espen congress gothenburg · pdf fileshould insulin be added to parenteral nutrition? jay m...
TRANSCRIPT
Should Insulin be added to Parenteral Nutrition?
Jay M Mirtallo
ESPEN Congress Gothenburg 2011
Educational Session - Pharmaceutical session (in collaboration with ASPEN)
Should Insulin be added to Parenteral Nutrition?
Jay M Mirtallo, MS, RPh, BCNSP, FASHP Associate Professor of Clinical Pharmacy The Ohio State University, College of Pharmacy Pharmacy Practice and Administration Division President, The American Society for Parenteral and Enteral Nutrition
Insulin Indications for PN
Manage hyperglycemia
Protein accretion (anabolism)
Anti-inflammatory activity
Insulin in PN: Outline
Indication: Manage Hyperglycemia
Frequency of hyperglycemia in PN patients
Association of adverse outcomes with hyperglycemia in PN patients
Variables associated with poor glucose control in PN patients
Issues with insulin in PN
Criteria for adding medications to PN
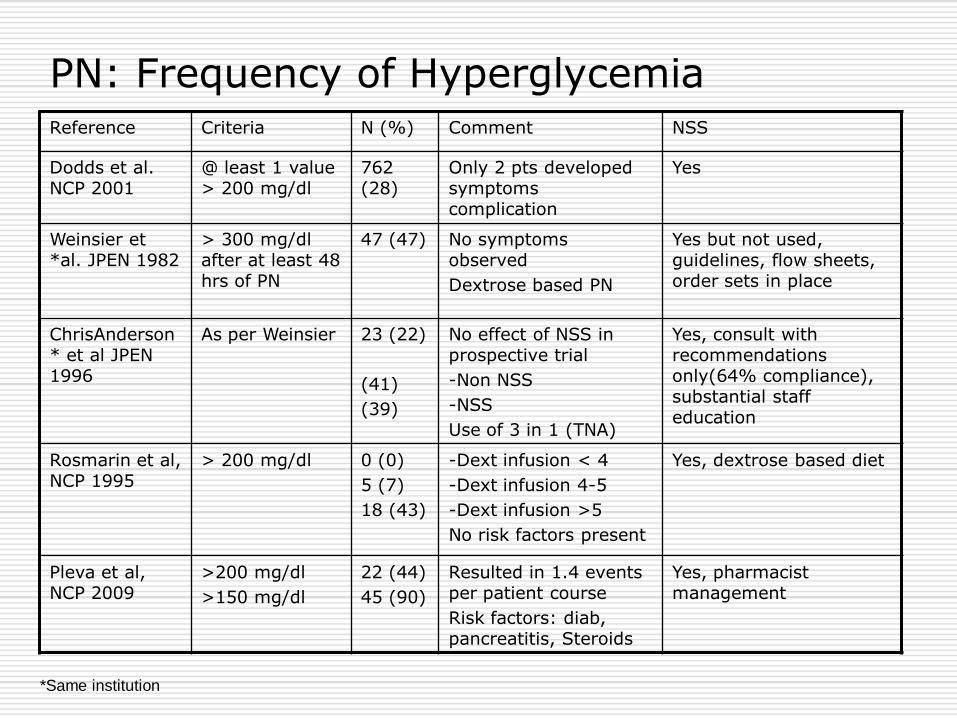
PN: Frequency of Hyperglycemia Reference Criteria N (%) Comment NSS
Dodds et al. NCP 2001
@ least 1 value > 200 mg/dl
762 (28)
Only 2 pts developed symptoms complication
Yes
Weinsier et *al. JPEN 1982
> 300 mg/dl after at least 48 hrs of PN
47 (47) No symptoms observed
Dextrose based PN
Yes but not used, guidelines, flow sheets, order sets in place
ChrisAnderson* et al JPEN 1996
As per Weinsier 23 (22)
(41)
(39)
No effect of NSS in prospective trial
-Non NSS
-NSS
Use of 3 in 1 (TNA)
Yes, consult with recommendations only(64% compliance), substantial staff education
Rosmarin et al, NCP 1995
> 200 mg/dl 0 (0)
5 (7)
18 (43)
-Dext infusion < 4
-Dext infusion 4-5
-Dext infusion >5
No risk factors present
Yes, dextrose based diet
Pleva et al, NCP 2009
>200 mg/dl
>150 mg/dl
22 (44)
45 (90)
Resulted in 1.4 events per patient course
Risk factors: diab, pancreatitis, Steroids
Yes, pharmacist management
*Same institution
PN and Hyperglycemia: Adverse Outcomes
Relation between blood glucose levels and outcomes
Myocardial infarction
Stroke
Cardiothoracic surgery
Critical illness
General hospitalized patients
Cheung NW et al Diabetes Care 2005; 28: 2367-2371
PN and Hyperglycemia: Adverse Outcomes
Risk of any complication 1.58 (p <0.01)
Infection
Septicemia
Acute renal failure
Cardiac complications
Death
Quartile analysis
Risk level increased at high quartile vs low quartile group
OR of 4.3 for complication, 10.9 for death
Cheung NW et al Diabetes Care 2005; 28: 2367-2371

Severity of Hyperglycemia
Stronger predictor of adverse outcomes than history of diabetes
Majority of PN patients who become hyperglycemic are not diabetic
Excluded from Rosmarin study
12% of Pleva study population
27% of Wah Cheung study population
Evidence that hyperglycemia in itself is harmful.
Cheung NW et al Diabetes Care 2005; 28: 2367-2371
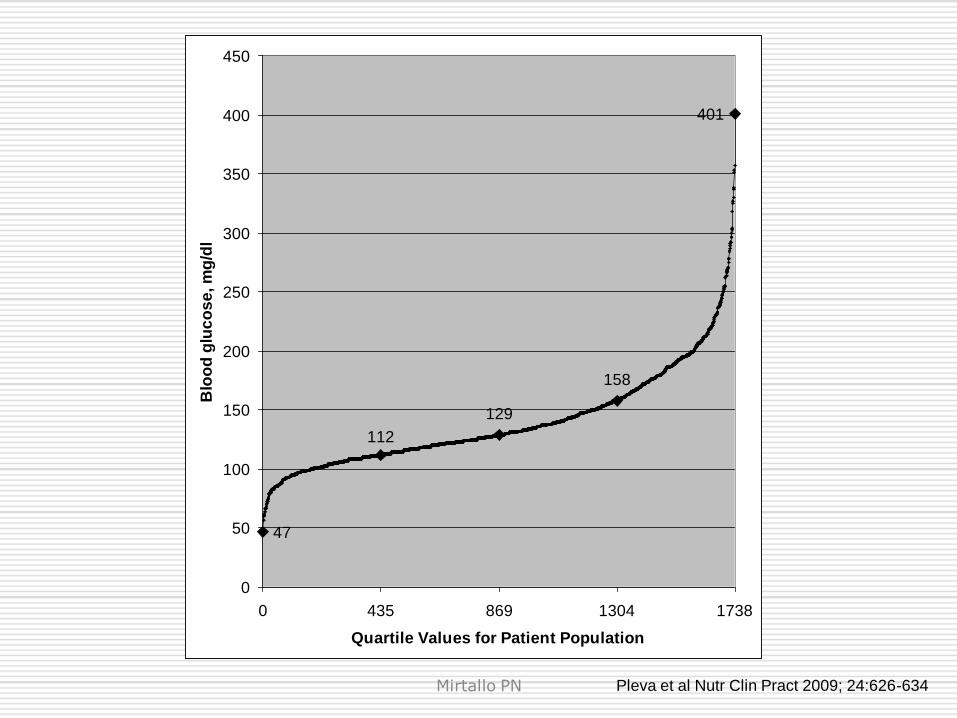
47
112
129
158
401
0
50
100
150
200
250
300
350
400
450
0 435 869 1304 1738
Quartile Values for Patient Population
Blo
od
glu
co
se
, m
g/d
l
Mirtallo PN Pleva et al Nutr Clin Pract 2009; 24:626-634

Variables Associated with PN Hyperglycemia
Caloric dose
Type of calorie provided
„Hidden‟ Sources of CHO
Target glucose range
Impact of controlling glucose to this range
Responsibility for glucose management
Use of sliding scale insulin
FEAR of hypoglycemia

Variables Associated with PN Hyperglycemia
No one method known to be effective in achieving target glucose
Lack of consensus for insulin use Long-acting insulin Sliding scale insulin Insulin drip Insulin in PN Any combination of the above
Practice varies widely among patient populations, disciplines and individual clinicians
Overall, management of hyperglycemia is most important Interdisciplinary nutrition care
Experience and skill of staff managing PN View as a process
Insulin in PN
Criteria for medications added to PN
Stable and compatible
Evidence supports clinical value of medication administered in PN
Frequency of dosage adjustment no more than every 24 hours
Insulin is associated with frequent harmful events in PN
Mirtallo et al. JPEN 28 (suppl) S39-S70, 2004

Management of Hyperglycemia: Alternative to Insulin-Hypocaloric PN
Reference Criteria Comment
Choban PS et al Am J Clin Nutr 1997
Hypocaloric 75 Cal:g nitrogen
Normal 150 Cal: g nitrogen
2 g Pro/kg IBW/d
Obese patients
12 pts received insulin (11/12 diabetic)
Less insulin days in NIDDM hypocaloric group
McCowen KC et al Crit Care Med 2000
Study: 1000 kcal, 70 g pro
Control: 25 kcal/kg, 1.5 g/kg pro
No difference in
Frequency of hyperglycemia – non diabetics
insulin use
Average glucose
worse nitrogen balance in hypocaloric group
Ahrens CL et al Crit Care Med 2005
Low Cal: 20 NPC/kg/d
Standard Cal: 30 NPC/kg/d
Excluded underweight/morbid obese
Used sliding scale insulin
Insulin in PN if >50% values > 200
Fewer hyperglycemic events and lower severity
Mean glucose lower (118 vs 172)

Insulin Availability from PN
Range: 10-95%
Composition of PN
Lipids, trace elements, vitamins
Final concentration of insulin
Assay for insulin
Laboratory simulation of clinical practice
Adequate monitoring of patient clinical response
Seres DS; NCP 1990;5: 111-116
Evidence Supporting Insulin Use
Diabetic Patients
Pre hospital insulin dose Reduced daily dextrose dose to start
100 g – Type 1 150 g – Type 2
Accept modest hyperglycemia to avoid hypoglycemia Sliding scale insulin: glucose > 250
Mean glucose around 200 mg/dl No hypoglycemic episodes
Insulin in PN Significant calories from enteral nutrition or tube feeding
Insulin separate from PN
Source of dextrose determines route of insulin Dialysis
Hongsermeier T et al. JPEN 17:16-19, 1993
Evidence Supporting Insulin Use: Insulin protocol
NSS: primarily pharmacist Capillary Blood glucose (CBG) every 6 hrs Criteria: glucose > 140 mg/dl
Insulin dose per g Carbohydrate (CHO) PN induced hyperglycemia
1 U/20 g CHO Diabetes/glucocorticoids
CBG <11.1 mmol/L (200 mg/dl) 1 U/10 g CHO + 0.15 U/kg/d
CBC > 11.1 mmol/L 1 U/5 g CHO + 0.25 U/kg/d
2/3 insulin dose in PN, 1/3 separate as long-acting insulin
Jakoby MG et al. JPEN @
http://pen.sagepub.com/content/early/2011/08/06/0148607111415628

Evidence Supporting Insulin Use: Insulin protocol
Mean CBG < in protocol group by 21 mg/dl
Higher CBG in diabetic group but better control with protocol
Hypoglycemia (CBG < 80)
more frequent in protocol group (3 vs 1%)
No episodes of severe hypoglycemia (CBG < 40)
Jakoby MG et al. JPEN @
http://pen.sagepub.com/content/early/2011/08/06/0148607111415628
Evidence Supporting Insulin Use: Computer-assisted, Critically Ill
Nurse centered computerized decision support for insulin administration “step-up” rule
Graded increases in amount of PN administered For glucose < 10 mmol/L (180 mg/dl)
End-point: achieve full PN at 24 hours along with glucose control during introduction period Goal: 25 kcal/kg/d, max = 2500 kcal
Use of insulin drip Desired caloric intake achieved within 24 hr Glucose levels
6.6 (119 mg/dl) to 7.6 (137 mg/dl) mmol/L (ave – 7.4 (133))
Insulin drip rate of 1.1-2.0 U/h
Hoekstra M et al. JPEN 34: 549-553. 2010
Should Insulin be Added to PN? It depends
Critically ill: separate insulin infusion (drip)
Significant calories from enteral or tube feeding: separate insulin as sliding scale or long-acting Minimize „Hidden‟ sources of glucose
Others: definitely use insulin in PN Evidence that better than using sliding scale insulin
Reasonable glucose control with minimal hypoglycemia
Consider insulin dose per gram of carbohydrate in PN Adjust dose daily with sliding scale insulin
2/3 previous days insulin dose
Systems Issues
Establish target glucose
Interdisciplinary involvement
Assign responsibility for glucose control
Provide algorithm or protocol to follow
Evaluate success in achieving target glucose values

A.S.P.E.N. Guideline
Insulin use in PN should be done in a consistent manner according to a method that healthcare personnel have adequate knowledge
Mirtallo et al. JPEN 28 (suppl) S39-S70, 2004
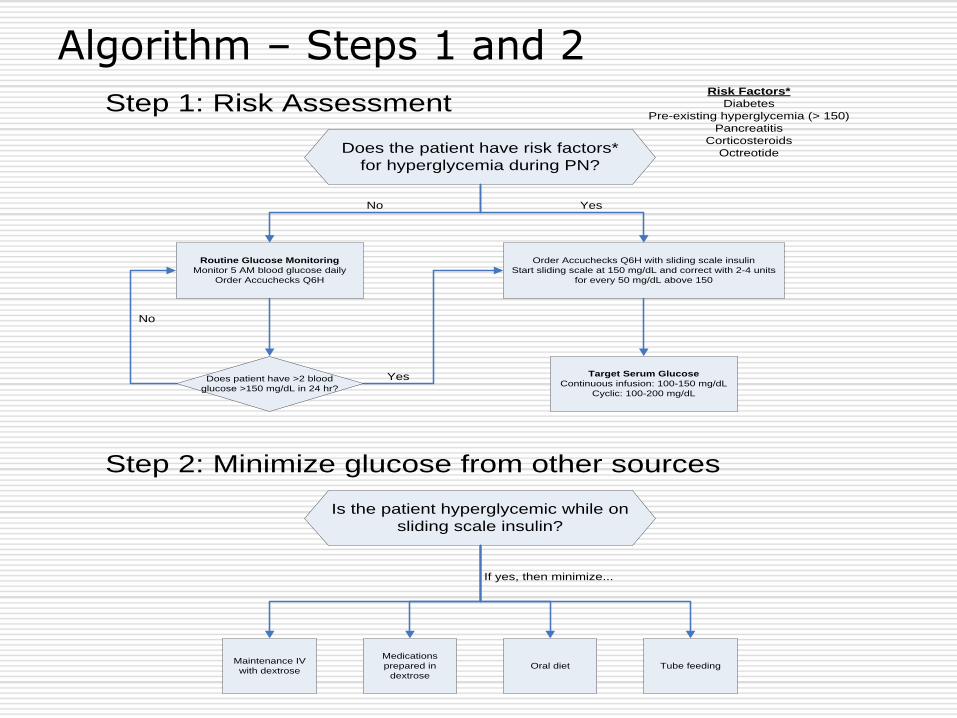
Algorithm – Steps 1 and 2
Does the patient have risk factors*
for hyperglycemia during PN?
Risk Factors*
Diabetes
Pre-existing hyperglycemia (> 150)
Pancreatitis
Corticosteroids
Octreotide
Routine Glucose Monitoring
Monitor 5 AM blood glucose daily
Order Accuchecks Q6H
Target Serum Glucose
Continuous infusion: 100-150 mg/dL
Cyclic: 100-200 mg/dL
Step 1: Risk Assessment
Order Accuchecks Q6H with sliding scale insulin
Start sliding scale at 150 mg/dL and correct with 2-4 units
for every 50 mg/dL above 150
YesNo
Does patient have >2 blood
glucose >150 mg/dL in 24 hr?
No
Yes
Step 2: Minimize glucose from other sources
Maintenance IV
with dextrose
Medications
prepared in
dextrose
Oral diet Tube feeding
Is the patient hyperglycemic while on
sliding scale insulin?
If yes, then minimize...
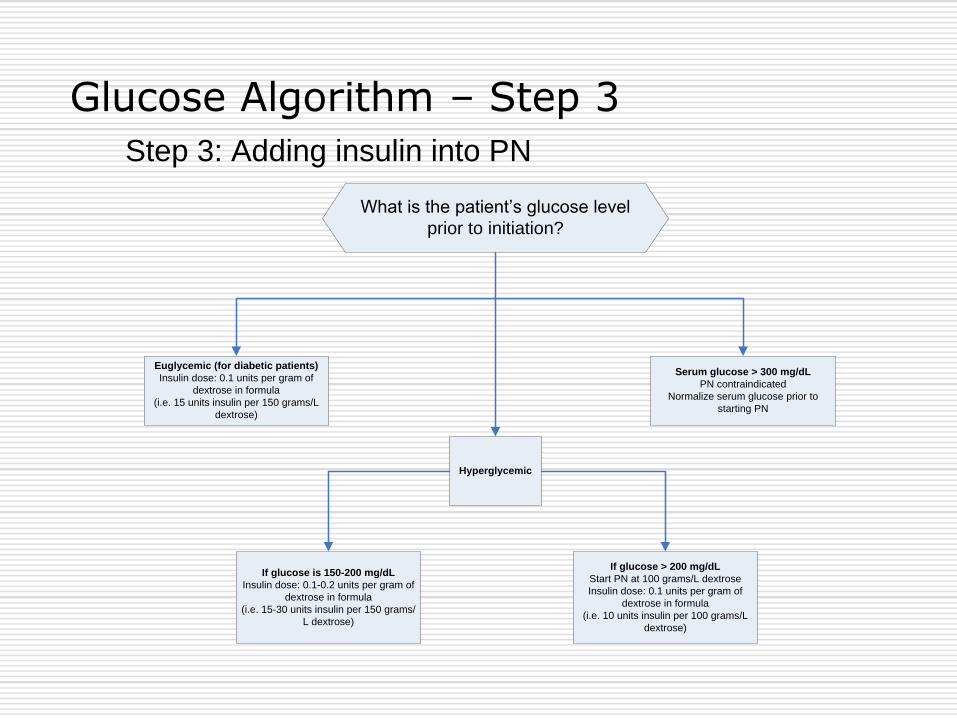
Glucose Algorithm – Step 3
Step 3: Adding insulin into PN
What is the patient’s glucose level
prior to initiation?
Euglycemic (for diabetic patients)
Insulin dose: 0.1 units per gram of
dextrose in formula
(i.e. 15 units insulin per 150 grams/L
dextrose)
If glucose > 200 mg/dL
Start PN at 100 grams/L dextrose
Insulin dose: 0.1 units per gram of
dextrose in formula
(i.e. 10 units insulin per 100 grams/L
dextrose)
Serum glucose > 300 mg/dL
PN contraindicated
Normalize serum glucose prior to
starting PN
Hyperglycemic
If glucose is 150-200 mg/dL
Insulin dose: 0.1-0.2 units per gram of
dextrose in formula
(i.e. 15-30 units insulin per 150 grams/
L dextrose)

Glucose Algorithm – Step 4 Step 4: Insulin monitoring
Monitor Q6H Accuchecks
Is the patient’s blood glucose within
goal range?
Continue current insulin regimen
Adjust insulin in PN by adding 75% of
insulin dose used via sliding scale in
previous 24 hours
Increase PN to goal rate
When glucose is controlled at 40 mL/hr
Monitor Q6H Accuchecks
Is glucose within range?
Monitor Q6H Accuchecks
Is glucose within range?
Monitor Q6H Accuchecks
Is glucose within range?
Increase PN to goal rate
When glucose is controlled at 40 mL/hr
Yes No
Yes
No
Yes
No
Yes
Adjust insulin in PN by adding 75% of
insulin dose used via sliding scale in
previous 24 hours
No
Glucose Algorithm - Notes
PN may be cycled if glucose is controlled on continuous PN while at goal rate
Taper insulin in PN when glucose < 100 mg/dL for 3 of 4 Accuchecks in a 24-hr period
Insulin limit in PN is 60 units/L.
If patient needs more insulin, then discontinue insulin in PN and begin insulin drip.

Summary
The use of insulin in PN is a controversial topic Primary indication: hyperglycemia
associated with PN
Original issues with bioavailability from PN
Little evidence evaluating outcomes of insulin use in PN
Considerable variability in types of patients and PN practices

Conclusion
Evidence and clinical practice suggests insulin is clinically effective in PN when dosage adjustments are suitable on a daily basis
References
Shizgal HM, Posner B. Insulin and the efficacy of total parenteral nutrition. Am J Clin Nutr 50:1355-63, 1989.
Cheung NW, Zaccaria C, Napier B, Fletcher JP. Hyperglycemia is associated with adverse outcomes in patients receiving total parenteral nutrition. Diabetes Care 28:2367-2371, 2005
Dodds ES, Murray JD, Trexler KM, Grant JP. Metabolic occrurences in total parenteral nutrition patients managed by a nutrition support team. Nutr Clin Pract 16:78-84, 2001
Weinsier RL, Bacon J, Butterworth CE. Central venous alimentation: a prospective study of the frequency of metabolic abnormalities among medical and surgical patients. J Parenter Enter Nutr 6: 421-425, 1982
ChrisAnderson D, Heimburger DC, Morgan SL et al. Metabolic complications of total parenteral nutrition: effects of a nutrition support service. J Parenter Enter Nutr 20:206-210, 1996
Rosmarin DK, Wardlaw GM, Mirtallo J. Hyperglycemia associated with high, continuous infusion rates of total parenteral nutrition. Nutr Clin Pract 11:151-156, 1996
Pleva M, Mirtallo JM, Steinberg SM. Hyperglycemic events in non-intensive care unit patients receiving parenteral nutrition. Nutr Clin Pract 24: 626-634, 2009
Mirtallo J, Canada T, Johnson D, et al. Safe practices for parenteral nutrition. J Parenteral Enter Nutr 28 (suppl):S39-S70, 2004
Choban PS, Burge JC, Scales D, Flancbaum L. Hypoenergetic nutrition support in hospitalized obese patients: a simplified method for clinical application. Am J Clin Nutr 66:546-550, 1997
McCowen KC, Friel C, Sternberg J, et al. Hypocaloric total parenteral nutrition: effectiveness in prevention of hyperglycemia and infectious complications – a randomized clinical trial. Crit Care Med 28:3606-3611, 2000
Ahrens CL, Barietta JF, Kanji S et al. Effect of low-calorie parenteral nutrition on the incidence and severity of hyperglycemia in surgical patients: a randomized, controlled trial. Crit Care Med 33:2507-2512, 2005\
Seres DS, Insulin adsorption to parenteral infusion systems: case report and review of the literature. Nutr Clin Pract 5:111-117, 1990
McMahon MM. Management of parenteral nutrition in acutely ill patients with hyperglycemia. Nutr Clin Pract 19:120-128, 2004
Hongsermeier T, Bistrian BR. Evaluation of a practical technique for determining insulin requirements in diabetic patients receiving total parenteral nutrition. J Parenter Enter Nutr 17:16-19, 1993
Jacoby MG, Nannapaneni N. An insulin protocol for management of hyperglycemia in patients receiving parenteral nutrition is superior to ad hoc management. J Parenter Enter Nutr accessed August 17, 2011. avaialble at: http://pen.sagepub.com/content/early/2011/08/06/0148607111415628
Hoekstra M, Schoorl MA, Iwan CC, et al. Computer-assisted glucose regulation during rapid step-wise increases of parenteral nutrition in critically ill patients: a prood of concept study. J Parenter Enter Nutr 34:549-553, 2010