enhancing compliance not a prerequisite for effective eradication of helicobacter pylori: the help...
TRANSCRIPT
Enhancing Compliance Not a Prerequisite for EffectiveEradication ofHelicobacter pylori: The HelP StudyAmanda Henry, B. Med. Sci., and Robert G. Batey, M.D. B.Sc.(Med), M.B. B.S., F.R.A.C.P., F.R.C.P. (UK)The University of Newcastle, and Department of Gastroenterology, John Hunter Hospital, Newscastle,New South Wales, Australia
OBJECTIVE: The aim of this study was to compare cure ratesof Helicobacter pylori (H. pylori) infection, compliance,and side effects in patients given 10 days of omeprazole 20mg b.d., amoxycillin 500 mgt.d.s., and metronidazole 400mg t.d.s.(OAM) or 10 days OAM plus compliance enhanc-ing measures.
METHODS: A total of 119 H. pylori-positive patients wereprospectively randomized to receive either 10 days OAM or10 days OAM plus compliance enhancing measures (med-ication in a dose dispensing unit, medication chart, an in-formation sheet aboutH. pylori treatment, and phone call 2days after starting therapy).H. pylori eradication was as-sessed by13C-UBT at least 4 wk after cessation of therapy,compliance by phone interview on the last day of therapyand returned pill count, and side effects by phone interviewand returned side effects form.
RESULTS: In 113 patients attending13C-UBT H. pylori waseradicated in 51 of 57 patients (89.5%) after 10 days OAMand in 48 of 56 (85.7%) after 10 days OAM plus complianceenhancing measures (p 5 0.54). In both groups 97% ofmedications were taken. Side effects were common (82% ofpatients). Both side effects (p 5 0.001) and ulcerversusnonulcer at endoscopy (p 5 0.016) were independent pre-dictors of treatment failure; side effects also predicted non-compliance (p 5 0.02).
CONCLUSIONS: Ten days of OAM was effective forH.pylori eradication in our clinical population. Patient com-pliance was excellent and attempts to increase compliancehad no impact on outcome or compliance. Side effects werevery common and were significantly associated with treat-ment failure and decreased compliance. (Am J Gastroenterol1999;94:811–815. © 1999 by Am. Coll. of Gastroenterol-ogy)
INTRODUCTION
In recent years there has been an explosion in the number ofpatients treated forHelicobacter pylori(H. pylori). Growingpublic awareness of the role ofH. pylori in gastroduodenalcomplaints, and increasing availability of reliable noninva-sive testing for the infection, means that this number islikely to continue to increase. Intention-to-treat analyses oftwo of the most readily available therapies, bismuth-based
triple therapy (BTT) and omeprazole-amoxycillin-metroni-dazole triple therapy (OTT), show eradication rates of 72%and 84% respectively (1, 2). Because success rates afterfailed triple therapy drop to approximately 50% when asecond course is attempted (3), it is important to attempt tooptimize success rates for first line treatment.
Factors that have been shown to be reasons for failure oftriple therapy include metronidazole resistance (4), pretreat-ment factors such as smoking (5), and poor compliance(6–9). Work to date suggests that cure rates of patients withmetronidazole resistant strains are lowered to approximately50% in BTT (4, 10, 11) but only drop to around 75% usingOTT (11, 12), so problems due to metronidazole resistancemay be at least partially overcome by using OTT. Smokingand other pretreatment factors are unlikely to be modified,so little can be done about their negative impact on curerates. Poor compliance, however, remains a potentiallymodifiable source of treatment failure.
Compliance with short term antibiotic therapy is knownto be poor (13, 14), with$90% of patients noncompliant byday 10 of therapy (15). However, the issue of compliancewith H. pylori therapy has received relatively little attentionsince it was reported as a major cause of BTT failure (6).Compliance with OTT is generally reported to be in.90%(16–18) but these figures are mostly from clinical trials withhighly filtered patient populations, and may not accuratelyreflect normal clinical practice. In addition, as compliance inthese studies is usually measured by interview or pill countonly, and both measures tend to overestimate compliance(19, 20), compliance rates for triple therapy may be lowerthan reported. A percentage of “unexplained” treatmentfailure may therefore be due to noncompliance. To attemptto optimize outcome ofH. pylori therapy and to examine therelationship of compliance and side effects to treatmentoutcome the HelP study was designed.
MATERIALS AND METHODS
Patient SelectionBetween March and August 1997 patients withH. pyloriinfection were prospectively recruited from the endoscopyunit and outpatient gastroenterological clinic of our teachinghospital and randomized to one of two treatment groups. Alladult patients (age.18 yr) were screened for eligibility.Exclusion criteria were inability or refusal to give informed
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 94, No. 3, 1999© 1999 by Am. Coll. of Gastroenterology ISSN 0002-9270/99/$20.00Published by Elsevier Science Inc. PII S0002-9270(98)00737-0

consent, contraindication to the study medication, consul-tant recommendation not to treat the patient, consultant wishto use anH. pylori therapy other than the study medication,and inpatient status (as patient compliance is imposed in thissituation). The trial was single-blinded in that, althoughpatients were aware of the names of the study medicationand the fact that the study was anH. pylori treatment trial,they were unaware of either the differences between thetreatment groups or the compliance enhancing purpose ofthe trial.
Diagnostic MethodsPatients were accepted as positive if the CLO-test, histopa-thology, or 13C-urea breath test (13C-UBT) was positive.Pretreatment endoscopy was not a prerequisite for entry butoccurred in all but three study patients. A total of 113patients were diagnosed on the basis of positive CLO testwith or without histopathology, three on13C-UBT only(without endoscopy), and one on histopathology only. Onepatient with an equivocal CLO-test but positive histopathol-ogy was accepted, as was one CLO-negative patient withpositive histology and positive PCR forH. pylori genes.
TreatmentAll patients received 10 days of omeprazole 20 mgb.d.,amoxycillin 500 mgt.d.s., and metronidazole 400 mgt.d.s.,as well as verbal advice on medication use and possible sideeffects, in an initial 20-min consultation. In addition, pa-tients in the intervention group (group 2) received medica-tion in dose-dispensing units (Webster Pak, Manrex P/L,Sydney, N.S.W., Australia), an information sheet onH.pylori treatment, and a medication chart. Compliance inintervention group patients was also encouraged by a phonecall 2 days after the start of therapy.
ComplianceCompliance was assessed by phone interview on day 10 oftherapy and by returned tablet count at the follow-up13C-UBT visit. Patients were defined as compliant if they wereassessed by both pill count and interview as taking$80% ofstudy medications. Total percentage of tablets taken in bothgroups was assessed by taking the lower of the two esti-mates of tablet consumption (pill count or interview data)for each patient.
Side EffectsSide effects were assessed by phone interview on day 10 oftherapy and by returned side effects form. Patients wereasked to rate specific side effects and give an overall ratingwhere none5 0, mild 5 1 (does not limit daily activities),moderate5 2 (interferes with daily activities), and severe53 (incapacitating, stops normal daily activities).
Follow-up13C-Urea breath test using kits sent to a single centrallaboratory for analysis was performed$1 month after ces-sation of H. pylori treatment and any other antimicrobial
therapy (including bismuth), 2 wk after cessation of proton-pump inhibitor therapy and 1 wk after cessation of hista-mine-receptor antagonists. An increase of 5 per million inthe13CO2 30 min after ingestion of13C-urea compared withbaseline measurement was considered positive forH. pylori.Treatment was considered successful if13C-UBT was neg-ative.
Statistical AnalysisThex2 and Fisher’s exact test were used to compare the twogroups at baseline, differences in outcome, compliance, andside effects in the two groups, and to identify univariatepredictors of treatment outcome. An exact 95% confidenceinterval (CI) was calculated when appropriate. An all pa-tients treated analysis (APT) was conducted for outcome inwhich all patients with known outcome were included. Aconservative intention to treat (ITT) analysis of outcomewas also conducted, assuming that patients not undergoing13C-UBT had failed treatment. Per protocol (PP) analysis,excluding patients who withdrew from the study, were lostto follow up, were noncompliant, or did not have13C-UBTas per protocol, was also performed. Side effects and com-pliance analysis was based on all patients for whom datawere available. Allp values,0.05 were considered to besignificant, and all tests of significance used were two tailed.A stepwise logistic regression model including sex, age,study group and factors with ap value,0.25 in univariateanalysis was constructed to determine factors predictive oftreatment failure.
EthicsEthical approval was obtained from the Hunter Area Re-search Ethics Committee and The University of Newcastle.Specific permission to avoid bias by concealing from pa-tients the compliance-enhancing purpose of the study anddifferences between study groups was granted on thepro-visothat patients be aware that they were participating in anH. pylori treatment trial and be well informed about theirstudy treatment. Written informed consent was obtainedfrom all patients.
RESULTS
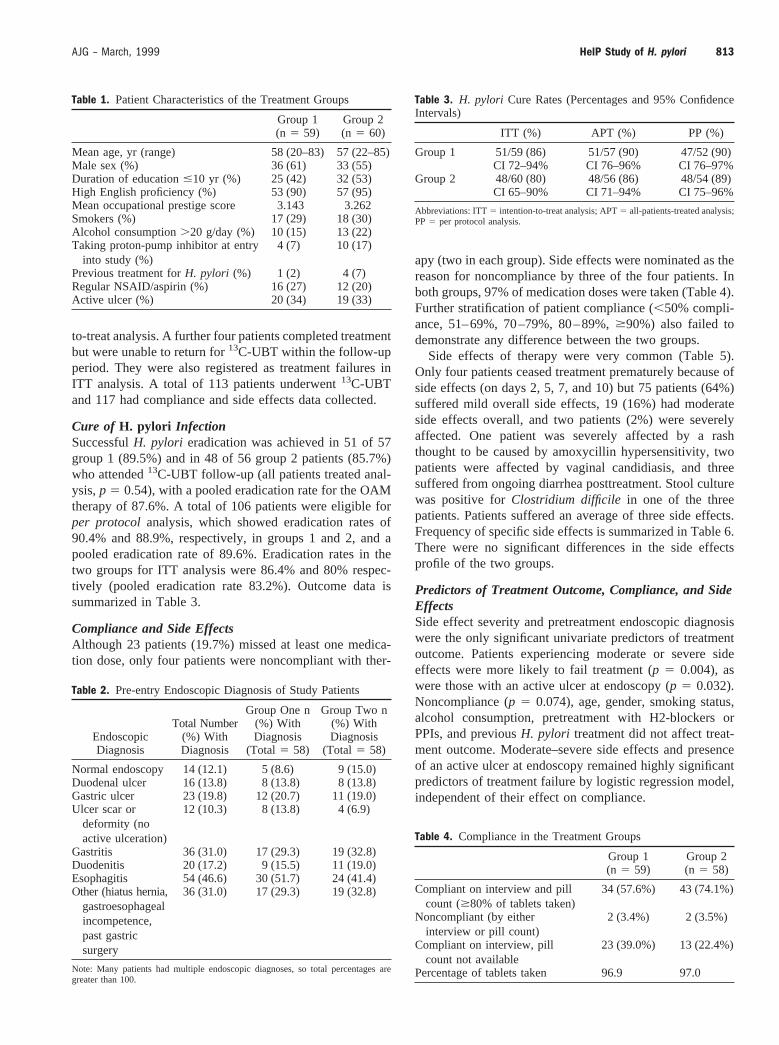
A total of 119 patients were studied. Characteristics ofpatients in the two treatment groups (group 15 control,group 25 intervention) are shown in Table 1 and pre-entryendoscopic diagnoses in Table 2. There were no significantdifferences between the two study groups at entry. Anadditional 54 patients were excluded. Nineteen exclusionswere because of consultant recommendation that the patientnot be treated, 13 patients had a contraindication to the studymedication, eight patients were unable to give informedconsent, and five refused consent or were not contactable.Five patients had treatment supervised by their consultant,and four were long term inpatients.
Two patients, both in group 2, withdrew from the studyand were registered as treatment failures in the intention-
812 Henry and Batey AJG – Vol. 94, No. 3, 1999
to-treat analysis. A further four patients completed treatmentbut were unable to return for13C-UBT within the follow-upperiod. They were also registered as treatment failures inITT analysis. A total of 113 patients underwent13C-UBTand 117 had compliance and side effects data collected.
Cure of H. pylori InfectionSuccessfulH. pylori eradication was achieved in 51 of 57group 1 (89.5%) and in 48 of 56 group 2 patients (85.7%)who attended13C-UBT follow-up (all patients treated anal-ysis,p 5 0.54), with a pooled eradication rate for the OAMtherapy of 87.6%. A total of 106 patients were eligible forper protocol analysis, which showed eradication rates of90.4% and 88.9%, respectively, in groups 1 and 2, and apooled eradication rate of 89.6%. Eradication rates in thetwo groups for ITT analysis were 86.4% and 80% respec-tively (pooled eradication rate 83.2%). Outcome data issummarized in Table 3.
Compliance and Side EffectsAlthough 23 patients (19.7%) missed at least one medica-tion dose, only four patients were noncompliant with ther-
apy (two in each group). Side effects were nominated as thereason for noncompliance by three of the four patients. Inboth groups, 97% of medication doses were taken (Table 4).Further stratification of patient compliance (,50% compli-ance, 51–69%, 70–79%, 80–89%,$90%) also failed todemonstrate any difference between the two groups.
Side effects of therapy were very common (Table 5).Only four patients ceased treatment prematurely because ofside effects (on days 2, 5, 7, and 10) but 75 patients (64%)suffered mild overall side effects, 19 (16%) had moderateside effects overall, and two patients (2%) were severelyaffected. One patient was severely affected by a rashthought to be caused by amoxycillin hypersensitivity, twopatients were affected by vaginal candidiasis, and threesuffered from ongoing diarrhea posttreatment. Stool culturewas positive forClostridium difficile in one of the threepatients. Patients suffered an average of three side effects.Frequency of specific side effects is summarized in Table 6.There were no significant differences in the side effectsprofile of the two groups.
Predictors of Treatment Outcome, Compliance, and SideEffectsSide effect severity and pretreatment endoscopic diagnosiswere the only significant univariate predictors of treatmentoutcome. Patients experiencing moderate or severe sideeffects were more likely to fail treatment (p 5 0.004), aswere those with an active ulcer at endoscopy (p 5 0.032).Noncompliance (p 5 0.074), age, gender, smoking status,alcohol consumption, pretreatment with H2-blockers orPPIs, and previousH. pylori treatment did not affect treat-ment outcome. Moderate–severe side effects and presenceof an active ulcer at endoscopy remained highly significantpredictors of treatment failure by logistic regression model,independent of their effect on compliance.
Table 1. Patient Characteristics of the Treatment Groups
Group 1(n 5 59)
Group 2(n 5 60)
Mean age, yr (range) 58 (20–83) 57 (22–85)Male sex (%) 36 (61) 33 (55)Duration of education#10 yr (%) 25 (42) 32 (53)High English proficiency (%) 53 (90) 57 (95)Mean occupational prestige score 3.143 3.262Smokers (%) 17 (29) 18 (30)Alcohol consumption.20 g/day (%) 10 (15) 13 (22)Taking proton-pump inhibitor at entry
into study (%)4 (7) 10 (17)
Previous treatment forH. pylori (%) 1 (2) 4 (7)Regular NSAID/aspirin (%) 16 (27) 12 (20)Active ulcer (%) 20 (34) 19 (33)
Table 2. Pre-entry Endoscopic Diagnosis of Study Patients
EndoscopicDiagnosis
Total Number(%) WithDiagnosis
Group One n(%) WithDiagnosis
(Total 5 58)
Group Two n(%) WithDiagnosis
(Total 5 58)
Normal endoscopy 14 (12.1) 5 (8.6) 9 (15.0)Duodenal ulcer 16 (13.8) 8 (13.8) 8 (13.8)Gastric ulcer 23 (19.8) 12 (20.7) 11 (19.0)Ulcer scar or
deformity (noactive ulceration)
12 (10.3) 8 (13.8) 4 (6.9)
Gastritis 36 (31.0) 17 (29.3) 19 (32.8)Duodenitis 20 (17.2) 9 (15.5) 11 (19.0)Esophagitis 54 (46.6) 30 (51.7) 24 (41.4)Other (hiatus hernia,
gastroesophagealincompetence,past gastricsurgery
36 (31.0) 17 (29.3) 19 (32.8)
Note: Many patients had multiple endoscopic diagnoses, so total percentages aregreater than 100.
Table 3. H. pylori Cure Rates (Percentages and 95% ConfidenceIntervals)
ITT (%) APT (%) PP (%)
Group 1 51/59 (86) 51/57 (90) 47/52 (90)CI 72–94% CI 76–96% CI 76–97%
Group 2 48/60 (80) 48/56 (86) 48/54 (89)CI 65–90% CI 71–94% CI 75–96%
Abbreviations: ITT5 intention-to-treat analysis; APT5 all-patients-treated analysis;PP5 per protocol analysis.
Table 4. Compliance in the Treatment Groups
Group 1(n 5 59)
Group 2(n 5 58)
Compliant on interview and pillcount ($80% of tablets taken)
34 (57.6%) 43 (74.1%)
Noncompliant (by eitherinterview or pill count)
2 (3.4%) 2 (3.5%)
Compliant on interview, pillcount not available
23 (39.0%) 13 (22.4%)
Percentage of tablets taken 96.9 97.0
813AJG – March, 1999 HelP Study of H. pylori
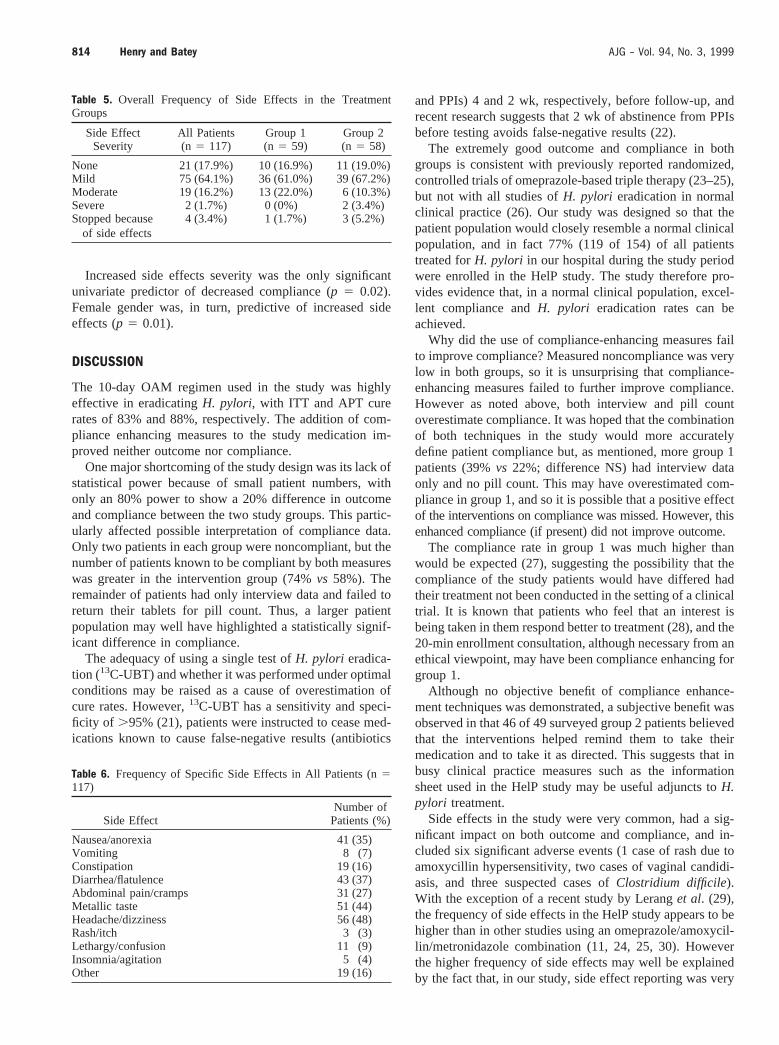
Increased side effects severity was the only significantunivariate predictor of decreased compliance (p 5 0.02).Female gender was, in turn, predictive of increased sideeffects (p 5 0.01).
DISCUSSION
The 10-day OAM regimen used in the study was highlyeffective in eradicatingH. pylori, with ITT and APT curerates of 83% and 88%, respectively. The addition of com-pliance enhancing measures to the study medication im-proved neither outcome nor compliance.
One major shortcoming of the study design was its lack ofstatistical power because of small patient numbers, withonly an 80% power to show a 20% difference in outcomeand compliance between the two study groups. This partic-ularly affected possible interpretation of compliance data.Only two patients in each group were noncompliant, but thenumber of patients known to be compliant by both measureswas greater in the intervention group (74%vs 58%). Theremainder of patients had only interview data and failed toreturn their tablets for pill count. Thus, a larger patientpopulation may well have highlighted a statistically signif-icant difference in compliance.
The adequacy of using a single test ofH. pylori eradica-tion (13C-UBT) and whether it was performed under optimalconditions may be raised as a cause of overestimation ofcure rates. However,13C-UBT has a sensitivity and speci-ficity of .95% (21), patients were instructed to cease med-ications known to cause false-negative results (antibiotics
and PPIs) 4 and 2 wk, respectively, before follow-up, andrecent research suggests that 2 wk of abstinence from PPIsbefore testing avoids false-negative results (22).
The extremely good outcome and compliance in bothgroups is consistent with previously reported randomized,controlled trials of omeprazole-based triple therapy (23–25),but not with all studies ofH. pylori eradication in normalclinical practice (26). Our study was designed so that thepatient population would closely resemble a normal clinicalpopulation, and in fact 77% (119 of 154) of all patientstreated forH. pylori in our hospital during the study periodwere enrolled in the HelP study. The study therefore pro-vides evidence that, in a normal clinical population, excel-lent compliance andH. pylori eradication rates can beachieved.
Why did the use of compliance-enhancing measures failto improve compliance? Measured noncompliance was verylow in both groups, so it is unsurprising that compliance-enhancing measures failed to further improve compliance.However as noted above, both interview and pill countoverestimate compliance. It was hoped that the combinationof both techniques in the study would more accuratelydefine patient compliance but, as mentioned, more group 1patients (39%vs 22%; difference NS) had interview dataonly and no pill count. This may have overestimated com-pliance in group 1, and so it is possible that a positive effectof the interventions on compliance was missed. However, thisenhanced compliance (if present) did not improve outcome.
The compliance rate in group 1 was much higher thanwould be expected (27), suggesting the possibility that thecompliance of the study patients would have differed hadtheir treatment not been conducted in the setting of a clinicaltrial. It is known that patients who feel that an interest isbeing taken in them respond better to treatment (28), and the20-min enrollment consultation, although necessary from anethical viewpoint, may have been compliance enhancing forgroup 1.
Although no objective benefit of compliance enhance-ment techniques was demonstrated, a subjective benefit wasobserved in that 46 of 49 surveyed group 2 patients believedthat the interventions helped remind them to take theirmedication and to take it as directed. This suggests that inbusy clinical practice measures such as the informationsheet used in the HelP study may be useful adjuncts toH.pylori treatment.
Side effects in the study were very common, had a sig-nificant impact on both outcome and compliance, and in-cluded six significant adverse events (1 case of rash due toamoxycillin hypersensitivity, two cases of vaginal candidi-asis, and three suspected cases ofClostridium difficile).With the exception of a recent study by Leranget al. (29),the frequency of side effects in the HelP study appears to behigher than in other studies using an omeprazole/amoxycil-lin/metronidazole combination (11, 24, 25, 30). Howeverthe higher frequency of side effects may well be explainedby the fact that, in our study, side effect reporting was very
Table 5. Overall Frequency of Side Effects in the TreatmentGroups
Side EffectSeverity
All Patients(n 5 117)
Group 1(n 5 59)
Group 2(n 5 58)
None 21 (17.9%) 10 (16.9%) 11 (19.0%)Mild 75 (64.1%) 36 (61.0%) 39 (67.2%)Moderate 19 (16.2%) 13 (22.0%) 6 (10.3%)Severe 2 (1.7%) 0 (0%) 2 (3.4%)Stopped because
of side effects4 (3.4%) 1 (1.7%) 3 (5.2%)
Table 6. Frequency of Specific Side Effects in All Patients (n5117)
Side EffectNumber ofPatients (%)
Nausea/anorexia 41 (35)Vomiting 8 (7)Constipation 19 (16)Diarrhea/flatulence 43 (37)Abdominal pain/cramps 31 (27)Metallic taste 51 (44)Headache/dizziness 56 (48)Rash/itch 3 (3)Lethargy/confusion 11 (9)Insomnia/agitation 5 (4)Other 19 (16)
814 Henry and Batey AJG – Vol. 94, No. 3, 1999
comprehensive, including all adverse events mentioned bypatients either during phone interview on day 10 or on thepatient side effects form.
CONCLUSIONS
In a randomized clinical trial comparing eradication rates in10 days OAMversus10 days OAM plus compliance en-hancing measures both treatment regimens were found to beeffective, with cure rates of 90% and 86%, respectively.Attempts to increase compliance in the intervention groupimproved neither compliance nor outcome above that of thecontrol group. OAM was less effective in a subgroup ofpatients with moderate-severe overall side effects and asubgroup of patients with active ulceration pretreatment.Side effects were of importance in our study as determinantsof both outcome and compliance.
ACKNOWLEDGMENTS
Thank you to Sr. E. Ianna for her help in carrying out the13C-urea breath testing. Thanks to Dr. E. Hewson, Dr. A.Lewis, Dr. N. Porter, Dr. G. Radvan, Dr. D. Routley, Dr. E.Smith, Dr. C. Thursby, and Dr. D. Vakil for their help inpatient recruitment.
Reprint requests and correspondence:Professor R. Batey, Gas-troenterology Department, John Hunter Hospital, Locked Bag No1, Hunter Region Mail Centre NSW 2310, Australia.
Received Apr. 16, 1998; accepted Oct. 7, 1998.
REFERENCES
1. Penston JG.Helicobacter pylorieradication—understandablecaution but no excuse for inertia. Aliment Pharmacol Ther1994;8:369–89.
2. Unge P. Review ofHelicobacter pylorieradication regimens.Scand J Gastroenterol 1996;31(Suppl 215):74–81.
3. Moshkowitz M, Konikoff FM, Peled Y, et al. One week tripletherapy with omeprazole, clarithromycin and tinidazole forHelicobacter pylori: Differing efficacy in previously treated anduntreated patients. Aliment Pharmacol Ther 1996;10:1015–9.
4. Graham DY, de Boer WA, Tytgat GA. Choosing the bestanti-Helicobacter pyloritherapy: Effect of antimicrobial re-sistance. Am J Gastroenterol 1996;91:1072–6.
5. Moayyedi P, Chalmers DM, Axon AT. Patient factors that predictfailure of omeprazole, clarithromycin and tinidazole to eradicateHelicobacter pylori. Eur J Gastroenterol 1997;32:124–7.
6. Graham DY, Lew GM, Malaty HM, et al. Factors influencingthe eradication ofHelicobacter pylori with triple therapy.Gastroenterology 1992;102:493–6.
7. Cutler AF, Schubert H. Patient factors affectingHelicobacterpylori eradication with triple therapy. Am J Gastroenterol1993;88:505–9.
8. Malfertheiner P. Compliance, adverse events and antibioticresistance inHelicobacter pyloritreatment. Scand J Gastro-enterol 1993;28(Suppl 196):34–7.
9. Delchier JC, Elamine I, Goldfain P, et al. Omeprazole-amoxy-cillin versus omeprazole-amoxycillin-clarithromycin in theeradication ofHelicobacter pylori. Aliment Pharmacol Ther1996;10:263–8.
10. Rautelin H, Seppala K, Retikonen OV, et al. Role of metro-
nidazole resistance in treatment ofHelicobacter pyloriinfec-tions. Antimicrob Agents Chemother 1992;36:163–6.
11. Bell GD, Powell KU, Burridge SM, et al.Helicobacter pylorieradication: Efficacy and side effect profile of a combinationof omeprazole, amoxycillin and metronidazole compare with 4alternative regimens. Q J Med 1993;86:743–50.
12. Moayyedi P, Sahay P, Tompkins DS, et al. Efficacy andoptimum dose of omeprazole in a new 1-week triple therapyregimen to eradicateHelicobacter pylori. Eur J GastroenterolHepatol 1995;7:835–40.
13. Abrahams J. Patient compliance in general practice. Aust FamPhysician 1977;6:1200–5.
14. Ettlinger PRA, Freeman JK. General practice compliancestudy: Is it worth being a personal doctor? Br Med J 1981 Apr11;282:1192–4.
15. Bergmann AB, Werner RJ. Failure of children to receivepenicillin by mouth. N Engl J Med 1965;268:1334–8.
16. Chiba N. Omeprazole and clarithromycin with and withoutmetronidazole for the eradication ofHelicobacter pylori. Am JGastroenterol 1996;91:2139–43.
17. Jaup BH, Norrby A. Low dose, short-term triple therapy forcure of Helicobacter pylori infection and healing of pepticulcers. Am J Gastroenterol 1995;90:943–5.
18. Laine L, Estrada R, Trujillo M, et al. Randomised comparisonof differing periods of twice a day triple therapy for theeradication ofHelicobacter pylori. Aliment Pharmacol Ther1996;10:1029–33.
19. Pullar T, Kumar S, Tindall H, et al. Time to stop counting thetablets? Clin Pharmacol Ther 1989;46:163–8.
20. Stephenson BJ, Rowe BH, Haynes RB, et al. Is this patient takingthe treatment as prescribed? JAMA 1993;269:2779–81.
21. Thijs JC, van Zwet AA, Thijs WJ, et al. Diagnostic tests forHelicobacter pylori: A prospective evaluation of their accu-racy, without selecting a single test as the gold standard. Am JGastroenterol 1996;91:2125–9.
22. Laine L, Estrada R, Trujillo M, et al. Prospective evaluation ofthe effect of proton pump inhibitor therapy onH. pyloridiagnostic testing. Gastroenterology 1998;11:A193 (abstract).
23. Bell GD, Bate CM, Axon AT, et al. Addition of metronidazoleto omeprazole/amoxycillin dual therapy increases the rate ofHelicobacter pylorieradication: A double-blind, randomizedtrial. Aliment Pharmacol Ther 1995;9:513–20.
24. Lind T, Veldhuyzen van Zanten S, Unge P, et al. Eradicationof Helicobacter pyloriusing one-week triple therapies com-bining omeprazole with two antimicrobials: The MACH 1study.Helicobacter1996;1:138–44.
25. Thijs JC, Van-Zwet AA, Thijs WJ, et al. One week tripletherapy with omeprazole, amoxycillin and tinidazole forHel-icobacter pyloriinfection: The significance of metronidazoleresistance. Aliment Pharmacol Ther 1997;11:305–9.
26. Deltenre M, Jonas C, Burette A, et al. Bazzoli-like schemes arenot optimal treatment for HP eradication in Brussels, Belgium.Gastroenterology 1996;110:A93 (abstract).
27. Haynes RB, McKibbon KA, Kanani R. Systematic review ofrandomised trials of interventions to assist patients to followprescriptions for medications. Lancet 1996;348:383–6.
28. Peck DF. Measurement in psychiatry. In: Kendell RE, ZealheyAK, eds. Companion to psychiatric studies, 5th ed. London:Churchill Livingstone, 1993:169–86.
29. Lerang F, Moum B, Haug JB. Highly effective twice dailytriple therapies forHelicobacter pylori infection and pepticulcer disease: Does in vitro metronidazole resistance have anyclinical relevance? Am J Gastroenterol 1997;92:248–54.
30. Annibale B, D’Ambra G, Luzzi I, et al. Does pretreatment withomeprazole decrease the chance of eradication ofHelicobacterpylori in peptic ulcer patients? Am J Gastroenterol 1997;92:790–4.
815AJG – March, 1999 HelP Study of H. pylori