evaluation of the cyanotic infant bill lefkowitz 16 nov 2000
TRANSCRIPT

Evaluation of the Cyanotic Evaluation of the Cyanotic InfantInfant
Bill LefkowitzBill Lefkowitz
16 NOV 200016 NOV 2000

OutlineOutline Cyanosis - define and describeCyanosis - define and describe Terms (PaOTerms (PaO22 v SaO v SaO22 v CaO v CaO22)) Differential of cyanosisDifferential of cyanosis The hyperoxia testThe hyperoxia test A few etiologiesA few etiologies Take home pointsTake home points Evaluation and intervention FlowchartEvaluation and intervention Flowchart

CyanosisCyanosis 3g/dL deoxyhemoglobin3g/dL deoxyhemoglobin Low flow areas with increased oxygen Low flow areas with increased oxygen
extraction have more extraction have more deoxyhemoglobindeoxyhemoglobin
High flow areas with less extraction High flow areas with less extraction should not have enough should not have enough deoxyhemaglobin to appear cyanoticdeoxyhemaglobin to appear cyanotic Under normal circumstances you should not be able to Under normal circumstances you should not be able to
extract enough Oextract enough O22 to have 3g/dL deoxyhemoglobin running to have 3g/dL deoxyhemoglobin running through the tongue and gums (lips OK when cold)through the tongue and gums (lips OK when cold)

Cyanosis Acro v CentralCyanosis Acro v Central
AcrocyanosisAcrocyanosis part of normal part of normal
transitiontransition may last 72hrmay last 72hr beware APGAR beware APGAR
of 10of 10 hypoperfusedhypoperfused severe anemiasevere anemia

CyanosisCyanosis

Cyanosis
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80
HCT
% S
atu
rati
on
CyanosisCyanosis
Cyanosis is Cyanosis is dependent on dependent on HCT and % SatHCT and % Sat
Florescent light Florescent light makes cyanosis makes cyanosis hard to see.hard to see.
Except in the Except in the extreme, cyanosis extreme, cyanosis is not obviousis not obvious
Any question, Any question, check a pulse check a pulse oxox

RA v. ORA v. O22 - Saturations - Saturations

TermsTerms PaOPaO22 Arterial Oxygen Arterial Oxygen PressurePressure
Measured on an ABG machineMeasured on an ABG machine Oxygen dissolved in plasmaOxygen dissolved in plasma
0.003 ml O0.003 ml O22/mmHg/dl plasma/mmHg/dl plasma
SaOSaO22 Percent Oxygen Percent Oxygen SaturationSaturation
Measured by saturation monitor (pulse-Ox)Measured by saturation monitor (pulse-Ox) ~1.34ml O2/g Hb~1.34ml O2/g Hb
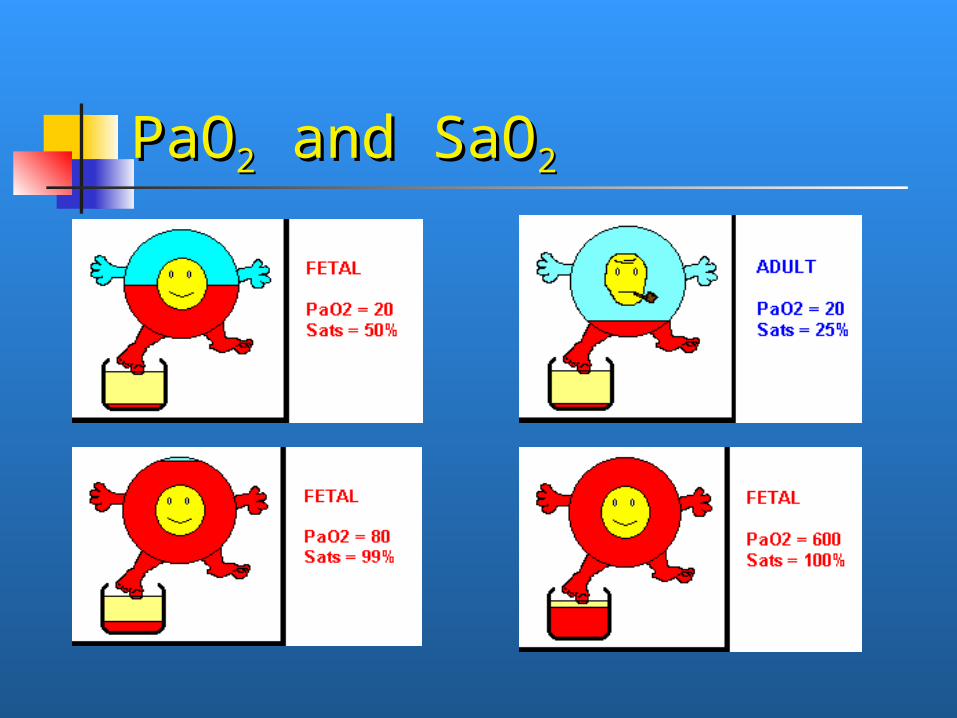
PaOPaO22 and SaO and SaO22

Oxyhemoglobin Oxyhemoglobin dissociationdissociation

TermsTerms CaOCaO22
Oxygen Content of the bloodOxygen Content of the blood bound to Hb + dissolved in plasmabound to Hb + dissolved in plasma
100% saturated100% saturated Hb 18g/dlHb 18g/dl 90 mmHg in plasma90 mmHg in plasma
= [1.0*18*1.34]+[0.003*90]= [1.0*18*1.34]+[0.003*90] = [24]+[0.25]= [24]+[0.25] Physiologically, saturations much more Physiologically, saturations much more
important to oxygen content important to oxygen content (0.003*600 (0.003*600 = 1.8)= 1.8)

CaOCaO22 Samples Samples
NORMALNORMAL95%, Hb 1895%, Hb 18PaO2 85PaO2 85[.95*18*1.34]+[0.003*8[.95*18*1.34]+[0.003*8
5]5]
[23]+[0.25]=[23]+[0.25]=2233
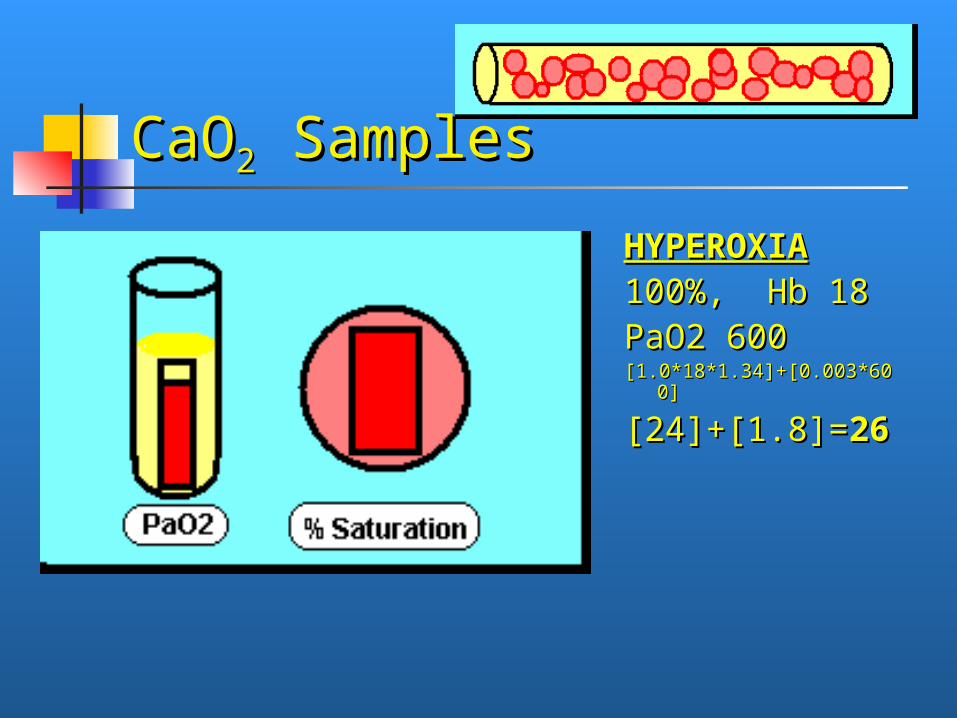
CaOCaO22 Samples Samples
HYPEROXIAHYPEROXIA100%, Hb 18 100%, Hb 18 PaO2 600PaO2 600[1.0*18*1.34]+[0.003*6[1.0*18*1.34]+[0.003*6
00]00]
[24]+[1.8]=[24]+[1.8]=2266

CaOCaO22 Samples Samples
ANEMIAANEMIA95%, Hb 10 95%, Hb 10 PaO2 85PaO2 85[.95*10*1.34]+[0.003*85][.95*10*1.34]+[0.003*85]
[13]+[0.25]=[13]+[0.25]=1313

CaOCaO22 Samples Samples
ANEMIA-ANEMIA-HYPEROXIAHYPEROXIA
100%, Hb 10 100%, Hb 10 PaO2 600PaO2 600[1.0*10*1.34]+[0.003*600][1.0*10*1.34]+[0.003*600]
[13]+[1.8]=[13]+[1.8]=1515

CaOCaO22 Samples Samples
CCHDCCHD75%, Hb 1875%, Hb 18PaO2 40PaO2 40[.75*18*1.34]+[0.003*40][.75*18*1.34]+[0.003*40]
[18]+[0.12]=[18]+[0.12]=1188

CaOCaO22 Samples Samples
CCHD-ANEMIACCHD-ANEMIA75%, Hb 1075%, Hb 10PaO2 40PaO2 40[.75*10*1.34]+[0[.75*10*1.34]+[0..003*40]003*40]
[10]+[0.12]=[10]+[0.12]=1010

Differential of cyanosisDifferential of cyanosis 3g of deoxyhemoglobin/dL 3g of deoxyhemoglobin/dL
(cyanosis)(cyanosis)
- Not enough oxygen in- Not enough oxygen in - Oxygen “mal-absorption”- Oxygen “mal-absorption” - Too much oxygen out- Too much oxygen out

Not enough oxygen inNot enough oxygen in ApneaApnea
neurologic and pharmacologic causesneurologic and pharmacologic causes Diffusion barrierDiffusion barrier
RDS, aspiration, pneumoniaRDS, aspiration, pneumonia ObstructionObstruction
pneumothorax, head positionpneumothorax, head position

Oxygen “mal-absorption”Oxygen “mal-absorption” Shunting lesionsShunting lesions
cardiaccardiac non-cardiac (like PPHN)non-cardiac (like PPHN)
HematologicHematologic methemoglobinemiamethemoglobinemia carboxyhemoglobinemiacarboxyhemoglobinemia

Too much oxygen outToo much oxygen out High oxygen consumptionHigh oxygen consumption
sepsissepsis low flow, high extractionlow flow, high extraction
acrocyanosisacrocyanosis hyperviscosity/polycythemiahyperviscosity/polycythemia extravasated (ie bruising)extravasated (ie bruising)
What is the Hyperoxia test?What is the Hyperoxia test?

Hyperoxia TestHyperoxia Test Infant on Room Air, get ABGInfant on Room Air, get ABG Infant on 100% oxygen, get ABGInfant on 100% oxygen, get ABG PaOPaO22 unchanged = fixed shunt = unchanged = fixed shunt =
CCHDCCHD Max PaOMax PaO22 <100 = CCHD <100 = CCHD Max PaOMax PaO22 >200 = No CCHD >200 = No CCHD

Hyperoxia TestHyperoxia Test Giving 100% overcomes the diffusion barrierGiving 100% overcomes the diffusion barrier
Normal -----------Normal ----------- Bad Lungs -------Bad Lungs -------
(diffusion barrier)(diffusion barrier)
Shunt -------------Shunt -------------
Shunt with Bad --Shunt with Bad --
LungsLungs

Hyperoxia TestHyperoxia Test
Hyperoxia Hyperoxia ProperProper
Hyperoxia Hyperoxia CPAPCPAP
Hyperoxia Hyperoxia hyper-hyper-ventilationventilation

Hyperoxia TestHyperoxia Test Jones: 1976Jones: 1976
8/109 with CCHD had PaO8/109 with CCHD had PaO22 > > 100mmHg100mmHg
7/23 without CCHD (bad RDS etc) had 7/23 without CCHD (bad RDS etc) had PaOPaO22 < 150mmHg < 150mmHg
HLHS > 300mmHgHLHS > 300mmHg TGA, TAPVR > 200mmHgTGA, TAPVR > 200mmHg Don’t be fooled by early high PaODon’t be fooled by early high PaO22ss

Hyperoxia TestHyperoxia Test Don’t do the room air partDon’t do the room air part
Looking for minimal PaOLooking for minimal PaO22 change from 21% change from 21% to 100% fiOto 100% fiO22
Hyperoxia test developed pre pulse-oxHyperoxia test developed pre pulse-ox With pulse-ox you can tell when PaOWith pulse-ox you can tell when PaO22s are s are
not changing despite big changes in fiOnot changing despite big changes in fiO22 (for sats that are between 70 and 95%)(for sats that are between 70 and 95%)
Probably the norm to have some degree of Probably the norm to have some degree of lung disease at the time of the test anywaylung disease at the time of the test anyway

Information neededInformation needed Clinical appearanceClinical appearance
““comfortably tachypneic and blue”comfortably tachypneic and blue” Pulses/perfusionPulses/perfusion
differential, delayeddifferential, delayed Pulse-Ox/ABGPulse-Ox/ABG
pre and post ductal, max PaOpre and post ductal, max PaO22
AuscultationAuscultation S2, MurmurS2, Murmur

Information neededInformation needed CXRCXR
heart shapesheart shapes snowman = TAPVRsnowman = TAPVR11
boot = pulm atresia, TOF, tricuspid atresiaboot = pulm atresia, TOF, tricuspid atresia egg on string = TGAegg on string = TGA
pulmonary vascularitypulmonary vascularity EKGEKG
axisaxis increased or decreased forcesincreased or decreased forces

TAPVRTAPVR11
SnowmanSnowman 50% type 150% type 1 50% 50%
snowmansnowman venous venous
connection at connection at VV to SVCVV to SVC

TOFTOF
Boot Boot shapeshape RVH lifting RVH lifting
apexapex loss of PA loss of PA
knobknob

TGATGA
Egg on a Egg on a stringstring alignment of alignment of
PA and Ao PA and Ao narrows the narrows the mediastinummediastinum

The 6 T’sThe 6 T’s
Total Anomalous Pulmonary VeinsTotal Anomalous Pulmonary Veins Tetrology of Fallot Tetrology of Fallot Tricuspid AtresiaTricuspid Atresia TranspositionTransposition Truncus ArteriosusTruncus Arteriosus
Total AcardiaTotal Acardia

Normal AnatomyNormal Anatomy normalnormal

PPHN - PDA shuntingPPHN - PDA shunting Pre and post Pre and post
ductal satsductal sats Head and Head and
coronaries get coronaries get well well oxygenated oxygenated bloodblood

Normal AnatomyNormal Anatomy normalnormal

PPHN - PFO shuntingPPHN - PFO shunting Head and Head and
coronaries coronaries get get hypoxemic hypoxemic bloodblood
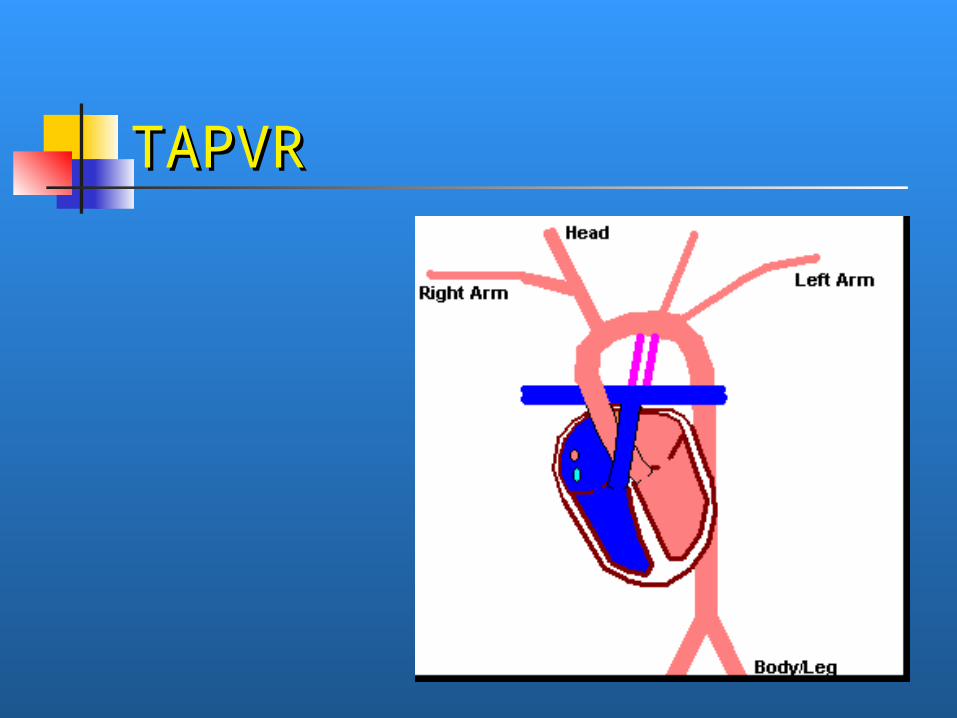
TAPVRTAPVR

TAPVRTAPVR Type 1 Type 1
(supracardiac)(supracardiac) 50% with 50% with
snowmansnowman can have can have
UE<LE satsUE<LE sats Type 2 (cardiac)Type 2 (cardiac) Type 3 Type 3
(infracardiac)(infracardiac) all can all can
obstruct, obstruct, infracardiac infracardiac almost always almost always doesdoes

Normal AnatomyNormal Anatomy normalnormal

TOFTOF OverridinOverridin
g Aortag Aorta VSDVSD PSPS RVHRVH
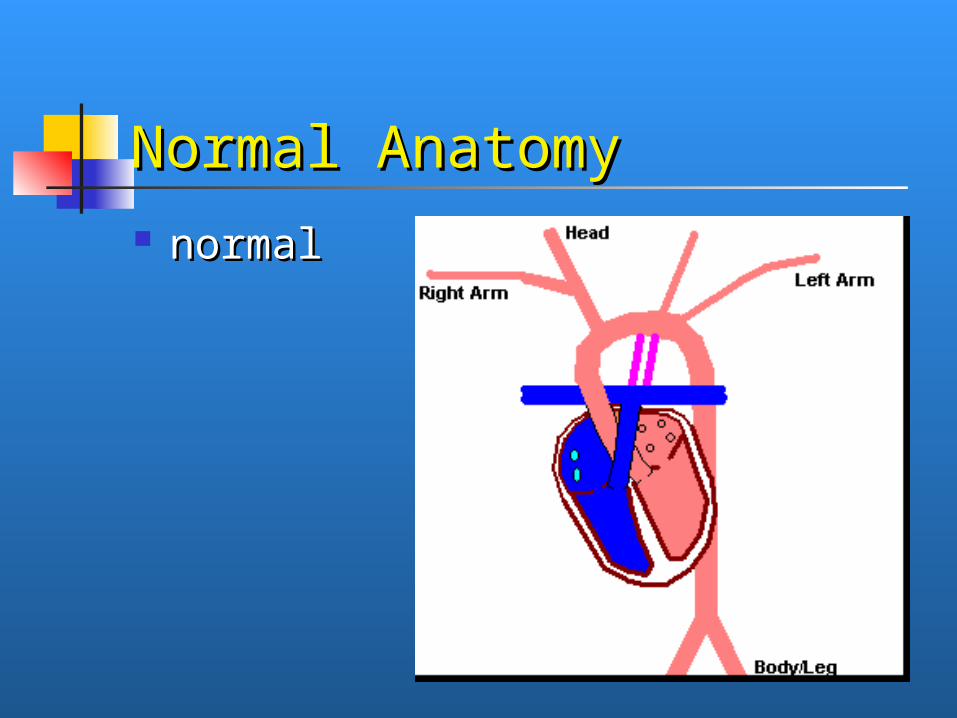
Normal AnatomyNormal Anatomy normalnormal

Tricuspid AtresiaTricuspid Atresia
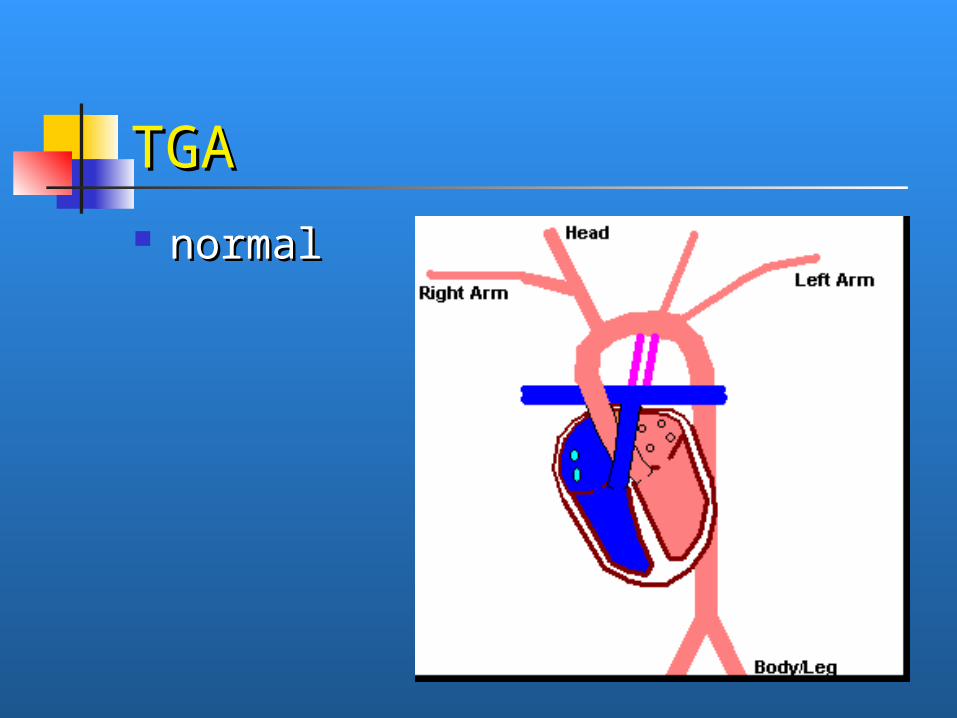
TGATGA normalnormal

TGA - no PPHNTGA - no PPHN Comfortably Comfortably
tachypneic tachypneic (usually big) (usually big) child with child with sats in the sats in the 50s on room 50s on room air or air or oxygenoxygen

TGA - with PPHNTGA - with PPHN TGA and TGA and
TAPVR type 1 TAPVR type 1 can present can present with higher with higher sats in then sats in then lower lower extremities extremities than the upper than the upper
extremitiesextremities
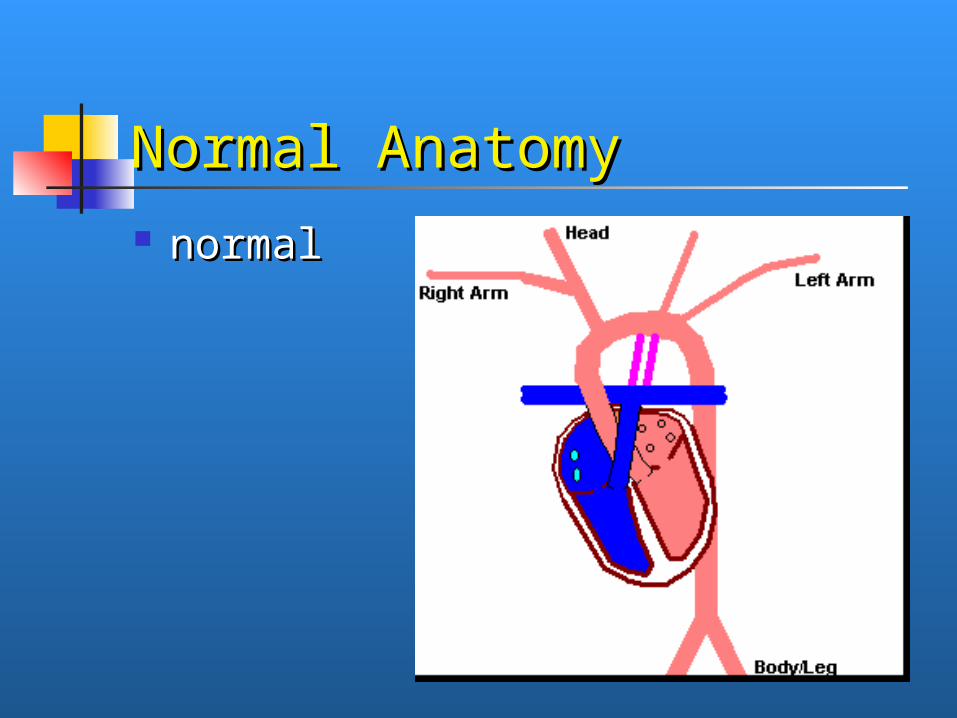
Normal AnatomyNormal Anatomy normalnormal
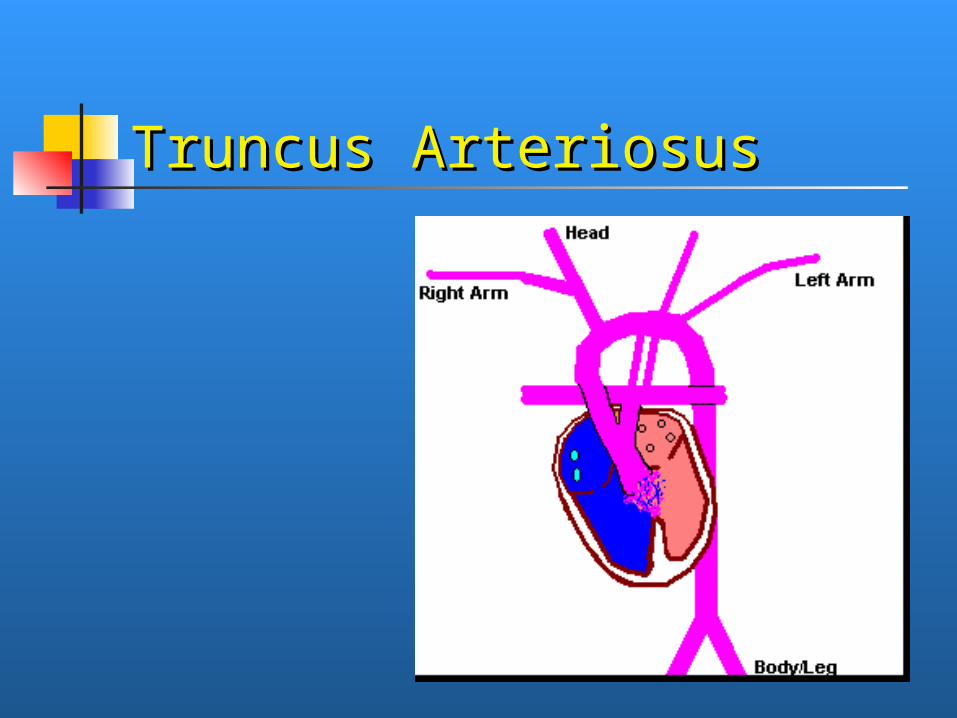
Truncus ArteriosusTruncus Arteriosus

Normal AnatomyNormal Anatomy normalnormal

Total AcardiaTotal Acardia Poor Poor
prognosis, prognosis, consider consider DNRDNR

Flow diagramFlow diagram There are bad acyanotic lesionsThere are bad acyanotic lesions There are bad cyanotic lesionsThere are bad cyanotic lesions A ductal dependent lesion is one that A ductal dependent lesion is one that
depends on the ductus to get adequate depends on the ductus to get adequate blood flow to the pulmonary and blood flow to the pulmonary and systemic circuits, or provide mixingsystemic circuits, or provide mixing
PSPS CoACoA TGATGA

Summary and Take Home Summary and Take Home PointsPoints
Check a pulse ox Check a pulse ox (murmur w/u, suspicion)(murmur w/u, suspicion) murmur w/u (š Sx) murmur w/u (š Sx) Pulse-OxPulse-Ox, EKG, 4-point BPs, EKG, 4-point BPs
Don’t be fooled by a reassuring Don’t be fooled by a reassuring hyperoxia test if suspicion remains highhyperoxia test if suspicion remains high
If you think you have a ductal If you think you have a ductal dependent lesion, start prostin (don’t be dependent lesion, start prostin (don’t be afraid of prostin)afraid of prostin)

Summary and Take Home Summary and Take Home PointsPoints
If a baby presents in shock in the first If a baby presents in shock in the first week week (or two)(or two) of life think sepsis & of life think sepsis & ductal dependant lesions & CAHductal dependant lesions & CAH
Cyanosis w/u includes antibioticsCyanosis w/u includes antibiotics Make sure your pharmacy carries Make sure your pharmacy carries
prostinprostin Don’t be afraid to use itDon’t be afraid to use it Know how to mix it!Know how to mix it!

QUESTIONS?QUESTIONS?