epistaxis- nose bleed overview and managment
TRANSCRIPT


Introduction and History
Acute hemorrhage from the nostril, nasal cavity, or nasopharynx
5-10% of the population experience an episode of epistaxis each year. 10% of those will see a physician. 1% of those seeking medical care will need a specialist.
REASONS FOR EXCESSIVE BLEEDING
Vascularity of noseBoth external and internal carotids. Anastomsis between arteries and veins.Blood vessels run just under the mucosa-
unprotected.Larger vessels on the turbinate run in bony
canals- cannot contract.
3
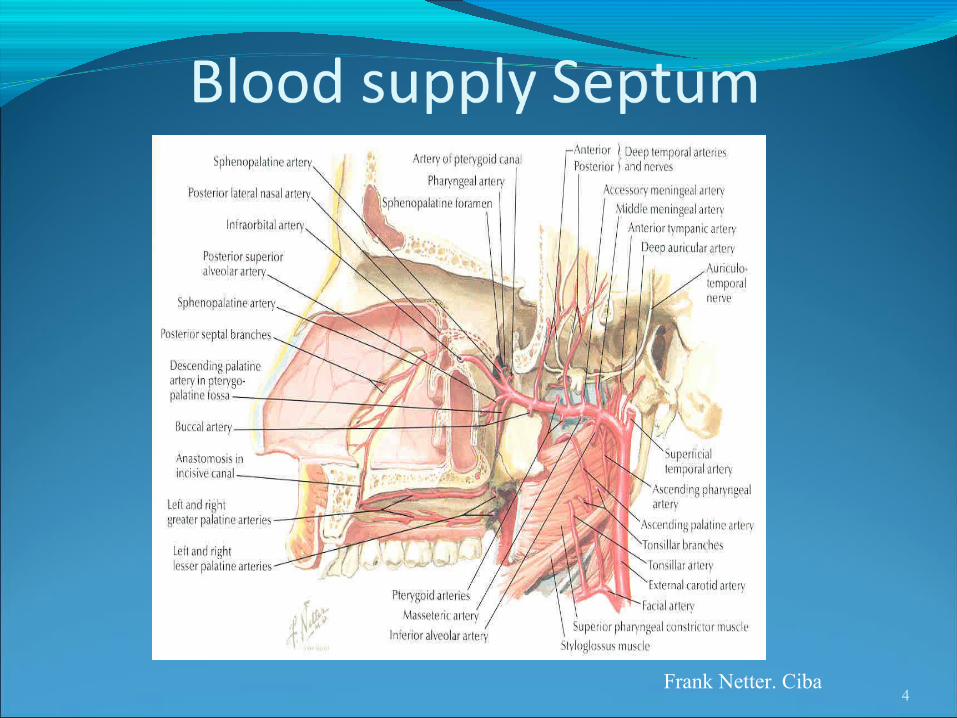
4Frank Netter. Ciba

5Frank Netter. Ciba
Kiesselbach‘s Plexus a.k.a Little’s area
1/2 inch from the caudal border of the septum antero-inferiorly.
Vessels anastomosing are; Anterior ethmoid, greater palatine, and sphenopalatine, and septal branch of superior labial.
Bleeding may be arterial or venous.
6

Kisselbach’s Plexus
7

Underlying CausesLocal irritation Use of ASA or NSAIDSHypertensionCoagulapathies / Bleeding disordersPlatelet dysfunction

Underlying CausesOccupational exposureAllergiesMalignancy Systemic disease such as granulomatous
disease(Wegener’s sarcoidosis)Hereditary hemorrhagic
telangiectasia(Osler-Weber-Rendu syndrome)
Cirrhosis, Renal Failure
9
Underlying Causes - TraumaNose pickingNose blowing/sneezingNasal fractureNasogastric/nasotracheal intubationTrauma to sinuses, orbits, middle ear, base of skullBarotrauma
Underlying causes - Iatrogenic nasal injury
Functional endoscopic sinus surgeryRhinoplastyNasal reconstruction

Local Factors – Dessication
Cold, dry air—more common in wintertimeDry heat—Phoenix and Death valleyNasal oxygenAnatomic abnormalitiesAtrophic rhinitisNasal septal deviationNasal septal perforation

Initial ManagementABC’sMedical history/MedicationsVital signs—need IV?Physical exam
Anterior rhinoscopyEndoscopic rhinoscopy
Laboratory examRadiologic studies
Laboratory StudiesCBCPT / PTTBleeding Time
14

TreatmentIV AccessIV FluidsBlood or Blood product transfusionControl of hypertensionCorrect coagulapathy
FFP, Vit. K, Protamine

Basic TreatmentMake the patient sit up, pinch nose, open
mouth and breath.
Ice on fore head and or gargle ice water
16

Ask the PatientPatients will almost always tell you the side of
bleedingWhich side did it start on Was in coming out the front or draining down
the throatNosebleeds rarely have bilateral sources
Anterior or PosteriorAnterior
Bright red blood from front of nose Posterior
Nausea, hematemesis, anemia, hemoptysis or melena.
No visualized anterior source of bleedingPost nasal drip of blood

TreatmentBe Prepared
Adequate equipment to the bedside HeadlightNasal SpeculumSuctionPacksCauteryAnesthetic
19

suction
good lightanesthetic
silver nitrate
merocels
gelfoam
bacitracin
endoscopes
suction bovie/bipolar
Afrin
Surgicel / Floseeal
epistat
bayonet forceptsvaseline gauze

TreatmentLocate the point after packing the nose with 4%
xylocaine and oxymetazolineSuction the NoseHave patient blow clots out of the nose

CAUTERIZATIONChemicals
Silver Nitrate stickElectrical
BovieBipolar
Avoid bilateral or excessive cautery
22

Pick a Pack, any pack

Nasal packsAnterior nasal packs
Merocel – Nasal TamponVaseline GauzeInflatable PacksSurgicel or Gelfoam
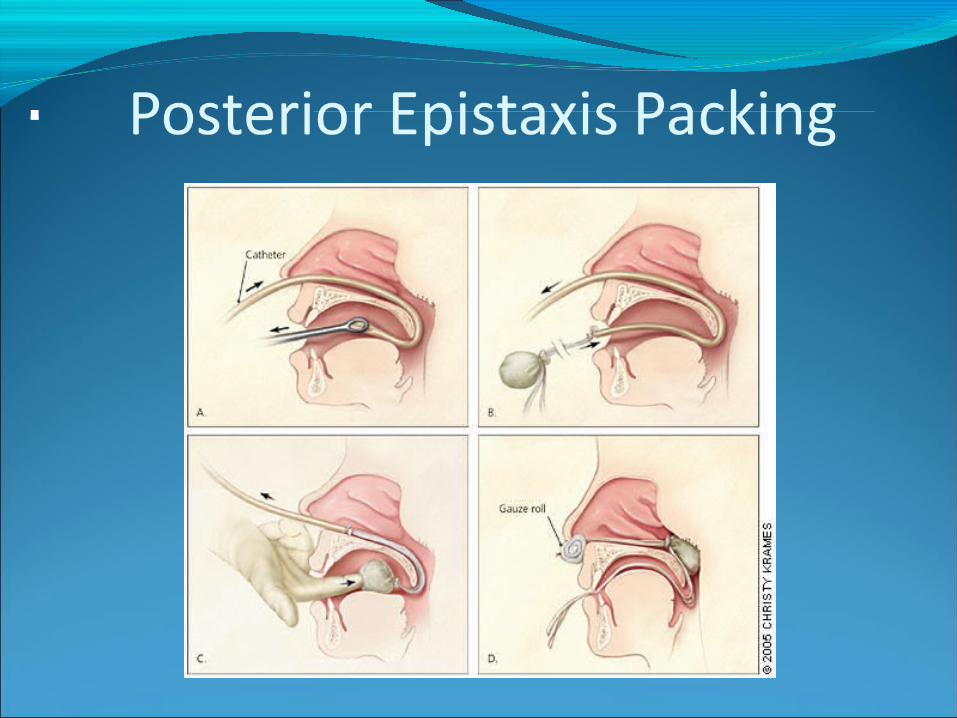

Posterior Epistaxis Packing
Posterior Epistaxis Packing

Epistaxis - ComplicationsSinusitisPossibility of airway obstructionToxic shock syndromeSeptal hematoma or abscessSeptal perforation Loose pack obstructing the airwayNasal scarring or stenosisAlar necrosis

Treatment after PackingRemoved as soon as possible
Typically 3-5 days AntibioticsPosterior or bilateral packing requires
admissionTransfuseContinue treatment of underlying condtionsOxygenICU Admit

Surgery / embolization Indications
Continued bleeding with packingRequired transfusion Nasal anomaly precluding packingPatient intolerance to packingPosterior bleed vs. failed medical mgmt
after >72hrs
Other Treatments

SurgeryLigation of vessels
Maxillary arteryEthmoid arteriesExternal Carotid artery
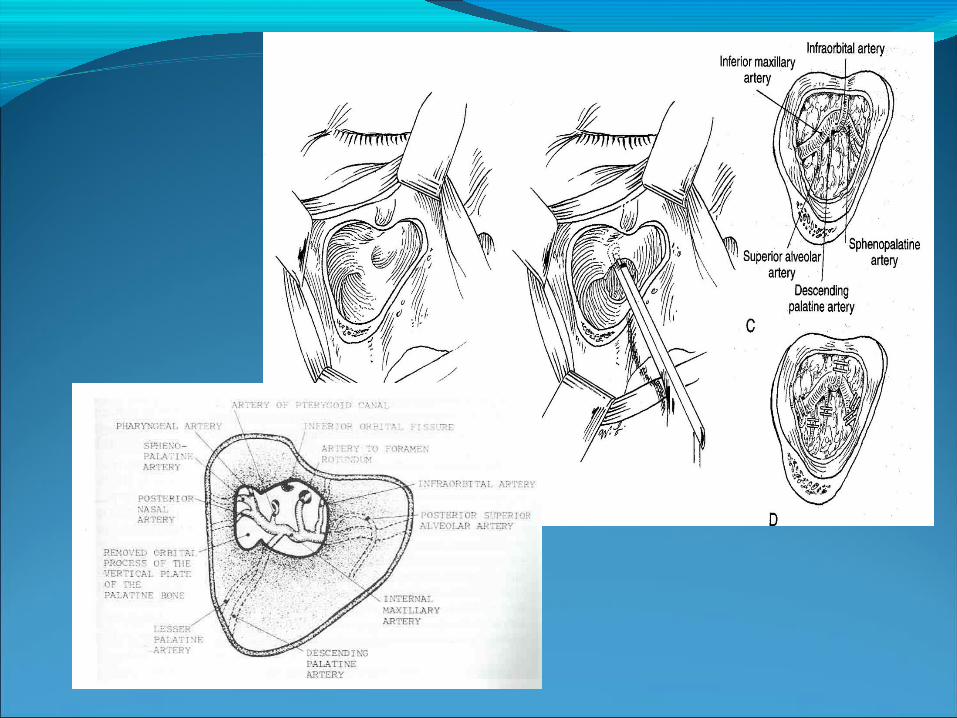
Transmaxillary IMA ligationWaters view Caldwell-LucElectrocautery of posterior wall before removalMicroscopic dissection and ligation of IMA
--descending palatine & sphenopalantine most important
Recurrence rate (failure rate) of 10-15%Complication rate of 25-30% (oa fistula,dental, n)Imax ligation now done commonly through
endoscopic approach

Ant./Post. Ethmoidal ligationPatients s/p IMAX ligation still bleeding, superior
nasal cavity epistaxis, or in conjunction when source unclear
Lynch incisionFronto-ethmoid suture line12-24-6 (14-18, 8-10, 4-6)
Transnasal Endoscopic Sphenopalatine Artery ligationFollow Middle Turbinate to posteriormost aspectVertical mucoperiosteal incision 7-8mm anterior to
post middle turb (between mid. and inf. turbs)Elevation of flap—ID neurovascular bundle at
foramenLigation with titanium clipReapproximate flapComplications –few, Failures—0-13%
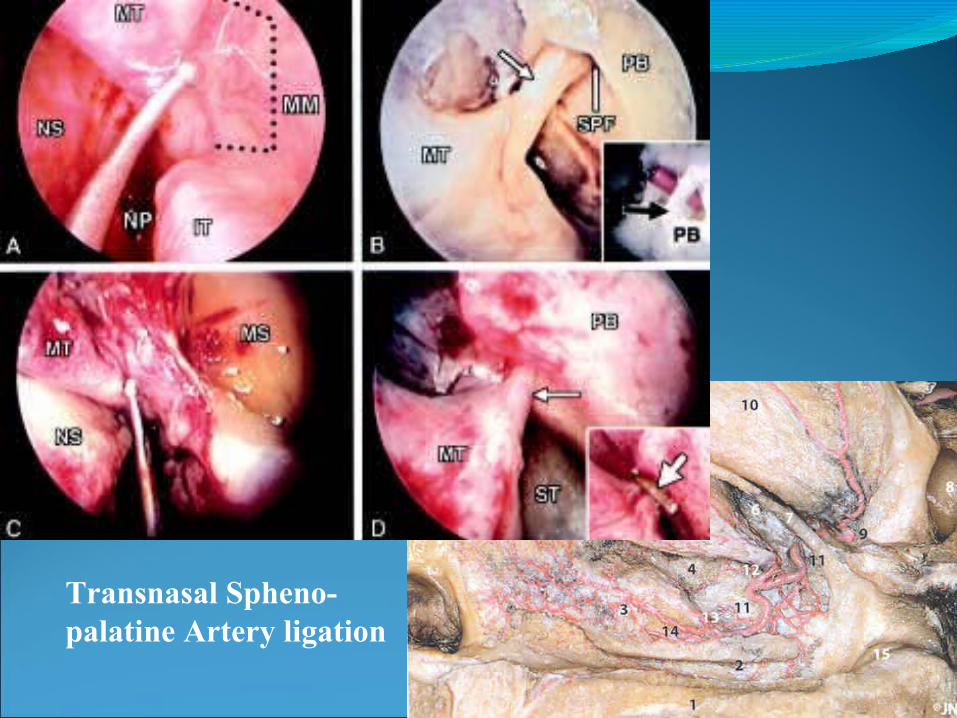
Transnasal Spheno-palatine Artery ligation
ECA ligationEffectivenessAnterior border of SCMID ECA/ICALigation after clear that surrounding structures are
safe.

Selective Angiography/embolizationHelps identify location of bleedingEmbolization most effective in patients who
Still bleeding after surgical arterial ligationBleeding site difficult to reach surgicallyComorbidities prohibit general anesthetic
Effective only when bleeding is >.5 ml/min90+% success rate, complication rate of 0.1%Only able to embolize external carotid & branchesComplications: minor (18-45%)/major (0-2%)Contraindicated in bad atherosclerosis, Ethmoid
bleed

Treatment after DischargeHumidity/emolientsDiscontinue offending medsNasal saline spraysAvoidance of nose picking/blowingSneeze with mouth openAvoid straining/bedrest