endoluminal metastasis of colon cancer to the urinary bladder via the ureter: report of a case
TRANSCRIPT
Surg Today (2010) 40:1093–1096DOI 10.1007/s00595-009-4192-5
Reprint requests to: L. BassoReceived: September 7, 2009 / Accepted: November 5, 2009
Case Report
Endoluminal Metastasis of Colon Cancer to the Urinary Bladder via the Ureter: Report of a Case
ANDREA GIULIANI1, GASPARE GALATI
1, MARTINO DEMORO1, MICHELE SCIMÒ
1, ANTONIO CIARDI2, and LUIGI BASSO
1
1 Department of Surgery “Pietro Valdoni”, University of Rome “Sapienza” 1st Medical School, Policlinico “Umberto I”, viale del Policlinico 155, 00161 Rome, Italy2 Department of Experimental Medicine and Pathology, Policlinico “Umberto I”, Rome, Italy
AbstractA 67-year-old woman was admitted for intermittent gross hematuria. Her medical history included a right colectomy for cancer of the ascending colon and removal of metastatic nodes adjacent to the right internal iliac vessels, respectively at 63 and 65 years of age. Cystos-copy detected a semi-pedunculated, nonpapillary (3.5–4 cm diameter) tumor situated above the right ure-teral orifi ce. The histological evaluation of the resected specimen revealed metastatic colonic adenocarcinoma. The history and pathological fi ndings were consistent with a mechanism of endoluminal implantation of ade-nocarcinoma of the large bowel to the bladder via the right ureter.
Key words Endoluminal · Metastasis · Colon · Cancer · Urinary · Bladder · Ureter
Introduction
The urinary bladder may be directly invaded by tumors of the rectum, prostate, and female genital tract,1–3 while metastases from adjacent or distant organs, via the hematic or lymphatic stream, are rare.4–7 Endoluminal secondary tumors that metastasize via the ureter are anecdotal and have never been reported in the English language literature.8 Any adenocarcinoma of the bladder should raise the suspicion of a distant primary cancer, and the histological similarity between primary bladder adenocarcinoma and metastatic colorectal ade-nocarcinoma can be challenging for the pathologist.9 This report presents a case of endoluminal implantation of adenocarcinoma of the large bowel to the bladder via the right ureter.
Case Report
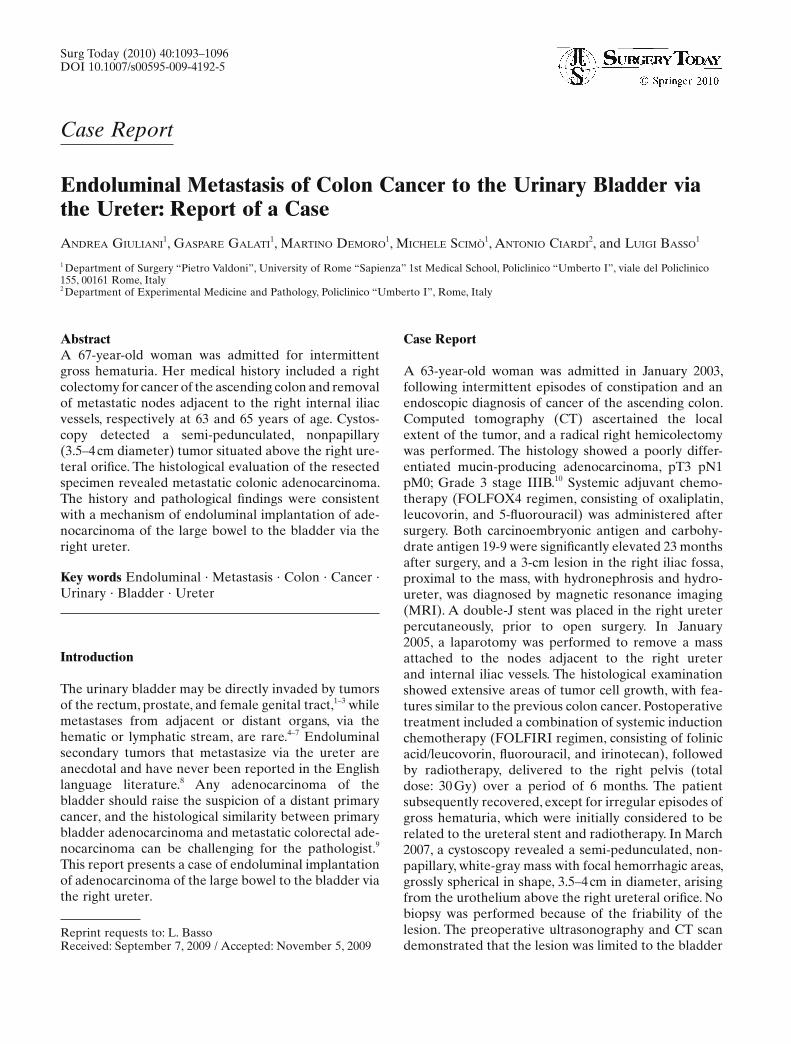
A 63-year-old woman was admitted in January 2003, following intermittent episodes of constipation and an endoscopic diagnosis of cancer of the ascending colon. Computed tomography (CT) ascertained the local extent of the tumor, and a radical right hemicolectomy was performed. The histology showed a poorly differ-entiated mucin-producing adenocarcinoma, pT3 pN1 pM0; Grade 3 stage IIIB.10 Systemic adjuvant chemo-therapy (FOLFOX4 regimen, consisting of oxaliplatin, leucovorin, and 5-fl uorouracil) was administered after surgery. Both carcinoembryonic antigen and carbohy-drate antigen 19-9 were signifi cantly elevated 23 months after surgery, and a 3-cm lesion in the right iliac fossa, proximal to the mass, with hydronephrosis and hydro-ureter, was diagnosed by magnetic resonance imaging (MRI). A double-J stent was placed in the right ureter percutaneously, prior to open surgery. In January 2005, a laparotomy was performed to remove a mass attached to the nodes adjacent to the right ureter and internal iliac vessels. The histological examination showed extensive areas of tumor cell growth, with fea-tures similar to the previous colon cancer. Postoperative treatment included a combination of systemic induction chemotherapy (FOLFIRI regimen, consisting of folinic acid/leucovorin, fl uorouracil, and irinotecan), followed by radiotherapy, delivered to the right pelvis (total dose: 30 Gy) over a period of 6 months. The patient subsequently recovered, except for irregular episodes of gross hematuria, which were initially considered to be related to the ureteral stent and radiotherapy. In March 2007, a cystoscopy revealed a semi-pedunculated, non-papillary, white-gray mass with focal hemorrhagic areas, grossly spherical in shape, 3.5–4 cm in diameter, arising from the urothelium above the right ureteral orifi ce. No biopsy was performed because of the friability of the lesion. The preoperative ultrasonography and CT scan demonstrated that the lesion was limited to the bladder
1094 A. Giuliani et al.: Endoluminal Metastasis of Colon Cancer
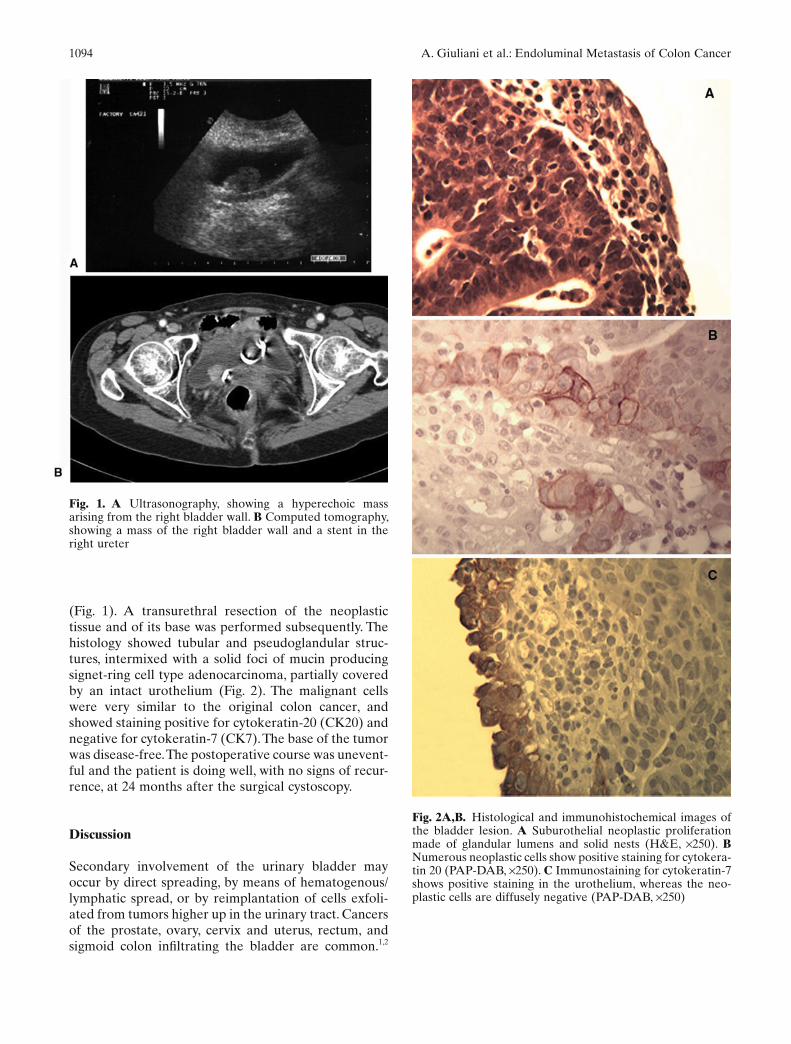
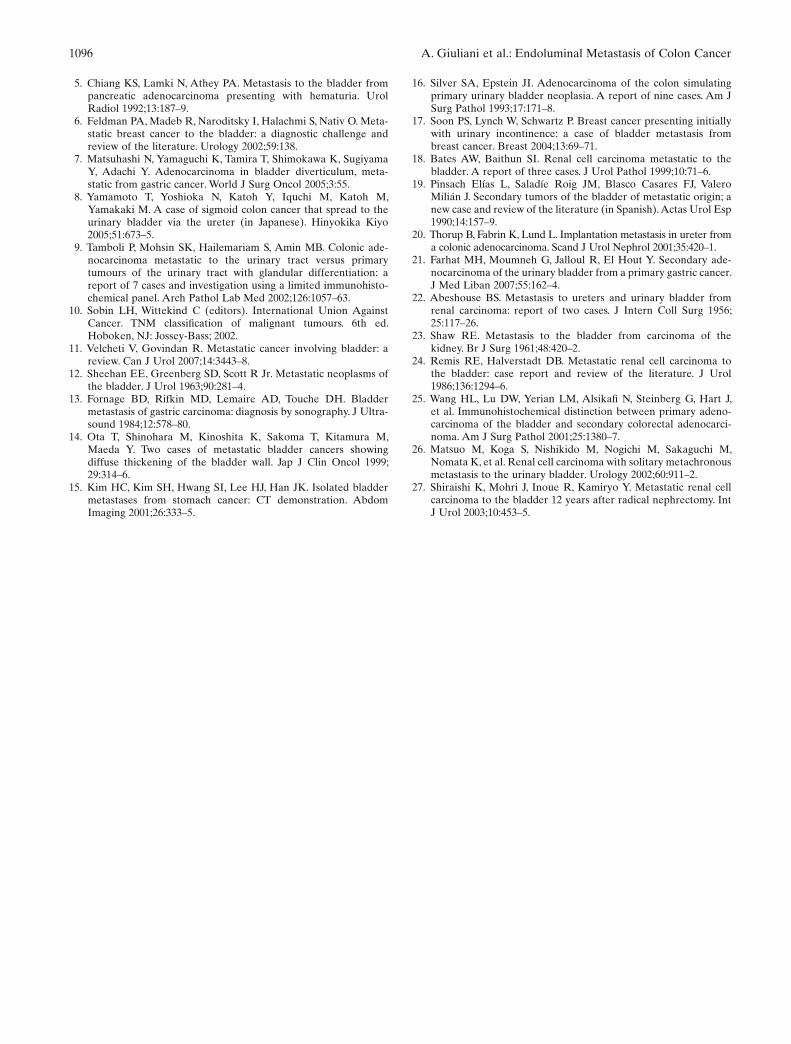
(Fig. 1). A transurethral resection of the neoplastic tissue and of its base was performed subsequently. The histology showed tubular and pseudoglandular struc-tures, intermixed with a solid foci of mucin producing signet-ring cell type adenocarcinoma, partially covered by an intact urothelium (Fig. 2). The malignant cells were very similar to the original colon cancer, and showed staining positive for cytokeratin-20 (CK20) and negative for cytokeratin-7 (CK7). The base of the tumor was disease-free. The postoperative course was unevent-ful and the patient is doing well, with no signs of recur-rence, at 24 months after the surgical cystoscopy.
Discussion
Secondary involvement of the urinary bladder may occur by direct spreading, by means of hematogenous/lymphatic spread, or by reimplantation of cells exfoli-ated from tumors higher up in the urinary tract. Cancers of the prostate, ovary, cervix and uterus, rectum, and sigmoid colon infi ltrating the bladder are common.1,2
Fig. 1. A Ultrasonography, showing a hyperechoic mass arising from the right bladder wall. B Computed tomography, showing a mass of the right bladder wall and a stent in the right ureter
Fig. 2A,B. Histological and immunohistochemical images of the bladder lesion. A Suburothelial neoplastic proliferation made of glandular lumens and solid nests (H&E, ×250). B Numerous neoplastic cells show positive staining for cytokera-tin 20 (PAP-DAB, ×250). C Immunostaining for cytokeratin-7 shows positive staining in the urothelium, whereas the neo-plastic cells are diffusely negative (PAP-DAB, ×250)

A. Giuliani et al.: Endoluminal Metastasis of Colon Cancer 1095
Primary colorectal tumors account for 20% of second-ary tumors involving the bladder, and for 30% of those directly invading the bladder.1 Similarly, abdominal or extra-abdominal cancers, which are widely dissemi-nated throughout the peritoneal surface of the abdomen and pelvis, frequently invade the bladder wall at the level of the trigone, posterior wall, or fundus.2 In these cases, the involvement originates at the outer wall of the bladder and progressively reaches the urothelial lining. In contrast, abdominal or extra-abdominal malignan-cies very rarely involve the bladder wall as isolated metastases. However, Velcheti and Govindan,11 after reviewing a total of 2405 abstracts published from 1953 to June 2005, found 264 cases of metastases to the bladder from several primaries (10.9%) including, in order of frequency, genitourinary tract (35%), large bowel (28.5%), melanoma (9.5%), breast (8.5%), and stomach (8%). The mechanism of metastasis to the urinary bladder, as well as the factors promoting this process, are obscure, although hematogenous and/or lymphatic spreads should always be taken into account. In these cases, a sequence of events beginning with deposition of cancer cells in the outer bladder muscle wall, and secondary involvement of more superfi cial layers can be hypothesized. This conclusion relies on imaging studies and macroscopic features that show focal or diffuse thickening of the bladder wall,5,12–15 as well as on microscopic fi ndings, showing metastatic infi ltration under an overlying intact urothelium.13,16,17 Metastases to the urinary bladder of cells exfoliated from tumors higher up in the urinary tract, such as renal carcinomas, are possible, albeit clinically rare and rela-tively unimportant.18 In addition, direct hematogenous metastases that directly invade the urothelium have been reported,19–21 and this rare possibility should also be considered when encountering such cases. Other mechanisms of spreading of renal tumors to the bladder have been taken into account, such as retrograde embo-lization of cancer cells through the venous or lymphatic vessels.22–24 The carcinomatous cells in the current patient may have exfoliated endoluminally from the stented stenosis of the ureter, and deposited in the vesicle mucosal layer. This hypothesis is supported by (1) the location of the tumor, in the immediate proxim-ity of the right ureteral orifi ce, (2) the protruding, semi-pedunculated appearance, (3) the microscopic observation that the urothelium did not totally overlay the tumor, and (4) the histologically proven disease-free base of the tumor. In addition, the imaging studies and the cystoscopy during the 18-month follow-up period did not show any recurrence of the disease. Other authors have similarly hypothesized spreading of malig-nant cells via the ureter as a possible mechanism of involvement of the bladder from cancer of the large bowel.8 Involvement of the bladder can be assessed by
ultrasonography, CT scan, MRI, and cystoendoscopy. Detection of an adenocarcinoma in the bladder should raise the suspicion of either a metastatic cancer from, mainly, a gastrointestinal focus, or from the upper urinary tract, as primary bladder adenocarcinoma is only found in 0.5%–2% of all primary bladder cancers.1 A thorough differentiation between the primary enteric-type adenocarcinoma of the bladder and secondary colorectal adenocarcinoma involving the bladder should be performed, because these two conditions are mor-phologically indistinguishable.1 An immunohistochemi-cal panel including CK7, CK20, villin, and β-catenin can help the diagnosis, because most lesions of colorectal origin have a CK7 negative profi le while showing a CK20-, villin-, and β-catenin-positive immunoprofi le.9,25 The lesion in the current patient was CK7-negative and CK20-positive, and this supported the colorectal origin of the metastatic lesion, although villin and β-catenin were not evaluated. The mechanism of involvement of the urinary bladder in colorectal carcinoma infl uences further treatment. Locally advanced cancer directly involving the bladder wall can be successfully treated by an en bloc partial or total cystectomy.3 The treatment of secondary adenocarcinomas, depending on the stage of the primary tumor and on its location, extent, and number of bladder metastases, can be performed by an open or transurethral resection, and/or by a combina-tion of chemo- and radiotherapy. However, due to the rarity of these conditions and to the lack of any large series comparing the various surgical options, the optimal treatment is unclear. Metastases due to endo-luminal implantation of cancer cells, as observed in the present case, may only require local resection.26,27
The possibility of metastases should be considered in patients with a history of colonic adenocarcinoma who present with adenocarcinoma of the bladder. The use of an immunohistochemical panel is recommended to differentiate between primary and metastatic tumors.
References
1. Melicow MM. Tumours of the urinary bladder: a clinico-patho-logical analysis of over 2500 specimens and biopsies. J Urol 1955;74:498–521.
2. Bates AW, Baithun SI. Secondary neoplasms of the bladder are histological mimics of nontransitional cell primary tumours: clini-copathological and histological features of 282 cases. Histopathol-ogy 2000;36:32–40.
3. Kobayashi T, Kamoto T, Sugino Y, Takeuchi H, Habuchi T, Ogawa O. High incidence of urinary bladder involvement in car-cinomas of the sigmoid and rectum: a retrospective review of 580 patients with colorectal carcinoma. J Surg Oncol 2003;84:209–14.
4. van Driel MF, Ypma AF, van Gelder B. Gastric carcinoma meta-static to the bladder. Br J Urol 1987;59:193–4.
1096 A. Giuliani et al.: Endoluminal Metastasis of Colon Cancer
5. Chiang KS, Lamki N, Athey PA. Metastasis to the bladder from pancreatic adenocarcinoma presenting with hematuria. Urol Radiol 1992;13:187–9.
6. Feldman PA, Madeb R, Naroditsky I, Halachmi S, Nativ O. Meta-static breast cancer to the bladder: a diagnostic challenge and review of the literature. Urology 2002;59:138.
7. Matsuhashi N, Yamaguchi K, Tamira T, Shimokawa K, Sugiyama Y, Adachi Y. Adenocarcinoma in bladder diverticulum, meta-static from gastric cancer. World J Surg Oncol 2005;3:55.
8. Yamamoto T, Yoshioka N, Katoh Y, Iquchi M, Katoh M, Yamakaki M. A case of sigmoid colon cancer that spread to the urinary bladder via the ureter (in Japanese). Hinyokika Kiyo 2005;51:673–5.
9. Tamboli P, Mohsin SK, Hailemariam S, Amin MB. Colonic ade-nocarcinoma metastatic to the urinary tract versus primary tumours of the urinary tract with glandular differentiation: a report of 7 cases and investigation using a limited immunohisto-chemical panel. Arch Pathol Lab Med 2002;126:1057–63.
10. Sobin LH, Wittekind C (editors). International Union Against Cancer. TNM classifi cation of malignant tumours. 6th ed. Hoboken, NJ: Jossey-Bass; 2002.
11. Velcheti V, Govindan R. Metastatic cancer involving bladder: a review. Can J Urol 2007;14:3443–8.
12. Sheehan EE, Greenberg SD, Scott R Jr. Metastatic neoplasms of the bladder. J Urol 1963;90:281–4.
13. Fornage BD, Rifkin MD, Lemaire AD, Touche DH. Bladder metastasis of gastric carcinoma: diagnosis by sonography. J Ultra-sound 1984;12:578–80.
14. Ota T, Shinohara M, Kinoshita K, Sakoma T, Kitamura M, Maeda Y. Two cases of metastatic bladder cancers showing diffuse thickening of the bladder wall. Jap J Clin Oncol 1999;29:314–6.
15. Kim HC, Kim SH, Hwang SI, Lee HJ, Han JK. Isolated bladder metastases from stomach cancer: CT demonstration. Abdom Imaging 2001;26:333–5.
16. Silver SA, Epstein JI. Adenocarcinoma of the colon simulating primary urinary bladder neoplasia. A report of nine cases. Am J Surg Pathol 1993;17:171–8.
17. Soon PS, Lynch W, Schwartz P. Breast cancer presenting initially with urinary incontinence: a case of bladder metastasis from breast cancer. Breast 2004;13:69–71.
18. Bates AW, Baithun SI. Renal cell carcinoma metastatic to the bladder. A report of three cases. J Urol Pathol 1999;10:71–6.
19. Pinsach Elías L, Saladíe Roig JM, Blasco Casares FJ, Valero Milián J. Secondary tumors of the bladder of metastatic origin; a new case and review of the literature (in Spanish). Actas Urol Esp 1990;14:157–9.
20. Thorup B, Fabrin K, Lund L. Implantation metastasis in ureter from a colonic adenocarcinoma. Scand J Urol Nephrol 2001;35:420–1.
21. Farhat MH, Moumneh G, Jalloul R, El Hout Y. Secondary ade-nocarcinoma of the urinary bladder from a primary gastric cancer. J Med Liban 2007;55:162–4.
22. Abeshouse BS. Metastasis to ureters and urinary bladder from renal carcinoma: report of two cases. J Intern Coll Surg 1956;25:117–26.
23. Shaw RE. Metastasis to the bladder from carcinoma of the kidney. Br J Surg 1961;48:420–2.
24. Remis RE, Halverstadt DB. Metastatic renal cell carcinoma to the bladder: case report and review of the literature. J Urol 1986;136:1294–6.
25. Wang HL, Lu DW, Yerian LM, Alsikafi N, Steinberg G, Hart J, et al. Immunohistochemical distinction between primary adeno-carcinoma of the bladder and secondary colorectal adenocarci-noma. Am J Surg Pathol 2001;25:1380–7.
26. Matsuo M, Koga S, Nishikido M, Nogichi M, Sakaguchi M, Nomata K, et al. Renal cell carcinoma with solitary metachronous metastasis to the urinary bladder. Urology 2002;60:911–2.
27. Shiraishi K, Mohri J, Inoue R, Kamiryo Y. Metastatic renal cell carcinoma to the bladder 12 years after radical nephrectomy. Int J Urol 2003;10:453–5.