espen congress copenhagen 2016 · espen congress copenhagen 2016 the nutrition support team:...
TRANSCRIPT

NUTRITION SUPPORT TEAMS: CLINICAL PRACTICE
K. Boeykens (BE)
ESPEN Congress Copenhagen 2016THE NUTRITION SUPPORT TEAM: 'TWO AND TWO EQUALS FIVE'

Nutrition Support Team
AZ Nikolaas- Belgium
Kurt Boeykens
CNNS

Learning objectives
• Nutrition support teams: Clinical practice
• Be able to illustrate through clinical practice
examples how a NST can enhance
(nutritional) patient care
• Understand how nutritional care can be
brought to a higher level with a intensified
multidisciplinary approach
2

3
2006

NST
• The multiprofessional team of physician, specialist nurse,
dietitian and pharmacist can do much to co-ordinate the
nutritional function of ward nurses, ward dietitians, ward
pharmacists and other physicians in the delivery of an
organized nutritional strategy.
• AZ Nikolaas:
• Specialist nurse(s): 2 (one = co-ordinator NST)
• Dietician(s): team
• NS pharmacist(s): 3 (TPN)
• NS physician: 1 (GE)
6

The roles in a NST
7

8
NS Dietician
NS Pharmacist
NSN
NS Physician

MD ward rounds
• Started weekly
• Selected patients (TPN, complex EN, ICU)
• Ad hoc
• Telephones daily:
• Pharmacy-dieticians-NSN-Speech therapists-
physicians
9

Liaison
10

Intramural liaison
• Dietetics
• Pharmacy
• Nursing teams
• Nursing management
• Lab
• Physicians
• Endoscopy
• PST/OST
• GST
• Diabetic team
• Radiology
• Consultations
• Social services
• ICT
11

Extramural liaison
• Home care providers
• General physicians
• Home care nurses
• Home NST
• Patient organizations
• Insurance companies
• Nutrition companies
• Nutrition societies
• Government
• Expert/workgroups
• Discussion forums
12

Steering Committee
• General advise and discussion on all aspects of nutrition in the hospital = POLICY
• Members of different departments• Hospital staff: nursing director, medical director
• Head dietician
• NS pharmacist (1) and head pharmacist
• Speech therapist
• Medical staff
• NS physician
• CNNS (co-ordinator NST)
• Meeting every 3-4 months

How did we start?
1. Who took the initiative?
2. Setting priorities: ‘road map’
3. First act?
4. Financial support

Initiative
• 2000
• Gastroenterologist
• Nutritional education/background/interest
• After ‘diplomatic survey’:
• dieticians
• ‘hotel manager’
• nursing director
• some surgeons, intensivists, physicians

Priorities
• Appointment of a CNNS/NSN
• Co-ordinator
• Establish Steering Committee and NST
• Road Map: education, protocols, qualityprojects, malnutrition pathway,…
• Nutritional benchmarking
• Ex. Use of TPN

• 2000: TPN questionnaire:
• 75 questions on all aspects of TPN
• Head nurses of all nursing departments
• Intentions:
• Introducing the nutrition support nurse
• Collecting data to help persuade management
• Identifying problems
• Tool for quality control

• Feeding line used for other purposes?
4
2
4
5
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
never rarely frequently always
n = 15

19
TPN questionnaire: conclusions
• No protocols or standards
• Every ward has its own ‘traditions’
• Some intolerable situations!
• Urgent need for protocols and
teaching

Financial support
• Small amount of money from the
government (pilot project NST)
• +/- 20.000 euro’s/year
• CNNS = funded by the hospital
• NST
• Fixed yearly budget for education, special
equipment, quality projects,….
21

Our NST
Translation of nutritional evidene or
care into clinical practise
22

• Specific protocol to identify at risk patients
• Rapid and simple
• Proces of re-screening
• Assessment
• NCP
23
Who was involved?
• Head nurses and ward nurses
• Nutrition reference nurses
• Head nursing departement
• Dietetics
• ICT and private software company
• Quality co-ordinator
24

Step 1
• Task manager: automatic list of all patients
who need a nutrition screening after
admission
25

Step 2
• Full NRS-based and how the patiënt is
measured
26

27
• Disease scores:
• ICU, internal medicine and surgery
• 1,2 or 3 points

Next steps
• Software:
• Generates total NRS score
• Asks for a nutritional assessment (only on the
PC’s of the dieticians, NSN) if NRS ≥ 3
• Asks for a NCP if at risk or malnourished
• Asks for a rescreening after a week
• Food intake, weight
• Transfers data to the individual patient file:
weight, length, BMI and how measured
• Software remembers the length for one year
28


NUTRITION DAY
AZ NIKOLAAS

Goals• Participation in the Worldwide Nutrition Day
• General sensitization for malnutrition in our hospital (main goal).• Intra muros screening of all patients
• Extra muros (press conference, radio, newspapers, television)
• Broad participation of wards and health care workers (nurses, dieticans, doctors, management, kitchen staff…)
• Special activities to support the main action.
• Data collection and analysis

LogoEating better = recovering
quicker
The NST is here for you

BMI measurements hospital staff

Fresh fruit juice

Donuts

Ambiance
2006

Breaking news!

Patients
• Flyer
• Special dessert

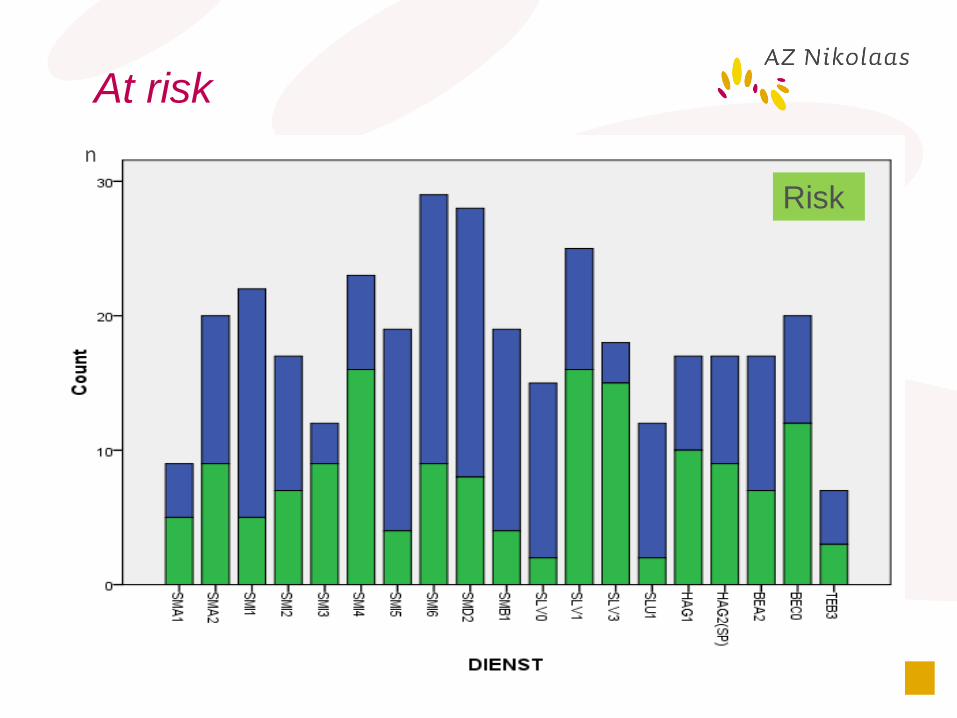
At risk
n
Risk
PEG-placement
From (contra) indications to home
care follow-up
41

Co-ordination by the NST
1. All patients are assessed by the NST
2. Rule out (contra) indications
3. Check-list to prepare patients
4. All PEG’s are placed by the CNNS
5. After care is done/supervised by the
CNNS
6. Transmural care/follow-up (HEN)
42
43
2005

Pre-op assessment
• Identify at risk patients or not suitable patients
• Refer at risk patients to a pre-op consultation (head &
neck cancers)
• Establish proper preparation/information/problem-solving
44

45
2016

After-care
• Database
• Complications, duration (H)EN therapy,
removal technique,….
• Transmural care
• Discharge letter with all aspects of HEN
therapy for home care nurses and physician
or for nursing homes
• Problem-solving
• Telephone, mail or website
46

HPN
47

HPN
48
Baxter

49

50

51

52