eso documentation - amazon s3documentation.pdfeso documentation henderson county rescue squad ems|mc...
TRANSCRIPT

ESO Documentation
Henderson County Rescue Squad
EMS|MC is not responsible for non-EMSMC published content.

Why is proper documentation important?
Your PCR is a PERMANENT medical and legal document.
Your PCR is also THE source on which all medical billing claims are based.
Your PCR helps track compliance.
Your PCR is part of data collection, determining needs for training, successful/unsuccessful
interventions, as well as use of supplies.

Patient Information
Demographic Information: Always verify the correct spelling of pt’s name, DOB, mailing
address, social security number, etc. Just because you pick someone up from a private
residence, does not mean that they receive their mail at the same place.
If there is a previous chart for your pt in ESO, once again, VERIFY the pt’s information. This
includes, PMH, allergies, medication and code status.
PMH, allergies and medications need to be documented for EVERY pt. If the information
cannot be obtained, document the reason.

Documentation Reminders
The ASSESSMENT portion needs to be filled out for EVERY pt. This does not mean every single tab and box needs to be checked. This means what is pertinent to the call. Keep in mind, a pt’s mental status, skin condition, quality of radial pulse and respiratory effort should be documented for every pt. Selecting No Abnormalities means you thoroughly assessed that complaint system and that it is completely normal. Don’t forget that pertinent negatives help paint a clearer picture.
Vital Signs: If an intervention is performed, for example, O2 administration, a set of VS reflecting the SPO2 of the pt prior to O2 administration, and a set of VS reflecting the SPO2 after O2 administration, needs to be obtained and documented.
Flow Chart: All interventions performed by crew need to be added to the Flow Chart. This includes continuation of tx, for example, O2 administration. Interventions performed PTA of crew that are pertinent to the call should be entered in the PTA section of the Flow Chart.

Narrative
Paints a clear picture of call from start to finish. This includes, assessments, interventions,
medications, supplies and equipment.
Contrast between the reason called, or the reason you were told the pt needed to be
transported via stretcher, and your actual findings.
Be sure to clearly state in your narrative why the pt requires a stretcher.
Medicare and Medicaid ONLY receive your narrative and is what reimbursement is based
off of, therefore be sure to clearly document any abnormal VS or findings in your narrative.
BE SPECIFIC, the new ICD 10 codes and training we all received, requires our assessments
and documentation to be very detailed.

ESO
The next slides serve as a guide to help clarify common problems that continue to arise in our
PCR’s.
**This is by no means a comprehensive and complete instruction list.

Incident-Response
o Run Type for convalescent
transports is either Non-
Emergency Interfacility
Transfer or Medical Transport.
If it is a 911 call, Run Type is
911 Emergency, regardless of response priority.
o Leave EMD section empty for
convalescent transports;
EMD is not performed
therefore should not be filled
in.
o EMD section does apply to
911 calls. The EMD Compliant
and EMD Card Number can be found on Mobile CAD.
911 ONLY
12345-67

Incident-Disposition
o If Diverted, or if pt care is
transferred to an ALS unit, etc.
make sure the proper Disposition is
selected.
o Convalescent transports with
medical necessity form, means
the Transport Due To: Physician
and Requested By: Physician.
o Make sure that if diverted, that
the actual destination is filled in,
not the original.

Incident-Additional Factors
o If there are other
responders/agencies on scene
please add them under
Additional Agencies or
Additional responders. This
includes Fire Dept., LEO, EMS,
etc. This applies even if you call
for lift assist!!
o Please include any delays in
the Delays section.
*
*
*

Narrative-Clinical Impression
o For convalescent transports, the
Primary Impression: Other. If you treat the pt for a complaint that
comes up during transport, that
can be entered under Secondary
Impression. For 911 calls, the
Primary Impression is what you believe to be the problem.
o The Chief Complaint for convalescent transports should
be as shown.
o The Supporting Signs/Symptoms section is a good place to
document the pt’s dx/reasons
why they must be transported via
stretcher.

Narrative-Injuries/Other Factors
o If a pt is injured, please fill out
the Injuries section.
o REMEMBER: Trauma isn’t always
an obvious open fx, if someone
complains of pain after a fall,
MVA, etc., that is still a
“Traumatic Injury.”
o The Other Factors section is where you can document any
language barriers,
combativeness, dementia or
altered pts, etc.
o When a pt is injured, please
move on to the Specialty Patientsection.
*

Specialty Patient
o When a pt is injured, the
Trauma Criteria section must be filled out.
o When a pt is injured due
to an MVA, the Motor
Vehicle Collision section must also be filled out
o Also note the other
sections available, in the
event that these
sections apply to your
pt, they must also be
filled out.

Specialty Patient-Trauma Criteria
o Trauma Criteria section applies to ANY ptthat has an injury as their chief complaint.
o Under the Other Risk Factors section, pay
attention to the Age option. Keep in
mind that the Provider Suspicion option when checked is just another way to
save your own back.
o Trauma Activation most times does not apply to our transports. If you transport a
pt to Mission, for example, and they put
your pt in as a trauma alert or code
trauma then there was a trauma
activation. Otherwise, just select No.
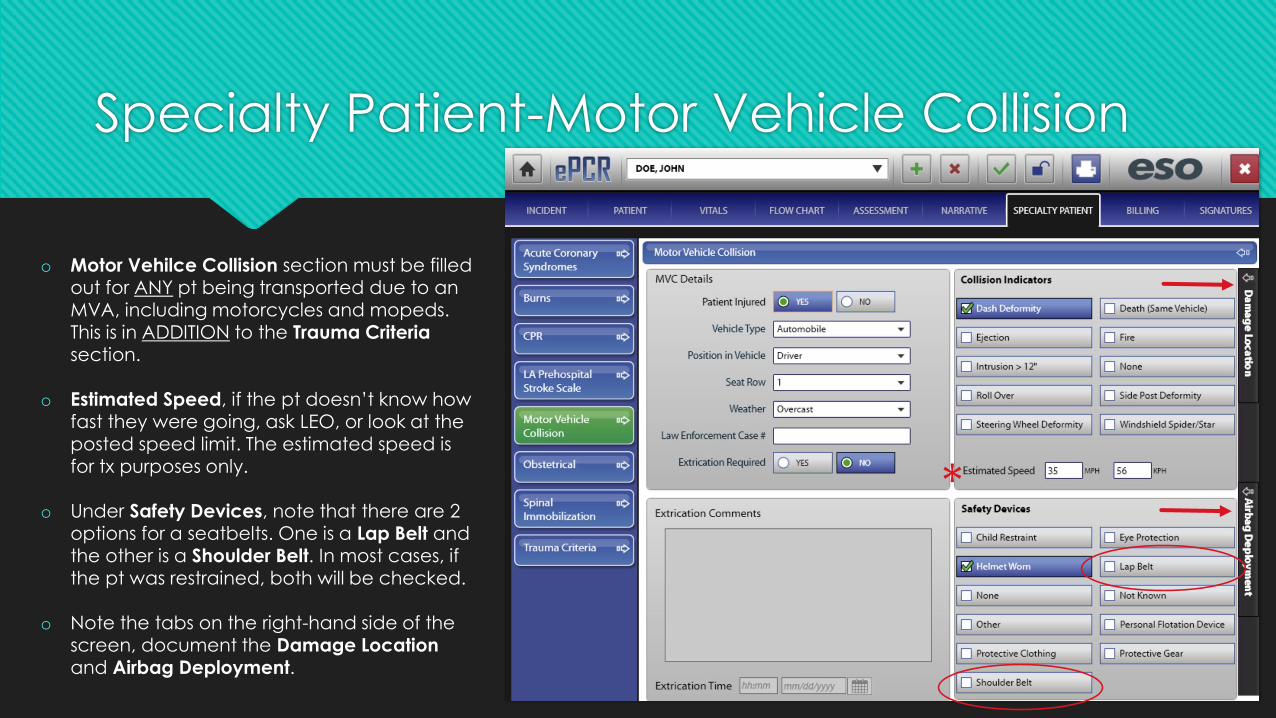
Specialty Patient-Motor Vehicle Collision
o Motor Vehilce Collision section must be filled out for ANY pt being transported due to an MVA, including motorcycles and mopeds. This is in ADDITION to the Trauma Criteriasection.
o Estimated Speed, if the pt doesn’t know how fast they were going, ask LEO, or look at the posted speed limit. The estimated speed is for tx purposes only.
o Under Safety Devices, note that there are 2 options for a seatbelts. One is a Lap Belt and the other is a Shoulder Belt. In most cases, if the pt was restrained, both will be checked.
o Note the tabs on the right-hand side of the screen, document the Damage Location and Airbag Deployment.
*

Loose Ends…
In the Flow Chart an IV that is started should be entered as IV Therapy. There have been numerous IV attempts entered as IV Bolus. An IV Bolus is the act of administering a NS bolus. So if you start an IV and give fluid, both should be listed in your flow chart. Note, if a pt has an INT in place from a facility an EMT-Basic can tech. However, if an EMT-Intermediate deems it necessary to start an IV, then the EMT-Intermediate must tech the call. Do not forget to check CBG!! There is now a button for Blood Draws as well.
An IV should not be started for the convenience of a doctor’s appointment, imaging appointment, etc. This changes the billing from BLS to ALS and the act of starting an IV must be properly justified.
Your PCR can determine whether or not you are called to court and also whether or not our agency stands behind you.
90% of the PCR’s at the moment are incorrect. Please take the time to do your documentation correctly. Repeat offenders will have additional remedial training.