epidemiology of poliomyelitis dr. rasha salama phd community medicine and public health suez canal...
TRANSCRIPT

Epidemiology of Epidemiology of PoliomyelitisPoliomyelitis
Dr. Rasha SalamaDr. Rasha SalamaPhD Community Medicine and Public HealthPhD Community Medicine and Public Health
Suez Canal UniversitySuez Canal University
EgyptEgypt
PoliomyelitisPoliomyelitisFirst described by Michael Underwood in First described by Michael Underwood in 17891789
First outbreak described in U.S. First outbreak described in U.S. in 1843in 1843
21,000 paralytic cases reported in the U. S. 21,000 paralytic cases reported in the U. S. in 1952in 1952
Global eradication in near futureGlobal eradication in near future
IntroductionIntroduction
A viral infection most often recognized by acute onset of flaccid paralysis.
Infection with poliovirus results in a spectrum of Infection with poliovirus results in a spectrum of clinical manifestations from inapparent infection clinical manifestations from inapparent infection to non-specific febrile illness, aseptic meningitis, to non-specific febrile illness, aseptic meningitis, paralytic disease, and death. paralytic disease, and death.
Poliomyelitis is a highly infectious disease Poliomyelitis is a highly infectious disease caused by three serotypes of poliovirus. caused by three serotypes of poliovirus.
Two phases of acute poliomyelitis can be Two phases of acute poliomyelitis can be distinguished: a non-specific febrile illness distinguished: a non-specific febrile illness (minor illness) followed, in a small proportion of (minor illness) followed, in a small proportion of patients, by aseptic meningitis and/or paralytic patients, by aseptic meningitis and/or paralytic disease (major illness). disease (major illness).
The ratio of cases of inapparent infection to The ratio of cases of inapparent infection to paralytic disease ranges from 100:1 to 1000:1.paralytic disease ranges from 100:1 to 1000:1.
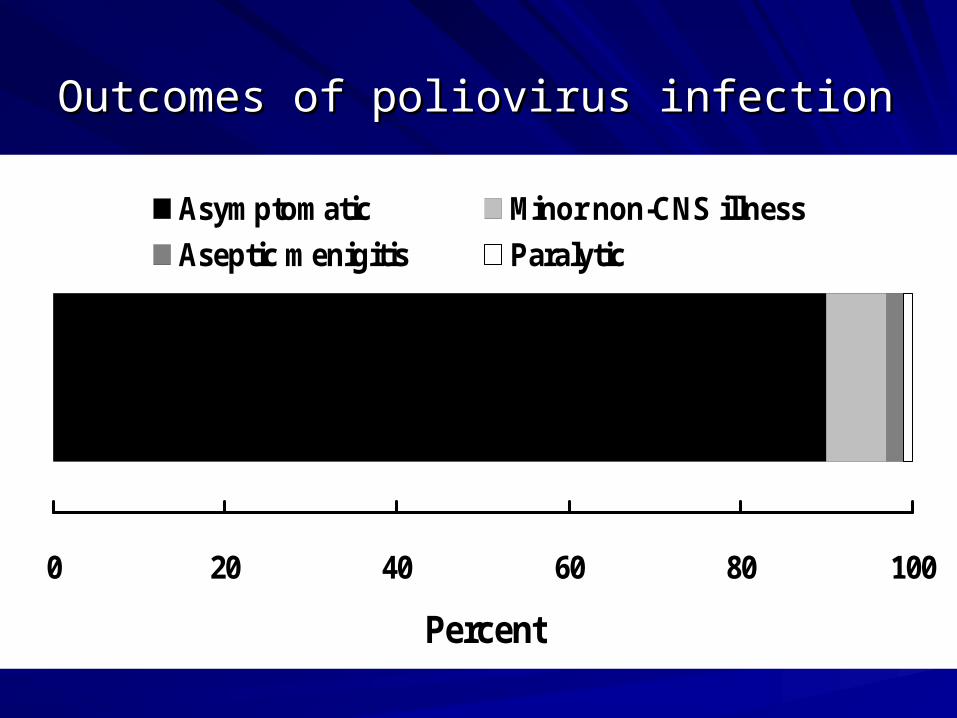
0 20 40 60 80 100
Percent
Asymptomatic Minor non-CNS illness
Aseptic menigitis Paralytic
Outcomes of poliovirus infectionOutcomes of poliovirus infection
Epidemiological patternEpidemiological pattern
The epidemiological pattern of polio depends The epidemiological pattern of polio depends upon the degree of the socioeconomic upon the degree of the socioeconomic development and health care services of a development and health care services of a country. country.
The pattern of the disease has been The pattern of the disease has been considerably modified by widespread considerably modified by widespread immunization.immunization.
According to the WHO; Three epidemiological According to the WHO; Three epidemiological patterns have now been delineated:patterns have now been delineated:
– Countries with no immunization: the virus infects all Countries with no immunization: the virus infects all children, and by age 5 years almost all children children, and by age 5 years almost all children develop antibodies to at least one of the 3 types of develop antibodies to at least one of the 3 types of polio virus. In that pattern paralytic polio cases are polio virus. In that pattern paralytic polio cases are frequent in infants.frequent in infants.
– Countries with partial immunization: In these countries, Countries with partial immunization: In these countries, wild polio virus is largely replaced by vaccine virus in wild polio virus is largely replaced by vaccine virus in the environment.the environment.
– Countries with almost total immunization coverage: in Countries with almost total immunization coverage: in these countries polio is becoming rare, however, these countries polio is becoming rare, however, sporadic cases do occur rarely. sporadic cases do occur rarely.
0
5000
10000
15000
20000
25000
1950 1956 1962 1968 1974 1980 1986 1992 1998 2004
Cases
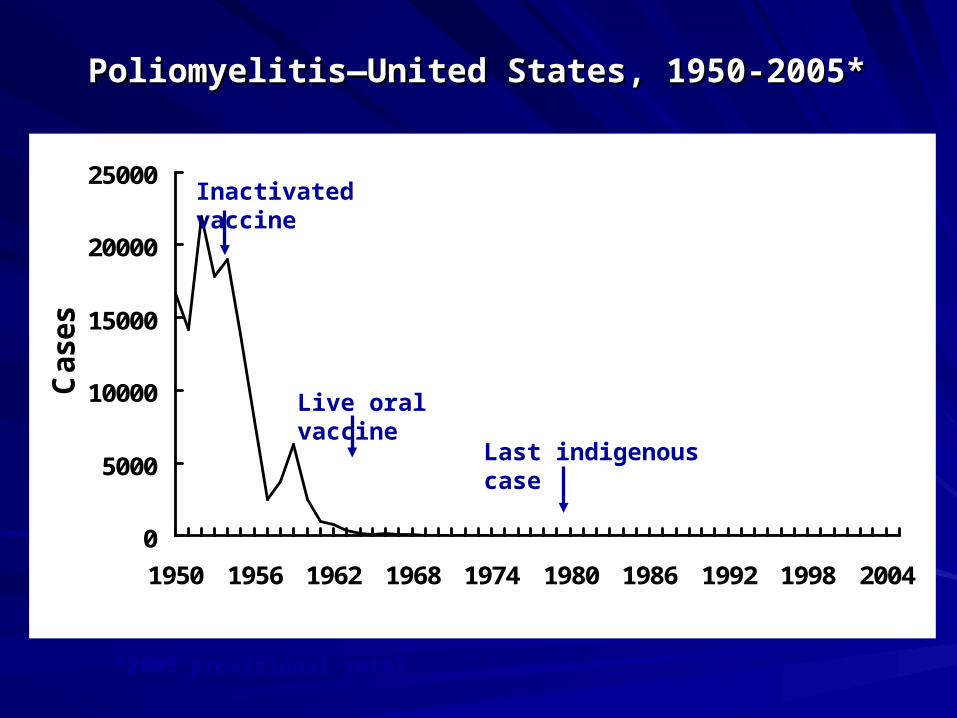
Poliomyelitis—United States, 1950-2005*Poliomyelitis—United States, 1950-2005*
Inactivated vaccine
Live oral vaccine
Last indigenous case
*2005 provisional total
Causative organismCausative organism
Poliovirus: belongs to “Picorna” viruses which are small Poliovirus: belongs to “Picorna” viruses which are small RNA-containing viruses.RNA-containing viruses.
Polioviruses have three antigenically distinct types, Polioviruses have three antigenically distinct types, giving no cross immunity:giving no cross immunity:– Type I: “Leon”; the commonest in epidemicsType I: “Leon”; the commonest in epidemics– Type II: “Berlinhide”; the prevailing type in endemic areas.Type II: “Berlinhide”; the prevailing type in endemic areas.– Type III: “Lansing”; occasionally causes epidemics.Type III: “Lansing”; occasionally causes epidemics.
Polioviruses are relatively resistant and survive for a long Polioviruses are relatively resistant and survive for a long time under suitable environmental conditions, but are time under suitable environmental conditions, but are readily destroyed by heat (e.g. pasteurization of milk, readily destroyed by heat (e.g. pasteurization of milk, and chlorination of water).and chlorination of water).
Reservoir of infectionReservoir of infection
Man is the only reservoir of infection of Man is the only reservoir of infection of poliomyelitis. poliomyelitis.
Man: cases and carriersMan: cases and carriers
Cases: all clinical forms of diseaseCases: all clinical forms of disease
Carriers: all types of carriers (e.g. incubatory, Carriers: all types of carriers (e.g. incubatory, convalescent, contact and healthy) except convalescent, contact and healthy) except chronic type. In endemic areas, healthy carriers chronic type. In endemic areas, healthy carriers are the most frequent type encountered.are the most frequent type encountered.
Foci of infectionFoci of infection
Pharynx: the virus is found in the Pharynx: the virus is found in the oropharyngeal secretions.oropharyngeal secretions.
Small intestine: the virus finds exit in Small intestine: the virus finds exit in stools.stools.
Modes of transmissionModes of transmission
Since foci of infection are the throat and small intestines, Since foci of infection are the throat and small intestines, poliomyelitis spreads by two routes:poliomyelitis spreads by two routes:
Oral-oral infection: direct droplet infectionOral-oral infection: direct droplet infection
Faeco-oral infection:Faeco-oral infection:– Food-borne (ingestion) infection through the ingestion of Food-borne (ingestion) infection through the ingestion of
contaminated foods. Vehicles include milk, water, or any others contaminated foods. Vehicles include milk, water, or any others that may be contaminated by handling, flies, dust….that may be contaminated by handling, flies, dust….
– Hand to mouth infection.Hand to mouth infection.
(polio virus has the ability to survive in cold environments. (polio virus has the ability to survive in cold environments. Overcrowding and poor sanitation provide opportunities for Overcrowding and poor sanitation provide opportunities for exposure to infection.)exposure to infection.)
Period of infectivityPeriod of infectivity
Contact and healthy carriers: about 2 weeksContact and healthy carriers: about 2 weeks
Cases: the cases are most infectious 7 to 10 days before Cases: the cases are most infectious 7 to 10 days before and after the onset of symptoms. In the feaces, the virus and after the onset of symptoms. In the feaces, the virus is excreted commonly for 2 to 3 weeks, sometimes as is excreted commonly for 2 to 3 weeks, sometimes as long as 3 to 4 months.long as 3 to 4 months.
In polio cases, infectivity in the pharyngeal foci is around In polio cases, infectivity in the pharyngeal foci is around one week, and in the intestinal foci 6-8 weeks.one week, and in the intestinal foci 6-8 weeks.
Incubation Period: 7-14 daysIncubation Period: 7-14 days
Susceptibility Susceptibility Age: more than 95% reported in infancy and childhood Age: more than 95% reported in infancy and childhood with over 50% of them in infancy.with over 50% of them in infancy.
Sex: no sex ratio differences, but in some countries, Sex: no sex ratio differences, but in some countries, males are infected more frequently than females in a males are infected more frequently than females in a ratio 3:1. ratio 3:1.
Risk factors: (provocative factors of paralytic polio in Risk factors: (provocative factors of paralytic polio in individuals infected with polio virus): fatigue, trauma, individuals infected with polio virus): fatigue, trauma, intramuscular injections, operative procedures, intramuscular injections, operative procedures, pregnancy, excessive muscular exercise… pregnancy, excessive muscular exercise…
Immunity: The maternal antibodies gradually disappear Immunity: The maternal antibodies gradually disappear during the first 6 months of life. Immunity following during the first 6 months of life. Immunity following infection is fairly solid, although infection with other types infection is fairly solid, although infection with other types of polio virus can still occur.of polio virus can still occur.
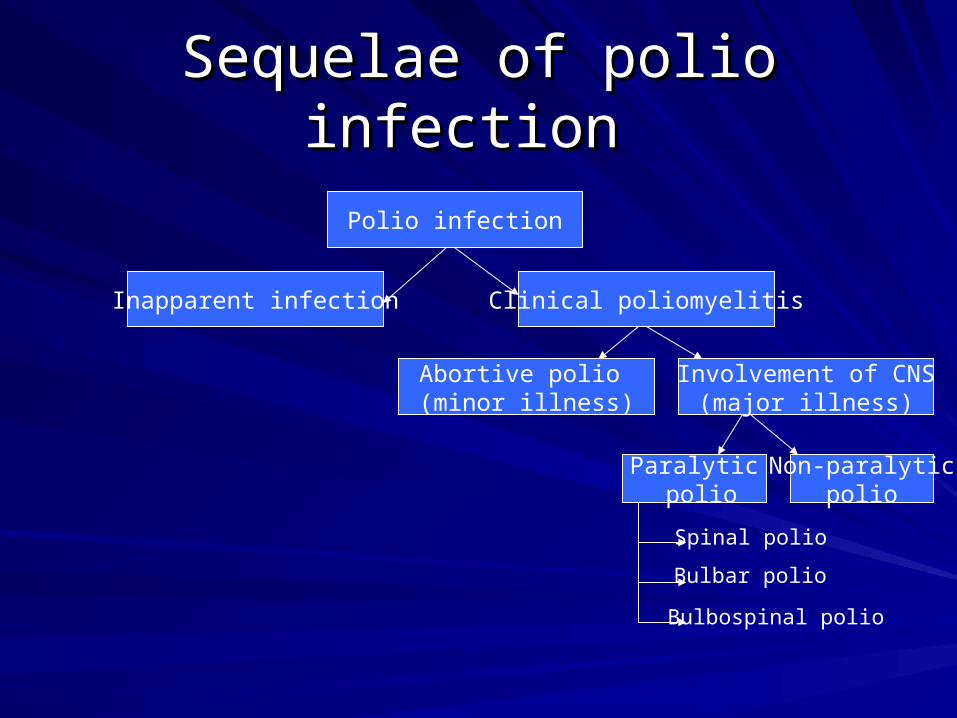
Sequelae of polio infection Sequelae of polio infection
Polio infection
Inapparent infection Clinical poliomyelitis
Abortive polio (minor illness)
Involvement of CNS(major illness)
Paralytic polio
Non-paralyticpolio
Spinal polio
Bulbar polio
Bulbospinal polio
Inapparent infectionInapparent infection
Incidence is more than 100 to 1000 times Incidence is more than 100 to 1000 times the clinical cases. the clinical cases.
No clinical manifestations, but infection is No clinical manifestations, but infection is associated with acquired immunity, and associated with acquired immunity, and carrier state.carrier state.
Clinical poliomyelitisClinical poliomyelitis
I.I. Abortive polio (minor illness):Abortive polio (minor illness):
The majority of clinical cases are abortive, with mild The majority of clinical cases are abortive, with mild systemic manifestations for one or two days only, systemic manifestations for one or two days only, then clears up giving immunity. Some abortive cases then clears up giving immunity. Some abortive cases may be so mild to pass unnoticed. may be so mild to pass unnoticed.
Manifestations:Manifestations:– Moderate feverModerate fever– Upper respiratory manifestations: pharyngitis and sore throatUpper respiratory manifestations: pharyngitis and sore throat– Gastrointestinal manifestations: vomiting, abdominal pain, Gastrointestinal manifestations: vomiting, abdominal pain,
and diarrhea.and diarrhea.
Clinical poliomyelitis (cont.)Clinical poliomyelitis (cont.)
II. Involvement of the CNS (major illness):II. Involvement of the CNS (major illness):
Affects a small proportion of the clinical cases, and Affects a small proportion of the clinical cases, and appears few days after subsidence of the abortive stage. appears few days after subsidence of the abortive stage. It takes two forms: nonparalytic and paralytic polio.It takes two forms: nonparalytic and paralytic polio.
Nonparalytic polio is manifested by fever, headache, Nonparalytic polio is manifested by fever, headache, nausea, vomiting, and abdominal pain. Signs of nausea, vomiting, and abdominal pain. Signs of meningeal irritation (meningism), and aseptic meningitis meningeal irritation (meningism), and aseptic meningitis (pain and stiffness in the neck back and limbs) may also (pain and stiffness in the neck back and limbs) may also occur.occur.
The case either recovers or passes to the paralytic The case either recovers or passes to the paralytic stage, and here the nonpralytic form is considered as a stage, and here the nonpralytic form is considered as a “preparalytic stage”.“preparalytic stage”.
Clinical poliomyelitis (cont.)Clinical poliomyelitis (cont.)
Paralytic poliomyelitis:Paralytic poliomyelitis:
Paralysis usually appears within 4 days after the Paralysis usually appears within 4 days after the preparalytic stage (around 7-10 days from onset of preparalytic stage (around 7-10 days from onset of disease).disease).
The case shows fever, headache, irritability, and The case shows fever, headache, irritability, and different paralytic manifestations according to the part of different paralytic manifestations according to the part of the CNS involved, with destruction of the motor nerve the CNS involved, with destruction of the motor nerve cells, but not the sensory nerve cells.cells, but not the sensory nerve cells.
Forms: spinal, bulbar, and bulbospinal.Forms: spinal, bulbar, and bulbospinal.
Spinal polioSpinal polio
Different spinal nerves are involved, due to Different spinal nerves are involved, due to injury of the anterior horn cells of the injury of the anterior horn cells of the spinal cord, causing tenderness, spinal cord, causing tenderness, weakness, and flaccid paralysis of the weakness, and flaccid paralysis of the corresponding striated muscles.corresponding striated muscles.
The lower limbs are the most commonly The lower limbs are the most commonly affected.affected.
Bulbar polioBulbar polio
Nuclei of the cranial nerves are involved, Nuclei of the cranial nerves are involved, causing weakness of the supplied muscles, and causing weakness of the supplied muscles, and maybe encephalitis.maybe encephalitis.
Bulbar manifestations include dysphagia, nasal Bulbar manifestations include dysphagia, nasal voice, fluid regurgitation from the nose, difficult voice, fluid regurgitation from the nose, difficult chewing, facial weakness and diplopiachewing, facial weakness and diplopia
Paralysis of the muscles of respiration is the Paralysis of the muscles of respiration is the most serious life-threatening manifestation.most serious life-threatening manifestation.
Bulbospinal polioBulbospinal polio
Combination of both spinal and bulbar Combination of both spinal and bulbar formsforms
Complications and case fatality Complications and case fatality
Respiratory complications: pneumonia, pulmonary Respiratory complications: pneumonia, pulmonary edemaedema
Cardiovascular complications: myocarditis, cor Cardiovascular complications: myocarditis, cor pulmonale.pulmonale.
Late complications: soft tissue and bone deformities, Late complications: soft tissue and bone deformities, osteoporosis, and chronic distension of the colon.osteoporosis, and chronic distension of the colon.
Case fatality: varies from 1% to 10% according to the Case fatality: varies from 1% to 10% according to the form of disease (higher in bulbar), complications and age form of disease (higher in bulbar), complications and age ( fatality increases with age).( fatality increases with age).

Case definitionCase definition
The following case definition for paralytic The following case definition for paralytic poliomyelitis has been approved by CDC (1997)poliomyelitis has been approved by CDC (1997)
Clinical case definitionClinical case definition
Acute onset of a flaccid paralysis of one or more Acute onset of a flaccid paralysis of one or more limbs with decreased or absent tendon reflexes limbs with decreased or absent tendon reflexes in the affected limbs, without other apparent in the affected limbs, without other apparent cause, and without sensory or cognitive loss.cause, and without sensory or cognitive loss.
Case classificationCase classification
Probable: Probable: A case that meets the clinical case definition.A case that meets the clinical case definition.
Confirmed: Confirmed: A case that meets the clinical case definition and in A case that meets the clinical case definition and in which the patient has a neurologic deficit 60 days after onset of which the patient has a neurologic deficit 60 days after onset of initial symptoms, has died, or has unknown follow-up status.initial symptoms, has died, or has unknown follow-up status.
Confirmed cases are then further classified based on epidemiologic Confirmed cases are then further classified based on epidemiologic and laboratory criteria. Only confirmed cases are included in the and laboratory criteria. Only confirmed cases are included in the Morbidity and Mortality Weekly Report (MMWR)Morbidity and Mortality Weekly Report (MMWR)..
Indigenous case: Indigenous case: Any case which cannot be proved to be Any case which cannot be proved to be imported.imported.
Imported case: Imported case: A case which has its source outside the country. AA case which has its source outside the country. A person with poliomyelitis who has entered the country and had person with poliomyelitis who has entered the country and had
onset of illness within 30 days before or after entryonset of illness within 30 days before or after entry
Diagnosis and laboratory testingDiagnosis and laboratory testing
Laboratory studies, especially attempted Laboratory studies, especially attempted poliovirus isolation, are critical to rule out poliovirus isolation, are critical to rule out or confirm the diagnosis of paralytic or confirm the diagnosis of paralytic poliomyelitis.poliomyelitis.
Virus isolationVirus isolation The likelihood of poliovirus isolation is highest from stool The likelihood of poliovirus isolation is highest from stool
specimens,specimens, intermediate from pharyngeal swabs, and very low from intermediate from pharyngeal swabs, and very low from
blood or spinal fluid.blood or spinal fluid.
Diagnosis and laboratory testing Diagnosis and laboratory testing (cont.)(cont.)
Serologic testingSerologic testingA four-fold titer rise between the acute and A four-fold titer rise between the acute and convalescent specimens suggests poliovirus convalescent specimens suggests poliovirus infection. infection.
Cerebrospinal fluid (CSF) analysisCerebrospinal fluid (CSF) analysisThe cerebrospinal fluid usually contains an The cerebrospinal fluid usually contains an increased number of leukocytes—from 10 to 200 increased number of leukocytes—from 10 to 200 cells/mm3 (primarily lymphocytes) and a mildly cells/mm3 (primarily lymphocytes) and a mildly elevated protein, from 40 to 50 mg/100 ml. elevated protein, from 40 to 50 mg/100 ml.
Prevention Prevention
General prevention:General prevention:
Health promotion through environmental Health promotion through environmental sanitation.sanitation.
Health education (modes of spread, Health education (modes of spread, protective value of vaccination).protective value of vaccination).
Prevention Prevention
Seroprophylaxis by immunoglobulins:Seroprophylaxis by immunoglobulins:
Not a practical way of giving protection Not a practical way of giving protection because it must be given either or before because it must be given either or before or very shortly after exposure to infection.or very shortly after exposure to infection.
(0.3 ml/kg of body weight).(0.3 ml/kg of body weight).
preventionprevention
Active immunization:Active immunization:– Salk vaccine (intramuscular polio trivalent Salk vaccine (intramuscular polio trivalent
killed vaccine).killed vaccine).– Sabin vaccine (oral polio trivalent live Sabin vaccine (oral polio trivalent live
attenuated vaccine).attenuated vaccine).
Inactivated Polio VaccineInactivated Polio VaccineContains 3 serotypes of vaccine virusContains 3 serotypes of vaccine virusGrown on monkey kidney (Vero) cellsGrown on monkey kidney (Vero) cellsInactivated with formaldehydeInactivated with formaldehydeContains 2-phenoxyethanol, neomycin, Contains 2-phenoxyethanol, neomycin, streptomycin, polymyxin Bstreptomycin, polymyxin B
Oral Polio VaccineOral Polio VaccineContains 3 serotypes of vaccine virusContains 3 serotypes of vaccine virusGrown on monkey kidney (Vero) cellsGrown on monkey kidney (Vero) cellsContains neomycin and streptomycinContains neomycin and streptomycinShed in stool for up to 6 weeks following Shed in stool for up to 6 weeks following vaccinationvaccination
Inactivated Polio VaccineInactivated Polio VaccineHighly effective in producing Highly effective in producing immunity to poliovirusimmunity to poliovirus>90% immune after 2 doses>90% immune after 2 doses>99% immune after 3 doses>99% immune after 3 dosesDuration of immunity not known with Duration of immunity not known with certaintycertainty
Oral Polio VaccineOral Polio VaccineHighly effective in producing Highly effective in producing immunity to poliovirusimmunity to poliovirus50% immune after 1 dose50% immune after 1 dose>95% immune after 3 doses>95% immune after 3 dosesImmunity probably lifelongImmunity probably lifelong
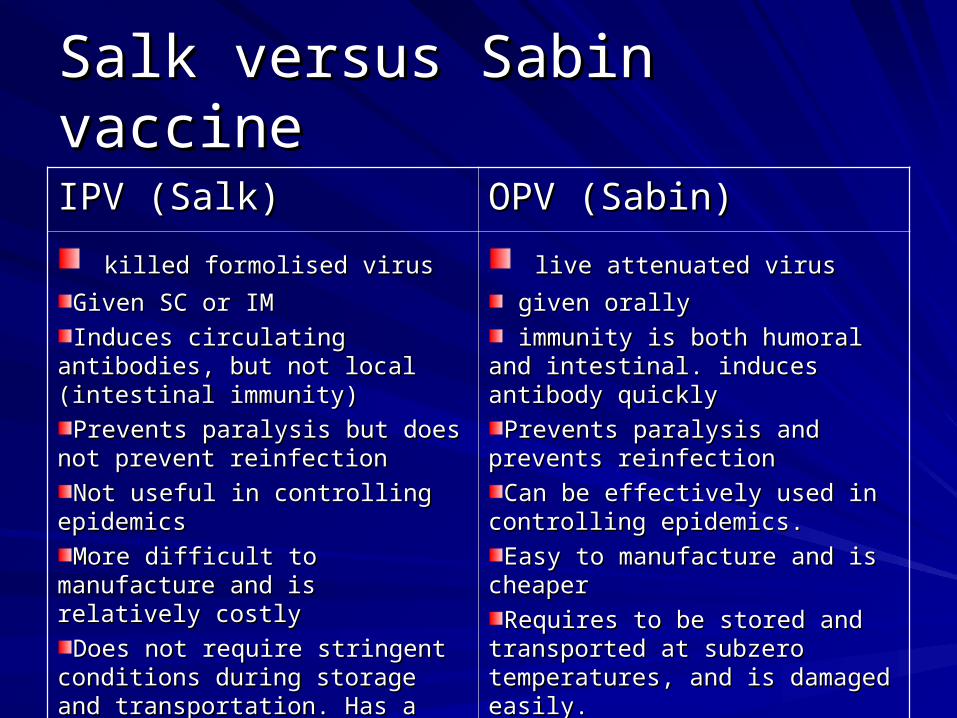
Salk versus Sabin vaccineSalk versus Sabin vaccine
IPV (Salk)IPV (Salk) OPV (Sabin)OPV (Sabin)
killed formolised viruskilled formolised virus
Given SC or IMGiven SC or IM
Induces circulating antibodies, but Induces circulating antibodies, but not local (intestinal immunity)not local (intestinal immunity)
Prevents paralysis but does not Prevents paralysis but does not prevent reinfectionprevent reinfection
Not useful in controlling epidemicsNot useful in controlling epidemics
More difficult to manufacture and is More difficult to manufacture and is relatively costlyrelatively costly
Does not require stringent conditions Does not require stringent conditions during storage and transportation. Has during storage and transportation. Has a longer shelf life.a longer shelf life.
live attenuated viruslive attenuated virus
given orallygiven orally
immunity is both humoral and immunity is both humoral and intestinal. induces antibody quicklyintestinal. induces antibody quickly
Prevents paralysis and prevents Prevents paralysis and prevents reinfectionreinfection
Can be effectively used in controlling Can be effectively used in controlling epidemics.epidemics.
Easy to manufacture and is cheaperEasy to manufacture and is cheaper
Requires to be stored and Requires to be stored and transported at subzero temperatures, transported at subzero temperatures, and is damaged easily.and is damaged easily.
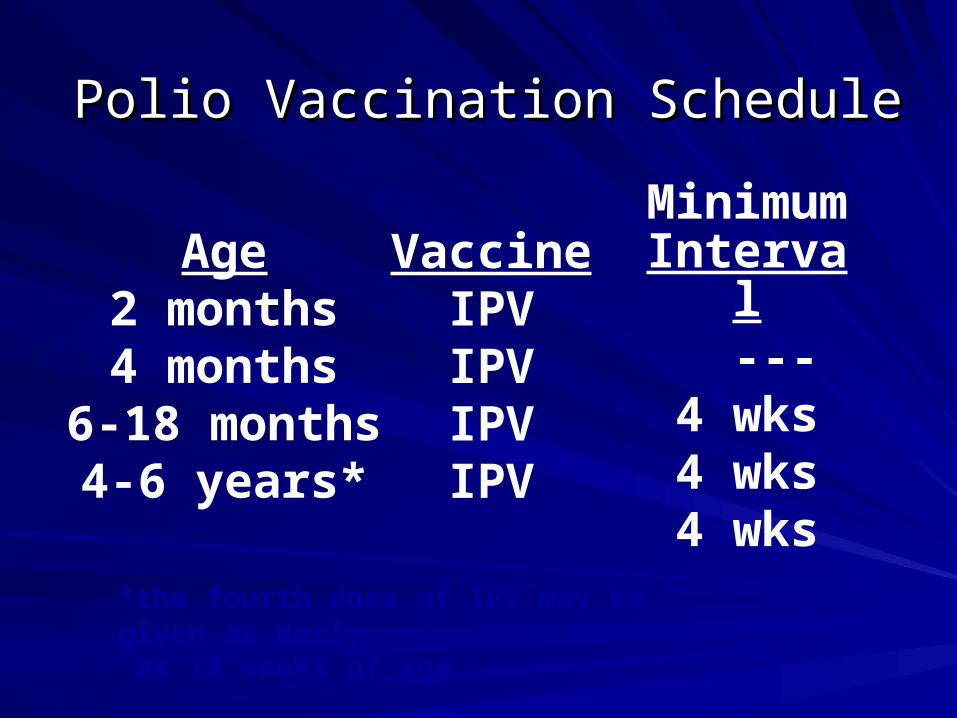
Polio Vaccination Schedule Polio Vaccination Schedule
VaccineIPVIPVIPVIPV
Age2 months4 months
6-18 months4-6 years*
MinimumInterval
---4 wks4 wks4 wks
*the fourth dose of IPV may be given as early as 18 weeks of age
Polio Vaccination of Polio Vaccination of Unvaccinated AdultsUnvaccinated Adults
IPVIPVUse standard IPV schedule if possible (0, 1-2 Use standard IPV schedule if possible (0, 1-2 months, 6-12 months)months, 6-12 months)May separate doses by 4 weeks if accelerated May separate doses by 4 weeks if accelerated schedule neededschedule needed
Polio Vaccination of Previously Polio Vaccination of Previously Vaccinated AdultsVaccinated Adults
Previously complete seriesPreviously complete series– administer one dose of IPVadminister one dose of IPV
Incomplete seriesIncomplete series– administer remaining doses in seriesadminister remaining doses in series
– no need to restart seriesno need to restart series
Polio Vaccine Adverse ReactionsPolio Vaccine Adverse Reactions
Rare local reactions (IPV)Rare local reactions (IPV)
No serious reactions to IPV have been No serious reactions to IPV have been documenteddocumented
Paralytic poliomyelitis (OPV)Paralytic poliomyelitis (OPV)
Vaccine-Associated Paralytic PolioVaccine-Associated Paralytic PolioIncreased risk in persons Increased risk in persons >>18 years18 yearsIncreased risk in persons with immunodeficiencyIncreased risk in persons with immunodeficiencyNo procedure available for identifying persons at risk No procedure available for identifying persons at risk of paralytic diseaseof paralytic disease5-10 cases per year with exclusive use 5-10 cases per year with exclusive use of OPVof OPVMost cases in healthy children and their household Most cases in healthy children and their household contactscontacts
Polio VaccinePolio VaccineContraindications and PrecautionsContraindications and Precautions
Severe allergic reaction to a vaccine Severe allergic reaction to a vaccine component or following a prior dose of component or following a prior dose of vaccinevaccine
Moderate or severe acute illnessModerate or severe acute illness
Polio VaccinePolio VaccineContraindications and PrecautionsContraindications and Precautions
Severe allergic reaction to a vaccine Severe allergic reaction to a vaccine component or following a prior dose of component or following a prior dose of vaccinevaccine
Moderate or severe acute illnessModerate or severe acute illness
B. Control of patient, contacts and the immediate environment:
1) Report to local health authority: Obligatory case report of paralytic cases as a Disease under surveillance by WHO, Class 1.
2) Isolation: Enteric precautions in the hospital for wild virus disease; of little value under home conditions because many household contacts are infected before poliomyelitis has been diagnosed.
3) Concurrent disinfection: Throat discharges, feces and articles soiled therewith. Terminal cleaning.
4) Quarantine: Of no community value.
5) Protection of contacts: Immunization of familial and otherclose contacts is recommended but may not contribute toimmediate control; the virus has often infected susceptibleclose contacts by the time the initial case is recognized.
6) Investigation of contacts and source of infection: Occurrenceof a single case of poliomyelitis due to wild poliovirus mustbe recognized as a public health emergency promptingimmediate investigation and planning for a large-scale
response.A thorough search for additional cases of AFP in thearea around the case assures early detection, facilitatescontrol and permits appropriate treatment of unrecognizedand unreported cases.
7) Specific treatment: None; however, Physical therapy is used to attain maximum function after paralytic poliomyelitis.
C. Epidemic measures:
In any country, a single case of poliomyelitis must now be considered a public health emergency, requiring an extensive supplementary immunization response over a large geographic area.
D. Disaster implications:
Overcrowding of non-immune groups and collapse of the sanitary infrastructure pose an epidemic threat.
E. International measures:
Poliomyelitis is a Disease under surveillance by WHO and is targeted for eradication by 2005.
National health administrations are expected to inform WHO immediately of individual cases and to supplement these reports as soon as possible with details of the nature and extent of virus transmission.
Planning a large-scale immunization response must begin immediately and, if epidemiologically appropriate, in coordination with bordering countries.
E. International measures (cont.):
Once a wild poliovirus is isolated, molecular epidemiology can often help trace the source.
Countries should submit monthly reports on case of poliomyelitis AFP cases and AFP surveillance performance to their respective WHO offices.
International travelers visiting areas of high prevalence must be adequately immunized.
Polio EradicationPolio Eradication
Last case in United States in 1979Last case in United States in 1979Western Hemisphere certified polio free in 1994Western Hemisphere certified polio free in 1994Last isolate of type 2 poliovirus in India in Last isolate of type 2 poliovirus in India in October 1999October 1999Global eradication goalGlobal eradication goal
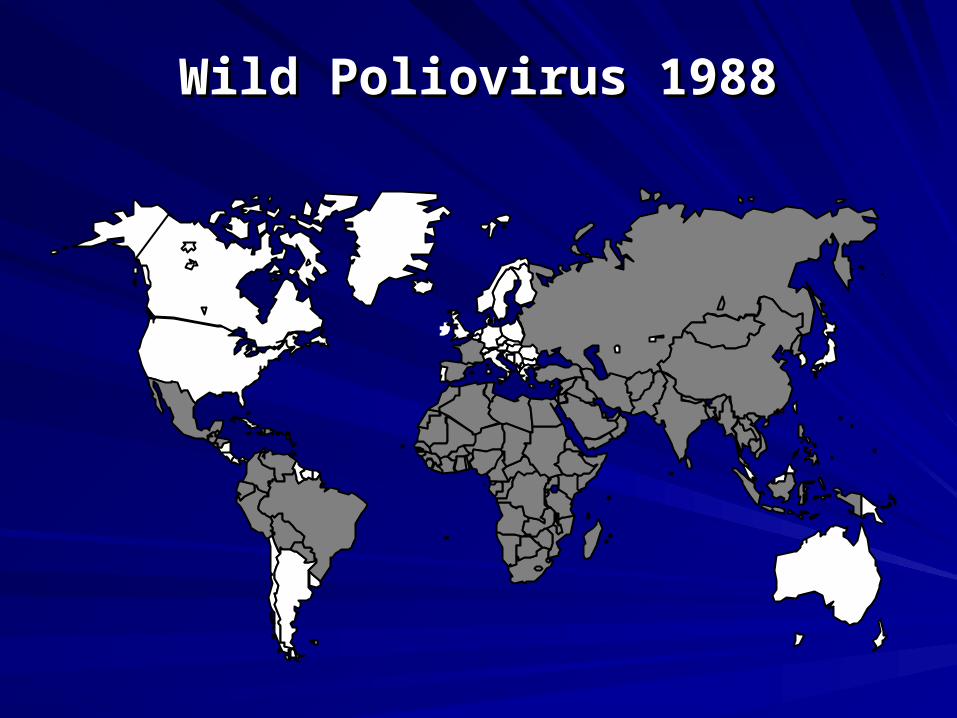
Wild Poliovirus 1988Wild Poliovirus 1988
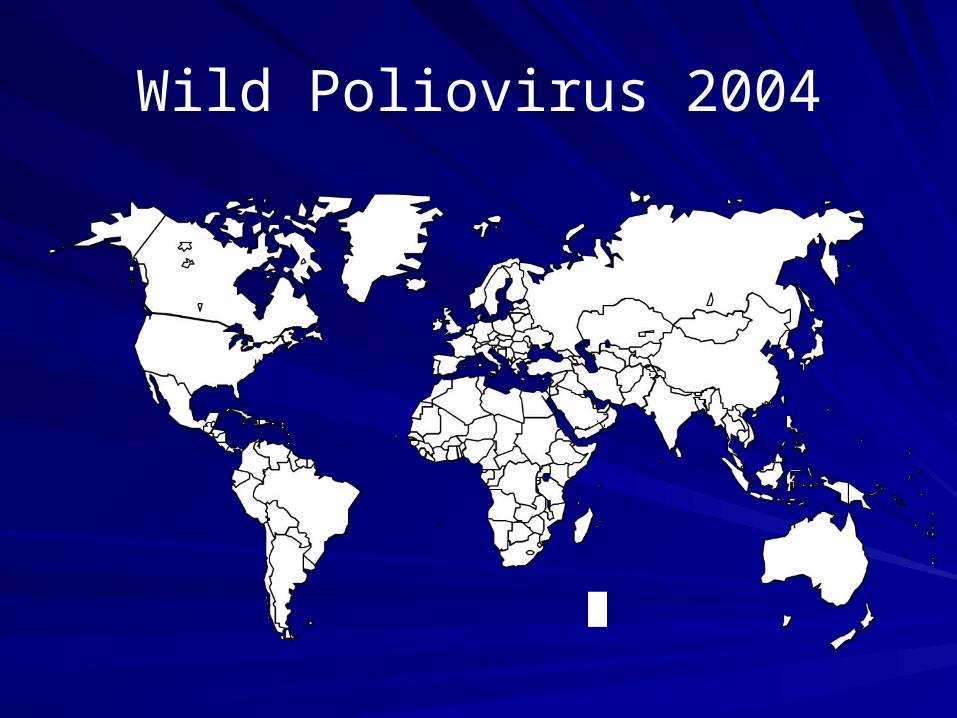
Wild Poliovirus 2004
Poliomyelitis Eradication is a Poliomyelitis Eradication is a crucial issue of discussion in crucial issue of discussion in “group discussion” session!!“group discussion” session!!
Please go and read about itPlease go and read about it
Thank YouThank You