evaluation of the borderline personality disorder ... · evaluation of the borderline personality...
TRANSCRIPT

1 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Evaluation of the
Borderline Personality Disorder
Awareness Workshops
for Service Users and Carers.
Project Report
By Clare Carter and Theresa Sired July 2014
Evaluation : S369

2 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Contents
Page no.
Executive summary …………………………………. 3
Introduction …………………………………...….…… 4
Aims of the project ………………………..……….… 6
Workshop design ………………………….…………. 7
Findings ……………………………………......……. .13
Discussion …………………………….…….….……. 26
Recommendations …………………………….…… 30
Actions ……………………………………………….. 31
References …………………………………..………. 32
Appendix ………………………………….………… 34

3 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Executive Summary Introduction The proposal for the awareness workshops was a result of direct consultations with Service Users and Carers of people who attract the diagnosis of Personality Disorder in Somerset, which identified the need for local education and training for service users and carers.
Aims The main aims of the project were to:
To design and deliver workshops for service users and carers to increase their awareness of Borderline Personality Disorder (BPD).
To increase knowledge of what the Trust provides in terms of treatment and support for service users and carers of BPD.
To outcome and evaluate the usefulness of the workshops.
Project delivery A single session model was delivered by two trainers using an interactive and interpersonal model of delivery. The workshops aimed to provide a safe, validating environment to aid learning. Each workshop accommodated a maximum of 12 service users or carers/ family members. The content included information on BPD diagnosis, aetiology, development and treatment and support available from the Trust. The workshops were evaluated using a specifically developed pre and post self-report measure (e-KALM) and completion of a ‘free text’ evaluation form.
Findings Five workshops were completed and a total of 31 people attended. Feedback was very positive from both service users and carers, with the most valued aspect being that of sharing experiences and realising “I’m not alone”. In regard to the e-KALM measures, there was a statistically significant increase in scores between those completed prior to the workshop (M= 25.30, SD= 4.68) and those completed afterwards (M=32.10, SD= 4.33); t (29) = 8.18, p < .001, demonstrating a significant increase in knowledge and understanding of BPD.
Recommendations 1. To continue to deliver the awareness workshops using a flexible and interpersonal model of delivery. 2. Complete a follow up measure with participants. 3. Share report with carers support services. 4. Contribute findings to the development of Mental Health Awareness training initiatives within the Trust. 5. Provide top up training for front line primary and secondary care staff in the Relational Recovery Approach.

4 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Introduction
This proposal was developed as a result of a previous project, Making Contact: A report on direct consultations with Service Users and Carers of people who attract the diagnosis of Personality Disorder in Somerset (Gordon, 2008). The consultation was funded by the South West Care Services Improvement Programme (CSIP SW) and its main aims were to:
Consult service users and carers to identify their needs Provide identified training and education Develop a support network Identify service users and carers who can inform and help develop mental
health services Develop and provide a central point of information for service users and carers
As part of the project the following needs were identified as being possible objectives of a psychoeducational group.
Summary of identified needs from the Making Contact Project:
Informed of the diagnosis as standard Diagnosis shared in a meaningful way Diagnosis to be reviewed and accurately recorded Consider sharing the diagnosis with carers Support groups for service users Information leaflets Local training and education for service users and carers
The proposal for the awareness workshops was also a development of training already being delivered in the Trust to staff members. The Relational Recovery Training is a whole systems approach to equipping frontline staff with the knowledge and skills to work effectively with people with personality disorder, and was developed by the Trust. The proposal to deliver awareness workshops is a development of this programme to provide the benefits of training directly to service users and carers. In regard to the evidence base for delivering the workshops, in addition to the results from the ‘Making Contact’ project, there is a lot of research and evidence for the benefits of psychoeducation for service users with various mental health problems (for example, see meta-analyses; Donker et al, 2009; Gregory et al, 2004). Psychoeducation is among the most effective of the evidence-based practices that have emerged in both clinical trials and community settings (Lukens & McFarlane, 2004).
As for including carers, there is also evidence for the effectiveness of involving family members in the treatment for the individual (e.g. meta-analysis :Martire et al, 2004). There seems to be limited research and evidence of the benefits of psychoeducational group work for service users and carers jointly in general within

5 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
mental health settings, however, some evidence has been found on a joint programme to show positive effects for family members. Koshknab et al, (2013) showed results from their RCT that highlighted the success of a 4 week group programme for caregivers of inpatients with acute phase schizophrenia, in reducing family burden on care givers.
More specifically, regarding personality disorders, research has shown psychoeducation for patients with a diagnosis of borderline personality disorder (BPD) to be beneficial (e.g. Rentrop et al, 2012; Banerjee et al, 2006; Colom et al, 2004). One particular study highlighted that psychoeducation alone can help reduce BPD symptoms in participants, namely impulsivity and “storminess of close relationships” (Zanarini et al, 2008). As well as research findings, national guidance highlights the importance of education around diagnosis and treatment. The Patients' Charter for Mental Health Services (DOH, 1997) states that a patient is entitled to both know and understand his or her diagnosis. Despite this, people with the diagnosis of a personality disorder are not always well informed about their disorder (Banerjee et al, 2006). In addition to this the NICE Guidelines for the treatment and management of Borderline Personality Disorder (2009) stress the importance of good communication and evidence-based information, to allow service users to make informed decisions about their care.
A proposal was therefore made to run a pilot project to deliver and evaluate psychoeducation, awareness workshops for service users and carers across Somerset Partnership NHS Foundation Trust.
A proposal was submitted to the Clinical Effectiveness and Research group prior to commencing delivery (see Appendix 7).

6 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Aims of the project
To design and deliver workshops for service users and carers to increase their awareness of BPD.
To provide a warm, safe forum to enable learning for participants.
To increase knowledge and understanding/ learning of BPD for service users and Carers.
To increase a positive attitude towards people with BPD.
To increase knowledge of what the Trust provides in terms of treatment and support for service users and carers of BPD.
To increase empathy towards self/ others regarding BPD.
To outcome and evaluate the usefulness of the workshops.

7 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Workshop Design
Location To ensure equity and greater access the workshops were distributed across the county: Yeovil x2, Chard, Taunton, Bridgwater x2, Frome, Glastonbury, Minehead, Wincanton, Chard.
Venues were chosen for good access, and where possible were held in Trust premises to help reduce costs. Community settings were also used to help normalise and reduce stigma. It was important when choosing accommodation, to ensure an environment where there was adequate space for participants to leave the room safely if necessary.
Timings
Each workshop was delivered over one day from 9.30-3.30pm. Timings through the day were made clear but were also flexible in order to meet the needs of participants. The workshop was designed with plenty of breaks to aid the processing of information and any emotions that may have been evoked.
Provision
Ten workshops were initially planned for delivery over 3 months, with 12 places maximum per workshop for service users and carers. An additional workshop was added during this time due to a need identified by some of the carers who felt they could not openly express themselves in front of service users. They believed they would feel more comfortable and get more benefit from a carers only workshop. Thus a total number of 11 workshops were planned.
Costs
The average cost to run one workshop was approximately £400. When the workshops were held in Trust premises this dropped to about £300. The costs include trainers’ time and resources. Please see Appendix 5 for details on the breakdown of costs.
11 Workshops were planned across the Trust
12 participants per workshop
Single session model 9.30‐3.30pm.
Average cost per workshop £400.

8 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Referral and Screening The target group were adult secondary mental health care users (see Appendix 1 for project proposal). Consideration was made as to which personality disorder type was most likely to want to access this workshop. Borderline Personality Disorder was identified as the most prevalent diagnosis of people referred to the Personality Disorder Service. Therefore, due to clinical need, the focus of the workshops was on a single personality disorder type, Borderline Personality Disorder, paying attention to the fact that service users may well attend with more than one personality disorder diagnosis, and other mental health problems. Any adult within secondary care mental health services (either registered on Rio as a client or a carer) that wanted to learn more about Borderline Personality Disorder was welcome to attend, and to bring an additional person with them if they wished. There were therefore three categories of attendee; Service User, Carer (registered on Rio) and Family Member/Friend.
Service users and carers were recruited via advertising of the workshops specifically to Care Co-ordinators, but also via email to all staff ‘Trust –wide’. Flyers were distributed to various premises across the Trust. The workshops were also advertised on the Trust website. People could be referred or preferably self-refer to the workshops. Service users and carers were asked to contact the trainers via specific BPD awareness email, or by phone. Trainers were therefore contactable to answer any queries people may have about the workshops prior to attending. Upon contacting trainers, prospective attendees were given basic information about the content of the workshop, invited to ask any questions they may have about the workshops and then asked whether they felt the group would be helpful for them. Information was provided about the sharing of and recording of information, i.e. documenting attendance in Electronic Patient Records, talking with Care-Coordinators where one is allocated, and being specific about how we manage information related to risk of harm. As part of the process Care Co-ordinators or Carer Support Workers were then informed about the individual’s referral and asked to confirm to the trainers if there was any reason they were aware of that would mean the workshop would not be suitable for the individual. There were very few times that this occurred, but on the odd occasion either the trainer or care co-ordinator would then speak to the individual to discuss this and offer alternatives where appropriate.
Focus of Workshop on Borderline Personality Disorder for any service user or carer who
wanted to know more.

9 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Content
The content of the workshops was specified in the proposal to include;
information on BPD diagnosis
diagnostic classifications (DSM IV, ICD 10)
aetiology, causes
development of BPD
relationships and attachment; theory and principles
treatments and support provided in the Trust.
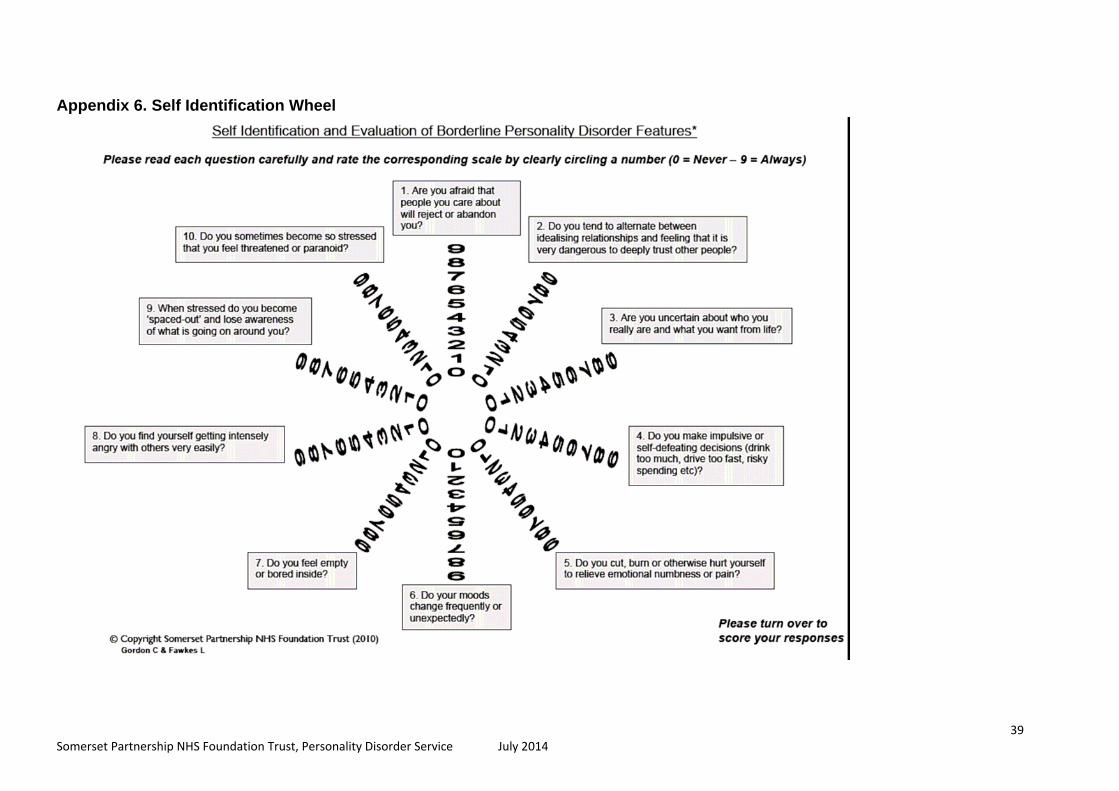
The programme consisted of a mixture of information sharing and discussion around the topics as outlined above (please see the Agenda in Appendix 2). The programme for the workshops was adaptable and flexible enough to accommodate individual group learning needs. A Power Point presentation was developed specifically for the one day workshops and the information was sensitive and balanced to the mix of service users, carers and family members that would attend. Alongside this, participants were provided with a resource pack including amongst other things: information about formal diagnostic classifications, The Self Identification Wheel (see Appendix 6), information on Attachment Theory and the development of BPD, Risk Matrix and leaflets and information on treatments and support services available in the Trust. A further patient information leaflet was developed as a result of the workshops to provide people with information on the basics of BPD.
The workshops also involved tasks in pairs or small groups, and included exploration of concepts using a Cognitive Analytic Model to describe repeating patterns of relating to self and others and formulating the effect these patterns have on view of self and others. An example formulation is described on the next page.
Self‐referral was promoted but with a ‘checking in’ discussion with care co‐ordinator and
brief Electronic Patient Record review to assess risk.
Diagnosis of BPD not imperative, but ability to work safely in a group was.
Working with both Service Users and Carers allowed the trainers opportunity to
incorporate a large relational element using a Cognitive Analytic Therapy informed model
of understanding relationships.

10 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Formulation
One method adopted in the workshops was to formulate with group members their experiences of relating to others, with a view to considering repeating patterns and understanding these patterns in the context of everyday life. By formulating these experiences it was hoped that group members could begin to see patterns and understand how the patterns affected them in terms of thoughts, feelings and consequences. Additionally, by considering other people’s points of view within the formulation awareness of problematic patterns could be further explored. These patterns were then related to the different dimensions of BPD as highlighted on the Self Identification Wheel (see Appendix 6) and also by reflecting back to the diagnostic criteria. We also hoped that this would facilitate reflection and recognition. Figure 1 below shows an example of a formulation.
Figure 1. “Why won’t they text me back?” Example formulation.
OR
11 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
As a result of the adaptations to the PD‐KASQ, the new tool was given the acronym
e‐KALM;
Empathy
Knowledge
Attitude
Learning
Management
This joint understanding allowed both service user and carer to see the interactions from each other’s perspective and consider alternative ways of managing the distress and how unhelpful the pattern has become in their relationship.
Evaluation methodology
When researching for a suitable method of evaluation the PDKASQ (Bolton et al ) was considered. This is an 18 item self report questionnaire that contains three factors; understanding, perceived capabilities, and emotional reactions, and was created as a means of fully evaluating staff training for a personality disorder course. It therefore seemed a helpful template for evaluating this workshop but was considered to be too long and some questions were not appropriate for use with service users and carers. The questionnaire was thus adapted to help measure the aims of the workshop for service users and carers. The new e-KALM self report questionnaire aimed to measure empathy, knowledge, attitudes, learning and management regarding BPD. Please see Appendix 3 for a copy. The questionnaire was completed by participants both pre and post workshop.
Participants also completed a ‘Workshop Evaluation Form’ at the end of the workshop which consisted of open ended questions about the quality of the workshop, trainers, resources and other aspects of the day (see Appendix 4 for a full list of the questions asked).
Trainers Two trainers were appointed to plan and deliver the workshops to help delivery of the content and manage group dynamics. Relevant trainer skills included being confident with group management and risk management. Psychotherapeutic skills were pertinent and important in offering an empathic environment, flexibility and sensitivity to individual group member needs as well as underpinning a good understanding of specific issues relating to Borderline Personality Disorder. This is important as it has been described previously that group leaders should have ‘a firm and accurate knowledge and understanding of the illness or condition’ (Brown, 2011).

12 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Combining the skills of an Assistant Psychologist with the skills of a Cognitive Analytic Therapist enabled the workshops to develop past a didactic delivery to an interpersonal and relational context.
Trainer skills: Knowledge of Borderline Personality Disorder within an
interpersonal context and ability to deliver safely in a group setting.

13 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Findings
Attendance In total 5 workshops were completed: Taunton, Yeovil x1, Bridgwater x2 and Glastonbury. A total number of 31 people attended across the 5 workshops, with an average number of 6 people attending per workshop (range= 5-8). The ratio of service users to carers/ family members per workshop ranged from 2:5 and 4:1 respectively. For the purposes of the evaluation a carer was defined as someone who was classified by the service user as a ‘carer’ and had an individual Electronic Patient Record on Rio, otherwise they were classed as a family member or friend. Of the workshops completed, there was an average of 76% attendance, with some people who did not attend (DNA) and cancellations. Due to limited demand, 6 workshops were cancelled: Yeovil x1, Chard x2, Minehead, Wincanton and Frome. Groups were cancelled when fewer than 3 participants were registered to attend. Five people attended the carers only workshop; 3 women and 2 men. A further 5 people were due to attend but unfortunately they cancelled or did not attend on the day. For one participant it was his second time at a workshop to allow for a different family member to attend with him. The following graphs provide demographic information on the people who attended the workshops. Age and Gender Twenty five of the participants were women and 6 were men, and one man attended twice. The age range was 18-60 years.
Age & Gender of Participants
0
1
2
3
4
5
6
18‐25
26‐31
32‐40
41‐50
51‐60
61‐70
70+
unknown
Age (years)
Number of people
female
male

14 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Participant type There was a mix of service users, carers and family members or friends that attended the workshops. In total, 14 people were service users and 17 carers or family members/ friends.
Participant type
32%
23%
45%Service User
Carer (as on RIO)
Family member/ Friend
Diagnosis Less than 20% of all participants had a formal diagnosis of Borderline Personality Disorder, and 16% had a different diagnosis. Of those with BPD diagnosis, there was an even split of those who had the diagnosis for less than one year and those who had the diagnosis for more than 1 year.
Diagnoses
6
18
7
5
19
7
3 3
0
2
4
6
8
10
12
14
16
18
20
yes no unknown yes no unknown <1 year >1 year
BPD diagnosis
number of people
1 or more other current
diagnosesDuration of BPD
diagnosis

15 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Recruitment method Over 1/3 of participants had found out about the workshop from their Care Co-ordinator and just under a 1/3 had learnt about it from another service user/ carer/ family member/ friend (generally the person they attended with).
Recruitment methods
0
2
4
6
8
10
12
CCO
Carer Support Worker
Poster
Other Service User/carer
Staff email
Therapist/Practitoner
Number of people
5 workshops completed with 31 people in total attending
45% service users, 55% carers/ family members
20% participants had a formal diagnosis of Borderline Personality Disorder
Over 1/3 participants had learnt about the workshop from their Care Co‐
ordinator.

16 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
e-KALM results In total 30 people, service users and carers completed both measures. The graphs below demonstrate the outcomes for total scores and for each question.
Total scores The total scores represent the cumulative score to answers regarding questions on knowledge, attitude, understanding and management of BPD. Thus the highest obtainable score of 40 may represent a greater awareness of BPD. Graph 1a shows the total pre and post scores for the e-KALM measure for each participant. Note that Question 9, relating to empathy towards those with BPD, was added to the questionnaire at a later date, so the scores for this question are not included in the total scores.
Graph 1. Total scores from e-KALM measure.
Total scores of e-KALM pre & post measures
0
5
10
15
20
25
30
35
40
1 4 7 10 13 16 19 22 25 28
participant
To
tal s
co
re
total pre
total post
A paired-samples t-test was conducted to compare the total score on the e-KALM at the start and at the end of the workshop. There was a statistically significant increase in scores between the e-KALM measure completed prior to the workshop (M= 25.30, SD= 4.68) and those completed afterwards (M=32.10, SD= 4.33); t (29) = 8.18, p < .001. In regard to comparison of service user and carers total scores, the average (mean) score for service users pre workshop was 23.4 and post 30.6. For carers, the average pre score was higher; 27 and was the post workshop score; 33.4.

17 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Q2- I have a good understanding of how BPD develops
17% 20%
40%
17%
6%0 0
10%
67%
23%
0%10%20%30%40%
50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
pre workshop
post workshop
The following graphs represent the scores for both service users and carers jointly for each of the questions in the e-KALM measure. The average (mean) score for both pre and post measures have been described along with the corresponding answer on the e-KALM measure.
Knowledge- diagnosis of BPD.
There was a considerable increase in scores for the question regarding knowledge of the diagnosis of BPD. The average (mean) pre score was 2.9 (‘uncertain’) and post workshop 4.2 (‘agree’) for service users and carers combined. Graph 2. Results from Question1 e-KALM- Knowledge of the diagnosis of BPD.
Learning- development of BPD
In regard to having a ‘good understanding of how BPD develops’, there was again an increase in score post workshop. The average (mean) score pre workshop was 2.8 (‘uncertain’) and post 4.1 (‘agree’).
Graph 3. Results from e-kalm question 2- Understanding of how BPD develops.

18 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Q3-I have a good understanding of why I, or the person I care for, self harms or may
behave in self-destructive ways
13%3%
40% 37%
7%0 0
13%
60%
27%
0%10%20%30%40%50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
pre workshop
postworkshop
Q4- I have a positive view of BPD
20%10%
37%27%
6%0
16% 20%
37%
27%
0%10%20%30%40%50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
preworkshoppostworkshop
Learning- explanations for self destructive behaviours.
In terms of having a good understanding of self harm or self destructive behaviours the average (mean) pre score was 3.2 (‘uncertain’) and post; 4.1 (‘agree’).
Graph 4. Results from e-KALM Question 3- Understanding of self harm.
Attitude- Views of BPD
There was a smaller difference in pre and post scores regarding having a positive view of BPD, with an average (mean) score pre workshop of 2.9 (‘uncertain’) and 3.8 (‘agree’) post workshop.
Graph 5. Results from e-KALM Question 4- views of BPD.

19 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Q5- I have a positive attitude tow ards people w ith B P D
3% 0
30%
57%
10%0 3%
40%
3%
54%
0%10%20%30%40%50%60%70%80%
stronglyd isagree
disagree uncerta in agree stronglyagree
prew orks hop
pos tw orks hop
Q6- I feel confident that I can make a positive impact on caring for myself or caring for
someone with BPD
0% 3%
60%
30%
7%0% 0
37% 40%
23%
0%10%20%30%40%50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
preworkshop
postworkshop
Attitude- towards people with BPD.
The pre workshop score for having a positive attitude towards people with BPD was higher than some other domains and the difference in scores pre and post less so. The average (mean) score pre workshop was 3.7 (‘agree’) and post workshop was 4.3 (‘agree’).
Graph 6. Results from e-KALM Question 5-attitudes of BPD.
Management – caring for myself or others
There was a small increase in scores pre and post workshop regarding confidence in making a positive impact on caring for myself or someone with BPD. The average (mean) score pre workshop was 3.4 (‘uncertain’) and 3.9 (‘agree’) post workshop.
Graph 7. Results from e-KALM Question 6- caring for myself or others

20 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Q8- I think I am able to make positive changes in my life or someone else's life.
13% 10%
54%
13% 10%3% 3%
13%
64%
17%
0%10%20%30%40%50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
pre workshop
postworkshop
Q7- I am aware of the options available to me in terms of treatment or support
13% 10%
54%
13% 10%3% 3%
13%
64%
17%
0%10%20%30%40%50%60%70%80%
stronglydisagree
disagree uncertain agree stronglyagree
preworkshoppostworkshop
Knowledge- Treatment options
There was an increase in scores post workshop regarding the knowledge of treatment options available, from an average (mean) score of 3 (‘uncertain’) pre workshop to 3.9 (‘agree’) post workshop.
Graph 8. Results from e-KALM Question 7- treatment options
Management- positive changes
There was an increase in scores for the question of ability to ‘make positive changes in my life or someone else’s life’ with a shift of an average (mean) score of 3.5 (‘uncertain’) to 3.8 (‘agree’) post workshop.
Graph 9. Results from Question 8- positive changes.

21 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Q9- I have empathy tow ards people w ith BPD.
0% 0%
18%
41% 41%
0% 0% 0%
35%
65%
0%10%20%
30%40%50%60%
70%80%
stronglydisagree
disagree uncertain agree stronglyagree
preworkshoppostworkshop
Empathy- towards people with BPD
The average pre score was higher for empathy compared to other domains with an average (mean) pre workshop score of 4.2 (‘agree’). Post workshop it increased to 4.6 (‘strongly agree’).
Graph10. Results from e-KALM Question 9- empathy.
* Question 9 was added to the questionnaire at a later date, so total no. of participant answers for this question is 17. For this reason the scores for this question are not included in the total scores.
Only 27% of participants’ described having a ‘good’ knowledge
of the diagnosis of BPD prior to completing the workshop.
Over 80% of participants ‘agreed or ‘strongly agreed’ that they
could make positive changes in their life or someone else’s
upon completion of the workshop.

22 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Qualitative results
The following themes are derived from feedback form the participant’s completed ‘workshop evaluation forms’ as well as trainers feedback of the workshops.
1. The workshop provided a warm, safe, validating environment.
Attendees reported finding the workshops warm, safe and validating. For example: “very impressed with course and how it was managed. Extremely helpful. Sensitive to needs.” (participant no. 2) and “…private and controlled environment. “ (participant no.9). Participants also described this from the start for example: “ felt really comfortable when starting the workshop...” (participant no.22)
Participants also described the trainers to be friendly and understanding, which may have helped to create the desired learning environment. For example: “ informative, gentle, encouraging. Felt a sense of understanding and empathy from both trainers, thank you.” (participant no.16) and “excellent. Friendly, supportive and very understanding.” (participant no.26).
There were occasions that participants (both service users and carers) needed some time to manage their emotions and chose to leave the room. Group members stuck to the ground rules established and let the trainers know when they needed some ‘time out’ and returned to the group when ready.
The groups were very accepting and containing and people looked after each other. Individuals managed their emotions well and the trainers did not encounter any group dynamics which were not manageable and containable. The group created their own safe and validating environment.
2. Flexible format and person centred approach. Providing flexibility to the delivery of the workshops and adapting the content to meet the needs of the participants present was seen as important. For example: “ very professional. Was a good balance of instructional information and allowing people to give their opinions.” (participant no.9)
The sharing of personal experiences was deemed invaluable by participants. For example: “ very well presented, allowing me to freely exchange experiences and check understanding of course content.” (participant no.25) and “ thought the trainers were excellent- patient, compassionate and took time to listen and understand people's points.” (participant no.8).
The formulation example on page 10 provides a good example of the flexible approach of the delivery in how an individual’s experience was used to describe and highlight some of the features of BPD.

23 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
3. Inclusion One of the most powerful aspects of the workshops, was the group format, allowing people to share their experiences and gain a sense of inclusion. As part of the workshop evaluation participants were asked ‘What was the most helpful or useful thing you learned today, if anything?’ (question 3). The most common answer (11/30 answers) was regarding the sharing of experiences with others who have BPD. For example: “I like the group format as it allowed the BPD sufferers a chance to share experiences.” (participant no.12) and “sharing with others- carers and people with the condition” (participant no.5).
A sense of being understood and not being judged also seemed important. For example: “I am not alone in experiencing the difficulties of BPD.” (participant no.6) and “being able to talk to people that understand and not being judged.” (participant no.26). The desire for inclusion may also have been highlighted by the choice of the participants to complete a group statement regarding BPD rather than doing individual statements. At the end of the workshop participants were invited to write a paragraph describing BPD in their words to help communicate their problems to others. An example of one of the group statements is as follows:
4. Motivation for change. There were many comments from the service users and carers that described a motivation for change as a result of the workshop. People commented on what they might do differently as a result of attending the workshop. For example: “.. I feel more confident to explain the disorders to my close friends- I have avoided doing this up to this point.” (participant no.8) and “found it motivational to learn about it so will be more determined to change my behaviour.” (participant no.31).
‘Having BPD isn't easy, it’s complicated because symptoms and severity can be different for everyone. I can’t just get better immediately. My emotions go up and down dramatically and they are very intense. It’s not my choice to be like this but things from the past continue to affect me and my behaviour now. I can misinterpret things easily. I am not attention seeking. What I'm striving for is security and consistency and to be loved.’ (example group statement explaining BPD)

24 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Participants described specific things they may do differently such as: “I will use the risk matrix form in the very near future” (participant no.15) and “… I will talk through the crisis plan we drew up with my therapist and CPN.” (participant no.16). As well as a motivation for change, a sense of empowerment was also observed, for example one carer informed the trainers and group at the beginning of the workshop that the service user she was attending with did not feel comfortable to talk in the group so would remain silent throughout. It was a big step to just attend the group as the service user would generally not leave the house or speak with anyone other than the carer. However, by the end of the workshop the service user was fully engaged with the workshop and talking to the group describing some of her own experiences.
Another service user had only intended to stay for a couple of hours as she was quite anxious about attending the workshop. She also rarely left the house or spoke to others outside her family. However, soon enough, the service user was providing opinions and discussing topics with the group and stayed for the whole of the workshop.
5. Support for carers. Many of the carers that attended described a need for further support for carers of people that have BPD. For example, some participants suggested : “may be carers and BPD sufferers separate (workshops)” (participant no.4). Following on from this workshop, a need was identified and a ‘carers only’ workshop was held. The carers that attended found this helpful and supportive and some suggested in their recommendations for : “….another carers only workshop.” (participant no.25). For some, more knowledge and tools in order to be able to help those with BPD was needed, for example: “there is a huge need to provide training/ workshops for family members and carers of BPD to provide practical tools and ways of helping people with BPD. This in turn could aid recovery and provide greater support for patients.” (participant no. 25).
6. Staff training There were a mix of views regarding peoples experiences of services within the Trust. Some participants described a general lack of understanding of healthcare professionals in their understanding of BPD and a need for further education/ training. For example: “I would personally like either some (user) groups for BPD that CPNs/ carers/ CCOs could attend to hear the clients experiences. Perhaps some more training or info for mental health teams.” (participant no. 16) and “ there are people that work within the Trust who in my opinion have a very limited or complete

25 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
lack of understanding of BPD and ways to help people with BPD and carers/ family members.” (participant no. 25). There were others that identified that there were individuals that had been really helpful and positive, although this wasn’t felt the ‘norm’. For example: “my CPN is fantastic and got me the info for this course, bar him very negative attitudes and a huge lack of knowledge and understanding.” (participant no.16).
It was generally noted that there were two distinct experiences of provision by services for service users and carers regarding BPD. That is, having what service users and carers deemed to be ‘good’ care and treatment, or alternatively, what service users and carers deemed to be unsatisfactory. This divide certainly raised angry feelings for some participants, however, the intensity of emotion and feelings were used to help participants motivate themselves for change and consider what they might do differently.

26 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Discussion Attendance
The most popular and well attended workshops were those in major towns, and/ or which had greater access namely Taunton, Bridgwater, Yeovil, Glastonbury. On average 76% of those who booked a place on the workshop, attended as planned. For those workshops that were cancelled due to lack of demand, a number of factors may have contributed to this:
* lack of service users and carers in that area that wanted to attend the workshops * lack of awareness of service users, carers and staff of the workshops in that area * lack of notice of the dates of the workshops * bad weather effecting travelling conditions
In addition it could be that the number of workshops planned, 11 workshops across 3 months, exceeded the demand. Thus, for future workshops, it may be worth having a smaller number of workshops planned across a longer period of time, therefore reducing the need to cancel workshops. It is also important that the dates for the workshops are communicated to staff and advertised across the Trust well in advance. This will allow more time for the recruitment process, and particularly the time required for people to self-refer to the workshops. It might also be helpful to attend team meetings to introduce and describe the workshops, so staff are more informed to advise service users and carers.
There was a fairly even mix of service users and carers/ family members that attended the workshops. This suggests the recruitment methods adopted reached both carers and service users alike. However, results show that most carers or family members were informed by the service user they attended with. This perhaps highlights a need to not only directly recruit registered Carers but also look to reaching those family members who are not registered as a carer within the Trust. It would also be helpful to consider rolling out the program to Primary Care audiences, possibly within Improving Access to Psychological Therapies (IAPT) service. The trainers were able to attend all workshops. However, to negate any difficulties for future delivery, it would be useful to have a ‘back up’ trainer available to facilitate in case one of the trainers was unable to attend for any reason. e-KALM results
Results of the e-KALM measure showed that the majority of participants (87%) did not have a good awareness of BPD prior to attending the workshop. This highlights the need for the awareness workshops, to help improve knowledge and understanding about the diagnosis and treatment options. It also suggests that those

27 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
attending were appropriate referrals, and reinforces the importance of the self –referral process. It seems that those who attended the workshops were those that required it.
Upon completion of the workshop most described having a good knowledge and understanding of BPD diagnosis and how it develops (67%).This shift in scores pre and post workshop indicates a self-reported increase in awareness of BPD across all domains of knowledge, learning, attitude and management. Using self-report measures means actual knowledge/understanding is not tested, however, for the purposes and intentions of the workshop individuals’ perceptions are considered sufficient. It is particularly encouraging that most people described feeling they would be able to make a positive change to their own or someone else’s life post workshop (81%). There was a statistically significant increase in scores between the e-KALM measures completed prior to the workshop (M= 25.30, SD= 4.68) and those completed afterwards (M=32.10, SD= 4.33); t (29) = 8.18, p < .001. Consideration needs to be made that the results are part of an evaluation of the workshops rather than a controlled study however, it perhaps shows promise that the workshops would be of benefit to others and further investigation may be warranted. It would aid the evaluation of the workshops to have a follow up measure asking participants who attended about any possible changes that they had made due to attending the workshop. It would also be useful to gain information on any other treatment or support accessed in the Trust post workshop as most participants (81%) described an increase in their knowledge of treatment options available to them. A large number of participants reported being ‘uncertain’ about many aspects of their knowledge and understanding about BPD prior to the workshop. The increase in certainty may show that the workshops ‘validated’ or confirmed knowledge they had but were unsure about, rather than that they learnt ‘new’ information. Adapting the questionnaire to ask ‘how would you rate your knowledge of BPD diagnosis’ using 1-5 scale (little- a lot) for example, might shed more light on this aspect for future workshops.
The e-KALM results also highlighted a positive shift in empathy and positive attitude towards people with BPD post workshop, however, the difference pre and post workshop was smaller to the other domains measured. This was primarily due to a higher level of empathy and positive attitude towards people with BPD, compared to knowledge about BPD, prior to the workshops. This perhaps could be expected as those with empathy may want to learn more about BPD to help themselves or others. Also, carers were generally family members with an in depth knowledge of the service user they are caring for which may well naturally increase levels of empathy.

28 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
It may also have an implication for services, as it can be common for the diagnosing of BPD to be seen as a negative interaction with service users and carers (Banjeree et al, 2006), possibly due to the historic view of BPD as being ‘untreatable’ (NIMHE, 2003). Our findings, although from a small sample, suggest that service users and carers often don’t hold a negative attitude to BPD, although it is important to take into account that as people self-selected to attend an awareness workshop on BPD they may already have more positive attitudes than most.
Flexibility of delivery Due to the nature of the ‘pilot’ project the delivery of the workshops was malleable. A need was identified early in the project for a carers only workshop, and so an additional workshop for that group was included in the timetable. It was important to be flexible and adapt to need, to ensure that the workshops were as effective as possible and able to help the people they intended to reach.
The feedback from the participants that attended the carers only workshop was positive. However, more notice of the workshop may have helped to increase attendance. It may also be necessary to use additional methods of advertising the workshop as the results show most heard about the workshop via the service users they attended with. Advertising to a wider range of people who are not classified as formal carers, directly targeting carer support workers, or via an external agency such as Somerset Carers Network may aid in this. As well as adding the carers only workshop a further adaptation to the workshops was the addition of the question regarding empathy on the e-KALM measure. This allowed for information to be gathered regarding any potential differences in self-reporting of levels of empathy towards people with BPD by participants post workshop. Interpretation of results is limited as the item was added part way through the project but results from those who did answer provide information that can be followed up in future workshops.
It was also important to provide flexibility within the delivery of the workshops themselves. Adapting the content of the session to individuals and using their experiences to explain and elaborate on the information provided not only aimed to aid learning but also to help provide a validating environment. Validation is important to encourage people to trust their own emotional and cognitive responses as valid interpretations of events (Golan 2012), particularly pertinent in the treatment of BPD.
Inclusion The workshops appeared to provide an invaluable forum for service users and carers to share experiences, and gain a sense of inclusion. This experience of a sense of

29 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
universality and cohesiveness helps them to realise that they are not alone in their experience of the illness and recovery process (Tantillo, 2006). The inclusion of service users and carers in the same workshop may allow them to become more open to difference, that is, different feelings, concerns, and perspectives of others. This may help create mutual relationships with one another and empower them to ultimately aid recovery (Miller & Stiver, 1997).
Conclusion The workshops provided a validating and safe learning environment which allowed for service users and carers alike to learn more about BPD. Service users and carers greatly appreciated the opportunity to meet others in a similar situation to themselves and share experiences. A longer period of notice of the workshops available may aid the self-referral process and central venues for greater access should allow for greater attendance. The shared experience seemed to offer reassurance to service users and carers, and a sense that learning about BPD is the beginning of a journey of self-discovery. There was a sense of relief in each group which we might attribute to being understood and heard by the group, in turn leading to attendees thinking about their own individual needs and planning what they might each do after the group to take the next step forward in the process of treatment or change.

30 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Recommendations
1. It would be recommended to continue to deliver the awareness workshops to service users and carers, using the following format:
Continue to hold 1 day workshops to both service users and carers
Maintain self-referral to the workshops
Maintain the content and flexible, personal delivery of the workshops
Deliver in localities across Somerset that have the greatest access- Taunton, Bridgwater, Glastonbury/Frome and Yeovil
Advertise workshops at least 2 months in advance of workshop date to maximise attendance
Plan for fewer workshops across a longer period of time, such as 4-8 over the year
Recruit a third trainer for back-up in case of trainer absence
2. Complete a follow up measure with participants to ascertain any changes they made post workshop or any perceived longer term effects of the workshop.
3. Share report with carer support services within the Trust to help understand the needs of carers/family and friends of those with BPD. 4. Contribute findings to the development of Mental Health Awareness training initiatives within the Trust.
5. Provide top up training for front line Primary and Secondary Care staff in the Relational Recovery Approach.

31 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Actions
1. Confirm funding for continued delivery of workshops
2. Arrange trainers and venues for the workshops, and advertise well in advance of planned dates
3. Devise follow up questionnaire and contact previous participants to gain feedback on any perceived longer term effects of the workshop
4. Liaise with Carer Support Service to discuss further support for carers
5. Share findings with Integration Phase II project manager regarding development of Mental Health Awareness training for staff.
6. Run Relational Recovery Training to capture for staff in the Trust who have not yet received this

32 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
References
Banerjee, P., Duggan, C., Huband, N., & Watson, N.(2006). Brief psychoeducation for people with personality disorder: A pilot study.Psychology and Psychotherapy: Theory, Research and Practice, 79/3 (385-394), 1476-0835;2044-8341.
Bolton, W., Feigenbaum, J., Jones, A., Sims, A. & Woodward, C. Development of the PD-KASQ. In preparation.
Brown, N. W (2011). Psychoeducational Groups. Process and practice. Third edition. Routledge.
Colom, F., Vieta, E., Sánchez-Moreno, J., Martínez-Arán, A., Torrent, C., Reinares, M., Goikolea, J. M., Benabarre, A. & Comes, M. (2004). Psychoeducation in bipolar patients with comorbid personality disorders. Bipolar Disorders 6 (4), 294–298. DOI: 10.1111/j.1399-5618.2004.00127.
Department for Health (1997).The Patients' Charter for Mental Health Services.
Donker, T., Griffiths, K. M., Cuijpers. P & Christensen, H (2009). Psychoeducation for depression, anxiety and psychological distress: a meta-analysis. BMCMedicine 2009, 7:79. doi:10.1186/1741-7015-7-79
Golan, M. (2012). Eating Disorders Treatment: An Integrative Model by Means of Narrative Counseling, Motivational Interviewing, and Traditional Approaches, Relevant topics in Eating Disorders, Prof. Ignacio Jáuregui Lobera (Ed.), ISBN: 978-953-51-0001-0. Gordon, C 2008. Making Contact: A report on direct consultations with Service Users and Carers of people who attract the diagnosis of Personality Disorder in Somerset. Somerset Partnership NHS Foundation Trust.
Gregory, R. J., Schwer Canning. S., Lee. T., & Wise, J. C. (2004). Cognitive Bibliotherapy for Depression: A Meta-Analysis. Professional Psychology: Research and Practice, 35(3), 275-280. doi: 10.1037/0735-7028.35.3.275
Khoshknab, F.,M, Sheikhona, M., Rahgouy, A., Rahgozar, M., Sodagari, F. (2013). The effects of group psychoeducational programme on family burden in caregivers of Iranian patients with schizophrenia.Journal of Psychiatric & Mental Health Nursing, DOI: 10.1093/brief-treatment/mhh019.
Lukens, E. P., & McFarlane, W, R. (2004) Psychoeducation as Evidence-Based Practice: Considerations for Practice, Research, and Policy. Brief Treatment and Crisis Intervention 4:205-225. Martire, L. M., Lustig, A.P., Schulz, R., Miller, G. & Helgeson, V. S. (2004). Is It Beneficial to Involve a Family Member? A Meta-Analysis of Psychosocial Interventions for Chronic Illness. Health Psychology, 23(6), 599-611. doi: 10.1037/0278-6133.23.6.599
Miller, J, B., & Stiver, I, (1997). The Healing Connection. Beacon Press.

33 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
National Institute for Mental Health in England (2003).Personality disorder: No longer a diagnosis of exclusion. Policy implementation guidance for the development of services for people with personality disorder. NICE Guidelines Borderline Personality Disorder (CG78). Borderline personality disorder: treatment and management. Clinical guidelines, CG78 - Issued: January 2009.
Rentrop, M., Reicherzer, M., Schwerthoffer, D., Bauml, J., & Horz, S. (2012). Psychoeducation for patients with borderline personality disorder and their relatives. Munich model: overview and theoretical background. Psychotherapeut, 57 (4), 291-300. 0935-6185;1432-2080.
Tantillo, M. (2006). A Relational Approach to Eating Disorders Multifamily Therapy Group: Moving From Difference and Disconnection to Mutual Connection. Families, Systems, & Health. 24,1, 82–102. DOI: 10.1037/1091-7527.24.1.82. Zanarini, M.C., Frankenburg, M.D. (2008) A premilimnary, randomized trial of psychoeducation for women with borderline personality disorder. Journal of personality disorders (22) 284-290.

34 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendices
Appendix 1. Awareness Workshops proposal.
The training will be targeted at the following groups:
Adult Service Users with Personality Disorder and their Carers Mothers with Borderline Personality Disorder Emerging Personality Disorder
The training will include the following modules:
Module 1 – Diagnosis o Historical development o Definitions o Comorbidity
Module 2 – Aetiology o Causes & triggers o Resilience
Module 3 – Treatment o Availability o Expectations
Module 4 – Reciprocal Relationships o Service users and service providers
The contents will be based upon Attachment theory, psychological mindedness, recovery principles and NICE guidelines
The content and delivery of the training will need to be sensitive to the target audience, detailed enough to be meaningful yet not too detailed to be traumatic particularly the aetiology with its association to childhood loss, neglect and trauma. Consideration of the duration of the workshops and any additional support will be required.
Strong collaboration is essential with direct service user involvement and consultancy with an external service user led organisation (Emergence)
Two options for the method of delivery have been suggested:
A one-day workshop including all modules Two half day workshops including Modules 1 & 2 and Modules 3 & 4.

35 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 2. Agenda for the BPD Awareness Workshops
Borderline Personality Disorder Awareness Workshop
Agenda
09:30am tea/coffee and signing in for the day
09:45 Brief overview of the day and facilitator introductions
Confidentiality and Contract
Facilities in venue and comfort breaks
Keeping safe
Evaluation form 1
10:00 Attitudes towards Borderline Personality Disorder
10:15 Diagnostic classification and self identification
Personality development and Attachment
11:00 Break
11:20 Why Do I have BPD? Understanding myself
12.0 Construction using tools, Map, seeking advice and help
12:30 Lunch
13:20 Reflection
14:00 How many people have BPD?
14:30 Getting help and making changes
14:45 Break
15:00 Making a plan for the future
15:15 Group feedback and discussion about the day.
15:15 Ending our day and saying goodbye
Filling in feedback forms on the day
Evaluation form 2.
15:30 End of the workshop

36 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 3. e- KALM Questionnaire.
Name: Date:
Str
on
gly
d
isag
ree
Dis
agre
e
Un
cert
ain
Ag
ree
Str
on
gly
agre
e
1. I have a good knowledge of the diagnosis of borderline personality disorder.
1 2 3 4 5
2. I have a good understanding of how Borderline Personality Disorder develops.
1 2 3 4 5
3. I have a good understanding of why I, or the person I care for, self harms or may behave in self-destructive ways.
1 2 3 4 5
4. I have a positive view of Borderline Personality Disorder. 1 2 3 4 5
5I have a positive attitude towards people with BPD. 1 2 3 4 5
6 I feel confident that I can make a positive impact on caring for myself or caring for someone with BPD.
1 2 3 4 5
7. I am aware of the options available to me in terms of treatment or support.
1 2 3 4 5
8. I think I am able to make positive changes in my life or someone else’s life.
1 2 3 4 5
9. I have empathy towards people with BPD. 1 2 3 4 5
Thank you for taking the time to fill out the questionnaire.

37 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 4. Workshop Evaluation Form
Thank you for your participation in the Borderline Personality Disorder Awareness Workshop. We would welcome your feedback on the usefulness and quality of the workshop. We would appreciate your honest views of the following areas:
(Questions:) 1. What were your impressions of the standard of this workshop and of the trainers? (please comment)
2. Was the information about Borderline Personality Disorder and the treatments available relevant to you?
3. What was the most helpful or useful thing you learned today, if anything? 4. What did you find least helpful about the day, if anything? 5. Do you think you might change anything you do as a consequence of what you learned on the workshop?
6. Were the workshop handouts helpful?
7. How was the length of the workshop, refreshments, venue, access etc.
8. Would you recommend this training to other people you know who may have BPD or their carers?
9. What is your experience of staff attitudes toward BPD?
10. Any further comments or suggestions?
Name: …………………….
(please leave blank if you wish the information to be anonymous)
Thank you for taking the time to fill out the questionnaire.

38 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 5. Costings Table. Estimated expenditure to run one workshop, including preparation:
Cost
2 days Band 4 Assistant Psychologist £100
1.5 days Band 7 CAT Therapist £130
room hire (if needed) £100
Refreshments £25
training materials £40
existing resources- lap top, projector £0
Total (excluding venue)
£395 £295
39 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 6. Self Identification Wheel

40 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014

41 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
Appendix 7. Service evaluation proposal
SURVEY PROPOSER: Clare Carter DIRECTORATE/SERVICE/ TEAM: Personality Disorder Service
SURVEY SUPERVISOR: Theresa Sired, Chris Gordon Relationship to Proposer: Manager
SURVEY TITLE: Evaluation of Borderline Personality Disorder Awareness Workshops
SURVEY/EVALUATION OBJECTIVE(S)
To evaluate the effectiveness of BPD awareness workshops for service users and carers ETHICS SCREENING LIST – Does the survey/evaluation (delete whichever does not apply): 1. Infringe any patient’s rights or risk breaching any
patient’s or carer’s confidentiality or privacy? No 6. Allocate any interventions differently among groups
of patients or staff? No
2. Pose any risk for or burden on a patient beyond those of his or her routine care?
No 7. Is there anyone involved with the survey who does
not normally have access to patient’s records or information?
No
3. Involve any clinically significant departure from usual clinical care?
No 8. Collect data directly from any patient or carer? Yes
4. Gather any information about a patient or carer beyond that collected in routine patient care?
Yes
5. Report any data that could be used to identify any patient or practitioner? No
8b. If Yes, could the study subject a patient or carer to more than minimal burdens or risks it if is time consuming or requests sensitive information?
No

42 Somerset Partnership NHS Foundation Trust, Personality Disorder Service July 2014
WORK PLAN
Planned date: Planned date: 1. Start by: 7th October 2013 3. Data analysed by: March 2014 2. Data collected by: January 2014 4. Report completed by: March 2014
5. Report to be submitted to: Chris Gordon
HELP NEEDED
Is help or support from any other department or service needed to complete the survey? No If yes, describe whose help is needed and the nature of the help:
PLANNED METHODOLOGY (eg. No. of clients, cases, episodes, instances and/or time period to survey. Attach any proposed questionnaires)
A number of one day workshops held across the Trust for service users and carers.
Maximum of 12 participants per workshop to include service users, service user carers (informal and formal) recruited from internal advertising only
We currently have 6 workshops planned, but this may increase to no more than 10 with the final workshop being no later than end of December 2013.
Participants complete a small questionnaire at the start and end of the day regarding their knowledge and attitudes about BPD. Please see attached the questionnaire.
At the end of the workshop we also gather general feedback from the day. Please see attached.