer Duke University Hospital.
39
Reporting Errors
State of Florida requires Continuous Quality Improvement meetings to occur quarterly.
Error reporting is held confidential due to HIPPA but all organizations must have a documentation system.
National Reporting Agencies ISMP: MERP
FDA: MedWatch
40
Reporting Errors
Error reporting is meant to be a recollection of the exact events as they occurred that can be used as an educational tool in order to prevent future events
It is very important to not place blame on an individual
Build a culture of safety
Conduct Root Cause Analysis when necessary
41
Objectives
Define the classifications of adverse drug events and med errors (Kelly)
Review patient cases and describe 2 different pathways to medication errors in the hospital setting and in the community setting. (Mandy and Kelly)
Discuss at least 2 error reduction strategies and prevention methods (Mandy and Kelly)
List at least 2 components of a culture of safety (Kelly)
Define a Root Cause Analysis (RCA) and list the steps and people involved (Mandy)
42
How do you define culture?
• Merriam-Webster: The beliefs, customs, arts, etc of a particular society, group place or time. A way of thinking, behaving or working that exists in a place or organization
• Alternate definitions:
• Shared set of basic assumptions
• Values + Beliefs + Behaviors = Culture
“The way we do things around here”

9/16/2016
8
43
An evolution from Punitive to No Blame to Just Culture
• Punitive: blames individuals when things go wrong• work carefully, counseling, discipline, procedural violations
unacceptable
• Blame Free: response to shortcomings of a punitive culture• workers who made honest errors were not truly blameworthy
• Just Culture: A set of values, beliefs and norms• What is important, how to behave• What behavioral choices and decisions are appropriately related
to occurrences of human error and near misses. • Emphasis on learning and shared accountability• Workers continually look for risk and are thoughtful about
behavioral choices• Managers look for system design features that are reliable
44
An Introduction to Just Culture
The single greatest impediment to error prevention in the medical industry is “that we punish people for making mistakes.”
Dr. Lucian Leape
Professor, Harvard School of Public Health
Testimony before Congress on
Health Care Quality Improvement
45
A Just Culture 46
Promoting a culture of safety
47
A Just Culture – Behavioral Choices48
A Just Culture
Good system design + good behavioral choices of staff = good results
Accountability is not dependent on outcome but behavioral choices under worker’s control
Shared accountability Four areas of focus:
learning/reporting culture open/fair culture design of safe systems management of behavioral choices

9/16/2016
9
49
A Just Culture
Recognizes errors are often system failures
Requires full disclosure Mistakes, errors, near misses, safety concerns, sentinel
events
Is a culture of accountability Counseling; Consoling; Coaching; Education
Corrective action?
50
A Just Case - to consider
An experienced surgeon sees a new piece of equipment at a conference. He is told this equipment will reduce surgical time from 6 hours to 3 hours.
A representative comes to the hospital and offers a free trial of the new equipment and the doctor decides it would be nice to try it out. The physician receives training via video, but he has never used the equipment before.
His first case, he accidentally punctures the patient’s bowel. The surgeon then has to do a second surgery to repair the bowel and the patient fully recovers.
The OR has a strict policy that says NO new equipment will be allowed in the OR until it has been fully approved and all staff have been trained.
51
Severity Bias Impacts Case
Scenario 1: Surgeon use of unapproved equipment – NO Harm to patient
Scenario 2: Surgeon us of unapproved equipment – Patient Dies
0
20
40
60
80
Staff 16 25 40 19
Manager 11 56 33 0
Executive 5 21 63 11
Physician 0 50 50 0
Take no action
Warn not to make
mistake
Encourage Different
Discipline or Punish
0
10
20
30
40
50
60
Staff 13 25 33 29
Manager 8 17 25 50
Executive 24 33 29 14
Physician 0 9 45 45
Take no action
Warn not to make mistake
Encourage Different
Discipline or Punish
52
Surgeon watched video and received verbal training from manufacturer
Surgeon confident in the process
Surgeon used an unapproved surgical instrument
Patient suffered harm
OR Staff does not stop physician prior to surgery
Examining the behavior
why
70-80% of human errors
go unexplained
70-90% of at risk behaviors
go unexplained
53
To Err is Human54
To Drift is Human

9/16/2016
10
55
Reckless behavior is a choice56
Managing the human behavior
Two Questions: Did the employee make the correct behavioral choices
in their task?
Is the employee effectively managing their own performance shaping factors? If yes , the only answer is to console the employee of the
error happened to them
Examine the system for improvement opportunities
57
If an error occurs
Root Cause AnalysisTool used to determine the system cause of
an error
Required by many places of a sentinel event occurs
58
Objectives
Define the classifications of adverse drug events and med errors (Kelly)
Review patient cases and describe 2 different pathways to medication errors in the hospital setting and in the community setting. (Mandy and Kelly)
Discuss at least 2 error reduction strategies and prevention methods (Mandy and Kelly)
List at least 2 components of a culture of safety (Kelly)
Define a Root Cause Analysis (RCA) and list the steps and people involved (Mandy)
59
Root Cause Analysis
Let’s change the outcome of the case of Mandy with patient John Smith. Let’s say that the Neo/Poly/HC Otic was dispensed to John with directions to Instill 2 drops into the right eye 3 times per day.
After 1 day John was complaining of severe irritation, the eye was inflamed and he complained of vision changes. He was taken back to the doctor. Mom took the bottle of drops to the office and it was noticed that it was ear drops that were being dispensed instead of eye drops. The doctor called the pharmacist.
60
Root Cause Analysis
Do we just blame this on Mandy being new? Absolutely Not
Who reports the error and when should it be reported? The pharmacist that was informed of the error files the
initial report on the same day they were notified
Who is to blame for the error? Blaming a person is not the goal of a root cause
analysis; we want to find out WHY a system failed
9/16/2016
11
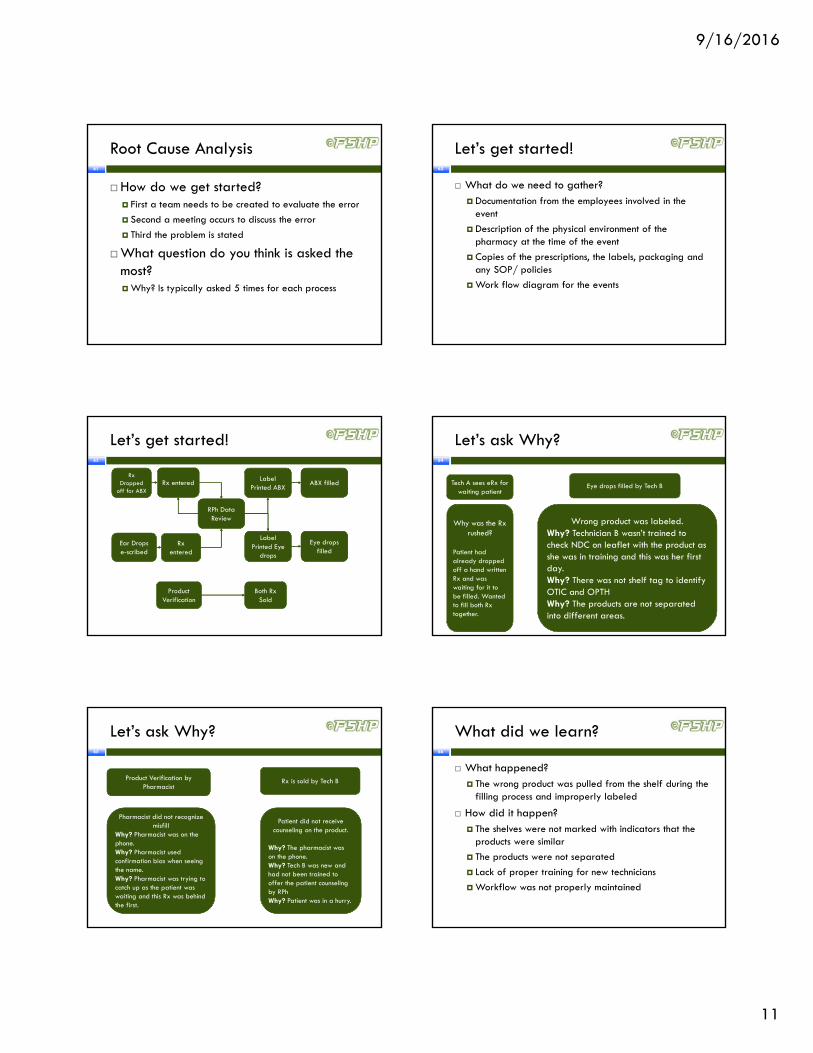
61
Root Cause Analysis
How do we get started? First a team needs to be created to evaluate the error
Second a meeting occurs to discuss the error
Third the problem is stated
What question do you think is asked the most? Why? Is typically asked 5 times for each process
62
Let’s get started!
What do we need to gather? Documentation from the employees involved in the
event
Description of the physical environment of the pharmacy at the time of the event
Copies of the prescriptions, the labels, packaging and any SOP/ policies
Work flow diagram for the events
63
Let’s get started!
Rx Dropped
off for ABXRx entered
RPh Data Review
Label Printed ABX
Label Printed Eye
drops
Ear Drops e-scribed
Rx entered
ABX filled
Eye drops filled
Product Verification
Both Rx Sold
64
Let’s ask Why?
Tech A sees eRx for waiting patient
Eye drops filled by Tech B
Why was the Rx rushed?
Patient had already dropped off a hand written Rx and was waiting for it to be filled. Wanted to fill both Rx together.
Wrong product was labeled. Why? Technician B wasn’t trained to check NDC on leaflet with the product as she was in training and this was her first day.Why? There was not shelf tag to identify OTIC and OPTHWhy? The products are not separated into different areas.
65
Let’s ask Why?
Product Verification by Pharmacist
Rx is sold by Tech B
Pharmacist did not recognize misfill
Why? Pharmacist was on the phone.Why? Pharmacist used confirmation bias when seeing the name.Why? Pharmacist was trying to catch up as the patient was waiting and this Rx was behind the first.
Patient did not receive counseling on the product.
Why? The pharmacist was on the phone.Why? Tech B was new and had not been trained to offer the patient counseling by RPhWhy? Patient was in a hurry.
66
What did we learn?
What happened? The wrong product was pulled from the shelf during the
filling process and improperly labeled
How did it happen? The shelves were not marked with indicators that the
products were similar
The products were not separated
Lack of proper training for new technicians
Workflow was not properly maintained

9/16/2016
12
67
What did we learn?
What can we do to prevent this from happening again? Follow a better training protocol for new hires
Review indicators to have better coverage for scheduling
Separate the ophthalmic and otic formulations of the product
Create shelf tags to mark the difference in the product.
Do not override SOP in the filling process
Counseling on new medications
68
To sum up Errors & RCA…
We should not be afraid to report errors
Errors are the greatest learning tool to prevent future events
Be honest in the reporting and look for the cause and effect instead of placing blame
Keep asking “why?” until you are at the very end.
Create and action plan and accountability for follow through on listed actionable items
Do NOT place blame; find the system issue
69
References
1) Preventing Medication Errors, Quality Chasm Series, IOM
2) National Coordinating Council for Medication Error Reporting and Prevention. Web. 15 Sept. 2011.<http://www.nccmerp.org/aboutMedErrors.html>.
3) Grissinger, Matthew. System Elements of Medication Use. Proc. of ISMP Medication Safety Intensive, Orlando, FL. 2010. Print.
4) Smetzer, Judy. Just Culture. Proc. of ISMP Medication Safety Intensive, Orlando, FL. 2010. Print.
5) Smetzer, Judy. Human Factors in Medication Safety. Proc. of ISMP Medication Safety Intensive, Orlando, FL. 2010. Print.
6) "ISMP's List of High Alert Medications.” www.ismp.org. 2008. Web. 16 Sept. 2011. <http://www.ismp.org/tools/highalertmedications.pdf>.
7) http://www.nccmerp.org/aboutMedErrors.html
8) https://www.ismp.org/faq.asp#Question_3
9) http://www.ashp.org/s_ashp/index.asp
10) https://www.ismp.org/Tools/institutionalhighAlert.asp
11) http://www.nccmerp.org/council/council1999-03-19.html
12) http://www.jointcommission.org
13) ISMP Medication Safety Alert, Volume 21, Issue 9 - May 5, 2016
14) ISMP Medication Safety Alert, Volume 13, Issue 23, November 20, 2008
15) IOM 1999 To Err is Human Report
16) JAMA.1995;274:29-34
17) ISMP Medication Safety Alert, What’s in a name? Ways to Prevent Dispensing Errors Linked to Name Confusion, June 12, 2002
18) http://www.uspharmacist.com/content/d/pharmacy%20law/c/16572/
Technician Education Day September 24, 2016 – Jacksonville, FL