endometrial cycle and infertility dr.rahul,physiology,sms mc jaipur email [email protected]...
TRANSCRIPT

GOOD MORNING
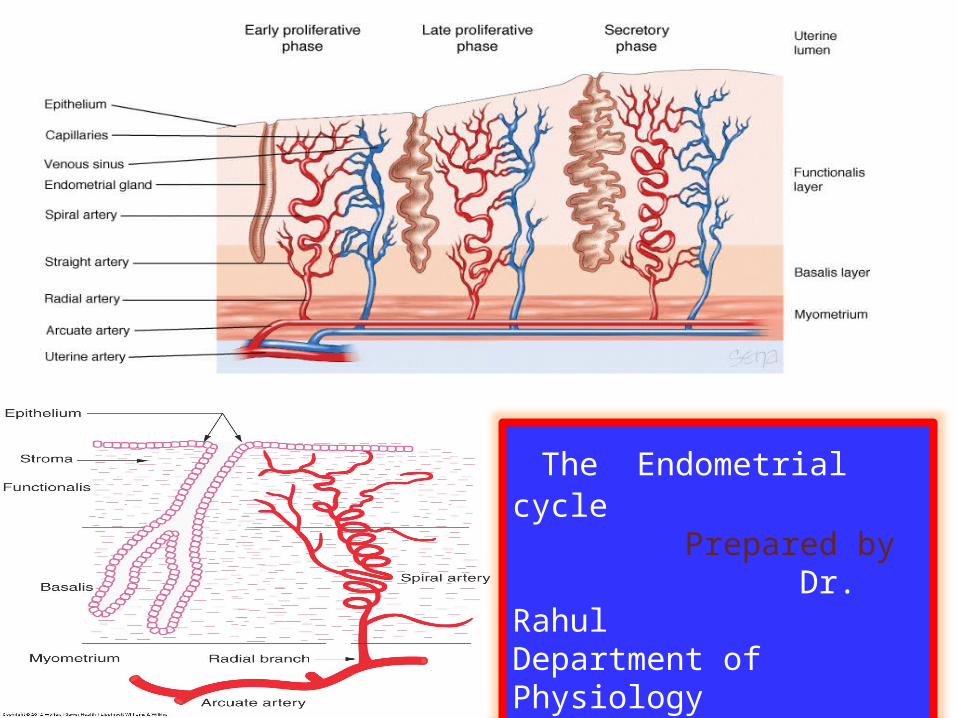
The Endometrial cycle Prepared by Dr. RahulDepartment of PhysiologySMS Medical College Jaipur
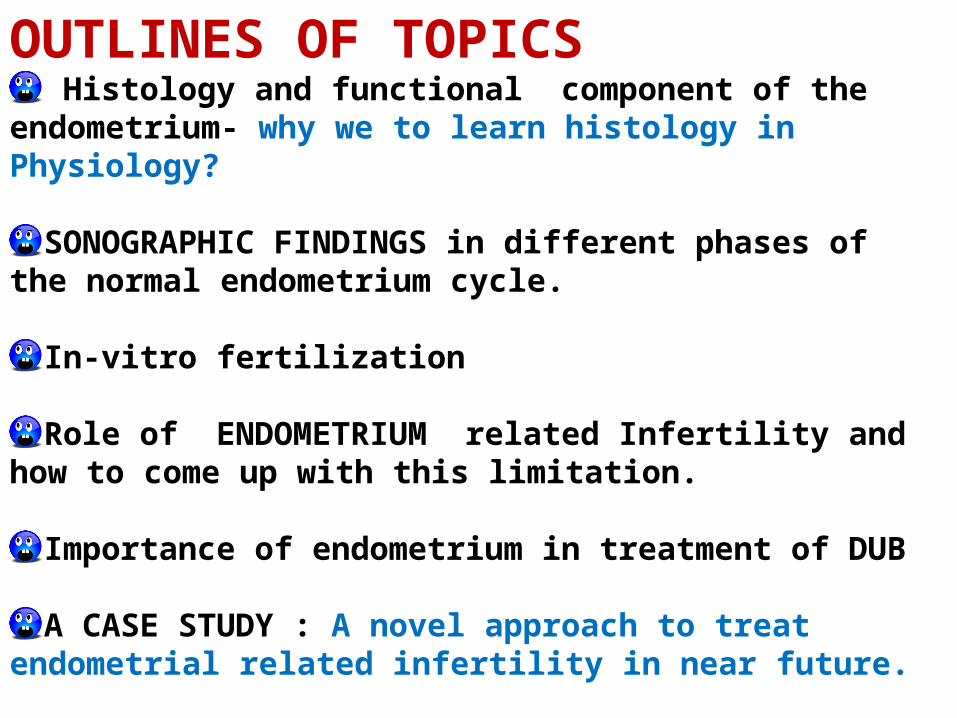
OUTLINES OF TOPICS Histology and functional component of the
endometrium- why we to learn histology inPhysiology?
SONOGRAPHIC FINDINGS in different phases of the normal endometrium cycle.
In-vitro fertilization
Role of ENDOMETRIUM related Infertility and how to come up with this limitation.
Importance of endometrium in treatment of DUB
A CASE STUDY : A novel approach to treat endometrial related infertility in near future.
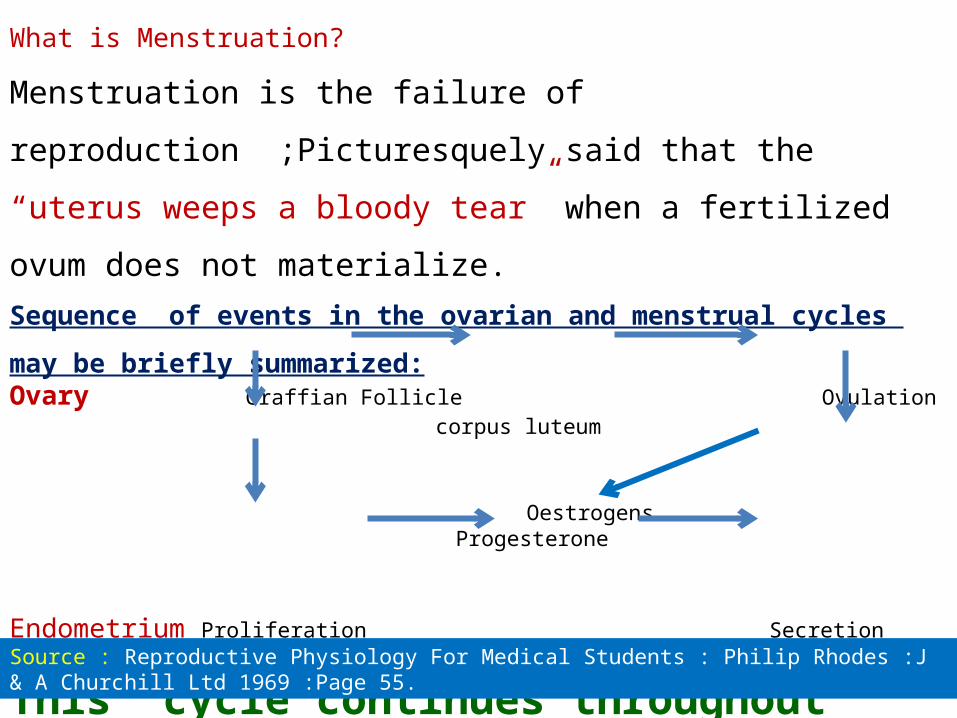
What is Menstruation?
Menstruation is the failure of reproduction ;Picturesquely said that
the “uterus weeps a bloody tear” when a fertilized ovum does not
materialize.
Sequence of events in the ovarian and menstrual cycles may
be briefly summarized:Ovary Graffian Follicle Ovulation corpus luteum
Oestrogens Progesterone
Endometrium Proliferation Secretion Menstruation
This cycle continues throughout reproductive life unless interrupted by childbirth or disease.
Source : Reproductive Physiology For Medical Students : Philip Rhodes :J & A Churchill Ltd 1969 :Page 55.
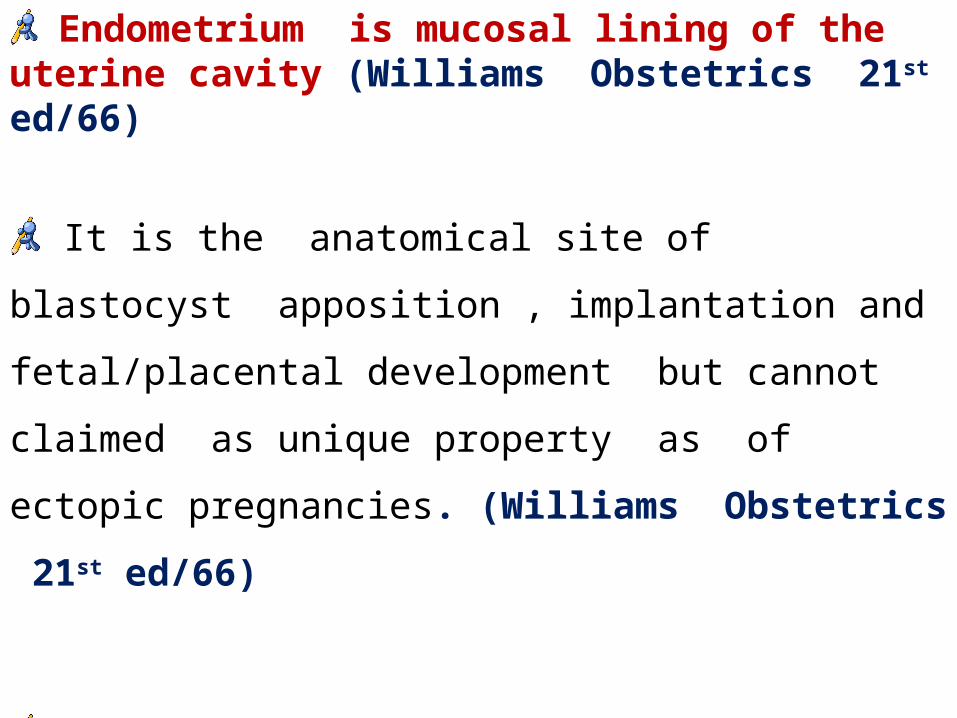
Endometrium is mucosal lining of the uterine cavity (Williams Obstetrics 21st ed/66)
It is the anatomical site of blastocyst apposition ,
implantation and fetal/placental development but cannot
claimed as unique property as of ectopic pregnancies.
(Williams Obstetrics 21st ed/66)
Endometrium is one principal target tissue of the
pituitary-gonadal axis, but has also been recognized as
an endocrine organ itself. (journal.1.)
Endometrium is formed by fusion of the mullerian ducts
between 8th and 9th post ovulatory weeks. (Blaustein's
Pathology/5th ed /chap9/383)
Until 20th week of gestation the endometrium is composed of
single layer of columnar epithelium supported by a thick layer of
fibroblastic stroma. (Blaustein's Pathology/5th ed /chap9/383)
By 20th week of gestation ,the surface epithelium invaginates
into the underlying stroma forming glandular structures that
extend towards the underlying myometrium.(Blaustein'sPathology)
EMBRYOLOGY OF ENDOMETRIUM
At birth uterus measures about 4 cm in length much of
which is made of cervix .the endometrial surface and
glands are lined by low columnar to cuboidal
epithelium ,which resembles as inactive endometrium
seen in menopause. (Blaustein's Pathology/5th ed /chap9/383)
The endometrium during the reproductive period
undergoes cyclic morphologic changes. (Blaustein's
Pathology/5th ed /chap9/383)
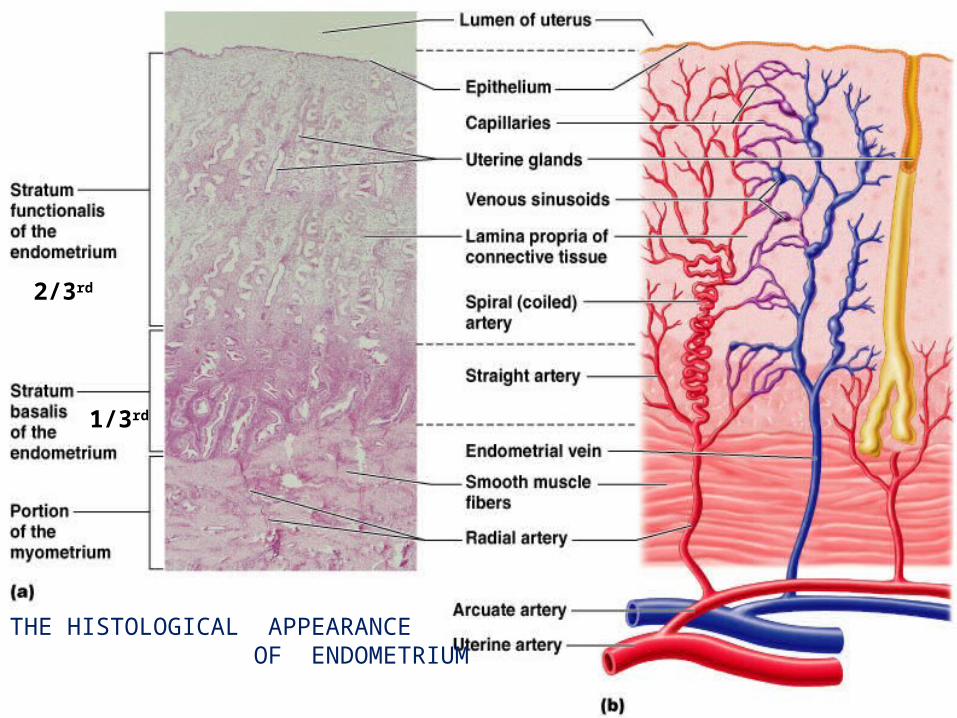
THE HISTOLOGICAL APPEARANCE OF ENDOMETRIUM
2/3rd
1/3rd
Histologically it is divided into two layers (Dutta’s textbook gynaecology;chap7/82)
Stratum basalis :
1/3 rd of total depth of the endometrium and lies in contact with the
myometrium.
Uninfluenced by hormones and no cyclic changes occur .
Supplied by basal arteries .
After shedding of superficial part during menstruation the regeneration
occurs from this zone.
It measures about 1mm.
Stratum functionalis :
Superficial 2/3rd of the endometrium that proliferates and ultimately
shed if pregnancy does not occur.
This zone is under the influence of fluctuating cyclic ovarian
hormones ,estrogen and progesterone.
The Uterine Endometrial Cycle can be divided into four phases: (Dutta’s textbook of gynaecology;chap7/83)
Stage of Regeneration
Proliferative (Preovulatory or follicular or estrogen )phase
Secretory (Postovulatory or luteal or progesterone ) phase
Mestrual phase
By convention first day of vaginal bleeding is called Day 1 of the
menstrual cycle.(Novak’s Gynecology 13th ed/159)
The first 4 days are occupied with menstruation.The remaining 24
days of the endometrial cycle consists of Proliferative and Secretory
phase. (Jeffcoate’s Gynecology 7th ed/79)
Proliferation Phase:
Extends from 5th or 6th day to 14th day .(1)
Proliferative changes occurs due to rise in level of
ovarian estrogens.(1)
Proliferation of all elements at first slowly but later on
rapidly.(2)
In early proliferative phase (Day 5 to 7) :
the endometrium is less than 2mm in thickness with
narrow straight glands.(2)
Glandular epithelium is composed of cubo-columnar
cells with moderately basophilic cytoplasm and oval or
rounded nuclei in which chromatin is coarse.(8)
Occasional mitoses in both glandular epithelium and
stroma.(5&8)
Stromal cells are oval to elongated with scanty
cytoplasm and oval ,rounded nuclei in which mitoses
are seen.(8)
In mid proliferative and late proliferative phase :
Proliferative activity reaches its maximum between 8th -10th
days of the cycle and by then glandular epithelium is taller.(8)
Epithelium becomes columnar and frequent mitosis is seen
in both glands and stroma .(1,8)
The glandular epithelial cells increases in size and become
pseudostratified(4)
Pseudostratified results because the resting nuclei
occupy basal position while actively dividing nuclei
occupy apical position(4)
Late proliferative phase(Day 11-14 of cycle )
:
The glandular growth out-strips that of the stromal as a
result glands become more convoluted and tortuous. (8)
Glandular epithelium shows marked Pseudostratification(4)
There is increase in stromal ground substance ,which is
edema . (3)
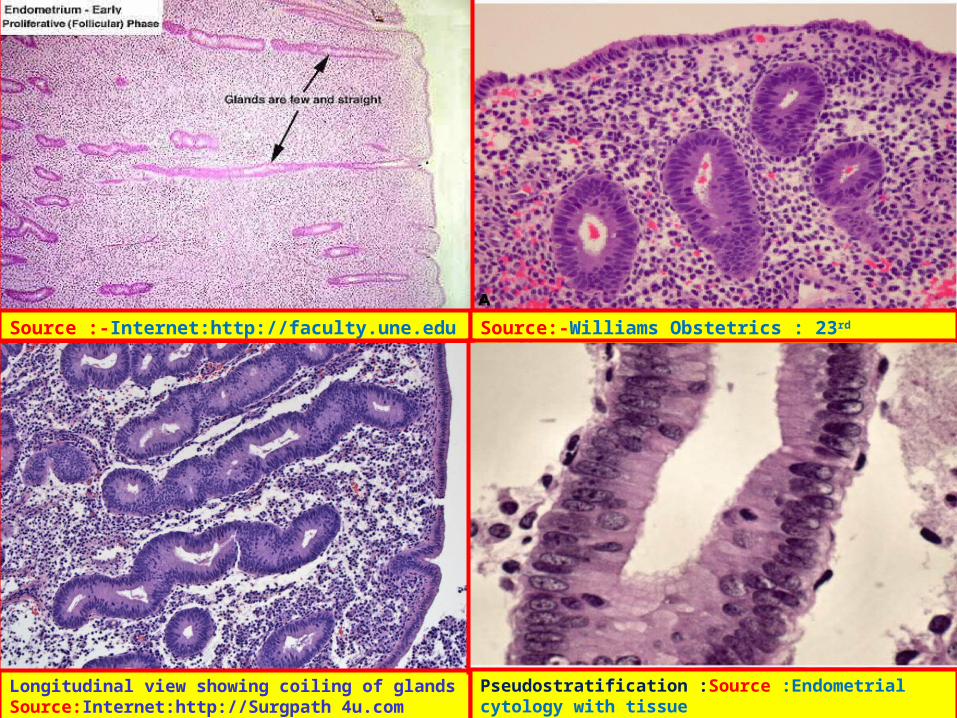
Source :-Internet:http://faculty.une.edu Source:-Williams Obstetrics : 23rd ed/fig.3.2A
Longitudinal view showing coiling of glands Source:Internet:http://Surgpath 4u.com
Pseudostratification :Source :Endometrial cytology with tissue correlations :Maksem .J.A et al:2009: Springer
Under the influence of Estrogen in the proliferative phase of
the cycle , the predominant activity is that of growth reflected
by increase in RNA in the glandular epithelium . (8)
The evidence of cellular proliferation has been demonstrated
by presence of Ki-67. (8)
Estrogens induces synthesis of growth factors like insulin-
like growth factors (IGFs, also called somatomedins;), TGFs,
and epidermal growth factor (EGF). These autocrine and
paracrine mediators are necessary for maturation and growth
of the endometrium. (6)
Tissue breakdown and Apoptosis is not characterstic in
Proliferative phase. (8)
Factors such as bcl-2 which blocks the apoptosis
pathway and causes cell persistence is high while factors
which promotes apoptosis like M30 reactivity are low but
in contrast ,in Secretory Phase the bcl-2 is low while M30
reactivity is high. (8)
Increased mitotic activity of the stromal and glandular
epithelium continues throughout the follicular phase of the
cycle and beyond, until approximately 3 days after ovulation(6)
The thickness of the endometrium increases from about 0.5 to
as much as 5 mm during the proliferative phase.(6)
Levels of estrogen rise early in the follicular phase and peak just
before ovulation.(6)
Levels of endometrial estrogen receptor are highest during the
proliferative phase and decline after ovulation in response to
changing levels of progesterone. (6)
Estrogen induces synthesis of progestin receptors in
endometrial tissue. (6)
Levels of progestin receptors peak at ovulation, when
estrogen levels are highest, to prepare the cells for the
high progestin levels of the luteal phase of the cycle. (6)
Estrogen causes the stromal components of the
endometrium to become highly developed. (6)
Progesterone, opposes the action of estrogen on the
epithelial cells of the endometrium and inhibits epithelial
cell proliferation. (6)
Day to day dating of the endometrium by histological
criteria is not possible during proliferative phase because of
considerable variation among women in the length of pre
ovulatory phase of the cycle .Secretory phase of cycle is
constant in duration.(3) is dictated by the fixed lifespan of the
corpus luteum. (7)
In normal fertile women the follicular phase may be as
short as 5 to 7 days and as long as 21 to 30 days. (3)
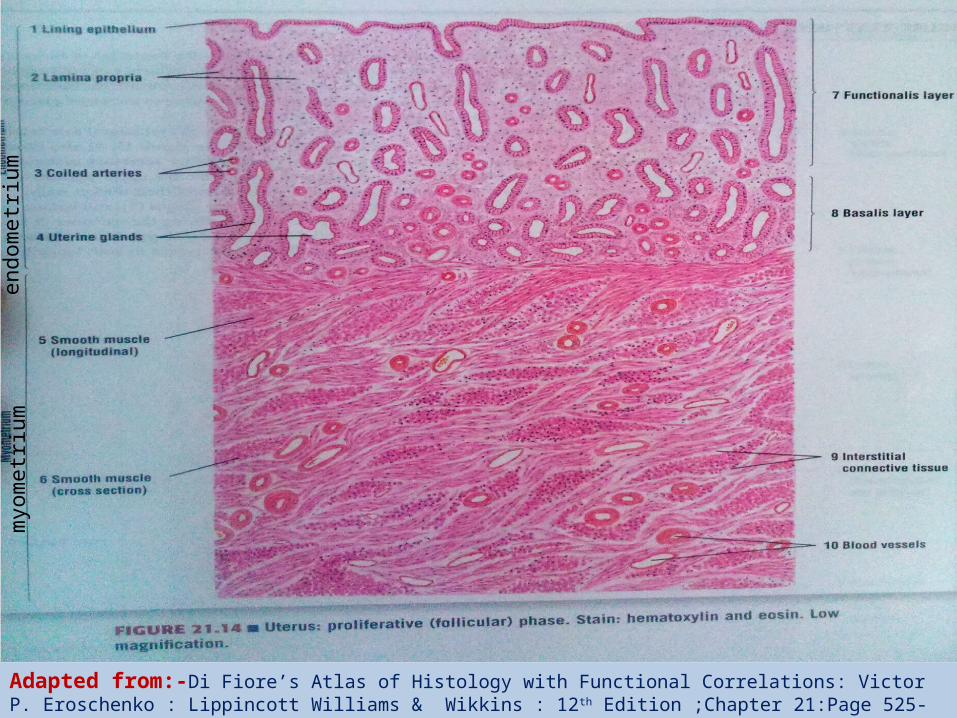
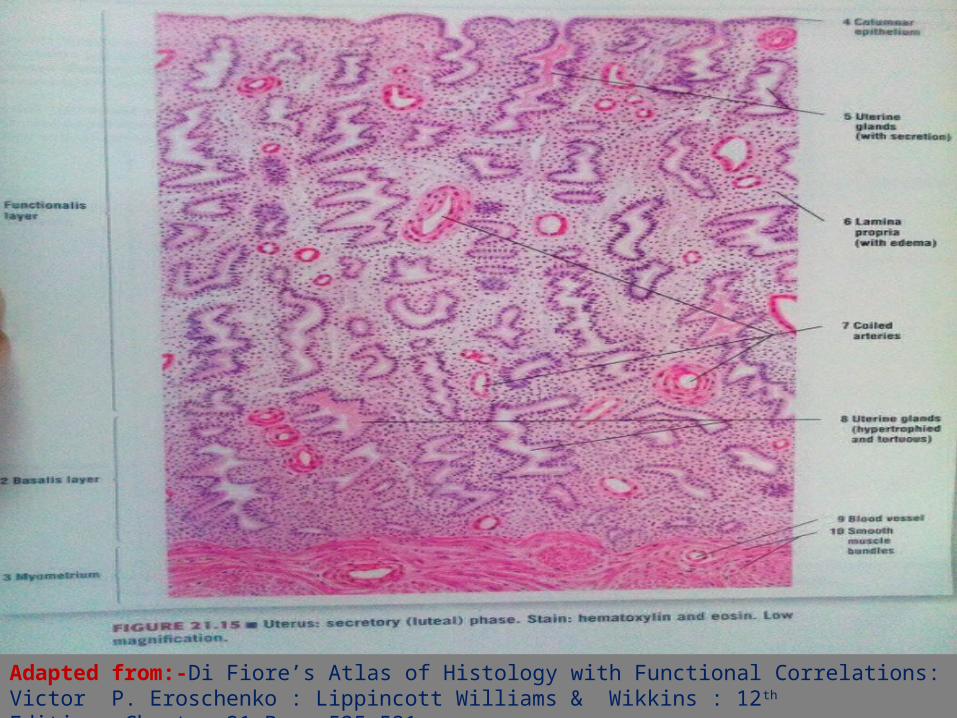
Adapted from:-Di Fiore’s Atlas of Histology with Functional Correlations: Victor P. Eroschenko : Lippincott Williams & Wikkins : 12th Edition ;Chapter 21:Page 525-531
myom
etr
ium
endom
etr
ium
Secretory Phase:
Secretory phase of endometrial cycle starts at
ovulation.(4)
The changes in the components are due to combined
effects of estrogen and progesterone liberated from the
corpus luteum after ovulation .(1)
The Progesterone can only act on the endometrium
previously primed by estrogen (1 & 3)
During this period the endometrium continues to grow
and reach a thickness of around 7 mm .Postovulatory
first 3 days the epithelial cells still undergo mitosis
thereafter mitosis ceases in the glandular epithelium but
can be seen in the stromal cells. (2)
By the Day 17 of the cycle , glycogen accumulates in
the basal portion of glandular epithelium creating
subnuclear vacuoles . This is the first sign of
ovulation that is histologically evident likely due to
direct progesterone action through receptors expressed
in glandular cells. (3)
Day 18, vacuoles move towards the apical portion of
the glandular lumen and pushes the nucleus to the base
of the cell. (3 & 2)
By Day 19-22 , the secretion enters the gland lumen .
This secretion is rich in glycogen ,fructose ,glucose and
has nutritive function for any fertilized ovum reaching the
uterus . (2)
Glandular cell mitosis ceases with secretory activity on
Day 19 due to rising progesterone levels, which
antagonize the mitotic effects of estrogen. (3)
Progesterone exerts its primary antiestrogen effects by
stimulating 17β-HSD and sulfotransferase, enzymes that
convert estradiol to weaker compounds which are
biologically less active compounds. (Journal.2& 3& 6)
Postovulatory day 6-7 (Day 20-21 by cycle )
secretory activity of the gland is maximal and the
endometrium is optimally prepared for
implantation of the blastocyst. (9) . This period has
been called The Implantation Window (Journal.2 & 3)
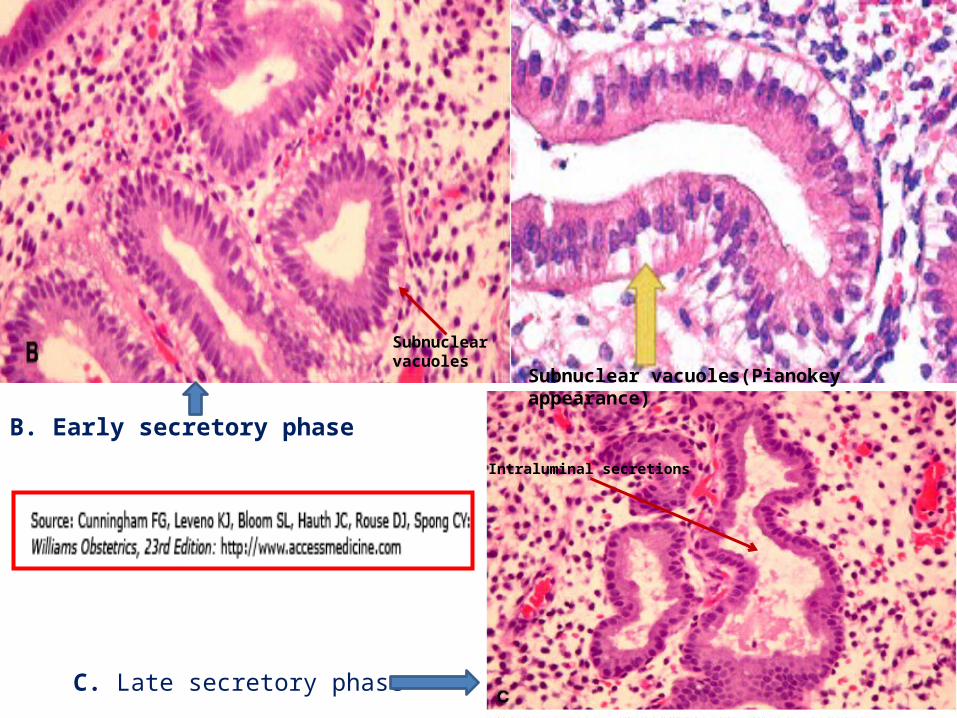
Subnuclear vacuoles(Pianokey appearance)
Subnuclear vacuoles
B. Early secretory phase
Intraluminal secretions
C. Late secretory phase
Ultrastructurally, pinopodes are evidenced during this
period, indicating that the endometrial surface epithelium is
receptive to the eventual implantation of a blastocyst.
(Journal.2 & 3)
The endometrial glands are engorged with
secretions,so they are no longer straight; instead, they
become tortuous and also because of increased pressure
from surrounding stroma the glands wall infold so they
appear corkscrew and finally saw toothed in
longitudinal section. (6,8,2)
This period is also associated with the secretion of a
certain number of progesterone regulated proteins. (Journal.2.)
Immunohistochemical studies have located these proteins
exclusively in the epithelial component. (Journal.2.)
They are: progesterone-associated endometrial protein
(PEP) , insulin growth factor binding protein 2 (IGFBP2) or
protein 14 or glycodelin ,crystalloglobulin , the integrins
and glycoproteins or type 1 mucins which are secreted into
the cytoplasm of the glands. (Journal.2.)
The physiological role played by these various proteins
is still not fully understood. (Journal.2.)
PP14 would seem to have role in facilitating embryo
implantation.
Evidence:-The uterine flushings of patients who
have had miscarriage show reduced PP 14
secretion. (Journal.2.)
Mucin, particularly muc-1, has important functions at
the luminal surface and plays a dominant role in
maintaining a functionally non-receptive uterine surface
with regard to blastocyst attachment.
It may inhibit implantation at the maternal cell
surface . (Journal.2.)
Mucin deficiency may enhance the chances of
lower quality embryos implanting successfully.
(Journal.2.)
Dating in the mid- to late-secretory phase relies on changes
in the endometrial stroma (3)
From Day 20, the stroma of the endometrium appears
oedematous. This is in response to prostaglandins (PG) E2
causing vascular permeability.
PGE2 stimulates capillary permeability either directly or
by means of increased histamine release which enhances
the appearance of oedema in the stroma. (Journal.2.)
Development of spiral arteries is a characteristic
feature of mid secretory phase(by days22-23of cycle)
and these vessels become increasingly coiled as their
length increases rapidly. (4)
During endometrial growth, spiral arteries lengthen at a
rate appreciably greater than the rate of increase in
endometrial tissue height or thickness. (3)
Specific angiogenic agents like members of VEGF family
produced from endometrial stroma cells and glandular
epithelium in response to estrogen and progesterone which
stimulates endothelial cell proliferation and increases
vascular permeability.(3 & 4)
Beginning 9 to 10 days after ovulation(Day 23-24),stromal
cells that surround the spiral arteries of the uterus enlarge
and develop eosinophilic cytoplasm, with a prominent Golgi
and endoplasmic reticulum. This process is referred to as
Pre decidualization(6)
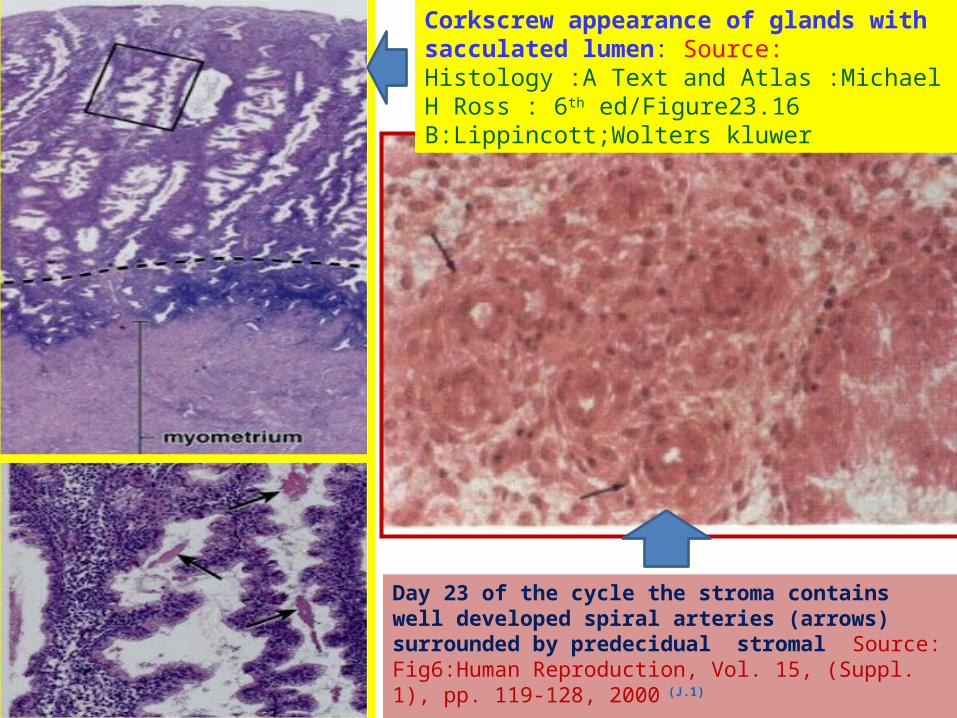
Day 23 of the cycle the stroma contains well developed spiral arteries (arrows) surrounded by predecidual stromal Source: Fig6:Human Reproduction, Vol. 15, (Suppl. 1), pp. 119-128, 2000 (J.1)
Corkscrew appearance of glands with sacculated lumen: Source:Histology :A Text and Atlas :Michael H Ross : 6th ed/Figure23.16 B:Lippincott;Wolters kluwer
Laminin, fibronectin and type IV collagen surround
matrices of decidualizing cells. (6,4) .
Laminin, and fibronectin may provide a surface that
facilitates attachment of the embryo . (6)
Type IV collagen facilitates the attachment of
trophoblastic cells regulating the permeability and
nutrition of trophoblastic and endometrial cells. (journal-2)
The rounded decidual cells differentiate from spindle-
shaped fibroblast-like stromal cells under the influence
of progesterone.(6)
Peridecidual cells secrete numerous substances that
may be nutritious, metabolic or immunosuppressive like
insulin growth factor binding protein 1
(IGFBP1) ,prolactin and relaxin. (Journal.2.)
Multiple foci of these decidual cells spread throughout the
upper layer of the endometrium and form a dense layer
called zona compacta. This spreading is so extensive that
the glandular structures of the zona compacta become
inconspicuous. (6)
Stroma in the midzone of the functionalis shows little
predecidual changes,remains edematous hence appears
less opaque this is known as zona spongiosum here the
endometrial glands are more prominent (6)
The process of predecidualization is mediated by
Progesterone and its receptors .oestrogens do not
influence predecidualization . (Journal.2)
Evidence: ovariectomized women whose menstrual
cycle is induced by oestrogen and progesterone
administration present similar predecidualization
whether or not they receive oestrogens during the luteal
phase. (Journal.2.)
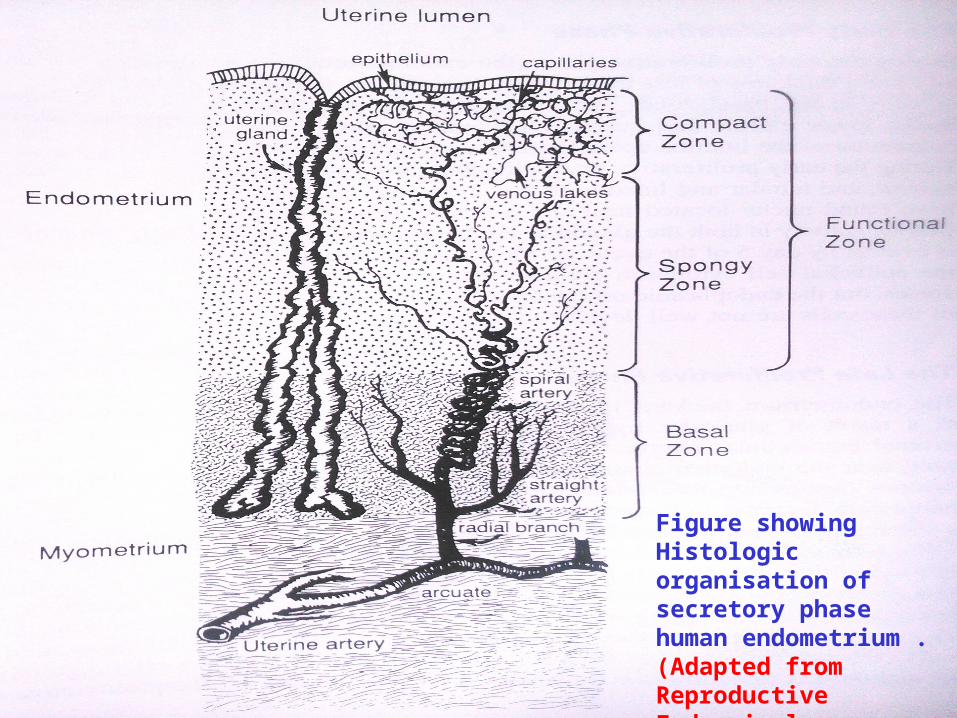
Figure showing Histologic organisation of secretory phase human endometrium .(Adapted from Reproductive Endocrinology Physiology ,PathoPhysiology and Clinical management; Yen,Jaffeand Barbieri ;4rth edition figure8-1)
Mitosis reappear in the stromal cells by day 26-27 as a
reflection of the decrease in progesterone activity which
marks a minor recrudescence of an estrogenic effect. (8)
In the Late premenstrual phase endometrium there is
infiltration of stroma by polymorphonuclear leukocytes . (3)
The endometrial stromal and epithelial cells produce
Interleukin-8(IL-8) ,a chemotactic /activating factor for
neutrophils which recruits neutrophils to the endometrium
just prior to the onset of menstruation (3)
Endometrium is capable of synthesizing Monocyte
chemotactic protein-1(MCP-1) chemoattractant for
monocytes. (3)
The rate of synthesis of IL-8 ,MCP-1 in the endometrial
stromal cells are modulated by Progesterone and
Transforming growth factor –β. (3)
In absence of fertilization, implantation and consequent lack of
sustaining quantities of HCG from the trophoblast , the otherwise
fixed lifespan of corpus luteum is completed ,and estrogen and
progesterone levels wane initiating the process of menstruation.(9)
Adapted from:-Di Fiore’s Atlas of Histology with Functional Correlations: Victor P. Eroschenko : Lippincott Williams & Wikkins : 12th Edition ;Chapter 21:Page 525-531
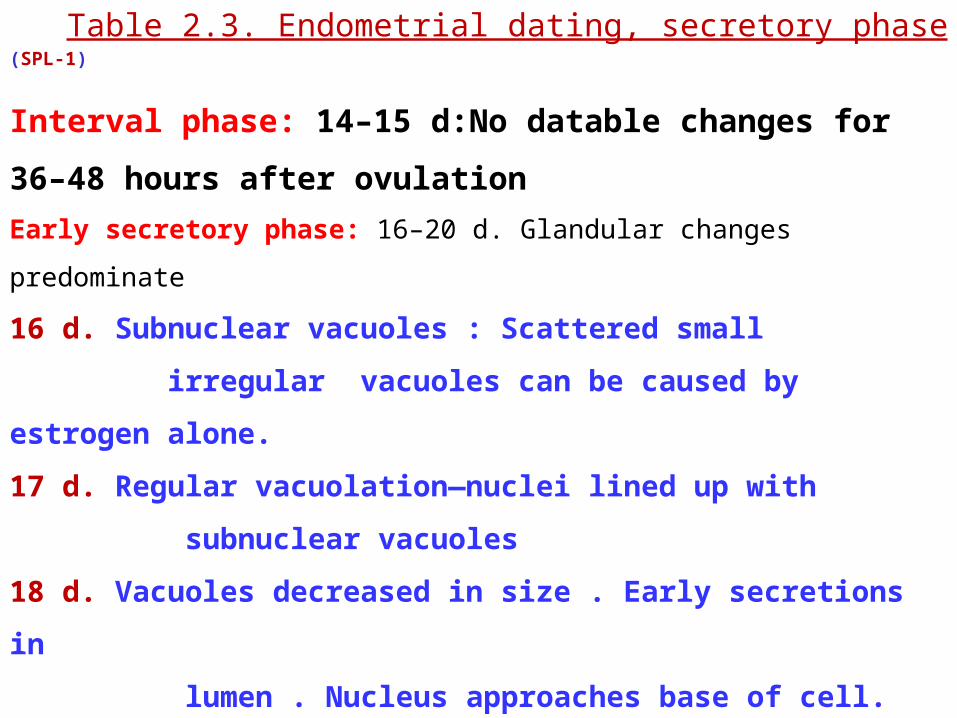
Table 2.3. Endometrial dating, secretory phase (SPL-1)
Interval phase: 14–15 d:No datable changes for 36–48
hours after ovulation
Early secretory phase: 16–20 d. Glandular changes predominate
16 d. Subnuclear vacuoles : Scattered small
irregular vacuoles can be caused by estrogen
alone.
17 d. Regular vacuolation—nuclei lined up with
subnuclear vacuoles
18 d. Vacuoles decreased in size . Early secretions in
lumen . Nucleus approaches base of cell.
19 d. Few vacuoles remain.Intraluminal secretion.
No pseudostratification, no mitoses
20 d. Peak of intraluminal secretions
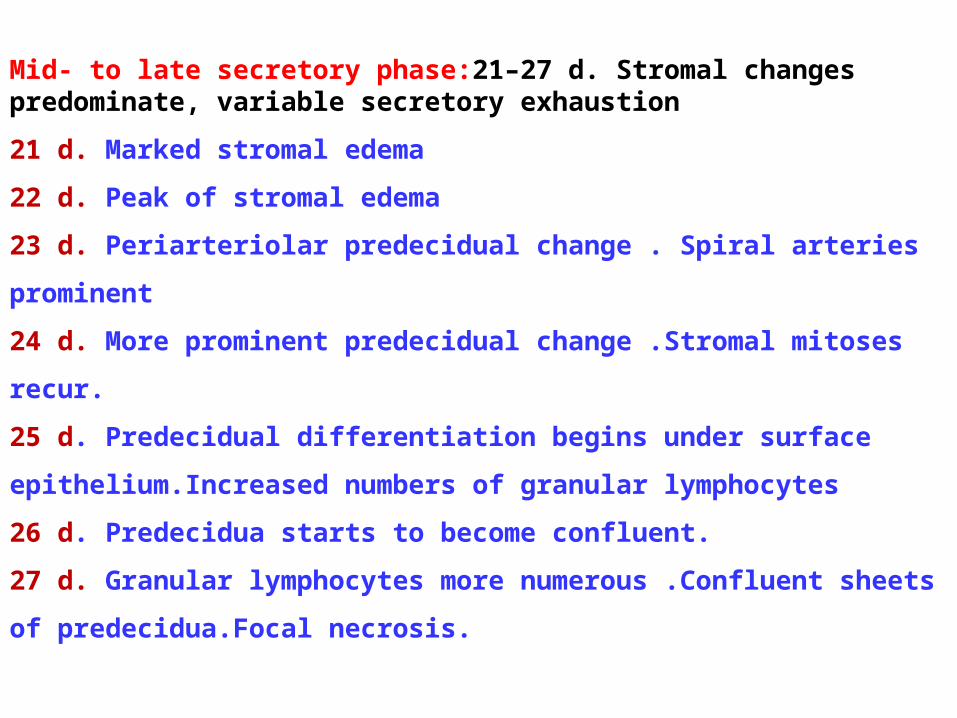
Mid- to late secretory phase:21–27 d. Stromal changes predominate, variable secretory exhaustion
21 d. Marked stromal edema
22 d. Peak of stromal edema
23 d. Periarteriolar predecidual change . Spiral arteries
prominent
24 d. More prominent predecidual change .Stromal mitoses
recur.
25 d. Predecidual differentiation begins under surface
epithelium.Increased numbers of granular lymphocytes
26 d. Predecidua starts to become confluent.
27 d. Granular lymphocytes more numerous .Confluent sheets
of predecidua.Focal necrosis.
Why dating of endometrium? (SPL-1)
Routine histologic evaluation remains a cost-effective method of
determining the relative degree of endometrial development
through the menstrual cycle.
Dating of the endometrium yields information about :
(1) Histologic evidence of ovulation
(2) Dating the secretory phase gives a general assessment of
progesterone production by the corpus luteum and the ability of
the endometrium to respond to progesterone.
(3) presence or absence of endometrial abnormalities that may be
responsible for infertility.
Pitfalls of endometrium dating :(SPL-1)
1.Endometrium with surface epithelium is best for interpretation.
Absence of surface epithelium compromises the interpretation.
2. Tissue from the lower uterine segment or basalis is not
satisfactory for dating. Endometrium from these regions does not
respond fully to hormones.
3. Scattered subnuclear vacuoles in glands are not sufficient
evidence of ovulation. To be certain that ovulation has occurred,
more than 50% of the glands must show subnuclear vacuoles.
4. Focal cystic glands or nonreactive glands can occur in
normal endometrium and have no significance by themselves.
5. Compact predecidua with spindleshaped stromal cells may
not be appreciated as a true predecidual reaction. Directing
attention to stromal changes around spiral arteries assistsin
the identification of predecidua.
6.Lymphocytes and granular lymphocytes normally become
prominent in the stroma of the late secretory phase.These do
not represent inflammation.
7.The endometrium cannot be dated accurately when polyps,
inflammation, or other abnormalities are present.
8. several artifacts often complicate the histologic patterns. One
frequent artifact is tissue fragmentation caused by mechanical
disruption of the tissue. As a result, glands are detached from the
surrounding stroma, and fragmented glands become randomly
oriented.
As this traditional method of histological dating has low predictive
value further refinements have been employed in evaluation of
normal endometrium may evolve that have clinical utility.
Morphometric analysis has been attempted to increase the
accuracy of endometrial histologic dating.
Five morphometric measurements, including mitotic rate in
gland cells, amount of luminal secretion, volume fraction of
gland occupied by gland cell, amount of pseudostratification
of gland cells, and amount of predecidual reaction, added
precision to histologic dating
Immunohistochemical analysis for specific secretory products
of the endometrium.
ContinuATION OF The Endometrial Cycle
Synopsis : Proliferative changes occurs due to rise in level of ovarian
estrogens. Extends from 5th or 6th day to 14th day .
Secretory changes in the components are due to
combined effects of estrogen and progesterone liberated
from the corpus luteum after ovulation . Extends from 15th to
28th day of the cycle
Mitosis and growth is seen in Proliferative phase while
secretory changes and prepration of endometrium for
implantation is evident in secretory phase
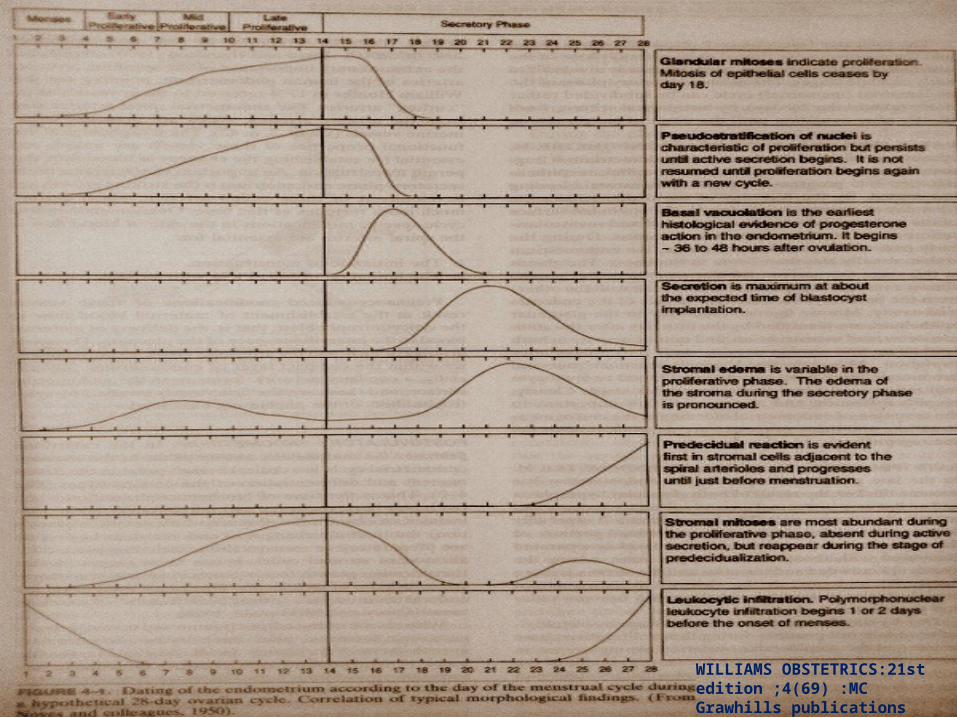
WILLIAMS OBSTETRICS:21st edition ;4(69) :MC Grawhills publications
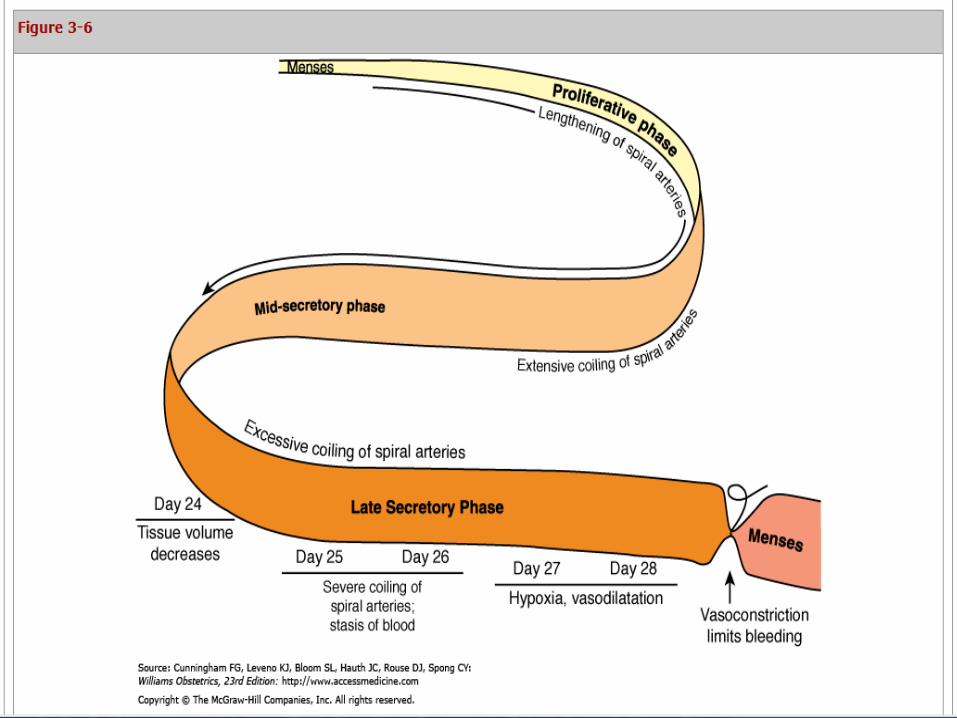
Endometrium growth regresses with the decline in
corpus luteum function compelling even greater coiling
of spiral arteries. (3)
Due to severe coiling of spiral arteries there is
increase in the resistance to the blood flow in these
vessels which is so marked that stasis develops
causing hypoxia of the endometrium (3&9)
Menstrual Phase
4 to 24 hours before bleeding into the endometrium there
is a period of intense vasoconstriction of spiral arteries at
the basal part. (3&4 )
Markee emphasized that intense vasoconstriction limits
the blood loss during menstruation. (3)
reduction in spiral artery blood flow and resultant stasis
before the time of vasoconstriction has been suggested as
primary cause of endometrial ischemia and tissue
degeneration. (3)
Endothelin -1 is a substance produced by endometrial
stromal cells in response to hypoxic endometrium which is a
potent vasoconstriction. (3)
Markee predicted that when an individual coiled artery
relaxed after a period of constriction , hemorrhage occurred
from that artery or its branches. (3)
This sequence of vasoconstriction ,relaxation and
hemorrhage appears to be well established but mechanisms
that actually brings about escape of blood from the vessels is
not certain. (3)
Menstruation is the result of enzymatic auto digestion and
ischemic necrosis. (Journal 2)
In the first part of the secretory phase, acid phosphatases
and lytic enzymes are confined to the lysosomes. Their release
is inhibited by Progesterone which stabilizes the lysosomal
membranes. (Journal 2 & 9)
with wanning of estrogen and progesterone levels, these
lysosomal membranes are disrupted and the enzymes are
released into the cytoplasm of epithelial , stromal and
endothelial cells (Journal 2 & 9)
These lytic enzymes digests their cellular elements,
leading to release of prostaglandins , extravasation of red
blood cells , tissue necrosis . (Journal2 & 9)
Invading leukocytes secrete enzymes that are members
of the matrix metalloproteinase (MMP) family which causes
the breakdown of the extracellular matrix and basal
membranes. As their action is localized, sloughing is
limited to the function of layer only. (Journal2 & 9& 3)
Haemostasis is the result of a balance between
coagulation and fibinolysis. (Journal 2)
Since progesterone maintains coagulation, any fall in
progesterone levels will give rise to fibrinolysis.(Journal 2) & 9)
Plasminogen activators are present in the menstrual
endometrium and originate from the endometrial vascular
endothelium. They convert plasminogen into plasmin
which in turn prevents the menstrual blood from clotting.
(Journal 2 )
Fibrinolysis increases progessively, leading to
menstrual bleeding. (Journal 2 & 9)
Vasomotor phenomena bring about vasoconstriction
and vascular relaxation. They are regulated by
Prostaglandin F2α which increase during the secretory
phase and reach peak levels during the menstrual
phase. (Journal 2 & 9)
PGF cause vasoconstriction of the basal arteries
which gives rise to circulatory arrest in the spiral arteries
and contraction of the myometrium at the boundary
between endometrium and myometrium. (Journal 2 & 9)
These tissue and vascular phenomena together lead
to tissue desquamation or sloughing and the shedding of
menstrual blood. (Journal 2 & 9)
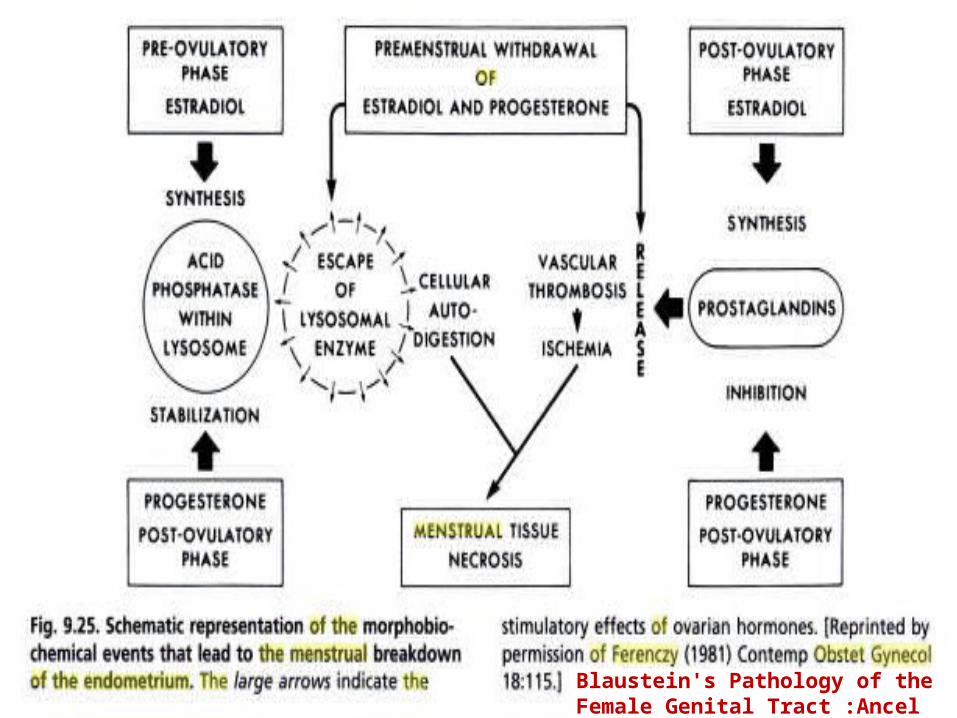
Blaustein's Pathology of the Female Genital Tract :Ancel Blaustein, Robert J. Kurman
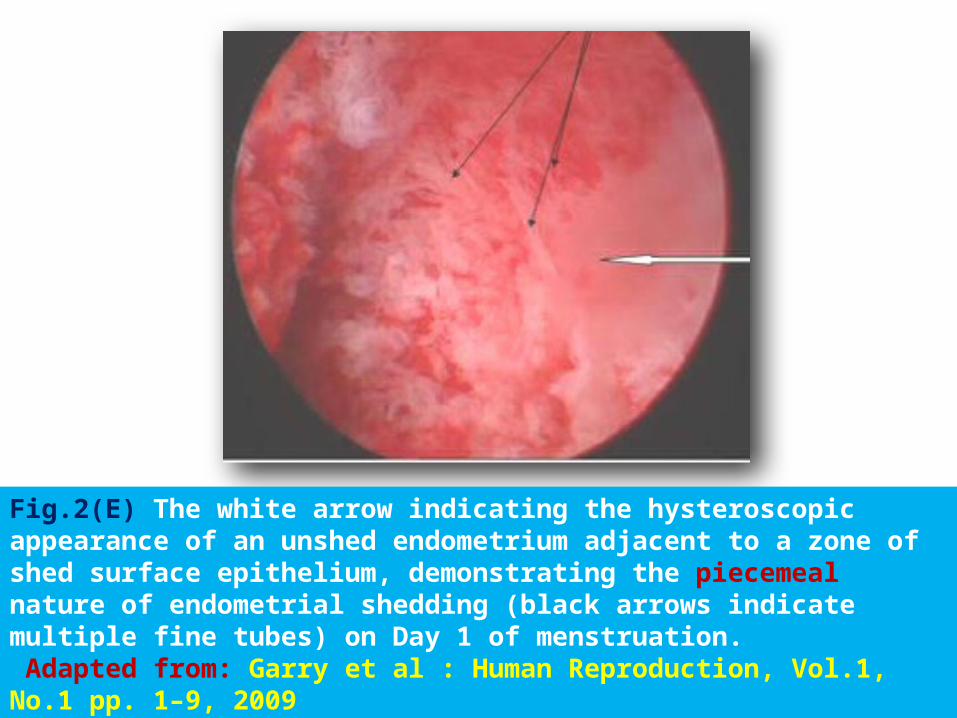
Fig.2(E) The white arrow indicating the hysteroscopic appearance of an unshed endometrium adjacent to a zone of shed surface epithelium, demonstrating the piecemeal nature of endometrial shedding (black arrows indicate multiple fine tubes) on Day 1 of menstruation. Adapted from: Garry et al : Human Reproduction, Vol.1, No.1 pp. 1–9, 2009
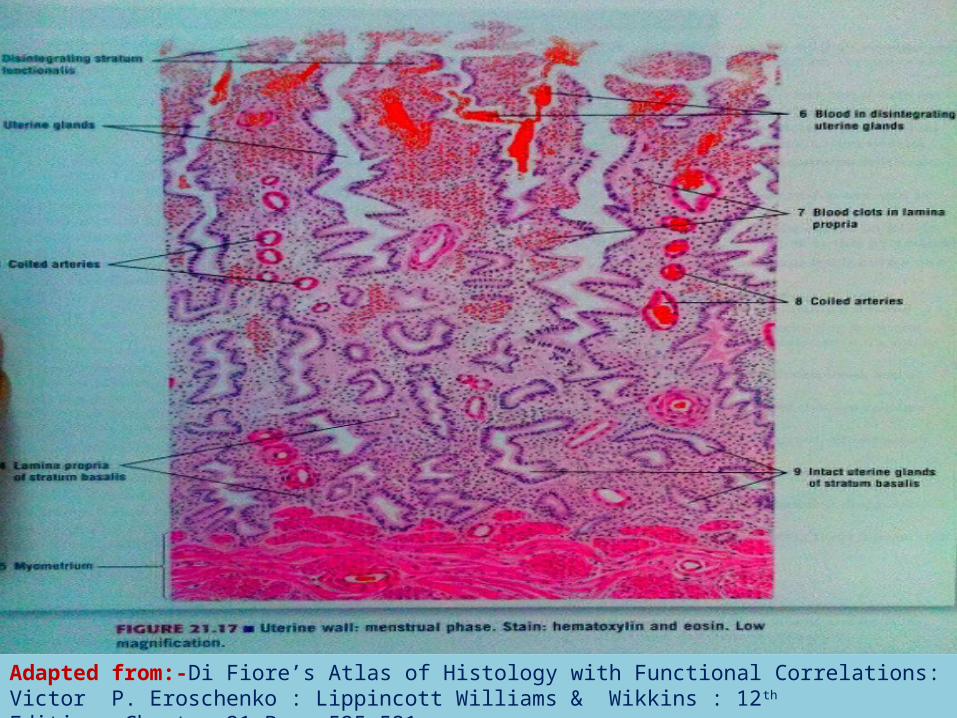
Adapted from:-Di Fiore’s Atlas of Histology with Functional Correlations: Victor P. Eroschenko : Lippincott Williams & Wikkins : 12th Edition ;Chapter 21:Page 525-531
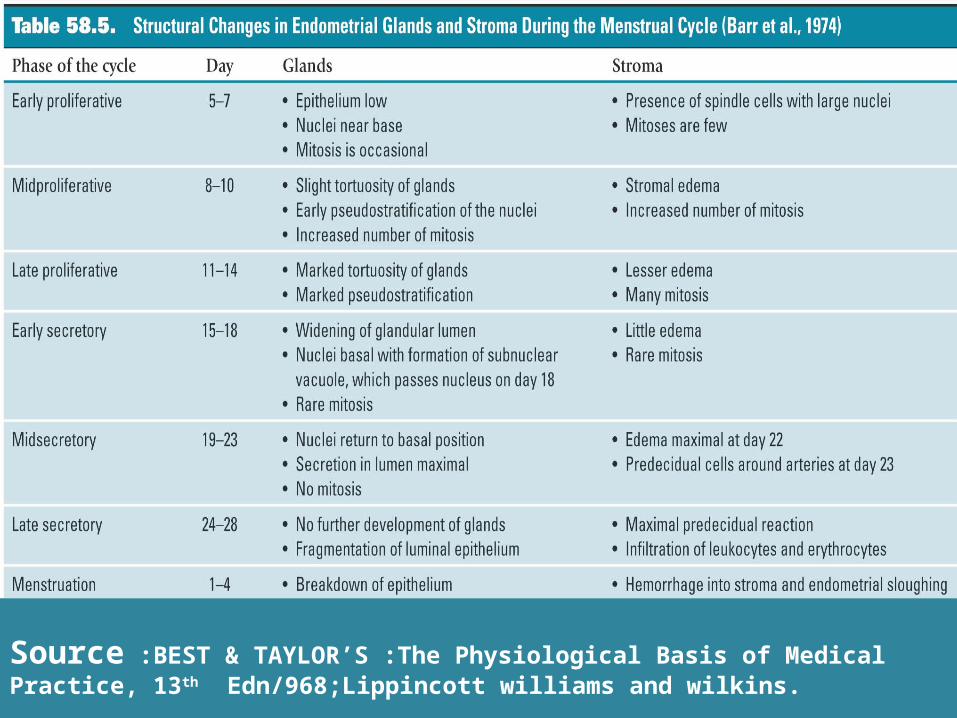
Source :BEST & TAYLOR’S :The Physiological Basis of Medical Practice, 13th Edn/968;Lippincott williams and wilkins.
Regenerative Phase
Starts at the moment of menstruation and constitutes
the first few days of the proliferative phase. (Journal 2)
Tissue necrosis provokes a marked inflammatory
response with the production of pro-inflammatory,
chemotactic and anti-inflammatory cytokines. (Journal 2)
Regeneration also depends on macrophages and
polymorphonucleacytes which help to clean up the necrotic
area. (Journal 2)
The stromal cells of the basal component of the
mucosa proliferate to replace the shed endometrium and
subsequently are active in re-establishing the
endometrium. (Journal 2)
This synthesis is associated with a regeneration of the
epithelium with gland proliferation, starting from the
basal component and in the surface epithelium
around the tubes and isthmus. (Journal 2 & 10)
This post-menstrual regenerated epithelium binds to the
fibroblasts of the underlying stroma, with the stromal cells
forming clumps onto which the surface epithelium can
migrate . (Journal 2 & 10)
Epithelial growth may in fact be stimulated by the
underlying fibroblast. (Journal 2 & 10)
Tenascin, a fibronectin-inhibitor synthesized by the
fibroblasts of the endometrial stroma, may also play a role
in facilitating epithelial migration (Journal 2 & 10)
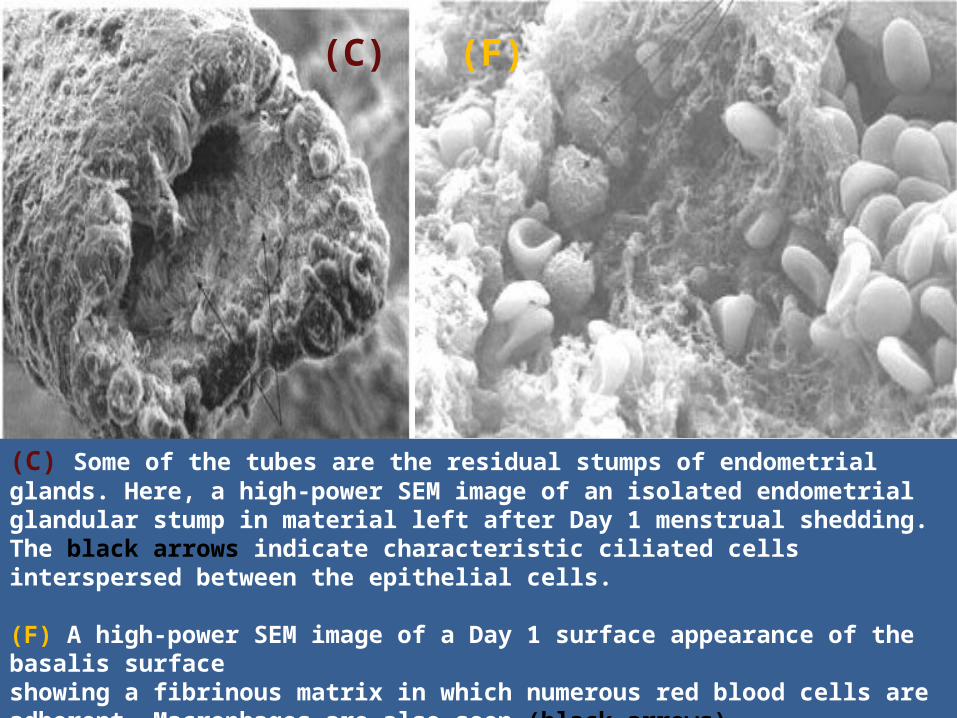
(C) Some of the tubes are the residual stumps of endometrial glands. Here, a high-power SEM image of an isolated endometrial glandular stump in material left after Day 1 menstrual shedding. The black arrows indicate characteristic ciliated cells interspersed between the epithelial cells.
(F) A high-power SEM image of a Day 1 surface appearance of the basalis surfaceshowing a fibrinous matrix in which numerous red blood cells are adherent. Macrophages are also seen (black arrows).ADAPTED from: Garry et al : Human Reproduction, Vol.1, No.1 pp. 1–9, 2009
(C) (F)
A remarkable feature seen in human females and
rhesus monkey endometrium in absence of pregnancy is
its regeneration on a cyclic basis attributed to a unique
stem cell population and its progenitor cells confined to
the basalis layer and belived to initiate and sustain the
process of regeneration(11)
.
.
The role of oestradiol in endometrial regeneration is only
evident after the necrotic area has been cleaned up.
(Journal2 )
Oestradiol serum titres are very low during the
menstrual phase and regeneration seems due initially just
to a repair mechanism. (Journal2 )
Evidence: Endometrial regeneration in ovariectomized
rabbits is identical to that of rabbits with normal ovaries
(Journal2 & 10)
Post menstrual endometrial remodelling is induced by
prostaglandins released following tissue breakdown and
there is no role of hormones with serum estrogen and
ER ,PR receptors as low as premenstrual values. ( 11)
Day 7-12 serum estrogens and ER ,PR concentrations
increase resulting in marked increase in DNA synthesis
and mitotic activity in endometrial cells (10)
VEGF (Vascular endothelial growth factor) produced
by endometrium in response to estrogen and hypoxia
plays an important role in angiogenesis and endometrial
repair. (2)
By the 5th day of cycle surface epithelium cuboidal in
nature is derived from gland lumina and stromal cells.
and revascularization of the endometrium is in progress. (1)
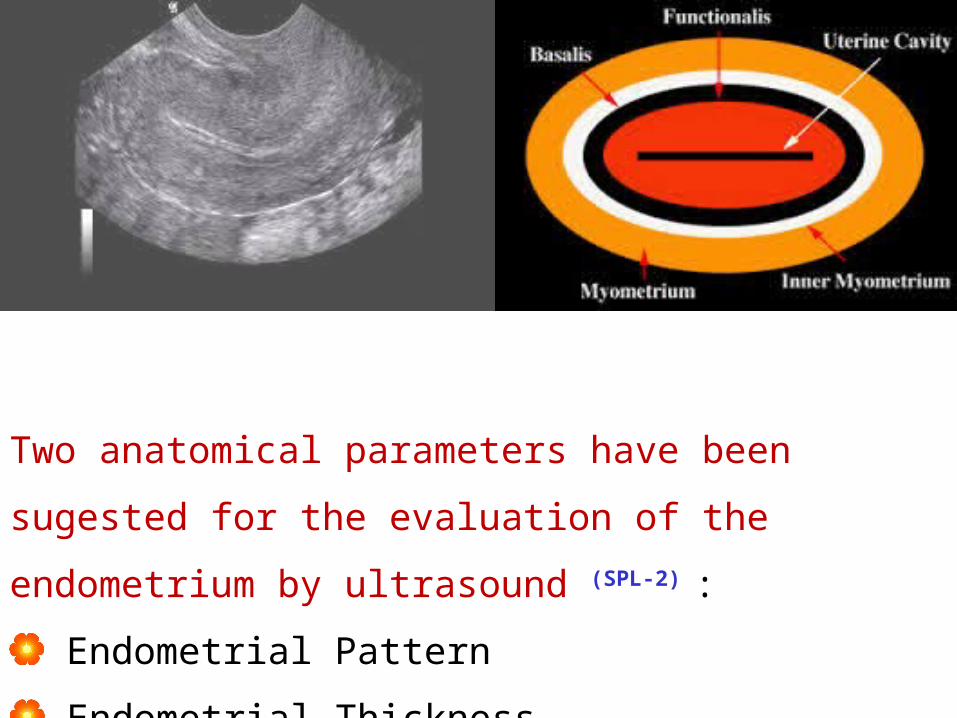
Two anatomical parameters have been sugested for the
evaluation of the endometrium by ultrasound (SPL-2) :
Endometrial Pattern
Endometrial Thickness
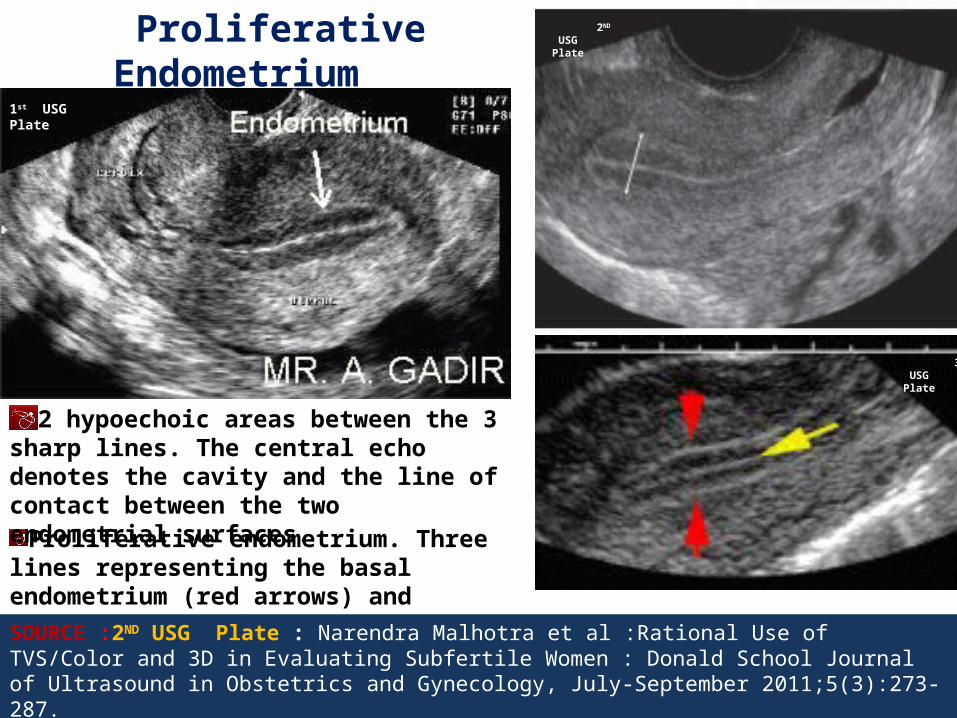
Proliferative endometrium. Three lines representing the basal endometrium (red arrows) and central endometrial cavity echo (yellow arrow)
2 hypoechoic areas between the 3 sharp lines. The central echo denotes the cavity and the line of contact between the two endometrial surfaces.
SOURCE :2ND USG Plate : Narendra Malhotra et al :Rational Use of TVS/Color and 3D in Evaluating Subfertile Women : Donald School Journal of Ultrasound in Obstetrics and Gynecology, July-September 2011;5(3):273-287.
Proliferative Endometrium
2ND
USG Plate
1st USG Plate
3rd USG Plate
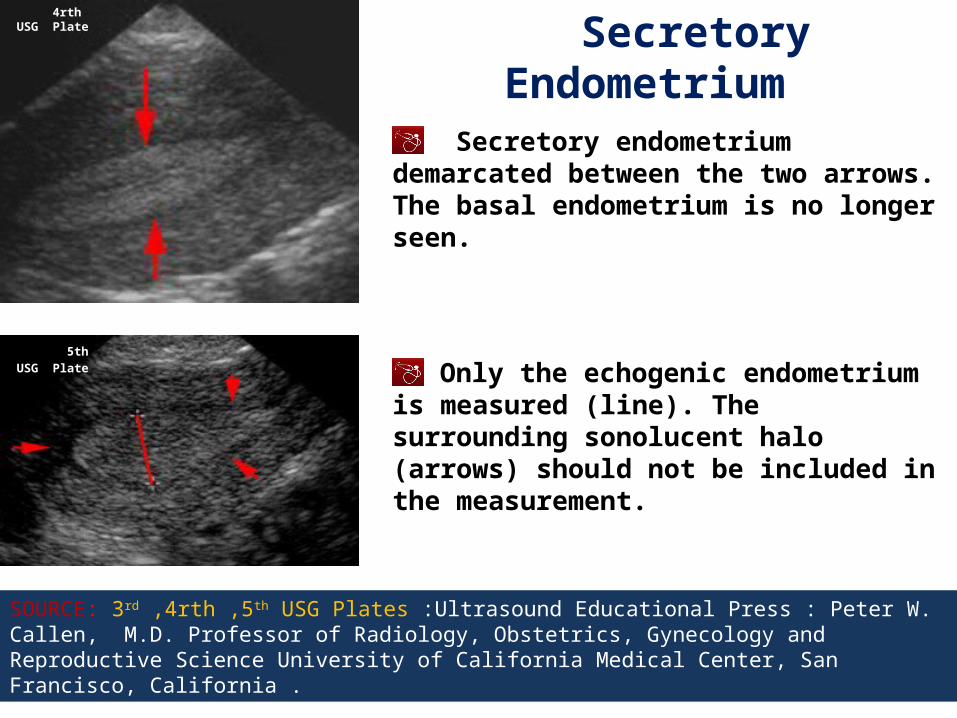
Secretory endometrium demarcated between the two arrows. The basal endometrium is no longer seen.
Only the echogenic endometrium is measured (line). The surrounding sonolucent halo (arrows) should not be included in the measurement.
SOURCE: 3rd ,4rth ,5th USG Plates :Ultrasound Educational Press : Peter W. Callen, M.D. Professor of Radiology, Obstetrics, Gynecology and Reproductive Science University of California Medical Center, San Francisco, California .
Secretory Endometrium
4rth USG Plate
5th USG Plate
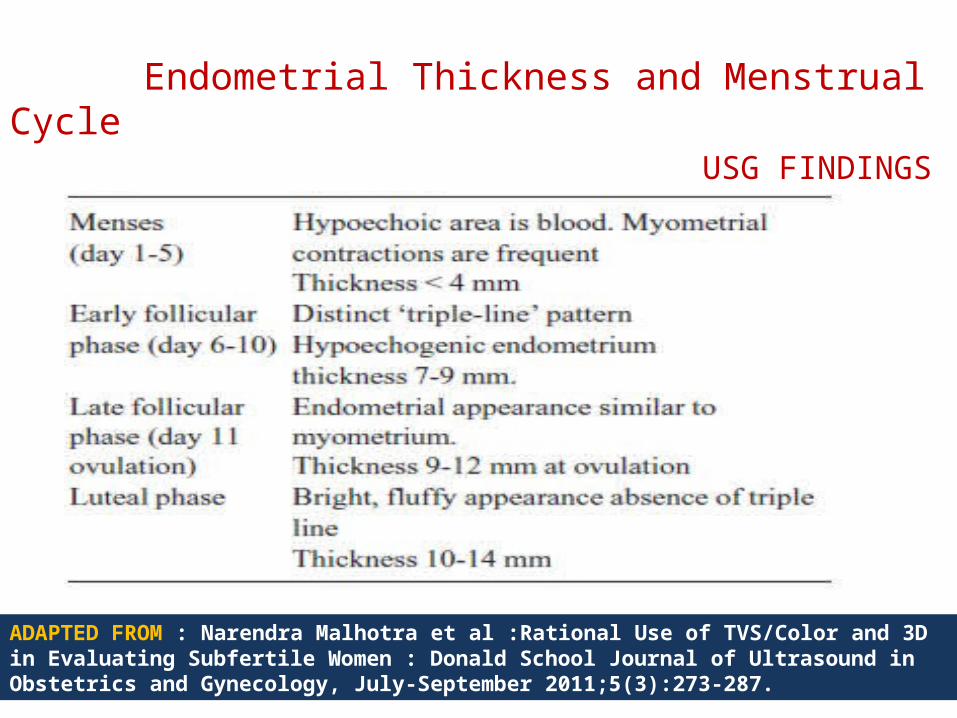
Endometrial Thickness and Menstrual Cycle USG FINDINGS
ADAPTED FROM : Narendra Malhotra et al :Rational Use of TVS/Color and 3D in Evaluating Subfertile Women : Donald School Journal of Ultrasound in Obstetrics and Gynecology, July-September 2011;5(3):273-287.
What’s the need to study endometrial pattern and endometrial thickness ?
There is various conflicting controversial observations
and no generalized consensus that the measurement of
endometrial thickness have predictive value for pregnancy
or not . (SPL-2)
However it has been suggested that the main advantage
of measuring endometrial thickness lies in its high
negative predictive values in cases where there is
minimal endometrial thickness. (SPL-2)
It has been observed that thin endometrium (<7mm) and thick
endometrium (>14mm) are frequently associated with
miscarriages. (SPL-2)
Sundstrom described a successful pregnancy in a patient
who’s endometrium measured only 4mm. (SPL-2)
Also poor endometrial pattern does not exclude pregnancy. (SPL-2)
Thus, endometrial pattern can serve as prognostic value in
both fresh IVF and frozen embryo transfer cycles as endometrial
pattern is not influenced by type of ovarian stimulation. (SPL-2)
REPRODUCTIVE ASSISTED FERTILIZATION
Assisted reproductive technologies is used for treatment
of infertility.
First successful birth of a "test tube baby", Louise brown
occurred in 1978 born at Oldham General Hospital by planned
Caesarean section delivered by John Webster.
Robert G Edwards the Physiologist who developed the
treatment was awarded the Nobel Prize in Physiology or Medicine
in 2010
Adrina Iliescu held the record of oldest women to give birth
using IVF and donated egg when she gave birth in 2004 at age of
66 .
Subhash Mukhopadhayay ;a Reproductive
Physiologist who created world’s 2nd and India’s 1st child using
in vitro fertilization Durga(Kanupriya Agarwal ) born 67 days
after 1st IVF baby in UK.
Thanks to TC Anand kumar to bring out this
information to the world .
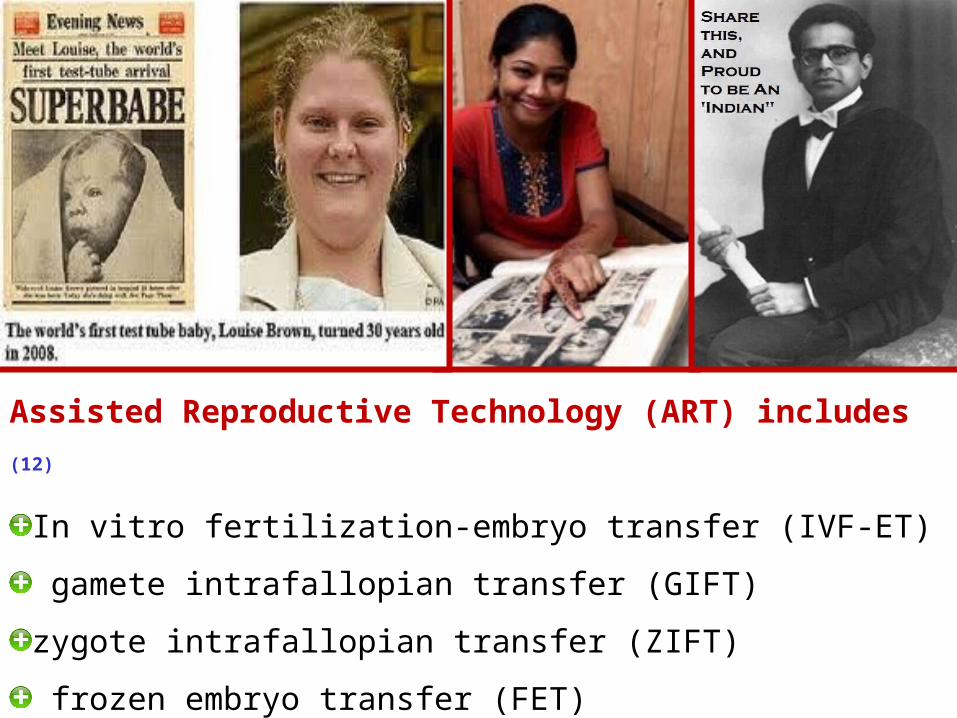
Assisted Reproductive Technology (ART) includes (12)
In vitro fertilization-embryo transfer (IVF-ET)
gamete intrafallopian transfer (GIFT)
zygote intrafallopian transfer (ZIFT)
frozen embryo transfer (FET)
Approximately 99 percent of ART cycles performed are IVF-ET
The basic steps in an IVF treatment cycle are (12)
Ovarian stimulation Egg retrieval Fertilization Embryo culture, Embryo transfer.
Ovarian Stimulation (12)
During ovarian stimulation or ovulation induction, medications or
“fertility drugs,” are used to stimulate multiple eggs to grow in the
ovaries rather than the single egg that normally develops each
month .
Multiple eggs are stimulated because some eggs will not
fertilize or develop normally after fertilization.
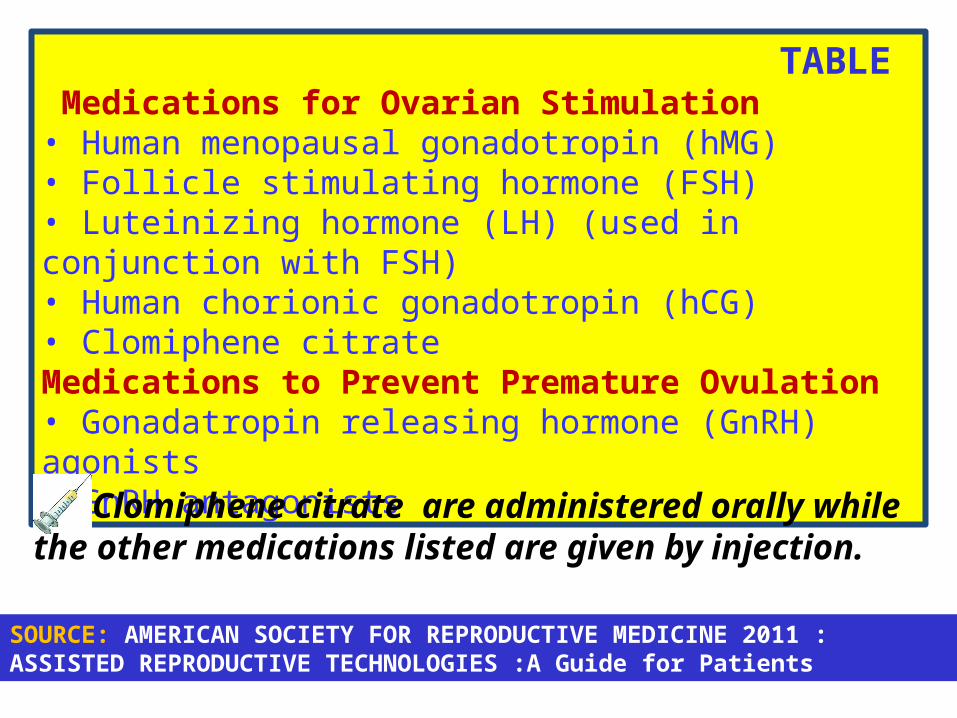
TABLE Medications for Ovarian Stimulation• Human menopausal gonadotropin (hMG) • Follicle stimulating hormone (FSH) • Luteinizing hormone (LH) (used in conjunction with FSH)• Human chorionic gonadotropin (hCG) • Clomiphene citrateMedications to Prevent Premature Ovulation• Gonadatropin releasing hormone (GnRH) agonists• GnRH antagonists
Clomiphene citrate are administered orally while the other medications listed are given by injection.
SOURCE: AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE 2011 : ASSISTED REPRODUCTIVE TECHNOLOGIES :A Guide for Patients
The ovaries are evaluated during treatment with
vaginal ultrasound examinations to monitor the
development of ovarian follicles . (12)
Blood samples are drawn to measure the response to
ovarian stimulation medications. (12)
Normally, estrogen levels increase as the follicles
develop, and progesterone levels are low until after
ovulation (12)
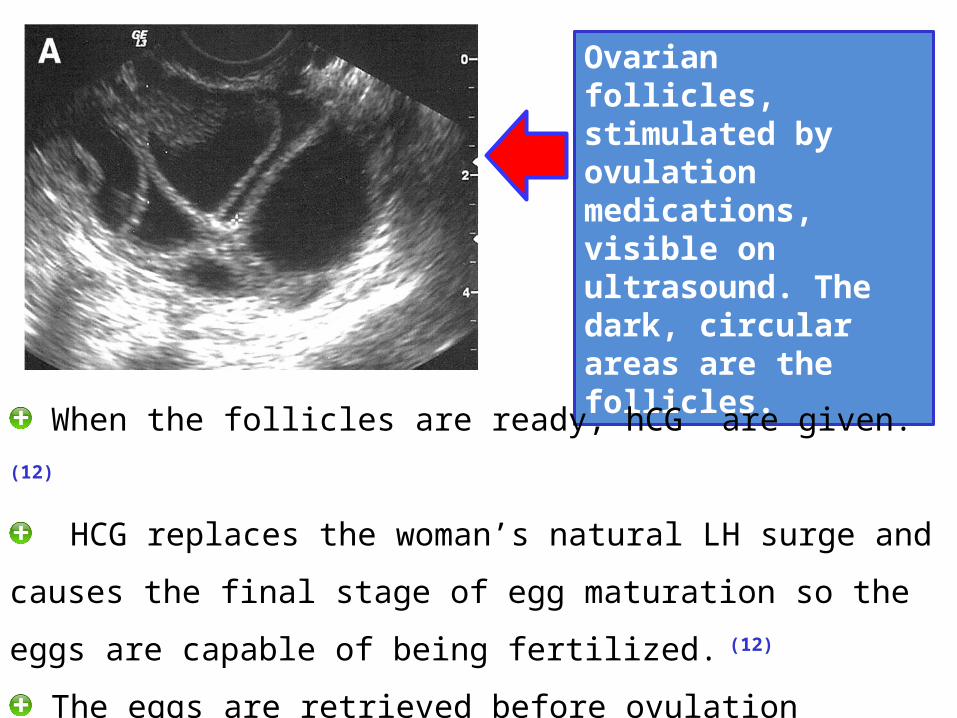
Ovarian follicles, stimulated by ovulation medications, visible on ultrasound. The dark, circular areas are the follicles.
When the follicles are ready, hCG are given. (12)
HCG replaces the woman’s natural LH surge and causes the
final stage of egg maturation so the eggs are capable of being
fertilized. (12)
The eggs are retrieved before ovulation occurs, usually 34 to 36
hours after the hCG injection is given. (12)
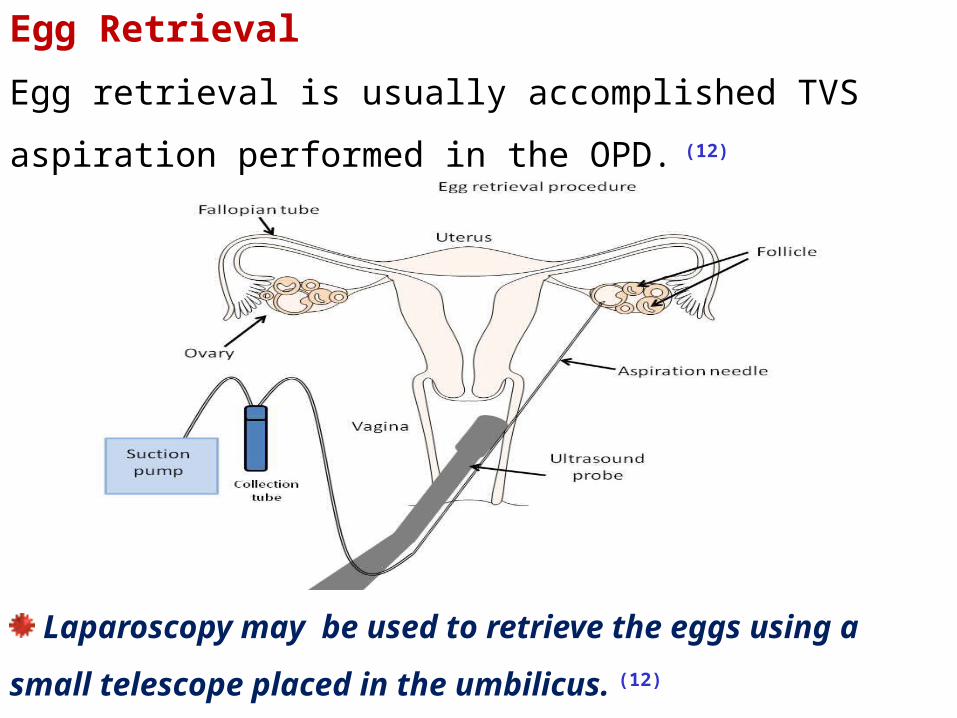
Egg Retrieval
Egg retrieval is usually accomplished TVS aspiration
performed in the OPD. (12)
Laparoscopy may be used to retrieve the eggs using a
small telescope placed in the umbilicus. (12)
Fertilization and Embryo Culture
After the eggs are retrieved, they are examined in the
laboratory for maturity and quality. Mature eggs are placed
in an IVF culture medium and transferred to an incubator to
await fertilization by the sperm. (12)
Sperm may be obtained from the testicle, epididymis, or vas
deferens or by manstrubation . (12)
Fertilization may be accomplished by insemination, where motile
sperm are placed together with the oocytes and incubated
overnight or by intracytoplasmic sperm injection (ICSI), where a
single sperm is directly injected into each mature egg (12)
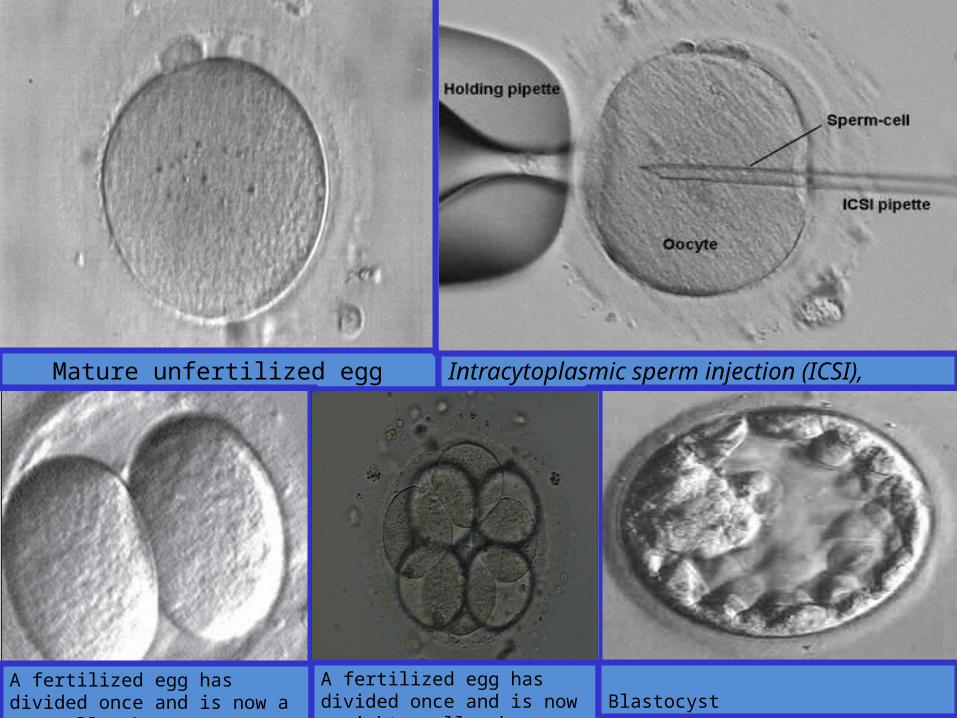
Mature unfertilized egg Intracytoplasmic sperm injection (ICSI),
A fertilized egg has divided once and is now a two-cell embryo.
A fertilized egg has divided once and is now a eight -cell embryo.
Blastocyst
By the third day, a normally developing embryo will
contain approximately 6 to 10 cells. (12)
By the fifth day, a fluid cavity forms in the embryo, and
the placenta and fetal tissues begin to separate. An
embryo at this stage is called a blastocyst. (12)
Embryos may be transferred to the uterus at any time
between one and six days after the egg retrieval. (12)
If successful development continues in the uterus, the
embryo hatches from the surrounding zona pellucida
and implants into the lining of the uterus approximately 6
to 10 days after the egg retrieval. (12)
Assisted hatching (AH) is a micromanipulation
procedure in which a hole is made in the zona pellucida
just prior to embryo transfer to facilitate hatching of the
embryo. (12)
Preimplantation genetic diagnosis (PGD) is performed at
some centers to screen for inherited diseases (12)
Embryos that do not have the gene associated with the
disease are selected for transfer to the uterus. (12)
Embryo Transfer
The next step in the IVF process is the embryo transfer. (12)
No anesthesia is necessary, although some women may
wish to have a mild sedative. (12)
One or more embryos suspended in a drop of
culture medium are drawn into a transfer catheter, a
long, thin sterile tube with a syringe on one end. (12)
The physician gently guides the tip of the transfer
catheter through the cervix and places
the fluid containing the embryos into the uterine cavity (12)
The physician identifies the cervix using a vaginal
speculum . (12)
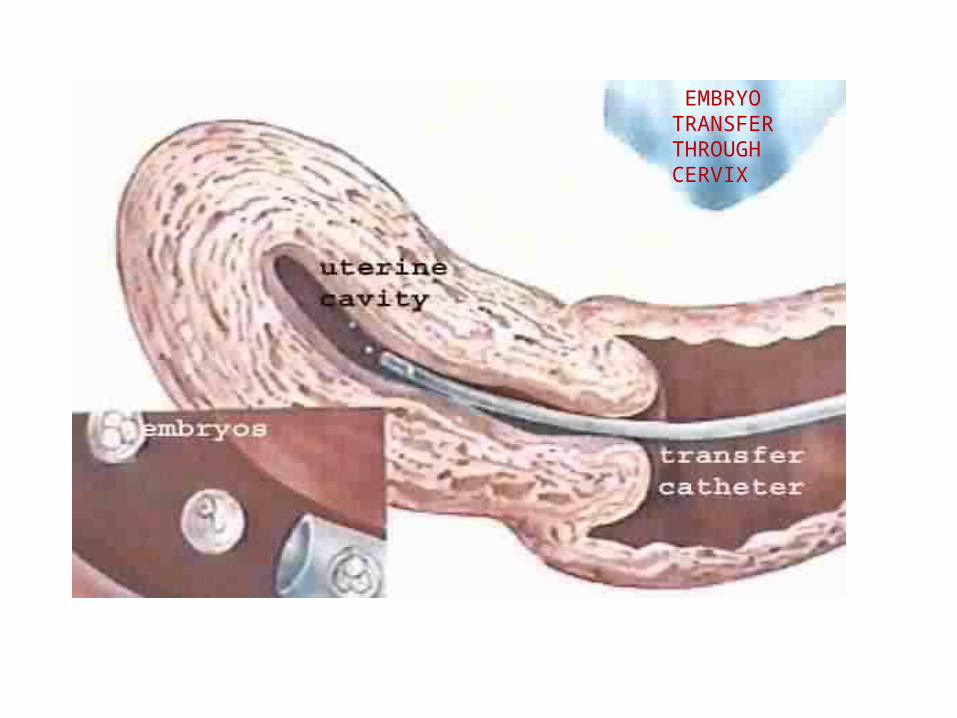
EMBRYO TRANSFER THROUGH CERVIX
CLINICAL IMPORTANCE OF ENDOMETRIUM :
The implantation potential of good quality embryos remains low
during IVF/ET treatment, despite advances in ovarian stimulation
regimens, the method of assisted fertilization and improved culture
conditions.
Successful implantation depends on a close dialog between the
blastocyst and the receptive endometrium.
Ultrasound parameters including endometrial thickness, endometrial
pattern, endometrial volume, Doppler study of uterine arteries and
endometrial blood flow have been used to assess endometrial
receptivity during IVF treatment.(SOURCE:Predictive value of endometrial thickness, pattern and sub-endometrial blood flows on the day of hCG by 2D doppler in in-
vitro fertilization cycles: A prospective clinical study from a tertiary care unit Neeta Singh , et al J Hum Reprod Sci. 2011 Jan-Apr; 4(1):
29–33.)
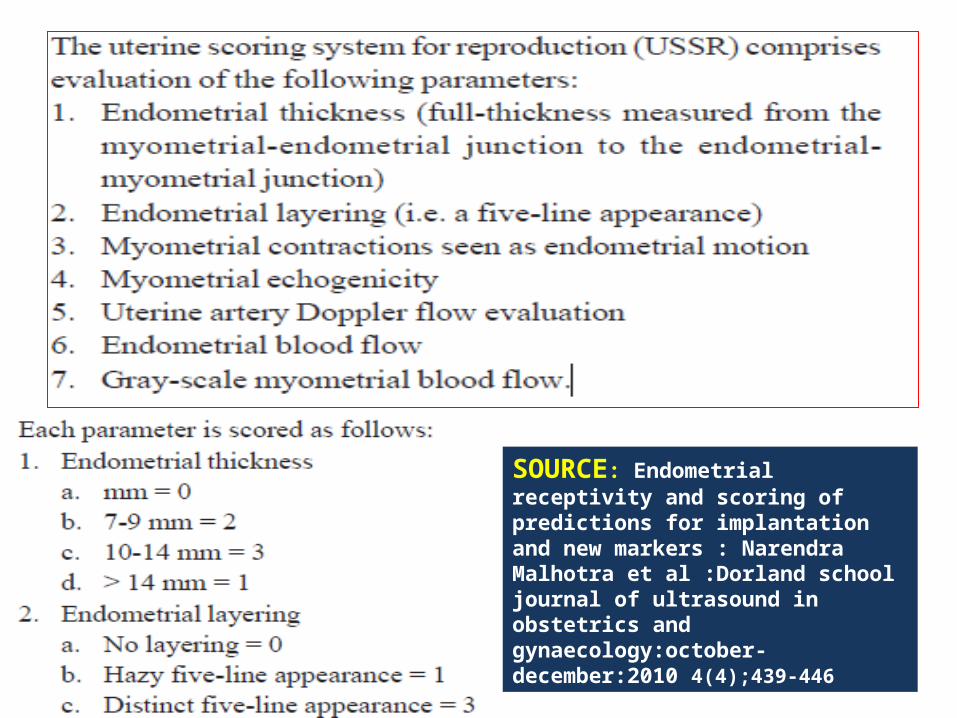
SOURCE: Endometrial receptivity and scoring of predictions for implantation and new markers : Narendra Malhotra et al :Dorland school journal of ultrasound in obstetrics and gynaecology:october-december:2010 4(4);439-446
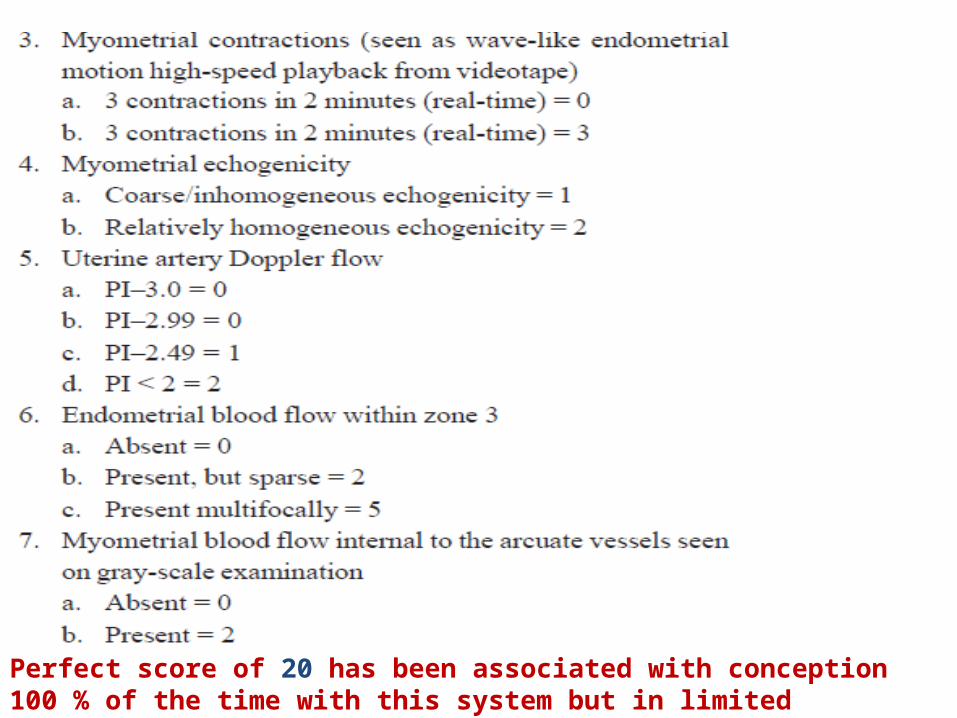
Perfect score of 20 has been associated with conception 100 % of the time with this system but in limited experience.
Attempt to Increase endometrial
thickness………………
Endometrial growth is thought to depend on uterine artery
flow and endometrial development has great importance on
in-vitro fertilization.
Nitric oxide relaxes vascular smooth muscles through c-
GMP mediated pathway and NO Synthase isoforms have
been identified in the uterus.
Phosphodiesterase hydrolyse c-AMP and c-GMP.
Sildenafil citrate (viagra) a type 5 specific
Phosphodiesterase inhibiting aguments the vasodilatory
effects NO by preventing degradation of c GMP.
Pulsatile index was decreased in 7 days after
sildenafil indicating increased blood flow.
Combination therapy of Sildenafil and oestradiol
valerate improved blood flow and endometrial thickness in
all patients as per below mentioned journal next slide .
NTG have been successfully used in improving
uterine blood flow and endometrial lining but with
increased side effects like hypotension and headaches.
Study on effects of sildenafil (vaginal suppositories) in
increasing uterine bleeding and endometrial thickness is
in preliminary phase and needs more intensive studies.
Source:Vaginal sildenafil(viagra):A preliminary report of a novel method to improve uterine artery blood flow and endometrial development in patients undergoing IVF :Geoffrey Sher et al :Human Reproduction :vol 15 no.4 pp.806-809 ,2000
NEWER Modality to increase endometrial thicknessG-CSF has also been employed in the proliferation of the
thin endometrium which fails to respond with standard therapy.
Evidence:1. Gleicher et al., perfused G-CSF transvaginally into
the uterus of four patients undergoing IVF with thin endometrium
after standard endometrial preparation.
This resulted in 7 mm of additional endometrial proliferation which
was previously resistant to estrogen and vasodilators therapy and
all the patients successfully underwent Endometrial Thickness and
conceived.
This demonstrates G-CSF as an innovative
remedy in patients with unresponsive,
inadequate, and thin endometrium.(Journal.8)
Evidence:2: Gleicher et al :described in 21 consecutive infertile
women with endometria <7 mm on the day of hCG administration
in their first IVF cycles. All previous cycles using traditional
treatments with estradiol, sildenafil citrate (Viagra™) and/or beta-
blockers had been unsuccessful.
G-CSF (Nupogen™) was administered per intrauterine catheter
by slow infusion before noon on the day of hCG administration.
Result: This cohort study is supportive of the effectiveness of G-
CSF in expanding chronically unresponsive endometria.
(Journal.9.)
Evidence:3: Pratap Kumar et al Evaluated the success rate of
IVF with supplementation of G-CSF in embryo culture media and
also the success of women undergoing IVF with thin endometrium
which fails to proliferate with standard treatment, but respond with
transvaginal instillation of G-CSF into the endometrium.
Results were remarkable as the survival rate of the embryo
cultured with G-CSF till 12th week and birth were significantly
higher which proves the efficacy of the G-CSF in assisted
reproduction technology.(Journal .10.)
Dysfunctional uterine bleeding (DUB)
defined as abnormal, irregular bleeding (excessively heavy,
prolonged, or frequent intervals of bleeding) in the absence
of demonstrable pelvic disease, complications of pregnancy
or systemic disease.
The exact mechanism is uncertain but is thought to be
caused by dysfunction of hypothalamic-pituitary-ovarian axis.
SOURCE: Management of dysfunctional uterine bleeding based on endometrial thickness: Ozgul Muneyyirci-Delale et al :International Journal of Women’s Health 2010:2 297–30
TVS is an excellent non-invasive tool to diagnose anatomic causes of dysfunctional uterine bleeding.
Getpook et al showed that ET of 8 mm or less is unlikely to be associated with malignant pathology.
Management of DUB based on endometrial thickness is an effective approach to control acute uterine bleeding.
SOURCE: Management of dysfunctional uterine bleeding based on endometrial
thickness: Ozgul Muneyyirci-Delale et al :International Journal of Women’s
Health 2010:2 297–30
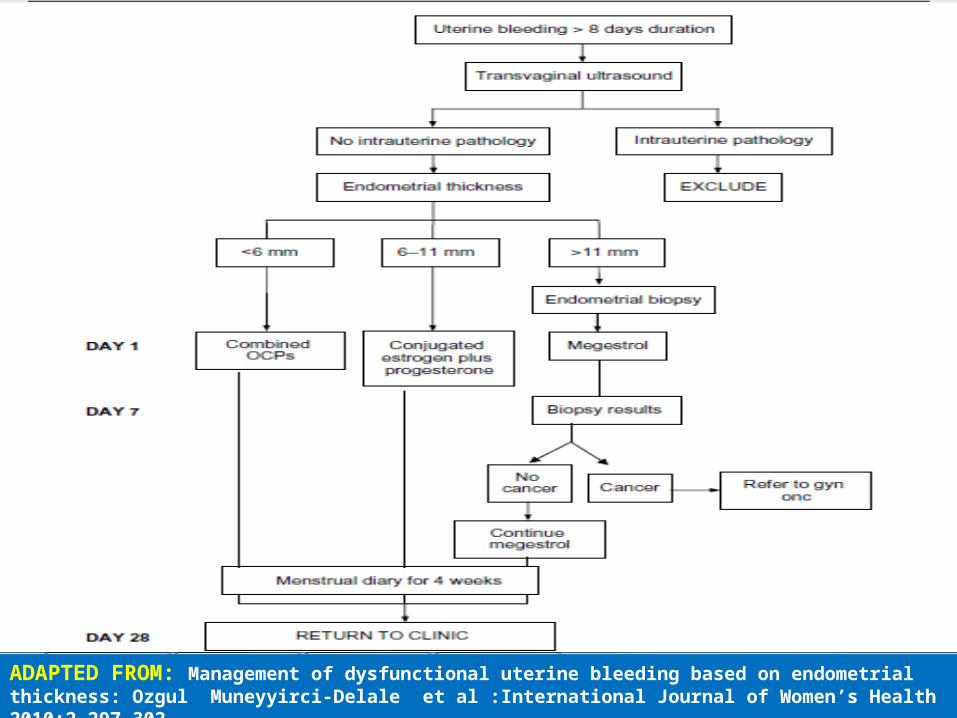
ADAPTED FROM: Management of dysfunctional uterine bleeding based on endometrialthickness: Ozgul Muneyyirci-Delale et al :International Journal of Women’s Health 2010:2 297–302
THE ENDOMETRIAL CYCLE
A CASE REPORT BY: Nagori.et al Done at: Dr.Nagori Institute
for Infertility Published at: J Hum Reprod Sci. 2011 Jan-Apr; 4(1): 43–48 (Journal.11.)
In a woman with severe Asherman's syndrome, curettage
followed by placement of intrauterine contraceptive device
(IUCD) (IUCD with cyclical hormonal therapy) was tried for 6
months, for development of the endometrium.
When this failed, autologous stem cells were tried as an
alternative therapy.
From adult autologous stem cells isolated from patient's
own bone marrow, endometrial angiogenic stem cells were
separated using immunomagnetic isolation.
These cells were placed in the endometrial cavity
under ultrasound guidance after curettage.
Patient was then given cyclical hormonal therapy.
Endometrium was assessed intermittently on
ultrasound. On development of endometrium with a
thickness of 8 mm and good vascularity, in
vitro fertilization and embryo transfer was done.
This resulted in positive biochemical pregnancy
followed by confirmation of gestational sac, yolk sac,
and embryonic pole with cardiac activity on ultrasound.
Endometrial angiogenic stem cells isolated from
autologous adult stem cells could regenerate injured
endometrium not responding to conventional treatment
for Asherman's syndrome.
1.Dutta’s textbook of gynaecology;chap7/83
2.Jeffcoate’s Gynecology 7th ed/79
3.Williams Obstetrics21st ed/66-76 ; 23rded/chap 3
4.Best & Taylor Physiology 13th ed/968-69
5.Physiology of reproduction ,Odell& moyer /35-36
6.Boron Physiology 2006/1161-62
7.Medical Physiology:Rodeney A
Rhodes :4thed:Lippincott:chap37/703
8.Hanes&Taylor:Obsterics & Gynaecology Pathology :Churchill
Livingstone :Vol.1/5th ed/391-409
9.Clinical Gynecology ,Endocrinology and Infertility:Leon
Speroff :Wolters
& Lippincott :7th ed / chap 4/115-131
10.Blaustein's Pathology of the Female Genital Tract,; A.Blaustein,
R.Kurman:Springer:5th ed/421-461
11.Knobil and Neill's Physiology of Reproduction:J.Neill :
Elsevier academic Press , 3rd Edition :vol.1/chap.9/368
Textbook Reference
12.Handbook on ASSISTED REPRODUCTIVE TECHNOLOGIES A guide for
patients :revised 2011:Pg:1-27:AMERICAN SOCIETY FOR REPRODUCTIVE
MEDICINE.
SPL-1: Mazur MT, Kurman RJ. Normal endometrium and infertility evaluation.
In: Mazur MT, Kurman RJ, editors. Diagnosis of endometrial biopsies and
curettings: A practical approach. 2 nd ed. New York: Springer Verlag; 2005. p.
7-33.
SPL-2: David K Gardner : Textbook of Assisted Reproductive Technologies .3rd
edn/648-652
Atlas: Di Fiore’s Atlas of Histology with Functional Correlations:
Victor P. Eroschenko : Lippincott Williams & Wikkins : 12th
Edition ;Chapter 21:Page 525-531
Atlas: Histology :A Text and Atlas :Michael H Ross : 6th ed/Figure23.16
B:Lippincott;Wolters kluwer
Journal.2. : Christine Bergeron: Morphological changes and protein
secretion induced by progesterone in the endometrium during the luteal
phase in preparation for nidation : Human Reproduction, Vol. 15, (Suppl.
1), pp. 119-128, 2000 .
Journal.3. : Garry et al : A re-appraisal of the morphological changes
within the endometrium during menstruation: a hysteroscopic,
histological and scanning electron microscopic study : Human
Reproduction, Vol.1, No.1 pp. 1–9, 2009
Journal References
Journal.1:I.Mylonas et al :Steroid receptors ERα, ERß, PR-A and PR-B are
differentially expressed in normal and atrophic human
endometrium :Histol Histopathol (2007) 22: 169-176
Journal.5. :Neeta Singh et al :Predictive value of endometrial thickness,
pattern and sub-endometrial blood flows on the day of hCG by 2D doppler
in in-vitro fertilization cycles: A prospective clinical study from a tertiary
care unit : J Hum Reprod Sci. 2011 Jan-Apr; 4(1): 29–33.
Journal.6. :Narendra Malhotra et al :Endometrial receptivity and scoring
of predictions for implantation and new markers : Dorland school journal
of ultrasound in obstetrics and gynaecology:october-december:2010
4(4);439-446
Journal.4. :Narendra Malhotra et al :Rational Use of TVS/Color and 3D in
Evaluating Subfertile Women : Donald School Journal of Ultrasound in
Obstetrics and Gynecology, July-September 2011;5(3):273-28
Journal.9. Gleicher N,Vidali A ,Barad DH: Successful treatment of
unresponsive thin endometrium: Fertil Steril. 2011 May;95(6):2123.e13-7.
Journal.8. Ozgul Muneyyirci-Delale et al :Management of dysfunctional
uterine bleeding based on endometrial thickness: :International Journal
of Women’s Health 2010:2 297–30
Journal.7.: Geoffrey Sher et al :Vaginal sildenafil(viagra):A preliminary
report of a novel method to improve uterine artery blood flow and
endometrial development in patients undergoing IVF:Human
Reproduction :2000 :vol 15 no.4 pp.806-809
Journal.10. Gleicher N et al :A pilot cohort study of granulocyte colony-
stimulating factor in the treatment of unresponsive thin endometrium
resistant to standard therapies. Hum Reprod 2013 Jan;28(1):172-7
Journal.11. Pratap Kumar and Siddharth Mahajan : Preimplantation and
postimplantation therapy for the treatment of reproductive failure:J Hum
Reprod Sci. 2013 Apr-Jun; 6(2): 88–92
Journal.12. Nagori CB et al Endometrial regeneration using autologous adult
stem cells followed by conception by in vitro fertilization in a patient of severe
Asherman's syndrome:J Hum Reprod Sci 2011 Jan;4(1):43-8

THANKS FOR PATIENT LISTENING